medicalprogramsideby - national institutes of health · occasionally, when garbling or noise...
TRANSCRIPT
A Symposium
atthe
Mid-SouthMedicalCenter Council
Annual Meeting
June 10, 1970
Holidaylnn-RivermOntMemphis,Term.
Participants
Joseph T. English, M.D.Harold Margulies, M.D.Eugene Fowinkle, M.D.
Harold R. SimsBland W. Cannon, M.D.
Moderator

The difficult task of charting new courses to better health care forcitizens of the Mid-South puts the Mid-South Medical Center Counciland the Memphis Regional MedicalProgramsidebyside in the samebattles. In many instances the two agencies work closely together toreach common goals. Publication of these proceedings of the MMCC’S1970 annual meeting is one example of that cooperation.
Making health-care professionals and laymen alike more aware of theissues facing the region and the nation, now and in the years to come,is an important job for both MMCC and the Memphis RMP. Leadersof both organizations felt that forthright comments by participants inthe symposium of the meeting would provide an excellent definitionof the issues and some stimulating insight into them for professionalsand laymen.
We feel that there are no more knowledgeable or more articulate com-mentators on the present and future crises in health care than themen who accepted invitations to appear on the symposium, HaroldMargulies, M. D., now director of the Regional Medical ProgramsService, Joseph T. English, M. D., then chief of Health Services andMental Health Administration, Eugene Fowinkle, M. D., state healthcommissioner for Tennessee, and Harold R. Sims, deputy executivedirector of the National Urban League. The symposium was ablymoderated by Bland W. Cannon, M. D., Memphis neurosurgeon and amember of the National Advisory Council of the Regional MedicalPrograms Service.
Dr. James W. Culbertson, program co-ordinator of the Memphis RMP,and Mr. Frank M. Norfleet, president of the MMCC, foresaw thebenefit of publishing the proceedings and gave their earnest approvalto the effort.
Staff members of the Memphis Regional Medical Program and theMid-South Medical Center Council cooperated in tape recording theproceedings and in preparing the transcript necessary to theproduction of this finished documentation of that meeting.
This publication has been edited only when necessary to achievebrevity and conciseness and to eliminate passages which were garbledelectronically or when some stray sound made a speaker’s wordsincomprehensible. Occasionally, when garbling or noise interferenceleft the speaker’s meaning unclear, passages were deleted ratherthan run the risk of altering or obscuring his intent. However, in a fewinstances, a speaker’s exact words and phraseology were leftundisturbed, even if the precise meaning were unclear, when theyhelped maintain continuity of comments.
We feel that the end result is a fair and accurate account of themeeting and an important document for the edification of personsinterested in health care in the Mid-South and the nation.
—The Editors
Clayton BraddockInformation OfficerMemphis Regional Medical Program ,.~
u
,, :... .... ,...,..;.1.A. Metz, Jr. ,<Director for Voluntary Health AgenciesMid-South Medical Center Council
.,...../-,-~ ,..,. .+~~.J,,...,
“./ ,.....:., M
.“14..,“,.
+ 7,
1
I reallytreasure this opportunity toshare some reflectionswith you aboutthree areas of problems that I am goingto try to statevery briefly that I thinkyou need to understand. The resolutionof these problems isgoing to determine,more than anything else,the future ofmedicine and health in this country inthe 1980s. The three problems are:(1) money (2) manpower and (3) someorganizational things, that we who areinterestedin health are going to have todo in this decade if we are going to haveany future in the nextdecade.
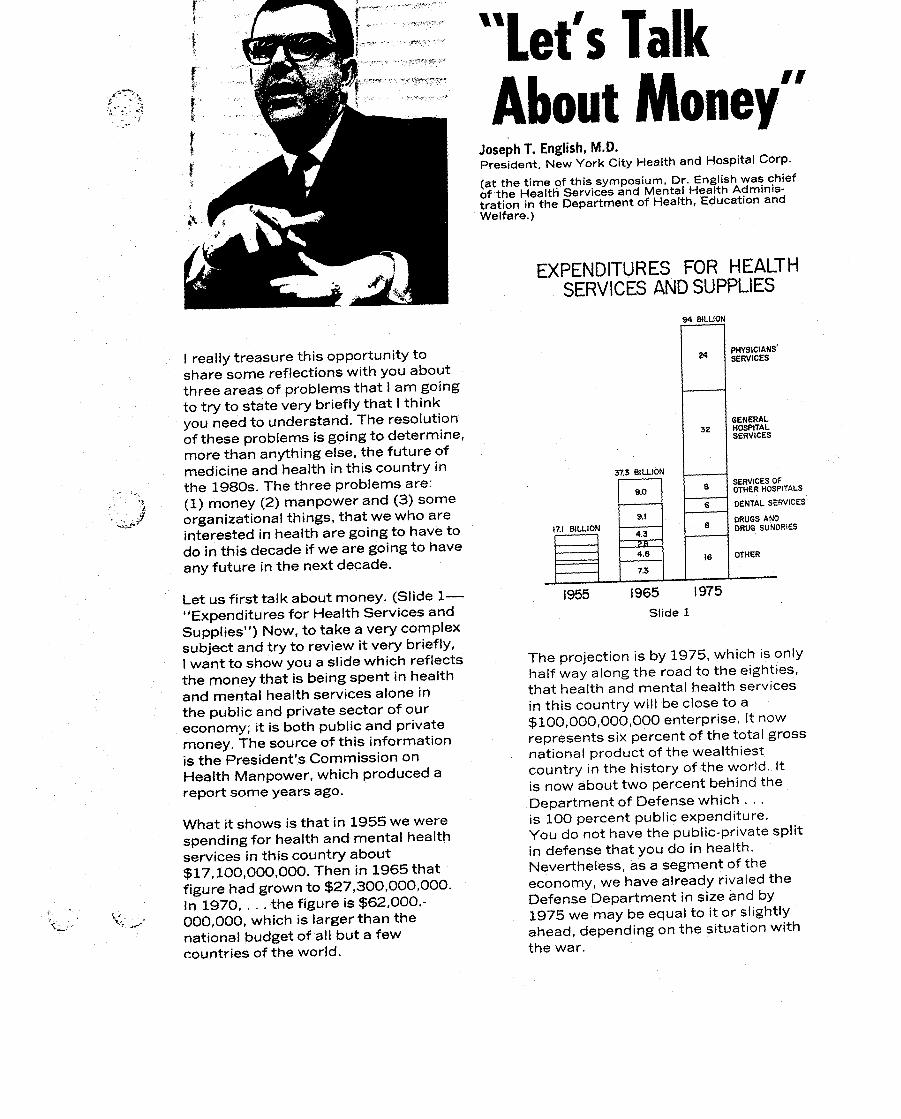
Let us first talk about money. (Slide l—“Expenditures for Health Services andSupplies”) Now, to take a very complexsubject and try to review it very briefly,Iwant to show you a slide which reflectsthe money that is being spent in healthand mental health servicesalone inthe public and private sector of oureconomy; it is both public and privatemoney. The source of this informationis the President’s Commission onHealth Manpower, which produced areport some years ago.
What it shows isthat in 1955 we werespending for health and mental healthservices in this country about$17,1OO,OOO,OOO.Then in 1965 thatfigure had grown to $27,300,000,000.In 1970, . . . the figure is $62,000, -000,000, which is larger than thenational budget of all but a fewcountries of the world.
“let’s TalkAbout Money”
JosephT. English,M,D.President, New York City Health and Hospital COrP.
(at the timeof this symposium, Dr. English was chiefof the Health Services and Mental Health Admtn!s-tration in the Department of Health, Education andWelfare. )
EXPENDITURESFOR HEALTHSERVICESANDSUPPLIES
nGENERAL32 HOSPITAL
SERVICES
3z3SILLION8 s3RVICESOF
9.0 OTHER HOSPITALS
6 DENTAL SERVICES
9.1s
DRUGS AND17.1 BILLION
4.3DRUG SUNORIES
2s4.8 16 OTHER
7.3
1955 1965 I975Slide 1
The projection is by 1975, which isonlyhalf way along the road to the eighties,that health and mental health servicesin this country will be closeto a$100,000,000) 000 enterprise. It nowrepresents six percent of the total grossnational product of the wealthiestcountry in the history of the world. Itis now about two percent behind theDepartment of Defense which . . .is 100 percent public expenditure,You do not have the public-privatesplitin defense that you do in health.Nevertheless, as a segment of theeconomy, we have already rivaiedtheDefense Department in size and by1975 we may be equal to it or slightlyahead, depending on the situationwiththe war.

