medicine matters
DESCRIPTION
Medicine Matters Issue 33TRANSCRIPT
Issue 33July 2011
medicineat the Leeds School of Medicine
Bradford Health Research - Then and Now
ALPS - A Review
30 years of the CL Fund
The Clinical Trials Research Unit
Community Education
Workhouse Chapel Anniversary
From Leeds to Helmand:Providing intimate medical support to deployed troops
In the previous edition we saw how the wool industry played a signifi cant role in the establishment of the Yorkshire College and how research into the properties of wool by William Astbury at the University of Leeds led to an understanding of molecular structure. The sheep, which fi rst appeared on the arms of the Yorkshire College, and whose fl eece provided that wool, is retained on the shield of the Medical School. However the fl eeces from certain sources also harboured disease and in this edition we hear how research in Bradford and Leeds over a period of fi fty years led to the discovery of the causes of anthrax in wool-sorters that was such a scourge of the woollen industry in Bradford and elsewhere in the West Riding. The Leeds – Bradford research link now enters a new phase of development.
Occupational diseases are less of a concern to medical researchers nowadays but the lack of work arising from recession and unemployment also has its consequences for health as demonstrated by Professor Martin McKee, who delivered this year’s Thackrah Lecture, named in honour of Charles Turner Thackrah, a founder of the School and author of the seminal work on occupational diseases.
The occupation probably with the highest risk is a career in a combat unit in our armed forces. Currently about ten of our graduates are serving in the armed services and in this edition Major Leon Roberts (qualifi ed 2000) describes his career and his recent tour in Afghanistan. With additional photographs provided by Army Media Services our centre-page spread gives a graphic picture of the role of medics in the Medical Emergency Response Teams (MERTs) and Base Hospitals in Helmand province.
Also highlighted is the Clinical Trials Research Unit. Within its current portfolio is research led by Mr David Jayne in robotic-assisted keyhole surgery. In mid-June this year the Royal College of Surgeons called for more funds for surgical research of this type. Leeds is already ahead of the game.
The next generation of graduates is developing their skills and in this edition we celebrate ten years of Community Education in the curriculum. We also hear of the award-winning work of ALPS to ensure that assessment and learning practices are right for the task. We highlight the achievements of our students and our appreciation of alumni generosity in assisting some of them to achieve their potential. Please visit our website www.leeds.ac.uk/medicine/matters to see more on these stories and additional ones for which there is insuffi cient room in these pages. I hope you enjoy this edition of Medicine Matters.
Bill MathieEditor, Medicine Matters
medicine
Edited by Bill MathieEmail: [email protected]
Correspondence address:The Editor, Medicine Matters,School of Medicine,Worsley BuildingUniversity of Leeds, LS2 9JT
Medicine MattersIs produced bi-annually by Leeds School of Medicine and distributed by the University Alumni Offi ce to over 8,000 alumni, and by the School to hundreds of others associated with medicine in Leeds.
AlumniThe Alumni Offi ce would like you to stay in touch, so please let it know of any changes to your details by emailing [email protected]
Or write to Alumni & Development Team, EC Stoner Building, University of Leeds, Leeds, LS2 9JT.
You can also visit its website at www.alumni.leeds.ac.uk and join the alumni online community.
Design: Leigh Marklew
AcknowledgmentsIn addition to those acknowledged in each article, thanks too to Jason Joy, Bradford Hospitals NHS Foundation Trust, Mr Richard Watt, Army Media and Communications, HQLF, Gerry McGowan, Bradford Museums and Galleries, Crestina Forcina, Wellcome Trust, Vicky Grindrod, West Yorkshire Archive Service, Anthonia James and Gill Rizzello, LIHS and Dr David Church.
Picture CreditsUniversity of Leeds unless stated.
Front cover imagePre-hospital in-transit care aboard a Chinook CH47 helicopter by the Medical Emergency Response team (MERT), Helmand, Afghanistan. (PO Sean Clee 3 Cdo Bde / © MoD Crown Copyright.)
More on the website This and Issues 25 onwards may be viewed on the School website www.leeds.ac.uk/medicine/matters

expansion of clinical research at Bradford in conjunction with Bradford NHS organisations.
The Bradford Institute for Health Research was established in premises in Field House on the Bradford Royal Infi rmary site. It has been the home of new research, including the Born in Bradford project (see Medicine Matters Issue 30, February 2010) led by Professor John Wright (MBChB Leeds 1987) who is also Director of the Institute, and the internationally recognised stroke research led by Professor John Young and Professor Anne Forster of the Medical School’s Academic Unit of Elderly Care and Rehabilitation.
BACKGROUNDBradford hospitals have provided clinical training opportunities for medical students from Leeds for over forty years, if not longer. In the modern era these well-established links were reinforced in 2002 with the partnership with Bradford University in the provision of Foundation Year opportunities to aspiring medical students as part of the School’s Widening Access programme
(see Medicine Matters Issue 29, July 2009), which now approaches its tenth successful year. This provision of undergraduate opportunities was matched by an
Alongside these high-profi le public health research programmes, the Institute also focuses on research which directly contributes to improving patient care in a range of areas including maternal and child health, diabetes, genetics, cancer and wound care.
The success of the Institute over the intervening years has led to a rapid expansion of its activities. Since its inception fi ve years ago, research income from national and international funding bodies has grown to £5 million a year. It is the second biggest recruiter of patients to research studies in the region.
Matters Issue 30, February 2010) led sby Professor John Wright (MBChB Leeds 1987) who is also Director of the Institute, and the internationally recognised stroke research led by Professor John Young and Professor Anne Forster of the Medical School’s Academic Unit of Elderly Care and Rehabilitation.
School’s Widening Access programme (see Medicine Matters
Issue 29, July 2009), which now approaches its tenth successful year. This provision of undergraduate opportunities was matched by an
expansion of its activities. Since its inception fi ve years ago, research income from national and international funding bodies has grown to £5 million a year. It is the second biggest recruiter of patients to research studies in the region.
Medicine Matters Issue 33, July 2011
1
Leeds – Bradford Links strengthened with a new phase of development for Bradford Institute for Health Research

medicine
2
(Top) The Bradford Institute for Health Research’s new £2.25million extension.(Middle) High Sheriff of West Yorkshire, Richard Clough, and Bradford Lord Mayor, Councillor Peter Hill, present Dame Sally Davies with a David Hockney print ‘A Bounce for Bradford’ (Bradford Teaching Hospitals NHS Foundation Trust)(Left) Dame Sally Davies (Bradford Teaching Hospitals NHS Foundation Trust)
EXPANSION New premises were needed and in March Professor Dame Sally Davies, Director General of Research and Development and Chief Scientifi c Adviser for the Department of Health and NHS, offi cially opened the Institute’s £2.25 million extension. The opening was integral to the Institute’s inaugural conference. Dame Sally in her address to the delegates at the conference said “Through the National Institute for Health Research (NIHR) we have transformed health research in this
country. A key part of that has been to encourage partnerships between researchers based in leading academic institutions and the NHS. Research is vital in providing the new knowledge needed to improve health outcomes and reduce inequalities.”
The Institute is a partnership between the primary and secondary care NHS Trusts in Bradford and Airedale and the Universities of Bradford, Leeds and York. It now employs nearly 100 research and support staff from these organisations.
Leeds Medical School contributors at the conference included Professor Anne Forster on stroke research and how research trials are improving the care of patients, Professor John Young on community hospitals, Dr Rebecca Lawton on patient involvement in research and Dr Ghazala Mir on addressing depression in Muslim communities.
THE IMPORTANCE OF THE BIHR DEVELOPMENTProfessor David Cottrell, Dean of the School of Medicine, on the signifi cance of this development in Bradford: “We are committed to working with NHS Trusts in Bradford to develop a major teaching and research centre to support undergraduate and postgraduate teaching, and to develop research programmes that will make a difference locally and globally. It is very encouraging to see the success that Bradford is having in all these areas and we look forward to continuing to work with our Bradford colleagues in the future.”
The Medical School is delighted to record that Professor Dame Sally Davies received an Honorary Degree from the University of Leeds in July 2011.
3
THE WOOLLEN INDUSTRY AND ILL-HEALTHThe consequences of employment on health had fi rst been publicly addressed by Charles Turner Thackrah, the Leeds doctor who published his seminal work in 1832 under the title of On the effects of Arts, Trades and Professions on Health and Longevity. We still celebrate his name in the Medical School today, through the Thackrah Building, home to the Leeds Institute for Health Sciences and the Thackrah Lecture.
Of wool industry workers Thackrah stated in 1832 that “Wool-sorters are occasionally annoyed with dust from lime which in some kinds of wool is used for separating the fl eece from the skin. No sensible effect is produced on health.” Wool-sorters were not to enjoy such benign conditions for long.
EARLY INVESTIGATIONS INTO WOOL-SORTERS DISEASEIn 1847, ten years after the introduction of alpaca and mohair into the West Riding, the earliest instance of a disease specifi c to wool-sorters was noted. It was such a specifi c disease that it was known as ‘maladie de Bradford’. In 1857 Dr John Henry Bell set up in practice in Bradford. Though born in Bradford he had grown up in Scotland, became an apprentice in Thornton, Ripon and then Leeds and attended lectures at Leeds Medical School. From his case-books we can note that the guiding rules of his professional life were: ‘Observe carefully, read thoughtfully, record accurately.’
He contended that every doctor had a duty to medical science and that each should pursue some line of original research and thus add to medical knowledge. He investigated hundreds of cases, derived from infected blood on fl eeces and skins, and suffered by wool-sorters, which generally resulted in death within one week of the fi rst signs appearing.
The Lancet in December 1879 ran an editorial and in February 1880 Dr Bell spoke to the Bradford Medico-Chirurgical Society and identifi ed the infective agent as a bacterium called the Bacillus Anthrax. The Society decided to form a commission of its own members to investigate the whole subject and reported at the end of 1882.
Following much medical and public debate and formal enquiries, rules (Bradford Rules) for the cleaning of fl eeces and safety of employees were introduced in 1884. However the infection of employees, though diminished, continued to remain high while these rules remained in force. In 1905 they were reviewed by the Bradford and District Anthrax Investigation Board.
