medicare bulletin - april 2016 · mm9536: april 2016 quarterly average sales price (asp) medicare...
TRANSCRIPT

HO
ME
HE
ALT
H &
HO
SP
ICE
Medicare BulletinJurisdiction 15
APRIL 2016 • WWW.CGSMEDICARE.COM
Reaching Out to the Medicare
Community
© 2016 Copyright, CGS Administrators, LLC.

Medicare BulletinJurisdiction 15
HO
ME
HE
ALT
H &
HO
SP
ICE
Bold, italicized material is excerpted from the American Medical Association Current Procedural Terminology CPT codes. Descriptions and other data only are copyrighted 2009 American Medical Association. All rights reserved. Applicable FARS/DFARS apply.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016 2
HOME HEALTH PROVIDERS
MM9474: New Condition Code for Reporting Home Health Episodes with No Skilled Visits 3
Probe and Educate Preliminary Results 5
SE1425 (Revised): Extension of Provider Enrollment Moratoria for Home Health Agencies and Part B Ambulance Suppliers 6
HOSPICE PROVIDERS
Calculating and Viewing the Two-tiered RHC and SIA Payment 8
HOME HEALTH & HOSPICE PROVIDERS
CGS Website Updates 11
Claims in a Suspended Status/Location (S/LOC) 13
Medicare Credit Balance Quarterly Reminder 13
MLN Connects™ Provider eNews 14
MM9390: Update to Pub. 100-08, Chapter 15 15
MM9454: Accredited Standards Committee (ASC) X12 Healthcare Claims Acknowledgement (277CA) Flat File Update 16
MM9536: April 2016 Quarterly Average Sales Price (ASP) Medicare Part B Drug Pricing Files and Revisions to Prior Quarterly Pricing Files 17
Provider Contact Center (PCC) Training 18
Quarterly Provider Update 18
SE1128 (Revised): Prohibition on Balance Billing Dually Eligible Individuals Enrolled in the Qualified Medicare Beneficiary (QMB) Program 19
SE1417 (Revised): Implementation of Fingerprint-Based Background Checks 22
Upcoming Educational Events 25
http://go.cms.gov/MLNGenInfo

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
3
For Home Health Providers
MM9474: New Condition Code for Reporting Home Health Episodes with No Skilled Visits
The Centers for Medicare & Medicaid Services (CMS) has issued the following Medicare Learning Network® (MLN) Matters article. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2016-MLN-Matters-Articles.html
MLN Matters® Number: MM9474Related CR Release Date: February 5, 2016 Related CR Transmittal #: R3457CP
Change Request (CR) #: CR 9474 Effective Date: Claims received on or after July 1, 2016Implementation Date: July 5, 2016
Provider Types Affected
This MLN Matters® Article is intended for Home Health Agencies (HHAs) submitting claims to Medicare Administrative Contractors (MACs) for services provided to Medicare beneficiaries.
Provider Action Needed
Change Request (CR) 9474 informs you of revisions of the Medicare billing instructions for home health claims to allow the use of a new condition code - 54. The code indicates that the HHA provided no skilled services during the billing period, but the HHA has documentation on file of an allowable circumstance. Make sure that your billing staffs are aware of these changes.
Background
Sections 1814(a)(2)(C) and 1835(a)(2)(A) of the Social Security Act require that, in order to be eligible to receive Medicare home health services, the beneficiary must have a skilled need (that is, require intermittent Skilled Nursing (SN) services, Physical Therapy (PT), and/or Speech Language Pathology (SLP) services or have a continuing need for Occupational Therapy (OT) services). In order to better enforce this requirement, CR9027 (see related article MM9027 at https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/mm9027.pdf) revised Original Medicare systems to return to the provider any claims for episodes that are the first episode in a sequence of episodes or are the only episode of care received by a beneficiary for which patient eligibility for the Medicare home health benefit has not been established (that is, no SN, PT, or SLP visits reported on the claim).
The Medicare Learning Network® (MLN), offered by the Centers for Medicare & Medicaid Services (CMS), includes a variety of educational resources for health care providers. Access Web-based training courses, national provider conference calls, materials from past conference calls, MLN articles, and much more. To stay informed about all of the CMS MLN products, refer to http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/MailingLists_FactSheet.pdf and subscribe to the CMS electronic mailing lists. Learn more about what the CMS MLN offers at http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNGenInfo/index.html on the CMS website.
Medicare Learning Network®: A Valuable Educational Resource!

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
4
Enforcing this requirement on claims for subsequent episodes of HH care could not be automated using previously existing codes. There may be circumstances which prevent the HHA from delivering the skilled services planned for an episode, such as an unexpected inpatient admission. Determining whether payment is allowable requires development of the claim. Chapter 7, Section 40.1.3, of the “Medicare Benefits Policy Manual” (https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c07.pdf) states:
Since the need for ‘intermittent’ skilled nursing care makes the patient eligible for other covered home health services, the intermediary should evaluate each claim involving skilled nursing services furnished less frequently than once every 60 days. In such cases, payment should be made only if documentation justifies a recurring need for reasonable, necessary, and medically predictable skilled nursing services.
Medicare requested the National Uniform Billing Committee to create a new code that would allow the HHA to indicate upon submission that such documentation exists. A new condition code 54 is effective on July 1, 2016, and is defined as “No skilled HH visits in billing period. Policy exception documented at the HHA.” Submission of this code will streamline claims processing for both the payer and provider. Claims without skilled visits that are submitted without the new condition code will be returned to the provider. This will allow the HHA to:
yy Add any accidentally omitted skilled services to the claim;
yy Submit the claim as noncovered, if appropriate; or
yy Append the new condition code.
These actions will prevent unnecessary reviews and denials for the HHA and allow Medicare to better target medical review resources.
Also, CR9474 address unintended consequences of the implementation of new Healthcare Common Procedure Coding System (HCPCS) codes for skilled nursing visits. CR9369 (see related article MM9369 at https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9369.pdf) terminated HCPCS code G0154, replacing it with two new codes, G0299 and G0300. During the implementation of CR9369, CMS discovered several other processes are affected by this coding change:
yy G0299 and G0300 were previously used to describe defibrillator services. An edit in Medicare systems requires certain diagnosis codes appropriate to support the need for dates of service on or after January 1, 2016.
yy Another edit in Medicare systems currently requires that revenue code 055x is always reported with HCPCS G0154 on hospice claims. This edit would set inappropriately on all hospice claims with dates of service on or after January 1, 2016.
The Centers for Medicare & Medicaid Services (CMS) directed the MACs to temporarily deactivate these two edits to prevent Medicare from returning claims in error. CR9474 revises these edits so MACs can reactivate them without any adverse impact.
Medicare systems also use HCPCS code G0154 in the criteria for identifying the earliest date when calculating Low Utilization Payment Adjustment (LUPA) add on amounts. When home health agencies can no longer report G0154, the earliest visit date for skilled nursing visits reported with G0299 or G0300 will not be used in the calculation. This will result in some claims not receiving LUPA add on amounts or receiving a payment based on the wrong service discipline. CR9474 corrects this error and instruct MACs to adjust home health claims to correct payments within 60 days of the implementation date of CR9474.
Finally, CR9474 contains a number of routine maintenance revisions to home health billing contained in the “Medicare Claims Processing Manual,” Pub. 100-04, Chapter 10, Home Health Agency Billing. The revisions include reformatting the presentation of remittance

