medical options in the treatment of acromegaly i m holdaway june 29 2013
TRANSCRIPT

Medical options in the treatment of acromegaly
I M Holdaway
June 29 2013

Medical treatments for acromegaly (non-surgical and non-radiotherapy)
• Older treatments- medroxyprogesterone- oestrogen (tablets or patches or look-alike preparations)
• Dopamine – like agents:- bromocryptine - cabergoline (special authority)
• Somatostatin analogues:- aqueous octreotide (subcut injection) (special authority)
- depot octreotide (sandostatin LAR) (special authority)
- Lanreotide (not marketed in NZ)
- Oral octreotide (under trial in USA)
- Pasireotide (not available in NZ)
• Pegvisomant (Named Patient Pharmaceutical Assessment)

Growth hormone
IGF-I (insulin-like growth factor-I)
Growth and metabolic effects
Pituitary gland
liver
Brain (hypothalamus)
A few direct effects of growth hormone e.g. on fat cells
Action of growth hormone and insulin-
like growth factor-I (IGF-I)

Older studies of the medical treatment of acromegaly
• Medroxyprogesterone (depot-provera & Megace)
• Oestrogen- oral oestrogen tablets
- oestrogen patches
- oestrogen – like agents, anti-oestrogens

JCEM 1970
(Note – later studies could not replicate these results)
Remission level of GH

Pituitary, 2012

45% cure level of IGF-I
Published series using oestrogen to treat acromegaly

Dopamine – like agents
• Bromocryptine• Cabergoline (longer duration of action, very low rate
of side-effects compared with bromocryptine)
Labelled dopamine binding to its receptor in the pituitary
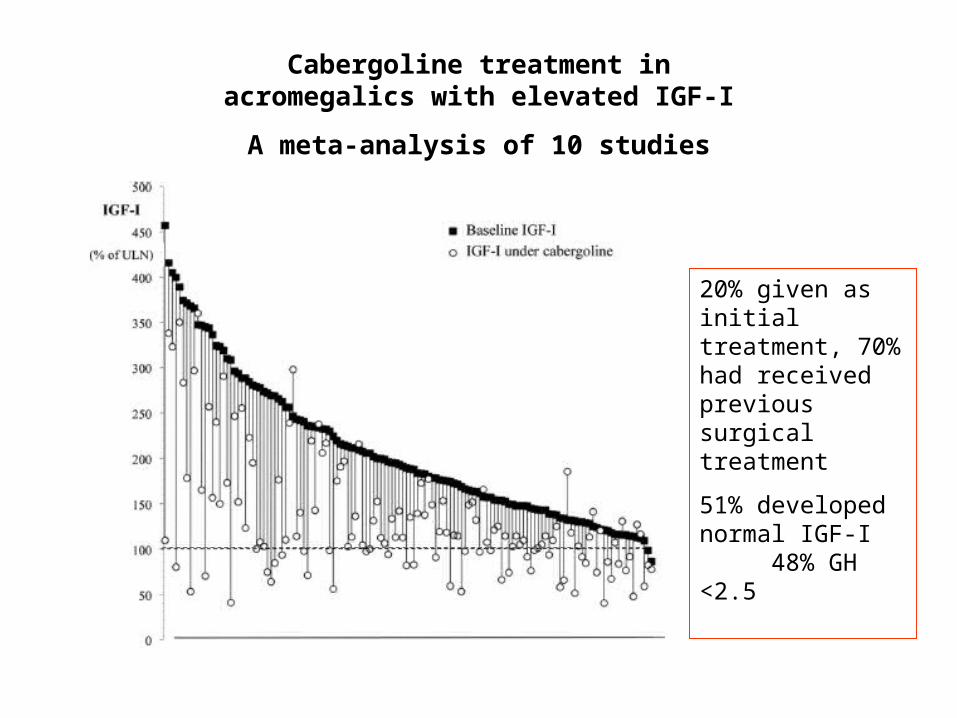
Cabergoline treatment in acromegalics with elevated IGF-I
A meta-analysis of 10 studies
20% given as initial treatment, 70% had received previous surgical treatment
51% developed normal IGF-I 48% GH <2.5

Individuals with elevated serum IGF-I during treatment with LAR octreotide, then treated
with addition of cabergoline
52% achieved normal IGF-I levels
45% GH <2.5ug/l

But you have to take tablets correctly……..