Medical Research in Bradford – an illustrious precedent
Medicine Matters Issue 33, July 2011
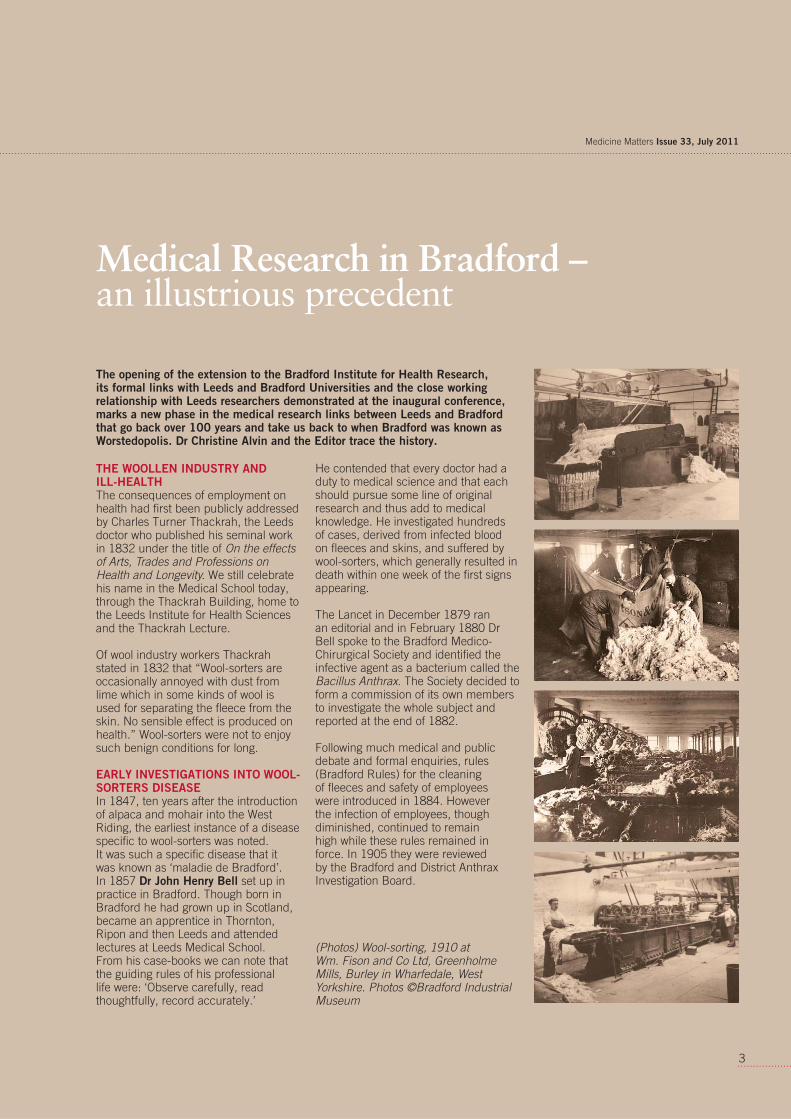
(Photos) Wool-sorting, 1910 at Wm. Fison and Co Ltd, Greenholme Mills, Burley in Wharfedale, West Yorkshire. Photos ©Bradford Industrial Museum
The opening of the extension to the Bradford Institute for Health Research, its formal links with Leeds and Bradford Universities and the close working relationship with Leeds researchers demonstrated at the inaugural conference, marks a new phase in the medical research links between Leeds and Bradford that go back over 100 years and take us back to when Bradford was known as Worstedopolis. Dr Christine Alvin and the Editor trace the history.
medicine
4
FURTHER INVESTIGATIONS INTO ANTHRAXIt was Dr Friederich W Eurich who was to take forward the investigations. He had grown up in Bradford’s German business community, trained in Edinburgh and returned to Bradford in 1896 to be a general practitioner. He had appointments at the Bradford Infi rmary and at the Eye and Ear Hospital where Dr Bell was consultant surgeon and where he came across his fi rst cases of anthrax. He worked with Dr Bell until the latter’s death at the age of 74 in 1906.
In 1900 he became a class assistant (an honorary position) at the Medical Department of the Yorkshire College, Leeds, teaching practical toxicology. At the end of that year he was appointed bacteriologist for the newly established Bradford Pathological and Bacteriological Laboratory and set up a research laboratory in a small room off a biology teaching laboratory at Bradford Technical College. In 1905 he was appointed by the Bradford and District Anthrax Investigation Board to study the origins of the anthrax bacilli. The isolation of the bacilli from the fl eeces and skins was undertaken by Dr Eurich and an assistant. But Dr Eurich was refused permission by the Bradford authorities to carry out animal experiments at the College. He was however able to undertake them at the Medical School at Leeds, where he was already teaching and which was now (since 1904) part of Leeds University.
On the resignation in 1908 of Professor Campbell, who held the fi rst chair of Forensic Medicine at Leeds, Dr Eurich became Professor of Forensic Medicine, a position he held until his own retirement in 1932, a period of 24 years. For this he was paid an honorarium of £38 p.a., a sum that was never increased! His investigations into the origins and causes and the introduction of measures to prevent it occupied him through much of his career. The fi rst 10 years were largely spent on identifying the bacilli and their origin. Two forms, internal anthrax derived from inhalation, and external or cutaneous anthrax, affl icted the workers
in the wool trades. Between 1900 and 1909 there were over 400 cases of anthrax nationally, half of which were in Bradford of whom 49 died in Bradford and 72 died elsewhere. Between 1916 and 1918 there were 194 cases nationally.
REMOVING THE EXPOSURE TO RISKIn 1913 a Home Offi ce Committee of Enquiry was set up commissioning Professor Eurich to devise a method of disinfecting hair and wool. In 1918 the recommendations for disinfecting stations were made and in 1921 the disinfecting station in Liverpool was opened. Cases of inhalation anthrax dropped dramatically – after 1922 there were only 5 and the last was in 1931. Cutaneous anthrax, treatable with penicillin and other antibiotics, has continued at low levels.
On his retirement in 1932 Professor Eurich received richly deserved accolades from the West Riding and the woollen industry for his achievements in improving health and reducing mortality. On his death in 1945 the Yorkshire Observer recorded ‘he did so much to conquer the disease of anthrax and [his] contributions in the cause of medicine were outstanding.’
Christine Alvin is a retired Medical Librarian, formerly at Bradford Royal Infi rmary. Her research into Dr Bell’s career and the proceedings of the Bradford Medico-Chirurgical Society, led to a PhD awarded by the University of Bradford (unpublished).
ReferenceDr Eurich of Bradford, by Margaret F Bligh, published by James Clark and Co, 1960
Professor FW Eurich, c 1914 Watercolour by John Sowden, , reproduced with the permission of Bradford Museums and Galleries.
Further information on the Bradford Medico-Chirurgical Society – the fi rst 50 years 1863-1913 may be found on the Magazine’s webpages at www.medicine.leeds.ac.uk/medicine/matters
Readers interested in the story of Forensic Pathology – the chair of which at Leeds was held by Professor Eurich between 1908 and 1932 - may be interested in a double bill of lectures on Forensic Pathology on Saturday 10th September at the Thackray Museum, from 10am to 12noon.
Speakers:Professor Michael GreenEmeritus Professor of Forensic Pathology, University of Sheffi eld on the Development of Forensic Pathology. Professor Green is an alumnus of the Medical School at Leeds (1962). MJ TrowBiographer and novelist, on Jack the Ripper, Forensic Pathology at the time of the Whitechapel murders.
Friends of
55
The HEFCE-funded Assessment & Learning in Practice Settings (ALPS) programme, led by the University of Leeds, came to a successful completion in September 2010 after winning a string of prestigious awards and demonstrating a strong impact across the partnership.
ALPS aim was to ensure that students are confi dent and competent to practise on graduation. This was to be done by improving the assessment and learning opportunities and support that were offered to students whilst training in clinical practice. The vision in 2004 was radical – ALPS aimed to create assessment tools which could be used across professions, allowing, for example, a nurse to assess the
communication skills of a medical student. Furthermore ALPS planned for students to access these assessment tools and learning materials on mobile devices – a technology that was in its infancy at that time.
ALPS did aim high and certainly encountered challenges and diffi culties along the way, as the technology did not always perform as expected. It took time to develop trust across the collaborative partnership and attitudes towards the use of mobile technology were not always positive. However, those high ambitions have been rewarded as ALPS work has been recognized as ground breaking and has infl uenced teaching and learning practices across the partnership. All fi ve universities have adopted learning resources and
approaches piloted by ALPS. They have enhanced staff, student and patient/carer skills and experience in the
areas of collaborative and inter-professional working, as well as
developing expertise in mobile and e-learning.
ALPS COMMON COMPETENCY MAPSALPS worked across the 16 health and
social-care professions to develop competency maps in Communication, Team Working and Ethical Practice,
chosen as they were relevant to all 16 professions. These maps
are now widely used across the ALPS partnership and increasingly beyond it. ‘The achievements of ALPS are a source of great pride and satisfaction to all staff, students and service users who have been involved in the CETL.’ says Professor Trudie Roberts, Director of Leeds Institute of Medical Education and of ALPS.
ALPS ASSESSMENT TOOLSALPS again worked inter-professionally and collaboratively to develop generic assessment tools for use in practice. The assessment tools are mapped to the three ALPS Common Competency Maps and the scenarios they cover are:
• Demonstrating respect for a service user or carer
• Gaining consent• Knowing when to consult or refer• Providing information to colleagues• Working inter-professionally
The tools allow students to gather 360 degree feedback, and include sections on self-assessment, inter-professional peer and practice assessor assessment and service-user/carer assessment. ALPS also developed the Competence in Practice Assessment (CIPA) tool, which can be used by students to record their perception of their own skills and competence. Initially developed to help evaluate the impact of the ALPS programme, this tool is now being developed so that students can use it to help with their own Personal Development Planning.
