medical error root cause analysis and disclosure ethan cumbler md, facp dimitriy levin md...
TRANSCRIPT

Medical ErrorMedical Error
Root Cause Analysis and DisclosureRoot Cause Analysis and Disclosure
Ethan Cumbler MD, FACPDimitriy Levin MD
Hospitalist SectionUniversity of Colorado Hospital
2012

How do Physicians Respond to How do Physicians Respond to Medical Error?Medical Error?

CASECASE
Transfers Can Be Transfers Can Be
Hazardous To Your HealthHazardous To Your Health

18 year old female notices 18 year old female notices fatigue, dyspnea on fatigue, dyspnea on exertion, periorbital and exertion, periorbital and extremity swelling and extremity swelling and decreased urine outputdecreased urine output
No significant past historyNo significant past history
No allergies to medicationsNo allergies to medications
Takes no medicationsTakes no medications
Social and family history Social and family history are unrevealingare unrevealing
Blood pressure 190/105Blood pressure 190/105
Blood urea nitrogen 142Blood urea nitrogen 142
Creatinine 10.5Creatinine 10.5
Potassium 6.9Potassium 6.9
Phosphorous 10Phosphorous 10
Hemoglobin 6Hemoglobin 6
Ultrasound shows Ultrasound shows small scarred small scarred atrophic solitary atrophic solitary kidneykidney

