medical advisory secretariat cardiac hta: the ontario experience american heart association...
TRANSCRIPT
Medical Advisory Secretariat
Cardiac HTA: The Ontario Experience
American Heart AssociationWashington DC
May 2010
Leslie Levin MB, MD, FRCP (Lon), FRCPCProfessor of Medicine, University of Toronto
Head, Medical Advisory Secretariat, Ministry of Health and Long-Term Care
HTA in Canada & the United States
Medical Advisory Secretariat
2
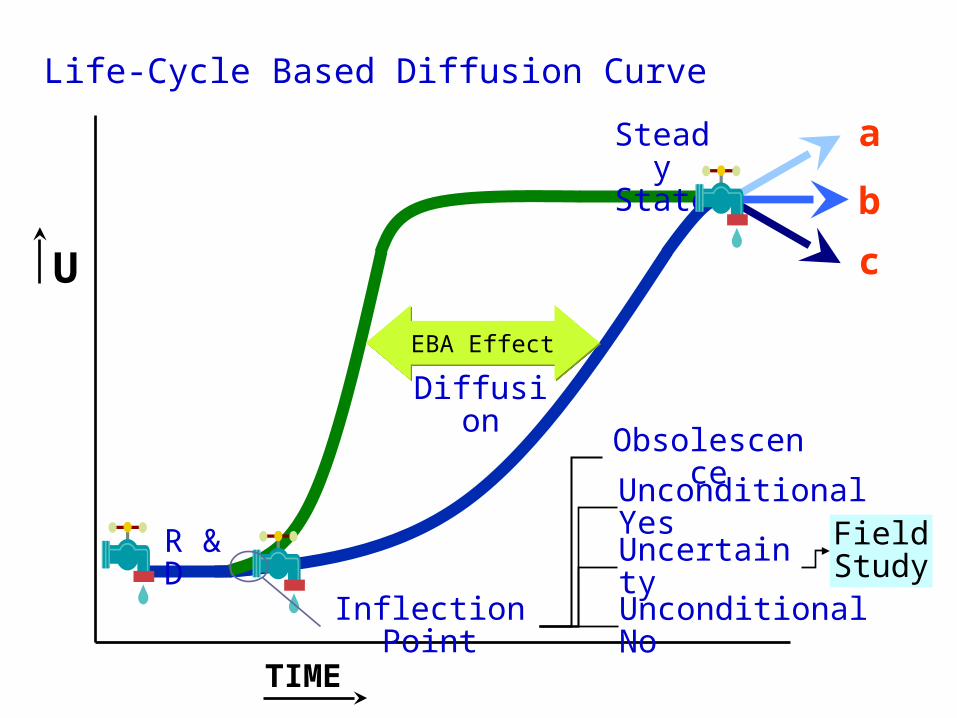
Life-Cycle Based Diffusion Curve
U
TIME
R & D
Diffusion
Steady State
Inflection Point
a
b
c
Unconditional Yes
Uncertainty
Unconditional No
Obsolescence
Field Study
EBA EffectEBA Effect
Medical Advisory Secretariat
3
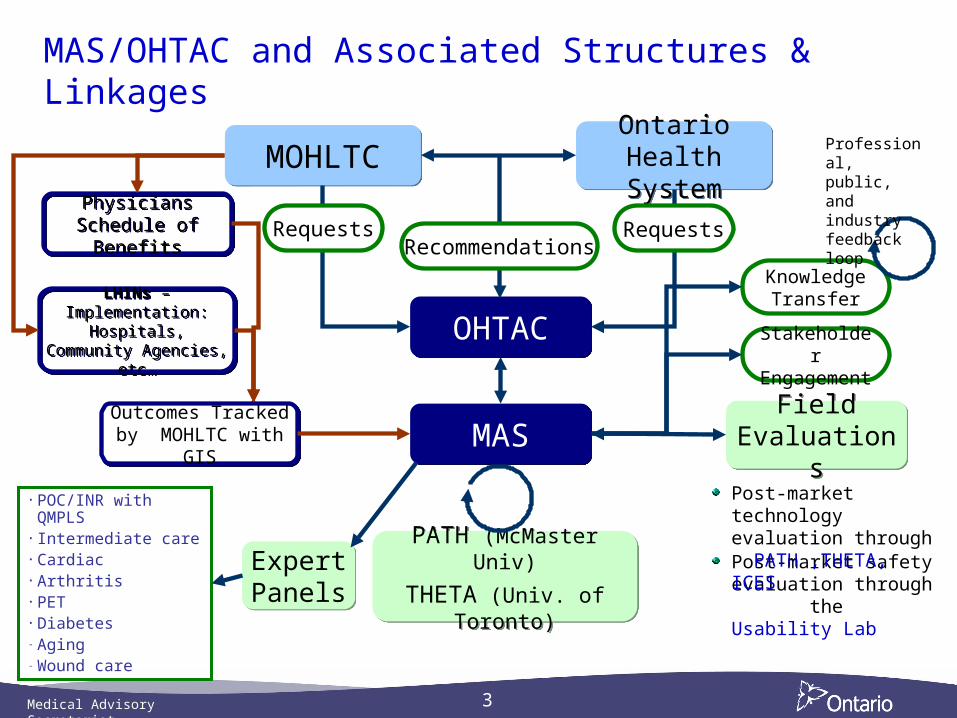
MAS/OHTAC and Associated Structures & Linkages
Outcomes Tracked by MOHLTC with GIS
Outcomes Tracked by MOHLTC with GIS MASMAS
OHTACOHTAC
MOHLTCMOHLTC Ontario Health System
Ontario Health System
Expert PanelsExpert Panels
PATH (McMaster Univ)
THETA (Univ. of Toronto)
PATH (McMaster Univ)
THETA (Univ. of Toronto)
Field Evaluations
Field Evaluations
Recommendations
PhysiciansSchedule of Benefits
PhysiciansSchedule of Benefits
LHINs – Implementation: Hospitals, Community
Agencies, etc…
LHINs – Implementation: Hospitals, Community
Agencies, etc…
Knowledge Transfer
Stakeholder Engagement
Professional, public, and industry feedback loop
Post-market safety evaluation through the Usability Lab
Post-market technology evaluation through PATH ,THETA, ICES
• POC/INR with QMPLS• Intermediate care• Cardiac • Arthritis• PET• Diabetes - Aging - Wound care
RequestsRequests
Medical Advisory Secretariat
4
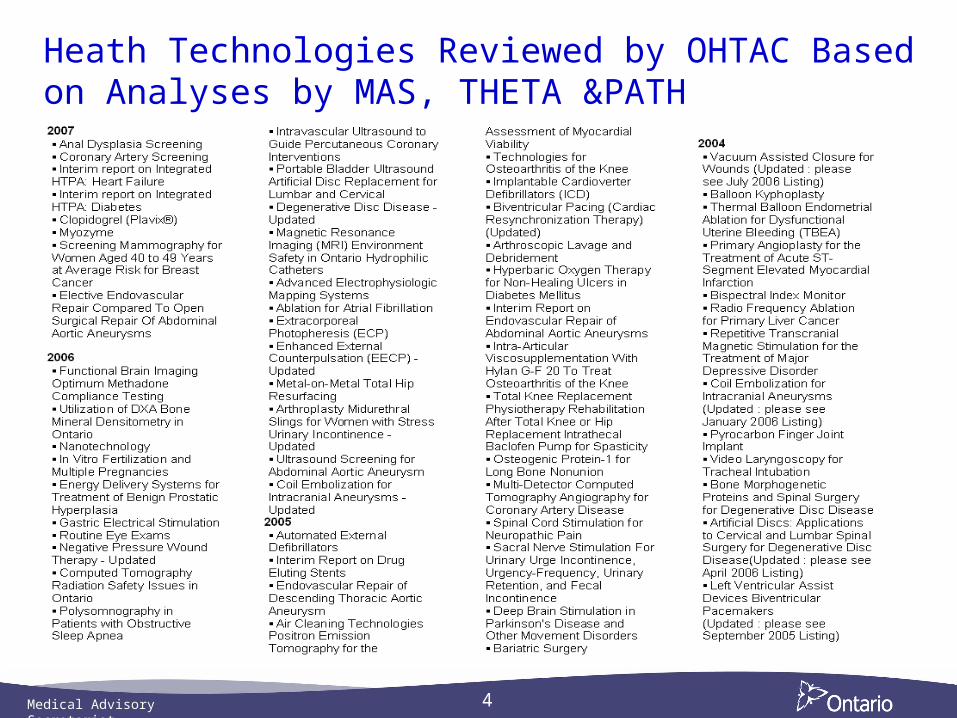
Heath Technologies Reviewed by OHTAC Based on Analyses by MAS, THETA &PATH
Medical Advisory Secretariat
5
Mega-Analysis and Policy Economic Modeling
Mega-analysis - disaggregation of technologies around a disease condition or health state and the re-aggregation for comparative effective analysis
Mega-analyses to date:Osteoarthritis of the knee MAS (2005)
Cardiac viability MAS (2005)
Aging in the community MAS/PATH (2008)
Colon cancer screening MAS/PATH (2008)
Diabetes MAS/PATH (2009)
Intermediate care MAS/THETA (2009)
Wound care prevention MAS/THETA (2008)
Cardiac diagnostic tests MAS/THETA (2010)
Robust micro-economic policy decision modelsOntario Diabetes Economic Model (PATH). (2006)
Ontario Cardiovascular Model (THETA). (2009)
Ontario Wound Prevention and Care Models (THETA). (2009)
Ontario Arthritis Model (PATH). (Commenced October 2009)
Ontario COPD Model (PATH). (Commenced April 2010)
Turn-around time ~ 6-8 months
Medical Advisory Secretariat
6
Field Evaluation Studies
Post-market assessment in the real world to improve decision making
Influences adoption by physicians who must be engaged
Remaining issues
Generalisability applies to most technologies including drugs
Broaden the scope since the payer absorbs the cost irrespectively?