(continues over)
ALPS is the award-winning programme led by the University of Leeds and partnered by Bradford, Huddersfi eld, Leeds Met and York St John Universities. It was funded by the Centres for Excellence in Teaching and Learning (CETL) initiative of HEFCE for fi ve years in 2005. Tamsin Treasure-Jones (ALPS Programme Manager) and Julie Laxton (ALPS Teaching Fellow) review the work of ALPS and how it is being embedded in teaching and learning practices.
Medicine Matters Issue 33, July 2011
in 2004 was radical – ALPS aimed tocreate assessment tools which could be used across professions, allowing, for example, a nurse to assess the
ALPS work has beenground breaking andteaching and learninthe partnership. Allhave adopted learni
approaches pThey havestudent skills an
areasand work
develmobile and
ALPSCOMALPSthe 1
social-cdevelop coin CommuWorking a
chosen as thall 16 profes
Assessment & Learning in Practice Settings
medicine
6
MOBILE TECHNOLOGYALPS innovative work in developing and evaluating mobile learning and assessment (using mobile technology to support the use of the ALPS maps, tools and other learning resources) has achieved national and international recognition. Awards include:
• IMS Global Learning Impact Gold Award – Winner 2011
• Finalist for ICT Initiative of the Year at the 2010 Times Higher Education Leadership & Management Awards
• Learning Impact Award – EDEN Conference 2010
• Winner of Best HE Innovation at the 2009 Handheld Learning Awards
• Finalist for Best Use of Mobile Learning at the 2009 E-Learning Awards
• Winner of the Mobility Project of the Year Award at Techworld 2008
WHAT NEXT?Although the HEFCE ALPS programme has fi nished, the ALPS work continues thanks to funding from the SHA and a commitment from the ALPS partners to continue to work together. Networks have been set up by staff, who have been involved in ALPS, to support joint working in six areas: mobile learning, e-portfolios, competency mapping, accessibility and technology-use, patient and carer voice and the use of the CIPA tool.
You can fi nd more information about the ongoing work of these networks, as well as all the ALPS outputs (maps, tools, resources and reports), on the ALPS website www.alps-cetl.ac.uk
The ALPS networks will be showcasing their work in September 2011. If you would be interested in attending the Showcase event or are interested in joining any of the ALPS networks then please email [email protected] ALPS is keen to share the knowledge, experience and expertise that we have built up over the last 6 years and to continue to work with others (academics, practice staff, students, patients, industry) to fi nd effective ways of enhancing and supporting student learning in practice.
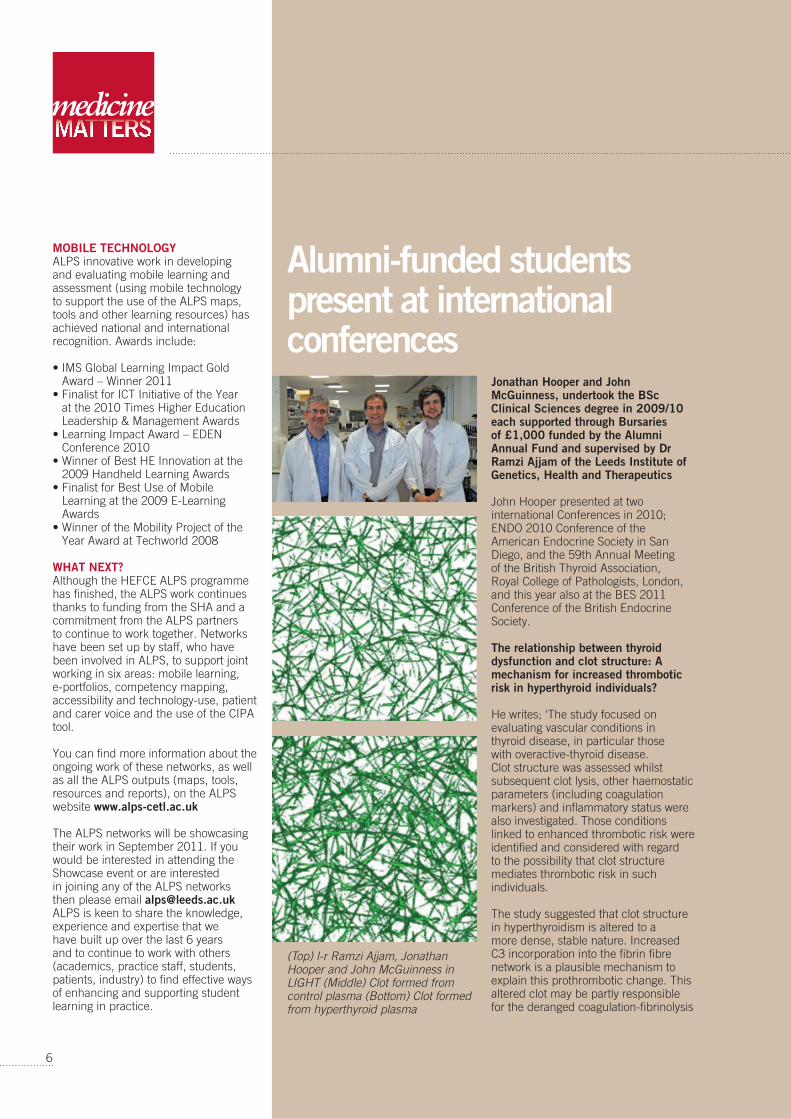
Jonathan Hooper and John McGuinness, undertook the BSc Clinical Sciences degree in 2009/10 each supported through Bursaries of £1,000 funded by the Alumni Annual Fund and supervised by Dr Ramzi Ajjam of the Leeds Institute of Genetics, Health and Therapeutics
John Hooper presented at two international Conferences in 2010; ENDO 2010 Conference of the American Endocrine Society in San Diego, and the 59th Annual Meeting of the British Thyroid Association, Royal College of Pathologists, London, and this year also at the BES 2011 Conference of the British Endocrine Society.
The relationship between thyroid dysfunction and clot structure: A mechanism for increased thrombotic risk in hyperthyroid individuals?
He writes; ‘The study focused on evaluating vascular conditions in thyroid disease, in particular those with overactive-thyroid disease. Clot structure was assessed whilst subsequent clot lysis, other haemostatic parameters (including coagulation markers) and infl ammatory status were also investigated. Those conditions linked to enhanced thrombotic risk were identifi ed and considered with regard to the possibility that clot structure mediates thrombotic risk in such individuals.
The study suggested that clot structure in hyperthyroidism is altered to a more dense, stable nature. Increased C3 incorporation into the fi brin fi bre network is a plausible mechanism to explain this prothrombotic change. This altered clot may be partly responsible for the deranged coagulation-fi brinolysis
Alumni-funded students present at international conferences
(Top) l-r Ramzi Ajjam, Jonathan Hooper and John McGuinness in LIGHT (Middle) Clot formed from control plasma (Bottom) Clot formed from hyperthyroid plasma
7
Medicine Matters Issue 33, July 2011
characterising the vascular environment in hyperthyroidism. If so, clot structure may play a key role in mediating thrombotic risk in hyperthyroid patients.’
John McGuinness’s study was in the Relationship between erectile dysfunction (ED) and cardiovascular risk, through an investigation of fi brin clot structure. He writes ‘ED is strongly associated with cardiovascular risk however the analysis of clot structure suggested that this relationship may be more complex than fi rst thought. Fibrin clots in ED patients have a lower thrombotic tendency than controls, suggesting protective mechanisms against thrombosis and cardiovascular risk.’ He presented his fi ndings this year at the European Society of Sexual Medicine Congress in Malaga, Spain
Further information on this research may be found at www.leeds.ac.uk/light/staff/ajjan_r.html
PRIZE FOR LEEDS CUTTING EDGE The Medical Students’ Surgical Society, Cutting Edge, has been awarded second prize in the ‘national surgical society of the year award 2011’ competition. The School is
delighted to see the Society gain this well-deserved award on
the 10th anniversary of the Society’s founding.
It was awarded by the Royal College of Surgeons (Edinburgh) at the
international UKMSA conference in Bournemouth in May 2011. Held
with the ASGBI (Association
of Surgeons
of Great Britain and ireland) international congress 2011, it provided an excellent opportunity for its members to meet surgeons from around the country.
Society Chair and Conference Co-director is Ms Tejal Parekh (fourth year medical student). She writes, ‘now with a membership of 1000 current students and recent graduates the Society provides a stimulating forum for aspiring surgeons. Registered with the Royal College of Surgeons of England (Charity No 212808) the Society provides a basic clinical skills course, an OSCE revision course, clinical anatomy sessions, interview and application advice and SCRUBS, a scheme to support student surgical research.
This year we organised ‘An Insight into Surgery Conference’ at St James’s attracting almost 100 student and young doctor delegates from around the region who heard high profi le speakers, Paul Renwick, Chairman of Core Surgical Training for Yorkshire and Humberside and Peter Lodge, himself an alumnus of Leeds Medical School (1983) and now Professor of Surgery at Leeds.
With the cooperation of the Transplant Surgery service at Leeds, delegates had a unique insight into this specialty.
Student Successes
Mr Raj Prasad – co-director of the Conference and Consultant Liver Transplant and Hepatobiliary Surgeon at St James’s said; ‘The Conference was a great success. I am delighted to see so many students and doctors passionate about surgery.’
