medication decisions and clinical outcomes in the canadian national outcomes measurement study in...
TRANSCRIPT

Medication decisions and clinical outcomesin the Canadian National OutcomesMeasurement Study in Schizophrenia
Introduction
Individuals with schizophrenia and related psychi-atric disorders often experience repeated periods ofhospitalization, impaired social functioning, cog-nitive impairments and a reduced level of quality oflife (1, 2). The most powerful predictors of goodoutcome are early interventions with both phar-macological and psychosocial interventions. Anumber of clinical trials have demonstrated thesuperiority of atypical (second generation) anti-psychotics over typical (first generation), anti-psychotics in terms of symptomatic improvement(especially negative symptoms), cognitive improve-ment, reduced rates of rehospitalization andimproved social functioning (3–5). Psychosocialtreatments such as stress reduction programmes (6)and education for families (7) have contributed toimproved patient outcomes, but these treatmentshave not been specifically evaluated in this pros-
pective, population-based study from centresacross Canada where stable out-patients weretreated with antipsychotic medications under con-ditions of routine clinical care.A number of epidemiological studies have estab-
lished a relationship between length of duration ofuntreated psychosis (DUP) and clinical outcome(8). In this regard increasing DUP is associatedwith both longer time to recovery from psychosisand a decrease in the percentage of patientsrecovering. Hollis (9) and Lay (10) have independ-ently demonstrated that an earlier age of onset ofpsychotic symptoms correlates with poorer func-tional outcome.Gender differences have been noted in respect to
age of onset of psychosis (males approximately5 years before females) (11); and female patientshave consistently shown a better response totreatment with lower rates of hospitalization andshorter in-patient stays than males (12). Seeman
Williams R, Kopala L, Malla A, Smith G, Love L, Balshaw R.Medication decisions and clinical outcomes in the Canadian NationalOutcomes Measurement Study in Schizophrenia.Acta Psychiatr Scand 2006: 113 (Suppl. 430): 12–21. ª 2006 BlackwellMunksgaard.
Objective: To evaluate over a 2-year period, patients from academic/non-academic centres, from each region of Canada, to determinewhether location or other variables such as medication type, gender orincome was associated with outcome as defined by non-hospitalizationand persistence on original treatment.Method: A total of 448 patients were recruited from academic andnon-academic centres across all provinces of Canada and followed upfor 2 years.Results: Patients from British Columbia had significantly lower ratesof hospitalization than patients from other provinces. Male patientsshowed greater symptomatic improvement at 2 years from initialassessment compared to females. Patients on clozapine, risperidoneand olanzapine were least likely to be hospitalized.Conclusion: There were some regional differences noted in bothutilization of types of antipsychotic medications and hospitalizationrates. In this sample of stable out-patients over 70% who started onmonotherapy with clozapine, risperidone, olanzapine and quetiapineremained on the same medication over the 2-year study period.
R. Williams1, L. Kopala1, A. Malla2,G. Smith1, L. Love3, R. Balshaw3
1Department of Psychiatry, University of BritishColumbia, Vancouver, BC, 2Department of Psychiatry,McGill University, Montreal, QC and 3SyreonCorporation, Vancouver, BC, Canada
Key words: schizophrenia; Canada; outcomeassessment; hospitalization
Richard Williams, Director Schizophrenia Service, EricMartin Pavilion, 2334 Trent Street, Victoria, BC, CanadaV8R 4Z3.E-mail: [email protected]
Acta Psychiatr Scand 2006: 113 (Suppl. 430): 12–21All rights reserved
Copyright ª Blackwell Munksgaard 2006
ACTA PSYCHIATRICASCANDINAVICA
12

(11, 13) and Harding (14) have also noted thatfemale patients have less residual negative symp-toms and a higher level of social functioning.Low socioeconomic status has been found by
Samele (15) and Brown (16) to be associated withboth lengthier and more frequent periods ofhospitalization in the patient population understudy. Similarly Drake (17) and Solakangas (18)demonstrated that good social supports resulted inthese patients having lower rehospitalization ratesand higher social functioning.Robinson (19) in a study of recovery from a first
episode of schizophrenia noted that better cogni-tive functioning prior to treatment predicted suc-cessful symptom remission. In this naturalisticstudy we have no data on cognitive measures.
Aims of the study
The aim of this study is to look at what happenedto 448 stable out-patients over a 2-year period,looking for possible differences between academicand community centres; between regions andbetween medication groups in terms of rehospital-ization rates and symptom change.
Material and methods
The Canadian National Outcomes MeasurementStudy in Schizophrenia (CNOMSS) involved 32community and academic sites across Canadaenrolling 448 patients diagnosed with schizophre-nia and other psychotic disorders to evaluatechanges over time. These patients were stableout-patients voluntarily enrolled into a prospectivestudy to assess clinical outcomes over a broadrange of measures, described in the introductorypaper in this supplement (20).A general linear model was used to examine
change in Brief Psychiatric Rating Scale (BPRS)scores after adjusting for variability in demographicand clinical variables observed at the initial visit.This allowed for comparisons between groupsapproximately as though the groups were identicalwith respect to the distribution of the initial cova-riates. In a similar way, a logistic regression modelwas used to examine the probability of hospitaliza-tion. Persistence on atypical monotherapies used atthe initial visit were analysed using a proportionalhazards regression model with a similar set ofcovariates. These models are used consistentlyacross studies (2–4) looking at patient outcomesover a 2-year period. In general,P-values below 0.05have been considered statistically significant, with-out adjusting for multiple inferences; however, allP-values should be considered as exploratory given
the observational nature of this study. Analyseswere conducted using SAS version 9.1.At entry, data were collected on 448 patients; at
the end of year 1 data were collected from 423patients, and from 347 at the end of year 2. Overthe 2 years from initial assessments 25 patientswithdrew their consent to continue in the study,and 36 were lost to follow-up including 15 patientsfrom one site which closed when the investigatormoved (see Table 1). The patients who failed tocomplete assessments at the end of years 1 and 2were a representative sample from those includedat the initial assessment (see Table 2) (20). Twopatients died during the course of the study.