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
5
advice codes and ensuring code pairs are compliant with CAQH/CORE requirements. They include an update to the Pricer logic section to reflect case-mix scoring changes for calendar year 2016 and to correctly reflect LUPA add-on calculations which were effective January 1, 2014.
Additional Information
The official instruction, CR9474, issued to your MAC regarding this change, is available at https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R3457CP.pdf on the CMS website.
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1.877.299.4500 and choose Option 1.
For Home Health Providers
Probe and Educate Preliminary Results
Preliminary results from CGS’s medical review of claims for the probe and educate edit shows the top denial reason was related to face to face documentation. As reported in the article, “Missing Home Health Face-to-Face Encounter Documentation” (posted on our website on January 6, 2016, and published in the February 2016 Home Health & Hospice Medicare Bulletin), the primary issue was providers not submitting the actual encounter document from the physician who performed the face to face with the beneficiary. Additional issues include the certifying physician not documenting the date of the F2F encounter or documenting a date which did not correspond to the documentation submitted as the face to face encounter. The second top denial reason has been no response to the Medical Review additional development request (MR ADR).
Specific numbers are as follows-
Number of claims paid 87Number of claims denied - Partial/Full 508# 1 denial reason Certification issues – 57% (breakdown below)
yy F2F missing/incomplete/invalid – 91%yy Untimely POC/certification – 2%yy POC/Certification not signed – 2%yy Missing certification/POC – 2%yy Recertification estimate missing – 1%yy Initial cert missing/invalid – 1%
# 2 denial reason No response to MR ADR – 30%# 3 denial reason Medical necessity of therapy services – 7%
Resources
yy Missing Home Health Face-to-Face Encounter Documentation - http://www.cgsmedicare.com/hhh/pubs/news/2016/0116/cope31607.html
yy Medical Review Additional Development Request (ADR) Process - http://www.cgsmedicare.com/hhh/medreview/adr_process.html
yy myCGS MR ADR Job Aid - http://www.cgsmedicare.com/hhh/pubs/news/2015/0415/cope28413.html
yy Missing/Incomplete/Untimely Face-to-Face Encounter Quick Resource Tool - http://www.cgsmedicare.com/hhh/education/materials/pdf/hh_5fftf_factsheet.pdf
yy Home Health Probe and Educate Medical Review - http://www.cgsmedicare.com/hhh/medreview/hh_probe_educate_mr.html

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
6
For Home Health Providers
SE1425 (Revised): Extension of Provider Enrollment Moratoria for Home Health Agencies and Part B Ambulance Suppliers
The Centers for Medicare & Medicaid Services (CMS) has revised the following Special Edition Medicare Learning Network® (MLN) Matters article. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2014-MLN-Matters-Articles.html
MLN Matters® Number: SE1425Related CR Release Date: N/A Related CR Transmittal #: N/A
Change Request (CR) #: N/AEffective Date: N/A Implementation Date: N/A
Note: This article was revised on February 2, 2016, to reflect an extension of the temporary moratoria for an additional 6 months, as noted in the article. All other information remains the same.
Provider Types Affected
This MLN Matters® Article is intended for home health agencies, home health agency subunits, and part B ground ambulance suppliers in certain geographic areas of Florida, Illinois, Michigan, Texas, Pennsylvania and New Jersey that provide services to Medicare, Medicaid and CHIP beneficiaries.
Provider Action Needed
STOP – Impact to YouEffective January 29, 2016, the temporary moratoria on new home health agencies, home health agency sub-units, and part B ground ambulance suppliers are being extended for an additional 6 months in certain geographic locations.
CAUTION – What You Need to KnowDuring the 6-month temporary moratoria, initial provider enrollment applications and change of information applications to add additional practice locations, received from home health agencies, home health agency sub-units, and Part B ground ambulance suppliers in the moratoria counties will be denied. Application fees that are paid for applications that are denied due to the temporary moratoria will be refunded.
GO – What You Need to DoEffective January 29, 2016, home health agencies, home health agency sub-units, and part B ground ambulance suppliers should not submit initial enrollment applications or change of information applications to add additional practice locations until the 6-month moratoria has expired. CMS will announce in the Federal Register when the moratorium has been lifted, extended, or changed.
Background
In accordance with 42 CFR §424.570(c) at https://www.gpo.gov/fdsys/pkg/CFR-2012-title42-vol3/pdf/CFR-2012-title42-vol3-sec424-570.pdf, the Centers for Medicare & Medicaid Services (CMS) may impose a moratorium on the enrollment of new Medicare providers and suppliers of a specific type or the establishment of new practice locations in a particular geographic area.
On January 29, 2016, CMS announced, in a Federal Register notice (http://federalregister.gov/a/2016-01835), the extension of temporary moratoria on the enrollment of new home health agencies, home health agency sub-units and part B ambulance suppliers in designated geographic locations.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
7
The moratoria initially became effective on July 30, 2013, and the implementation was announced in the Federal Register which may be accessed on the internet at: https://federalregister.gov/a/2013-18394. The moratoria were expanded on January 30, 2014, and the expansion was announced in the Federal Register which may be accessed at: https://federalregister.gov/a/2014-02166.
Moratoria Extension
Effective January 29, 2016, the temporary moratorium on new home health agencies and home health agency sub-units is being extended for an additional 6 months in the areas stated in Table 1, below.
Table 1: Home Health Agencies and Home Health Agency Sub-units under Temporary MoratoriumCity and State CountiesFort Lauderdale, FL BrowardMiami, FL Miami-Dade MonroeDetroit, MI Macomb
MonroeOakland Washtenaw Wayne
Dallas, TX Collin Dallas
Denton Ellis
Kaufman Rockwall
Tarrant
Houston, TX Brazoria Chambers
Fort Bend Galveston
Harris Liberty
Montgomery Waller
Chicago, IL Cook DuPage
Kane Lake
McHenry Will
In addition, the temporary moratorium on new part B ground ambulance suppliers is being extended for an additional 6 months in the areas stated in Table 2, below.
Table 2: Part B Ambulance Suppliers Under 6-month Temporary MoratoriumCity and State CountiesHouston, TX Harris
Brazoria Chambers Fort Bend
Galveston Liberty
Montgomery Waller
Philadelphia, PA Bucks (PA)Delaware (PA)
Montgomery (PA) Philadelphia (PA)
Burlington (NJ)Camden (NJ)
Gloucester (NJ)
Initial provider enrollment applications and change of information applications to add additional practice locations received from home health agencies, home health agency sub-units, and Part B ground ambulance suppliers in the above listed counties will be denied in accordance with 42 CFR §424.570(c). Application fees that are paid for applications that are denied due to the temporary moratoria will be refunded.
Note: Home health agencies, home health agency sub-units, and Part B ground ambulance suppliers are afforded appeal rights. However, the scope of review will be limited to whether the temporary moratorium applies to the provider or supplier appealing the denial. CMS’ basis for imposing a temporary moratorium is not subject to review.
Additional Information
For more information regarding CMS’ use of temporary moratoria, please review MLN Matters® article MM7350 at http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM7350.pdf on the CMS website.
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1.877.299.4500 and choose Option 1.
HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
8
For Hospice Providers
Calculating and Viewing the Two-tiered RHC and SIA Payment
In an effort to enhance hospice provider’s understanding of the two-tiered payment structure (two hospice routine home care (RHC) rates) and the Service Intensity Add-On (SIA) payment implemented by Change Request (CR) 9201 on January 1, 2016, please refer to the following information.
RHC Two-tiered Payment Structure
For claims with dates of service on or after January 1, 2016, there are two hospice RHC rates. A hospice day billed at the RHC level in the first 60 days of a hospice election is paid at the high RHC rate. A hospice day billed at the RHC level on day 61 or later of the hospice election is paid at the low RHC rate. Medicare systems count 60 days from the date of admission regardless of whether some days are covered or non-covered.
For a hospice patient that is discharged and readmitted to hospice services within 60 days of the discharge, the hospice days will continue to follow the patient. If the hospice patient is discharged from hospice care for more than 60 days, a new election to hospice will initiate a reset of the patient’s 60-day window. The new admission will pay at the RHC high rate.
Example:
yy Patient elected hospice for the first time on 01/10/XX.
yy The patient revoked hospice on 01/30/XX.
yy The patient re-elected hospice on 02/16/XX.
yy The patient discharged deceased from hospice care on 03/28/XX.
Since the break in hospice care from 01/30 to 02/16 was less than 60 days, the patient day count continues on the second admission.
RHC provided during the first election from 01/10 to 01/30 accounts for 21 days that the high RHC rate would apply. The 60 day count continues with the second admission on 2/16 and the high RHC rate would apply for an additional 39 days. Day 61 begins the low RHC rate on 3/27.
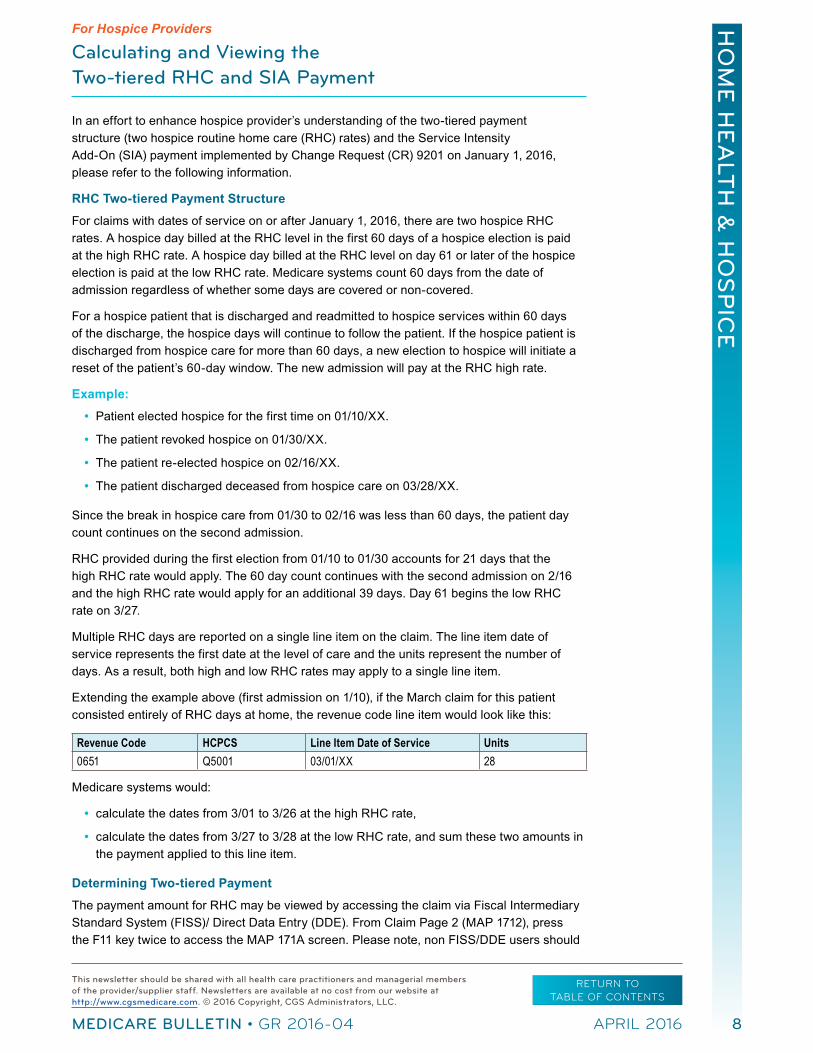
Multiple RHC days are reported on a single line item on the claim. The line item date of service represents the first date at the level of care and the units represent the number of days. As a result, both high and low RHC rates may apply to a single line item.
Extending the example above (first admission on 1/10), if the March claim for this patient consisted entirely of RHC days at home, the revenue code line item would look like this:
Revenue Code HCPCS Line Item Date of Service Units 0651 Q5001 03/01/XX 28
Medicare systems would:
yy calculate the dates from 3/01 to 3/26 at the high RHC rate,
yy calculate the dates from 3/27 to 3/28 at the low RHC rate, and sum these two amounts in the payment applied to this line item.
Determining Two-tiered Payment
The payment amount for RHC may be viewed by accessing the claim via Fiscal Intermediary Standard System (FISS)/ Direct Data Entry (DDE). From Claim Page 2 (MAP 1712), press the F11 key twice to access the MAP 171A screen. Please note, non FISS/DDE users should

