medgate today-may june 2013
DESCRIPTION
Special issue on Hospital FurnituresTRANSCRIPT

The Gateway to Health & Medical World
Scan the QR Code to know more
www.medgatetoday.com
Volume IV || Issue I || May-June 2013
News Update | Doctor Speak | Dental Care | Product Line | Interview | Healthcare Management
PRICE : 100
HospitalFurniture


May – June 2013 3

4 May-June 2013

May – June 2013 5

6 May-June 2013
Volume-IV Issue-I May-June 2013
EditorDr. M.a. KaMaLEditorial AdviserGp Capt. (Dr.) Sanjeev SoodDr. Sharad Lakhotia
National HeadAfzal Kamal
Cheif CorrespondentSA Rizvi l Dr HN Sharma
Design and LayoutKakul
Sales and MarketingAmjad KamalNeetu Sinha S.Y Ahmed Khan
Subscribtion & CirrculationPallavi Gupta Saba Khan
All right Reserved by all everts are made to
insure that the information published is cor-
rect, Medgate today holds no responsibility
any unlikely errors that might occur.
Published by:
Circulation Office :92/17 Zakir Nagar,Opp. New Friends Colony, Okhla New Delhi–110 025Tel: +91 11 26981342Fax: +91 11 26982464M: +91 9212366351Email: [email protected]@gmail.comVisit us: www.medgatetoday.comMumbai Office:7 Ground Floor, Aradhna CHS Ltd. Bal Samant Marg, Bandra (W), Mumbai–400 050Chennai Office:11, Krishnan, Koil Street 3rd Floor Rotary LaneChennai-600001
Printed byArtxel, 76, DSIDC Shed, Okhla Industrial Area , Phase-II, New Delhi-110020
Editor’s NoteThe Global Endoscopy Market Outlook
The global healthcare industry has seen a shift inparadigm and is now skewed toward less-invasivetherapies that not only cures serious illnesses, but also have fewer serious side effects. Demand for endoscopy has increased manifolds over the past decade owing to patient preference for minimally invasive surgeries.
The global endoscopy devices market was valued at $6.1 billion in the year 2011 and is expected to be $9.7 billion in the year 2016. North America was the largest endoscopy market, followed by Europe andJapan (2011). In the next five years, Asian countries are slated to register a maximum CAGR of 14.42% owing to increased healthcare spending by the government, healthcare reforms and increased patient awareness about minimally invasive surgeries (MIS).
Global endoscopy market is broadly segmented into the following product categories; rigid endoscopes, flexible endoscopes, endoscopy visualization systems, endoscopic ultrasounds, endoscopy fluid management systems, and endoscope accessories. Introduction of new, but expensive technologies such as HD cameras, 3DHD systems, HDTV three-chip systems, Narrow Band Imaging, Capsule Endoscopy, Natural Orifice Transluminal Endoscopic Surgery (NOTES), Picture Archiving and Communication Systems (PACS),Mucosal Ablation Therapy, Robotic Endoscopes etc. are expected to drive the global endoscopy market for the coming five years.
Have an insightful reading.Your suggestions are most welcome!E-mail: [email protected]

May – June 2013 7
Volume-IV Issue-I May-June 2013
6
42
24
22
Manufacturers of hospital furniture are updating theirproduct designs to meet new demands in health care environments. One big consideration is the creation of afamily-friendly hospital experience for the relatives and friends of patients. Other areas of emphasis includeaesthetics, ease of cleaning, sustainability, ergonomics and furnish-ings for large people.
Breastcancer drugs underused:expert
new Value
Model for
Wound Care
HospItal
tender
exHIBItIon &
conferencesFrequent Diabetes Monitoring & Intensive Management to Rise
Diabetes Management Future Trends
INTERVIEWDr Pervez
Ahmed 47
50-59

8 May-June 2013
Breastcancer drugsunderused: expert
Tamoxifen and raloxifene can halve the risk of developing breast cancer in at-risk women and should be used more widely forprevention, a major review suggests. The drugs reduce the incidence of invasive breast cancer by 30-68% compared with placebo, depend-ing on the woman’s baseline risk, the system-atic review concluded. Tamoxifen was more effective than raloxifene. In absolute terms, the drugs could prevent seven to nine cases of breast cancer per 1,000 women taking them over five years, researchers wrote in the Annals of Internal Medicine.
The review was conducted for the USPreventive Services Task Force, an influential government expert group that makesevidence-based recommendations forpreventive medicine in primary care.Associate Professor Kelly Phillips, a medical oncologist and head of the Breast Cancer Risk Management Clinic at the Peter MacCallum Cancer Centre, Melbourne, said preventive medicines for breast cancer were underused in Australia.
Despite guidelines recommending tamoxifen and raloxifene be considered for women at high or moderate risk of breast cancer, uptake was less than one percent among those groups. Professor Phillips cited concern about sideeffects, doctors’ lack of confidence inprescribing the medications and difficulties inassessing risk status for the low rates ofprescribing. The US paper showed thepreventive benefits came at a cost in sideeffects: both medications increased theincidence of thromboembolic events and tamoxifen increased the overall incidence of endometrial cancer.
8
UPDATENEWS

May – June 2013 9
Common pregnanCyCompliCations double diabetes risk
women with a history of hypertensivedisorders in pregnancy are at high-risk fof diabetes in later years and should be offered screening.The call comes in response to the publication of a Canadian study of over one million women, which found two common conditions in pregnancy - preeclampsia and gestational hypertension - can double the risk of diabetes up to 16 years after giving birth.
Furthermore women who had gestationaldiabetes in addition to one of thehypertensive conditions had a staggering 18 fold increased risk of diabetes, thepopulation-based study with an averagefollow-up of 8 years found. While the study adjusted for several such as maternal age and previous hypertension, the study waslimited by its failure to take into accountobesity, BMI, and glucose and blood pressure, the researchers wrote in PLOS.
Nevertheless, their findings had importantimplications for maternal health, especially given the increase in obesity related diseases.
“A history of preeclampsia or gestational hypertension during pregnancy should alert clinicians to the need for preventativecounselling more vigilant screening fordiabetes,” they concluded. While currentevidence did not support the idea thatwomen with a history of hypertensivedisorders in pregnancy be systematically
screened for diabetes, inaction was not anoption either. “Based upon this new study,women experiencing hypertensive pregnancydisorders with or without GDM should be con-sidered as a population at high risk forsubsequently developing diabetes,” he wrote.
“All women with a history of hypertensivedisorders in pregnancy should be counselled about their potential increased risk of DM and the possible opportunity for screening as well as preventive interventions”.
UPDATENEWS