Results
Pharmacological therapies
Of the 448 patients diagnosed with schizophreniaand related psychotic disorders entering the study,all but seven were on antipsychotic medications atbaseline. Patients in the study could be switchedmedication at any time at the discretion of theinvestigator and without having to meet anycriteria for symptom change or side effects (routineclinical care). At initial assessment 62% of patientswere on monotherapy atypical agent; 5% were onsingle oral typical; 5% on combined oral typicaland atypical; 6% were on single typical depotmedications and 10% were in randomized clinicaltrials (see Table 2). The dropout rate from eachgroup (on an intent-to-treat basis) is similar at year1 and year 2. There were no statistically significantdifferences in use of medications by age, gender,household income, ethnicity or academic vs. com-munity treatment location.Table 2 shows a breakdown of medication usage
at initial assessment. In particular, clozapine wasused by 61 of 448 patients (13.6%). Regionalvariation is shown in Table 3. There were notableand statistically significant regional differences atinitial assessment (clozapine vs. non-clozapinetreatment group compared by chi-squared test,P ¼ 0.023) with low usage in Saskatchewan/Mani-
Table 1. Number of declared dropouts by year in study and reasons for dropout
Reason
Last year in study, n (%)
Year 1 Year 2
Death 1 (4.0) 1 (1.3)Withdrew consent 7 (28.0) 18 (24.0)Lost to follow up 2 (8.0) 19 (25.3)PI withdrew 2 (8.0) 13 (17.3)Other 13 (52.0) 24 (31.9)Total 25 (100.0) 75 (100.0)
Canadian measurement study in schizophrenia
13

toba (five of 76, 7%), moderate usage in Ontario(10 of 97, 10%) and Quebec (four of 49, 8%) andhigh usage in British Columbia (BC) (11 of 64,17%) and Alberta (17 of 70, 24%) (see Table 3).Interestingly in this study sample, olanzapine
usage was highest in BC (19 of 64, 30%) eventhough its cost is not covered as a first-linetreatment of patients with schizophrenia by theprovincial healthcare plan. Quetiapine had thelowest usage of all atypicals across all provinces asmonotherapy, but was not in wide usage at thetime (1999–2000) when patients were beingenrolled into the study.Depot monotherapy medications in the initial
assessment group was used by 6% but again had
regional variations with most usage in BC (eight of64, 13%) and lowest in Quebec (one of 49, 2%).This pattern of use whilst clinically interesting isstatistically non-significant. Multiple medicationswere used least in BC and Saskatchewan/Manitobaand most in Ontario, Quebec and Atlantic Prov-inces, the reasons for this are unclear, as we did nothave further information on norms for medicationusage in the data set collected.It is of note that the dosage of medications used
by patients at time of study entry. The mean doseswere risperidone 3.5 mg (SD 2.2), quetiapine296 mg (SD 211) olanzapine 14.8 mg (SD 7.8),and clozapine 326 mg (SD 162). There was relat-ively little change in dosage used over the 2-year
Table 2. Medication usage at initial assessmentand persistence at year 1 and year 2
Initial therapy Initial assessment, n (%)
Retention, n (%)
Year 1 Year 2
Atypical monotherapyClozapine 61 (13.6) 53 (86.9) 45 (73.8)Olanzapine 92 (20.5) 73 (79.3) 55 (59.8)Quetiapine fumarate 21 (4.7) 15 (71.4) 11 (52.4)Risperidone 102 (22.8) 74 (72.5) 55 (53.9)
Other therapiesSingle typical 21 (4.7) 17 (81.0) 11 (52.4)Multiple typical 5 (1.1) 2 (40.0) 3 (60.0)Typical + atypical 24 (5.4) 18 (75.0) 15 (62.5)Multiple typical (incl. depot) 8 (1.8) 5 (62.5) 5 (62.5)Single typical (depot) 28 (6.3) 17 (60.7) 15 (53.6)Typical (depot) + atypical 15 (3.3) 9 (60.0) 5 (33.3)Randomized clinical trial� 46 (10.3) 39 (84.8) 29 (63.0)No medication� 7 (1.6) 3 (42.9) 1 (14.3)Multiple atypicals� 18 (4.0) 10 (55.6) 7 (38.9)Total 448 (100.0) 335 (74.8) 257 (57.4)
At initial assessment, percentages indicate proportion of study population using each therapy. Retention at years 1and 2 indicate patients who remain in the study and on the initial therapy.�Subjects on these therapies at the initial assessment were not included in regression models.