Admitted for initiation of dialysis for End Stage Admitted for initiation of dialysis for End Stage Renal DiseaseRenal Disease
Her half-sister agrees to a living-donor Her half-sister agrees to a living-donor transplanttransplant
She is re-admitted for kidney transplantationShe is re-admitted for kidney transplantation
4 days after transplant she is ready for 4 days after transplant she is ready for transfer to the floor.transfer to the floor.
ICU General Medical Ward
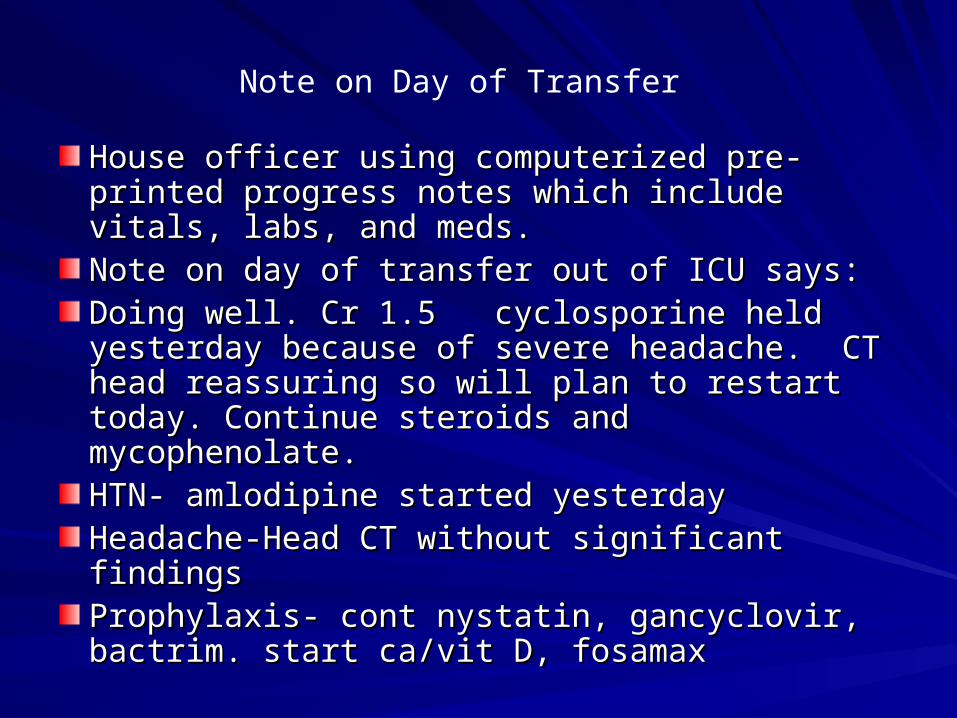
House officer using computerized pre-printed House officer using computerized pre-printed progress notes which include vitals, labs, and progress notes which include vitals, labs, and meds. meds. Note on day of transfer out of ICU says:Note on day of transfer out of ICU says:Doing well. Cr 1.5 cyclosporine held yesterday Doing well. Cr 1.5 cyclosporine held yesterday because of severe headache. CT head because of severe headache. CT head reassuring so will plan to restart today. Continue reassuring so will plan to restart today. Continue steroids and mycophenolate.steroids and mycophenolate.HTN- amlodipine started yesterdayHTN- amlodipine started yesterdayHeadache-Head CT without significant findingsHeadache-Head CT without significant findingsProphylaxis- cont nystatin, gancyclovir, bactrim. Prophylaxis- cont nystatin, gancyclovir, bactrim. start ca/vit D, fosamaxstart ca/vit D, fosamax
Note on Day of Transfer
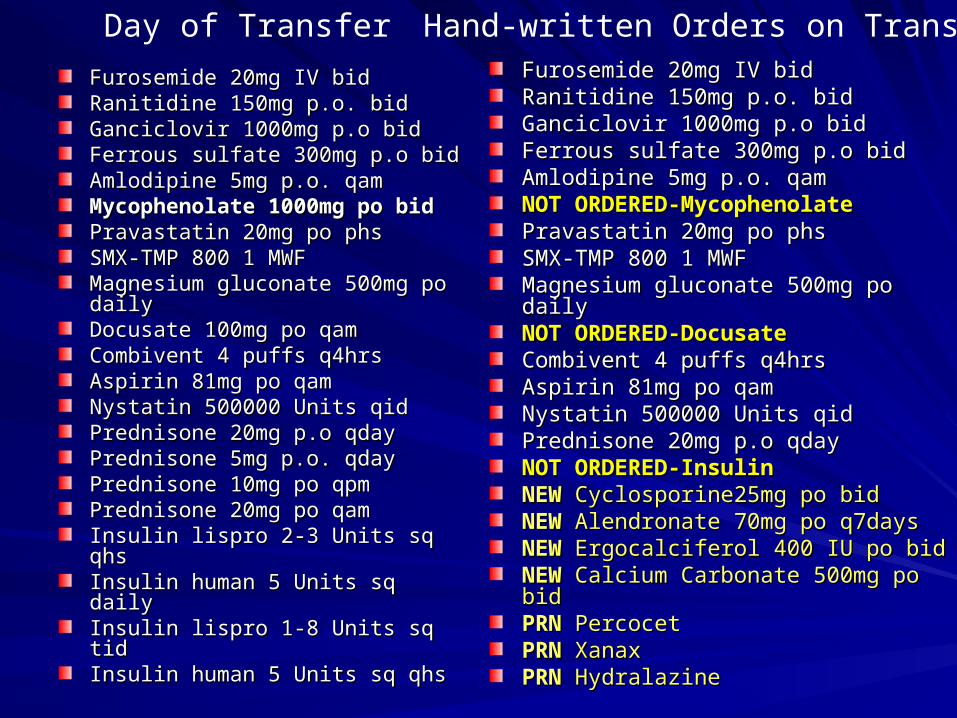
Furosemide 20mg IV bidFurosemide 20mg IV bidRanitidine 150mg p.o. bidRanitidine 150mg p.o. bidGanciclovir 1000mg p.o bidGanciclovir 1000mg p.o bidFerrous sulfate 300mg p.o bidFerrous sulfate 300mg p.o bidAmlodipine 5mg p.o. qamAmlodipine 5mg p.o. qamMycophenolate 1000mg po bidMycophenolate 1000mg po bidPravastatin 20mg po phsPravastatin 20mg po phsSMX-TMP 800 1 MWFSMX-TMP 800 1 MWFMagnesium gluconate 500mg po Magnesium gluconate 500mg po dailydailyDocusate 100mg po qamDocusate 100mg po qamCombivent 4 puffs q4hrsCombivent 4 puffs q4hrsAspirin 81mg po qamAspirin 81mg po qamNystatin 500000 Units qidNystatin 500000 Units qidPrednisone 20mg p.o qdayPrednisone 20mg p.o qdayPrednisone 5mg p.o. qdayPrednisone 5mg p.o. qdayPrednisone 10mg po qpmPrednisone 10mg po qpmPrednisone 20mg po qamPrednisone 20mg po qamInsulin lispro 2-3 Units sq qhsInsulin lispro 2-3 Units sq qhsInsulin human 5 Units sq dailyInsulin human 5 Units sq dailyInsulin lispro 1-8 Units sq tidInsulin lispro 1-8 Units sq tidInsulin human 5 Units sq qhsInsulin human 5 Units sq qhs
Furosemide 20mg IV bidFurosemide 20mg IV bidRanitidine 150mg p.o. bidRanitidine 150mg p.o. bidGanciclovir 1000mg p.o bidGanciclovir 1000mg p.o bidFerrous sulfate 300mg p.o bidFerrous sulfate 300mg p.o bidAmlodipine 5mg p.o. qamAmlodipine 5mg p.o. qamNOT ORDERED-MycophenolateNOT ORDERED-MycophenolatePravastatin 20mg po phsPravastatin 20mg po phsSMX-TMP 800 1 MWFSMX-TMP 800 1 MWFMagnesium gluconate 500mg po dailyMagnesium gluconate 500mg po dailyNOT ORDERED-DocusateNOT ORDERED-DocusateCombivent 4 puffs q4hrsCombivent 4 puffs q4hrsAspirin 81mg po qamAspirin 81mg po qamNystatin 500000 Units qidNystatin 500000 Units qidPrednisone 20mg p.o qdayPrednisone 20mg p.o qdayNOT ORDERED-InsulinNOT ORDERED-InsulinNEWNEW Cyclosporine25mg po bid Cyclosporine25mg po bidNEWNEW Alendronate 70mg po q7days Alendronate 70mg po q7daysNEWNEW Ergocalciferol 400 IU po bid Ergocalciferol 400 IU po bidNEWNEW Calcium Carbonate 500mg po bid Calcium Carbonate 500mg po bidPRNPRN Percocet PercocetPRNPRN Xanax XanaxPRNPRN Hydralazine Hydralazine
Day of Transfer Hand-written Orders on Transfer

