medication safety and admissions avoidance: a perspective steve williams consultant pharmacist in...
TRANSCRIPT

Medication Safety and admissions avoidance: A
perspective
Steve Williams Consultant Pharmacist in
Medicine & Medication Safety
Honorary Clinical Lecturer, Manchester Pharmacy School
June 2015

Outline for Session
– How big is the issue?– Is the situation getting better or worse?– Does the NHS take Medication Review
seriously enough?– What should we all be doing about it ?
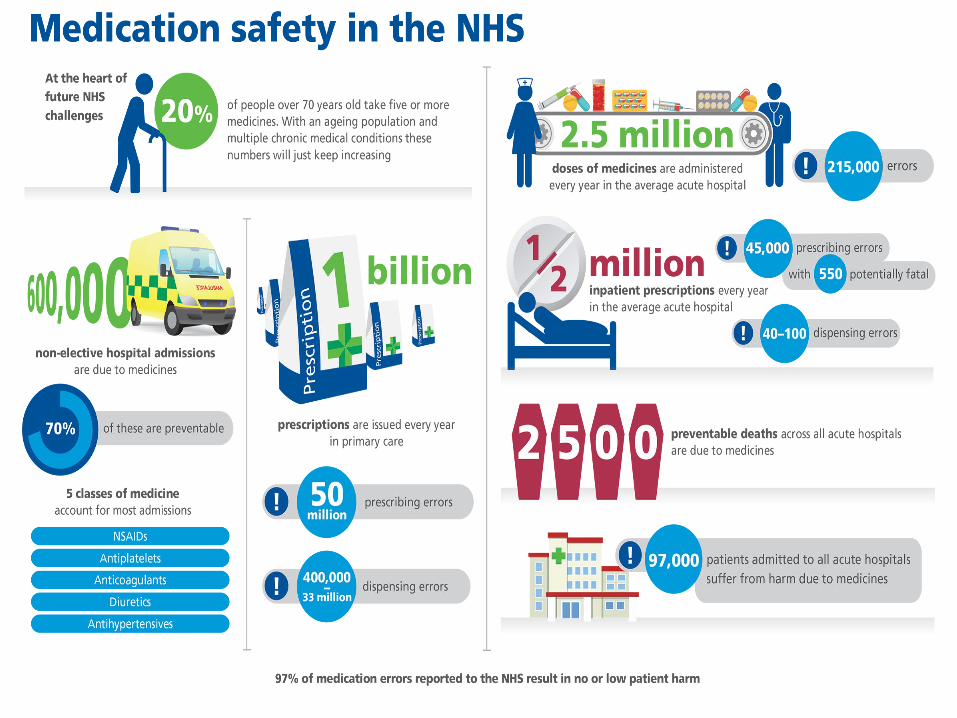
How many non elective admissions to English hospitals every year are due to medicines?
– Think of a number…..

Important academic references
– 11.2% patients had adverse drug events (ADEs) causing hospital admission (47.6% preventable)
– Patient age , time since starting new medicine and total number of medicines independently predictors of admission
– Antiplatelets, anticoagulants , diuretics, ACE inhibitors and anti – epileptics major culprits
Kongkaew, C., Hann, M., Mandal, J., Williams, SD, Metcalfe, D., Noyce, P. & Ashcroft, D. Risk Factors for
Hospital Admissions Associated with Adverse Drug Events. Pharmacotherapy 2013; 33: 827-837

Important academic references
– 6.5% UK hospital patients admitted due to Adverse Drug Reactions (ADRs)
(72% preventable) Pirmohamed et al BMJ 2004;329:15-19
– Preventable drug related problems accounted for 3.7% of hospital admissions. Antiplatelets, Diuretics, NSAID’s accounted for 50% of all admissions
Howard et al BJCP 2007;63:136-4
– 20.8% patients readmitted to hospital due to ADR within 1 year of first admission.
Diuretics & Antiplatelets most frequent culprits Davies EC et al BJCP 2010;70:749-55

BUT under recognised because under reported ?
– International Classification of Disease (ICD) coding from hospital databases are not reliable for identifying ADRs Hohl CM,Karpov A, Reddekopp Let al. ICD-10 codes used to identify
adverse drug events in administrative data: a systematic review J Am Med Inform Assoc 2014;21:547–557
– Only 9% of adult patients admitted to a UK hospital with a confirmed medication related harm (ADRs , medication errors, non-adherence) had a related ICD code documented. Reynolds M et al. A
descriptive exploratory study of how admissions caused by medication-related harm are documented within inpatients’ medical records. BMC Health Service Research 2014; 14: 257
– Hohl CM,Karpov A, Reddekopp Let al. ICD-10 codes used to identify adverse drug events in administrative data: a
systematic review J Am Med Inform Assoc 2014;21:547–557

BUT under recognised because under reported ? (2)
– 31.5% of children admitted to a UK hospital with a confirmed ADR had a related ICD code documented Bellis et al. BMC Pharmacology and Toxicology 2014, 15:72.
Clinical coding of prospectively identified paediatric adverse drug reactions – a retrospective review of patient records

And the situation is only getting (and will get even) worse


Polypharmacy meets Multi-morbidity

Does the NHS take Medication Review seriously enough?