Therefore, one way to lookat the moneyproblem—as we are in a period of timewhen we want to do many things andmoney is tight— isto seethat in thissegment of the economy, not doingthings for a lackof money is a cop-out,becausewe are guaranteed growth.Growth in some ways, as we approachthe 1980s, is one of the great threatsto us in health, for a very simple reason—because our country has been sogenerous in investing in health.Thismay not really be enough interms ofthe importance of healthto the nationallife of a country to even maintainingdomestictranquility in a country.
It has been said by many observers ofcountries in development that if youdo not meet something as fundamentalto life itselfas health, that it may beimpossibleto maintain order in acountry. And therefore, we are notfirst in the percentage of our grossnational product in investment inhealth. There are other nationsthatpercentagewiseinvest far more thanwe do and therefore I do not think thatwe should fear the growth we are goingto experience;rather, we should fearthe use that is made of that growthbecausethat is the problem.
Q‘“$s.:,.!..’. ,..#.
“->
The thing that is frightening about thisprojection is the situationthat we facein 1970. If there are not major changesin the way in which this growth ishandled, we could find ourselves in1975 worse off in terms of health andmental health servicesto the Americanpeople—the quality of health andmedicalcare provided to the Americanpeople in 1975, despite nearly doublingof the investment that the total public-private sector puts in—than we are in1970. I do not think that any of uswould lookforward to the decadeofthe ninetieswhere, despite the tre- ,~:mendous growth of the sixtiesand
u...-.;.,:.,!
seventies, in spite of that growth, .:,.?-.
people ended up lesswellserved thanthey were in mid-1970,
4
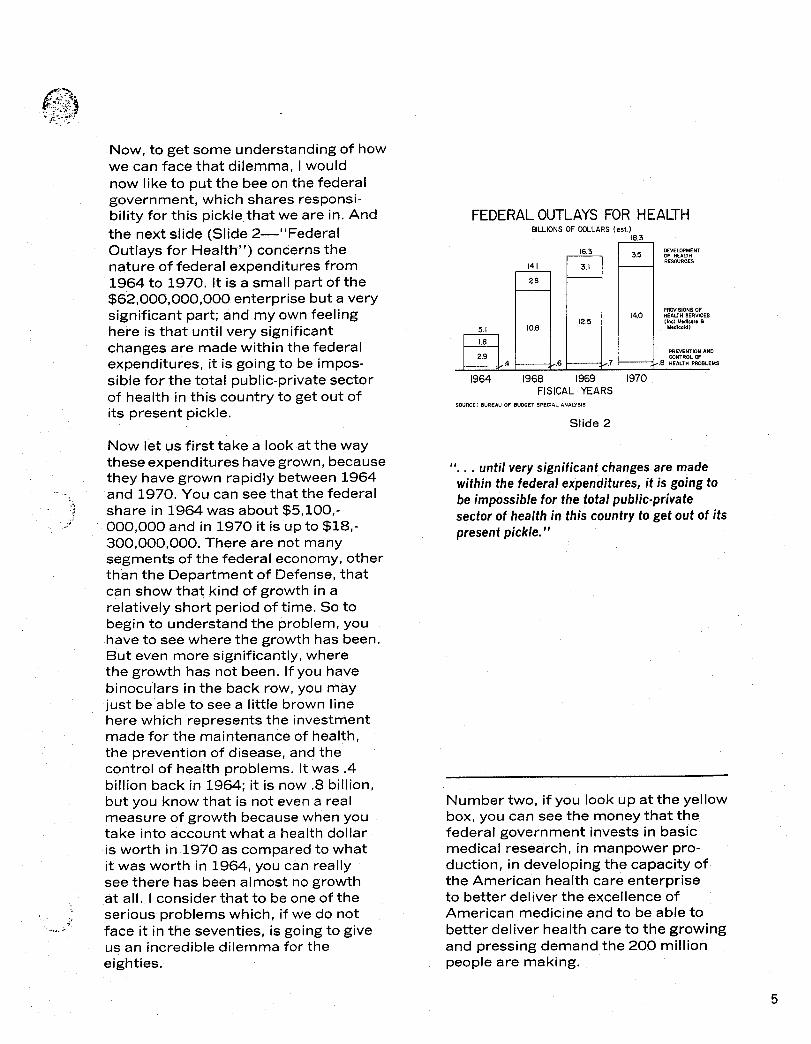
Now, to get some understanding of howwe can face that dilemma, I wouldnow liketo put the bee on the federalgovernment, which shares responsi-bilityfor this pickle.thatwe are in. And FEDERALOUTLAYSFOR HEALTHthe nextslide (Slide 2—’’Federal BILLIONSOF MLLARS (est. )
Outlays for Health”) concernsthenature of federal expendituresfrom1964 to 1970. It is a small part of the$62,000,000,000 enterprise but a verysignificant part; and my own feelinghere is that until very significantchanges are made within the federalexpenditures, it is going to be impos-sible for the total public-privatesectorof health in this country to get out ofits present pickle.
Now let us first take a lookat the waytheseexpenditureshavegrown, becausethey have grown rapidly between1964and 1970, You can seethat the federalshare in 1964 was about $5,100,-000,000 and in 1970 it is up to $18,-300,000,000. There are not manysegments of the federal economy, otherthan the Department of Defense, thatcan show that kind of growth in arelativelyshort period of time. So tobegin to understand the problem, youhave to see where the growth has been.But even more significantly,wherethe growth has not been. If you havebinoculars in the back row, you mayjust be able to seea littlebrown linehere which representsthe investmentmade for the maintenance of health,the prevention of disease,and thecontrol of health problems. Itwas .4billion back in 1964; it is now .8 billion,but you know that is not even a realmeasure of growth becausewhen youtake into accountwhat a healthdollaris worth in 1970 as compared to whatit was worth in 1964, you can reallysee there has been almost no growthat all. I consider that to be one of theserious problems which, if we do notface it in the seventies, isgoing to giveus an incredibledilemma for theeighties.
14.1
F
2.8
d5.1 10.8
1.8
2,99
1964 1968
16.3
[
3.1
12,5
6
18.3
[
3.5
14,0
.7
1969 1970-,-,FISICALYEARSSOURCE: BUREAU OF BUDGET SPECIAL ANALYSIS
Slide 2
EVE~PMEWOF HEAUHREWRCES
P~SlONS OFHEALTHSERVIC=(1”,1 Mdlcar, @
M,d!c,id)
PRE=NTION ANDCONTROLW
.8 HEALTH PWLEMS
II,.. untilverysignificantchangesaremadewithinthefederalexpenditures,itisgoingtobeimpossibleforthetotalpublic-privatesectorofhealthinthiscountrytogetoutofitspresentpickle.”
Number two, if you look up at the yellowbox, you can see the money that thefederal government invests in basicmedical research, in manpower pro-duction, in developing the capacityofthe American health care enterpriseto better deliver the excellenceofAmerican medicine and to be able tobetterdeliver health care to the growingand pressing demand the 200 millionpeople are making.
5
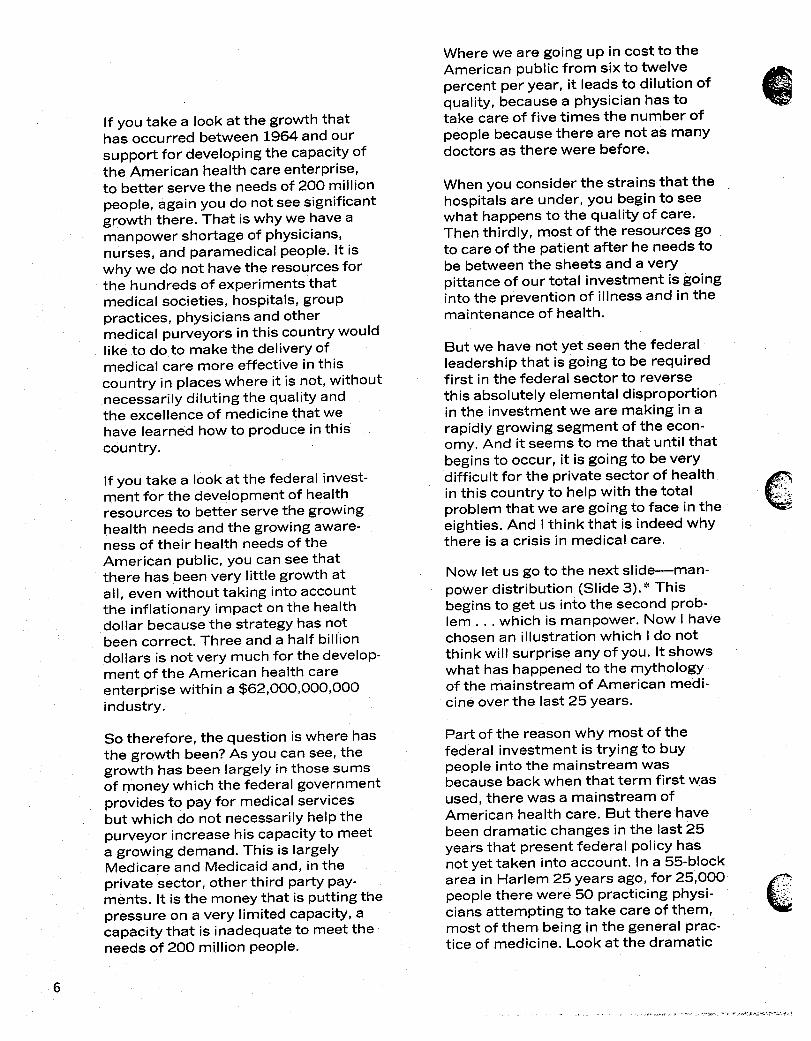
If you take a look at the growth thathas occurred between 19W and oursupport for developingthe capacityofthe American health careenterprise,to better serve the needsof 200 millionpeople, again you do notseesignificantgrowth there. That iswhy we haveamanpower shortage of physicians,nurses, and paramedical people. it iswhy we do not have the resourcesforthe hundreds of experimentsthatmedicalsocieties,hospitals,grouppractices,physiciansand othermedical purveyors in this country wouldliketo do to make the deliveryofmedical care more effectivein thiscountry in placeswhere it is not, withoutnecessarilydiluting the quality andthe excellenceof medicinethat wehave learned how to produce inthiscountry.
If you take a look at the federal invest-ment for the development of healthresourcesto betterserve the growinghealth needs and the growing aware-ness of their health needsof theAmerican public, you can see thatthere has been very littlegrowth atall, even without taking into accountthe inflationary impact on the healthdollar becausethe strategy has notbeen correct. Three and a half bill’iondollars is not very much for the develop-ment of the American health careenterprise within a $62,000,000,000industry.
So therefore, the question iswhere hasthe growth been?As you can see,thegrowth has been largely in those sumsof money which the federal governmentprovides to pay for medicalservicesbut which do not necessarilyhelpthepurveyor increasehis capacityto meeta growing demand. This is largelyMedicare and Medicaid and; in theprivate sector, other third party pay-ments. It isthe money that is puttingthepressure on a very limitedcapacity,acapacitythat is inadequateto meettheneeds of 200 million people.
Where we are going up in costto theAmerican public from sixto twelvepercent per year, it leadsto dilution of
@
.....quality, becausea physician has totake care of five times the number ofpeople becausethere are not as manydoctors as there were before.
When you consider the strains that thehospitalsare under, you begin to seewhat happens to the quality of care.Then thirdly, most of the resources goto careof the patient after he needs tobe betweenthe sheets and a verypittanceof our total investment is goingintothe prevention of illnessand in themaintenanceof health.
But we have not yet seen the federalleadershipthat is going to be requiredfirst in the federal sector to reversethis absolutelyelemental dispropotiionin the investment we are making in arapidly growing segment of the econ-omy. And it seems to me that until thatbeginsto occur, it isgoing to be verydifficult for the private sector of healthin this country to help with the totalproblem that we are going to face in theeighties.And Ithink that is indeed whythere is a crisis in medical care.
Now let us go to the nextslide—man-power distribution (Slide 3). * Thisbeginsto get us into the second prob-lem . . . which is manpower. Now 1havechosen an illustrationwhich I do notthink willsurprise any of you. Itshowswhat has happened to the mythologyof the mainstream of American medi-cine over the last25 years.
Part of the reason why most of thefederal investment is trying to buypeople into the mainstream wasbecauseback when that term first wasused, there was a mainstream ofAmerican health care. But there havebeen dramatic changes in the last25years that present federal policy hasnot yet taken into account. In a 55-blockarea in Harlem 25 years ago, for 25,000peoplethere were 50 practicing physi-ciansattempting to take care of them,most of them being in the general prac-tice of medicine. Look at the dramatic
c.,’!;::...,;.:,:;..,,,.
6
-.,.-,..,.:.--...,.-.....!