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
9
inquire with their software vendors as to how to view these payments outside of FISS/DDE.
Press the F6 key to scroll down until you reach the revenue code line (REV field) 0651. The reimbursement made to this line item displays in the PROV reimbursement field.
MAP171A PAGE 02 CGS J15 MAC - HHH REGION ACPFA052 XX/XX/XXXXXXXX SC INST CLAIM INQUIRY C201135E XX:XX:XXDCN XXXXXXXXXXXXXXXX HIC XXXXXXXXXA RECEIPT DATE XXXXXX TOB 811STATUS P LOCATION B9997 TRAN DT XXXXXX STMT COV DT 0301XX TO 0326XX 4 SERV SERV UTN PGM CAH REV HCPC MODIFIERS DATE RATE TOT-UNT COV-UNT TOT-CHRG COV-CHRG 0651 Q5001 0301XX 28 28 ANES CF ANES BV FQHCADD PC/TC IND HCPC TYPE DEDUCTIBLES COINSURANCE ESRD-RED/ VALCD-05/ BLOOD CASH WAGE-ADJ REDUCED PSYCH/HBCF OTHER PAT -> MSP -> ANSI -> PAY/HCPC MSP -> OUTLIER -> APC CD 00000 PAYER-1 PAYER-2 OTAF DENIAL OCE FLAGS MSP -> IND 1 2 3 4 5 6 7 8 9 ID -> B 3 1 0 0 0 2 0 00 REIMB RESP PAID REDUCT-AMT ANSI PAT -> LABOR NON-LABORPROV -> 4879.87 MED -> 4879.87 PRICER PAY ASC ADJUSTMENT ANSI AMT RTC METHOD IDE/NDC/UPC GRP %CONTR- 37186 <== REASON CODESPRESS PF2-1712 PF3-EXIT PF5-UP PF6-DOWN PF7-PREV PF8-NEXT PF10-LEFT PF11-RIGHT
To determine the rates that apply to the high and low RHC amounts, refer to the “Hospice Payment Rates Calculator” Web page at http://www.cgsmedicare.com/medicare_dynamic/Hospice_Rate_Calculator/Index.asp.
1. From the drop down menu, select the FY applicable to the claim in question. The RHC two-tiered payment structure only applies to services on and after January 1, 2016.
2. Select the state where the beneficiary (patient) received services.
3. Either select the appropriate area from the “Select by Area” drop down menu or select the core-based statistical area (CBSA) from the “Select by CBSA” drop down menu (value code 61 or G8).
4. The 2016 hospice payment rates will display. Refer to example below.
5. Again, extending the example above, the first 26 days are paid at the high RHC payment rate of $180.60 per day (180.60 x 26 = $4695.60). The last 2 days are paid at the lower RHC payment rate of $141.93 per day ($141.93 x 2 = $283.86), for a total reimbursement amount for RHC of $4979.46. Note that a 2 percent Sequestration reduction applies ($4979.46 x .02 = $99.59) which is subtracted from the reimbursement rate ($4979.46 – $99.59= $4879.87).