What Set-ups For Error Can You What Set-ups For Error Can You Identify?Identify?
Day 1 after TransferDay 1 after TransferPhysician different than the one who wrote the Physician different than the one who wrote the transfer orders uses computerized preprinted transfer orders uses computerized preprinted progress noteprogress noteComputer generated med list lists the Computer generated med list lists the medications ordered on transfermedications ordered on transferHouse officer has underlined the most important House officer has underlined the most important medications by handmedications by hand
Mycophenolate is not on the list as it was not Mycophenolate is not on the list as it was not ordered on transferordered on transfer
Day 1 after TransferDay 1 after Transfer
A/P- Doing great. Cr 1.5A/P- Doing great. Cr 1.5
Will restart cyclosporine with up-titration now Will restart cyclosporine with up-titration now that neuro issue resolved.that neuro issue resolved.
Continue Mycophenolate and steroidsContinue Mycophenolate and steroids
Was this an error of Omission or Commission?Was this an error of Omission or Commission?


Day 2 after TransferDay 2 after Transfer
Computerized preprinted progress note Computerized preprinted progress note used. Most important meds underlinedused. Most important meds underlined
Mycophenolate still not on med listMycophenolate still not on med list
A/P- Doing great. Cr 1.6 Approaching A/P- Doing great. Cr 1.6 Approaching discharge.discharge.
Continue steroids and mycophenolate.Continue steroids and mycophenolate.
Change cyclosporine to 125/150 in pmChange cyclosporine to 125/150 in pm
Day 3 after TransferDay 3 after Transfer
Computerized preprinted progress note Computerized preprinted progress note used. Most important meds underlinedused. Most important meds underlined
Mycophenolate still not on med listMycophenolate still not on med list
A/P- Creatinine now 2.0 A/P- Creatinine now 2.0
Continue mycophenolate, prednisone Continue mycophenolate, prednisone 20mg, cyclosporine 125/15020mg, cyclosporine 125/150
Day 4 after TransferDay 4 after Transfer
Computerized preprinted progress note Computerized preprinted progress note used. Most important meds underlinedused. Most important meds underlined
Mycophenolate still not on med listMycophenolate still not on med list
A/P- Cr 2.5 urine output decreasing. A/P- Cr 2.5 urine output decreasing.
Biopsy todayBiopsy today
Continue cyclosporine and mycophenolateContinue cyclosporine and mycophenolate
Day 5 after TransferDay 5 after Transfer
Computerized preprinted progress note Computerized preprinted progress note used. Most important meds underlinedused. Most important meds underlinedMycophenolate still not on med listMycophenolate still not on med listA/P- Cr 2.8 A/P- Cr 2.8 Biopsy results returned with rejectionBiopsy results returned with rejectionPlan- IV methylprednisolone burst startedPlan- IV methylprednisolone burst startedContinue cyclosporine and mycophenolateContinue cyclosporine and mycophenolateIncrease cylcosporineIncrease cylcosporine