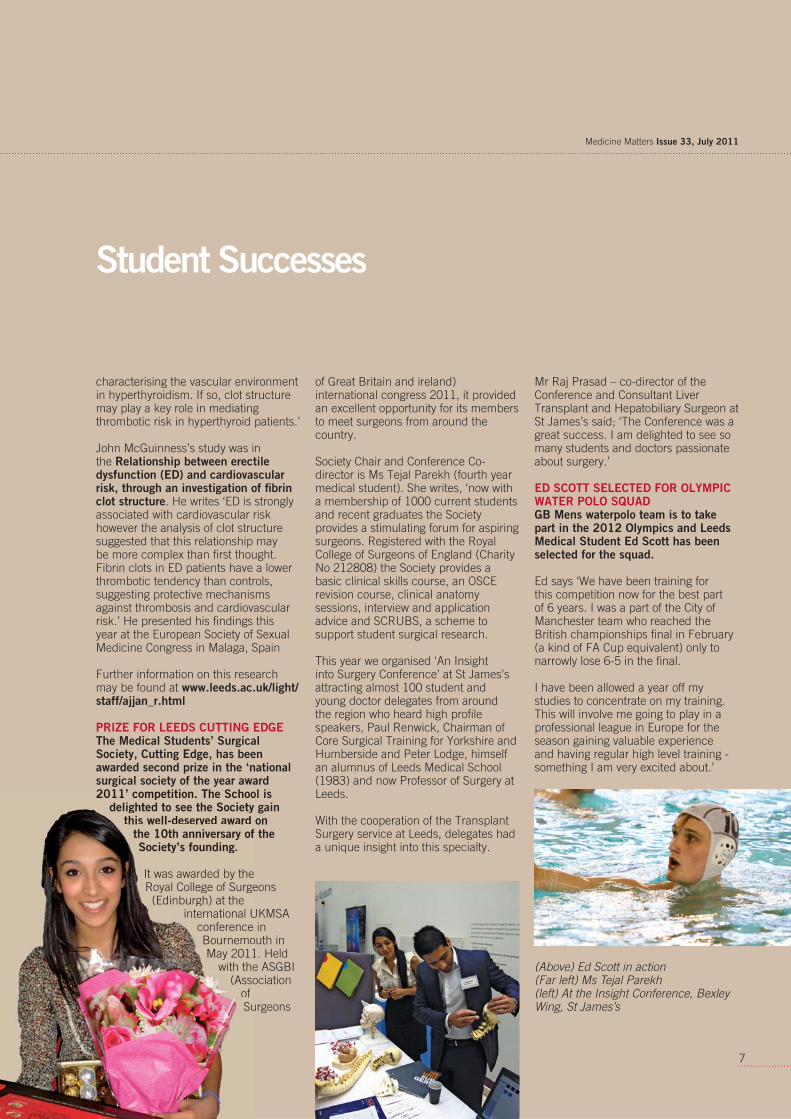
ED SCOTT SELECTED FOR OLYMPIC WATER POLO SQUADGB Mens waterpolo team is to take part in the 2012 Olympics and Leeds Medical Student Ed Scott has been selected for the squad.
Ed says ‘We have been training for this competition now for the best part of 6 years. I was a part of the City of Manchester team who reached the British championships fi nal in February (a kind of FA Cup equivalent) only to narrowly lose 6-5 in the fi nal.
I have been allowed a year off my studies to concentrate on my training. This will involve me going to play in a professional league in Europe for the season gaining valuable experience and having regular high level training - something I am very excited about.’
(Above) Ed Scott in action (Far left) Ms Tejal Parekh (left) At the Insight Conference, Bexley Wing, St James’s
2011’ competition. The Schoodelighted to see the Society
this well-deserved awardthe 10th anniversary ofSociety’s founding.
It was awarded by theRoyal College of Surge(Edinburgh) at the
international UconferenceBournemoMay 2011
with the(Asso
of Su
medicine
8
On 1 April 2011 the 1st Bn. Irish Guards returned to their depot in Windsor after completing a tour of seven months in Helmand Province, Afghanistan in support of the NATO mission there. Here Major Leon J Roberts MBE MBChB RAMC who qualifi ed from Leeds in 2000, refl ects on his career and the challenges of the role of an Army Medical Offi cer.
During the occasional lull in the pace of activity in Afghanistan I often wondered how it was that I found myself training and living
alongside the nascent Afghan National Army (ANA). Since graduating
from the Leeds School of Medicine in 2000, my post-graduate training and experiences have been a most rewarding challenge. What follows is a brief account of my life and career in the Royal Army Medical Corps (RAMC) to date, focusing on both training opportunities in military medicine and my extremely varied experiences of providing medical care to the armed forces.
Following an introductory visit to the army medical training depot mid-way through my second year of study at Leeds, I decided to apply
for a military medical cadetship. I attended formal interviews later that year and was commissioned, on probation, into the RAMC on 1 August 1997 just prior to the start of third year studies. I have never looked back for one moment and
have no regrets about this early career choice. I continued studies in Leeds until passing the 5th year fi nal MB examinations in 2000.
I undertook both pre-registration house offi cer jobs in the Yorkshire region, the second as a young army Lieutenant at The Friarage Hospital in Northallerton, which is also a Ministry of Defence hospital unit (MDHU).
Promotion to Captain was associated with starting my fi rst six-months SHO job in Emergency Medicine, requiring a move to Frimley Park Hospital in Surrey, also a MDHU. This was followed by six months of offi cer and military medical training, which included a few months at the Royal Military Academy, Sandhurst complete with passing-out parade, marching in time to a military band. The military medical training included specialist subjects such as primary health care in isolated locations, pre-hospital emergency care and advanced life support, occupational health and work-place assessments, public health medicine and management of infectious disease outbreaks, introduction to sports and exercise medicine and injury management, dispensing for doctors and a major incident medical management system (MIMMS) course.
The additional training was critical as I was pulled off the course early having received orders to deploy at short notice to Kosovo for four months in the autumn of 2002. I worked in primary health care in Pristina and then forward on the Serbian border as a junior medical offi cer with a squadron of armoured vehicles where the focus was on medical planning and incident management during regular military operations. On return to the UK I commenced GP training in Catterick in North Yorkshire and was fortunate to
From Leeds to Helmand: providing intimate medical support to deployed troops

9
Medicine Matters Issue 33, July 2011
intersperse the training with two further deployments, to Iraq in 2003 during the initial invasion and then to provide medical support to military training in Canada.
I completed a further two six-months SHO jobs in obstetrics and gynaecology and acute medicine, and then a nine-months attachment to an NHS GP trainer to complete my vocational training in November 2005. As a trained GP I have had a number of opportunities to practise military medical care in austere environments. These have included three months in Belize at the Forces jungle training school, fi ve further months in Iraq around Basra, fi ve weeks in Sierra Leone supporting military development and six weeks in Kenya, training for Afghanistan deployment. Belize was by far one of the highlights due to the diversity of the role. I provided primary care for all the instructors, families and training units, whilst also crewing an army response helicopter on 24 hours-a-day standby to fl y out to any serious UK casualties in the jungle or local civilians needing medical transport to Belize City hospital. My case-load included snake bites, severe head trauma and near-drowning victims from diving off the coast.
The Army posts its medical offi cers to Regiments on a rotational basis for tours of duty of between two and three years. I am currently the Regimental Medical Offi cer for the 1st Battalion Irish Guards, who are based in Windsor. I provide primary health care for 650 soldiers and offi cers in barracks working out of a single doctor medical centre, housed within the base. The army is able to provide medical care due to the hard work and commitment of all in the team and I am fortunate to work alongside a supportive medical sergeant and a team of 8 combat medical technicians. We are directed to provide primary care during the working day, a duty member of staff overnight and weekends, support any military training away from Windsor and take a full and active part in medical training of all troops.
It goes without saying that my practice population has very different needs to an average NHS practice list. The patients are generally young, fi t, highly motivated and generally chronic-disease free. This population has specifi c primary care needs such as sports injury medicine and sexual health services and advice. A large proportion of consultation time is weighted towards occupational health considerations and recommendations. Can a soldier with tonsillitis work indoors only and be protected from an eight mile run in the afternoon? Can someone with D and V stay in the barrack block with twelve colleagues or should they be isolated from others? Finally, the job regularly creates clinical confi dentiality issues between the sick, the medical staff and the chain of command. There can be confl icts of interests and demands for information from line managers and friends. Informed consent from patients and regular education to staff on medical confi dentiality issues is essential.
And so in mid-2010 I found myself in the strangely-named Camp Tombstone in Helmand, Afghanistan with the most fantastically varied job and responsibilities. Working in extremes of weather and terrain with a small team, housed in a Nissen hut in a small UK base adjacent to an Afghan National Army (ANA) Brigade Headquarters, we provided primary health care and also mentoring and tutoring for our Afghan medical colleagues. The team also deployed out into the battle space alongside the ANA during any planned operations in our area of responsibility. The Afghans are keen to learn by doing and are steadily taking an increased role in medical-care provision and training in the brigade. The medical, military and mentoring challenges have been fascinating and rewarding on all fronts during a long Afghan winter.
At the end of March I handed over to my successor, another army medical offi cer with another military unit, who will continue to mentor the Afghan medics and doctors for another seven months stint. I am now with my very supportive wife, children, family
and friends. After a short period of ‘normalisation’ in Windsor we received a fi ve weeks block of post-tour leave. Returning then to my medical facility in barracks, I am currently co-ordinating care for the war injured, both physically and mentally, which includes a large proportion of time for many in rehabilitation.
The army has also supported my postgraduate development. I sat the DRCOG examination in 2006 and the MRCGP at the end of my GP training. My specialist interest is in pre-hospital emergency care, and I am an active member of a local group of doctors, members of the British Association of Immediate Care Schemes (BASICS), who voluntarily respond alongside the ambulance service to medical and traumatic emergencies. It was in June last year that both my work in the army and the voluntary response work were recognised formally with the award of the MBE in the Queen’s birthday honours list. I am married to Amie, an NHS midwife, and have two children aged 4 and 2 years.
I really enjoy my job, working as a small cog in the world of the military medicine machine serving in the British Army. The work is very exciting, varied and challenging. I will retire from the army in fi ve years and begin a second career in NHS primary care. I will look back on an exhilarating time after graduation and will not have a single regret about the choice I made in the second year at Leeds University when I decided to complete the Royal Army Medical Corps application forms. I highly recommend the military medical services as a career option to all involved in the clinical care of the sick.