10 May-June 201310 april-May 2013
UPDATENEWS
A revolution in wound therapy, Quantum, helpshospitals gain better control of wound care costs while potential-ly enhancing carequality
ADVANCED wound care spe-cialist, Innovative Therapies, Inc. (ITI), has launched the first fully-loaded negative pressure wound therapy (NPWT) device with simultaneous irrigation. The wound therapy system, Quan-tum™, is expected to help hospi-tals gain better control of wound care costs while potentially en-hancing care quality by providing continuous healing for patients.
Beyond a technological advance-ment, Quantum offers a new form of innovation for wound care – a cost-efficient purchase model in which hospitals pay only
for therapy hours used versus the industry-standard rental model.“Wound care is a very costly and clinically-important part of patient care,” said ITI chief oper-ating officer Matthew Dambeck. “ITI developed Quantum because we believe device innovation is no longer solely about technology, but about total value to the hos-pital. The rental model in wound care is not sustainable. Hospitals should not be paying for assets they’re not using. With Quantum, hospitals only pay for the hours in use – not when the device is sitting on a shelf. It offers the opportunity to achieve quality care for more patients in a more economically efficient model.”
Therapy hours are preloaded onto Quantum based on hospital and outpatient needs, offering a seamless hospital-to-home system, helping to minimize cross-con-tamination. This purchase model allows the institution to own the device without the costs or incon-veniences of maintenance, clean-ing or misplacement penalties.
ITI offers the only NPWT on the market that delivers simultaneous irrigation. Unlike other devices where fill volumes must be calcu-lated and NPWT must be discon-tinued to apply irrigant, Quan-tum constantly delivers irrigation solution to the entire wound bed, including tunnels and under-mined area, without sacrificing continuous negative pressure. The durable foam dressings protect and promote wound healing.
Quantum works seamlessly across all healthcare settings—inpatient or outpatient, as well as short and long-term therapy. The device is extremely lightweight, and has an intuitive user interface for ease of use and offers up to 24 hours of battery life

May – June 2013 11

12 May-June 201312 april-May 2013
UPDATENEWS
New research has added weight to the view that bisphosphonates may have a role to play in the treatment of osteoarthritis. The observational study of 55 patients takingbisphosphonates and 268 non-users found treatment reduced pain over a three year period, even after adjusting for analgesic use. But the benefits did not continue after patients stopped treatment.
Annals of the Rheumatic Diseases they suggested that bisphospho-nates may have an effect on the subchondral bone andosteochondral junction.
The drugs may also have animmediate analgesic benefit, which might explain why pain relief did not persist beyond the period of drug use.
Bisphospho-nates may work in osteoarthritis
A new therapy for pancreaticcancer has been developed us-ing listeria bacteria to selectively infect tumour cells and deliver radioisotopes to them.
The treatment radically reduced the number of metastases in mice with pancreatic cancer without harming healthy tissue,researchers from the AlbertEinstein College of Medicine in New York found the research built on a 2009 study that demonstrated a weakened form of listeria monocytogenes could infect tumours while sparing healthy cells.
listeria usedto targetpancreaticcancer
Minimal access surgery compared with medical management for gas-tro-oesophageal reflux disease: five year follow-up of a randomised controlled trial (REFLUX)
Trials of laparoscopic fundopli-cation surgery provide promis-ing evidence of better short term symptomatic relief than contin-ued medical management among people who would otherwise re-quire continuous or intermittent medication for reasonable control of gastro-oesophageal reflux dis-ease (GORD). Uncertainty re-mains about whether benefits are sustained and outweigh risks, sub-sequent drug use, and unwanted symptoms such as dysphagia and flatulence. Therefore undertook five year follow-up within a mul-ticentre, UK based, randomised controlled trial, the REFLUX tri-al.
surgery better in long-term for gordsymptoms

May – June 2013 13
UPDATENEWS
U.S. FDA clearance of its MAGPIX instrument, with its xTAG Gastrointestinal Pathogen Panel (xTAG GPP). This is the first clinical assay to be cleared on MAG-PIX. xTAG GPP is the first U.S. IVD cleared test that can simultaneously detect 11 common viral, bacterial, and parasitic causes of infectious gastroenteritis from a single patient sample.
“Receiving FDA clearance of MAGPIX opens the door for clinical laboratories of all sizes to use xTAG GPP on this innova-tive instrument,” said Patrick J. Balthrop , president and chief executive officer of Luminex. “By bringing a compact, cost-effective, easy-to-deploy multiplexing solution to the clinical market, MAGPIX makes molecular testing more accessible to all laboratories.”
Based on Luminex’s xMAP Technology, the easy-to-use instrument is a versatile multiplexing platform capable of perform-ing qualitative and quantitative analysis of proteins and nucleic acids in a variety of sample matrices. MAGPIX is compact making it attractive to laboratories with limited bench space. This affordable system can perform up to 50 different tests in a single reaction volume, greatly reducing sample input, reagents, and labor while improving productivity.Traditional GI testing technologies and methods can take several days to deliver a single result depending on the pathogen. xTAG GPP is capable of delivering multi-ple results within five hours. Simultaneous molecular testing on a single sample within a single shift provides significant benefits
fda-cleared test detects 11gastrointestinal pathogens
to laboratories in terms of workflow and resource utilization.xTAG GPP detects the following potential causes of gastroenteritis: Campylobacter, Clostridium difficile toxin A/B, Escherichia coli O157, Enterotoxigenic E. coli (ETEC) LT/ST, Salmonella, Shigella and Shiga‐like Toxin producing E. coli (STEC) stx 1/stx 2; Norovirus and Rotavirus A; and Crypto-sporidium and Giardia.
“Tests such as the xTAG GPP that can detect viruses, bacteria, and parasites from one sample at the same time can help clinicians more quickly identify and treat what’s causing gastroenteritis,” said Alberto Gutierrez , Ph.D., director of the Office of In Vitro Diagnostics and Radiology at the FDA’s Center for Devices and Radiological Health in an FDA press release when xTAG GPP was first approved by the Agency. “The test could also allow clinicians and public health professionals to more quickly identify and investigate the source of potential gastroenteritis outbreaks.”Infectious gastroenteritis is an inflamma-tion of the stomach and intestines caused by certain viruses, bacteria, or parasites. Common symptoms include vomiting and diarrhea, which can be more severe in infants, the elderly, and people with sup-pressed immune systems. Gastroenteritis can be spread easily through person-to-per-son contact and contaminated food, water, and surfaces.
Diarrheal disease strikes more than two billion times globally each year, and is a leading cause of child morbidity and
mortality worldwide. In the United States alone, 99 million cases of Gastrointestinal (GI) infection occur annually, leading to more than 250,000 hospitalizations and 17,000 deaths — inflicting a significant toll on the healthcare system. Diagnosis of some causes of infectious gastroenteritis has traditionally required multiple tests across the microbiology, virology, and molecular laboratories for which results may not be available for several days.
The researchers audiotaped and translat-ed 142 oncology consults involving 78 patients diagnosed with metastatic disease. Twenty-four were native Chinese speakers, 12 Greek and 11 Arabic. The remainder were Australian-born, serving as a control group.Dubious translations commonly removed doctors’ uncertainty and caveats, for exam-ple turning “there is a 40% chance that the treatment will prolong your life” into “the treatment will prolong your life”.
Another example of softening the blow saw a “very, very unlikely” chance of cure become “the possibility is not very high”.
Oncologists, for their part, were fairly consistent in their content and style when delivering a prognosis. However, they did use more jargon and less hope-inspiring language when speaking through interpret-ers.
The flow of information was even worse in the other direction: 59% of patients’ ques-tions about their prognosis were altered or blocked by interpreters.