changethat has occurred today wheretwicethe number of people are livingin that area, and there are now onlyfive physiciansthere. [f you look at whothose five physicians are, you are goingto find that they are, in general, oldermen and there are no younger mencoming in to take their place.
You could give countless illustrationsof this in most of the citiesof our coun-try, You could show it in poor ruralareas too, but the nextslide indicatesthat it is not just a problem of the poor;it is a problem of some relativelywell-to-do areas in rural parts of our coun-try as well. [t is a problem that goesbeyond socio-economicparameters.(Slide +“Physician-Popul ationRatio, 1943’’ )$’
This concentrates again on physician-population ratio in the urban core ofour cities in 1943. Back at that time,
‘.. the ratio of doctors to patients,potential.:.;:.. patients,was 1 to 500 and out in the
suburbs in 1943 it was 1 to 2,000. Takea look at what happened as early as1968; the change was dramatic. Youhave a situation now where in the urbancore of our major cities that ratio hasgone from 1 to 500 to 1 to 10,000 andyou now have a situation in the suburbswhere it has gone, in that same period,from 1 to 2,000 to 1 to 500.
Just as the money problem is notsimple, which Ithink the former illus-trations tried to show, it isvery clearthat the manpower problem is notsimple either. it is not just a questionof producing more doctors, morenurses, more medical personnel ofother kinds; it is a question of how, in afree and democratic society,we getthose medical personnel and thosemedical facilitiesto the placeswherethey are needed. And I again want toemphasize that this problem is not justin poor areas of our country, but in a,- :,.-->, great number of relativelywell-to-dorural areas where you havethe samekinds of changes going on.
Let us move on to the nextslide now(Slide &“ Physician-PopulatiOfl Ratio,1943”) and just take a couple of min-utes to try to projecta littlebit into thefuture what may have to happen bythe 1980s if we are not going to see. . . federal medicine—governmentmedicine,whateverthat is. Because ifthere are not basicchanges, if we keepinvestingmore and more money inhealth, as we are at the present time,without the consumer, without thecitizenseeing his medicalcare or healthcare improved as a result of that, theconsumer outrage isgoing to producea situation in the Congress that is goingto convert us very rapidly to a publicutilityor to a federal form of directmedicalcare as has been done for theIndians and for other populations. Ithink that would be tragic in thiscountry.
-@ HosPITAL]PHYSICIAN~jjGRo”PPRAcT,=*MENTAL HEALTHcENTER 6 NHGHBORHOODHEALTHCENTER
Slide 6
Now what are some of the things thatare going to have to occur if we are toavoid unfortunate outcomes of thiscrisis?(Slide 6—’ Community Puzzleof Hospitals, Group Practice,etc.”)
The first thing Ithink you see evidenceof is a variety of groups, representingthe purveyor and the consumer and theteachers of medicine and the people
‘:Slides 3, 4 and 5 not reproduced for proceedings.
7

interested in medical research, comingtogether and recognizingthat in onearea of a community there may be nodoctors at all.
This would be the case right here (re-ferring to slide) and that might be the
@HOSmAL jmYSICIAN)~~@O”PpRAcT,c~~mALWLTHCmTERfi NEIGH~RH~D HE~THcENTER
Slide 7
reason why, through some federal effortor some private effoti, something likea neighborhood health center is startedto try to re-attract physiciansback intothat area and to put them together withparamedical people that extend thehands of the relativelyfew physicians.In other parts of the country we mayhave a group practice in a hospital.Way over here (referring to slide)there may be a mental health center ina hospitaland just a few solo practi-tioners. Over here there may besomething else. But it isvery rare, inmost parts of the country, that thereis any public-private institutiondevel-oped to survey that wholescene andto try to figure out howto make the bestuse of the resources that are there, thenew resourcesthat needto come in, bethey public or private.
We have not yet seen that institutionaldevelopment in this country and it isreally through Comprehensive HealthPlanning and the Regional MedicalPrograms that we are beginning tosee the start. So I would suggest thatby the eighties, if these programs aregiven the priority whichthey shouldhave, in . . . what is already a $62,000, -000,000 enterprise, this will help turn
those dollars into better health care forthe American people. If that does nothappen, then I think we are going to bein difficulty.
Iwould hope that wewould begin to seea varietyof different ways of comingtogether at the locallevel,as we seebeing done here (on slide diagram) tosee how those piecescan fit togethermore effectively,whether they arethrough an areawide health planningagency, a Regional Medical Programor cooperationbetweenthose twoprograms and other efforts. This issomething which does not yet exist inthis country in health: a communitytrusteeship—a coming together of the
Slide 8
publicand private sector at the mostlocalof levelswhere the citizen mandateis there with the community, where allsegments of the community are rep-resented—the taxpayer, who suppliesthe money increasinglyfor theseservices,and also all of the purveyors,too.
My convictionis that, though the re-sponsibilityof those in Washington isgreat, the real difference is going tobe made by the initiativesyou exertright here at the locallevelto do someof the most elementalthings that needto be done if we are to be optimisticabout what we can do in health, perhapsone of the most important dimensionsof the quality of life in our societyinthe 1980s.
e:.,.,,..,,8
.. ... . . ... ,...: ..... ..:...!.

1thought as a sub-name I wouldchoosethe “Cost of ServiceVersusthe Value of Care. ” I remember itwassaid that, “That which is immediatetakes precedenceover that which isimportant and that which is importantonly getsattended to when it is urgent,and then it may be too late.”
You know, I am very happy to be here.I feel, sitting here on this stage today,that systems have changed, becausewhen I finished Booker T. WashingtonHigh School (in Memphis) in 1952, Idon’t think there was any less likeli-hood that a student of the University ofTennesseewould be sitting here oranywhere near anybody like me butthere was no likelihoodthat I wouldget in the University of TennesseeMedicalSchool or anywhereelse. I amhappy to make that note.
“Costof Servicevs theValue of Care”
HaroldR.SimsActing Executive Director, National Urban League
(Mr. Sims was deputy executive director atthe time of the symposium)
When I attended high school in Mem-phis during those years I mentioned,I became quite fond of an old Chineseproverb whichfollowed me through theyears; I am sure you are familiar withit: “If you would plant for one year,”said the old quotation, “plant grapes.If you wou-ldplant for ten years, planttrees. But if you would plant for etern-ity, plant men,”
Given the current status of man, womanand child in the American world today,our commitment to planting menrather than things istragically in doubt.In the face of unprecedented scientifictechnology and technologicalprogress,wefail to commit and demonstrate ourcapacityand resourcesto the magni-tude of the problem which we havehere at home. Our citiesand ruralareas are in an ever-deepening crisis,with both qualitativeand quantitativedefects robbing our children and ouryouth of the occasionalopportunityneeded to facilitatetheir maximumgrowth and development.
9
A housing crisiscontinuesto worsenwith blight decayingthe slums, breed-ing crime and delinquency in everymajor urban city. Our living environ-ment is in a crisis,through pollution,poisonous air, dirty water, the rodentsrampant and clutter-it is becomingan increasing . . . problem.
Of all the crises we face today, none ismore critical or urgent than the growingdeterioration of health care and serv-ices.For without a healthy body andmind, none of the other crises or op-portunities really matter in the march-ing hierarchy of human needs. Now,this health-carecrisis in our age ex-presses itself in many insensitiveandironicways.
Although the statisticsare used froma variety of sources during the decadeof the sixties,nothing has changed verymuch to alter the picture. For example,despite spending $62,000,000,000, or6.7 percentof the United States grossnational product on healthcare in 1969,our lifeexpectancyisstillonly 18th formales and 1lth for females in the wholeworldwide rankings. Despitethe factthat we have the highest levelof medi-cal competenceand are expendinggreater resourcesfor health-careserv-icesthan any other nation in the world,our ranking again inthe world orderhas consistentlydeclined in the lasttwenty years, particularlyin the areaof infant mortality,wherewe wentfromsecond in 1953-55 to eleventh placein 1960 to fourteenth in 1967-1969. Asof today, we rank belowEast Germanyin this regard. And as for our blackcitizens,above all, they rank belowJamaica, Japan, Italy,and Greece—in 28th placeon the world order scale.
This factor ought to be particularlyimportant to you here in the South. In1968, the East-South Central regionwhich included Kentucky,Tennessee,and Mississippiand, I believe,Alabama,had the highest infant mortality ratein America for both races,white andblack. Despite the creationand devel-opment of a multi-billion-dollarhealth
insurance industry which collectivelytook in about 11 billiondollars worthof premiums in 1967, the costto themedical consumer increased5.8 per-cent from 1965 to 1968 alone. Forthere was only a 3.3 percent increasein other consumer priceswithoutcomparable income increases.
During the period of deteriorating serv-icesand world standing in health care,despitethe criticalshortage of doctorsand the necessityto “import” tosurvive, many of America’s medicalschools consistentlycomplained andthreatened to closefor lackof funds.The other day in California, peoplewere so insensitiveto this great needthat they voted down the creation oftwo new medicalschools,despitethecriticalneed.
6
,.”%,.....‘..... i!::.;.,J
Despite all the rhetoric of the medicalprofession of prevention and mainte-
10
nance, the health-care delivery systemof this country is stilldesigned toreact rather than preclude, to supportsocio-economiC classes rather thanall people on the basis of need. At thepresent rate of United States retrogres-sion in health-care areas and at thepresent order of United States prior-ities, unless drastic changes are im-mediately undertaken, by the 1980sthe United States may very well befirst in the race for the conquering andpopulation of barren . . . outer spacebut last in the race for viable Iifefulearth or human space.
The plight of health care today forblack America is two to four timesworse than white America, althoughproportionately more black malescontribute to Social Security thanwhite males. Given the present mor-tality rate, the average black man atbirth cannot expectto live long enoughtoday to collecthis Social Security.Most black families without healthinsurance, and many with it,are con-fined to the wards of over-crowdedmunicipal facilitieswhere daily hospitalcharges are somewhat lessthan thevoluntary hospitals. About six percentof black mothers— eight percent in theSouth—had no medical care beforethe birth of their child, compared to onlyone percent of white mothers—threepercent in the South—in a nationalmortality survey in 1963.
At the same levelof income and educa-tion, black mothers are more.likelythanwhite mothers to have been seen atpublic medical facilitiesrather than bya private physician. Both blackandwhite mothers receive littledental carebefore the birth of a child, althoughpregnancy is known to affect themother’s teeth critically.Regardless ofincome, black mothers very seldom seea dentist before childbirth, or they seethem much less often than whitemothers do; over 90 percentof theblack mothers— compared to 70percent of the white mothers, accordingto a 1963 survey again—did not see adentist at all during the twelvemonthsbefore birth of the child.
“Theplightofhealthcareforb/ackAmericaistwotofourtimesworsethanwhiteAmerica,althoughproportionatelymoreblackmalescontributetoSocialSecuritythanwhitemales.”
The black maternal death rate isalmostfour times the white, in spite of thedrastic reductions in the last threedecades (69.5 compared to 19.5).Life expectancyis lowerfor blacksthanfor whitesof all ages. In the prime oflife,the prime working years, 20-35,black men and women average fiveyears less life expectancythan whitemen and women. The difference beginsto taper off in lateryears and is greateramong women than among men,Blacks have a much higher death ratethan whites in communicable disease.Particularly blacksare more than likelyto die more often from tuberculosis,influenza, and pneumonia.
One positive note: suicide is moreprevalent among whitesthan blacksand is consistentlyloweramong blackwomen, And someone rationalizedthisin an article in The New York Timesthat talked about the psychicadvan-tagesof urban life.That may havesomething to do with it. I do not want tosimply re-emphasizethe horror but todramatize the opportunity availabletous. Iwant to differentiate somethingthat ought to be clearto you. Iwon’telaborate on this becauseof the time,but do not get too optimisticabout thestatusof white health in this country,becauseeven the optimum averagewhite health care isstill much lowerthan in some Communist countries.And we turn to the relative improve-ment the whites have made in the lastten years. Really what has happened isthat the blacksare moving closertothe inferior level.
11