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
10
Service Intensity Add-On (SIA) Payments
Effective for hospice services with dates of service on and after January 1, 2016, there is an additional payment that will be made in the last 7 days of life for skilled registered nursing (SN) visits (055X and HCPC G0299) and medical social worker (MSW) visits (056X). The SIA payment amount is calculated by multiplying the continuous home care (CHC) rate (per 15 minutes) by the number of units for the combined visits for the day (payment not to exceed 16 units) and adjusted for geographic differences in wages.
In the example below, the patient died on January 26, 2016. Therefore, the SIA payment is applied to claim line 6 and claim line 8. SIA payments are not applied to post mortem visits (PM modifier), or SN visits by a licensed practical nurse (G0300).
TOT COV SERV CL REV HCPC MODIFS RATE UNIT UNIT TOT CHARGE NCOV CHARGE DATE 1 0250 00008 00008 6.00 012016 2 0250 00006 00006 6.00 012016 3 0250 00002 00002 6.00 012016 4 0250 00002 00002 6.00 012016 5 0250 00015 00015 6.00 012016 6 0551 G0299 00007 00007 100.00 012016 7 0651 Q5001 00007 00007 1400.00 012016 8 0561 G0155 00004 00004 50.00 012116 9 0571 G0156 00004 00004 25.00 012116 10 0551 G0300 00002 00002 25.00 012216 11 0551 G0299 PM 00002 00002 25.00 012616 12 0001 1655.00
To determine the SIA payment, access the “Hospice Payment Rates Calculator” at http://www.cgsmedicare.com/medicare_dynamic/Hospice_Rate_Calculator/Index.asp on the CGS website.
1. Find the Continuous Home Care (CHC) rate.
2. Divide this rate by 4 (representing the number of 15 minute increments in an hour).
- The CHC rate is $38.68 ($38.68/4 = 9.67). The $9.67 amount is the SIA payment per every 15 minutes.
In the above example:
- Line 6 (0551) was billed with 7 units ($9.67 x 7 = $67.69)
- Line 8 (0561) was billed with 4 units ($9.67 x 4 = $38.68).
As with the two-tiered RHC payment, access MAP 171A from Claim Page 2 (MAP 1712), and press the F11 key twice. Scroll through the revenue code lines until you reach lines 6 and 8. Below is an example of line 6.
Press the F6 key to scroll down until you reach the revenue code line (REV field) 0551. The reimbursement made to this line item displays in the PROV reimbursement field. Remember that the 2 percent Sequestration reduction also applies. Therefore, the SIA payment of $67.69 - $1.35 (2% sequestration) = $66.34.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
11
MAP171A PAGE 02 CGS J15 MAC - HHH REGION ACPFA052 XX/XX/XXXXXXXX SC INST CLAIM INQUIRY C201135E XX:XX:XXDCN XXXXXXXXXXXXXXXX HIC XXXXXXXXXA RECEIPT DATE XXXXXX TOB 811STATUS P LOCATION B9997 TRAN DT XXXXXX STMT COV DT 0301XX TO 0326XX 6 SERV SERV UTN PGM CAH REV HCPC MODIFIERS DATE RATE TOT-UNT COV-UNT TOT-CHRG COV-CHRG 0551 G0299 012016 7 7 ANES CF ANES BV FQHCADD PC/TC IND HCPC TYPE DEDUCTIBLES COINSURANCE ESRD-RED/ VALCD-05/ BLOOD CASH WAGE-ADJ REDUCED PSYCH/HBCF OTHER PAT -> MSP -> ANSI -> PAY/HCPC MSP -> OUTLIER -> APC CD 00000 PAYER-1 PAYER-2 OTAF DENIAL OCE FLAGS MSP -> IND 1 2 3 4 5 6 7 8 9 ID -> B 3 1 0 0 0 2 0 00 REIMB RESP PAID REDUCT-AMT ANSI PAT -> LABOR NON-LABORPROV -> 66.34 MED -> 66.34 PRICER PAY ASC ADJUSTMENT ANSI AMT RTC METHOD IDE/NDC/UPC GRP %CONTR- 37186 <== REASON CODESPRESS PF2-1712 PF3-EXIT PF5-UP PF6-DOWN PF7-PREV PF8-NEXT PF10-LEFT PF11-RIGHT
NOTE: When multiple SN and/or MSW visits are made on the same day, the reimbursement for the revenue code lines for the same dates will be combined and will display a reimbursement amount in the PROV reimbursement field on only one of those revenue code lines. For example, if a SN and MSW visit were both made on 01/20/16, the PROV field for the SN revenue code line will reflect the reimbursement for both the SN and MSW visit, where the PROV field for the MSW revenue code line will be blank.
Resources
yy CR 9201 / MM9201- https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/2015-Transmittals-Items/R3326CP.html
yy FY 2016 Hospice Final Rule - https://www.gpo.gov/fdsys/pkg/FR-2015-08-06/pdf/2015-19033.pdf
yy CR 9369 / MM9369 - https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/2015-Transmittals-Items/R3378CP.html
yy Centers for Medicare & Medicaid Services (CMS) Internet Only Manual (IOM), Medicare Claims Processing Manual, Publication 100-04, Ch. 11 – Processing Hospice Claims, https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf, Sections 30.2 and 30.2.2.
For Home Health and Hospice Providers
CGS Website Updates
CGS has recently made updates to their website, giving providers additional resources to assist with billing Medicare-covered services appropriately.
Please review the following updates:
yy A new hospice form, “Hospice Dispute Request for Assistance” is now available at http://www.cgsmedicare.com/hhh/forms/pdf/hospice_dispute_form.pdf on the “Forms” Web page at http://www.cgsmedicare.com/hhh/forms/index.html. This form was developed to assist hospice providers in resolving an overlap situation with another Medicare provider. In addition, a new Web page, “Hospice Overlap Dispute” has been

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
12
developed and is available at http://www.cgsmedicare.com/hhh/education/materials/hospice_overlap_dispute.html to explain how to request assistance from CGS.
yy The “Medicare Secondary Payer (MSP) Billing & Adjustments” quick resource tool at http://devinternet/hhh/education/materials/pdf/msp_billing.pdf was revised to include the changes implemented with Change Request 8486 allowing providers to submit MSP claims and adjustments via the Fiscal Intermediary Standard System (FISS) Direct Data Entry (DDE).
yy The “Hot Topics” list on the Home Health & Hospice home page at http://www.cgsmedicare.com/hhh/index.html has been updated to include access to the most current hot topics.
yy The following chapters of the Fiscal Intermediary Standard System (FISS) Guides have been updated.
y� Chapter One: FISS Overview - http://www.cgsmedicare.com/hhh/education/materials/pdf/chapter_1-fiss_overview.pdf
y� Chapter Three: Inquiry Menu - http://www.cgsmedicare.com/hhh/education/materials/pdf/chapter_3-inquiry_menu.pdf
yy The list of Quick Links on the Home Health and Hospice home Web page at http://www.cgsmedicare.com/hhh/index.html was reformatted by making the top five links accessible without having to click on the “expand/collapse” button. The option to expand/collapse then follows the five top links allowing access to additional quick links.
yy The “Home Health Probe and Educate Medical Review” Web page at http://www.cgsmedicare.com/hhh/medreview/hh_probe_educate_mr.html has been updated to include the educational article, “Missing Home Health Face-to-Face Encounter Documentation” to the Resources section.
yy The hospice “Claim Page 02 – Entering a Hospice Claim” Web page at http://cgsmedicare.com/hhh/education/materials/claim_page_2.html was updated to include instruction that separate lines should not be reported for the same level of care unless the site of service Q code changes. This information is included in the first paragraph, and in the REV code description.
yy The answer to question #9 on the “Sequestration Q&A” Web page at http://cgsmedicare.com/hhh/education/faqs/sequestration_faqs.html was updated to indicate that the sequestration order continues until further notice.
yy The “Probe & Educate Process” Web page at http://www.cgsmedicare.com/hhh/medreview/hh_probe_educate_mr.html was updated to clarify that the process applies to all home health claims with an admit date of August 1, 2015, or after.
yy The “Provider Enrollment Revalidation Frequently Asked Questions” at http://www.cgsmedicare.com/hhh/education/faqs/per.html have been revised. All revalidation questions/answers have been removed and replaced with one question related to the Provider Enrollment Revalidation – Cycle 2. Addition questions/answers will be provided as necessary.
yy All “Frequently Asked Questions” at http://www.cgsmedicare.com/hhh/education/faqs/index.html have been reviewed and updated as necessary.
yy The “Provider Enrollment Revalidation” Web page at http://www.cgsmedicare.com/hhh/enrollment/Revalidation.html was updated to include information about the provider enrollment revalidation - cycle 2, which was provided in the Medicare Learning Network (MLN) Matters® Special Edition article, SE1605 (https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/SE1605.pdf).