Further Information:www.army.mod.uk/army-medical-services/5318.aspx
Dr Leon J Roberts MBE MBChB MRCGP Dip IMC RCSEd DRCOG [email protected]
medicine
10
1
2 4
3
11
Medicine Matters Issue 33, July 2011
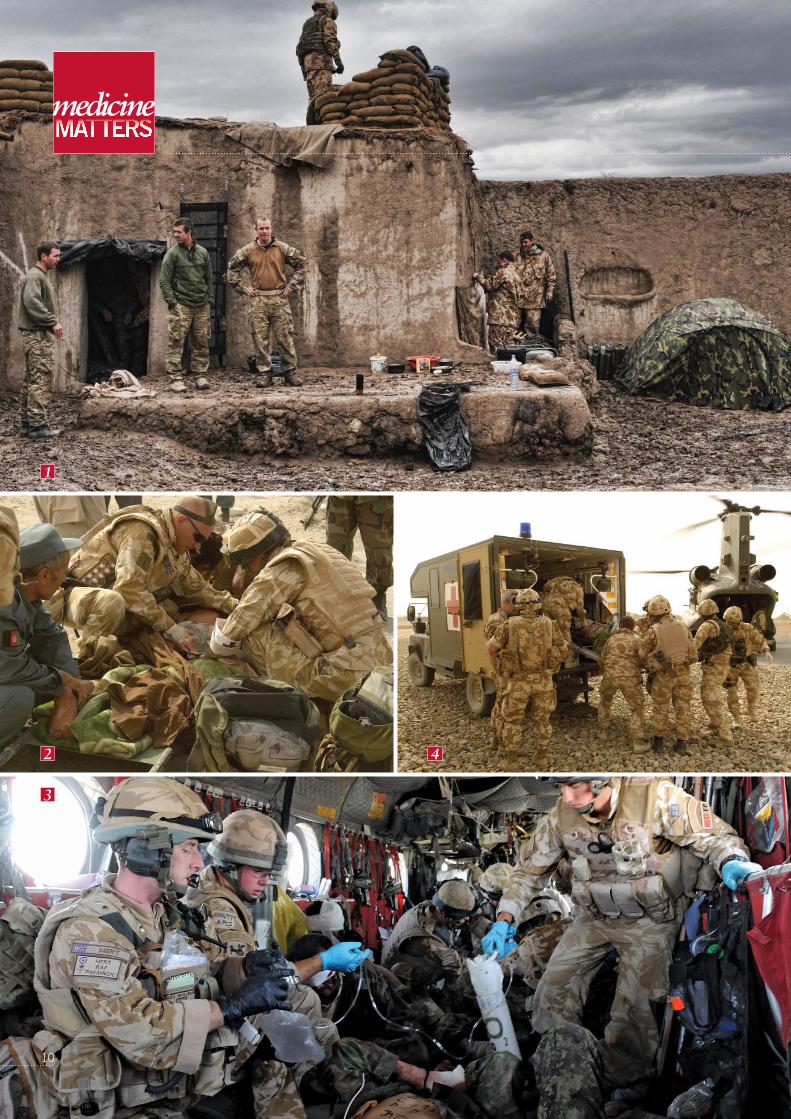
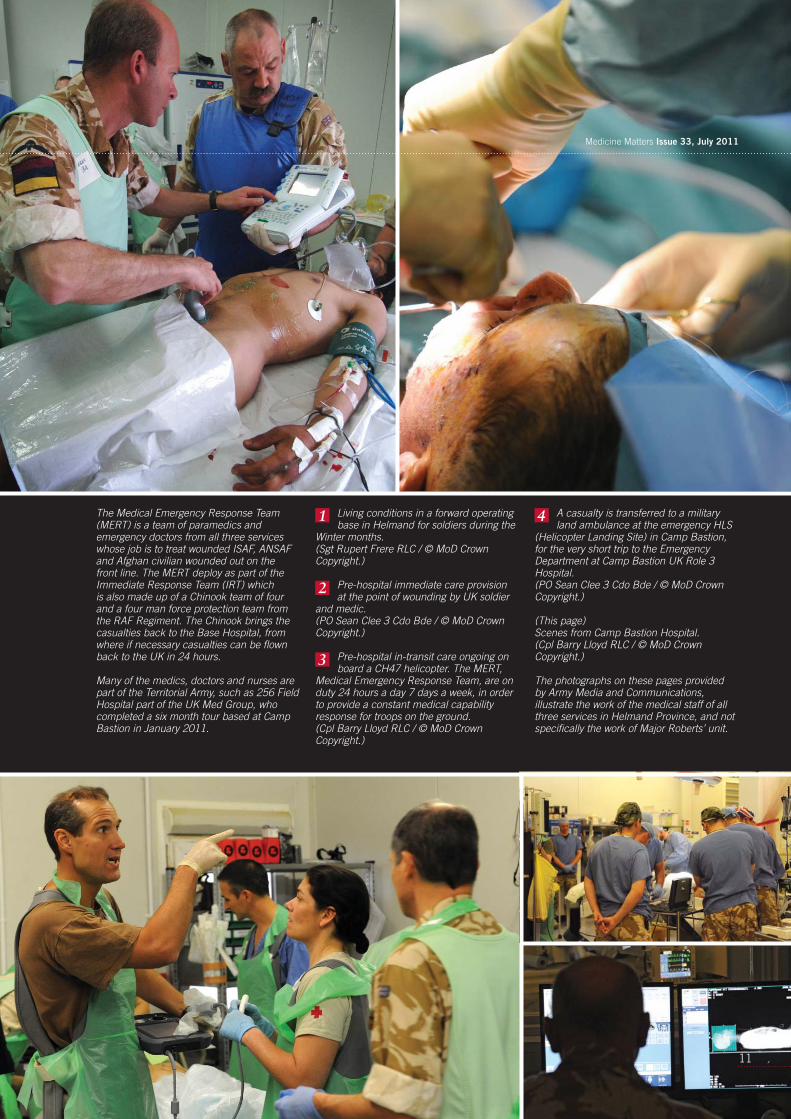
The Medical Emergency Response Team (MERT) is a team of paramedics and emergency doctors from all three services whose job is to treat wounded ISAF, ANSAF and Afghan civilian wounded out on the front line. The MERT deploy as part of the Immediate Response Team (IRT) which is also made up of a Chinook team of four and a four man force protection team from the RAF Regiment. The Chinook brings the casualties back to the Base Hospital, from where if necessary casualties can be fl own back to the UK in 24 hours.
Many of the medics, doctors and nurses are part of the Territorial Army, such as 256 Field Hospital part of the UK Med Group, who completed a six month tour based at Camp Bastion in January 2011.
Living conditions in a forward operating base in Helmand for soldiers during the
Winter months.(Sgt Rupert Frere RLC / © MoD Crown Copyright.)
Pre-hospital immediate care provision at the point of wounding by UK soldier
and medic.(PO Sean Clee 3 Cdo Bde / © MoD Crown Copyright.)
Pre-hospital in-transit care ongoing on board a CH47 helicopter. The MERT,
Medical Emergency Response Team, are on duty 24 hours a day 7 days a week, in order to provide a constant medical capability response for troops on the ground.(Cpl Barry Lloyd RLC / © MoD Crown Copyright.)
A casualty is transferred to a military land ambulance at the emergency HLS
(Helicopter Landing Site) in Camp Bastion, for the very short trip to the Emergency Department at Camp Bastion UK Role 3 Hospital.(PO Sean Clee 3 Cdo Bde / © MoD Crown Copyright.)
(This page) Scenes from Camp Bastion Hospital.(Cpl Barry Lloyd RLC / © MoD Crown Copyright.)
The photographs on these pages provided by Army Media and Communications, illustrate the work of the medical staff of all three services in Helmand Province, and not specifi cally the work of Major Roberts’ unit.
1
2
4
3
medicine
12
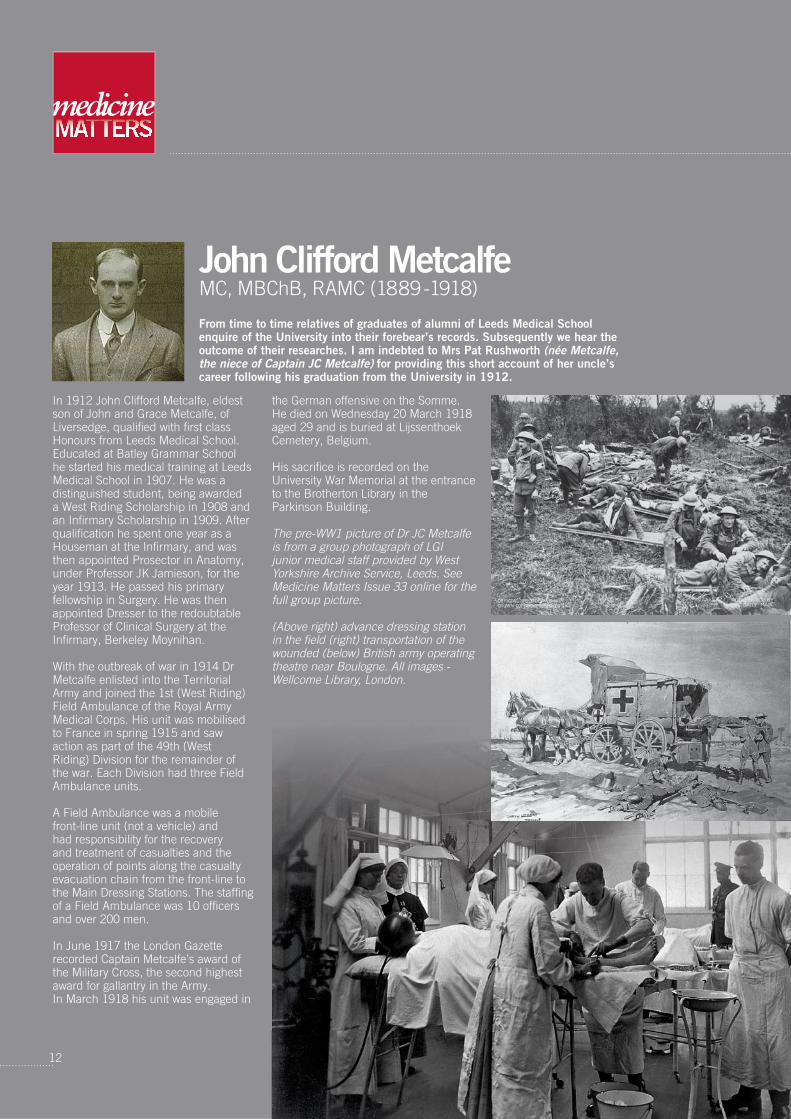
John Clifford MetcalfeMC, MBChB, RAMC (1889-1918)
In 1912 John Clifford Metcalfe, eldest son of John and Grace Metcalfe, of Liversedge, qualifi ed with fi rst class Honours from Leeds Medical School. Educated at Batley Grammar School he started his medical training at Leeds Medical School in 1907. He was a distinguished student, being awarded a West Riding Scholarship in 1908 and an Infi rmary Scholarship in 1909. After qualifi cation he spent one year as a Houseman at the Infi rmary, and was then appointed Prosector in Anatomy, under Professor JK Jamieson, for the year 1913. He passed his primary fellowship in Surgery. He was then appointed Dresser to the redoubtable Professor of Clinical Surgery at the Infi rmary, Berkeley Moynihan. With the outbreak of war in 1914 Dr Metcalfe enlisted into the Territorial Army and joined the 1st (West Riding) Field Ambulance of the Royal Army Medical Corps. His unit was mobilised to France in spring 1915 and saw action as part of the 49th (West Riding) Division for the remainder of the war. Each Division had three Field Ambulance units.