Since we did not come hereto drama-tize the horror that dramatizes theopportunity, let’s talk about the plan-ning. An alternate range of strategicplanning in all areas may have manycontroversial meanings, but morepractitioners agree it isto plan for andput in placetoday, which willmaximizewhat we want to happen tomorrow. TheNational Urban League has recentlyrecognized the criticalnature of theseventies. No telling what may happenin the eighties.
We calledfor a consumer-orientednational health system—a frameworkwhich addresses itselfto designingmechanisms by which health, as aright and not as a privileg+and wemaintain health as a right-an beachieved as a reality for all Americans.
/
We calledfor an action-orientedhealthsvstemwith a program and a platform @ .- ,,./’.whichencompassesall employees ofhealth, health maintenance,diseaseprevention, medicalcare delivery, fi-nancingconsumer participation,train-ing, and education.
In this new system—for maximizationin the eighties,and for maximizationnow—we calledfor a complete neworganization of the health care systemof the United States, an organizationthat would reflectthe national healthpolicywhich is responsiblefor the fivebasicassumptions which I hope toelaborateon during the discussionperiod.
We also calledfor a commitment to asystem of public educationfor allcategoriesof the health profession—doctors, nurses, technicians,with aservice commitment which can beutilizedto provide a more even distri-
0
,.‘...... \bution of health careservices.
-...,“.W.”;.... .,
We alsocalledfor the re-orientationofthe health care systemto help add itsmaintenance rather than only attendingdiseaseand illness.[f you willcarefullyexamine most of your health policiesand all the things you carry, you willfind that they are not designed to helpyou prevent and maintain yourself;they are designed to reactand torespond.
We are callingfor a national healthinsurance plan, whichwe will alsoelaborateon during the discussionperiod. For the final analysis,we agreewiththe lateWalter Reuther, who said:“We call for, pleadfor, indeed demanda healthcare system nowthat willeliminatethe wasteand the inefficiencyof the present non-system,a systemmoreover that will bring the poor intothe mainstream of medicalcare, asystem that can, in an organized
a
.,...!,\.,’.:.1
manner, begin to bring about the effec- ‘+1:~tive use of our health manpower, ourhealthfacilities,and our economicresources.’

,,;.:
Ten years ago I heard Dr. Cannonsay, “What this community really needsis an effective planning organizationthat can develop good appropriate plansfor the future development of thismedicaland health community.” Wesaw the birth of this idea. We saw itnurtured through bitih and childhood byDr. Cannon, Mr. Norfleet, and many ofyou here in this room and now we havean effectiveand mature organizationand I think we are all justly proud of it.
Public health, as its name implies, isboth public and health. Consequently,public health is acted upon both bypublic forces and by forces which aregenerated from within the health in-dustry. One important and profoundpublicforce which is influencing us nowis that all institutions, agencies, sys-tems, traditions, or even individuals,are on trial now by society. We arebeing tested continuously for ourvalidity.The American health systemnow is certainly on trial and is beingtestedfor itsvalidity. Ithink in the1970s and on into the 1980s thesystem will be tested. The variouscomponents of the system will becontestedfor validity and some replace-ments and changes willdoubtless be
ConcernandProfessionalJudgmentEugeneFowinkle,M.D.Tennessee Commissioner of Health
made. This phenomenon was put verynicelyby a well-known physician:“These are days of deep dissatisfaction.Cries of dissension and loud demandsfor change fill the air, Nothing isfair—government, the press, industry, labor,religion,the educationalsystem, philan-thropy. Nothing! An uneasy concernblows acrossthe land and around theearth, already shaking all the leavesand already some worthwhilemightytrees have fallen. Necessarilycaught inthe relentlessmovement isthe field ofhealth, with all itsvarious manifesta-tions, its professional schools, itsestablisheddisciplines, itstraditionalprograms, itstime-honored approachesto planning, public relationsand serv-ice.” So what he issaying and whatI’m saying isthat we are on trial. We arebeing tested for our validity. I thinkwe will see many aspectsof our healthsystem strengthened by the existingtesting process becausea number ofthose components that are not validwill fall by the wayside.
Another public force which has had aprofound effect upon the health systemis, of course, the socialmandate that
13