Table 3. Treatment at initial assessment by region
Treatment
Region, n (%)
British Columbia Alberta Saskatchewan/Manitoba Ontario Quebec Atlantic Total
Clozapine 11 (17.2) 17 (24.3) 5 (6.6) 10 (10.3) 4 (8.2) 14 (15.2) 61 (13.6)Olanzapine 19 (29.7) 16 (22.9) 17 (22.4) 14 (14.4) 9 (18.4) 17 (18.5) 92 (20.5)Quetiapine fumarate 4 (6.3) 2 (2.9) 5 (6.6) 9 (9.3) 1 (1.1) 21 (4.7)Risperidone 13 (20.3) 13 (18.6) 23 (30.3) 19 (19.6) 5 (10.2) 29 (31.5) 102 (22.8)Single typical 3 (4.7) 2 (2.9) 7 (9.2) 5 (5.2) 1 (2.0) 3 (3.3) 21 (4.7)Multiple typical 1 (1.4) 1 (1.3) 1 (1.0) 2 (4.1) 5 (1.1)Typical + atypical 2 (3.1) 2 (2.9) 3 (3.9) 8 (8.2) 7 (14.3) 2 (2.2) 24 (5.4)Multiple typical (depot) 2 (3.1) 4 (4.1) 2 (2.2) 8 (1.8)Single typical (depot) 8 (12.5) 4 (5.7) 5 (6.6) 3 (3.1) 1 (2.0) 7 (7.6) 28 (6.3)Typical + atypical (depot) 1 (1.4) 4 (5.3) 4 (4.1) 2 (4.1) 4 (4.3) 15 (3.3)Randomized clinical trial� 8 (11.4) 5 (6.6) 15 (15.5) 12 (24.5) 6 (6.5) 46 (10.3)No medication� 2 (3.1) 1 (1.4) 1 (1.3) 1 (2.0) 2 (2.2) 7 (1.6)Multiple atypicals� 3 (4.3) 5 (5.2) 5 (10.2) 5 (5.4) 18 (4.0)Total 64 (100.0) 70 (100.0) 76 (100.0) 97 (100.0) 49 (100.0) 92 (100.0) 448 (100.0)
Usage of clozapine vs. other treatments across regions compared by chi-square test, P ¼ 0.023.�Subjects on these therapies at the initial assessment were not included in regression models.
Williams et al.
14

period in any of the atypical monotherapy groupswho persisted in the study on their originalmedications.Figure 1 shows the number of patients switching
from one medication to another over time. Cloza-pine patients were most likely to stay with initialtreatment (53 of 61 at year 1, 86.9%). Over timemany patients switched from initial medication toanother neuroleptic, and a not insignificantnumber in the 2 year completers had switchedback to baseline medication (see Fig. 1). Theretention of patients on typical depot was low at42.9% (12 of 28) at the end of year 2.A survival analysis (Kaplan–Meier survival
curves; see Fig. 2) for persistence on atypicalmonotherapies at the initial assessment indicated
87% of clozapine patients, 83% of olanzapinepatients, 76% of quetiapine and 75% of risperi-done patients remained on that medication at theend of 1 year. At the end of the second year 80% ofclozapine, 77% of olanzapine, 67% of risperidoneand 66% of quetiapine patients remained on initialmedication. After adjusting for differences incovariates at the initial assessment using a propor-tional hazards regression model, persistence oninitial atypical monotherapy varied significantly byatypical monotherapy (see Table 4). Specifically,clozapine and olanzapine patients are approxi-mately twice as likely to stay on original medica-tion as risperidone patients (P ¼ 0.021 and 0.049respectively). As a switch to clozapine is usuallybecause of treatment resistance with other phar-
Risperidone (n = 53)
Dropout (n = 13)
Other (n = 8)
Risperidone (n = 74)
Other (n = 16)
Dropout (n = 4)
Risperidone (n = 2)
Clozapine (n = 1)
Other (n = 23)
Dropout (n = 5)
Risperidone (n = 102)
Olanzapine (n = 55)
Dropout (n = 12)
Other (n = 6)
Olanzapine (n = 73)
Other (n = 9)
Dropout (n = 4)Other (n = 13)
Dropout (n = 5)
Dropout (n = 1)Clozapine (n = 1)
Olanzapine (n = 92)
Clozapine (n = 43)
Dropout (n = 7)
Other (n = 3)
Clozapine (n = 53)
Other (n = 3)
Clozapine (n = 2)
Dropout (n = 1)
Other (n = 6)
Dropout (n = 2)
Clozapine (n = 61)
Quetiapine furmarate (n = 11)
Dropout (n = 3)
Other (n = 1)
Quetiapine furmarate (n = 15)
Other (n = 2)
Clozapine (n = 1)
Dropout (n = 1)
Other (n = 4)
Other (n = 1)Clozapine (n = 1)
Dropout (n = 1)
Quetiapine furmarate (n = 21)
Single typical (n = 11)
Dropout (n = 3)
Other (n = 3)
Single typical (n = 17)
Other (n =3)
Dropout (n = 1)Other (n = 4)
Single typical (n = 21)
Single typical (DEPOT) (n = 12)
Dropout (n = 2)
Other (n = 2)
Clozapine (n = 1)
Single typical (DEPOT) (n = 17)
Other (n = 6)
Single typical (DEPOT) (n = 3)
Dropout (n = 1)
Other (n = 10)
Dropout (n = 1)
Single typical (DEPOT) (n = 28)
Fig. 1. Treatment switching by studyyear.