A Field Ambulance was a mobile front-line unit (not a vehicle) and had responsibility for the recovery and treatment of casualties and the operation of points along the casualty evacuation chain from the front-line to the Main Dressing Stations. The staffi ng of a Field Ambulance was 10 offi cers and over 200 men.
In June 1917 the London Gazette recorded Captain Metcalfe’s award of the Military Cross, the second highest award for gallantry in the Army. In March 1918 his unit was engaged in
the German offensive on the Somme. He died on Wednesday 20 March 1918 aged 29 and is buried at Lijssenthoek Cemetery, Belgium.
His sacrifi ce is recorded on the University War Memorial at the entrance to the Brotherton Library in the Parkinson Building.
The pre-WW1 picture of Dr JC Metcalfe is from a group photograph of LGI junior medical staff provided by West Yorkshire Archive Service, Leeds. See Medicine Matters Issue 33 online for the full group picture.
(Above right) advance dressing station in the fi eld (right) transportation of the wounded (below) British army operating theatre near Boulogne. All images - Wellcome Library, London.
From time to time relatives of graduates of alumni of Leeds Medical School enquire of the University into their forebear’s records. Subsequently we hear the outcome of their researches. I am indebted to Mrs Pat Rushworth (née Metcalfe, the niece of Captain JC Metcalfe) for providing this short account of her uncle’s career following his graduation from the University in 1912.
13
Medicine Matters Issue 33, July 2011
THE CL FUND CAMPAIGNThe campaign to mark 150 years since the opening of the School (and thus named The CL Fund Campaign) was launched at a time when Area Health Authorities were being abolished and the Conservative government presided over NHS and higher education cuts. This was the climate thirty years ago, how little has changed! Professor Wood aimed to raise money to support medical students taking an intercalated degree.
By this time there were about 4000 alumni of Leeds Medical School and the former Secretary, Mr Arthur Lockyer, who had retired just the previous year, administered the appeal. 400 generously made a donation to the CL fund which also benefi ted from the profi ts from the publication of A History of the Leeds School of Medicine 1831-1981 by Dr S T Anning and Dr W K J Walls (now out of print).
HOW IS THE CL FUND USED?The CL Fund provides an award to the most meritorious student selected to intercalate at Leeds. The bursary is currently worth approximately £7000. In the fi rst few years a selection panel was convened to listen to presentations of potential recipients. Since 1995, the School has ranked student academic performance based on scores achieved
in summative assessments. In 1996 regulations were
amended to allow for the award of one or more
additional scholarships. All recipients have
outstanding academic achievements and
use the bursary to help towards
payment of tuition, accommodation and travel fees for the additional year. Currently, tuition fees are £3375, and from 2015 intercalating medical students will face a tuition fee of £9000. Here two CL award holders speak of the opportunities that the CL Fund provides.
Karin DuckettKarin is 22 and ranked fi rst out of 247 students in the third year of the Leeds MBChB programme and in 2010/11 is following the BSc Primary Care programme organised by Dr Kristan Toft of the Academic Unit of Primary Care in Leeds Institute for Health Sciences. Karin is the sole benefi ciary of the CL Fund bursary in 2010-11.
Students undertake a longitudinal clinical placement linked to a General Practice and with sessions both in the practice and on community placements. Each student spends one day per week in clinical practice, over the academic year. The clinical experience includes time in the wider primary-care environment and includes attachments with out-of-hours providers, ambulance services, services for the socially excluded, HM prison service plus community pharmacist, optometrists, and dentists.
The aim of the clinical attachment is to help develop a good understanding of the host practice and the practice population; experience what it is like to be a member of a practice team; reinforce theoretical learning about the primary health care trust and wider primary care environment; and have a range of clinical experiences to use in the formal teaching sessions and the research project.
Karin said, “The CL fund has made a real difference to me. It meant that I could reduce my hours on my part-time job, and this allows me more time to study. I don’t have to worry about fi nding money to travel to my community placements as the bursary covers these expenses. The scholarship also funded the purchase of a new laptop.
“I grew up in Middlesbrough which like most towns has its poverty-stricken areas and I understand the impact that poverty has on a community. By devoting this year to primary care, I intend to build my skills in communication and aim to have a fulfi lling career as a general practitioner.”
Tejal ParekhNow in Year 4 of the MBChB, Tejal, known as Tej, intercalated in BSc International Health in 2009-10. She was awarded a bursary of £300 from the CL fund and this was matched by funding from other alumni sources. Tej, 23, is from Denton in Manchester and has family in Mumbai in India.
In her intercalated year, Tej conducted research in Khartoum, Sudan entitled Exploring the use and access of contraceptive methods among married Sudanese women. “My intercalated degree has enabled me to combine my interest in research and working abroad, and it developed my organisational skills. I owe this to the CL fund, and am most grateful to the generosity of alumni who contributed to it.”
Karen LeeSenior Teaching Fellow and Academic Sub-Deanwww.leeds.ac.uk/medicine/intercalated
Thirty years on: the CL FundIn 1981, the School of Medicine celebrated its 150 year anniversary and the Dean, Professor Derek R Wood, appealed to alumni of the School for funds to support a medical student in their studies. Anniversary appeals were not new. On the centenary of the School in 1931 an appeal to the 1,100 alumni of the School for £3,500 to support a scholarship of £150 was launched by the Vice-Chancellor in the fi rst edition of The Medical Society Magazine (pictured below). This scholarship is still fulfi lling that aim 80 years in the form of the Centenary (and Hardwick) Award, and is now supporting intercalated students. Dr Karen Lee describes how the CL Fund, launched in 1981, is used.
14
medicine
INTRODUCTIONThe School of Medicine’s Clinical Trial Research Unit was established in 1998. The Unit is part of the Leeds Institute of Molecular Medicine of the School and is based at Fairbairn House, formerly the home of the Nuffi eld Institute. Working in partnership with clinicians, other trialists and methodologists, over 100 members of staff provide the experience, expertise and infrastructure for the promotion and organisation of high quality, innovative, multi-centre, randomised clinical trials and research projects across NHS priority areas. The CTRU specialises in complex trials and associated methodological work (including statistical methods and patient reported outcomes) informing the academic development of this specialised fi eld of clinical research. CURRENT WORKThe range of current work is wide. It has one of the largest clinical trials portfolios in Europe with over 80 on-going trials and research studies and more than £60million in research grant funding. During 2010, over 7,000 patients worldwide were studied.The CTRU structure is based on thematic research groups which specialise in trial design and delivery within a number of NHS priority areas organised through Divisions of the CTRU as follows;
Pictured l-r Dr Helen Howard (CTRU), Professor Julia Brown, Dr Carly Rivers (CTRU), Mrs Helen Marshall (CTRU), Mr David Jayne (Department of Surgery), Professor Charles Tsang (University of Singapore)
• Cancer Division: Breast, Colorectal and Haematological portfolios
• Health Sciences Division: Mental Health, Obesity, Older People and Stroke portfolios
• Comprehensive Health Research Division: Cardiovascular, Dentistry, Musculoskeletal and Skin portfolios
• Methodology Division: Early Phase Designs, Statistical Modelling, Outcome and Measures, Safety and Harm, Therapy Effects/clustering and Complex Interventions.
Three particular trials are currently being conducted which demonstrate clearly how the Unit is putting the School of Medicine at the forefront of cancer research, world-wide. “We have an impressive track record in cancer clinical trials, and the CTRU is well-established and experienced in this area,” says Professor Brown. “To be the only one of nine clinical trials units in the UK to be accredited by the National Cancer Research Institute is important to cancer research funders. They want assurances that the projects they fund will answer the questions addressed as well as meeting stringent regulatory requirements. The CTRU has expertise in all areas of clinical research design, management, and analysis to meet these expectations.”
ROBOTIC-ASSISTED KEY-HOLE SURGERY FOR RECTAL CANCER PATIENTSThe evaluation of robotic-assisted key-hole surgery compared with conventional key-hole surgery when removing tumours from rectal cancer patients is the remit of the £1m ROLARR project, headed by David Jayne (Section of Translational Anaesthetic & Surgical Sciences). This research grant has been awarded by the Effi cacy and Mechanism Evaluation (EME) programme, which is funded by the Medical Research Council and managed by the National Institute for Health Research. The study began in January 2011 and aims to recruit 400 patients within 18 months from some 20 sites across Europe, the US and South East Asia. Initial results are expected after two years, with follow-up data available within fi ve years.
The ROLARR trial has three clinical leads. In addition to David Jayne they are; Associate Professor Charles Tsang (Co-Investigator/SE Asia Clinical Lead) Research Professor of Surgery, Division of Colorectal Surgery, University of Singapore and Professor Alessio Pigazzi (Co-Investigator/North American Clinical Lead) Assistant Clinical Professor of Surgery, City of Hope National Medical Center, California, USA
Professor Julia Brown (pictured) on the role of the Medical School’s Clinical Trials Unit, accredited by the National Cancer Research Institute and registered by the UK Clinical Research Collaboration.
