mediastinal masses in children with hodgkin's disease. an analysis of the children's...
TRANSCRIPT

2755
Mediastinal Masses in Children With Hodgkin’s Disease An Analysis of the Children’s Hospital of Philadelphia and the Hospital of the University of Pennsylvania Experience
Amit Muity, MD,*,$,§ Joel W. Goldwein, MD,**$ Beverly Lunge, Molt*$ and Giulio J. D‘Angio, MD*,$
From 1970 to 1988,121 patients younger than 18 years of age who had newly diagnosed Hodgkin’s disease were treated at the Children’s Hospital of Philadelphia (CHOP) and the Hospital of the University of Pennsylvania (HUP), Philadelphia, Pennsylvania. Fifty-five of 79 chil- dren with mediastinal masses (MM) had pretreatment chest radiographs from which a mediastinal mass ratio (MMR) could be calculated. Within a range of MMR val- ues, 0.25 was the best prognosticator for event-free sur- vival (EFS) for all patients. In those treated with radia- tion therapy (RT) alone, the intrathoracic relapse rate was zero of five patients with small MM (MMR less than 0.25) versus five of eight patients with large MM (P = 0.09). For combined-modality therapy (CMT), there were intrathoracic relapses in zero of four patients with small MM versus 5 of 32 patients with large MM (P = 0.8). For CMT, the intrathoracic relapse rates for those receiv- ing more than 3500 cGy versus less than 2500 cGy were 0 of 4 patients and 5 of 27 patients, respectively (P = 0.8). The intrathoracic relapse rate in children with large MM was significantly lower for CMT than for RT (5 of 32 pa- tients versus 5 of 8 patients) (P = 0.02). The authors con- cluded that in pediatric Hodgkin’s disease, a MM with a MMR greater than or equal to 0.25 may be associated with poor intrathoracic control after RT alone. Despite this, children with large MM treated with RT alone had an excellent overall survival rate. Cancer 1992; 69:2755- 2760.
Presented at the 75th Annual Meeting of the American Radium Society, Montreal, Canada, May 4-8, 1991.
From the *Department of Radiation Oncology, Hospital of the University of Pennsylvania, the tDivision of Pediatric Oncology, Children’s Hospital of Philadelphia, and the $University of Pennsyl- vania School of Medicine, Philadelphia, Pennsylvania.
5 Recipient of an American Cancer Society Clinical Fellowship during the course of this study.
Address for reprints: Amit Maity, MD, Department of Radiation Oncology, Donner 2, Hospital of the University of Pennsylvania, 3400 Spruce Street, Philadelphia, PA 19104.
Accepted for publication February 27, 1992.
Large mediastinal adenopathy is a poor prognostic fac- tor for relapse-free survival in adults treated for early stage Hodgkin’s disease with radiation therapy (RT) alone.’-3 Few series have examined this issue specifi- cally in children4 or in advanced-stage disease treated with combined-modality therapy (CMT).5 Of particular interest in pediatric Hodgkin’s disease is whether low- dose radiation (2000 to 2500 cGy) in conjunction with chemotherapy6-” is adequate to control bulky medias- tinal disease. Such treatment is increasingly being used to avoid long-term skeletal and soft tissue hypopla- sia.’*-14 In this study, the authors investigated the signif- icance of mediastinal adenopathy in children of all stages treated at the Children’s Hospital of Philadelphia (CHOP) and the Hospital of the University of Pennsyl- vania (HUP), Philadelphia, Pennsylvania.
Materials and Methods
From 1970 to 1988,139 patients younger than 18 years of age who had newly diagnosed Hodgkin’s disease were treated at CHOP. RT, if part of the treatment, was usually administered at HUP. Eighteen children re- ceived RT at other facilities and were excluded from this analysis.