14 May-June 201314 april-May 2013
UPDATENEWS
14 april-May 2013
UPDATENEWS
Jaslok, one of the most reputed hospitals in Mumbai, will adopt Napier’s next genera-tion mobile electronic health records plat-form that will empower over 1,100 users from the hospital to render faster, more effi-cient services to its patients.
Napier Healthcare Solutions, a leading healthcare software pro-vider, is pleased to announce that Jaslok Hospital of Mumbai has selected the Napier EHRm (pronounced EHR mobile) manage-ment suite of products for its end-to-end hospital management needs.The fully mobile-enabled solution is Napier’s next-generation platform that helps deliver the vision of a Digital Hospital. The Napier EHRm is an open-source based platform; when fully deployed in the course of the next few months, it will be used by over 1,100 users from the hospital.
“Napier has been a strategic partner in our growth and has helped support our needs over the years. The entire Napier EHRm product is accessible on mobile devices, thereby “unlim-iting” our options for making use of mobile solutions in every aspect of Jaslok’s operations. Combined with a Patient Portal, the mobile solution will help us foster better relationship between the patient and the Doctor, thereby improving the overall quality of care,” said Ms. Kanta Masand, Managing Trustee of Jaslok Hospital.
Ms. Viloo Williams, CIO at Jaslok, envisions numerous opera-
tional benefits and said, “The open source, web-enabled, tech stack on which the new Napier EHRm platform is built, will provide scalability whilst seamlessly integrating with 3rd party systems. Napier EHRm will lower Total Cost of Ownership (TCO) due to parameterization, modularity and flexibility in adapting process changes with ease. Napier EHRm will fulfill our need-of-the-hour which is anywhere, anytime accessibility; just what our Doctors, Patients and Management need today!”
“We are confident that Napier EHRm will contribute to re-defining mobility in healthcare services delivery and establish a new benchmark. The mobility solution will help hospitals ren-der quality healthcare more easily and in a more transparent and cost-effective manner,” opined Karthik Tirupathi, CEO of Napi-er Healthcare Solutions.
“We are extremely pleased to further strengthen our relationship with Jaslok Hospital that has used our solutions for more than five years,” he added. “The Napier EHRmsolution upgrade not only validates our product development strategy to leverage the latest web and mobile technologies but also reaffirms our strong value proposition to healthcare providers with mature opera-tions.”
Mumbai’s Jaslok Hospital opts fornapier eHrm solution

May – June 2013 15
UPDATENEWS
seminar on ‘Best practices in HealthInsurance - strategies & accountability’ The Insurance companies can play a vital role in improvising the current state of Health sector in order to eliminate the difference in the facilities available to elite and poor class. He urged to provide fair and equal treatment to everyone across the country. Treatment meted out to the patient with or with-out insurance is different when they approach the hospital. Presently, patient has to stay in the hospital for 24 hours to get an Insurance claim that can be settled in a few hours said Sunil Gupta, Director, General Insurance Corporation in a Seminar organized by Health Committee of PHD Chamber on 17th of May at PHD House, Delhi.
He recommended the Day Care & pathology tests to be cov-ered in the insurance policy to prevent hospitalization. This indeed will cut off the un-necessary hospital admissions and save the resources. He agreed to the suggestion that inclusion of alternate system of medication such as Ayurveda/ Home-opathy and Naturopathy has to be covered in the insurance policy. The government and insurance companies should work together and there is a need of inflation oriented insur-ance policy as the expenditure on the health care is increasing every year he added.
Dr Kamat mentioned that RSBY (Rashtriya Swasthya Bima Yojna) Scheme is spreading out to cover most of the poor segment of the community.
Dr. Praneet Kumar, CEO, B L Kapur Memorial Hospital em-phasized on the issues and challenges being faced by the pri-mary stakeholder in settling an insurance claim. The Custom-er-Provider-Insurance/TPA inter relationship seems to have been changed these days and there is a lack of trust amongst them. The current practice of non standardized processes & Non standard documentation was brought into the attention, which in turn results in substantial delays in issuance of a claim, said Dr. Praneet.
Sanjay Seth, Executive Vice President, IFFCO TOKIO General Insurance Co Ltd spoke about Settling of claims and emphasized on the inter-relation between the Business ethics and profitability. He insisted on building up trust with primary stake holders as Customers prefer dealing with the organizations they trust. Access to the insurance policies should be made online and the insurers must have a compet-itive knowledge of the industry as to let the customer make a rightful choice said S.K. Sethi, Director, Insurance Brokers Association of India.
Ms. Raunak Jha, Member, Advisory Group on Health In-surance, Institute of Actuaries of India laid stress on the role
of actuaries in filling the gap between the policy holder and Insurer. Several conflicts like Cost of treatments, data sharing, scope of insurance cover among Policy Holders & Insurance Companies -& Care Providers.
Insurer’s business and focus has changed amidst of a high competition where large amounts have replaced large num-bers with a higher cost of service and man power and time said Dr George E Thomas, Associate Professor, College of Insur-ance, Insurance Institute of India,
Dr. Saini, Hony. Secretary General, Indian Medical Associa-tion recommended insurance companies to develop products for the poor at reasonable and low premiums. Government spends 0.9% -1% of GDP towards Health sector, where as Private Sector exceeds up to spending 5% of GDP towards the same. That is where Insurance companies should pool in and health care services can be rendered by everyone across the society. Also, special policies for rural population should be made where the cost of medication is low.
Some experts participated in the technical session raised following pertinent issues in the seminar:
• Need for innovative plans to cover different groups of peo-ple exposed to specific risks• Having affordable plans on policies for senior citizens and retired corporate employees• Corporate and Group policies should be allowed to carry forward in case of transition to another company
A collective suggestion was made by the panelists and experts to form an advisory board to take up issues and send recom-mendations to the department of financial services and Delhi government.
16 May-June 2013
Wellness sector in India is expected to touch Rs. 950 billion by 2014
• Care World TV launches India’s first wellness shopping Channel • To expand distribution network, engage 15,000 vendors across the country• Targets 1 million audiences in the first year • Observing rapid growth in the tele-shopping sector, the channel aims to capitalize its leadership in the healthcare segment
Care World TV, Asia’s only satellite Health Chan-nel has launched India’s first Wellness Shopping Channel. Initially launched as a 3 hour slot titled ‘Wellness Mall’ within Care World TV, it will soon be migrated to a dedicated television channel.
Care World TV is India’s first and only healthcare channel. With its venture into Wellness Shopping, the channel will showcase and sell a range of prod-ucts in 6 broad categories viz. Beauty Care, Fitness and Slimming, Health and Wellness, Food and Beverages, Rejuvenation & Alternate therapy. With attractive deals and offers, products from across the globe will be sourced and made available to con-sumers.
Speaking about this new venture Mr. Ajit Gupta, Managing Director, Care World TV said, “For a while now Care World TV has been leading the viewership in the health space. The response towards our channel has grown by many folds. Viewers have been interacting constantly with us via website, email, social media and popular shows like ‘Ask the Doctor’ and ‘Psychology Behind Love’
among others. Hence, launching the Wellness mall was an obvious extension.”
The Wellness Sector in India is expected to touch Rs. 950 billion by 2014 and will grow at a Com-pound Annual Growth Rate of 18%-20% as per a new report by PWC-FICCI (PricewaterhouseC-oopers’ – Federation of Indian Chambers of Com-merce and Industry). The sector size was estimated at Rs.590 billion in 2011 recording a growth of 20% over the previous year. Key driver for this growth would be the 40 + age group.
Rising disposable income, changing lifestyle, easy payment options and availability of range of brands
May-june 2013
UPDATENEWS
16
Mr. Ajit GuptaManaging Director, Care World TV