Focus on the Clinical Trials Research Unit

Low testosterone levels can cause problems such as fatigue, weight gain and reduced sex drive. For six months, half of the trial participants will use a testosterone gel and the other half a placebo gel. During regular clinic visits participants will have their testosterone levels recorded and will answer a range of questions about their physical well-being and quality of life. This is a double blind trial and will take three years to recruit 268 patients, across 10 centres in the UK. It is due to start in July 2011 and will fi nish in 2015.
For more information see our Website at http://ctru.leeds.ac.ukOr write to CTRU, University of Leeds, 71-75 Clarendon Road, LS2 9JT
15
Medicine Matters Issue 33, July 2011
In order to have effective international trial management, ROLARR is operating on a ‘hub-and-spoke’ model, with the CTRU in Leeds acting as the hub for the trial taking on the pan-world collaboration and central data and grant management, as well as being the coordinating trials unit for European sites. We will have two spoke units assisting us with site set-up and site management in Singapore (for SE Asia), and in California (for the USA and possibly Brazil), to tie in with the institutions of the two above-mentioned co-investigators. The countries in which we have sites being set up are as follows:
• UK - Italy (3+ sites), Spain (2+ sites), France, Germany
• USA (approximately 6 sites)• Singapore• South Korea
ADVANCED BREAST CANCERThe LANTERN project focuses on patients with advanced breast cancer which has spread to the brain, who are being treated with the drug Herceptin®. Herceptin® is proven to control cancer in the body but not in the brain, which may be due to its large molecules which cannot pass the blood/brain barrier. The trial will monitor two groups of patients taking drugs over a six-month period, one group will continue with Herceptin® and the other will use a chemotherapy agent lapatinib. Lapatinib has smaller molecules than Herceptin® but targets the same cancers.
The £1m study, which is being led by Professor David Dodwell, is a collaboration between Leeds Teaching Hospitals NHS Trust and GlaxoSmithKline. It will take two years to recruit 130 patients and be coordinated across 12 UK hospitals. There are two sub-studies within LANTERN – one being run by Professor David Buckley which is using MRI scan to analyse permeability of the blood/brain barrier, and another in which Professor Galina Velikova is asking patients, who are receiving treatment, about their quality of life.
CANCER IN YOUNG MALESThe third study – TRYMS – is funded (£0.5m) by Cancer Research UK, and led by Professor Richard Ross and Dr Jennifer Walsh at the University of Sheffi eld with statistical design and trial management conducted by Leeds CTRU. This study will investigate the effects of testosterone treatment on young male cancer survivors who have had testicular cancer, leukaemia or lymphoma, and who have low testosterone levels.
medicine
16
COMDIS, a communicable diseases research consortium, has received a new award of £7.5m from the UK’s Department for International Development (DFID) for six years, to support the drive to eradicate world poverty and help maintain progress towards the Millennium Development Goals. The award to COMDIS- HSD (Health Services Delivery) is to be led by the Nuffi eld Centre for International Health and Development at Leeds Institute of Health Sciences. As James Newell (Co-Director of COMDIS-HSD) explains, ‘it is built on a successful record of research in the last fi ve years. This addressed the treatment of communicable diseases such as HIV/AIDS, malaria and tuberculosis.’ (as previously reported in Medicine Matters Issue 25).
The new research focuses specifi cally on improving the delivery of basic health services, for communicable diseases including tuberculosis, malaria, some tropical diseases, HIV/AIDS and reproductive tract infections, for non-communicable diseases such as diabetes and coronary vascular disease (CVD), and for improving health policy and practice. It is particularly directed towards the common diseases in slums and marginal rural areas, to help ensure that aid is not wasted
and to contribute towards long-term economic development and greater self-reliance in the countries where the programme operates. The programme works in collaboration with national health services and research partners (Universities and NGOs such as the Malaria Consortium) in Bangladesh, China, Nepal, Pakistan, Tanzania, Ghana, Uganda, Southern Sudan and Nigeria.
Professor John Walley, Co-Director of COMDIS-HSD, expands, “Using our partners’ extensive networks, we understand the developmental aims of health ministries in the partner countries. We can work right from the start of the project with them and the NGOs. They already have the resources for drugs and trials, staff and facilities. Our expertise lies in helping them to develop the technical details, guidelines and materials required to deliver care in the best and most effective way. Then we trial and study the effectiveness within the ministry of health pilot sites, prior to national scale-up.
We are particularly interested in providing improved health care in urban areas where population growth has been so great and rapid that government health services have
not been able to keep pace. We will develop and test models of treatment and prevention for health centres that are sustainable, cheap, feasible and replicable across different countries. We will research and develop continuing care for non-communicable diseases including how to maintain adherence to treatment.”
“We estimate that millions have already benefi ted from our research and at the end of this project, COMDIS-HSD will have improved health service provision for millions more.”
www.comdis.org
Research NewsNew funding for COMDIS

YOUNG INVESTIGATOR AWARD
Dr Nick West, Academic Clinical Fellow at the Leeds Institute of Molecular Medicine has been awarded the British Oncological Associations Young Investigator Award.
His research confi rms that carefully removing a specifi c part of the diseased colon (tissue, blood vessels and lymph nodes) from the bowel of colon cancer patients, results in a 15% greater overall survival at fi ve years compared to using current standard surgical techniques. Judges at the 2010 Excellence in Oncology Awards in Liverpool in November 2010, praised the work and said it was an example of a surgical education programme at its best.
17
NEW FUNDING FOR GENETIC RESEARCH
A Leeds Institute for Molecular Medicine (LIMM) research team, led by Professor Colin Johnson, has been awarded £1.2m from the Sir Jules Thorn Charitable Trust. The fi ve year research project aims to identify genes that cause certain types of severe genetic diseases.
These diseases are those linked to genetic conditions with recessive inheritance, such as cystic fi brosis and some types of childhood blindness and are a major cause of infant death and childhood disability in some local communities. In the UK annually an estimated 2,300 children are born with a severe recessive condition. It is more likely where consanguinity or marriage between blood relatives occurs. In these circumstances the risk of a child inheriting two copies of a disease- causing gene – one from each parent – is increased.
The research will be using a ‘next generation’ genetic sequencer available through the Leeds Teaching Hospitals NHS Trust and the Yorkshire Regional Genetic Service.
Professor Johnson says: “Once we have identifi ed the disease-causing gene and worked up the clinical features of the condition, we can offer improved diagnosis for patients and counselling for families. Our genetic counsellors are very important to the process, acting as key intermediaries. If families decide to have testing we can work out who carries specifi c genes and give families a defi nitive risk assessment which allows them to make informed decisions about future marriages and family planning.”
l-r: Professor Peter Selby (University of Leeds), Professor Tim Bishop (University of Leeds/Chair of the Leeds Cancer Research UK Centre), Teri Wadsworth (patient), Peter Sneddon (Cancer Research UK), Dr Geoff Hall (Leeds teaching Hospitals NHS Trust). Photo: Yorkshire Post Newspapers
Medicine Matters Issue 33, July 2011
Leeds Cancer Research UK Centre celebrates fi rst anniversary
ELIPSE – A KNOWLEDGE TRANSFER SUCCESS
Elipse is a prenatal screening software to identify pregnancies in which the risk of fetal anomaly is high enough to warrant an invasive diagnostic test. It has been in development for over 20 years by the School of Medicine, in collaboration with the Leeds Teaching Hospitals NHS Trust and US multi-national, Perkin-Elmer. With the combination of Elipse and LifeCycle™ this screening software is now in operation in over 30 countries world-wide. For more information about this success read the full story on the Medicine Matters Issue 33 web edition at www.leeds.ac.uk/medicine/matters
18
medicine
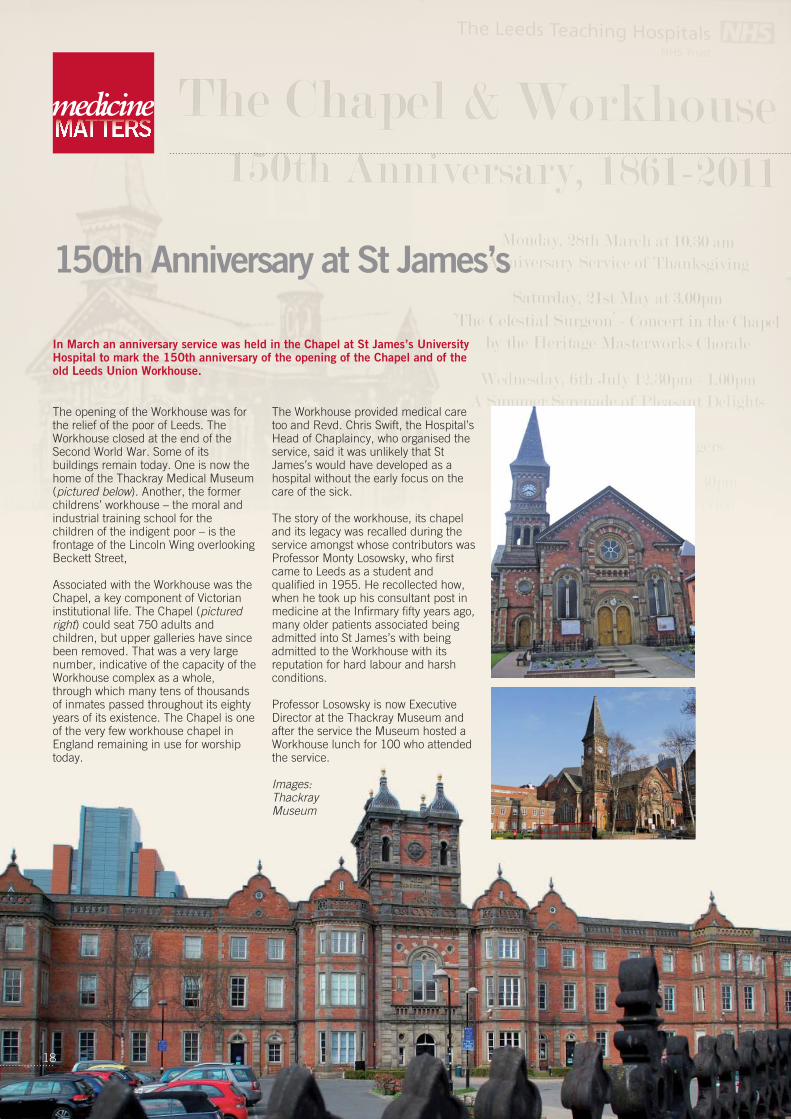
The opening of the Workhouse was for the relief of the poor of Leeds. The Workhouse closed at the end of the Second World War. Some of its buildings remain today. One is now the home of the Thackray Medical Museum (pictured below). Another, the former childrens’ workhouse – the moral and industrial training school for the children of the indigent poor – is the frontage of the Lincoln Wing overlooking Beckett Street,
Associated with the Workhouse was the Chapel, a key component of Victorian institutional life. The Chapel (pictured right) could seat 750 adults and children, but upper galleries have since been removed. That was a very large number, indicative of the capacity of the Workhouse complex as a whole, through which many tens of thousands of inmates passed throughout its eighty years of its existence. The Chapel is one of the very few workhouse chapel in England remaining in use for worship today.