Somatostatin look-alike agents
• Octreotide – a potent somatostatin-like agent- aqueous octreotide injection (short duration of action)
- depot octreotide injection (long duration of action)
- aqueous and depot lanreotide similar
• Pasireotide – a somatostatin-like agent with a broader range of action than octreotide
• Orally active octreotide

SR 1
SR 2SR 3 SR 4
SR 5
Signal to interior of pituitary cell to stop
making growth hormone
Main receptor for octreotide and lanreotide
Somatostatin action on growth hormone – producing pituitary cells
Cell wall
SR = somatostatin receptor


1 year
5 years
Pre-treatment
Effect of 1 and 5yrs LAR octreotide therapy on GH and IGF-I levels in acromegalic men
Safe level
Safe level
Colao 2009

Serum GH with LAR therapy(mean SD)
Auckland patients
Basal GH On LAR05
101520253035404550556065
seru
m G
H (
ug
/l)
P = 0.002

Serum IGF-I with LAR therapy(Z-score, expressed as mean SD)
Auckland patients
Basal IGF-I IGF-I on LAR0
1
2
3
4
5
6
7
Ser
um
IG
F-I
(Z
-sco
re)
P = <0.001

baselineLarge adenoma
smaller
Almost gone
6 months LAR octreotide
18 months LAR octreotide treatment
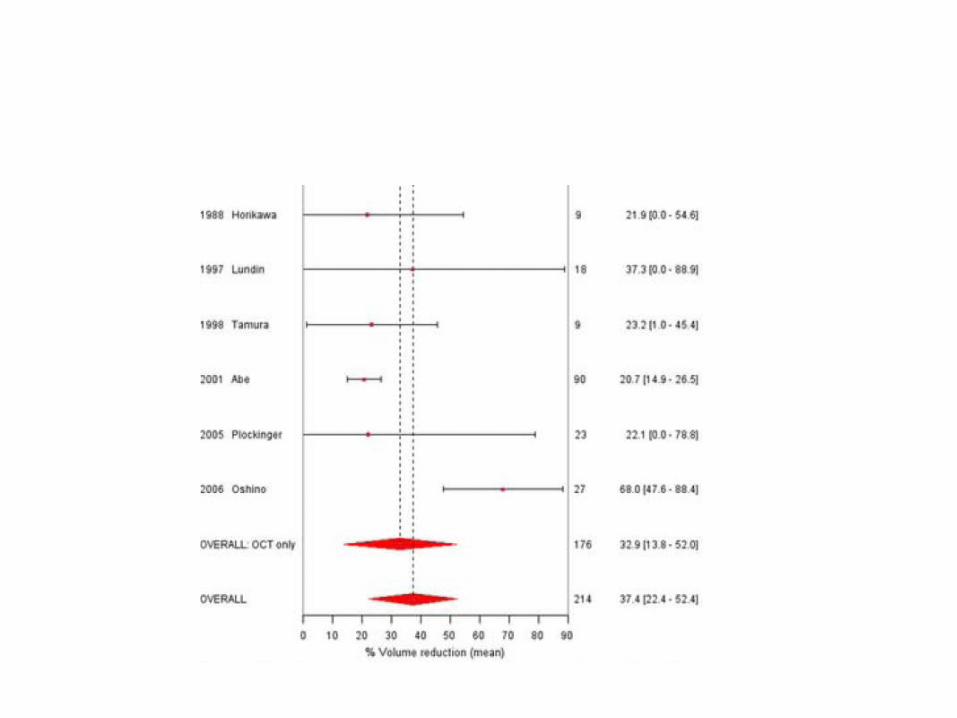
Shinkage of acromegaly adenoma with LAR
octreotide