Day 6 after TransferDay 6 after Transfer
Computerized preprinted progress note Computerized preprinted progress note used. Most important meds underlinedused. Most important meds underlined
Mycophenolate still not on med listMycophenolate still not on med list
A/P- Cr 3.0 A/P- Cr 3.0
Continue IV methylprednisoloneContinue IV methylprednisolone
Continue cyclosporine and mycophenolateContinue cyclosporine and mycophenolate

Day 7 after TransferDay 7 after Transfer
Computerized preprinted progress note used. Computerized preprinted progress note used. Most important meds underlinedMost important meds underlinedMycophenolate still not on med listMycophenolate still not on med listA/P- Clinically doing wellA/P- Clinically doing wellCr 3.2Cr 3.2s/p 3 days IV methylprednisolone- change to s/p 3 days IV methylprednisolone- change to prednisoneprednisonePrednisone 60mg, cyclosporine 250 bid, and Prednisone 60mg, cyclosporine 250 bid, and mycophenolate 1000mg bid.mycophenolate 1000mg bid.Mycophenolate is circled in the A/P with a note Mycophenolate is circled in the A/P with a note which reads which reads ““where is this?where is this?””

Day 7 after TransferDay 7 after Transfer
Patient restarted on IV steroids.Patient restarted on IV steroids.
Addendum comments on the patient Addendum comments on the patient missing 7 days of mycophenolate which missing 7 days of mycophenolate which ““had fallen off the MAR for some reasonhad fallen off the MAR for some reason””

Selective PerceptionSelective Perception
– Information we receive will be processed in a manner Information we receive will be processed in a manner that harmonizes with and supports our current beliefs.that harmonizes with and supports our current beliefs.
Root Cause AnalysisRoot Cause Analysis

ButWHY????
ButWHY????

What is RCAWhat is RCA
Systematic investigation to find the root Systematic investigation to find the root cause(s) of an eventcause(s) of an event
» There is always a root causeThere is always a root cause

Five Identifiable StepsFive Identifiable Steps
1.1. Define the problemDefine the problem
2.2. Collect dataCollect data
3.3. Identify possible causal factorsIdentify possible causal factors
4.4. Identify Root CausesIdentify Root Causes
5.5. Recommend and implement solutionsRecommend and implement solutions

Adverse events vs. errorsAdverse events vs. errors
Adverse eventAdverse event is injury from medical care is injury from medical careErrorError is doing the wrong thing is doing the wrong thing
(commission) or not doing the right thing (commission) or not doing the right thing (omission)(omission)
» Not all adverse events are due to errorsNot all adverse events are due to errorsAdverse events due to error are potentially Adverse events due to error are potentially
preventablepreventable
Define the problemDefine the problem

Collect DataCollect Data
Proof?Proof?Expert and front line inputExpert and front line inputImpact of the problemImpact of the problem
Identify Causal FactorsIdentify Causal Factors
As many potential causal or contributing As many potential causal or contributing factorsfactors
ToolsTools– AppreciationAppreciation
– 5 Whys5 Whys
– Drill DownDrill Down
– Fishbone/Cause and Effect DiagramsFishbone/Cause and Effect Diagrams

Identify the Root Cause (s)Identify the Root Cause (s)
Why does the causal factor exist?Why does the causal factor exist?
Above the surface:“The Weed”
Below the surface:“The Root”

How to RCAHow to RCA
IdentifiedProblem
Domains DomainsDomains
Contributing factor

How to RCAHow to RCA
Create a fishbone diagramCreate a fishbone diagramSelect a domainSelect a domainAsk Ask whywhy Repeat until a root cause is identifiedRepeat until a root cause is identified

Process inputs - DomainsProcess inputs - Domains
1. Materials1. Materials
2. People2. People
3. Machines3. Machines
4. Environment4. Environment
5. Management5. Management
6. Methods6. Methods

Process inputsProcess inputs
MaterialsMaterials– Defective, shortage, wrong typeDefective, shortage, wrong type
PeoplePeople– Lack of skills, lack of knowledge, lack of Lack of skills, lack of knowledge, lack of
motivation, stress, lack of capabilitymotivation, stress, lack of capability
MachinesMachines– Wrong tools, improper maintenance, bad Wrong tools, improper maintenance, bad
design, defectivedesign, defective