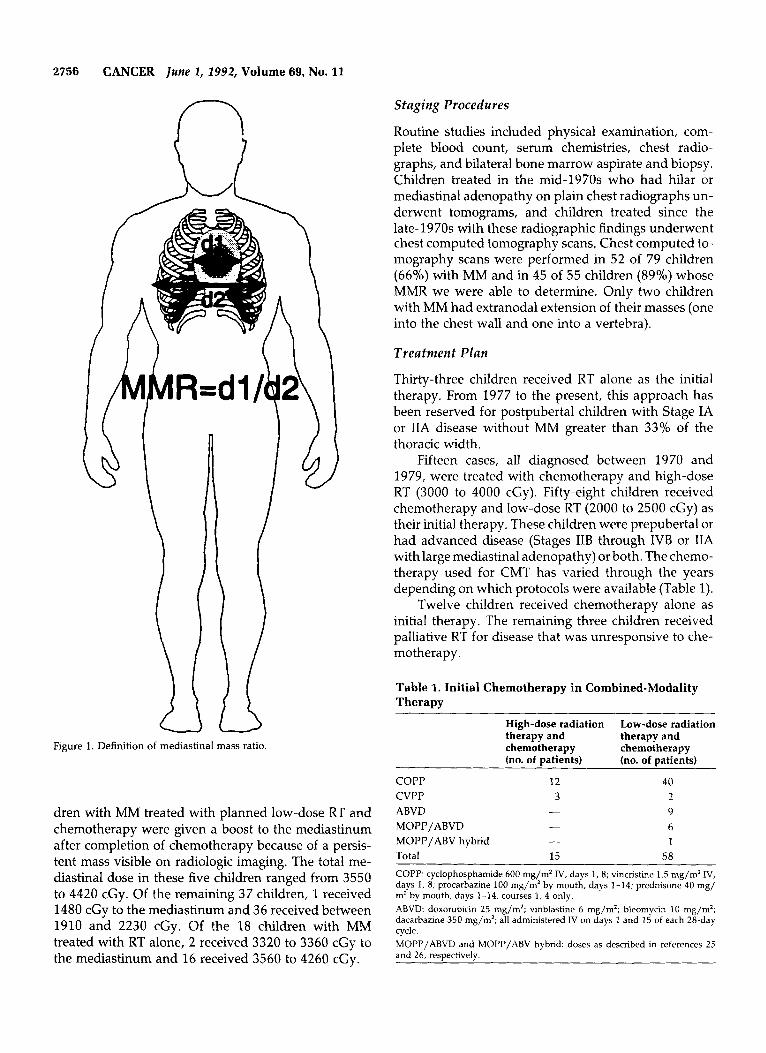
Seventy-nine of the 121 children (65%) had me- diastinal masses (MM). Of these, we were able to obtain the pretreatment upright posterior-anterior chest radio- graphs of 55 patients. The mediastinal mass ratio (MMR) was determined from these radiographs. The MMR was defined as the maximum width of the mass (excluding the hila) divided by the maximum intratho- racic width (Fig. 1). Most of the children whose chest radiographs were lost had been treated in the 1970s.
The dose to the mediastinum was calculated from dosimetric information in the RT charts. Five of 42 chil-
2756 CANCER Iune 2, 2992, Volume 69, No. 11
n
Figure 1. Definition of mediastinal mass ratio
dren with MM treated with planned low-dose RT and chemotherapy were given a boost to the mediastinum after completion of chemotherapy because of a persis- tent mass visible on radiologic imaging. The total me- diastinal dose in these five children ranged from 3550 to 4420 cGy. Of the remaining 37 children, 1 received 1480 cGy to the mediastinum and 36 received between 1910 and 2230 cGy. Of the 18 children with MM treated with RT alone, 2 received 3320 to 3360 cGy to the mediastinum and 16 received 3560 to 4260 cGy.
Staging Procedures
Routine studies included physical examination, com- plete blood count, serum chemistries, chest radio- graphs, and bilateral bone marrow aspirate and biopsy. Children treated in the mid-1970s who had hilar or mediastinal adenopathy on plain chest radiographs un- derwent tomograms, and children treated since the late-1970s with these radiographic findings underwent chest computed tomography scans, Chest computed to- mography scans were performed in 52 of 79 children (66%) with MM and in 45 of 55 children (89%) whose MMR we were able to determine. Only two children with MM had extranodal extension of their masses (one into the chest wall and one into a vertebra).
Treatment Plan
Thirty-three children received RT alone as the initial therapy. From 1977 to the present, this approach has been reserved for postpubertal children with Stage IA or IIA disease without MM greater than 33% of the thoracic width.