Canadian measurement study in schizophrenia
15
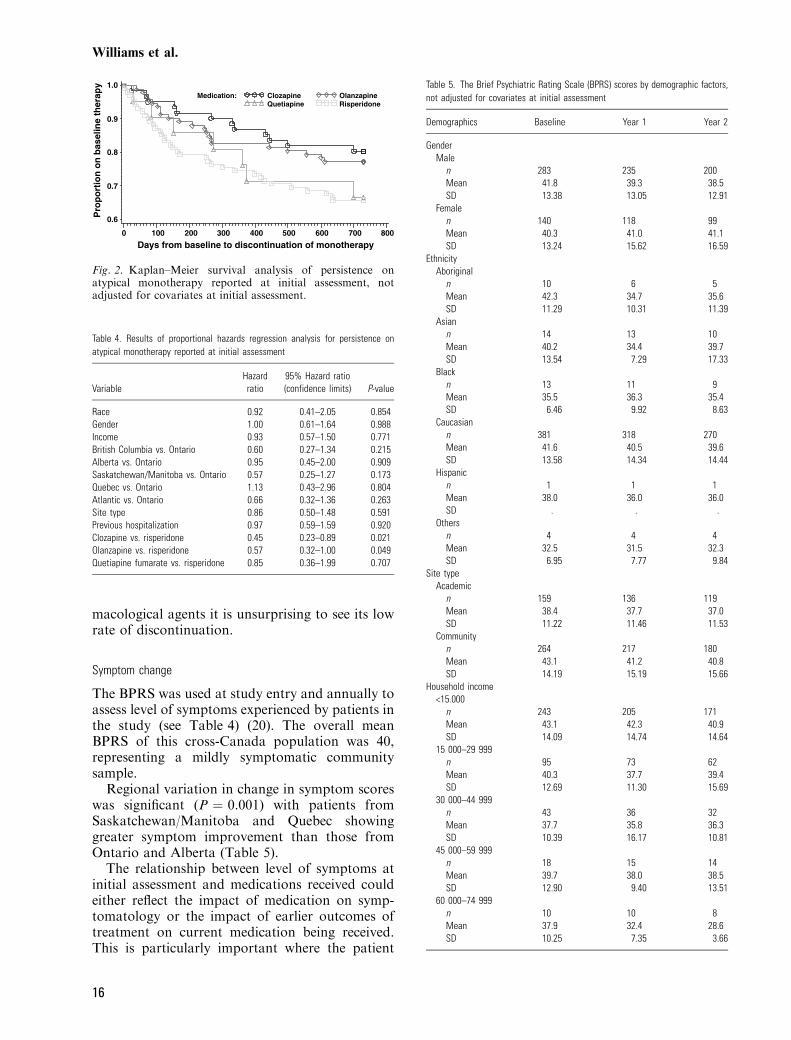
macological agents it is unsurprising to see its lowrate of discontinuation.
Symptom change
The BPRS was used at study entry and annually toassess level of symptoms experienced by patients inthe study (see Table 4) (20). The overall meanBPRS of this cross-Canada population was 40,representing a mildly symptomatic communitysample.Regional variation in change in symptom scores
was significant (P ¼ 0.001) with patients fromSaskatchewan/Manitoba and Quebec showinggreater symptom improvement than those fromOntario and Alberta (Table 5).The relationship between level of symptoms at
initial assessment and medications received couldeither reflect the impact of medication on symp-tomatology or the impact of earlier outcomes oftreatment on current medication being received.This is particularly important where the patient
Medication: Clozapine OlanzapineQuetiapine Risperidone
Pro
po
rtio
n o
n b
asel
ine
ther
apy
0.6
0.7
0.8
0.9
1.0
Days from baseline to discontinuation of monotherapy0 100 200 300 400 500 600 700 800
Fig. 2. Kaplan–Meier survival analysis of persistence onatypical monotherapy reported at initial assessment, notadjusted for covariates at initial assessment.
Table 4. Results of proportional hazards regression analysis for persistence onatypical monotherapy reported at initial assessment
VariableHazardratio
95% Hazard ratio(confidence limits) P-value
Race 0.92 0.41–2.05 0.854Gender 1.00 0.61–1.64 0.988Income 0.93 0.57–1.50 0.771British Columbia vs. Ontario 0.60 0.27–1.34 0.215Alberta vs. Ontario 0.95 0.45–2.00 0.909Saskatchewan/Manitoba vs. Ontario 0.57 0.25–1.27 0.173Quebec vs. Ontario 1.13 0.43–2.96 0.804Atlantic vs. Ontario 0.66 0.32–1.36 0.263Site type 0.86 0.50–1.48 0.591Previous hospitalization 0.97 0.59–1.59 0.920Clozapine vs. risperidone 0.45 0.23–0.89 0.021Olanzapine vs. risperidone 0.57 0.32–1.00 0.049Quetiapine fumarate vs. risperidone 0.85 0.36–1.99 0.707
Table 5. The Brief Psychiatric Rating Scale (BPRS) scores by demographic factors,not adjusted for covariates at initial assessment
Demographics Baseline Year 1 Year 2
GenderMale
n 283 235 200Mean 41.8 39.3 38.5SD 13.38 13.05 12.91
Femalen 140 118 99Mean 40.3 41.0 41.1SD 13.24 15.62 16.59
EthnicityAboriginal
n 10 6 5Mean 42.3 34.7 35.6SD 11.29 10.31 11.39
Asiann 14 13 10Mean 40.2 34.4 39.7SD 13.54 7.29 17.33
Blackn 13 11 9Mean 35.5 36.3 35.4SD 6.46 9.92 8.63
Caucasiann 381 318 270Mean 41.6 40.5 39.6SD 13.58 14.34 14.44
Hispanicn 1 1 1Mean 38.0 36.0 36.0SD . . .