Study designs needed that do not restrict access and can be conducted within short time
Medical Advisory Secretariat
7
Field Evaluations: Process Overview
Conducted by third party (PATH or THETA) who receive:
Core grant support from Ministry of Health (MOHLTC)
Additional funding for each field evaluation
Average funding for each evaluation is $600,000
Additional funding to cover costs of the technology
PATH/THETA responsible for study design, execution, collection and synthesis of data and reporting.
Work with key opinion leaders and Academic Health Science Centres
Average time to completion of most studies 3 years
Since 2003, 19 completed and 17 have resulted in policy decisions. Most published in peer-reviewed journals.
Medical Advisory Secretariat
8
Examples of Policy Driven by Evidence to be Presented
Drug Eluting Stents
Cardiac imaging for intermediate risk CAD
CT angiography
Medical Advisory Secretariat
9
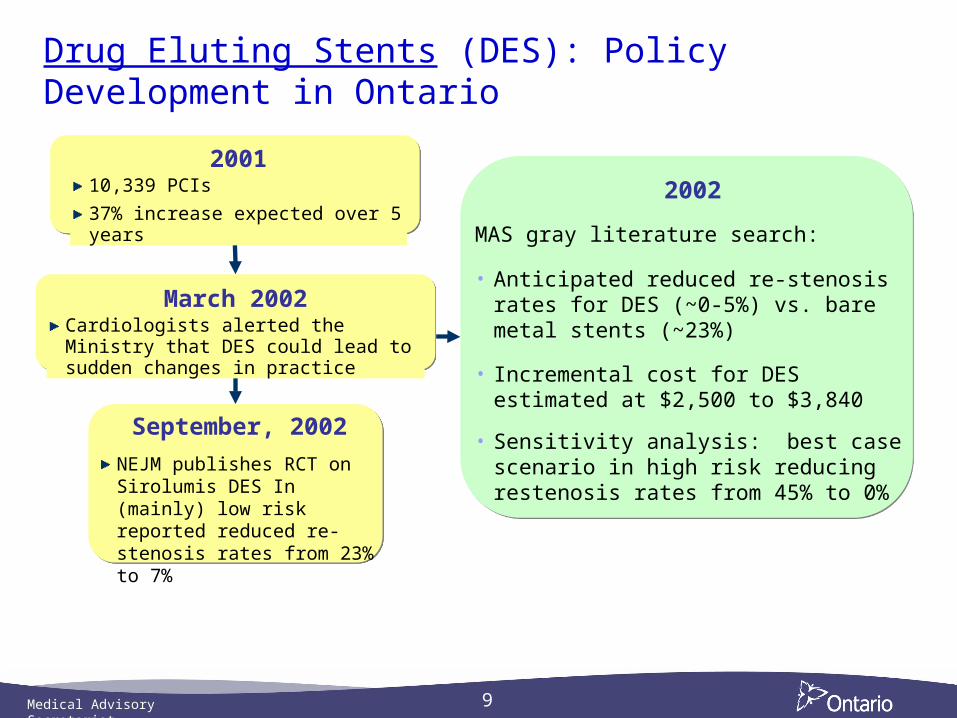
Drug Eluting Stents (DES): Policy Development in Ontario
200110,339 PCIs
37% increase expected over 5 years
September, 2002
NEJM publishes RCT on Sirolumis DES In (mainly) low risk reported reduced re-stenosis rates from 23% to 7%
2002
MAS gray literature search:
• Anticipated reduced re-stenosis rates for DES (~0-5%) vs. bare metal stents (~23%)
• Incremental cost for DES estimated at $2,500 to $3,840
• Sensitivity analysis: best case scenario in high risk reducing restenosis rates from 45% to 0%
March 2002Cardiologists alerted the Ministry that DES could lead to sudden changes in practice
Medical Advisory Secretariat
10
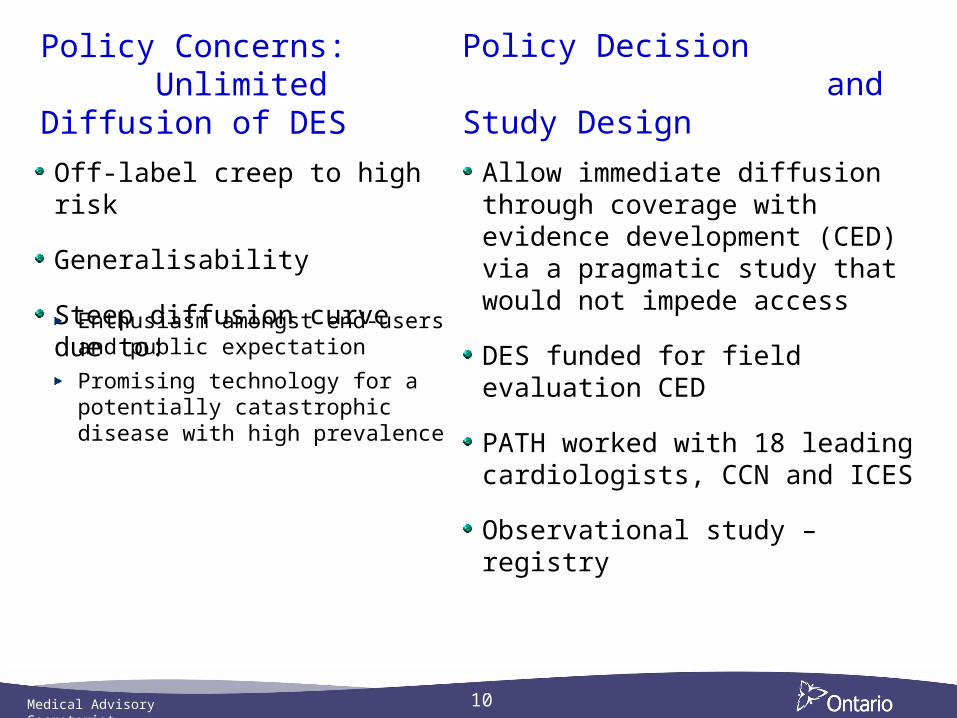
Policy Concerns: Unlimited Diffusion of DES
Off-label creep to high risk
Generalisability
Steep diffusion curve due to:
Policy Decision and Study Design
Enthusiasm amongst end-users and public expectation
Promising technology for a potentially catastrophic disease with high prevalence
Allow immediate diffusion through coverage with evidence development (CED) via a pragmatic study that would not impede access
DES funded for field evaluation CED
PATH worked with 18 leading cardiologists, CCN and ICES
Observational study – registry
Medical Advisory Secretariat
11
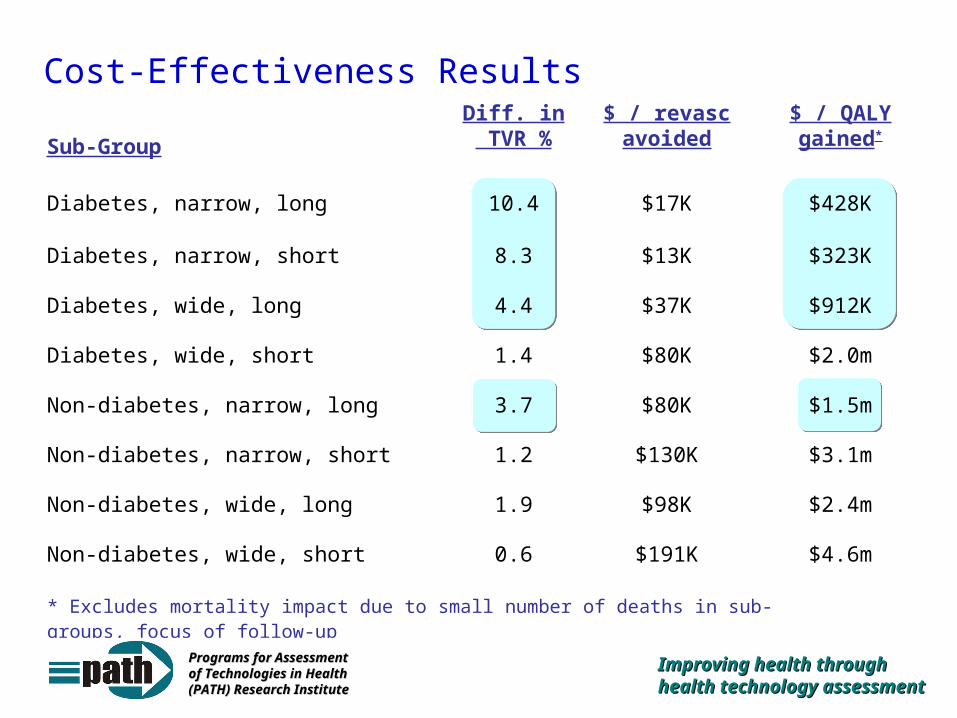
Cost-Effectiveness Results
Sub-Group
Diff. in TVR %
$ / revasc avoided
$ / QALY gained*
Diabetes, narrow, long 10.4 $17K $428K
Diabetes, narrow, short 8.3 $13K $323K
Diabetes, wide, long 4.4 $37K $912K
Diabetes, wide, short 1.4 $80K $2.0m
Non-diabetes, narrow, long 3.7 $80K $1.5m
Non-diabetes, narrow, short 1.2 $130K $3.1m
Non-diabetes, wide, long 1.9 $98K $2.4m
Non-diabetes, wide, short 0.6 $191K $4.6m
* Excludes mortality impact due to small number of deaths in sub-groups, focus of follow-up
Improving health through Improving health through health technology health technology assessmentassessment
Programs for Assessment Programs for Assessment of Technologies in Health of Technologies in Health (PATH) Research Institute(PATH) Research Institute
Medical Advisory Secretariat
12
DES in Ontario - End Product
Study published by Tu, JV et al, NEJM October 2007
35% conversion from bare-metal to DES v 90% in U.S.