Fifteen cases, all diagnosed between 1970 and 1979, were treated with chemotherapy and high-dose RT (3000 to 4000 cGy). Fifty-eight children received chemotherapy and low-dose RT (2000 to 2500 cGy) as their initial therapy. These children were prepubertal or had advanced disease (Stages IIB through IVB or IIA with large mediastinal adenopathy) or both. The chemo- therapy used for CMT has varied through the years depending on which protocols were available (Table 1).
Twelve children received chemotherapy alone as initial therapy. The remaining three children received palliative RT for disease that was unresponsive to che- motherapy.
Table 1. Initial Chemotherapy in Combined-Modality Therapy
High-dose radiation Low-dose radiation therapy and therapy and chemotherapy chemotherapy (no. of patients) (no. of patients)
COPP 12 40 CVPP 3 2
9 ABVD - 6 MOPP/ABVD - 1 MOPP/ABV hybrid -
Total 15 58 COPP: cyclophosphamide 600 mg/m2 IV, days 1,8; vincristine 1.5 mg/m’ IV, days 1, 8; procarbazine 100 mg/m’ by mouth, days 1-14; prednisone 40 mg/ m2 by mouth, days 1-14, courses 1, 4 only. ABVD: doxorubicin 25 mg/m*; vinblastine 6 mg/m2; bleomycin 10 mg/m2; dacarbazine 350 mg/m2; all administered IV on days 1 and 15 of each 28-day cycle. MOPP/ABVD and MOPP/ABV hybrid: doses as described in references 25 and 26, respectively.

Mediastinal Masses in Pediatric Hodgkin's Disease/Maity et al.
U M 0 4 - E R
0 3. F
c 2~ H I L D 1 - R E
0 -
2757
All patients who received RT received 150 to 200 cGy per day, 5 days a week. Seventeen children, all treated before 1976, received RT to anterior fields every other day, alternating with posterior fields. Since then, equally weighted anterior and posterior fields have been used daily. Mantle and paraaortic fields were treated with a 6-MeV linear accelerator. Additional de- tails regarding therapy are published elsewhere."
Statistical Analysis
Survival and event-free survival (EFS) were calculated actuarially from the date of diagnosis using the product limit method of Kaplan and Meier.15 In the EFS analy- sis, an event was defined as progression on therapy or relapse after a complete response. Survival curves were compared using the Mantel-Haensel test.I6 The Yates chi-square statistic was used to evaluate differences be- tween discrete variables.
Results
Table 2 shows the pretreatment characteristics of the 121 children analyzed. The length of follow-up for children with MM ranged from 1.9 to 19.7 years (me- dian, 7.0 years). The length of follow-up for children without MM ranged from 2.2 to 17.8 years (median, 5.4 years). Girls were more likely than boy to have a MM (79% versus 57%) (P = 0.02), as were children with nodular sclerosis histologic type than all other histo- logic types (78% versus 39%) (P = 0.0001). Children older than 12 years of age were more likely to have a
Table 2. Pretreatment Characterstics
Total no. of No. of patients P oatients with MM (%) value
~
Gender Male 74 42 (57) 0.02 Female 47 37 (79)
NS 82 64 (78) MC 15 0.0001
LD MISC 11 7
Absent 84 48 (57) 0.009 Present 37 31 (83)
- < 12 38 17 (45) 0.003 > 12 83 62 (67)
Total 121 79 (65)
MM: mediastinal masses; NSL nodular sclerosis; MC: mixed cellularity; LD: lymphocyte predominant; LD: lymphocyte depleted; MISC: miscellaneous.
Histologic type
LP 12 1 2 '1- (39)
B symptoms
Age at diagnosis (yr)
Table 3. Initial Therapy as a Function of Mediastinal Mass
Mediastinal mass uresent
MMR MMR No MM known unknown Total
RT alone 15 13 5 33 Low-dose RT + CT 16 34 8 58 High-dose RT + CT 4 2 9 15
12 CT alone 7 5 1 2 3 Palliative -
Total 42 55 24 121 MM: mediastinal mass; MMR: mediastinal mass ratio; R T radiation therapy; CT: chemotheranv.