We have some evidence

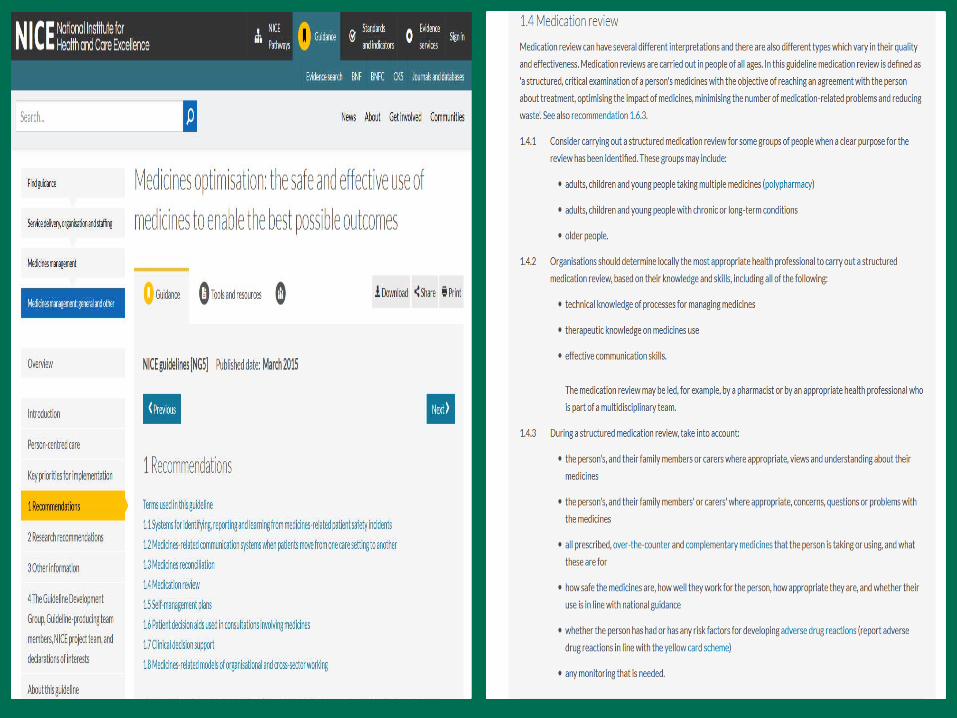
And there are plenty of tools to help
– NICE Medicines Optimisation guidance – Kings Fund , Scottish and Welsh
Polypharmacy documents (CPPE focus too 2016)
– Seven steps to managing polypharmacy: Specialist pharmacy Services document
– Reducing Inappropriate Polypharmacy: The Process of Deprescribing Scott IA et al JAMA Intern Med 2015.
doi:10.1001/jamainternmed.2015.0324
– STOPP START Gallagher P et al Int J Clin Pharmacol Thera 2008;46:72-83
– No Tears Using the NO TEARS tool for medication review. T Lewis. BMJ 2004;329:434

Does the NHS take Medication Review seriously enough?
Can we compare it with a routine Total Knee Replacement (TKR) ?

Total Knee Replacement
– Preoperatively (50 mins)
– Preop assessment clinic (30 minutes Nurse + 20 minutes Doctor)
– Tests: ECG, bloods, and MRSA swabs
– Consent form
– Day of Surgery (150mins)– Anaesthetic pre-op
assessment (10 min) – Anaesthesia-spinal or GA
(20 min) Anaesthetist plus ODP or nurse
– Surgery (90mins) 2 scrub nurses, 2 surgeons,1 anaesthetist, 1 runner

Total Knee Replacement (2)
– Post operatively– Recovery (60 mins)
1 Anaesthetic nurse– 3-4 days on ward,
OT and PT twice a day
– Post discharge – Continue physiotherapy for
several weeks individually in a group depending on the patients needs
– Follow up clinic appt with doctor

A typical Medication Review?
– Play video

A typical Medication Review?
– 1 GP (10 mins)

Does the NHS take Medication Review seriously enough?
– Fail to plan , plan to fail!

So what could the NHS be doing about it ?

Thomas J. A multidisciplinary approach to reducing avoidable medication-related harm/hospital admissions. Clinical Leadership Conference 2013. www.learningwales.tv/group_items/view/1354


2020: NHSE Medicines Optimisation Dashboard to include Medication related admissions per CCG ?

2020: NHSE Medicines Optimisation Dashboard to include Medication related admissions per CCG ?
– But it is going to need some levers




But finally what could YOU be doing about it ?

Is balancing the Prescription Equation your key to medication related admissions avoidance?
“If we just keep adding, and not subtracting, we just multiply the medication problems”
Thanks for listening
– Any questions?