Ongoing registry to measure long-term effects including safety
Medical Advisory Secretariat
13
Cardiac ImagingCardiac Imaging: Mega-Analysis of Technologies
Research Questions1. What is the diagnostic accuracy
compared to coronary angiography?
2. What is the clinical utility of these non-invasive cardiac tests?
Project Rationale
Use of non-invasive cardiac imaging technologies has risen rapidly
Uncertainty re- appropriate choice, sequence and frequency of tests
In July 2009, MAS was asked to undertake an EBA of effectiveness and cost-effectiveness of cardiac imaging for intermediate risk CAD patients
Technologies reviewed:a) SPECT
b) Stress ECHO without contrast
c) Stress ECHO with contrast agents
d) Cardiac MRI
e) CT Angiography
Medical Advisory Secretariat
14
Strategy for Cardiac Imaging Analysis
Technologies were reviewed separately but used consistent study criteria, populations, and outcome measures
Pooled estimates of Sensitivity and Specificity
Summary Receiver Operator Characteristic (SROC) Curves & AUC
Economic analysis – decision analytic models (THETA)
Diagnostic accuracy of the different technologies compared
Expert panel assisted in contextualizing the evidence
Medical Advisory Secretariat
15
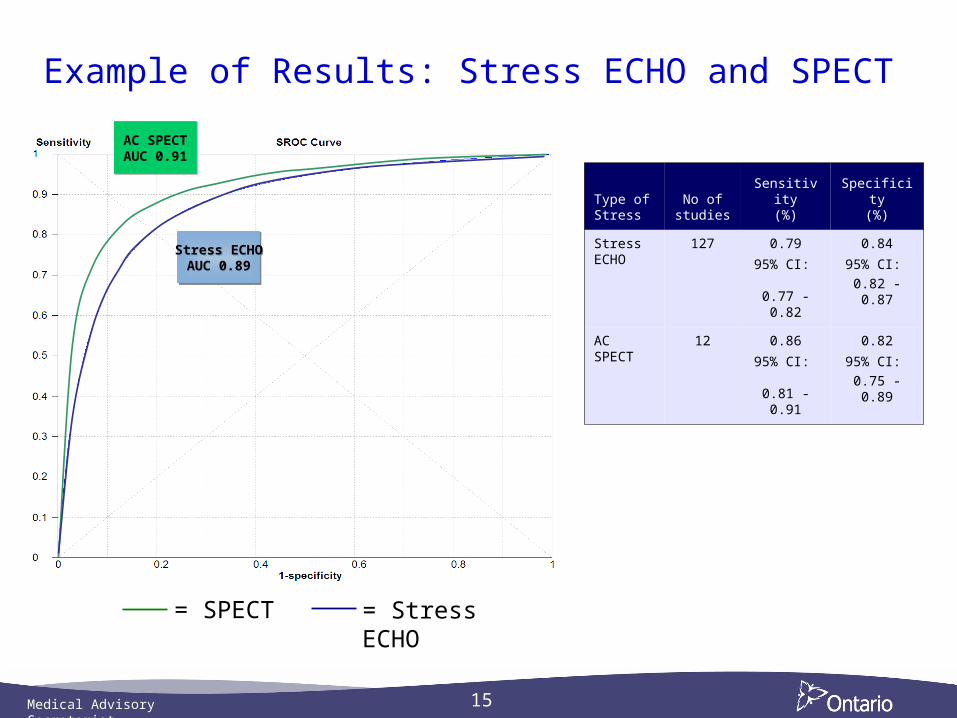
Example of Results: Stress ECHO and SPECT
= SPECT = Stress ECHO
Type of Stress
No of studies
Sensitivity(%)
Specificity(%)
Stress ECHO
127 0.79
95% CI: 0.77 -
0.82
0.84
95% CI:
0.82 - 0.87
AC SPECT
12 0.86
95% CI: 0.81 -
0.91
0.82
95% CI:
0.75 - 0.89
AC SPECTAUC 0.91
AC SPECTAUC 0.91
Stress ECHOAUC 0.89
Stress ECHOAUC 0.89
Medical Advisory Secretariat
16
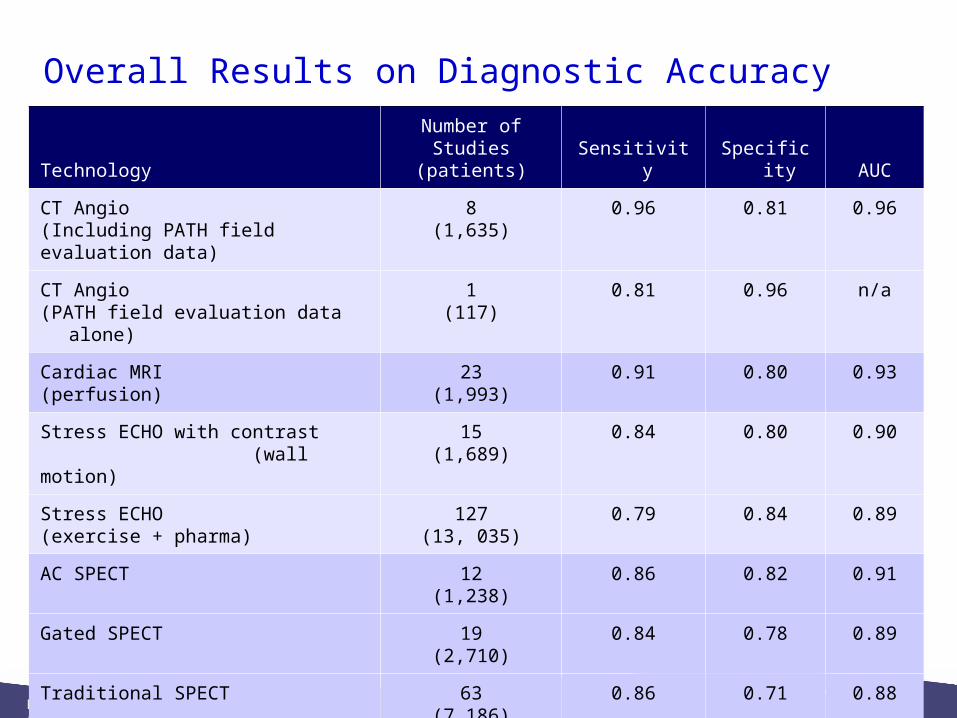
Overall Results on Diagnostic Accuracy
TechnologyNumber of Studies
(patients) Sensitivity Specificity AUC
CT Angio(Including PATH field evaluation data)
8(1,635)
0.96 0.81 0.96
CT Angio (PATH field evaluation data alone)
1(117)
0.81 0.96 n/a
Cardiac MRI(perfusion)
23(1,993)
0.91 0.80 0.93
Stress ECHO with contrast (wall motion)
15(1,689)
0.84 0.80 0.90
Stress ECHO (exercise + pharma)
127(13, 035)
0.79 0.84 0.89
AC SPECT 12(1,238)
0.86 0.82 0.91
Gated SPECT 19(2,710)
0.84 0.78 0.89
Traditional SPECT 63(7,186)
0.86 0.71 0.88
Medical Advisory Secretariat
17
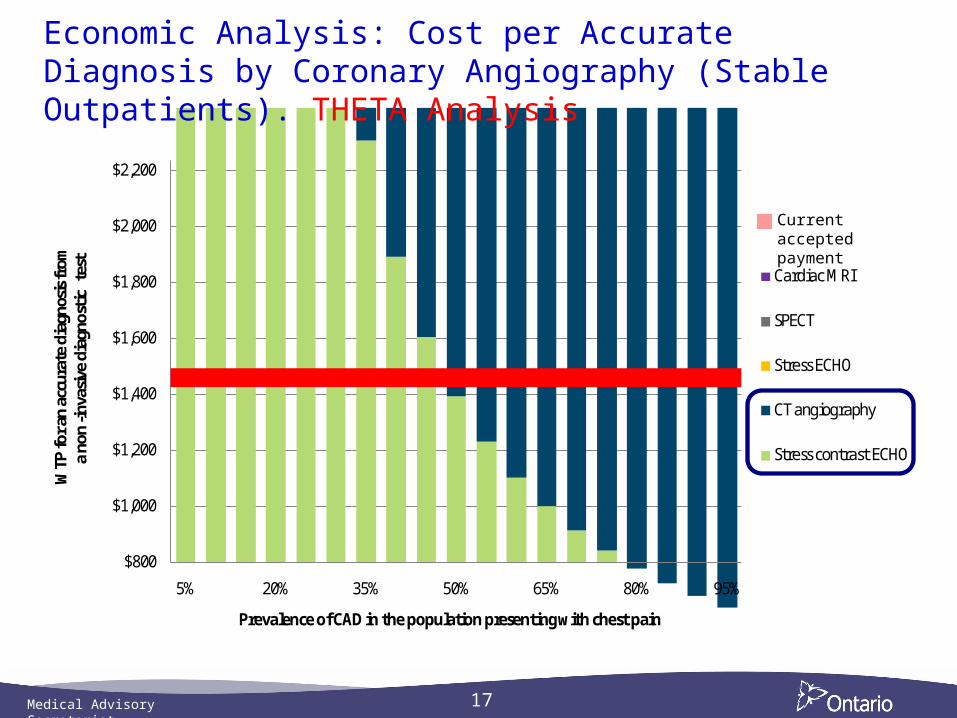
$800
$1,000
$1,200
$1,400
$1,600
$1,800
$2,000
$2,200
5% 20% 35% 50% 65% 80% 95%
Cardiac MRI
SPECT
Stress ECHO
CT angiography
Stress contrast ECHO
WTP
for a
n ac
cura
te d
iagn
osis
from
a no
n-in
vasiv
e di
agno
stic
test
Prevalence of CAD in the population presenting with chest pain
Current accepted payment