Meta-analysis
53% of individuals with acromegaly show more than 20% shrinkage of
their adenoma with LAR octreotide (average
volume reduction 50%)
53%
Effect of LAR octreotide on adenoma size
Giustina et al, 2012

Mean ± SEM proportion of acromegalicpatients achieving safe hormone levels
with LAR octreotide
GHIG
F-I0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n w
ith
tar
get
lev
els
Meta-analysis by Freda et al, 2005, n= 612
Remission ratewith surgery
0
10
20
30
40
50
60
70
80
90
all tumours microadenomas
Per
cen
t re
mis
sio
n
17 surgical series 1987-2011
Remission of acromegaly with initial surgery or with LAR octreotide
SR 1
SR 2SR 3 SR 4 SR 5
Signal to pituitary cell to stop making growth
hormone
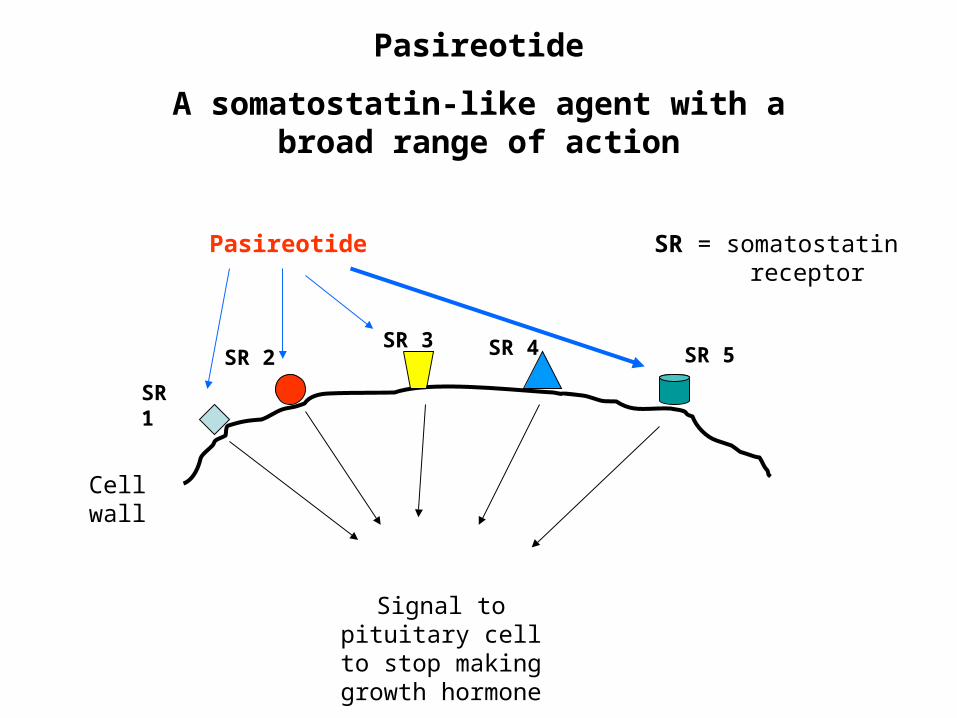
Pasireotide
A somatostatin-like agent with a broad range of action
Cell wall
SR = somatostatin receptor
Pasireotide

Pituitary tissue – microscopic view, stained for various somatostatin receptors
Type 1
Type 2
Type 3
Type 4
Type 5

Use of the somatostatin receptor analogue, Pasireotide in the treatment of acromegaly
Bronstein M US Endo Soc meeting 2012

Serum IGF-I and GH levels in an acromegalic subjectgiven a single injection of pasireotide
June
2011
July
201
1
Aug 201
1
Sept 2
011
Oct 2
011
Nov 20
11
Dec 2
011
0
200
400
600
0.0
0.2
0.4
0.6
0.8
IGF-I Growth hormone
PS
eru
m I
GF
-I (
ug
/l) S
erum
GH
(ug
/l)

Sent from my iPad
.
TPE absorption system for small peptides such as octreotide
Oral octreotide - the way of the future?