Othersn 4 4 4Mean 32.5 31.5 32.3SD 6.95 7.77 9.84
Site typeAcademic
n 159 136 119Mean 38.4 37.7 37.0SD 11.22 11.46 11.53
Communityn 264 217 180Mean 43.1 41.2 40.8SD 14.19 15.19 15.66
Household income<15.000
n 243 205 171Mean 43.1 42.3 40.9SD 14.09 14.74 14.64
15 000–29 999n 95 73 62Mean 40.3 37.7 39.4SD 12.69 11.30 15.69
30 000–44 999n 43 36 32Mean 37.7 35.8 36.3SD 10.39 16.17 10.81
45 000–59 999n 18 15 14Mean 39.7 38.0 38.5SD 12.90 9.40 13.51
60 000–74 999n 10 10 8Mean 37.9 32.4 28.6SD 10.25 7.35 3.66
Williams et al.
16

population is on more than one medication, asthis usually reflects poor response on one medi-cation (of which many may have been tried beforethe clinician decided to use polypharmacy). Thuswhilst patients on monotherapy with atypicalagents appeared to have better outcomes (lesssymptoms) than patients on multiple medicationsafter 2 years of being in the study this could aseasily reflect that patients on multiple medicationswere on this because of having a more refractoryillness, than that monotherapy treatment wassuperior. Table 6 summarizes raw scores forinitial entry, 1 year and 2 year symptom (BPRS)scores; after adjusting for level of symptomatol-ogy and other covariates recorded at the initialassessment we found there were statisticallysignificant differences with regard to region, age,gender and type of medication at year 1. Nodifferences were found in BPRS scores withregard to income, ethnicity, previous hospitaliza-tion, years with illness and site (academic vs.community) (Table 7).Comparisons between monotherapy atypical
agents showed no significant differences. However,clozapine, risperidone and olanzapine (but notquetiapine) showed greater symptom improvementcompared to patients on �other� medications(Table 8). This group included patients on mono-
therapy typical, multiple typical and depot medi-cations.After adjusting for initial covariates, changes in
BPRS from initial assessment to year 2 showedstatistically significant differences with regard togender (P ¼ 0.022), region (P < 0.0001) anddifferences approaching statistical significance for
Table 5. Continued
Demographics Baseline Year 1 Year 2
‡75 000n 11 11 9Mean 32.6 32.8 32.6SD 9.51 9.27 10.25
RegionBritish Columbia
n 63 56 38Mean 42.1 40.4 44.0SD 15.22 11.46 16.64
Albertan 61 49 44Mean 45.0 46.7 47.1SD 15.94 19.36 18.49
Saskatchewan/Manitoban 73 55 49Mean 41.0 35.7 32.5SD 12.69 11.73 8.04
Ontarion 91 77 68Mean 41.4 42.3 40.5SD 12.89 15.75 13.24
Quebecn 47 35 27Mean 47.4 43.6 42.2SD 12.08 12.21 11.93
Atlanticn 88 81 73Mean 35.1 34.3 34.6SD 8.45 8.14 11.43
Table 6. The Brief Psychiatric Rating Scale (BPRS) scores by therapy at initialassessment, not adjusted for covariates at initial assessment
Therapy at initial assessment Baseline Year 1 Year 2
Clozapinen 59 51 44Mean 43.1 41.8 40.9SD 13.09 13.66 15.14
Olanzapinen 87 72 57Mean 40.9 39.1 38.3SD 13.45 13.63 13.25
Quetiapine fumaraten 20 17 13Mean 44.9 39.9 36.7SD 16.06 13.35 11.38
Risperidonen 97 84 71Mean 38.3 34.9 35.1SD 11.45 10.46 11.04
Single typicaln 21 17 13Mean 36.4 38.6 33.7SD 15.58 16.10 16.72
Multiple typicaln 4 4 3Mean 57.3 50.5 52.3SD 14.93 14.55 23.07
Typical + atypicaln 24 22 19Mean 48.8 55.1 46.1SD 14.70 19.67 15.25
Multiple typical (depot)n 8 8 7Mean 54.0 48.9 49.7SD 22.68 16.38 18.19
Single typical (depot)n 27 23 23Mean 35.6 38.0 43.6SD 8.13 11.38 19.62
Typical + atypical (depot)n 14 8 9Mean 42.6 37.3 47.7SD 11.75 11.03 17.47
Randomized clinical trial�n 39 27 24Mean 40.5 37.6 35.8SD 9.43 10.69 5.91
No medication�n 7 6 3Mean 44.9 41.3 38.7SD 18.48 14.33 9.61
Multiple atypicals�n 16 14 13Mean 45.5 44.9 45.2SD 12.06 13.72 14.26
�Subjects on these therapies at the initial assessment were not included inregression models.
Canadian measurement study in schizophrenia
17

medications (P ¼ 0.056). As in the year 1 compar-isons there were no statistically significant differ-ences with regard to race, age range, familyincome, site type, previous history of hospitaliza-tion or years with illness. In this 2-year cohorthousehold income was not a predictor of symptomchange. In contrast to other studies (4, 15, 19) andto year 1 assessments male patients improvedsymptomatologically more than female patients(P ¼ 0.022). There is no obvious explanation forthis finding; female patients [consistent with (4, 15)]had slightly lower BPRS scores at entry to study,but over the 2-year study male patients continuedto show symptomatic improvement whilst femalesdid not.