Economic Analysis: Cost per Accurate Diagnosis by Coronary Angiography (Stable Outpatients). THETA Analysis
Medical Advisory Secretariat
18
Conclusion From Cardiac Imaging Mega-Analysis
Either stress echo or SPECT are equally effective for predicting CAD using CA as a gold standard
Stress echo with contrast and CTCA are the most cost-effective strategies
If contrast stress echo and CTCA are not available, stress echo and SPECT are both cost-effective
QA issues regarding stress ECHO need to be addressed before considering implementation strategies
Medical Advisory Secretariat
19
64 Slice CTCA Study (OMCAS) Preliminary Results
Multicentre, multi-vendor, single-blind study
Four Academic Health Science Centres in Toronto and Ottawa
Study Coordination by PATH
Patients booked for CA received a CTCA within 10 days
Group 1 - Valvular heart disease, cardiomyopathy & congenital heart disease
Group 2 - CAD with intermediate probability CAD (10-90%)
Medical Advisory Secretariat
20
OMCAS: Methods
CTCA and CA read by two blinded readers at each site. Third consensus read when discrepancies occurred. All readers trained prior to study.
17 segment model of the coronary arteries and 4 point grading score used for evaluation of coronary stenosis:
normal
mild (<50%)
moderate (50-69%)
severe (≥70%)
For CTCA, plaque identified as soft, calcified or both
Obstructive CAD evaluated as stenosis ≥50% and ≥70%
Medical Advisory Secretariat
21
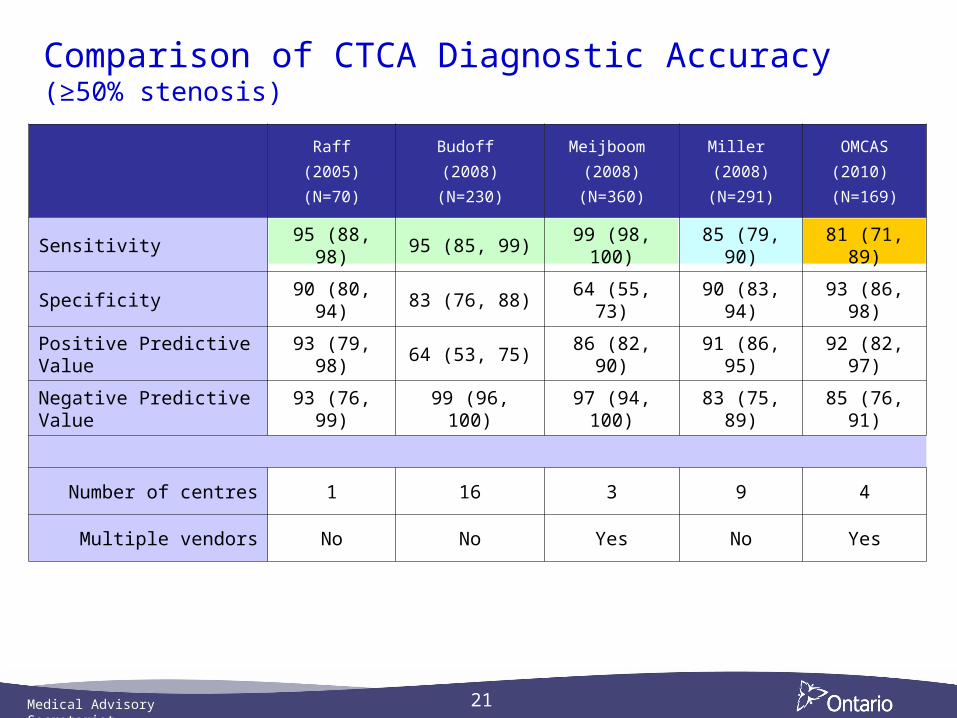
Comparison of CTCA Diagnostic Accuracy (≥50% stenosis)
Raff
(2005)
(N=70)
Budoff
(2008)
(N=230)
Meijboom
(2008)
(N=360)
Miller
(2008)
(N=291)
OMCAS
(2010)
(N=169)
Sensitivity 95 (88, 98) 95 (85, 99) 99 (98, 100) 85 (79, 90) 81 (71, 89)
Specificity 90 (80, 94) 83 (76, 88) 64 (55, 73) 90 (83, 94) 93 (86, 98)
Positive Predictive Value 93 (79, 98) 64 (53, 75) 86 (82, 90) 91 (86, 95) 92 (82, 97)
Negative Predictive Value 93 (76, 99) 99 (96, 100) 97 (94, 100) 83 (75, 89) 85 (76, 91)
Number of centres 1 16 3 9 4
Multiple vendors No No Yes No Yes
Medical Advisory Secretariat
22
Issues and Options Arising from OMCAS
If OMCAS accuracy data are used:stress contrast echo is the only cost-effective strategy for stable intermediate risk CAD patients
If contrast stress echo is not available, CTCA becomes the most cost-effective strategy
Possible Options:Limit insurability of CTCA to a few AHSCs until accuracy issue resolved
Do not insure CTCA because hospitals may substitute for CA (both are anatomic imaging) and >20% of CAD could be missed
Insure CTCA with an expectation that CA will be performed in patients with a negative CTCA – but many positives and negatives may then undergo CA.