was referred to by Mr. Sims, that everyAmerican citizen receiveessentialbasichealth services regardlessof his abilityto pay. This mandate has been readout in a number of ways. Some haveread this to mean that every citizenshould have gold-plated health care;others say every citizenshould havetoken health care. I think, in general,what we hear isthat every Americancitizenshould have at leastessentialbasic health services.This socialmandate has manifested itelf in avariety of ways. One isthat it has pro-duced, in the mid-1960s, two of themost profound health legislativeactsin American history. The health systemis staggering under the weight of thissocio-politicaldecision now and willcontinue to wrestlewith itthroughthe 1970s and hopefully willfind solu-tions as we go intothe 1980s.
Another public force or influencewhichis acting upon the health system of thiscountry and which is a corollaryto thissocial mandate is involvementof thefederal government. This was pointedout to you very clearly by Dr. English.The question used to be, “Will thefederal government involve itself in thehealth industry?” but the question nowis, “How will the federal governmentinvolve itself in the health industry?”
As I see it, there are two major alterna-tives. One is to socializethe system, toput health providers on federal payrollsand develop national health programsas some of the European and Asiaticcountries have. Ithink that few clear-thinking Americans at this time thinkthat this isthe best way to providehealth care for the citizensof thiscountry. Built in and ingrained into ourvery way of life is the quality building,quality maintaining, private enterprisemotivethat exists not only in our healthsystem but in our entire economicstructure. The other alternativetofederal involvement in the health in-dustry isfederalhealth system.
subsidy to the existing
@“Built in and ingrainedinfoour verywayof life ~,is the qualitybuildingand qualitymaintaining
/.,
privateenterprisemotivethat existsnot onlyin our healthstructurebut in our entireeconomicstructure.”
This, in fact, isthe present trend,Medicare and Medicaid being the twomost profound examples. As you know,they provide buying power to individualswho can then go to the private marketif they so choose, and purchase theirhealth care just as any other individual.So the present trend is federal subsidyto the existing health system, both
a
:,,’\private and public. 1think that we have .a.........to say, however, that there are some red ‘L:’flags waving.
Another powerful public force which isacting upon the health system, espe-ciallyon public health, isthe publicdemand to stop further deteriorationof our environment. During the en
/years I have been in public hea} ‘h, Ihave seen a variety of levelsof publicinterestand concern on matters relatedto health. However, I have never seenany reactionof the publicto any matterrelatedto health as strong and asintense,as enthusiasticas the presentexpressionsof concern about our en-vironment that are now being given tous. We have a very strong signal fromthe public that further deterioration ofour environment is to stop. Publicdemand is here; it has not always beenhere on the environmental problem.Ten years ago I heard the surgeongeneral of the Public Health Service fl.>warn that this country is headed toward
L
=::.,,,....
serious environmental health problems. ‘;”However, at the same time, he pre-dicted that very littlewould be done
years becauseof the lackof publicconcern.We have publicconcern now—but just how adequateto developadequate environmental quality con-trol. Although public concern andpublic demand, whether they relate tothe environment or to the predicamentof the present health system of thiscountry, are important and essential,they must be tempered by professionaljudgment.
One of the greatest problems which weare going to encounter in the 1970s isdealing withthe public clamor that nowexistsabout our health system andabout our environment. This is im-portant but yet perhaps it is beingoverdone.
Let me illustrate.A few weeksago ourApollo 13 spaceship got intotrouble
and the immediate response of 200million Americans was to say, “turnit around, bring it home. This was anexpression of public concern that wewanted our people back home safely,but it was tempered with professionaljudgment, in that the men at the con-trols in Houston realized that if theywere to try to turn the ship aroundimmediately and bring it back, itwouldbe destructiveto the people that itserved. So with the intent of gettingthem back, they used the momentum,the forward motion, that the ship had,but they guided iton the proper course.They made periodic and frequentadjustments to it,got it on the rightcourse, and steered it back home safely.Public concern wasthere, but itwastempered by professional judgment.
There are those who say, “Let’s com-pletelydo awaywith our existinghealthsystem and start over.” There arethose who say, “Let’s immediatelysolve our environmental health prob-lems,” I think this will have the sameeffect as trying to turn the spaceshiparound while it isgoing away from theearth. Itwould be destructive to thevery people that we are trying to serve.I think we must temper these expres-sions of public concern with profes-sional judgment.
So in summary, I do think we needpublic involvement,We need publiccriticism.We need public participationin policydecisions in the health in-dustry. But yet I hope we can have theingenuity, the knowledge and thestrength to temper this appropriatelywith professional judgment so that wedo produce the best possible productfor our consumer in the 1970s and intothe 1980s. Comprehensive HealthPlanning brings together, at interface,the public concern and the professionalknowledgeand experienceand judg-ment, So Ithink CHP is one of the besttools that we haveto achievethe taskthat liesahead of us in this decade.
15
You’ve heard a number of things thisafternoon which are pointingtowardwhat may be our health-caresystemor our health-care problems in the1980s. But because I haveto deal withthem in a very direct fashion, Ithink Iam going to haveto be a littlemoreexplicit.We have heard problems andI think Ican add to them, but I wouldliketo balance up the record veryquickly and point to some of the thingswhich Ithink are going to occurandmake it as clear as possibleto you thatthe answer to the question of whatmedicinewillbe in the 1980s is not atthis table. It is in this audience. And Idon’t think you quite begin to recognizethat fact.
Dr. Englishtold you some things thatthe federal government has been doing,which he thinks it should not have beendoing, and he pointed to a certain levelof inexpertisein the federal governmentfrom which I am sure he exempted meand himself. I feel confident about that.But I would liketo point out, just tobalancewhat we are talking abouttoday, what has gotten us intothe kindof situationwhich he describedandwith whichyou are familiar.
MakingChoicesHaroldMargulies,M.D.Director, Regional Medical Programs Service
(at the time of the symposium, Dr. Margulieswas acting director of RMPS.)
Because I have only briefly enteredfederal service, I think I can look at itwith that kind of a perspective.What W2has happened since Ifinished medicineat the University of Tennessee? in thoseyears there has been a rapid increasein the use of hospitals,a rapid increasein specialization,a rapid increase inphysicianconcentration and nurseconcentration in certain areas andabandonment of others, a rapid risein the costof medicaleducation with adisappearance of private sources andfunds to pay for it, and a rapidly in-creaseddependence upon allied healthmanpower, all of which you are familiarwith, none of which was created byfederal government or any other kindof government. These were the prod-uctsnot only of the medical professionsbut of the public.
At the present time—and 1think Mr.Sims’ presentation is fairly character-isticof it—we are still not able tonarrow our purposes down to what itiswe really want. We have a wholekaleidoscopicrange of interestssayingwe want this, and this, and this, andthis, meaning we want everything all
G,.’... ,,.. ,,,.,..
t,’. ,~,... .

......;
...,.’
at one time and not reallybeing ableto settledown on exactlywhat we willgive up in order to get what we reallywant. We hear the usual range of morephysicians, more allied health people,more hospitals, more acutecare, morechronic care, more preventivecare, andso forth. What is it that we are reallywillingto bargain for withthe six per-cent or eight or ten percentof thegross national product we are talkingabout? I think this isgoing to get settled,and I think it is going to be settledbefore the 1980s so what occursthenis really the issueof the 1970s. Andmore than that, it is the issueof thenextthree years.
I believewe must recognizethe factthat, despite the interestof the peopleat this table and the interestof thosewho are in the audience, concern withhealth care in this country isstillmarked primarily by apathy. This istrue of the medical profession and alllevelsof health skills. It istrue of thepublic in general. Look at any generalsurvey of the major issueswhich peoplespontaneously bring up and somewhere. . . they will talk about health issues.This will change. Itwillchange as thepoliticalclimateof this country isprogressivelychanging. Because, inthis decade, the issuesare going tomove away, as they already have, fromthose we are familiar with, to thosewith which we are becoming increas-ingly familiar.
They are going to have to do with suchthings as peace,as something we be-lieve in, and for which young people aregoing to prefer candidates.They aregoing to haveto do with educationavailableto everyone—all colors, aliareas, all creeds. They are going tohave to do with decent housing whichis currently not availableand which isdisappearing even more rapidly than itis appearing. And it isgoing to have todo with health. And in this decade, theissueof health isgoing to riseto a majorpoliticalissue,and I mean politicalwitha small “p” as wellas with a big “P.”And what happens as a consequence is
going to be a reflectionof how success-ful the present efforts are to do some-thing about the health care system.
We are lackingcertain kinds of basicingredients.One of the ingredientsweare lackingis an understanding of whatit is that we wish to have as our majorpriority, And our choices,becausethisis going to become political,and in-creasinglyfederal and increasinglygovernmental in the payment system,our choicesare going to be tougherand they are going to be a combinationof political,fiscal, and moral choices.What are they going to be?
We are going to have to decide onwhether we are going to preserve thelife of 85 year olds or preserve the lifeof eight year olds. We are going to haveto decide whether we are going to putall of our efforts intoacuteepisodiccare for peoplewho may or may not dieor put them intothe maintenance ofhealth. And we are not going to havethe opportunity to do both. Because inthe nextthree years the problems whichwe have been describing here today,which Dr. English laidout for you veryeffectively,are going to get worse. Ourhealth manpower shortages are goingto be exaggerated.The costsof medicalcare are going to go up. The deteriora-tion of hospitals isgoing to be accele-rated. Accessto medicalcare is goingto be unimproved. Medicaid is goingto be as paralyzed as it has been in thepast and have very limited benefitsfor very limited numbers of people.Andthe agony will increaseprogressivelyuntil we are ready to make the kindsof politicaljudgments about what wereallywant out of this health care sys-tem and what we want to purchase withour moneyi
And then some things are going tooccur. If I had more time, I could sketchfor you, Ithink without much difficulty,a logicalconclusionabout where weare going to be very quickly. If I didthat and ran through the range of thingsthat have happened these lastten ortwenty years, Iwould come to this
1/
“Thereis still a reluctancein makethechoices,the hardchoices betweenwhatis obviousand visibleand excitingand whatis muchlessattractivelike preventivemedicine,healthmaintenance,and the wholeconceptofplan-ningfor the total community.”
conclusion:That the high cost ofmedicalcare, which can be increasinglyidentifiedas beingfrom federal sources,isgoing to lead to an increasingdemandthat we have a measurement of whatwe are purchasing. And one of therising issuesbefore 1975 is going tohave to do with the quality of medicalcare which is being purchased byfederal and private money. And this isgoing to produce some profoundchanges in attitudes.
Public hospitalswhich currently pro-vide miserable medicalcare for peoplebecausethey are indigentsare going tohave to face the fact that this care isunacceptable.Payment systems aregoing to identify the difference betweengood and bad care at levelsof sophis-ticationwhich none of us feels readyto take on. Now the government iswellaware of this; you are well aware of it.The federal system is lunging in a num-ber of directionstrying to decide how weare going to copewith this very clifficultproblem. Of the total increaseof over
one billion dollars for this nextfiscalyear in health, 83 percent is going forMedicare and Medicaid, merely mean-ing paying more money without any ,.,
increasein the accessor quality ofx,-.,”
medicalcare. This isan uncontrollablecostwhich at the present time isstrangling all other efforts.
Now you know that one of the thingswhich has been going on in this countryis an attempt at some kind of decen-tralization.The federal government hassaid to itself, “We reallycan’t handlethis, It istoo big for us. The problemis out there; the solution should be outthere.”
On the way down hereon the plane Iread an articleby Dwight Ink,who isone of the leading budget managerialtheorists in the country and in thefederal government. He described avariety of basicways in which thepoliticalprocess is going to movetoward the solution of problems whichhave becometoo central and must bedecentralized. It intrigued me that he
o
‘,.......did not identify the very specialquality -,y..,”.’.,of the Regional Medical Programs in
“f,
this country. Because of the wholefederal system, they have remainedunique. There is no arrangement avail-able to any branch of the federal gov-ernment which allowsfor a federal-private mixto identify problems, toattack problems, and resolvethoseproblems. This is the one option in thehealth system which remains open asan effective mechanism for dealinglocallywith local issues.
Now since I have come intothe RegionalMedical Programs, and I knew itwellbefore that time, 1have been even moreimpressed with the very specialchar-acter of that activity,not only for thehealth field, but as a measure of whatkind of mix we can maintain betweenfederal and private efforts and skillsand talents to produce a desirable re-sult. 1haveto say that what 1have seenso far in . . . those programs is not
a
..~........... ,.;very exciting.I have seen a range of .,;..:.:.
/activitieswhich continueto reflectcon-cepts and prioritieswhich are already