-
MM than those younger than 12 years of age (67% ver- sus 45%) ( P = 0.003), as were children with B symptoms (fever greater than 38"C, drenching night sweats, or unexplained weight loss greater than 10% body weight over the preceding 6 months) versus those with none (83% versus 57%) (P = 0.009). Table 3 shows the initial treatment given to children with and without MM. Fig- ure 2 shows the distribution of MMR for 55 children who had MM and whose MMR were known. The MMR ranged from 0.17 to 0.63 (median, 0.29).
Figure 3 shows that 79 children with MM had a poorer EFS than 42 without MM (58% versus 87% at 10 years) (P = 0.004). The overall survival rates for the two groups were not significantly different (82% and 94% at 10 years, respectively) (P = 0.2).
The effect of MMR on survival and EFS was ana- lyzed using MMR values of 0.4, 0.33, 0.3, and 0.25 as cutoff points. The 24 children who had MM but whose MMR were not known were excluded from this analy- sis. We found that a value of 0.25 resulted in the best discrimination for EFS (Table 4). Henceforth, masses
N " 1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7
MEDIASTINAL MASS RATIO (MMR) Figure 2. Distribution of mediastinal mass ratios in 55 children with mediastinal masses whose initial chest films were available.

2758 CANCER June 1, 1992, Volume 69, No. 11
R 0 60.- B A B 40.. I
100 %
P W R
3 0 A B40 I L + EFS - MM Present Survival - MM Present . EFS-MMAbsent Survival-MMAbse.nt T I B
I p =0.001
l l T J "-- - -- - t
p 4.3 ' 4 1
Ill It1
{ + + t i l b t -i I I I I
0 4 8 12 = is - 20 v - .
TIME FROM DIAGNOSIS (Yrs) Figure 3. Overall survival and event-free survival as a function of presence or absence of mediastinal mass in all 121 children.
with MMR greater than or equal to 0.25 are referred to as large and those less than 0.25 are referred to as small.
Figure 4 shows the EFS curves for subgroups based on MM size. Although the curves for children with large MM versus small MM diverged (10-year EFS were 50% and 74'10, respectively), this difference did not reach statistical significance ( P = 0.3). The difference was significant, however, when those with large MM were compared with those with small or no MM (10- year EFS were 50% and 84%, respectively) ( P = 0.0014). The overall 10-year survival rates were also significantly different between these two groups (76% and %YO, respectively) ( P = 0.04).
The data were examined separately according to initial treatment with RT or CMT. Table 5 shows the distribution of children by stage, treatment, and MM size. Among 28 children who were initially treated with RT alone and whose MMR were known (Fig. S), the 10-year EFS rates were 38% for those with large MM (Group 1, eight children) and 80% for those with small MM (Group 2, five children) (P = 0.23). The 10-year EFS rates for those with no or small MM (Group 3, 20 children) was 72% ( P = 0.11, Group 1 versus Group 3). The 10-year survival rates for Groups 1, 2, and 3 were loo%, loo%, and %YO, respectively. The data were
100
%
also analyzed restricted only to children with Stage I1 disease who were treated with RT alone (total, 19); the results were generally the same.
For 56 children treated with initial CMT whose MMR were known (Fig. 6), the 10-year EFS rates were 53% for those with large MM (Group 1, 32 children) and 50% for those with small MM (Group 2 , 4 children) ( P = 0.7). The 10-year EFS rate for those with small or no MM (Group 3, 24 children) was 88% ( P = 0.02, Group 1 versus Group 3). The 10-year survival rates for Groups 1, 2, and 3 were 72%, loo%, and 96%, respec- tively ( P = 0.4, Group 1 versus Group 2; P = 0.11, Group 1 versus Group 3).
For children treated with RT alone, there were no relapses among the five children with small MM versus five relapses in eight children with large MM ( P = 0.09). Of these five relapses, two were true infield failures, two were marginal misses, and one had an infield and an out-of-field component.
For children treated with CMT, there were no re- lapses among the four children with small MM versus five relapses in 32 children with large MM ( P = 0.9). Of
Table 4. Event-Free Survival by Mediastinal Mass Ratio
Event-free survival No. of patients 5 y r (YO) 10 y r (Yo) P value
58 7 O.1° MMR t 0.33 26 64 MMR < 0.33 or no MM 71 74 71 MM present and MMR 2 0.25 43 58 MMR < 0.25 or no MM 54 84
0.001
0.3 :: 7
MM present and MMR < 0.25 12 74 74
MMR: mediastinal mass ratio; MM: mediastinal mass. Twenty-four children who had mediastinal masses but whose mediastinal mass ratios were unknown were excluded.