May – June 2013 17
UPDATENEWS
May-June 2013 17
Care World TVabout
are attracting more and more buyers to avail the modern retail facility. It is estimated that out of about 220 million households in India, approx 130 million have cable or direct to home (DTH) TV connection. Considering the trouble-free access to the channel, Care World Tv expects to reach to about 1 million udiences by end of Dec 2013. It has already started building its distribution network and will be engaging about 20,000 vendors across the country to cater the market withindecided timeframes. It aims to target mainly the Hindi speaking belt, whose annual income isupwards of Rs. 2,00,000.
“The wellness sector is booming in today’s age. With the Wellness Shopping Show we will be catering to Tier 1, Tier 2 and Tier 3 Cities. The call centers will be manned by Experts who will provide necessary information instantly. We are expecting 25% of the turn-over from repeat purchase,” concluded Mr. Ajit Gupta.
18 May-June 2013
a collaborative project between the Department of Assistive Technology, Indian Spinal Injuries Centre (ISIC) and the Human Engineering Research Laboratories (HERL), University of PittsburghWith increasing demand for a low cost electric wheelchair, a new Single Motor Propelled Wheelchair (SiMPl-WC) is being developed through a collaborative project between the Department of Assistive Technology at Indian Spinal Injuries Centre (ISIC) and the Human Engineering Research Laboratories (HERL), University of Pittsburgh. The SiMPL wheelchair is being designed to be a low cost electric power wheelchair keeping in mind the varied terrain commonly found in less resource settings.
Understanding the need to serve the in-digenous population, the Department of Biotechnology, Ministry of Science and Technology, India and National Institute for Health together decided to fund the project. The conviction of the present initiative is to facilitate joint activities between US and Indian scientists for the development of low cost medical devices, address medical needs in low resource settings and take advantage of opportunities and technological advanc-
es through the development of appro-priate, low cost medical devices. Medical technologies developed through Indo US collaboration will also benefit other low resource settings globally.
According to the World Health Organi-sation (WHO), approximately 65 million wheelchairs (WCs) are needed world-wide. In the present scenario, less-re-sourced environments (LREs), such as India, often face obstacles in accessing devices that can provide functional mobility at an affordable price. In the past decade, evidence has revealed that converting low-cost western-style manu-al wheelchairs into powered wheelchairs fails to address the needs of the people. This has been primarily due to many reasons like devices being challenging to propel, failure to sustain in extreme environmental conditions of LREs, and most importantly, inability of the device being repaired with indigenous tools and materials.
“In India there has always been a tre-mendous need for an affordable and well designed electric power wheel chair to cater to the services of the needy. While a normal power wheelchair may range between Rs 60,000 to Rs 10,50,000, we plan to reduce the price by half through this venture.” says Nekram Upadhyay,
Head of the Department of Assistive Technology at Indian Spinal Injuries Centre
Speaking on this joint initiative, Dr HS Chhabra, Medical Director and Chief of Spine Services of Indian Spinal Injuries Centre and also the principal investigator of this collaborative study said “The objective of the collaborative study is not only to develop a low cost electric wheelchair, but to develop one techni-cally best suited for Indian environment, whether urban or rural. The study would help in translating the vast experience of the American scientists in the field of wheelchair design in developing one most suitable for Indian environment using the expertise and experience of the Indian experts.”
Although, several organizations are mounting international efforts to address these shortcomings by designing ap-propriate manual WCs and establishing clinical and technical resources in LREs to meet this ongoing need. However, these efforts have not addressed the needs of people who would benefit from electric powered wheelchairs (EPWs). Consequently, low-cost western style devices have started to crowd the market despite the fact that they perform poorly, fail prematurely, and in some cases have been discontinued in the western markets.
UPDATENEWS


20 May-June 2013
doctors on care world tVMay- June 2013do watch These doctors on care world tv
Dr Hrishikesh D Pai - Gynaecologist & Infertility Specialist (Mumbai)
Dr Bhavna Parikh - M D (Mumbai)
Dr Nagraj Huilgol -D G O , M D F M A Sc(Mumbai)
Dr R Gopal M D (Mumbai)
Dr Sudeep SarkarM S , F I C S (Mumbai)
Dr Ganesh Shinde Gynecologist (Mumbai)
Dr Vivel AllahbadiaOrthopedic & Joint Replace-ment Surgeon (Mumbai)
Dr Sanjay DudhatM S (Mumbai)
Dr Indu Bansal Aggarwal M B B S , M D , D H M(New Delhi) w
ww.
care
wor
ldtv
.com
UPDATENEWS

May – June 2013 21

EVENTPRE
22 May-June 2013
The demand for Hospital beds in India is expect-ed to be around 2.8 million by 2014 to match the global average of 3 beds per 1000 population from the present 0.7 beds. India needs 100,000 beds each year for the next 20 years at over US $ 10 billion per year. Healthcare has emerged as one of the most progressive and largest service sectors in India with an expected GDP spend of 8% by 2012 from 5.5% in 2009. 20 Health cities are expected to come up in the next 5 years. Understanding these statistics, AMEN and HOSPACCX India Systems present a series of Conferences on Hospital Planning, Design and Architecture across various cities of the coun-try in 2013-14..
HospiArch.. India’s BIGGEST Conference series on Hospital Planning, Design & Architecture has been conducted in Chennai, Hyderabad, Mumbai, Ban-galore, Delhi and Kochi in 2012 and at Vijayawada, Chandigarh and Lucknow until April 2013. “The series has received amazing response and we’d like to conduct more HospiArch Conferences across the country starting from Jaipur in July 2013”, mentioned Mr. Paniel Jayanth, Founder & Chief Strategist, AMEN, India’s leading Healthcare Event Organizers. “The places we have identified include-Jaipur, Coimbatore, Jammu, Goa, Kolkata, Nagpur, Pune, Bhubaneshwar, Ahmadabad, Guwahati etc.”, he continued.
Topics at HospiArch would touch upon various issues related to Hospital Architecture including:
• Architectural challenges involved in Building a new Hospital.• Planning & Designing a New Hospital.• Re-planning & Re-Designing an Existing Hospital• Budgeting & Financial Planning for a New Hospi-tal Project• Planning a Green Hospital • Medical Equipment Planning• Planning & Designing Lab and other Diagnostic areas of the hospital.• Marketing Strategies & Branding for a New Hos-pital.• Man power planning for new hospital.• Designing a CSSD. Techniques and Trends.• Quality standards applicable to Hospital Planning• Medical Gas Pipeline • Hospital Engineering and Architectural Innova-tions
HospiArch is India’s BIGGEST Conference series on Hospital Planning, Design & Architecture with Eminent Speakers from across the country at all of its Conferences. “The Event is unique and one-of-kind creating a very rare opportunity for Doctors, Hospital Administrators, Architects and Consul-tants to interact and network on one Platform”, said Mr. Tarun Katiyar, Principal Consultant, and HOSPACCX India Systems. HospiArch would also feature an Innovative Quiz on Hospital Architec-ture which will help enhance the knowledge of the participants.
HOSPIARCH INDIA 2013-14
Mr. Tarun KatiyarPrincipal Consultant
Hospaccx India Systems, Mumbai