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
13
yy The link “Enrollment Application Status Check” was added to the Enrollment left side menu at http://www.cgsmedicare.com/hhh/enrollment/index.html. This link directs you to the CGS Application Status Check tool at http://www.cgsmedicare.com/medicare_dynamic/pe/login.asp, which allows you to check the status of your enrollment application by entering the reference number from the acknowledgment letter.
For Home Health and Hospice Providers
Claims in a Suspended Status/Location (S/LOC)
CGS continues to receive a high volume of calls from home health and hospice providers regarding claims that are in a suspended S/LOC. These claims can be identified in the Fiscal Intermediary Standard System (FISS) by a status code beginning with an “S” (example: S B0100).
All Medicare billing transactions will temporarily suspend in different S/LOCs as they process through FISS. Generally, providers only need to take action when they have claims in the following status/locations:
yy S B6001 – An additional development request (ADR) has been requested by CGS to assist with adjudicating a Medicare claim. For additional information about Medical Review (MR) ADRs, and non-MR ADRs, refer to the “Additional Development Request (ADR) Overview” Web page (http://www.cgsmedicare.com/hhh/claims/overview_adr.html).
yy T B9997 – The claim is suspended in the Return to Provider (RTP) file. Claims go to this status/location when there is missing or incorrect information on the claim. Providers need to access the RTP file to correct the claim. For additional information, refer to the “Return to Provider (RTP)” Web page (http://www.cgsmedicare.com/hhh/education/materials/Return_to_Provider.html).
Claims may suspend due to system issues that prevent Medicare billing transactions from processing appropriately. Billing transactions impacted by these issues may be suspended for more than 30 days. CGS provides updates to processing issues on the “Fiscal Intermediary Standard System Claims Processing Issues” Web page at: http://www.cgsmedicare.com/hhh/claims/fiss_claims_processing_issues.html.
The “Fiscal Intermediary Standard System (FISS) Common Locations” Web page at http://www.cgsmedicare.com/hhh/claims/fiss_locations.html is also available as a resource to questions about status/locations.
Please review these resources to help reduce unnecessary calls to the CGS Provider Contact Center (PCC) regarding claims in a suspended S/LOC.
For HHA and Hospice Providers
Medicare Credit Balance Quarterly Reminder
This article is a reminder to submit the Quarterly Medicare Credit Balance Report. The next report is due in our office postmarked by April 30, 2016, for the quarter ending March 31, 2016. A Medicare credit balance is an amount determined to be refundable to the Medicare program for an improper or excess payment made to a provider because of patient billing or claims processing errors.
Each provider must submit a quarterly Medicare Credit Balance Report (CMS-838) and certification for each individual PTAN, which is available at http://www.cms.gov/Medicare/CMS-Forms/CMS-Forms/downloads/CMS838.pdf. The report must be postmarked by
HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
14
the date indicated above. If the report is received with a postmark date later than the date indicated above, we are required to withhold 100 percent of all payments being sent to your facility. This withholding will remain in effect until the reporting requirements are met. If no credit balance exists for your facility during a quarter, a signed Medicare Credit Balance Report certification is still required. Please include your Medicare provider number on the certification form.
Refer to the Medicare Credit Balance Report (CMS-838) form for complete instructions. However, for additional assistance in completing the form, refer to the “Tips on Completing a Credit Balance Report (Form CMS-838)” Web page at http://www.cgsmedicare.com/hhh/financial/838_form_tips.html on the CGS website.
To ensure timely receipt and processing, send the CMS-838/Certification within 30 days of the quarter end date using one of the options below:
yy Reports may be faxed to: MCBR Receipts Attn: Credit Balance Reporting Fax: 1.615.664.5987
yy Regular and Certified Mail: CGS Attn: HHH Credit Balance Reporting PO Box 20014 Nashville, TN 37202
yy ed Ex/UPS/Overnight Courier: CGS J15 Credit Balance Reporting 2 Vantage Way Nashville, TN 37228
Please note that if you have or will be submitting an adjustment, please send the UB-04 along with the CMS-838 form.
yy If you are issuing a refund check for a credit balance:
Send the CMS-838 and a copy of the refund check using one of the options listed above.
Send the refund check with a copy of the CMS-838 or documentation that indicates the check is for a credit balance, the quarter end date, and provider number associated with the check to the following address:
CGS - J15 Home Health and Hospice PO Box 957124 St. Louis, MO 63195-7124
If you have general questions related to the Credit Balance report, refer to the CGS Credit Balance Report (Form CMS-838) website at http://www.cgsmedicare.com/hhh/financial/CMS-588.html or call the Provider Contact Center at 1.877.299.4500 (Option 1). If you have questions about withholding, call 1.877.299.4500 and select Option 4.
For Home Health and Hospice Providers
MLN Connects™ Provider eNews
The MLN Connects™ Provider eNews contains a weeks worth of Medicare-related messages issued by the Centers of Medicare & Medicaid Services (CMS). These messages ensure planned, coordinated messages are delivered timely about Medicare-related topics. The following provides access to the weekly messages. Please share with appropriate staff. If you wish to receive the listserv directly from CMS, please contact CMS at [email protected].