Mediastinal Masses in Pediatric Hodgkin’s Disease/Maity et al. 2759
Table 5. Distribution of Children by Stage, Therapy, and Size of Mediastinal Mass
Radiation alone Combined modality
No Small Large No Small Large Stage MM MM MM MM MM MM
- IA 8
IIA 6 5 B
IIIA B 1
IVA B
Total 15 5
- - B
- - - -
- - -
- -
-
-
7 5 6 2 3 9
32 MM: mediastinal mass. Twenty-two children who had mediastinal masses but whose mediastinal mass ratios were unknown were excluded.
these five failures, one was a true infield relapse, one was a marginal miss, and three had infield and out-of- field failures. In children with large MM, those treated with CMT had a significantly lower relapse rate than those given RT (5 of 32 versus 5 of 8) (P = 0.02).
Out of 32 children with large MM who received CMT, there were no relapses in the 4 patients who re- ceived more than 3500 cGy versus five relapses in 27 patients who received less than 2500 cGy (P = 0.8). One child who received 3000 cGy did not relapse.
Discussion
Our general findings regarding MM in children confirm those of Roskos et ~ 1 . ~ We found that female patients and children older than 12 years of age at diagnosis were more likely to have MM than male patients or
3
I T20 Y
0 0 4 s 12 16
TIME FROM DIAGNOSIS (Yrs) Figure 5. Overall survival and event-free survival in 28 children treated with radiation alone. Five children with mediastinal masses whose MMR could not be determined were excluded.
%
P R
B * +
t
t Epj - childieo withSmallor no MM Survival - Chldren with Large hlM
0 4 0 3 6 9 i2
TIME FROM DIAGNOSIS (Yrs)
Figure 6. Overall and event-free survival in 56 children treated with combined-modality therapy. Seventeen children with mediastinal masses whose MMR could not be determined were excluded.
younger children. Also, MM were more common in children with nodular sclerosis histologic type or B symptoms than in those children without nodular scle- rosis histologic type or B symptoms.
Children with MM had a significantly poorer EFS than those without MM, although there was no statisti- cally significant survival difference. This result is highly biased because those with MM were more likely to have higher stage disease than those without MM and were more likely to have been treated with CMT.
The authors examined the effect of MM size on EFS. It was found found that using a MMR of 0.25 resulted in the best discrimination and was superior to using 0.33. Therefore, a large MM was defined as one with a MMR greater than or equal to 0.25.
Despite a large difference in 10-year EFS rates be- tween those with large MM and those with small or no MM (38% versus 72%) among children treated with RT alone, this was not statistically significant (P = 0.11). This may have been due to the small numbers in the analysis. The small numbers may also have obscured any significant difference in intrathoracic relapse rate between those with large and small MM (5 of 8 uersus 0 of 5) (P = 0.09). Despite the poor EFS in those with large MM, good salvage therapy resulted in excellent overall survival. The 10-year actuarial survival rate was 100°/o. One child died at 11 years of follow-up secondary to treatment complications.
In children treated with CMT, those with large MM had a significantly poorer 10-year EFS rate than those with small or no MM (53% versus 88%) (P = 0.02). This may have been a function of the inequality in stage distribution between the two groups. There was no dif-
5

2760 CANCER June 2, 2992, Volume 69, No. 13
ference in intrathoracic relapse rate between those with large and small MM (5 of 32 versus 0 of 4) (P = 0.9).
Among children with large MM, those receiving CMT had a significantly lower intrathoracic relapse rate than those treated with RT alone (5 of 32 versus 5 of 8) ( P = 0.02). Regarding dose to the mediastinum in CMT, we found no significant difference in intrathoracic re- lapse rate between those receiving more than 3500 cGy versus less than 2500 cGy (0 of 4 versus 5 of 27) ( P = 0.8). This is in agreement with Dowling et a1.,I7 who were unable to show any difference in local relapse in patients receiving greater than or less than 2500 cGy to the mediastinum.