May – June 2013 23
EVENTPRE
You may have the BEST Product or Service on Earth, but it cannot become Big without the RIGHT Marketing Strategy. Marketing, today has become a vital compo-nent of all Hospital & Healthcare Operations owing to the rise in the number of Hospitals and immense com-petition.. The Indian Hospital industry would be worth USD 280 billion by 2020 as against USD 44 billion in 2010. During 2010-2015 the Indian Hospital service in-dustry is projected to grow at a CAGR of more than 9%. Medical tourism market is valued to be worth USD 310 million and is expected to generate USD 2.4 billion by 2012. With the introduction of Face book, Twitter and other Social networking sites, Marketing has become a lot easier than before. INLEAD Indian Institute of Learning & Advanced Development, Gurgaon, is conducting a 3 Day MDP (Management Development Program) on HEALTH-CARE MARKETING that would address all issues and queries pertaining to various Strategies & Processes in Healthcare Marketing. This MDP is in association with AMEN, India’s leading Healthcare Event Organizers... & HOSPACCX India Systems, one of India’s fastestgrowing Healthcare Management Consultancies.
Topics that would be addressed in the MDP include:• Healthcare Marketing in the 21st Century. Issues, Challenges and Opportunities• Marketing Mix and the 4 P’s. Positioning and Re-Posi-tioning your Brand• CRM and its impact on Business Development. Inter-nal Marketing and its effect on Hospital Efficiency• Ethics and Legal Issues related to Healthcare Market-ing (+ Case Study)• Planning / Improvising the Marketing Department. Effectively Recruiting Marketing Professionals.
• Strategically Marketing today’s Single / Multi-Specialty Hospitals• Public Relations and Media Management as a Market-ing tool• NABH and other Quality Standards applicable to Healthcare Marketing• International Marketing Strategies and Medical Tour-ism (+ Case Study)• Effectively managing your Sales Force for better results and profitability.• Market Research and Competitor Analysis. Strategies to out-perform them• Tele Marketing & its optimum utilization. Innovative techniques to ensure Customer Delight• Hospital Architecture as a Marketing tool.• Challenges in Marketing a Medical College / Teaching Hospital.• Marketing, Branding and Advertising. The future and its challenges
The MDP would also consist of 3 Interesting work-shops...including:• Effectively Designing your Logo, Brochures, Website and other Marketing Tools• Branding Strategies for Hospitals and Healthcare.Designing & Executing an Effective Ad campaign• Online Marketing & the Social Media - How to market your services on TGIF: Twitter, Google, Internet &Face book.
Participants would include Hospital & HealthcarePromoters, CEOs, Administrators, Marketing andBusiness Development Professionals, MarketingExecutives and Consultants and HealthcareManagement Consultants
HEALTHCARE MARKETING
Mr. Paniel JayanthFounder and Chief Strategist
AMEN, Bangalore

24 May-June 201324 May-June 2013
UPDATENEWS
Schiller India launches a new MRIMonitor – MAGLIFE Serenity
Schiller India, a leading Swiss Joint Venture Company in the field of Medical Diagnostics, has launched anew MRI compatible monitor called MAGLIFESerenity.The MAGLIFE Serenity guarantees highest ECGquality during magneticresonance imaging (MRI)scanning – even under strongest gradient influence. It monitors all vital parameters duringanesthesia in an MRIenvironment and is specifically designed for adults, children and neonates.
According to Mr. Hormazd Cooper, Vice President, Sales, “Schiller’s MAGLIFE Serenity has already clocked up major sales in Europe with its capability of being used with MRI scanners upto 3.0 Tesla. Its combination of monitoring basic / vital signs plus additional param-eters such as CO2, temperature monitoring etc. ensures that the Serenity system becomes the mon-itor of choice for small diagnostic MRI centres, as well as, full fledged hospital MRI departments, where critical & high risk patients are scanned. A major advantage of the Serenity system is that all optional parameters are field upgradeable and can be purchased individually thereby negating obsolescence and protecting the hospitals investment.”
Features of MAGLIFESerenity:• Large 12.1” color TFT display• Widely adjustable color display for various viewing angles• Compatible with 0.2 to 3 Tesla scanners of all manufacturers• Choice of 3 leads for artifact free ECG & enhanced accuracy of QRS detection• New generation SpO2 probes are much lighter for enhanced patient comfort and are available in varied lengths• Enhanced accuracy in temperature monitoring due to state-of-art sensors based on Fluorescence technology• Standard monitoring of ECG, SpO2& NIBP• Auto identification of anesthetic gases• Display & measurement of inspired and expired values of all gases• O2 measurement in same sample as CO2 & anesthetic agents• Magnetic field detector built in main unit & Power box• MAGLIFE Serenity can be connected to more than one MAGSCREEN Serenity (slave monitor) and vice versa• Non magnetic trolley provided as standard• Certification: CE 0459

May – June 2013 25

26
Dr Pervez Ahmed Founder & Managing Director, Aapka Urgicare Pvt. Ltd Transforming his vision of providing high quality,timely and affordable healthcare to all into reality, Dr Pervez Ahmed founded Aapka Urgicare Pvt. Ltd. With Dr Ahmed at the helm as Managing Director, AapkaUrgicare seeks to provide immediate attention to those who need emergency treatment. The company also seeks toprovide healthcare management solutions to medicalfacilities for better outcomes
To provide Good, Affordable Primary & Emergency Care to the Local Neighbour-hood Population in North & East India
Setting up Free Standing Urgent Care Center Hospitals in densely populatedNeighbourhoods to provide Urgent & Emergency Care to the catchment area population. These are 24x7 Centers staffed with trained Emergency Medicine Doctors, Nurses, EMT’s and fully equipped with EmergencyMedicine Equipment’s, Minor OT,Diagnostics,Pathology & Pharmacyfacilities with ALS Ambulance. These are Walk In Centers. Because of the lack of Ur-gent Care in local neighbourhoods, people had to go toEmergency Rooms of Hospitals which entailed long waits and were expensive too. In the crucial Golden Hour there was a need for a First Response Facility in local neigh-bourhoods. Further statistically 75% of ER Patients do not need hospitalization and can be tended to in our facilities.
Objective of UCC?
26 May-June 2013
INTERVIEW