OHTAC recommendation will await final results of OMCAS being reported June 2010
Medical Advisory Secretariat
Health Technology Diffusion - Examples
2010 OHTAC Annual Report
Medical Advisory Secretariat
24
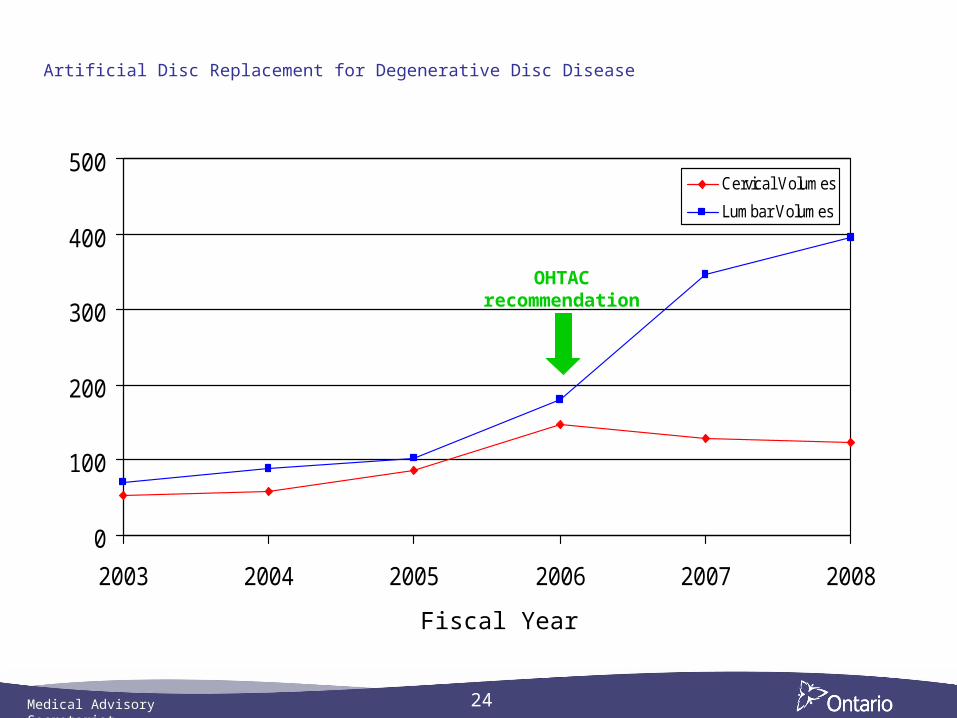
Artificial Disc Replacement for Degenerative Disc Disease
0
100
200
300
400
500
2003 2004 2005 2006 2007 2008
Cervical Volumes
Lumbar Volumes
Fiscal Year
OHTAC recommendation
Medical Advisory Secretariat
25
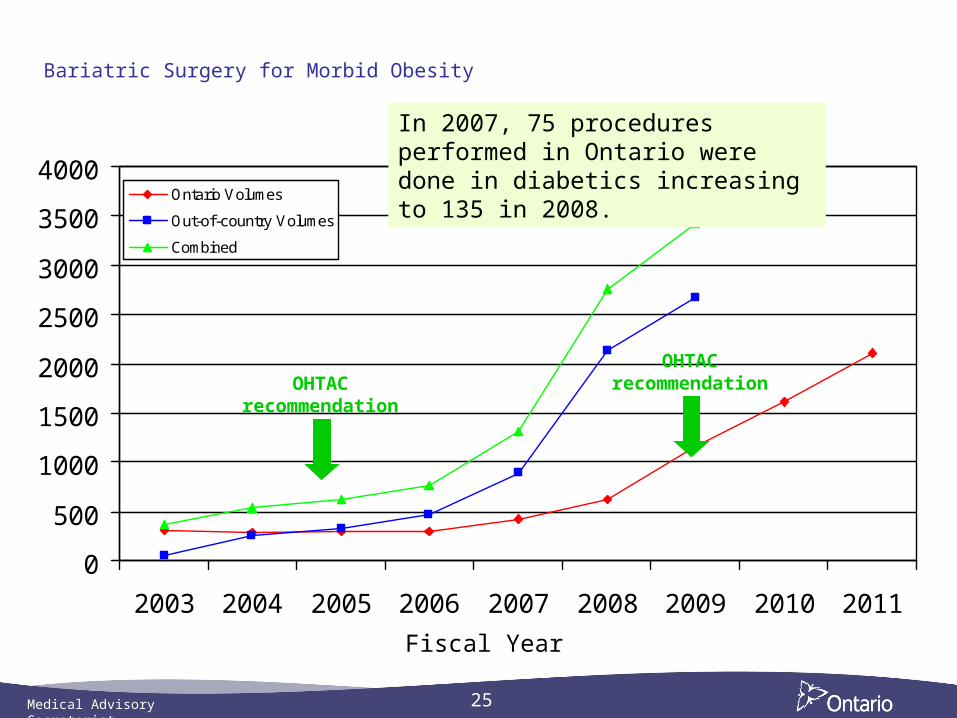
Bariatric Surgery for Morbid Obesity
0
500
1000
1500
2000
2500
3000
3500
4000
2003 2004 2005 2006 2007 2008 2009 2010 2011
Ontario Volumes
Out-of-country Volumes
Combined
Fiscal Year
In 2007, 75 procedures performed in Ontario were done in diabetics increasing to 135 in 2008.
OHTAC recommendation
OHTAC recommendation
Medical Advisory Secretariat
26
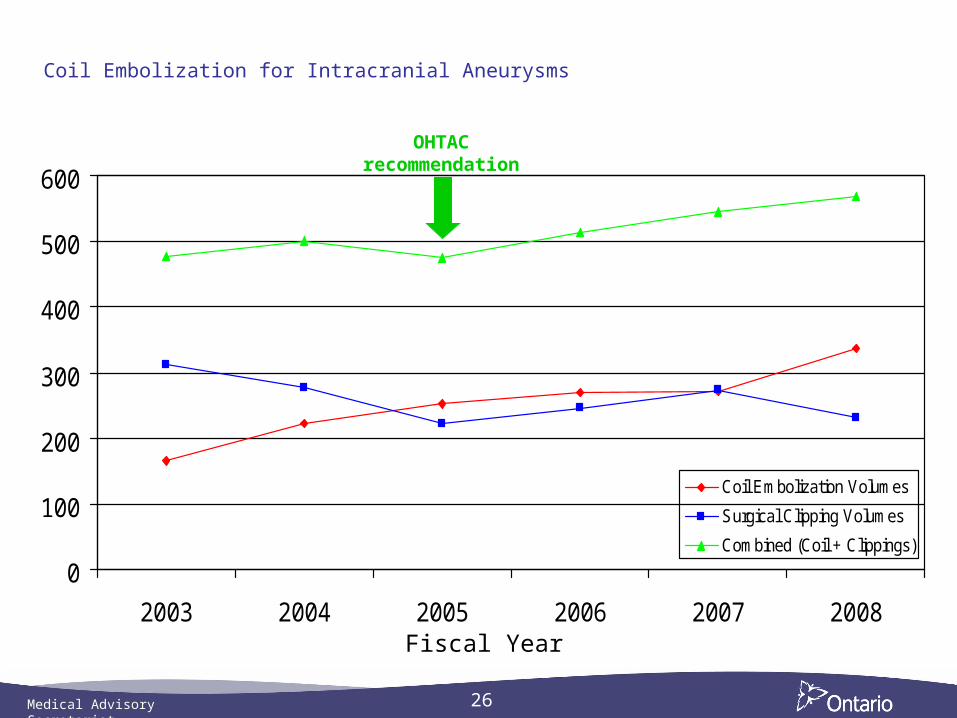
Coil Embolization for Intracranial Aneurysms
0
100
200
300
400
500
600
2003 2004 2005 2006 2007 2008
Coil Embolization Volumes
Surgical Clipping Volumes
Combined (Coil + Clippings)
Fiscal Year
OHTAC recommendation
Medical Advisory Secretariat
27
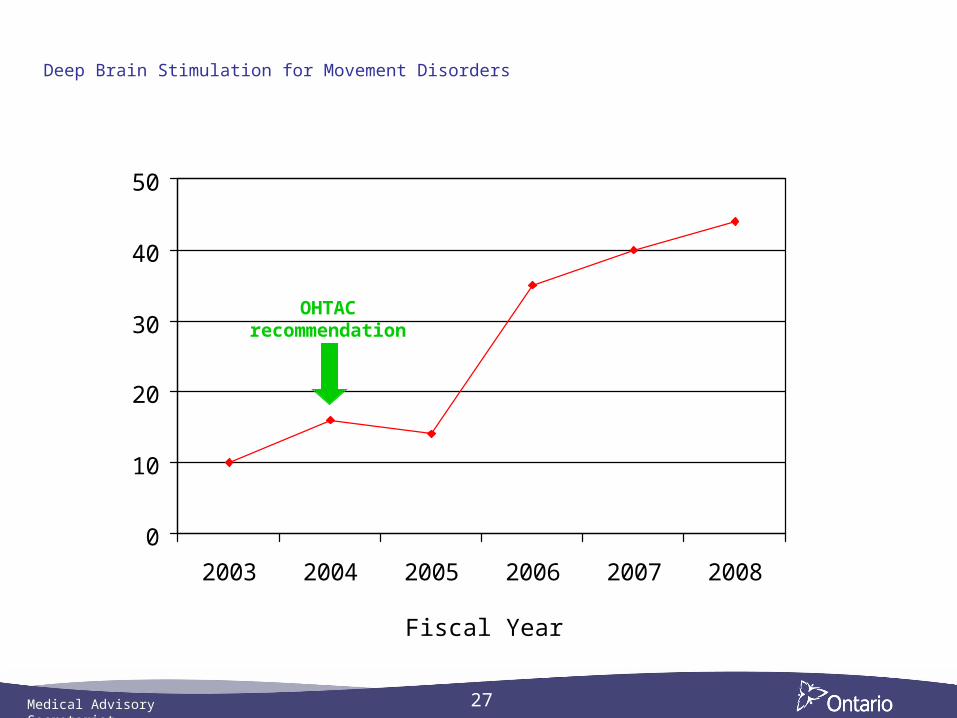