The Workhouse provided medical care too and Revd. Chris Swift, the Hospital’s Head of Chaplaincy, who organised the service, said it was unlikely that St James’s would have developed as a hospital without the early focus on the care of the sick.
The story of the workhouse, its chapel and its legacy was recalled during the service amongst whose contributors was Professor Monty Losowsky, who fi rst came to Leeds as a student and qualifi ed in 1955. He recollected how, when he took up his consultant post in medicine at the Infi rmary fi fty years ago, many older patients associated being admitted into St James’s with being admitted to the Workhouse with its reputation for hard labour and harsh conditions.
Professor Losowsky is now Executive Director at the Thackray Museum and after the service the Museum hosted a Workhouse lunch for 100 who attended the service.
Images: Thackray Museum
150th Anniversary at St James’s
In March an anniversary service was held in the Chapel at St James’s University Hospital to mark the 150th anniversary of the opening of the Chapel and of the old Leeds Union Workhouse.
In a wide and rapid sweep of economic policy and the consequences of recessions on the health of populations, Professor McKee, who has produced over 500 papers and 38 books, gave an incisive analysis of the issues as identifi ed by research into periods of decline of economic activity since the Great Crash of 1929. The wealth of data that he provided from each of the economic downturns since then and from elsewhere was impressive. The comparison of the consequences in different countries of government policy (or lack of it) on health was at the heart of the lecture drawing on examples from the USA, post-communist Soviet Union, East Asia in the 1990s, Europe and Iceland. Evidence showed that strong welfare systems in, for example, Sweden, Austria and Iceland mitigated the consequences of economic downturn. The analysis thus offered some opportunity to anticipate the consequences of current economic policy on health in the UK.
His conclusions;
• Economic Turmoil is just one of a the many infl uences on health
• We are pushing epidemiology to its limits and can only hope to detect the short-term effects of economic policy
• Major economic shocks can kill, especially from suicide, homicide and alcohol abuse
• Support networks have been shown to mitigate the effects on individuals. The decline of voluntary associations and of membership of trades unions, social clubs and religious bodies is thus of concern.
• Government is part of the solution, not part of the problem and when the private sector is disinvesting in employment the public sector must step in.
• The private sector needs the public sector as a provider of the necessary infrastructure
For more on Professor McKee and his work visit www.lshtm.ac.uk/people/mckee.martin
Martin McKee’s views on contemporary health issues can be found on Twitter @martinmckee
Medicine Matters Issue 33, July 2011
sweep of economic equences of ealth of populations, ho has producedd 38 books, gave an he issues as h into periods of activity since the . The wealth of data m each of the s since then and impressive. The onsequences in f government policy lth was at the heart
ng on examples from munist Soviet Union, 0s, Europe and howed that strong for example, d Iceland mitigated f economic ysis thus offered anticipate the rrent economic he UK.
p pprivate sector is disinvesting in employment the public sector must step in.
• The private sector needs the public sector as a provider of the necessary infrastructure
For more on Professor McKee and his work visit www.lshtm.ac.uk/people/mckee.martin
Martin McKee’s views on contemporary health issues can be found on Twitter @martinmckee
19
2011 Thackrah Lecture
Martin McKee CBE, Professor of European Health at the European Centre on Health of Societies in Transition at the London School of Hygiene and Tropical Medicine, delivered the 2011 Thackrah Lecture, Health in an age of economic turmoil: what have we learned? on 20 May 2011.
The lecture was organised by the Leeds Institute of Health Sciences.
The Thackrah Lecture is named after Charles Turner Thackrah (1795 -1833), one of the founders of the Leeds Medical School, a social campaigner for the health of employees in ‘arts, trades and professions’ and considered to be the father of occupational medicine through the publication of his seminal work in 1832.
www.leeds.ac.uk/medicine/history/thackrah

NEW SKILLS CENTRE OPENSA £2.85m Centre funded by the Yorkshire and Humber SHA opened in June at St James’s providing the most up-to-date clinical skills training facilities for medical students and other trainee and qualifi ed NHS staff.
medicine
Alumni Reunions News
20
DIAMOND ANNIVERSARY REUNION – MEDICINE CLASS OF 1951 The 1951 graduates held a 60th anniversary reunion at the Parkway Hotel, Leeds on Saturday 26 March. Ten graduates and seven family members met for coffee and nine graduates and four family members sat down for a long chatty lunch.
In accordance with tradition established at reunions every fi ve years since 1976 we observed the Loyal toast and toasts to “Medicine” proposed by Janet Waddelow (nee Shaw) and to “Absent Friends” by John Metcalfe who included messages from ten colleagues unable to attend.
The occasion, happy if more subdued than some of its predecessors, featured the same warm friendships and camaraderie which has characterised all our reunions.
FORTHCOMING MEDICS ALUMNI REUNIONS11 – 13 Sept 2011: 1961 30 Sept – 2 Oct 2011: 1957 30 Sept – 2 October 2011: Medics started 1961 1 October 2011: 1986 15 October 2011: 1976 15 October 2011: 1981
For more information on these reunions or advice on organising your own reunion, go to https://alumni.leeds.ac.uk/ Or write to Alumni & Development Team, EC Stoner Building, University of Leeds, Leeds, LS2 9JTEmail: [email protected] Tel: 0113 343 7520Fax: 0113 343 4029
Join Leeds alumni online at www.alumni.leeds.ac.uk
UNIVERSITY AWARDS FOR TWO MEDICAL STUDENTSTwo School of Medicine undergraduates were honoured at this year’s Access Programme and Adult Learner Awards. Aishah Beaumont (middle) - ‘Special Commendation’ in the Access Programme Award Collette Isabel Stadler (right) - winner of the Adult Learner Award
The winners received their awards from Professor Viv Jones at a lunchtime ceremony in University House on 11 May.
More student successes
Medicine Matters Issue 33, July 2011
Barry Ewart has been Community Education Development Offi cer at the Medical School since February 2000 and here refl ects on over 10 years’ of community engagement in the medical students’ curriculum.
The initiative for my post, established in 1998, came from the GMC report ‘Tomorrow’s Doctors’ (1993) which encouraged Medical Schools to enable students to learn in the community, to learn from patients, carers, service users and voluntary and community groups.
In Year 1 all students (in pairs) visit volunteer patients (usually in the patient’s own home) to develop their communication skills. They have also visited GP Practices, nursing homes and community organisations to learn about different peoples’ experiences of healthcare.
As part of Year 2 students have heard speakers from among 80 groups on the theme of Engaging with People (People
and Power) and took part in seminars on issues like Poverty, Domestic Violence and Deaf Awareness.
Over the last 9 years we have also brought in 30 or so community organisations or individuals to run 200 interactive workshops in Year 2 as part of the Valuing Diversity Programme and issues covered (several suggested by the students themselves) include Mental Health and Discrimination, Sexuality, Race, Social Class, and Bereavement.
Over 500 second and third year students have spent time over two weeks in December with voluntary and statutory sector organisations as part of the Student Selected Component (SSC) part of the curriculum. Primary schools have provided opportunities for many years for second and third year students to teach and learn, and all within the national curriculum framework.
A Community Newsletter shares our work with all our community contacts and includes reports by students on their community placements. It contributes to the demystifi cation of medical education and provides a space for news and views, and for voluntary and community groups to promote themselves. 35 issues have appeared since it was fi rst published in late 2000 and it was highly praised by a GMC visit to the School several years ago.
Medical education will always face new challenges brought about by societal change such as the potential obesity crisis and the longer-term consequences of increases in alcohol intake. Increased migration leads to a more diverse patient group
and part of our task is I believe is to make students aware of these new challenges. We have a new curriculum but our commitment to community engagement is fi rmly established.
Did you take part in the Community Engagement programme? How has it helped in professional practice? I’d like to hear from you with ideas and refl ections. Thank you. Barry [email protected]: 0113 343 4358www.leeds.ac.uk/medicine/
Community EngagementFocus on …

Printed on recycled paper
In its dramatic interior the Leeds Institute of Health Sciences exhibited in February the work of Richard Bailey, showing his series Sarah after Vermeer. This exhibition marked the 40th anniversary of the Down’s Syndrome Association and was mounted in collaboration between the Association and GlaxoSmithKline. GSK has renewed support of Shifting Perspectives until 2013 and the exhibition is travelling nationwide during the current year.
This was the second time Shifting Perspectives has exhibited at the Institute. Director Allan House says of the Exhibition; “Our research explores the different ways that people think about and respond to health, illness and disability – an important way of planning what sort of health service we need. Collaboration with art projects like Shifting Perspectives is a great way of stimulating us to think about new approaches to research, to teaching and to communicating to others. It reminds us that difference is not the same as disability.”
Images from Sarah after Vermeer by Richard Bailey – reproduced with permission
www.richardbaileyphotography.co.ukwww.shiftingperspectives.orgwww.downs-syndrome.org.uk
When you have fi nished reading this magazine, if you are tempted to bin it for recycling why not instead send to a friend, doctors’ or dentists’ surgery or elsewhere for others to read.
Shifting Perspectives40th Anniversary Exhibition of the Down’s Syndrome Association