May – June 2013 27
“For the first time a new healthcare initiative now available in your neighborhood providing afford-able emergency and non emergency medical care needs round the clock in a good, fast and kind manner”Urgent care is the delivery of ambulatory care in a facility dedicated to the delivery of emergen-cy medical care outside of a hospital emergency department, usually on an unscheduled, walk-in basis. Our Urgent care centre Hospitals not only special-ize in dealing with all kinds of medical emergencies but can also take care of all your routine health-care needs in the neighborhood of your home or workplace. You have the convenience of walking in at any time of the day without worrying for an appointment to see our Urgent Care doctors. Because urgent care practitioners are on the “front lines” of medicine, they are proficient in evaluating and caring for any patient who walks into an urgent care centre. We also work in collaboration with
your primary care physicians and special-ists to ensure continuity of care when they are unavailable to care for you. Our con-sult rooms provide you the opportunity to see specialists like cardiologists, surgeons, neurologist in your own neighborhood. You can get your blood tests, urine tests, ECGs, X rays, vaccination etc done at any time convenient to you as we are 24 hours open. Urgent care centre Hospitals have treatment beds and patients can be admit-ted for treatments required. Some patients may require transfer to higher facility if they need any specific intervention like major surgery, angioplasty etc. Our team and ambulance service ensures that you reach the right facility in a timely and safe manner. Urgent Care centre Hospitals are your neighborhood healthcare providers!
Future Plans?UCC plans to have 30/34 UCC Hospitals in Delhi NCR, 20 in Kolkata and a total of 110 in North & East India covering Tier 2 & 3 cities like Varanasi, Patna, Allahabad, Kanpur etc.
This will lead to Immediate Care within walking distance in local neighbourhoods. Build a team of trained Emergency Doctors, Nurs-es and EMT’s
Affordable & Accessible Urgent CareComplement the Family Doctors role in providing good immediate care for their patients 24x7The Model Can be tweaked to cater to local health & disease profiles
Indian Healthcare Industry – Future?The healthcare sector by definition, is wide andencompasses pharmaceuticals, manufacturing and sup-ply of medical equipment and ancillary supplies, hospital care,pathology services, diagnostics, clinical research, telemedicine and specialty health care.
As per research reported on India Brand Equity Founda-tion website, the Indian healthcare industry is expected to reach USD 79 billion in 2012 and USD 280 billion by 2020. Further, the hospital services market, which represents one of the most important segments of the Indian healthcare industry, is expected to be worth US$ 81.2 billion by 2015.
The Indian healthcare industry is unique as compared to other developed and developing economies in that it has the challenge of meeting the needs of the second-most populous country in the world, while private spending on healthcare remains one of the highest as compared to other developed and emerging economies.
What is Urgent Care?
INTERVIEW

28 May-June 2013
Encephalitis in Children
Encephalitis literally means an inflammation of the brain. In most cases, this inflammation is caused by a virus. Encephalitis is a rare disease that occurs in approximately 0.5 per 100,000 individuals — most commonly in children, the elderly, and people with weakened immune systems (e.g., those with HIV/AIDS or cancer).
Although several thousand cases of encephalitis (also called acute viral encephalitis or aseptic encephalitis) are reported to the Centers for Disease Control and Prevention (CDC) every year, experts suspect that many more go unreported because the symptoms can be very broad.
Signs and SymptomsSymptoms in milder cases of encephalitis usuallyinclude:• fever • headache • poor appetite • loss of energy• a general sick feeling
In more severe cases of encephalitis, a person is more likely to experience high fever and any of a number of symptoms that relate to the central nervous system, including:• severe headache • nausea and vomiting • stiff neck• confusion • disorientation • personality changes• convulsions (seizures) • problems with speech or hearing • hallucinations • memory loss • drowsiness • coma
It’s harder to detect some of these symptoms in infants, but important signs to look for include:• vomiting• a full or bulging soft spot (fontanel)• crying that doesn’t stop or that seems worse when an infant is picked up or handled• body stiffness
Because encephalitis can follow or accompany common viral illnesses, there sometimes are signs and symptoms of these illnesses beforehand. But often, the encephalitis appears without warning.
The diagnosis of encephalitis is made after the sudden or gradual onset of specific symptoms and after diag-nostic testing. During the examination, your child’s doctor obtains a complete medical history of your child, including his or her immunization history. Your child’s doctor may also ask if your child has recently had a cold or other respiratory illness, or a gastrointestinal illness, and if the child has recently had a tick bite, has been around pets or other animals, or has traveled to certain areas of the country.
Diagnostic tests that may be performed to confirm the diagnosis of encephalitis may include the following:• X-ray - A diagnostic test that uses invisible electro-
How is encepha-litis diagnosed?
28 May-June 2013
SPEAKDOCTOR
Dr. Rajiva KumarChild Specialist, Muzaffarpur

magnetic energy beams to produce images of internal tissues, bones, and organs onto film.• Magnetic resonance imaging (MRI)- A diagnostic procedure that uses a combination of large magnets, radiofrequencies, and a computer to produce detailed images of organs and structures within the body.• Computed tomography scan (also called a CT or CAT scan) - A diagnostic imaging procedure that uses a combination of X-rays and computer technology to produce horizontal, or axial, images (often called slices) of the body. A CT scan shows detailed images of any part of the body, including the bones, muscles, fat, and organs. CT scans are more detailed than general X-rays.• Blood tests • Urine and stool tests • Sputum culture - A diagnostic test performed on the material that is coughed up from the lungs and into the mouth. A sputum culture is often performed to deter-mine if an infection is present.• Electroencephalogram (EEG)- A procedure that records the brain’s continuous, electrical activity by means of electrodes attached to the scalp.• Lumbar puncture (spinal tap). A special needle is placed into the lower back, into the spinal canal. This is the area around the spinal cord. The pressure in the spinal canal and brain can then be measured. A small
amount of cerebral spinal fluid (CSF) can be removed and sent for testing to determine if there is an infection or other problems. CSF is the fluid that bathes your child’s brain and spinal cord.• Brain biopsy - In rare cases, a biopsy of affected brain tissue may be removed for diagnosis.
India develops world’s first JEvaccineThe world’s first vaccine against Japanese Encephalitis (JE), created using an Indian strain of the virus, is now ready.
National Institute of Virology (NIV), Pune had provided Bharat Biotech with a strain of the JE virus collected from Kolar in Kar-nataka — a hotbed for JE infections, for the vaccine. Bharat has just submitted the re-sults from the final human trials to the drug controller general of India for marketing clearance.
SPEAKDOCTOR
May – June 2013 29

30 May-June 20133030
STORYCOVER

May – June 2013 31
Hospital FurnitureDesign, Development and ChallengesManufacturers of hospital furniture are updating theirproduct designs to meet new demands in health careenvironments. One big consideration is the creation of afamily-friendly hospital experience for the relatives and friends of patients. Other areas of emphasis includeaesthetics, ease of cleaning, sustainability, ergonomics and furnishings for large people.
MEDGATE recently discussed these trends with manufacturers of hospital furniture.
STORYCOVER

32 May-June 201332
STORYCOVER

May – June 2013 33
STORYCOVER
Manufacturers are incorpor¬ating aesthetics into their designs to make their products look “homey.” The goal is to combine functionality with beauty. Given the realities of the hospital environment, however, this can be tricky.
Expert says that successful health care facilities incorporate a warm and inviting atmosphere where patients and guests can relax. In making furni-ture selections, however, facilities must take into account the wear and tear and number of guests using each space.
“A facility manager should consider an integrated look throughout waiting areas, treatment rooms and corridors,” he says. “Incorporating color waves and collection styles and determining whether a facility is traditional or contemporary—or some-where in between—goes a long way toward es-tablishing a facility’s overall look and experience, making it feel more like home.”
According to Industry ., updated designs can help take the edge off the clinical look of hospital furni-ture. So the company regularly reviews its recliners.
Hospital Furniture concept“If we find more aesthetically pleasing components that can support the clinical purpose of the chair without compromising function or performance, we will use them. The company also strives to bal-ance price point with aesthetics.
“We can make a fabulous ‘designer’ chair that no one can afford. So it’s a matter of balancing prior-ities with patient and staff safety our highest pri-ority.” strives to design products that have strong aesthetic appeal and a design that puts people at ease and makes them think less about the environ-ment they’re in.
“When facility managers tell designers or architects they want a ‘homey’ environment, they really mean they want an environment that supports the heal-ing process,” says Phyllis Goetz, vice president of sales.
“They want the same feeling of comfort they would have at home.”