Deep Brain Stimulation for Movement Disorders
0
10
20
30
40
50
2003 2004 2005 2006 2007 2008
Fiscal Year
OHTAC recommendation
Medical Advisory Secretariat
28
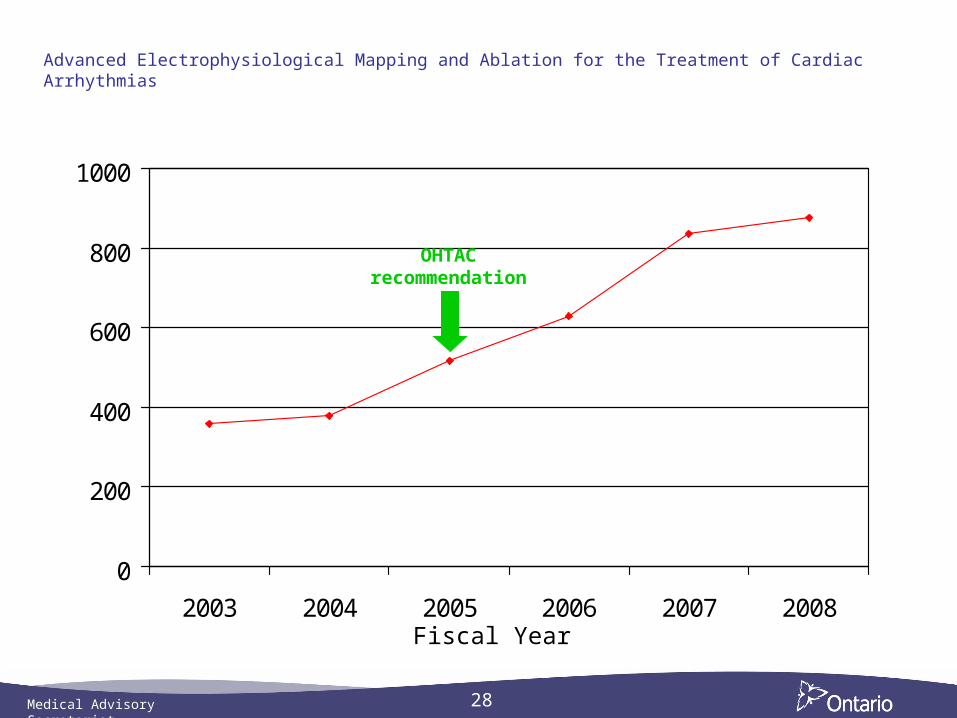
Advanced Electrophysiological Mapping and Ablation for the Treatment of Cardiac Arrhythmias
0
200
400
600
800
1000
2003 2004 2005 2006 2007 2008Fiscal Year
OHTAC recommendation
Medical Advisory Secretariat
29
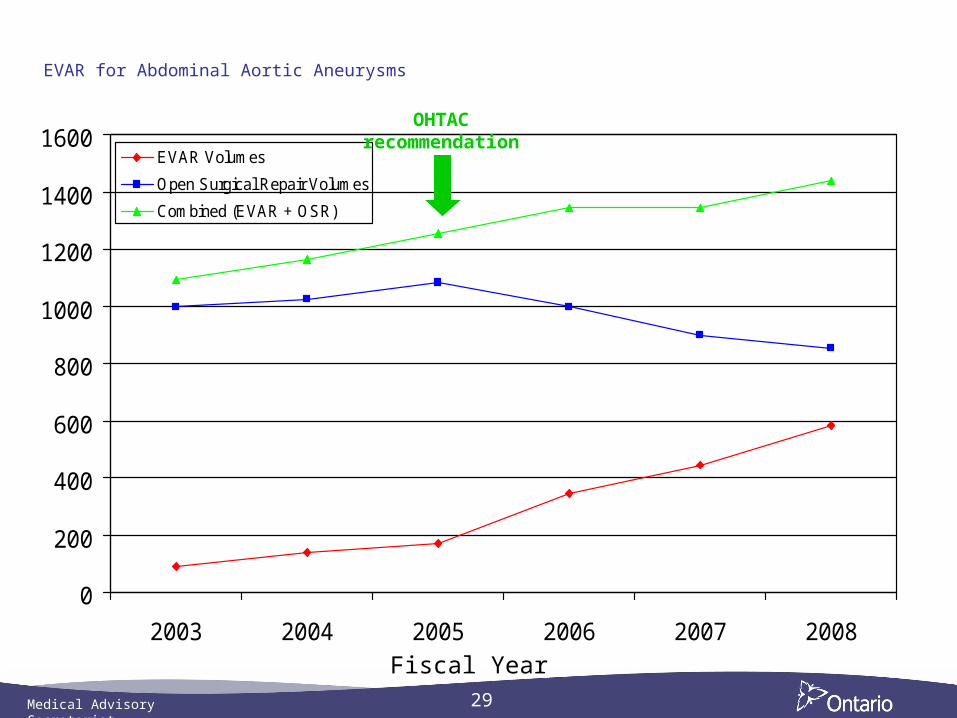
EVAR for Abdominal Aortic Aneurysms
0
200
400
600
800
1000
1200
1400
1600
2003 2004 2005 2006 2007 2008
EVAR Volumes
Open Surgical Repair Volumes
Combined (EVAR + OSR)
Fiscal Year
OHTAC recommendation
Medical Advisory Secretariat
30
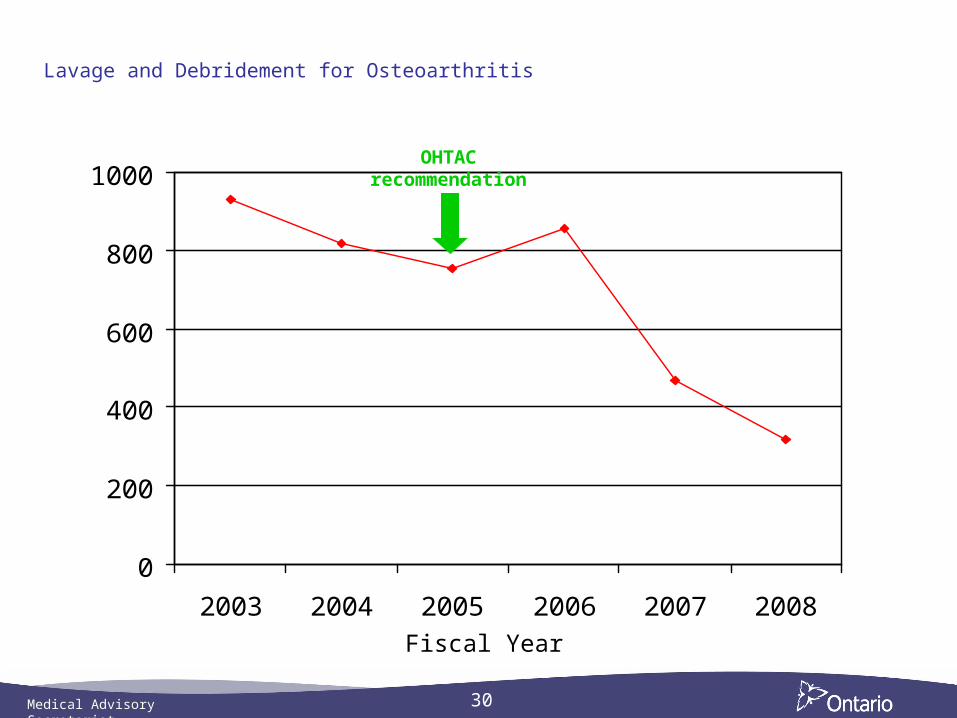
Lavage and Debridement for Osteoarthritis
0
200
400
600
800
1000
2003 2004 2005 2006 2007 2008
Fiscal Year
OHTAC recommendation
Medical Advisory Secretariat
31
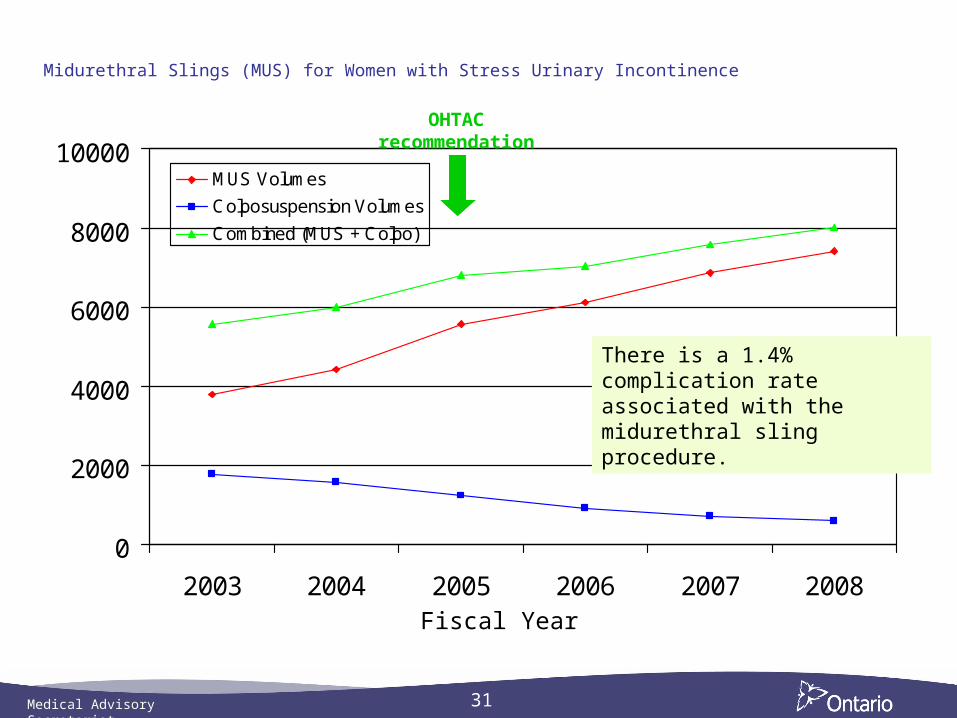
Midurethral Slings (MUS) for Women with Stress Urinary Incontinence
0
2000
4000
6000
8000
10000
2003 2004 2005 2006 2007 2008
MUS Volumes
Colposuspension Volumes
Combined (MUS + Colpo)
Fiscal Year
There is a 1.4% complication rate associated with the midurethral sling procedure.