can reflectfederal thrust, can be re-sponsive to consumer interests,unlessthese two can do it, then clearlytheywill have to be abandoned in favor ofsomething which is much less likelytobe successful.
Now what disturbs me about it morethan anything else isthat it is new, it isfragile. It represents, in itsessence,thebest of the American genius, which isthe capacityfor people of differentkinds to work together toward a com-mon purpose withintheir own com-munity, But there isstill reluctanceinmaking the choices,the hard choicesbetween what is obvious, and visible,and excitingand what is much lessat-tractive like preventive medicine,healthmaintenance, and the whole conceptofplanning for the total community. Be-cause these choicesare ones whichpeople are reluctantto make, I have myown skepticisms,
Now Ican pledge to you that so long asI have the responsibilityfor RegionalMedical Programs and have the accessI have to thinking about Comprehen-sive Health Planning, researchanddevelopment in the medicalarea, solong as I have that responsibility, Iwilldo my best to bring these functionstogether because I am confident that ifwhat we are trying to do now is notsuccessful, itwill be replaced by some-thing else and in the courseof time willhave to start all over again to createwhat is now Regional Medical Program
out of date at the time they are initiated. and Comprehensive Health Planning.I have seen very littlereal integrationofthe conceptof planning totally for the I also recognizethe fact that they aretotal population on one hand and total young and have had very littletime toresponse and total conflictfrom the find out whether or not they can work.professional side on the other hand. In the same moment I must tell you
that there is no time leftto be delib-Regional Medical Programs by itself is crate, to be doubtful, to be hesitant. Ifa totally ineffectiveinstrument. Com- you mean to make this area, the Mid-prehensive Health Planning by itself is South, an area which the whole nationa totally ineffectiveinstrument. They is looking at, one in which people wishare so interdependent upon one another to live because health care is availablethat the failure to recognizethat inter- to them at a good quality level,you willdependence constantlyastonishesme. have to work vigorously and effectivelyAnd unlessthere isa way in whichthese and with a kind of humility which is es-two can serve total community needs, sential to good community activity.
19

QUESTIONS AND ANSWERSDR. ENGLISH: Let me read two of thequestionsthat I have just received:“Who reallymakes the healthdecisionsat HEW? ~ncurrently, why is healthreceivingthe short end of the stickatHEW? Dr. English, you impliedthat theWhite House should havean advisor inhealth.Could Robert Finch fill that role?If so, willhe be askedto do so?”
I think they are very good and pertinentquestionsand, not necessarilystickingwiththe tradition of federal bureaucrats,I will try to be direct, honestand mostresponsiveas well as brief in myresponse.
Who reallymakes the healthdecisionsin HEW? The big decisionsare not madein HEW. The big decisionshave beenmade in the White House. Part of thereasonthat poses a problem isthat thenation’s top health officer is excludedfrom the decision-makingprocess inthe White House. He has publicly la-mented that fact on numerous occa-sions. Who makes the decision in theWhite House is very difficultto deter-mine, exceptto say that inthis situationit is almostwithout precedent. No onewithin the White House is presentlyassignedthat we knowabout to the
$62,000,000,000 enterprise whichhealth and mental health servicesnowis in this country. Regardless of wherethe decisions are made, I do not think
a
- ,,,,.F- ‘g..,we are going to see progress in the .;::::C.
crisis in health care in this country until, ‘1
withinthe placewhere the decisionsaremade, someone is assigned the re-sponsibility for knowing somethingabout this criticalarea of the Americaneconomy.
And now the second part of the ques-tion: “Will Mr, Finch’s going to theWhite House as counselor to the Presi-dent help with this?”
I must say that all of us are terriblyoptimisticthat he may be able to help.Others would point out that if he haddifficulties as Secretary, will it reallybe different as he joins the White Housestaff itself?I would say that most of usretain great optimism, becausetheSecretary understands these problems.We hope that he will be helpful. I doubtthat he would becomethe President’shealth advisor. I think he realizesthegreater need for expertise.Hopefully, he .::,lek
may be able to get the nation’s topb:.;.,.:...,,,e.~ (
health officer intothe White Housedecision-making processwhere up

until this time he has been excluded,the reason being given that he is aphysician and a physician in thosecouncils could not be objective: hewould be an advocate.
DR. CANNON: Dr. English, Ithink Ishould ask you one questionfor clarifi-cation. Some people might associatethe White House as meaning PresidentNixon. I think you ought to give someclarificationto that, becausereallyitmay be a different ballgamethan isperceived by your comments. I do notwant to put you on the spot.
DR. ENGLISH: No, Iam delightedto beon the spot. These are times when apublic official should be on the spotand I am delighted to be in that posi-tion, I do not think that this reflectstheterrible problem of any presidentdur-ing times when the nationalcrisesaretoo numerous to mention, when hisattention is focused on many things.With his dependency on the peoplethatboth control accessto him and advisehim, I think that the Presidentwould befar betterserved if there weresomeone,recognized by the departments of gov-ernment, by the professions in thiscountry, by the consumers who areinterested in health in his own house, inthe decision-making process,to insurethat the President getsthe adviceof thenation’s top health officer.
MR. SIMS: 1have several relatedques-tions here: “What are the four majoritems that you observed during yourtalk to be the top items to be consideredin health care for the future? How doyou think that compulsory nationalhealth insurance should be financed?”
First of all, let me explainsomething.Perhaps I am the consumer up here,in terms of my actual involvement.Ifyou give a littlecredibilityto what I amsaying, I am from a very successfulfamily of purveyors. i am from a familyof doctors and teachers. I have livedaround them all my life. Secondly, theinput through the National UrbanLeague is rather unique, in that it bringstogether, if you will, the “establish-
ment’ of the people. The recommenda-tions come from peoplewho areeminently involved in the medicalfield.And we developed our positionon ourthorough examination of the AMAdraft billon health care and health-care insurance,the AFL-CIO proposal,the Griffin Bill, the Jackson proposal,the Committee for National HealthInsurance,the Rockefeller proposal,and a variety of taxpayers’ proposals.I also want to emphasize that we arenot talking here about socialism. Ithinkthat the Urban League is committed tothe democratic processand we havecommitted to the processa surge ofpeople, as well as machines and things.So all that concernsyou isdeliveringthis kind of thing.
Perhaps if I can read in full as quicklyas I can the position of the UrbanLeague on health care and health in-surance, I may answer a lotof thesequestions. We calledfor this reorgani-zation of the health care system, whichdid not mean so much throwing out asbetter utilizing.Our aim is not so muchto provide for new kinds of costs, al-though we believe it is inadequate costeffectivenessto the American people,to the consumer, to bring about agreater value for the current medicaldollar. And the five assumptions wetalked about, in referenceto whathealth care, or health care policy,orthe health care system ought to contain,are:
1) That we believea national healthsystem should be conceivedand func-tion to meetthe needs of the consumerand provide opportunity for appropri-ate consumer participationand controlof the system that will serve him. Moreconsumer-oriented than provider-oriented system. The current system ismainly oriented toward the provider.The consumer should have somethingto say about his health and the healthcare of his children.
2) The national health system shouldbe oriented toward health and its main-tenance rather than simply disease.This involvesprevention and distribu-
21

tion, not simply reaction. For example,how many health care policiespay foryour annual physical,which may becriticalto your survival?We say the fee-for-service concept is not acceptableina health care system in which the basicconcern is for the health care needsofthe consumer. The elimination of afee-for-service principlewill be uselesswithoutthe development of interrelatedpositionsof health professionals, theredefinition of rolesand tasks, and areorientationfrom diseaseto healthcare.
3) And we assume, and we say, thatthe health care system must be de-signed to provide an even distributionof comprehensive health care servicesin all communities, irrespectiveof theirracial and their economic base. A sys-tem of tax-suppofied public educationwith a servicecommitment for all healthprofessionals is essentialto achieveanequitable solutionfor manpower needs.It is inconceivablethat America wouldvalue its soldiers more than itvaluesthe people who make those soldierspossible.
4) The general tax revenue shouldbe the source of financing for universalhealth insurance. Economists say,“While the socialsecurity mechanism. . . can be perhaps modified, a progres-sivetaxation method is preferable.” Wedo not see this costingyou about thesame money for better servicesfor allpeople, irrespectiveof your age or eco-nomic status. A major concern of oursor any national health insurance pro-gram isto placea significant emphasison the improvement of the geographicaldistribution of health services.We saythat national health insurance must becommitted to the development of asingle health system without socialorracial discrimination. We oppose reim-bursement formulas and the utilizationof private insurance carriers.
5) We support a system of publicfinancing, including stipends, for edu-cation in the health professions. Suchpublic financing would make inherenta community serviceobligation and is
based on the premise that all membersof societymust have equal accesstoeducation in the health professions for
@
..,
whichthere will be in turn an obligation 2&-to that society.We feel that some formof funding for health profession educa-tion must bean essentialcriteria of anynational health insurance program.
DR. FOWINKLE: “What part should areal group practiceplay in the 1980s?”
Until the mid-1960s, the major prob-lem of entering intothe existing healthsystem was the financing. As Dr.English indicated,the big input into thefinancing of health care has been in thearea of providing serviceor financing.We havesomewhat overcome the fi-nancing problem and have overdone itso that nowwe have put on the healthsystem such a tremendous demandthat it isoverwhelmed and is producingpredictableresults.
If you overwhelm any economic sub-system with an excessdemand whichhas taken the form of some $12-14,000,000,000 of new buying powerwithin the past half decade, you canpredictthat you willget an increase incost and a decrease in quality, and anincreasein consolidationof bigness orinstitutionalization.And this has, ofcourse, occurred in the health caresystem. So what we have now is not afinancing problem but a capabilityproblem, as Dr. English said.
Group practicefits intothis question inmy opinion as being a potentialsolu-tion to part of our capabilityproblem.We have a number of capabilityex-panders. One is Comprehensive HealthPlanning. Anything that can make oursystem more efficient in delivery willexpand our capability.CHP would beone of them.
Another important capabilityexpanderisoperations or systems or administra-tive research. I think group practiceshould be classifiedat this point in
L
;~’>;history as a research endeavor. Iwould -.}hate to seegroup practiceimplementedtotallyand widelywithout an adequate