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
15
yy February 18, 2016 - https://www.cms.gov/Outreach-and-Education/Outreach/FFSProvPartProg/Downloads/2016-02-18-eNews.pdf
yy February 25, 2016 - https://www.cms.gov/Outreach-and-Education/Outreach/FFSProvPartProg/Downloads/2016-02-25-Enews.pdf
yy March 3, 2016 - https://www.cms.gov/Outreach-and-Education/Outreach/FFSProvPartProg/Downloads/2016-03-03-eNews.pdf
yy March 10, 2016 - https://www.cms.gov/Outreach-and-Education/Outreach/FFSProvPartProg/Downloads/2016-03-10-eNews.pdf
For Home Health and Hospice Providers
MM9390: Update to Pub. 100-08, Chapter 15
The Centers for Medicare & Medicaid Services (CMS) has issued the following Medicare Learning Network® (MLN) Matters article. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2016-MLN-Matters-Articles.html
MLN Matters® Number: MM9390Related CR Release Date: February 4, 2016 Related CR Transmittal #: R636PI
Change Request (CR) #: CR 9390Effective Date: March 4, 2016 Implementation Date: March 4, 2016
Provider Types Affected
This MLN Matters® Article is intended for providers, including Home Health Agencies (HHAs), submitting claims to Medicare Administrative Contractors (MACs) for services to Medicare beneficiaries.
Provider Action Needed
Change Request (CR) 9390, from which this article was developed, makes several minor revisions to Chapter 15 of the “Medicare Program Integrity Manual.” These changes include, but are not limited to:
1. Clarifying the process for verifying correspondence telephone numbers;
2. Clarifying the process for validating the credentials of technicians of Independent Diagnostic Testing Facilities (IDTFs); and
3. Identifying the timeframe by which approval letters must be sent and to whom they must be sent.
Make sure that your billing staffs are aware of these revisions.
Background
Chapter 15 of the “Medicare Program Integrity Manual” contains instructions regarding the processing of Form CMS-855 applications. CR9390 makes the following key changes:
1. If online verification of an IDTF technician’s credentials is not available or cannot be made, the MAC will request a copy of the technician’s certification card.
2. The MAC will not request a social security card to verify an individual’s identity or social security number.
3. Absent a CMS instruction or directive to the contrary, the MAC will send enrollment approval letters within 5 business days of approving the enrollment application.
4. For all applications other than the Form CMS-855S, the MAC will send development/approval letters/revocation letters, etc., to the contact person if one is listed; otherwise, the contractor may send the letter to the provider or supplier at the provider’s/supplier’s correspondence address or special payments address.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
16
Note: CR9390 does not involve any legislative or regulatory policies and is restricted to changes in operational procedures.Many of the other Chapter 15 revisions are small, such as inserting single words or short sentences, etc. Others are more significant and those revisions are in the revised Chapter 15, which is attached to CR9390.
Additional Information
The official instruction, CR9390, issued to your MAC regarding this change is available at https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R636PI.pdf on the CMS website.
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1.877.299.4500 and choose Option 1.
For Home Health and Hospice Providers
MM9454: Accredited Standards Committee (ASC) X12 Healthcare Claims Acknowledgement (277CA) Flat File Update
The Centers for Medicare & Medicaid Services (CMS) has issued the following Medicare Learning Network® (MLN) Matters article. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2016-MLN-Matters-Articles.html
MLN Matters® Number: MM9454Related CR Release Date: February 4, 2016 Related CR Transmittal #: R1609OTN
Change Request (CR) #: CR 9454Effective Date: July 1, 2016Implementation Date: July 5, 2016
Provider Types Affected
This MLN Matters® Article is intended for physicians, providers, and suppliers submitting claims to Medicare Administrative Contractors (MACs) for services provided to Medicare beneficiaries.
What You Need to Know
Change Request (CR) 9454 updates the Accredited Standards Committee (ASC) X12 Healthcare Claims Acknowledgement (277CA) flat file to allow for larger monetary amounts to meet Medicare’s needs. The 277CA amount fields are currently the same size as the size used for the input files.
Additional Information
The official instruction, CR 9454, issued to your MAC regarding this change is available at https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/2016-Transmittals-Items/R1609OTN.html on the CMS website.
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1.877.299.4500 and choose Option 1.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
17
For Home Health and Hospice Providers
MM9536: April 2016 Quarterly Average Sales Price (ASP) Medicare Part B Drug Pricing Files and Revisions to Prior Quarterly Pricing Files
The Centers for Medicare & Medicaid Services (CMS) has issued the following Medicare Learning Network® (MLN) Matters article. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2016-MLN-Matters-Articles.html
MLN Matters® Number: MM9536Related CR Release Date: February 4, 2016 Related CR Transmittal #: R3450CP
Change Request (CR) #: CR 9536Effective Date: April 1, 2016Implementation Date: April 4, 2016
Provider Types Affected
This MLN Matters® Article is intended for physicians, providers, and suppliers submitting claims to Medicare Administrative Contractors (MACs), including Durable Medical Equipment MACs (DME MACs) and Home Health & Hospice MACs (HH&H MACs), for Part B drugs provided to Medicare beneficiaries.
Provider Action Needed
Medicare will use the April 2016 quarterly Average Sales Price (ASP) and Not Otherwise Classified (NOC) pricing files to determine the payment limit for claims for separately payable Medicare Part B drugs processed or reprocessed on or after April 4, 2016, with dates of services from April 1, 2016, through June 30, 2016.
Change Request (CR) 9536 instructs MACs to implement the April 2016 ASP Medicare Part B drug pricing file for Medicare Part B drugs, and if they are released by the Centers for Medicare & Medicaid Services (CMS), to also implement the revised January 2016, October 2015, July 2015, and April 2015 files. Make sure your billing personnel are aware of these changes.
Background
The ASP methodology is based on quarterly data submitted to CMS by manufacturers. CMS will supply contractors with the ASP and NOC drug pricing files for Medicare Part B drugs on a quarterly basis. Payment allowance limits under the Outpatient Prospective Payment System (OPPS) are incorporated into the Outpatient Code Editor (OCE) through separate instructions that are in the “Medicare Claims Processing Manual,” Chapter 4, Section 50 (https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c04.pdf).
The following table shows how the files will be applied.
Files Effective Date for Dates of ServiceApril 2016 ASP and ASP NOC April 1, 2016, through June 30, 2016January 2016 ASP and ASP NOC January 1, 2016, through March 31, 2016October 2015 ASP and ASP NOC October 1, 2015, through December 31, 2015July 2015 ASP and ASP NOC July 1, 2015, through September 30, 2015April 2015 ASP and ASP NOC April 1, 2015, through June 30, 2015
Additional Information
The official instruction, CR9536 issued to your MAC regarding this change is available at https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R3450CP.pdf on the CMS website.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
18
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1.877.299.4500 and choose Option 1.
For Home Health and Hospice Providers
Provider Contact Center (PCC) Training
Medicare is a continuously changing program, and it is important that we provide correct and accurate answers to your questions. To better serve the provider community, the Centers for Medicare & Medicaid Services (CMS) allows the provider contact centers the opportunity to offer training to our customer service representatives (CSRs). The list below indicates when the home health and hospice PCC at 1.877.299.4500 (option 1) will be closed for training.
Date PCC Training/ClosuresThursday, April 14, 2016 Thursday, April 28, 2016
8:00 a.m. – 10:00 a.m. Central Time
The Interactive Voice Response (IVR) (1.877.220.6289) is available for assistance in obtaining patient eligibility information, claim and deductible information, and general information. For information about the IVR, access the IVR User Guide at http://www.cgsmedicare.com/hhh/help/pdf/IVR_User_Guide.pdf on the CGS website. In addition, CGS’ Internet portal, myCGS, is available to access eligibility information through the Internet. For additional information, go to http://www.cgsmedicare.com/hhh/index.html and click the “myCGS” button on the left side of the Web page.
For your reference, access the “Home Health & Hospice 2016 Holiday/Training Closure Schedule” at http://www.cgsmedicare.com/hhh/help/pdf/2016_holiday_schedule.pdf for a complete list of PCC closures.
For Home Health and Hospice Providers
Quarterly Provider Update
The Quarterly Provider Update is a comprehensive resource published by the Centers for Medicare & Medicaid Services (CMS) on the first business day of each quarter. It is a listing of all nonregulatory changes to Medicare including transmittals, manual changes, and any other instructions that could affect providers. Regulations and instructions published in the previous quarter are also included in the update. The purpose of the Quarterly Provider Update is to:
yy Inform providers about new developments in the Medicare program;
yy Assist providers in understanding CMS programs and complying with Medicare regulations and instructions;
yy Ensure that providers have time to react and prepare for new requirements;
yy Announce new or changing Medicare requirements on a predictable schedule; and
yy Communicate the specific days that CMS business will be published in the Federal Register.
To receive notification when regulations and program instructions are added throughout the quarter, go to https://www.cms.gov/Regulations-and-Guidance/Regulations-and-Policies/QuarterlyProviderUpdates/CMS-Quarterly-Provider-Updates-Email-Updates.html to sign up for the Quarterly Provider Update (electronic mailing list).

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
19
We encourage you to bookmark the Quarterly Provider Update website at https://www.cms.gov/Regulations-and-Guidance/Regulations-and-Policies/QuarterlyProviderUpdates/index.html and visit it often for this valuable information.
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1-877-299-4500 and choose Option 1.
For Home Health and Hospice Providers
SE1128 (Revised): Prohibition on Balance Billing Dually Eligible Individuals Enrolled in the Qualified Medicare Beneficiary (QMB) Program
The Centers for Medicare & Medicaid Services (CMS) has issued the following Special Edition Medicare Learning Network® (MLN) Matters article on February 2, 2015. CMS then issued another revised article on February 5, 2016. The following reflects the revised article issued on February 5, 2016. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2011-MLN-Matters-Articles.html
MLN Matters® Number: SE1128 RevisedRelated CR Release Date: N/A Related CR Transmittal #: N/A
Change Request (CR) #: N/AEffective Date: N/AImplementation Date: N/A
Note: This article was revised on February 4, 2016, to include updated information for 2016 and a correction to the second sentence in paragraph 2 under Important Clarifications Concerning QMB Balance Billing Law on page 3. All other information is the same.
Provider Types Affected
This article pertains to all Medicare physicians, providers and suppliers, including those serving beneficiaries enrolled in original Medicare or a Medicare Advantage plan.
What you Need to Know
STOP – Impact to YouThis Special Edition MLN Matters® Article from the Centers for Medicare & Medicaid Services (CMS) reminds all Medicare providers that they may not bill beneficiaries enrolled in the QMB program for Medicare cost-sharing (such charges are known as “balance billing”). QMB is a Medicare Savings Program that exempts Medicare beneficiaries from Medicare cost-sharing liability.
CAUTION – What You Need to KnowThe QMB program is a State Medicaid benefit that covers Medicare deductibles, coinsurance, and copayments, subject to State payment limits. (States may limit their liability to providers for Medicare deductibles, coinsurance and copayments under certain circumstances.) Medicare providers may not balance bill QMB individuals for Medicare cost-sharing, regardless of whether the State reimburses providers for the full Medicare cost-sharing amounts. Further, all original Medicare and MA providers --not only those that accept Medicaid—must refrain from charging QMB individuals for Medicare cost-sharing. Providers who inappropriately balance bill QMB individuals are subject to sanctions.
GO – What You Need to DoRefer to the Background and Additional Information sections of this article for further details and resources about this guidance. Please ensure that you and your staffs are aware of the federal balance billing law and policies regarding QMB individuals. Contact the Medicaid Agency in the States in which you practice to learn about ways to identify QMB patients in your State and procedures applicable to Medicaid reimbursement for their Medicare cost-sharing. If you are a Medicare Advantage provider, you may also contact the MA plan for