As in the year 1 cohort, at 2 years the sameregional differences persisted (P < 0.0001). Medi-cation findings persisted (Tables 5, 7 and 8) withclozapine, risperidone and olanzapine (but notquetiapine) showing significantly greater symptomimprovement from entry than patients on othermedications.
Hospitalization
Hospitalization rates are important because of thefinancial costs associated (21) and the burden theyimpose on patients and their families. Of the 423patients completing the first year of the study, 61(14.4%) patients were admitted to hospital
Table 7. Results of linear model analysis of BriefPsychiatric Rating Scale (BPRS) change from initialassessment
Source df Mean square F-value P-value
(a) Initial assessment to year 1BPRS at initial assessment 1 5181.94 55.65 <0.0001Gender 1 427.65 4.59 0.032Race 1 330.82 3.55 0.061Age at initial assessment 1 362.76 3.90 0.050Family income 1 228.75 2.46 0.118Region 5 404.35 4.34 0.001Site type 1 149.13 1.60 0.207Previous psychiatric hospitalization 1 208.85 2.24 0.135Therapy at initial assessment� 4 234.92 2.52 0.041Years with illness 1 42.47 0.46 0.500
(b) Initial assessment to year 2BPRS at initial assessment 1 6937.27 54.82 <0.0001Gender 1 674.94 5.33 0.022Race 1 27.23 0.22 0.643Age at initial assessment 1 25.35 0.20 0.655Family income 1 2.54 0.02 0.888Region 5 768.90 6.08 <0.0001Site type 1 376.84 2.98 0.086Previous psychiatric hospitalization 1 356.71 2.82 0.094Therapy at initial assessment� 4 295.93 2.34 0.056Years with illness 1 4.86 0.04 0.845
�Therapy coded as: clozapine, olanzapine, quetiapine fumarate, risperidone and other therapies (any of: single typical,multiple typical, typical + atypical, multiple typical (incl. depot), single typical (depot), typical (depot) + atypical).
Table 8. Estimated change in Brief PsychiatricRating Scale (BPRS) from initial assessment bytreatment, after adjusting for covariates at initialassessment
TreatmentAdjustedmean
StandardError
P-value
vs. clozapine vs. olanzapine vs. quetiapine vs. risperidone
(a) Initial assessment to year 1Clozapine )3.30 1.620Olanzapine )3.53 1.476 0.905Quetiapine fumarate )3.69 2.597 0.895 0.953Risperidone )4.59 1.378 0.484 0.510 0.732Therapy: other 0.40 1.301 0.037 0.018 0.134 0.003
(b) Initial assessment to year 2Clozapine )3.43 2.064Olanzapine )4.22 1.956 0.734Quetiapine fumarate )5.51 3.411 0.576 0.718Risperidone )3.91 1.751 0.836 0.881 0.645Therapy: other 1.04 1.600 0.043 0.013 0.067 0.017
The adjusted mean is an estimate of the mean change after adjusting for covariates; P-values have not been adjustedfor multiple testing.
Williams et al.
18

(Table 9). Of the 61 admissions 45 were because ofdecompensated psychotic illness and 16 were formedical reasons including pneumonia, childbirth,breast reduction, biopsy and appendicitis.After adjusting for differences in covariates at
study entry, two factors were found to be signifi-cantly correlated with risk of hospitalization
during both year 1 and year 2 of the study(Table 10a,b); these were history of hospitalizationin the 2 years prior to study entry and the region ofCanada the patient was from. There were nostatistically significant findings with respect togender or age of the patient, ethnicity, householdincome initial medications (on intent to treat basis)or duration of illness.For those patients who had been hospitalized
(n ¼ 164) in the 2 years prior to baseline, 21%were readmitted in the first year of the study and28% by the end of the second year (see Table 11).Again adjusting for differences in the covariatesrecorded at the initial assessment, those patientswho had been hospitalized in the 2 years prior toentry to the study were significantly more likely tobe (re)admitted at both 1 year (P ¼ 0.008) and2 years (P ¼ 0.001)(Table 10a,b).The patients from BC had a significantly lower
rate of hospitalization compared to other provincesat year 2 (P ¼ 0.030)(Table 10b). In contrastpatients from Quebec had a significantly higher
Table 10. Results of logistic regression analysis for admission to hospital
Parameter df Wald chi-square P-value
(a) Initial assessment to year 1Gender (female) 1 0.02 0.902Previous psychiatric
hospitalization (no/unknown)1 7.07 0.008
Race (Caucasian) 1 3.23 0.072Age at initial assessment 1 0.24 0.626Income (<$30 000) 1 0.40 0.525Region
Alberta 1 2.84 0.092Atlantic 1 0.087 0.768British Columbia 1 6.69 0.100Ontario 1 0.56 0.456Quebec 1 11.88 0.001
Site type (academic) 1 0.78 0.376Treatment
Clozapine 1 0.14 0.713Olanzapine 1 3.32 0.068Quetiapine fumarate 1 2.53 0.112Risperidone 1 0.57 0.451
Years with illness 1 0.78 0.378(b) Initial assessment to year 2Gender (female) 1 1.21 0.272Previous psychiatric
hospitalization (no/unknown)1 10.40 0.001
Age at initial assessment 1 1.92 0.166Income (<$30 000) 1 2.83 0.092Region
Alberta 1 1.96 0.162Atlantic 1 0.15 0.701British Columbia 1 4.70 0.030Ontario 1 0.62 0.432Quebec 1 10.39 0.001
Site type (academic) 1 6.77 0.009Treatment
Clozapine 1 0.18 0.669Olanzapine 1 3.50 0.062Quetiapine fumarate 1 1.32 0.250Risperidone 1 0.37 0.543
Years with illness 1 1.08 0.300
Table 9. Admission to hospital for any reason not adjusted for covariates at initialassessment