,$p,period of testing. I am afraid that we
.,: $have run intothe same types of unex-:’...:?.:.
--.z.-~ pected problems that we did with Medi-care and Medicaid. So it is a thing thatneeds to betotally researched and isbeing researched in many areas. Itdoesmany things to the delivery system.First, it changes the mechanism ororganizes or systematizesthe mech-anism of entry into the health caresystem. Furthermore, it carries theindividual in an orderly fashion throughthe system in accordancewith needrather than in accordancewith the per-ceivedwants. Itchanges somewhat themotivation and control of utilization. Iconsider group practiceat this point asa very good idea in conceptthat needsto be further tested, applied on a fairlylarge scale—and it is, in fact, going tobe—before it is totally implemented indelivering health care in this country.
The nextquestion, in short, asks:
,..:- “We cannot hope to get enough physi-6~!,,,- ;<; cians produced in the nextfew years to......+ meet our physician manpower needs;
consequently,we will have to use ‘physi-cian-expanders’ of some type. How willthese physician-expanders be acceptedby the public and by the medical pro-fession?”
I think they would be acceptedboth bythe public and by the medical profes-sion, provided certain things can bedone.
You know, when you go to a bank, youdo not alwaysexpectto see the presi-dent and do not always need to see thepresident. Your needs can be takencare of very adequately by another typeof individual. When you go for healthcare, the same situation can and prob-ably should exist. However, there arecertain medical, legaland technicalproblems that make this very difficultand somewhat impractical in many in-stances. 1think we are moving rapidlynow toward surrounding this concept
“J: with adequate medical-legalsupportwith standards, licensing,and definitionof specialties.
Many PhySIClanS are using tne concep~withoutthe medicaIor legaldefinitions.There are some question marks aroundthis, but Ithink through practicewe aredevelopinga trend whichwill make thelegalaspectsof it much easier.
DR. MARGULIES: Some of the ques-tions I receivedare alsoon the subjectof health manpower. Let me lump themtogether and pick up what has alreadybeen said; and then there is anotherexplicitquestion which Iwill address ina moment. In order to do that, IthinkIshould retreat back intothe 1980sbecauseIwas not specificenough whenI spoke earlier about the way Ithinkthings are going to be. For one thing, Ibelievepre-payment systems probablywillbe fairly universalby that time.Secondly, Iwant to remind you that wehave been addressing certain myths uphere and some of those myths aregoing to be examinedeven further.
A myth we did not speakabout isthatbiologicalresearch necessarilymeansbetter health care. We found that wasnot true. The second myth was that ifyou increasethe abilityto purchasecare, the system is infinitelyexpansibleand can respond. We found that is nottrue. And the third one, which we aregetting into a better understanding on,isthat increasingthe number of peopleavailableto provide medicalservices isthe way to overcomethe manpowershortage. That is pre-eminentlyfalse.If you are to trace an investment in theeducationof a physician,relativeto anarea of need in the middle of Arkansas,you will find that the drop off betweenthe thousand dollars invested in themedicaIschool and the point of servicein the middle of Arkansas is astonish-ing. Now as ,aconsequence,we arefacing an interestingdilemma as we gointo the seventiesand eighties. If weare to maintain expertisein the qualityof medicalcare and make sure that it isavailable,what isthe role of the physi-cian and what isthe role of the people?I believethe followingevent willoccurby the eighties:
S~ecialistswill continueto be trained;they will be confined for the most part
23
to hospitals; they will be governed bythe hospitalsrather than by other kindsof systems.The majority of medicalcare is going to be provided by otherindividualsunder a system of mainte-nanceand supervision whichwillde-pend upon a different kind of physician.Some of this will be in group practice,but I must say that if there isanythingworse than an incompetent physicianin solo practice,it is a group of them.
So we have a few things to learn abouthow to manage group practice.But, ingeneral, Ithink we will discoverthat itis not necessaryto see a physicianfora very large percentageof those ail-ments which are now brought to theattentionof a physician. And if we looka Iittlefurther intothe seventies,I thinkwe are going to discover that a signifi-cant portion of the time spent by profes-sional people is spent giving attentionto individualswho do not needto beintothe health-caresystem at all.
A major input is going to be the use ofautomated techniques and I believethiswill includescreening methods whichwill have their concentrationon healthmaintenance rather than on the identi-fication of acute kinds of illnesses.
As a consequence,there willbe a dif-ferent use of allied health manpower.And although this may startleyou alittle,I think our current efforts to (1)increasethe output of medicalschools,associatedwith our efforts to (2)* re-organize the way in which health careis being provided, will leadto a discov-ery somewhere along the linethat weare training too many physicians. Ifthe latter is successful,the former isunwise. If the former is pursued andthe latter is not, we are going to have toget around to itat a later date. So allthese efforts to vastly increasemedicalschools,withthe illusionthat this willprovide medicalcare, are going to bere-examinedand, in the courseof time,i think are going to be dropped.
The solution lies,not in adding to thenumbers, but in
‘Numerals added.+ds.
making more effective
use of the way in whichthey spend theirtime. This means that responsibilitiesfor all levelsof providers are going tobe increasedand under supervised
@
!>...circumstances.And people are going
P&- ,-,
to be free to do those things which needto be done, where they needto be done,which iswhere people are ill. I thinkthat as a consequencethere is going tobe a regulationof the way in whichhospitalsare used.
Now the other question has to do witha much more precise issue,whichsounds rather small after I had beenoperating at that positivelevel. “ShouldRMP and CHP be combined?” Theanswer to that question is unequivo-cally “no,” They serve a different kindof a purpose and if I have my prefer-ences, Iwould say that CHP and RMPsshould operate in such a way that theyhave a productive tension betweenthem, one forcing demands on theother, the other dealing with those de-mands, They should have a basis be-tween them for an effectivenegotiationbetweenwhat the community needs
o
;,:V”with a resolution in capacity,the identi- ,%:-”
‘,,...fication of reasonable priorities,and .
the reachingtoward those prioritiesbya common understanding.
DR. ENGLISH: Just to expressaslightly different shade of opinion onthat manpower question, I agree withDr. Marguliestotally that we are movinginto the area of a new mythology if wethink that manpower, in terms of pro-ducing more of the same, is going to bethe solutionto the crisisof health care.Itobviously is much more complexthanthat, as he has pointed out so well.Buteven in medicalcare systems wherethere has been an attempt to utilizephysician manpower better, whereother kinds of present health manpowerare being utilized betteror where newkinds of health manpower are beingutilizedvery effectively,there is muchyet to be learned.
Iwould saythere isone example of thisthat I think you probably knowwell. It
G
.:?;~,,.,...,,::7,..Jis becoming increasinglyknown in this ,.
country as the Kaiser PermanencePro-gram. Even there, when you talk with
– ,– ,-they willtell you that one of their majorproblems in trying to expand is a short-age of medical manpower. 1think theproblem and the mythology isthat justproducing more manpower is not thesolutionany more than investingin bio-medicalresearch would solveourproblem.
I think to reallydeal withthe healthcare crisis,you have to face a wholerange of strategieswithouttolerancefor any mythology that begins with thenewconceptionsof howto organize anddelivercare. Only when you haveworked that out with a variety of ex-perimentation . . . can you figure outwhat your real manpower needsare andonly then can you figure out the pur-chasing power mechanism,the thirdparty payment mechanismsthat willsupport these new structures. I thinkour problem in the past is that we havenever had united strategy covering fi-nancing, manpower production, andthe issuesof organization and delivery.
This leads, I suppose, to a question thatwas asked, and which is, Ithink, perti-nent to many of the questionsthat wereceived.Iwill just read itto you. “Whydoes healthcare expenditure continueto increasewithout correspondingincreasein the quality of care?’
I think everyone up here has dealt withthat. I think Dr. Fowinkle in his lastremarks dealt with itwith real clarity.
Suppose that five years ago the Con-stitutionalscholars had discoveredthatthe Constitution had a basic humanright in itthat nobody reallyever noticedbefore. And that basichuman right wasto have in the living room of everyAmerican family a 23-inch color tele-vision set with a 14-foot antenna upon the roof and a lifetime maintenancecontractto make sure that itworkedterribly well. Itwas there in the Consti-tution all this time but we just neverpaid attentionto it. So the Congressdecidedto redress this oversight. Andit realizedthat itwould costabout $600a year to provide that televisionset toevery American and that some could
need some help in trying to pay itsothey started working on what was calleda National T. V. Aid Bill. And itwas veryclearthat itwas a very politicallypopu-lar measure and itwould take a littlework to get it through the Congress.But within three years itwould getthrough, and it would provide to everyAmerican—some on a 100 percentbasis, but others would have to contrib-ute something to the cost of that set—the purchasing power to put such aninstrument in every American home.
If we were back at that time, I thinkyou could imagine what outfits likeGeneral Electric,Zenith, RCA, andAdmiral would be doing. Itwould bemy prediction that they would be outborrowing money to expand their abil-ityto produce, even if the interestrateswere 15 to 20 percent. Why? Becausethey were going to be guaranteed atremendous source of purchasing powerwhen that legislationwent through. Itwould compensate them very wellfortaking that risk, even at very high in-terest rates. I think it is also very pre-dictablethat you and Iwould be outbuying all the stockwe could in thosecompanies, becausewith that kind ofguaranteed purchasing power itwouldnot be hard to predict howthey weregoing to do.
Our problem in health isthat we havebeen misunderstood and thought to belikethat. First, we kidded ourselvesinto thinking we had the capacity inthis country in health to serve the needsof 200 million people and then we sawthat mythology exploded when $14,-500,000 of purchasing power wasgiven to consumers to test. That istheseed of the present crisis,and itseemsto me that’s the reason why, althoughthe money going into health care isrising dramaticalIy,the quality on thisoverburdened system—if you can callit a system—of health care is being ex-posed greatly every day. And of coursethe implicationsof national health in-surance— which would expand thepurchasing power almost beyond ourpresent ability to imagine—would dem-onstrate our present inadequaciestorespond even more dramatically.
25
That is the critical importance of thePartnership for Health and RegionalMedical Program. if we are not given,publicly and privately, the money toexpand, whether it is in manpower ornew methods of organization and de-livery,whether it is in the newthingswe need to know about howto deliverhigh qua!ity care, the new kind of re-search that is required, wewillcontin-ually be in this bind, even though thetotal number of dollars grows. Ithinkthat is what we havegot to understandand that is what we havegot to helpthe American people understand andthat is why the nextquestion is a verypertinent one: “What are the chancesthat the private sectorwillmove rapidlyenough and the voters be patientenough to avoid a government-controlledmonolithicsystem?”
How do we encourage provider changeand voter patience?On the basisof pastperformance, the chancesthat theprivatesectorwill move rapidly enoughare very slim. Federal leadershiphasbeen very important. We are not seeingthat federal leadershiptoday neces-sarily in measure to what the crisis is.So therefore 1think our dependencyon the private sector is greater thanever, I do not see sufficientoptimisticsignsthat the private sector is going tomove rapidly enough exceptin suchprograms as RMP and the Partnershipfor Health, medicalsocieties,health de-partments and hospitalsand programslikethe neighborhood healthcenter.
But the major hang-up right now isresources in that area to do all thethings they would liketo do. That iswhy the only thing that isgoing to helpus with the voter is the extentto whichhe seeswe are concernedand that weare trying, the extenthe understandsour difficultiesand helps us change theway that $93,000,000,000 isgoing tobe spent in 1975.
DR. CANNON: If the response is notadequate, how much time before weconsider the crisisto have reachedthepoint of a burst and something ratherradical happens in the health caresystem?
DR. ENGLISH: I think that when youconsider that it took us nearly two
e’
...
centuries to develop the excellenceof.,
American medicine, an excellenceinthis country that is unrivaled anywherein the world, maybe you should arguethat we should have another centuryat leastto deal with the nextgreat issue,which is ‘‘equity’ —how to translatethat excellenceinto equity and effici-ency and respectfor human dignity inthe delivery of that excellenceto200,000,000 Americans.
But Ithink the real problem isthat weare not going to get a century. As amatter of fact, things are changingmuch too rapidly for that. The con-sumer is becoming much too sophisti-cated and he recognizesfor the firsttime that our national resources arelimited and there is going to be greatcompetitionwithin major segments ofthe societyfor those resources. Ibelievethat we have about five yearsto do what needs to be done and Ithink
Q
4;.<;,‘ithat isgoing to take tremendous initia- .’.,.,,~;....tive from the private sector in our coun- ““’”’btry ifwe are going to make any progress.
I think if it is not done in five years—that is, if we do not increaseour capac-ityto provide care in five years—then inthe second half of this decade, we aregoing to see things like national healthinsurance and they are going to abso-lutely expose our present inadequacyin delivering care ten times as dramatic-ally as it is being exposedtoday. We willsee our profession, whether it isthepracticing physicianor the hospitalsofthis country or any other segment ofthat profession, thoroughly discreditedbefore the consumer will understandthat the money is going up, that thecosts are going up and the service isgetting worse, Ithink that is how acountry finds itself in governmentmedicine.That iswhy Ithink this willbe the most historicdecade in medicinein this country rivaled by only that first fi.?idecade back in 1785 when the first
L
.......:,.,,....medical school, hospital, and mental
..... -‘i
hospital were started in this countryin Philadelphia.