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
20
more information. Finally, all Medicare providers should ensure that their billing software and administrative staff exempt QMB individuals from Medicare cost-sharing billing and related collection efforts.
Background
This article provides CMS guidance to Medicare providers to help them avoid inappropriately billing QMBs for Medicare cost-sharing, including deductibles, coinsurance, and copayments. This practice is known as “balance billing.”
Balance Billing of QMBs Is Prohibited by Federal Law
Federal law bars Medicare providers from balance billing a QMB beneficiary under any circumstances. See Section 1902(n)(3)(B) of the Social Security Act, as modified by Section 4714 of the Balanced Budget Act of 1997. (Please note, this section of the Act is available at http://www.ssa.gov/OP_Home/ssact/title19/1902.htm on the Internet.)
QMB is a Medicaid program for Medicare beneficiaries that exempts them from liability for Medicare cost-sharing. State Medicaid programs may pay providers for Medicare deductibles, coinsurance and copayments. However, as permitted by federal law, States can limit provider reimbursement for Medicare cost-sharing under certain circumstances. See the chart at the end of this article for more information about the QMB benefit.
Medicare providers must accept the Medicare payment and Medicaid payment (if any) as payment in full for services rendered to a QMB beneficiary. Medicare providers who violate these billing prohibitions are violating their Medicare Provider Agreement and may be subject to sanctions. (See Sections 1902(n)(3)(C); 1905(p)(3); 1866(a)(1)(A); 1848(g)(3)(A) of the Social Security Act.)
Inappropriate Balance Billing Persists
Despite federal law, erroneous balance billing of QMB individuals persists. Many beneficiaries are unaware of the billing restrictions (or concerned about undermining provider relationships) and simply pay the cost-sharing amounts. Others may experience undue distress when unpaid bills are referred to collection agencies. See Access to Care Issues Among Qualified Medicare Beneficiaries (QMB), Centers for Medicare & Medicaid Services July 2015 at https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/Downloads/Access_to_Care_Issues_Among_Qualified_Medicare_Beneficiaries.pdf on the CMS website.
Important Clarifications Concerning QMB Balance Billing Law
Be aware of the following policy clarifications to ensure compliance with QMB balance billing requirements. First, know that all original Medicare and MA providers-- not only those that accept Medicaid—must abide by the balance billing prohibitions.
In addition, QMB individuals retain their protection from balance billing when they cross state lines to receive care. Providers cannot charge QMB individuals even if the patient’s QMB benefit is provided by a different State than the State in which care is rendered.
Finally, note that QMBs cannot choose to “waive” their QMB status and pay Medicare cost-sharing. The federal statute referenced above supersedes Section 3490.14 of the “State Medicaid Manual,” which is no longer in effect.
Ways to Improve Processes Related to QMBs
Proactive steps to identify QMB individuals you serve and to communicate with State Medicaid Agencies (and Medicare Advantage plans if applicable), can promote compliance with QMB balance billing prohibitions.
1. Determine effective means to identify QMB individuals among your patients. Find out what cards are issued to QMB individuals so you can in turn ask all your patients if they have them. Learn if you can query state systems to verify QMB enrollment among your

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
21
patients. If you are a Medicare Advantage provider contact the plan to determine how to identify the plan’s QMB enrollees.
2. Discern what billing processes apply to seek reimbursement for Medicare cost-sharing from the States in which you operate. Different processes may apply to original Medicare and MA services provided to QMB beneficiaries. For original Medicare claims, nearly all states have electronic crossover processes through the Medicare Benefits Coordination & Recovery Center (BCRC) to automatically receive Medicare-adjudicated claims.
- If a claim is automatically crossed over to another payer, such as Medicaid, it is customarily noted on the Medicare Remittance Advice.
- Understand the processes you need to follow to request reimbursement for Medicare cost-sharing amounts if they are owed by your State. You may need to complete a State Provider Registration Process and be entered into the State payment system to bill the State.
3. Make sure that your billing software and administrative staff exempt QMB individuals from Medicare cost-sharing billing and related collection efforts.
QMB Eligibility and BenefitsDual Eligibility Eligibility Criteria BenefitsQualified Medicare Beneficiary (QMB only)
yy Resources cannot exceed $7,280 for a single individual or $10,930 in 2015 for an individual living with a spouse and no other dependents.yy Income cannot exceed 100% of the Federal
Poverty Level (FPL) +$20 ($1,001/month – Individual $1,348/month – Couple in 2015).
Note: These guidelines are a federal floor. Under Section 1902 (r)(2) of the Social Security Act, states can effectively raise these limits above these baseline federal standards.
Medicaid Pays Medicare Part A and B premiums, deductibles, co-insurance and co-pays to the extent required by the State Medicaid Plan.yy Exempts beneficiaries from Medicare
cost-sharing chargesyy The State may choose to pay the
Medicare Advantage (Part C) premium.
QMB Plus Meets all of the standards for QMB eligibility as described above, but also meets the financial criteria for full Medicaid coverage.
Provides all benefits available to QMBs, as well as all benefits available under the State Plan to a fully eligible Medicaid recipient
Additional Information
For more information about dual eligible categories and benefits, please visit http://www.medicare.gov/Publications/Pubs/pdf/10126.pdf on the Internet. Also, for more information about QMBs and other individuals who are dually eligible to receive Medicare and Medicaid benefits, please refer to the Medicare Learning Network® publication titled “Medicaid Coverage of Medicare Beneficiaries (Dual Eligibles),” which is available at https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/medicare_beneficiaries_dual_eligibles_at_a_glance.pdf on the CMS website.
For general Medicaid information, please visit the Medicaid Web page at http://www.medicaid.gov/index.html on the CMS website.
Document History
Date of Change DescriptionFebruary 4, 2016 The article was revised on February 4, 2016, to include updated information for 2016
and a correction to the second sentence in paragraph 2 under Important Clarifications Concerning QMB Balance Billing Law on page 3.
February 1, 2016 The article was revised to include updated information for 2016 and a clarifying note regarding eligibility criteria in the table on page 4.
March 28, 2014 The article was revised on to change the name of the Coordination of Benefits Contractor (COBC) to Benefits Coordination & Recovery Center (BCRC).