Region
Year 1 cohort Year 2 cohort
n (%) Total n (%) Total
British Columbia 2 (3.1) 63 5 (9.0) 55Alberta 14 (22.9) 61 16 (32.6) 49Saskatchewan/Manitoba 7 (9.5) 73 6 (11.5) 52Ontario 15 (16.4) 91 17 (21.7) 78Quebec 13 (27.6) 47 12 (37.5) 32Atlantic 10 (11.3) 88 13 (16.0) 81Total 61 (14.4) 423 69 (19.8) 347
Table 11. Admission to hospital by history of previous psychiatric hospitalization in2 years before enrolment, not adjusted for covariates at initial assessment
Previous psychiatric hospitalization
Initial assessmentto year 1
Initial assessmentto year 2
n (%) Total n (%) Total
Unknown 0 (0.0) 2 0 (0.0) 1No 26 (10.1) 257 33 (15.1) 218Yes 35 (21.3) 164 36 (28.1) 128Total 61 (14.4) 423 69 (19.8) 347
Table 12. Admission to hospital for any reason by intent to treat
Treatment group
Initial assessmentto year 1
Initial assessmentto year 2
n (%) Total n (%) Total
Atypical monotherapyClozapine 9 (15.2) 59 12 (23.5) 51Olanzapine 7 (8.0) 87 9 (12.8) 70Quetiapine fumarate 5 (25.0) 20 5 (31.2) 16Risperidone 10 (10.3) 97 14 (17.5) 80
Other therapiesSingle typical 2 (9.5) 21 2 (11.7) 17Multiple typical 2 (50.0) 4 2 (50.0) 4Typical + atypical 10 (41.6) 24 10 (45.4) 22Multiple typical (depot) 1 (12.5) 8 2 (25.0) 8Single typical (depot) 3 (11.1) 27 4 (16.6) 24Typical + atypical (depot) 3 (21.4) 14 3 (33.3) 9Randomized clinical trial� 3 (7.6) 39 2 (6.8) 29No medication� 2 (28.5) 7 0 (0.0) 4Multiple atypicals� 4 (25.0) 16 4 (30.7) 13Total 61 (14.4) 423 69 (19.8) 347
Analysis of treatment group and cohort, not adjusted for covariates at initialassessment.�Subjects on these therapies at the initial assessment were not included inregression models.
Canadian measurement study in schizophrenia
19

rate of hospitalization (P ¼ 0.001 at year 1 andP ¼ 0.001 at year 2) (see Table 10a,b).In the academic centres those with less than
3 years duration of illness were less likely to behospitalized than those from non-academiccentres, at year 2 (P ¼ 0.009) though not at year1 (see Table 10b).At the completion of year 1, patients on risperi-
done, olanzapine and clozapine were least likely tobe hospitalized (seeTable 12). Interestingly those onsingle typical depot (11.1%) had similarly low ratesof hospitalization [however, see Ref. (3) for theirreduced quality of life]. Patients onmultiple typicals(50%) were most likely to be hospitalized, followedclosely by those on a combination of typical andatypical (41.6%). However, none of these findingsreached statistical significance once adjustmentswere made for differences at study entry.
Discussion
In this survey of routine clinical practice in Canadawithin the 2-year period reported on, most of thefindings were statistically non-significant but oftenshowed trends of clinical interest. Regional differ-ences were noted in both utilization of types ofantipsychotics and hospitalization rates. Thesefactors warrant further exploration. As in otherstudies patients with prior hospitalizations did lesswell than those without previous hospitalizations,in respect to likelihood of hospitalization in theperiod under study.The atypical neuroleptics clozapine, risperidone
and olanzapine produced similar amelioration ofsymptoms over the 2-year study period and werestatistically significantly superior to typical neuro-leptics. Medication type had no significant impacton hospitalization. Patients on clozapine andolanzapine were more likely to persist on treatmentthan other medication groups.Clearly the data must be interpreted cautiously
given that the sample size of 448 patients withschizophrenia and related psychotic disorders(although the largest sample of Canadian patientsstudied in depth for an extended period of time) issmall compared to the total number of patientstreated for these illnesses in Canada (approxi-mately 200 000).
Acknowledgements
This study was sponsored by Janssen-Ortho, Inc. and admin-istered by Syreon Corporation, Canada.The Scientific Advisory Committee:Dr Lili Kopala, Vancouver, BCDr Ashok Malla, Montreal, PQ
Dr Geoff Smith, Vancouver, BCDr Richard Williams, Victoria, BCWe acknowledge the participation of the members of theCNOMSS group:Dr Jean-Michel Beau, Malartic; Dr Linda Beauclair, Montreal;Dr Pierre Chue, Edmonton; Dr Hubert Colohan, Claresholm;Dr Norman Costigan, Red Deer; Dr John Dougan, Acton;Dr Angelo Fallu, Sherbrooke; Dr Brian Hoffman, Toronto;Dr Sunny Johnson, Mississauga; Dr Jamie Karagianis,St Johns; Dr Lili Kopala, Halifax; Dr Ivan Kowalchuk,Winnipeg; Dr Alain Labelle, Ottawa; Dr Pierre Landry,Montreal; Dr Paul Latimer, Kelowna; Nadia Lesnikova,Vancouver; Dr Henry Leung, Sault Ste Marie; Dr WilsonLit, Guelph; Dr Ashok Malla, London; Dr Fiona McGregor,Vernon; Dr Alexander McIntyre, Penticton; Dr CharlesMesser, Regina; Dr Roumen Milev, Regina; Dr HeatherMilliken, Halifax; Dr Javad Moamai, Hull; Dr David Mulhall,Kentville; Dr Saibal Nandy, Medicine Hat; Dr KizhakeRamachandran, North Battleford; Dr Jeff Reiss, Winnipeg;Dr Satish Shrikhande, Saskatoon; Dr Jatindar Takhar,London; Dr Mark Triantifillou, Charlottetown; Dr NormanWhite, Powell River; Dr Richard Williams,Victoria.