34 May-June 2013
STORYCOVER
Family friendlyFurniture manufacturers also are incorporating family-friendly features into their products. The goal is to make families comfortable when they stay all day or overnight. This consideration is especially important when furnishing patient rooms.
Sleepers accommodate hospital guests and patients. Featuring plush cushions and easy pulloutmechanisms, they are designed for tight-fitting spaces. They combine the comfort of an easy chair with the pullout functionality of a sleeper sofa.
Any sleeper can be folded up as a guest chair or opened for overnight visits.
Keeping it cleanEase of cleaning is another importantconsideration, given the hospital environment and preponderance of stains it can inflict on furniture. Plastic arm caps and metal frames to accommodate rigorous cleaning demands.
“Design alternatives to maintain sanitaryconditions include upholstery choices that are easy to clean and help prevent infiltration of moisture and bacteria “Available furnishing options also feature antimicrobial properties, moisture barriers and seamless construction.”
Champion designs its recliners with an “openconcept” that allows bodily fluids to fall to the ground, which facilitates cleanup and dis-infection. A removable seat (standard on all medical reclin-ers) is also helpful, and when paired with a swing-away arm, helps achieve infection control.
“Improving a hospital experience for patients and em¬ployees starts by taking the work out of clean-ing and maintenance and allotting it to patient care,”
34
STORYCOVER

May – June 2013 35
Indeed, many environmental friendly initiatives are being incorporated into hospital furniture design. The goal is to achieve sustainability and good indoor air quality. Recycling also is important as suppliers strive to use materials that can be recycled at the end of aproduct’s lifecycle.
“[Sustainability] has become a big factor for health care and in virtually all facilities over recent years and will continue to gain momentum.In furniture design, sustainability and indoor air quality of the end-user environment are focal points to ensure that furnishings are not detrimental to caregivers, patients and the heal-ing process.”
The trend is for hospital purchasing departments to be environmentally responsible when deciding which products to acquire.
One example of green design ,which uses paints that contain no volatile organic compounds (VOCs) in its hospital lockers, thus providing healthy air quality for the life of the product. “This is an important im-provement in hospital facilities.”The antimicrobial, silver-based compound is inorganic and protects against mold, bacteria and some facility-born viruses.” As a result, the lockers are easily cleaned with a mild soap. No harsh chemicals are required.
Another example is hospital furniture manufactured which incorporates zero urea-formaldehyde and low-VOC finishes, promoting healthy indoor air quality, With an eye on the indoor environment, the company uses water-based adhesives for laminate application and water-based wood glue on all joints to ensure no odor or VOC emissions. The UV finish on plywood is 99 percent solids, which nearly eliminates off-gassing once the finish is cured.
‘Green’ initiatives
STORYCOVER

36 May-June 2013
Another trend is growth in the area of ergonom-ics. “In the health care arena, ergonomic furnish-ings are more critical than ever—from specialized seating used in the operating room to that used by patients post-surgery, as today’s re¬covery regi-mens mandate patients sit up sooner and for longer periods of time.
Ergonomic features also are designed for hospital employees, allowing them to work more efficiently and injury-free.
Back talk“You can look at ergonomics in two ways—prod-ucts that are designed to support the way people move; you also can look at ergonomics from a safety perspective—are we keeping patients, their families and the staff safe during their time in a health care facility
36
STORYCOVER

May – June 2013 37
Bariatrics is anotherimportant factor in hospital furniture design.Considerations for thispatient segment continue to rise. The goal is to meet the needs of large patients in a safe and re-spectful manner.
“Bariatrics is an important element of furniture design. “Patients are getting bigger and heavier. We are seeing higher weight requirements. In fact, 500-pound-weight-capacity chairs are becoming popular. Hospitals are even asking for 750- or 1,000-pound capacity.” Larger arms are critical on bariatric seating, so that bariatric patients can grab them to keep their balance, Miles notes.
Oversized chairs should be available in public
Challenge of the industryareas such as lobbies and waiting rooms as well as examination rooms and other patient areas.
“Many hospitals have a room or two on each wing specially designed for this type ofpatient.
“These rooms require larger beds, tables, seating and lifting equipment … not to mention specialty bathroom design and fixtures. Larger capacity recliners and patient chairs for bariatric patient rooms are a popular request.”Furniture manufacturers must meet the needs of large patients in a safe and respectful manner, while preventing injuries to staff that assist them. Bariatric patients are often frail and need special consideration during handling.
STORYCOVER

38 May-June 2013
Gum DiseaseConsiderations:
Gum disease is basically an infection of your gums, where the bacterial infection might cause gum swelling, and even very dangerous scarring to the gum tissue.
When the gums are not healthy, they will start re-tracting, and then the teeth become lose in the pock-ets. This is when the teeth might be permanently lost, because they cannot be kept stable by the gums.
Gum disease is a condition which is actually caused by excess plaque buildup. The plaque is an extremely sticky film of bacteria that cover the teeth.
CAREDENTAL
‘Gum disease affects so much more than just your dental health, and this is a widely accepted statement by the best dental health specialists’
Whenever you consume foods or drink beverages, the tooth enamel is destroyed little by little because of the acids that are released by the dental plaque. All these problems can be nicely avoided if you make sure to get regular professional dental cleanings.
You need to make sure to respect proper dental hy-giene by brushing and flossing your teeth, plus get-ting dental cleanings at regular intervals. When too much tartar builds up, your gums will be extremely affected.
BeyondDental Health