The effect our findings may have on the treatment of pediatric Hodgkin’s disease is debatable. The role of RT alone is diminishing because of a movement toward the routine use of low-dose RT and chemotherapy, es- pecially for patients who are prepubertal or have ad- vanced disease. For these patients, our data suggest that doses less than 2500 cGy to the mediastinum can result in good intrathoracic control in selected cases. It is im- portant to note that a number of children ultimately received greater than 3500 cGy to the mediastinum be- cause of a boost dose for a persistent mass after chemo- therapy.
For the group of postpubertal children with early stage disease in whom RT alone might be considered, our results suggest that it may result in poor intrathora- cic control for those with a MMR greater than 0.25. Despite this, we have found these children to have an excellent overall survival due to effective salvage therapy.
References
Mauch P, Goodman R, Hellman S. The significance of medias- tinal involvement in early stage Hodgkin‘s disease. Cancer 1978;
Prosnitz LR, Curtis AM, Knowlton AH, Peters LM, Farber LR. Supradiaphragmatic Hodgkin’s disease: Significance of large mediastinal masses. Int J Radzat Oncol Biol Phys 1980; 6:809- 813. Hoppe RT, Coleman CN, Cox RS, Rosenberg SA, Kaplan HS. The management of stage 1-11 Hodgkin’s disease with irradiation
42:1039-1045.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
alone or combined modality therapy: The Stanford experience.
Roskos RR, Evans RC, Gilchrist GS, Burgert EO, Ilstrup DM. Prognostic significance of mediastinal mass in childhood Hodg- kin’s disease. Cancer Treat Rep 1982; 66:961-968. Anderson H, Jenkins JPR, Brigg JD et a / . The prognostic signifi- cance of mediastinal bulk in patients with stage IA-IVB Hodg- kin’s disease: A report from the Manchester Lymphoma Group. Clin Radiol 1985; 36:449-454. Donaldson SS, Link MI’. Combined modality treatment with low-dose radiation and MOPP chemotherapy for children with Hodgkin’s disease. ] Clin Oncol 1987; 5:742-749. Jenkin D, Doyle J, Berry M et at. Treatment with MOPP and low-dose, extended field irradiation without laparotomy late re- sults and toxicity. Med Pediatr Oncol 1990; 18:265-272. Dionet C, Oberlin 0, Habrand JL et al. Initial chemotherapy and low-dose radiation in limited fields in childhood Hodgkin’s dis- ease: Results of a joint cooperative study by the French Society of Pediatric Oncology (SFOP) and Hopital Saint-Loius, Pans. Znt J Radiat Oncol Biol Phys 1988; 15:341-346. Schellong G, Bramswig JH, Schwarze EW, Wannenmacher MF. An approach to reduce treatment and invasive staging in child- hood Hodgkin’s disease: The sequence of the German DAL multicenter studies. Bull Cancer 1988; 75:41-51. Fryer CJ, Hutchinson RJ, Krailo M et al. Efficacy and toxicity of 12 courses of ABVD chemotherapy followed by low-dose re- gional radiation in advanced Hodgkin’s disease in children: A report from the Children’s Cancer Study Group. J Clin Oncol
Maity A, Goldwein J, Lange B, D’Angio GJ. Comparison of high and low dose radiation with and without chemotherapy for chil- dren with Hodgkin’s disease: An analysis of the experience at the Children’s Hospital of Philadelphia and the Hospital of the University of Pennsylvania. J Clin Oncol (in press). Mauch PM, Weinstein H, Botnick L, Belli J, Cassady RJ. An eval- uation of long-term survival and treatment complications in children with Hodgkin’s disease. Cancer 1983; 51:925-932. Donaldson SS, Kaplan HS. Complications of treatment of Hodgkin’s disease in children. Cancer Treat Rep 1982; 66:977- 989. Probert JC, Parker BR, Kaplan HS. Growth retardation in chil- dren after megavoltage irradiation of the spine. Cancer 1973;
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53:457-481. Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 1966;
Dowling SW, Peschel RE, Portlock CS, Kramer C, Farber LR, Knowlton AH. Mediastinal irradiation in combined modality therapy for Hodgkin’s disease. Int J Radiat Oncol Biol Phys 1990;
Blood 1982; 59~455-465.
1990; 8: 197 1-1 980.
32:634-639.
50:163-170.
19:543-546.