Process inputsProcess inputs
EnvironmentEnvironment– Physical layout of the workspace, physical Physical layout of the workspace, physical
demands of the task, forces of naturedemands of the task, forces of nature
ManagementManagement– Inattention, lack of supervision, lack of Inattention, lack of supervision, lack of
communication, lack of proper trainingcommunication, lack of proper training
MethodsMethods– Lack of process/procedure, deviation from Lack of process/procedure, deviation from
written procedures, poor communicationwritten procedures, poor communication
Recommend and Implement SolutionsRecommend and Implement Solutions
““An Ounce of prevention”An Ounce of prevention”Implementation logisticsImplementation logisticsRisksRisks
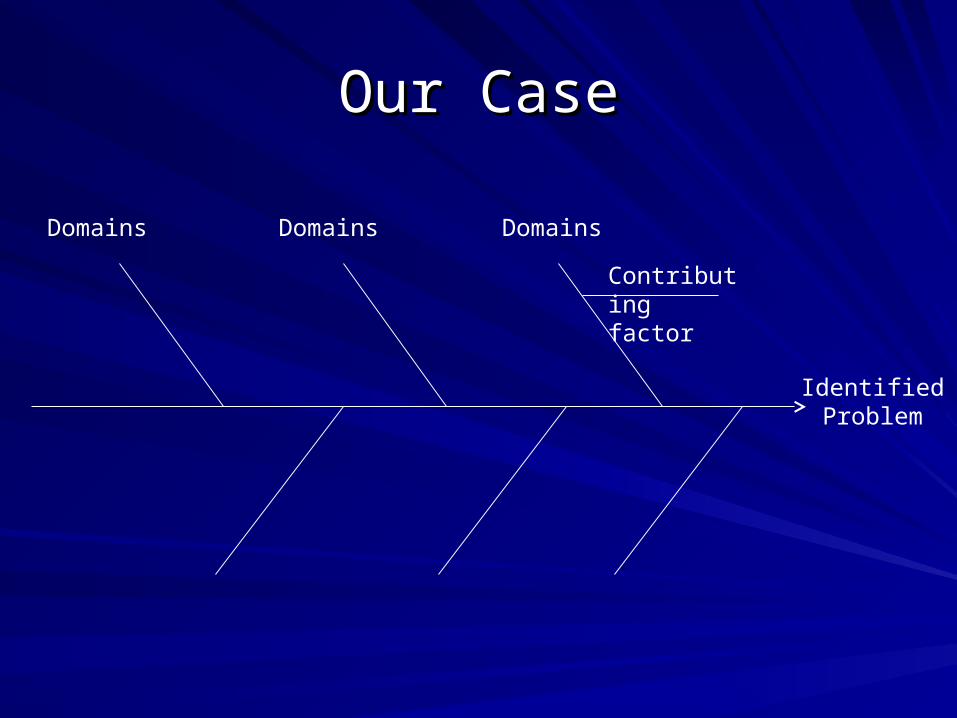
Our CaseOur Case
IdentifiedProblem
Domains DomainsDomains
Contributing factor


DISCLOSUREDISCLOSURE
What would you disclose in this caseWhat would you disclose in this case
Would you apologizeWould you apologize
How?How?

We DonWe Don’’t Discloset Disclose In one study of house staff, 50% did not discuss a In one study of house staff, 50% did not discuss a
serious clinical error with colleaguesserious clinical error with colleagues11
– only 25% disclosed to the patient or family.only 25% disclosed to the patient or family.
Disclosure rate is 30%-50% across a number Disclosure rate is 30%-50% across a number of surveys in Europe and Americaof surveys in Europe and America2-42-4..
X

Why DonWhy Don’’t We Disclose?t We Disclose?
Fear of increasing chance of litigationFear of increasing chance of litigationDesire not to lose the trust of the patientDesire not to lose the trust of the patient
– Particularly if the event did not result in Particularly if the event did not result in harmharm
Desire to avoid conflictDesire to avoid conflictDesire to avoid shameDesire to avoid shamePreservation of our self imagePreservation of our self imageWe donWe don’’t know how to do it well.t know how to do it well.