Tight junctions between cells (impermeable)
Tight junctions opened up by oily film (allows entry of larger molecules into circulation)
Blood flow
Intestinal contents
Cells lining the intestine
Barrier to absorbing large molecules from the intestine

Stimulated GH
Stimulated GH after oral octreotide
Effect of oral octreotide (Chiasma) on growth hormone secretion
stimulated by GHRH
Tuvia, 2012
Pegvisomant
A drug designed to block the growth hormone receptor and prevent the adverse effects of high growth hormone levels in acromegaly

Growth hormone
IGF-I (insulin-like growth factor-I)
Growth and metabolic effects
Pituitary gland
liver
Brain (hypothalamus)
A few direct effects of growth hormone e.g. on fat cells
Action of growth hormone and insulin-
like growth factor-I (IGF-I)
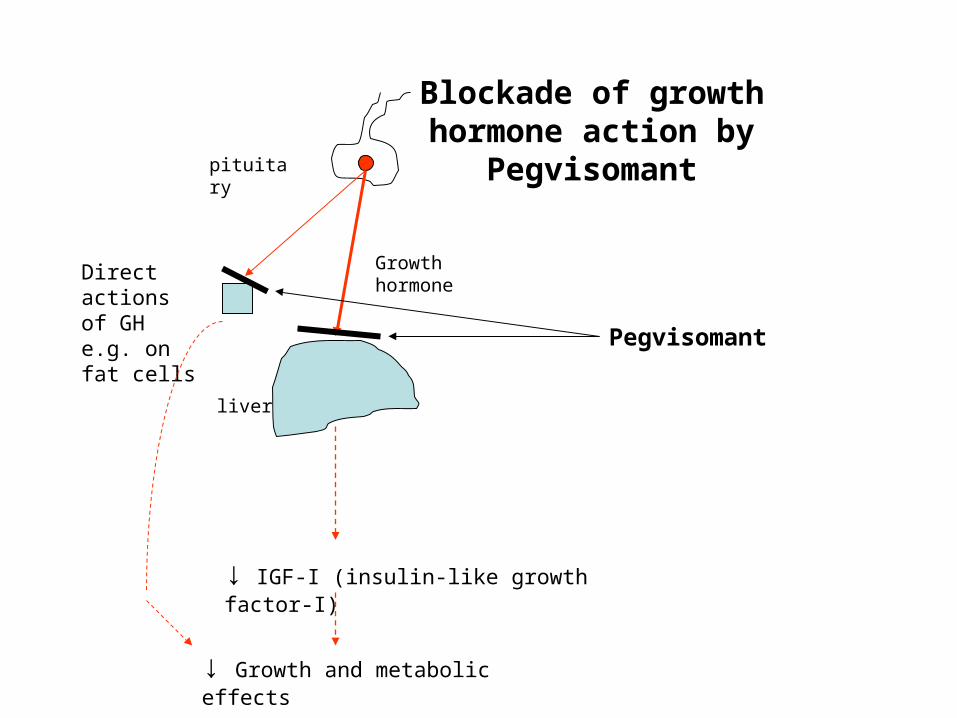
Growth hormone
↓ IGF-I (insulin-like growth factor-I)
↓ Growth and metabolic effects
Pegvisomant
Blockade of growth hormone action by
Pegvisomantpituitary
liver
Direct actions of GH e.g. on fat cells

Design of Pegvisomant


Serial IGF-I measurements during pegvisomant treatment in the German observational study
Schreiber et al, 2007
76% normalised
n = 229

What of the future?
• Effective oral octreotide
• By-passing surgery and using medical treatment as first option
• Treatment with a drug linked to either a chemotherapy agent such as tozolamide, or linked to a radioactive agent to kill the tumour cells
• A combined dopamine/octreotide agent

THE END!