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
22
For Home Health and Hospice Providers
SE1417 (Revised): Implementation of Fingerprint-Based Background Checks
The Centers for Medicare & Medicaid Services (CMS) has revised the following Special Edition Medicare Learning Network® (MLN) Matters article. This MLN Matters article and other CMS articles can be found on the CMS website at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/2014-MLN-Matters-Articles.html
MLN Matters® Number: SE1417 RevisedRelated CR Release Date: N/A Related CR Transmittal #: N/A
Change Request (CR) #: N/AEffective Date: N/AImplementation Date: N/A
Note: This article was revised on January 27, 2016, to update language in the article and to emphasize affected providers and suppliers in the Caution Section.
Provider Types Affected
This MLN Matters® Special Edition article is intended for all providers and suppliers who submit claims to Medicare Administrative Contractors (MACs) for services provided to Medicare beneficiaries.
Provider Action Needed
STOP – Impact to YouThis Special Edition article is being provided by the Centers for Medicare & Medicaid Services (CMS) to announce the implementation of fingerprint-based background checks as part of enhanced enrollment screening provisions contained in Section 6401 of the Affordable Care Act.
CAUTION – What You Need to KnowFingerprint-based background checks are generally completed on individuals with a 5 percent or greater ownership interest in a provider or supplier that falls under the high risk category. A 5 percent or greater owner includes any individual that has any partnership (general or limited) in a high risk provider or supplier. Note that the high level of risk category applies to providers and suppliers who are newly enrolling Durable Medicare Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) suppliers or Home Health Agencies (HHA). It also applies to providers and suppliers who have been elevated to the high risk category. CMS may adjust a particular provider or supplier’s screening level from “limited” to “high” or “moderate” to “high” if any of the following occur:
yy CMS has imposed a payment suspension within the last 10 years;
yy Has been excluded from Medicare by the OIG;
yy Has had billing privileges revoked by CMS within the previous 10 years;
yy Has been excluded from any Federal Health Care program;
yy Has been subject to any final adverse action, in the previous 10 years;
yy Has been terminated or is otherwise precluded from billing Medicaid; or
yy CMS lifts a temporary moratorium for a particular provider or supplier type and a provider or supplier that was prevented from enrolling based on the moratorium, applies for enrollment as a Medicare provider or supplier at any time within 6 months from the date the moratorium was lifted.
GO – What You Need to DoSee the Background and Additional Information sections of this article for further details.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
23
Background
As part of the enhanced enrollment screening provisions contained in the Affordable Care Act (see http://www.gpo.gov/fdsys/pkg/BILLS-111hr3590enr/pdf/BILLS-111hr3590enr.pdf), the Centers for Medicare & Medicaid Services (CMS) implemented fingerprint-based background checks. The fingerprint-based background checks will be used to detect bad actors who are attempting to enroll in the Medicare program and to remove those currently enrolled. Once fully implemented, the fingerprint-based background check will be completed on all individuals with a 5 percent or greater ownership interest in a provider or supplier that falls under the high risk category. A 5 percent or greater owner includes any individual that has any partnership (general or limited) in a provider or supplier. Fingerprint- based background checks are also required for any provider or supplier who has been elevated to the high risk category for any of the following reasons:
yy CMS has imposed a payment suspension within the last 10 years;
yy Has been excluded from Medicare by the OIG;
yy Has had billing privileges revoked by CMS within the previous 10 years;
yy Has been excluded from any Federal Health Care program;
yy Has been subject to any final adverse action, in the previous 10 years;
yy Has been terminated or is otherwise precluded from billing Medicaid; or
yy CMS lifts a temporary moratorium for a particular provider or supplier type and a provider or supplier that was prevented from enrolling based on the moratorium, applies for enrollment as a Medicare provider or supplier at any time within 6 months from the date the moratorium was lifted.
Please refer to 42 CFR 424.518(c)(3) at http://www.ecfr.gov/cgi-bin/text-idx?SID=a39ae0804106965d82b5ae6413ba550e&node=42:3.0.1.1.11.12.5.11&rgn=div8 on the Internet and the “Medicare Program Integrity Manual” (Chapter 15 (Medicare Enrollment), Section 15.19.2.1C (Screening Categories-Background-High)) at http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/pim83c15.pdf on the CMS website.
Note: The fingerprint-based background checks will be applied to providers and suppliers in the high level of risk category, which includes newly enrolling Durable Medicare Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) suppliers, Home Health Agencies (HHA) and providers and suppliers who have been elevated to the high risk category in accordance with enrollment screening regulations.
The fingerprint-based background check implementation has been phased in beginning in 2014.
Affected providers and suppliers will receive notification of the fingerprint requirements from their MAC. The MAC will send a notification letter to the affected providers or suppliers listing all 5 percent or greater owners who are required to be fingerprinted. The notification letter will be mailed to the provider or supplier’s correspondence address and the special payments address on file with Medicare. Generally, an individual will be required to be fingerprinted only once, but CMS reserves the right to request additional fingerprints if needed.
The relevant individuals will have 30 days from the date of the notification letter to be fingerprinted. If the provider or supplier finds a discrepancy in the ownership listing, the provider or supplier should contact their MAC immediately to communicate the discrepancy and take the appropriate action to update the enrollment record to correctly reflect the ownership information.
The notification letter will identify contact information for the Fingerprint-Based Background Check Contractor (FBBC). The relevant individual(s) are required to contact the FBBC prior to

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
24
being fingerprinted to ensure the fingerprints are accurately submitted to the Federal Bureau of Investigation (FBI) and results are properly returned to CMS. Providers/suppliers may contact the FBBC by telephone or by accessing the FBBC’s website. Contact information for the FBBC will be provided in the notification letter received from the MAC. Once contacted, the FBBC will provide at least three fingerprint locations convenient to the relevant individual’s location. One of these locations will be a local, state, or federal law enforcement facility.
The relevant individuals who are required to undergo the fingerprint-based background check will incur the cost of having their fingerprints taken, and the cost may vary depending on location. Once an individual has submitted his/her fingerprints, if that individual is subsequently required to undergo a fingerprint-based background check in accordance with 42 CFR 424.518(c), CMS will, to the extent possible, rerun the fingerprint-based background check rather than requiring resubmission of fingerprints. You can review 42 CFR 424.518(c) at http://www.ecfr.gov/cgi-bin/text-idx?SID=f14b263d1175a355d736e9f38f3a6baf&node=42:3.0.1.1.11.12.5.11&rgn=div8 on the Internet.
Fingerprinting can be completed on the FD-258 form or electronically at certain locations. CMS strongly encourages all required applicants to provide electronic fingerprints, but CMS will accept the FD-258 card instead. If the FD-258 form is submitted, the FBBC will convert the paper form to electronic submission to the FBI. You can review the FD-258 form at https://www.fbi.gov/about-us/cjis/identity-history-summary-checks/fd-258-1 on the Internet.
Once the fingerprint process is complete, the fingerprints will be forwarded to the FBI for processing. Within 24 hours of receipt, the FBI will compile the background history based on the fingerprints and will share the results with the FBBC. CMS, through the FBBC, will assess the law enforcement data provided for the fingerprinted individuals. The FBBC will review each record and provide a fitness recommendation to CMS. CMS will assess the recommendation and make a final determination.
All fingerprint data will be stored according to:
yy Federal requirements;
yy FBI Security and Management Control Outsourcing Standards for Channelers and Non-Channelers; and
yy The FBI Criminal Justice Information Services (CJIS) Security Policy.
The FBBC will maintain Federal Information Systems Management Act (FISMA) certification and comply with the FBI (CJIS) Security Policy. All data will be secured in accordance with the Privacy Act of 1974 and the FBI CJIS Security Policy.
CMS will rely on existing authority to deny enrollment applications and revoke existing Medicare billing privileges per 42 CFR §424.530(a) and §424.535(a) (http://www.ecfr.gov/cgi-bin/text-idx?SID=f14b263d1175a355d736e9f38f3a6baf&node=42:3.0.1.1.11.12.5.15&rgn=div8) if an individual who maintains a 5 percent or greater direct or indirect ownership interest in a provider or supplier has submitted an enrollment application that contains false or misleading information. Providers or suppliers will be notified by CMS if the assessment of the fingerprint based background check results in the denial of its enrollment application or revocation of its existing Medicare billing privileges.
Additional Information
If you have any questions, please contact a CGS Customer Service Representative by calling the CGS Provider Contact Center at 1.877.299.4500 and choose Option 1.
Document History
Date of Change DescriptionJanuary 27, 2016 The article was revised to update language in the article and to emphasize affected
providers and suppliers in the Caution Section.

HO
ME
HE
ALT
H &
HO
SP
ICE
This newsletter should be shared with all health care practitioners and managerial members of the provider/supplier staff. Newsletters are available at no cost from our website at http://www.cgsmedicare.com. © 2016 Copyright, CGS Administrators, LLC.
MEDICARE BULLETIN • GR 2016-04 APRIL 2016
RETURN TO TABLE OF CONTENTS
25
For Home Health and Hospice Providers
Upcoming Educational Events
The CGS Provider Outreach and Education department offers educational events through webinars and teleconferences throughout the year. Registration for live events is required. For upcoming events, please refer to the Calendar of Events Home Health & Hospice Education Web page at http://www.cgsmedicare.com/hhh/education/Education.html. CGS suggests that you bookmark this page and visit it often for the latest educational opportunities.