OHTAC recommendation
Medical Advisory Secretariat
32
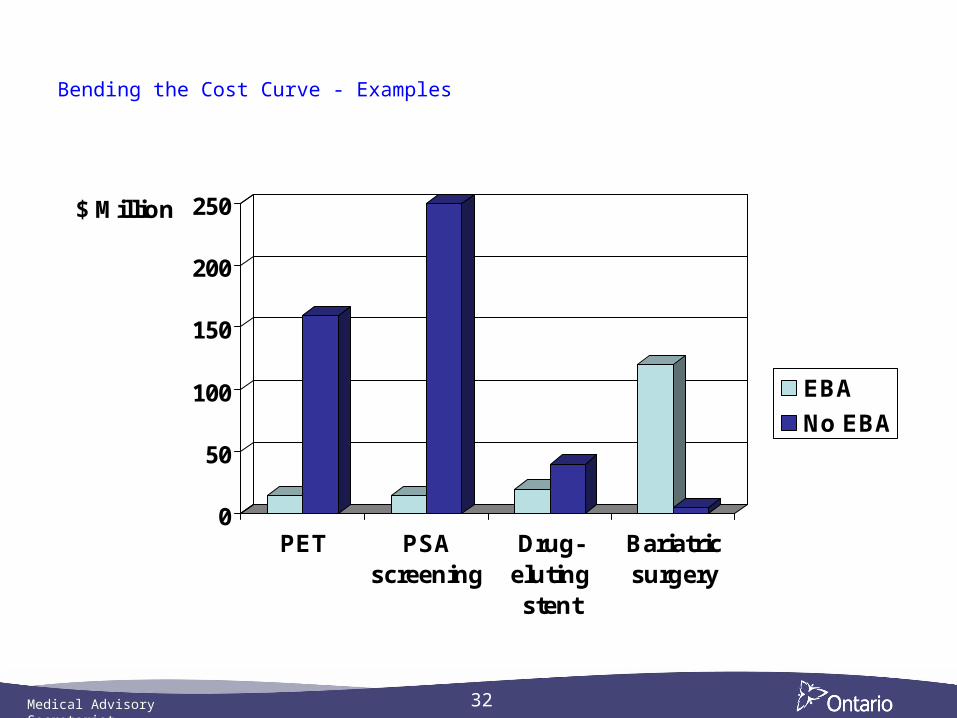
Bending the Cost Curve - Examples
0
50
100
150
200
250$ Million
PET PSAscreening
Drug-elutingstent
Bariatricsurgery
EBA
No EBA
Medical Advisory Secretariat
33
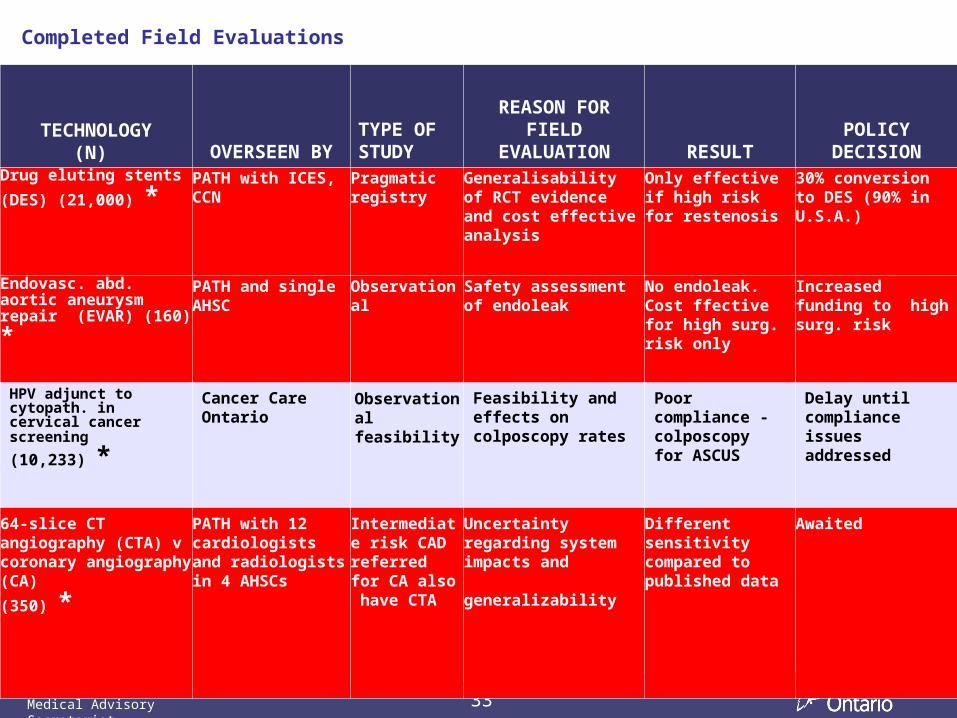
Completed Field Evaluations
TECHNOLOGY(N) OVERSEEN BY
TYPE OF STUDY
REASON FOR FIELD
EVALUATION RESULTPOLICY
DECISIONDrug eluting stents
(DES) (21,000) *PATH with ICES, CCN
Pragmatic registry
Generalisability of RCT evidence and cost effective analysis
Only effective if high risk for restenosis
30% conversion to DES (90% in U.S.A.)
Endovasc. abd. aortic aneurysm repair (EVAR)
(160) *
PATH and single AHSC
Observational Safety assessment of endoleak
No endoleak. Cost ffective for high surg. risk only
Increased funding to high surg. risk
HPV adjunct to cytopath. in cervical cancer screening
(10,233) *
Cancer Care Ontario
Observational feasibility
Feasibility and effects on colposcopy rates
Poor compliance -colposcopy for ASCUS
Delay until compliance issues addressed
64-slice CT angiography (CTA) v coronary angiography (CA)
(350) *
PATH with 12 cardiologists and radiologistsin 4 AHSCs
Intermediate risk CAD referred for CA also have CTA
Uncertainty regarding system impacts and generalizability
Different sensitivity compared to published data
Awaited
Medical Advisory Secretariat
34
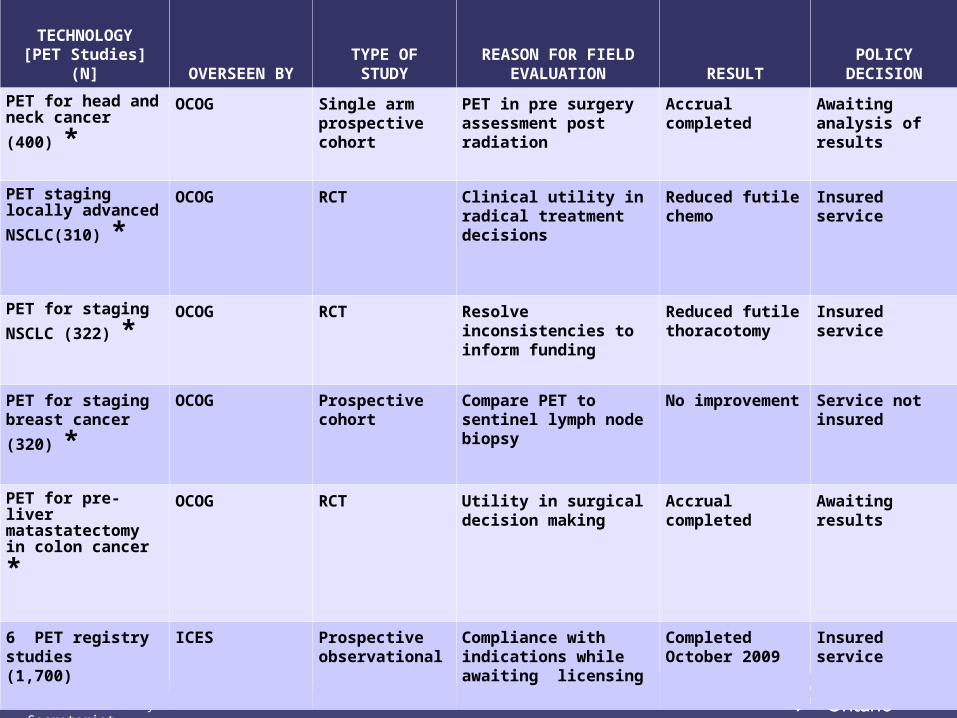
TECHNOLOGY[PET Studies]
(N] OVERSEEN BYTYPE OF STUDY
REASON FOR FIELD EVALUATION RESULT
POLICY DECISION
PET for head and
neck cancer (400) *OCOG Single arm
prospective cohort
PET in pre surgery assessment post radiation
Accrual completed
Awaiting analysis of results
PET staging locally advanced
NSCLC(310) *
OCOG RCT Clinical utility in radical treatment decisions
Reduced futile chemo
Insured service
PET for staging
NSCLC (322) *OCOG RCT Resolve inconsistencies
to inform funding Reduced futile thoracotomy
Insured service
PET for staging breast cancer
(320) *
OCOG Prospective cohort
Compare PET to sentinel lymph node biopsy
No improvement Service not insured
PET for pre-liver matastatectomy in
colon cancer *
OCOG RCT Utility in surgical decision making
Accrual completed
Awaiting results
6 PET registry studies (1,700)
ICES Prospective observational
Compliance with indications while awaiting licensing
Completed October 2009
Insured service
Medical Advisory Secretariat
35
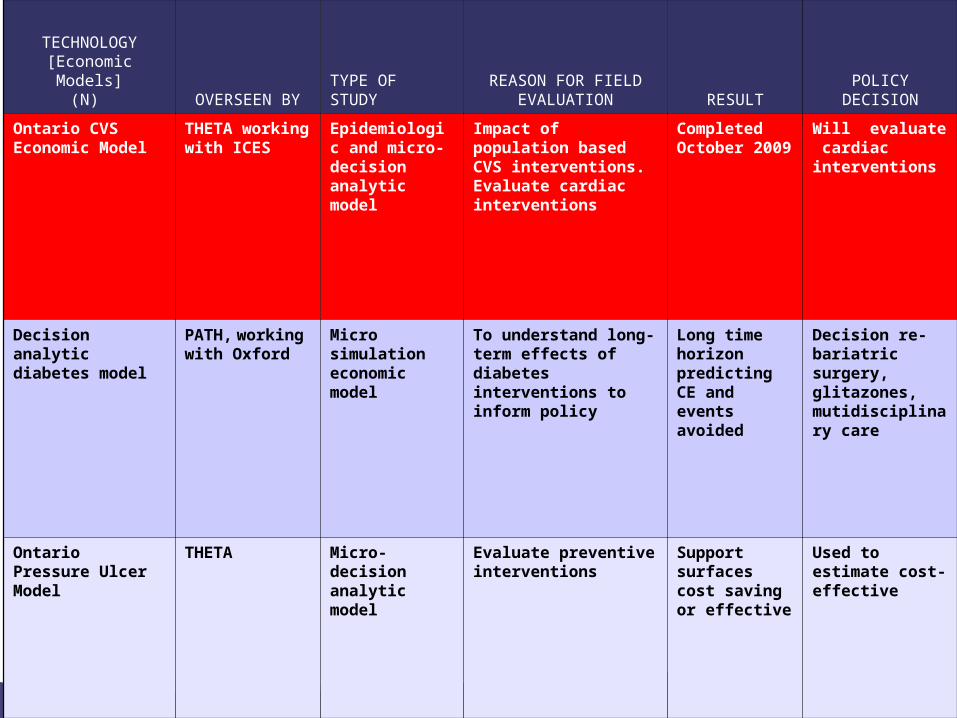
TECHNOLOGY[Economic Models]
(N) OVERSEEN BYTYPE OF STUDY
REASON FOR FIELD EVALUATION RESULT
POLICY DECISION
Ontario CVS Economic Model
THETA working with ICES