Australian acromegaly awareness campaign
• While there was minimal mainstream print, radio and television consumer media coverage the more targeted media ran the story. Targeting magazines was effective.
• The medical media release hit all the targets and more with the smaller groups keen to run the story for their local newsletters.
• An increase in the Australian Pituitary Foundation website hits saw June (????), July (907 hits), August (982 hits), September (583 hits) (Note- medical media release issued mid July and consumer media release issued 1 August)
• A key learning is that mainstream media may not always be the best approach when it comes to disease awareness campaigns of this type.
• This a good example of widespread medical and patient/consumer coverage via non-mainstream mediums.

Pretreatment with SSAs prior to pituitary surgeryin acromegaly
contro
l
pretre
ated
contro
l
pretre
ated
0
10
20
30
40
50
60
70
80
90
POTA study (Norway)
Abe & Ludecke (Hamburg)
Per
cen
t cu
red
at
surg
ery
Abe et al, 2001
concept
57 90
30
32

Symptomatic response to octreotide LAR (n=10)
Symptom n before n afterHeadache 4 0
OSA - like 7 1
Arthralgia 5 2
Sweating 6 1
CTS 4 0
Hypertension 3 2
Diabetes 2 2
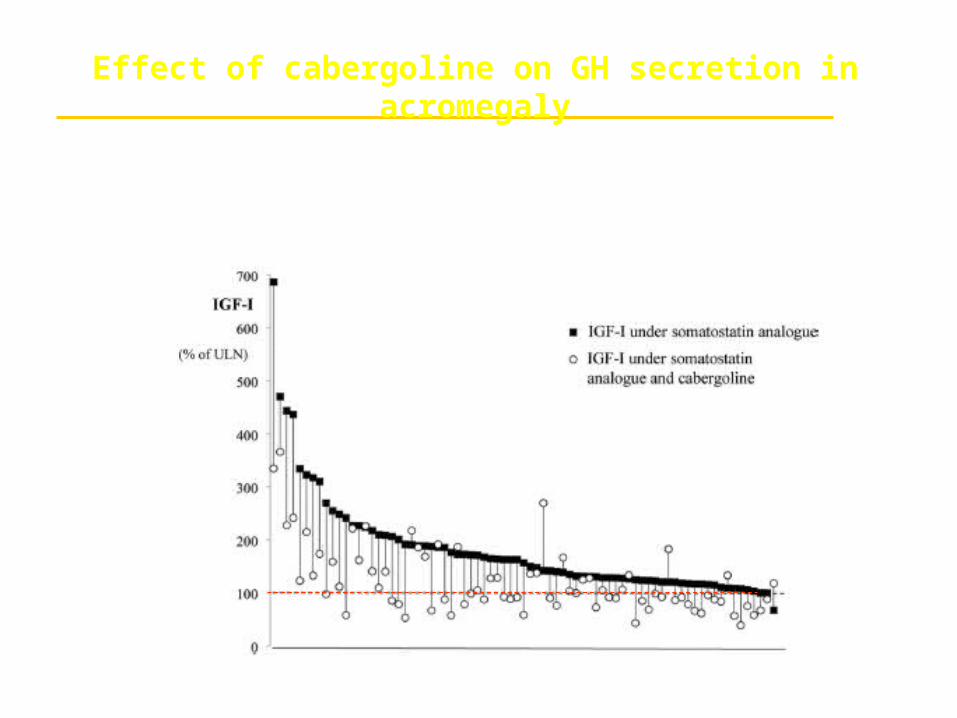
Cabergoline + LAR octreotide therapy
Individual patientsSandret et al, 2011
Effect of cabergoline on GH secretion in acromegaly
52% had normal IGF-I