Declaration of Interests
G. Smith, L. Kopala, R. Williams and A. Malla are consultantsfor Janssen-Ortho. L. Love and R. Balshaw are employees ofSyreon Corporation, the contract research organization hiredby Janssen-Ortho to collect, manage and analyse the data fromCNOMSS. Statistics were performed by D. Talling andR. Balshaw, Syreon Corporation.The protocol is available from Janssen-Ortho, Inc. by contact-ing Doanh Luong ([email protected]).
References
1. Liberman RP, Kopelowicz A, Ventura J, Gutkind D.Operational criteria and factors related to recoveryfrom schizophrenia. Int Rev Psychiatry 2002;14:256–272.
2. Malla AK, Norman RM,McLean TS et al. Determinants ofquality of life in first-episode psychosis. Acta PsychiatrScand 2004;109:46–54.
3. Procyshyn RM, Zerjav S. Drug utilization patterns andoutcomes associated with in-hospital treatment with ris-peridone or olanzapine. Clin Ther 1998;20:1203–1217;discussion 1192–1203.
4. Rabinowitz J, Lichtenberg P, Kaplan Z, Mark M, Nahon D,Davidson M. Rehospitalization rates of chronically illschizophrenic patients discharged on a regimen of risperi-done, olanzapine, or conventional antipsychotics. Am JPsychiatry 2001;158:266–269.
5. Tran PV, Hamilton SH, Kuntz AJ et al. Double-blindcomparison of olanzapine vs. risperidone in the treatmentof schizophrenia and other psychotic disorders. J ClinPsychopharmacol 1997;17:407–418.
6. Norman RM, Malla AK, McLean TS et al. An evaluationof a stress management program for individuals withschizophrenia. Schizophr Res 2002;58:293–303.
7. Falloon IR, Boyd JL, McGill C: Family care of schizo-phrenics. New York: Guildford Press, 1984.
8. Ucok A, Polat A, Genc A, Cakir S, Turan N. Duration ofuntreated psychosis may predict acute treatment responsein first-episode schizophrenia. J Psychiatr Res2004;38:163–168.
Williams et al.
20

9. Hollis C. Adult outcomes of child and adolescent onsetschizophrenia: diagnostic and predictive validity. ActaPsychiatr Scand 2002;106:337–342.
10. Lay B, Blanz B, Hartmann M, Schmidt MH. The psycho-social outcome of adolescent-onset schizophrenia: a 12-year follow-up. Schizophr Bull 2000;26:801–816.
11. Seeman MV. Gender differences in treatment response toschizophrenia. In: Seeman MV, ed. Gender and schizo-phrenia. Washington, DC: APA Press, 1995:227–251.
12. Usall J, Ochoa S, Araya S, Marquez M. Gender differencesand outcome in schizophrenia: a 2-year follow-up study ina large community sample. Eur Psychiatry 2003;18:282–284.
13. Lewine RRJ, Seeman MV. Gender, brain and schizophre-nia. In: Seeman MV, ed. Gender and schizophrenia.Washington, DC: APA Press, 1995:131–158.
14. Harding CM, Hall GM. Long-term outcome studies ofschizophrenia: do females continue to display better out-come as expected? Int Rev Psychiatry 1997;9:409–419.
15. Samele C, Van Os J, Mckenzine K et al. Does socioeco-nomic status predict course and outcome in patients with
psychosis. Soc Psychiatry Psychiatr Epidemiol 2001;36:573–581.
16. Brown AS, Susser ES, Jandorf L, Bromet EJ. Social class oforigin and cardinal symptoms of schizophrenic disordersover the early illness course. Soc Psychiatry PsychiatrEpidemiol 2000;35:53–60.
17. Drake RE, Wallach MA, Teague GB, Freeman DH, PaskusTS, Clark TA. Housing instability and homelessnessamong rural schizophrenic patients. Am J Psychiatry1991;148:330–336.
18. Salokangas RK. Living situation, social network andoutcome in schizophrenia: a five-year prospective follow-up study. Acta Psychiatr Scand 1997;96:459–468.
19. Robinson DG, Woerner MG, McMeniman M, Mendelowitz
A, Bilder RM. Symptomatic and functional recovery froma first episode of schizophrenia or schizoaffective disorder.Am J Psychiatry 2004;161:473–479.
20. Smith G, Malla A, Williams R, Kopala L, Love L, BalshawR. The Canadian national outcomes measurement study inschizophrenia: overview of the patient sample and meth-odology. Acta Psychiatr Scand 2006;113(Suppl. 430):2–9.
Canadian measurement study in schizophrenia
21