Epidemiologic and micro-decision analytic model
Impact of population based CVS interventions. Evaluate cardiac interventions
Completed October 2009
Will evaluate cardiac interventions
Decision analytic diabetes model
PATH, working with Oxford
Micro simulation economic model
To understand long-term effects of diabetes interventions to inform policy
Long time horizon predicting CE and events avoided
Decision re- bariatric surgery, glitazones, mutidisciplinary care
Ontario Pressure Ulcer Model
THETA Micro- decision analytic model
Evaluate preventive interventions
Support surfaces cost saving or effective
Used to estimate cost-effective
Medical Advisory Secretariat
36
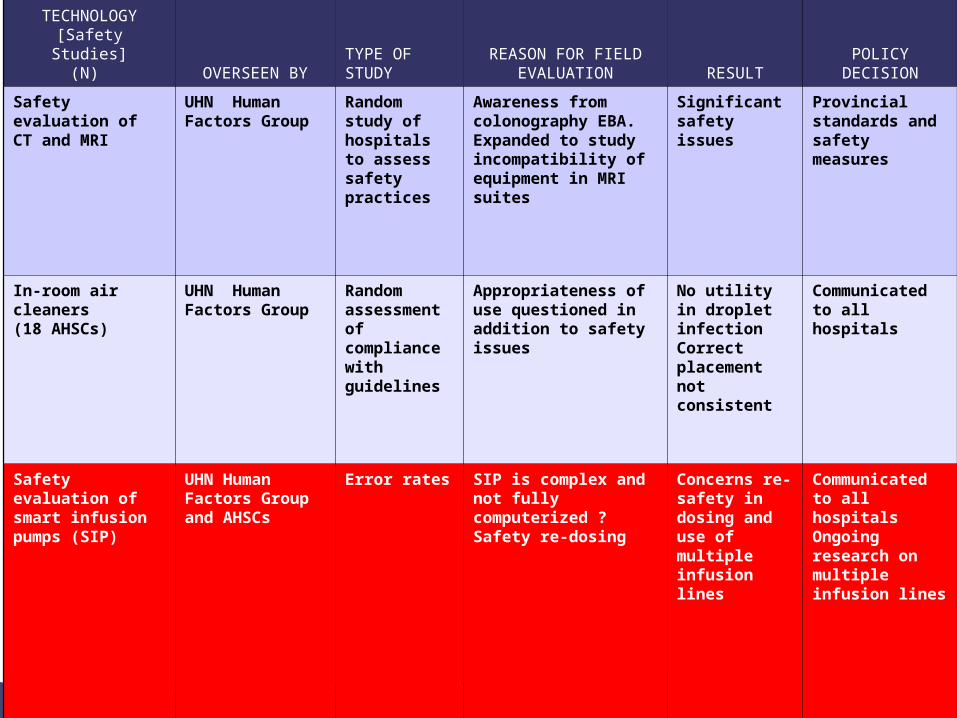
TECHNOLOGY[Safety Studies]
(N) OVERSEEN BYTYPE OF STUDY
REASON FOR FIELD EVALUATION RESULT
POLICY DECISION
Safety evaluation of CT and MRI
UHN Human Factors Group
Random study of hospitals to assess safety practices
Awareness from colonography EBA. Expanded to study incompatibility of equipment in MRI suites
Significant safety issues
Provincial standards and safety measures
In-room air cleaners(18 AHSCs)
UHN Human Factors Group
Random assessment of compliance with guidelines
Appropriateness of use questioned in addition to safety issues
No utility in droplet infectionCorrect placement not consistent
Communicated to all hospitals
Safety evaluation of smart infusion pumps (SIP)
UHN Human Factors Group and AHSCs
Error rates SIP is complex and not fully computerized ? Safety re-dosing
Concerns re-safety in dosing and use of multiple infusion lines
Communicated to all hospitals Ongoing research on multiple infusion lines
Medical Advisory Secretariat
37
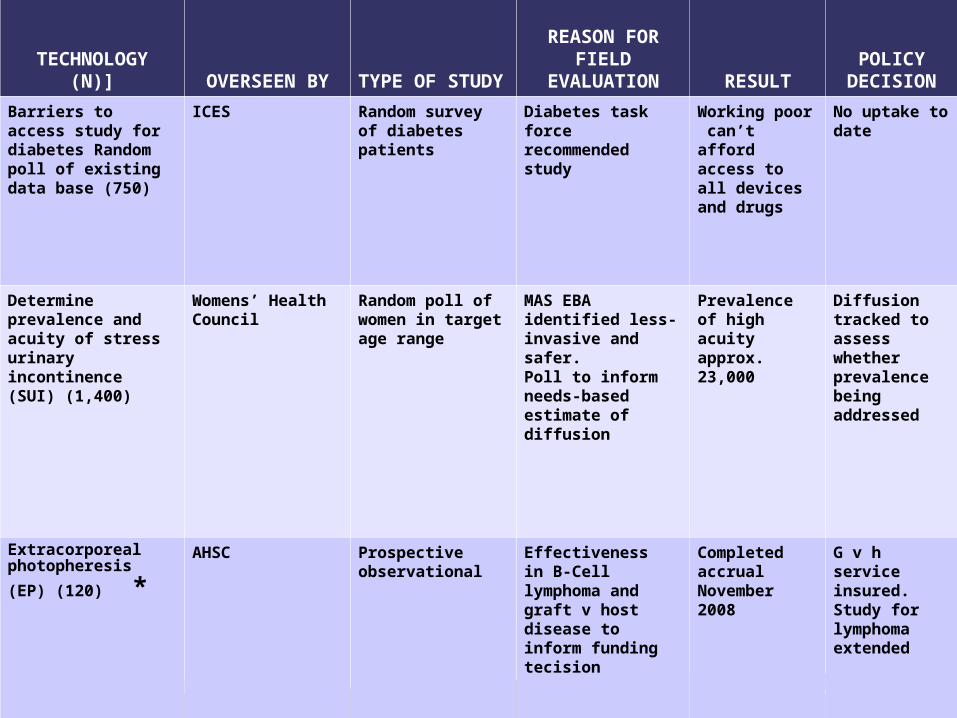
TECHNOLOGY(N)] OVERSEEN BY TYPE OF STUDY
REASON FOR FIELD
EVALUATION RESULTPOLICY
DECISION
Barriers to access study for diabetes Random poll of existing data base (750)
ICES Random survey of diabetes patients
Diabetes task force recommended study
Working poor can’t afford access to all devices and drugs
No uptake to date
Determine prevalence and acuity of stress urinary incontinence (SUI) (1,400)
Womens’ Health Council
Random poll of women in target age range
MAS EBA identified less-invasive and safer. Poll to inform needs-based estimate of diffusion
Prevalence of high acuity approx.23,000
Diffusion tracked to assess whether prevalence being addressed
Extracorporeal photopheresis (EP)
(120) *
AHSC Prospective observational
Effectiveness in B-Cell lymphoma and graft v host disease to inform funding tecision
Completed accrual November 2008
G v h service insured. Study for lymphoma extended