What Are the Consequences?What Are the Consequences?
Patients who discover error causing an Patients who discover error causing an adverse event later are likely to lose trust.adverse event later are likely to lose trust.88
– May be more likely to pursue legal actionMay be more likely to pursue legal action
A culture of non-disclosure prevents open A culture of non-disclosure prevents open discussion of errors, which impairs the discussion of errors, which impairs the ability of the system to improve.ability of the system to improve.

What does the evidence show?What does the evidence show?98.8% of patients report desiring disclosure of even 98.8% of patients report desiring disclosure of even
minor errors.minor errors.88
12% of patients report that they would sue for a 12% of patients report that they would sue for a moderate severity error if the physician informed the moderate severity error if the physician informed the patient about the error.patient about the error.77
– An even higher 20% of patients report they would sue if they An even higher 20% of patients report they would sue if they discovered the error by another means.discovered the error by another means.
36% of parents report that they would be less likely to 36% of parents report that they would be less likely to pursue legal action if an error involving their children pursue legal action if an error involving their children was disclosed.was disclosed.1515

Impact of Disclosure/Apology/Compensation
The Lexington Kentucky VAThe Lexington Kentucky VA1616
– Claims payment rate went from one of the Claims payment rate went from one of the highest in the nation to one of the lowest.highest in the nation to one of the lowest.
Michigan Statewide policy17
– Reduced lawsuits and total cost almost by half
Copic 3Rs program18

State Protections for Disclosure VaryState Protections for Disclosure Vary
Many states offer immunity for sympathy but not Many states offer immunity for sympathy but not for statements of fault.for statements of fault.
Colorado has one of the strongest protections-Colorado has one of the strongest protections-– A 2003 Colorado statute reads, A 2003 Colorado statute reads, ““In any civil action brought by an In any civil action brought by an
alleged victim of an unanticipated outcome of medical alleged victim of an unanticipated outcome of medical care….any and all statements, affirmations, gestures, or conduct care….any and all statements, affirmations, gestures, or conduct expressing apology, fault, sympathy, commiseration, expressing apology, fault, sympathy, commiseration, condolence, compassion, or a general sense of benevolence condolence, compassion, or a general sense of benevolence which are made by a health care provider….related to the which are made by a health care provider….related to the discomfort, pain, suffering, injury, or death of the alleged victim discomfort, pain, suffering, injury, or death of the alleged victim as the result of the unanticipated outcome of medical care shall as the result of the unanticipated outcome of medical care shall be inadmissible as evidence of an admission of liability.be inadmissible as evidence of an admission of liability.””

Would You Disclose?Would You Disclose? Would you disclose an error that led to fatality?Would you disclose an error that led to fatality?
Would you disclose an error that led to a major harm?Would you disclose an error that led to a major harm?
Would you disclose an error that led to minor harm?Would you disclose an error that led to minor harm?
Would you disclose an error which reached the patient Would you disclose an error which reached the patient but did not cause an adverse event?but did not cause an adverse event?
Would you disclose an error that did not reach the Would you disclose an error that did not reach the patient?patient?
When do you Have to Disclose a When do you Have to Disclose a Mistake?Mistake?1414
If the event had a perceptible clinical effectIf the event had a perceptible clinical effect If an event necessitated a change in patient careIf an event necessitated a change in patient care If an event presents a known risk in the futureIf an event presents a known risk in the future If a near-miss was evident to the patient or If a near-miss was evident to the patient or
family memberfamily member
You do not have to disclose errors which were You do not have to disclose errors which were corrected prior to reaching the patient.corrected prior to reaching the patient.

Two Forms of RegretTwo Forms of Regret
““II’’ m sorry your dog was run over m sorry your dog was run over””versusversus
““II’’m sorry I ran over your dogm sorry I ran over your dog””
The first apology is appropriate for a complication that The first apology is appropriate for a complication that occurs despite standard of care. occurs despite standard of care.
The second is the more appropriate apology for a The second is the more appropriate apology for a medical error.medical error.

How do you accomplish this?How do you accomplish this?
PreparationPreparation
SettingSetting
ParticipantsParticipants
Body LanguageBody Language
ContentContent
PreparationPreparationMake sure the facts are known completely before Make sure the facts are known completely before
disclosure.disclosure.
It is appropriate to tell a patient or family that an It is appropriate to tell a patient or family that an adverse event is being investigated prior to your adverse event is being investigated prior to your full discussion with them.full discussion with them.– This may require two meetings to do correctlyThis may require two meetings to do correctly
Discuss an medical error leading to major adverse Discuss an medical error leading to major adverse event, especially if it involves other individuals, event, especially if it involves other individuals, with risk management prior to talking to familywith risk management prior to talking to family

SettingSetting
The setting should be one that conveys The setting should be one that conveys calm.calm.
Participants should be at the same level, Participants should be at the same level, preferably sitting.preferably sitting.
Avoid interruptions.Avoid interruptions.