S U M M A R Y S TAT E M E N T SMR. SIMS: People with not as muchexperienceas Dr. Margulies, their mainconcern was that the distribution ofservicesand the public health profes-sion’s education ought to be majorcomponents of any health caresystem. . . We are concerned with all kinds ofmanpower . . . Doctors are extremelyconcerned about consumers takingpre-eminent roles in what they feelought to be their rolesdetermining whatmedicalcare ought to be at any givenpoint in time.
DR. FOWINKLE: On the consumer,I think it is clear to most of us in thehealth administration businessthatthe consumer is going to be involvedmore substantially in the determinationof health policy. I think what the con-sumer really wants is a good productand he wants it at an affordable price.I think he istelling us very clearlywhathe wants and is probably telling us thatif he does not get it, he is going to trysome method of his own to help usproduce it.
I think we will have to deal effectivelywith the consumer and his demand,but yet Istill feel very keenly about theneed for professional involvement inthe policy-making process. I think theconsumer is going to have to tell us
what he wants and he willdo it fortun-ately as a voter. Yet I am hoping we cantemper this with professional judgmentand knowledge.The consumer wantsa good product and he wants it at anaffordable price and he is burdening iton our backto produce it.
In summary, I would liketo dealwith the question of national health in-surance. When willwe have it?Shouldwe have it?As an administrator of thestate program for financing medicalcare to the tune of about $50,000,000—i would very much liketo see nationalhealth insurance. Itwould relievefromthe state at least part of the burden oftheir share of the financing and a tre-mendouslyoverwhelming administrativetask of running this thing. We have a$50,000,000 program superimposedupon a $20,000,000 agency. So wehave the tail wagging the dog and thisis happening all over the country. Statesare staggering under the administrativeand physical load of Medicaid. So Ithink from the state standpoint, 1wouldlikevery much to have national healthinsurance. This would standardize itand Iift the burden somewhat off thestate.
Looking at it from the health-systemstandpoint, I think we must emphasize
27
that it would make a more efficientfinancing mechanism, which wouldhave the same effect and adding to thefinancing of health care, which wouldsimply throw coal on the fire by pro-ducing further inflation and furtherdecreasing quality. So we have got tochange our national, state, and localpriorities for capability expansion ratherthan financing, and this includesna-tional health insurance in the foresee-able future.
DR. MARGULIES: I would liketoanswer one question, because it did notcome out of the audience and becauseits deficiencydisturbs me. In decidingwhat health care should be like in theeighties, determining it by what hap-pened in the seventies,we have to faceone of the most difficult issues,whichis the concern more at this point of thenon-professionals than it isthe profes-sionals. Over the last25-30 years, thepublic has been lured into having ap-petitesfor yellow refrigerators, orwhatever it may be, whichwe mustlearn to change into other kinds ofappetites.
The creed now is a transplant in everygarage—the exotic,the sophisticated,in fact, the whole kind of concepttheRMP began with and withwhich I neveragreed, even in the early days. If weare to be effective in RMP and CHP,the problem is a double one. Not onlymust we be responsive to consumers,but we must be able to interpret toconsumers the difference between anirrational and the rational effort to meettheir basic needs. And because it isasophisticated issue and becausethehealth care system is complex, it meansthat the professional efforts of an RMPor any other organization needs the fullunderstanding, the full exploitation,andthe most minute interpretationto thecommunity so they can appreciatethedifference betweenthe visible,theglittering and the glamorous and whatreally is essentialfor health mainte-nance for control of costand for thebasic health of the community.
DR. ENGLISH: Iwould liketo share justtwo dreams. One would be to proceedwith confidenceand go to the placeswhere we are going to need help beforewe can do the job in the 1980s. One of
es:,
the placesI think we need to go, aspracticingphysicians,as hospital ad-ministrators, as officialsof the states,of the cities, in the whole purveyorsystem, isto the school of business.Iwould liketo see by 1980 two to threepercentof the graduating classof everyschoolof business administration inthis country producing people who willcome and help us with what, by thattime, will be a $100,000,000,000 enter-prise. I do not think the physicians andhealth professionals should become themajor managers in an enterprise of thismagnitude, of this size, of this complex-ity. There is littlein our training andthere is littlein what brings us into thefield of healththat equips us for this.
So, I think we should welcome helpfrom those institutionswhich producepeoplewho have this kind of expertisebut who have not yet come, often be-causethey have not yet been asked, to ,;,.$,’;help us in one of the largestsegments ‘t~”~”of one of the most important segmentsof our national life.That, I hope, willoccur by the 1980s,
The secondthing that I hope will haveoccurred by that time isthat we wouldbe having meetings likethis but ex-panded intowhat one might call, “townmeetings” in health, around the crisisof health care all over the country, thathealth would becomethe critical issuethat I believeDr. Margulies and othermembers of the panel have predictedit will increasinglybecome,
The consumer isthe best ally we havein the tremendous competitionforresources. But rather than waiting forthem to come to us, we willgo out tothem, gain their understanding, theirhelp, their partnership. If in the 1980swe seethat alliancebetweenthe healthprofessionalsand the consumers in
G
,...~~..this country, Ithink we can proceed with ‘X-.;’~~l+.:great confidenceto be sure that we willserve the national interestsas the publicin this country hopes that we will.

,~~,:.j!. ..3,,:......,
.. ... .,., ...
- x -“
“Should RMP and CHP be combined?The answer to that question is unequiv-ocally ‘no. They serve a different kindof a purpose and if I have my prefer-ences, i would say that CHP and RMPsshould operate in such a way that theyhave a productivetension betweenthem, one forcing demands on theother, the other dealingwith those de-mands. They should have a basis be-tweenthem for an effectivenegotiationbetweenwhat the community needswith a resolution in capacity,the identi-fication of reasonable priorities,andthe reachingtoward those prioritiesbya common understanding . . .
“if we are to be effectivein RMP andCHP, the problem isa double one. Notonly must we be responsiveto con-sumers, but we must be able to interpretto consumers the difference betweenan irrational and the rational effort tomeet their basic needs. And becauseit is a sophisticated issueand becausethe health care system is complex, itmeans that the professionaleffort of anRMP or any other organization needsthe full understanding, the full exploi-tation, and the most minute interpreta-tion to the community so they canappreciatethe difference betweenthevisible,the glittering and the glamorousand what really is essentialfor healthmaintenancefor controlof costandfor the basic health of the community,”
—Dr. Harold Margulies