ParticipantsParticipants
Avoid having too many people present.Avoid having too many people present.
Avoid finger pointing between participants.Avoid finger pointing between participants.
You may want a representative from other You may want a representative from other disciplines (nursing, pharmacy) if the disciplines (nursing, pharmacy) if the explanation of the error involves processes with explanation of the error involves processes with which you are not familiar.which you are not familiar.
You may want the patient care advocate.You may want the patient care advocate.
You may want a representative from risk You may want a representative from risk management.management.

Body LanguageBody Language
Patient and physician at the same levelPatient and physician at the same levelOpen body posture (not crossing arms or Open body posture (not crossing arms or
legs)legs)Leaning forwardLeaning forwardAvoiding expressions of psychomotor Avoiding expressions of psychomotor
agitation (tapping feet).agitation (tapping feet).Unconscious mimicry of body positionUnconscious mimicry of body positionEye contactEye contact
ContentContent
Factual Explanation Recognition of Distress
Redress of HarmExpression of Regret
Keep it simple.Keep it simple.Avoid becoming defensive.Avoid becoming defensive.Take responsibility (if appropriate) Take responsibility (if appropriate) Apologize personally (if appropriateApologize personally (if appropriate ))

ContentContent
Offer concrete actions that will be taken to Offer concrete actions that will be taken to rectify the situation rectify the situation – You will need risk management to assist with You will need risk management to assist with
any financial promises.any financial promises.
Discuss how this event will create Discuss how this event will create change in your actions or in the change in your actions or in the system.system.

Why do Apologies FailWhy do Apologies Fail
Appearing insincereAppearing insincere Overly vague--Overly vague--““I am sorry for any errors that were madI am sorry for any errors that were mad
e.e.”” Using passive tense--Using passive tense--““Mistakes were made.Mistakes were made.”” Adding conditions--Adding conditions--““If any errors occurred, then I am If any errors occurred, then I am
sorry.sorry.”” Unacceptable explanations--Unacceptable explanations--““I had to leave the surgery I had to leave the surgery
to go to the bank.to go to the bank.”” Arrogance--Arrogance--““Even the best doctors make mistakes at Even the best doctors make mistakes at
times.times.””
A botched apology may be worse than no apology at all.A botched apology may be worse than no apology at all.
Case of Difficult DisclosureCase of Difficult Disclosure
Two volunteersTwo volunteers– Transplant RecipientTransplant Recipient– Attending Physician post-transferAttending Physician post-transfer
Not individual who committed the error of omission but was Not individual who committed the error of omission but was the doctor who cared for the patient for the last 4 days before the doctor who cared for the patient for the last 4 days before error identifiederror identified
Pharmacist also did not catch errorPharmacist also did not catch error
Lets Role Play!Lets Role Play!
ReferencesReferences1.1. Wu AW, Folkman S, McPhee SJ, Lo B. So House Officers Learn Wu AW, Folkman S, McPhee SJ, Lo B. So House Officers Learn
From Their Mistakes? JAMA 1991;265:2089-2094From Their Mistakes? JAMA 1991;265:2089-20942.2. Gallagher TH, Waterman AD, Garbutt JM, et al. US and Canadian Gallagher TH, Waterman AD, Garbutt JM, et al. US and Canadian
PhysiciansPhysicians’’ Attitudes and Experiences Regarding Disclosing Attitudes and Experiences Regarding Disclosing Errors to Patients. Arch Intern Med 2006;166:1605-1611Errors to Patients. Arch Intern Med 2006;166:1605-1611
3.3. Boyle D, OBoyle D, O’’Connell D, Platt FW, Albert RK. Disclosing Errors and Connell D, Platt FW, Albert RK. Disclosing Errors and Adverse Events in the Intensive Care Unit. Crit Care Med Adverse Events in the Intensive Care Unit. Crit Care Med 2006;34:1532-15372006;34:1532-1537
4.4. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. PatientsPatients’’ and Physicians and Physicians’’ Attitudes Regarding the Disclosure of Attitudes Regarding the Disclosure of Medical Errors. JAMA 2003;289:1001-1007Medical Errors. JAMA 2003;289:1001-1007
5.5. Gallagher TH, Garbutt JM, Waterman AD et al. Choosing Your Gallagher TH, Garbutt JM, Waterman AD et al. Choosing Your Words Carefully: How Physicians Would Disclose Harmful Words Carefully: How Physicians Would Disclose Harmful Medical Errors to Patients. Arch Intern Med 2006;166:1585-1593Medical Errors to Patients. Arch Intern Med 2006;166:1585-1593
ReferencesReferences6.6. Stewart RM, Corneille MG, Johnston J, et al. Transparent and Stewart RM, Corneille MG, Johnston J, et al. Transparent and
Open Discussion of Errors Does Not Increase Malpractice Risk in Open Discussion of Errors Does Not Increase Malpractice Risk in Trauma Patients. Ann Surg 2006;243:645-651Trauma Patients. Ann Surg 2006;243:645-651
7.7. Witman AB, Park DM, Hardin SB. How Do Patients Want Witman AB, Park DM, Hardin SB. How Do Patients Want Physicians to Handle Mistakes? A Survey of Internal Medicine Physicians to Handle Mistakes? A Survey of Internal Medicine Patients in an Academic Setting. Arch Intern Med Patients in an Academic Setting. Arch Intern Med 1996;156:abstract1996;156:abstract
8.8. Mazor KM, Simon SR, Yood RA, et al. Health Plan MembersMazor KM, Simon SR, Yood RA, et al. Health Plan Members’’ Views About Disclosure of Medical Errors. Ann Intern Med Views About Disclosure of Medical Errors. Ann Intern Med 2004;140:409-4182004;140:409-418
9.9. Gallagher TH, Studdert D, Levinson W. Disclosing Harmful Gallagher TH, Studdert D, Levinson W. Disclosing Harmful Medical Errors to Patients. NEJM 2007;356:2713-0Medical Errors to Patients. NEJM 2007;356:2713-0
10.10. Brazeau C, Disclosing the Truth About a Medical Error. AAFP Brazeau C, Disclosing the Truth About a Medical Error. AAFP 1999;60:1999;60:

ReferencesReferences11.11. Lazare A. Apology in Medical Practice. JAMA 2006;296:1401-Lazare A. Apology in Medical Practice. JAMA 2006;296:1401-
1404140412.12. Malaty W, Crane S. How Might Acknowledging a Medical Error Malaty W, Crane S. How Might Acknowledging a Medical Error
Promote Patient Safety? Journal of Family Practice 55:775-780Promote Patient Safety? Journal of Family Practice 55:775-78013.13. Berlin L. Will Saying Berlin L. Will Saying ““II’’m Sorrym Sorry”” Prevent a Malpractice Lawsuit? Prevent a Malpractice Lawsuit?
ARJ 2006;187:10-15ARJ 2006;187:10-1514.14. Butterfield S. Apologize like a Pro.ACP Hospitalist Jan 2008:14-Butterfield S. Apologize like a Pro.ACP Hospitalist Jan 2008:14-
161615.15. Hobgood C, et al. Parental Preferences for Error Disclosure, Hobgood C, et al. Parental Preferences for Error Disclosure,
Reporting, and Legal Action After Medical Error in the Care of Reporting, and Legal Action After Medical Error in the Care of Their Children Their Children Pediatrics 2005; 116:1276 -1286 Pediatrics 2005; 116:1276 -1286

ReferencesReferences
16.16. Kraman SS, Hamm G. Risk management: extreme honesty may Kraman SS, Hamm G. Risk management: extreme honesty may be the best policy. Ann Intern Med 1999;131:963-967be the best policy. Ann Intern Med 1999;131:963-967
17.17. Clinton HR, Obama B. Making patient safety the centerpiece of Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med 2006;354:2205-2208medical liability reform. N Engl J Med 2006;354:2205-2208
18.18. http://www.callcopic.com/home/what-we-offer/coverages/medical-http://www.callcopic.com/home/what-we-offer/coverages/medical-professional-liability-insurance-co/physicians-medical-practices/professional-liability-insurance-co/physicians-medical-practices/special-programs/3rs-program/ Last accessed 2/28/2012. special-programs/3rs-program/ Last accessed 2/28/2012.