May – June 2013 39
CAREDENTAL
The gums can actually retract or become separat-ed from the teeth, and then very deep pockets will form between your teeth and gums. Within these pockets, the bacteria can thrive and cause a lot of damage not only to your dental health, but overall health.
Gingivitis and periodontitis are the two main stages of gum disease. Gingivitis is the milder complica-tion when your gums start bleeding, and your gums are reddish and inflamed. At this point, you can re-vert back to good health if you get proper treatment.When periodontitis sets in, it is not only your gum-line which has to suffer, but also your bones and tis-sues. Permanent tooth loss can happen if periodon-titis is not treated properly.
Possible health complica-tions caused by gumdisease:Problems with diabetes- When the blood sug-ar levels are not managed properly, you are exposed to a very high risk of developing periodontitis. This is why patients with diabetes are most likely to de-
velop periodontitis. These patients should get deep dental cleanings more often than a patient without diabetes.
Complications during pregnancy- statistics show that women who develop gum disease during their pregnancy, are exposed to a very high risk of low birth weight of their baby, or even preterm birth.
Women should pay attention to these complications and:• get a thorough dental checkup before becoming pregnant- the dentist will perform all the necessary dental treatments, and perform a thorough profes-sional dental cleaning• If you have just found out that you are pregnant, you should make a dental appointment for dental cleaning, to eliminate the plaque already deposit-ed. Prevent future tartar deposits by checking often with your dentist during pregnancy, and of course by respecting a thorough daily dental care regimen
Lung disease complications- when the tartar and plaque bacteria are not cleaned proper from the surface of your teeth, you will inhale those harm-ful bacteria. This can lead to complications such as pneumonia, or COPD (Chronic Obstructive Pul-monary Disease).
‘You need to make sure to respect proper dental hygiene by brushing and flossing your teeth, plus getting dental cleanings at regular intervals’.
40 May-June 201340 May-June 2013
LINEPRODUCT
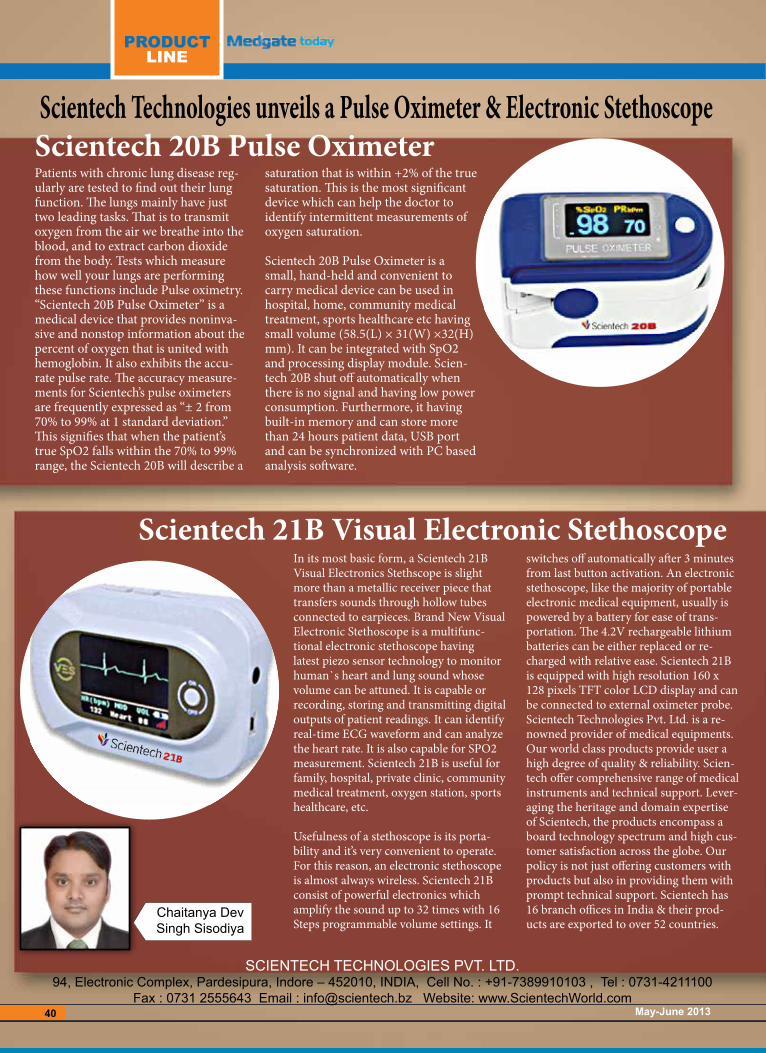
Scientech Technologies unveils a Pulse Oximeter & Electronic Stethoscope
Patients with chronic lung disease reg-ularly are tested to find out their lung function. The lungs mainly have just two leading tasks. That is to transmit oxygen from the air we breathe into the blood, and to extract carbon dioxide from the body. Tests which measure how well your lungs are performing these functions include Pulse oximetry. “Scientech 20B Pulse Oximeter” is a medical device that provides noninva-sive and nonstop information about the percent of oxygen that is united with hemoglobin. It also exhibits the accu-rate pulse rate. The accuracy measure-ments for Scientech’s pulse oximeters are frequently expressed as “± 2 from 70% to 99% at 1 standard deviation.” This signifies that when the patient’s true SpO2 falls within the 70% to 99% range, the Scientech 20B will describe a
saturation that is within +2% of the true saturation. This is the most significant device which can help the doctor to identify intermittent measurements of oxygen saturation.
Scientech 20B Pulse Oximeter is a small, hand-held and convenient to carry medical device can be used in hospital, home, community medical treatment, sports healthcare etc having small volume (58.5(L) × 31(W) ×32(H) mm). It can be integrated with SpO2 and processing display module. Scien-tech 20B shut off automatically when there is no signal and having low power consumption. Furthermore, it having built-in memory and can store more than 24 hours patient data, USB port and can be synchronized with PC based analysis software.
Scientech 21B Visual Electronic Stethoscope In its most basic form, a Scientech 21B Visual Electronics Stethscope is slight more than a metallic receiver piece that transfers sounds through hollow tubes connected to earpieces. Brand New Visual Electronic Stethoscope is a multifunc-tional electronic stethoscope having latest piezo sensor technology to monitor human`s heart and lung sound whose volume can be attuned. It is capable or recording, storing and transmitting digital outputs of patient readings. It can identify real-time ECG waveform and can analyze the heart rate. It is also capable for SPO2 measurement. Scientech 21B is useful for family, hospital, private clinic, community medical treatment, oxygen station, sports healthcare, etc.
Usefulness of a stethoscope is its porta-bility and it’s very convenient to operate. For this reason, an electronic stethoscope is almost always wireless. Scientech 21B consist of powerful electronics which amplify the sound up to 32 times with 16 Steps programmable volume settings. It
switches off automatically after 3 minutes from last button activation. An electronic stethoscope, like the majority of portable electronic medical equipment, usually is powered by a battery for ease of trans-portation. The 4.2V rechargeable lithium batteries can be either replaced or re-charged with relative ease. Scientech 21B is equipped with high resolution 160 x 128 pixels TFT color LCD display and can be connected to external oximeter probe.Scientech Technologies Pvt. Ltd. is a re-nowned provider of medical equipments. Our world class products provide user a high degree of quality & reliability. Scien-tech offer comprehensive range of medical instruments and technical support. Lever-aging the heritage and domain expertise of Scientech, the products encompass a board technology spectrum and high cus-tomer satisfaction across the globe. Our policy is not just offering customers with products but also in providing them with prompt technical support. Scientech has 16 branch offices in India & their prod-ucts are exported to over 52 countries.
Scientech 20B Pulse Oximeter
SCIENTECH TECHNoloGIES PVT. lTD.94, Electronic Complex, Pardesipura, Indore – 452010, INDIA, Cell No. : +91-7389910103 , Tel : 0731-4211100
Fax : 0731 2555643 Email : [email protected] Website: www.ScientechWorld.com
Chaitanya Dev Singh Sisodiya


42 May-June 201342
VIEWSEXPERT
Hospitals in India have a high burden of infections in their intensive care units (ICU) and general wards, many of which are resistant to antibiotic treatment, according to a report by Global Antibiotic Resistance Partnership (GARP) – India Working Group and Centre for Disease Dynamics, Economics and Policy (CDDEP). The 2011 GARP report, Situation Analysis: Antibiotic Use and Resistance in India, also states that a large proportion of these hospital-acquired infections (HAI) are preventable with increased infection control measures.
Antibiotic resistant infections are difficult, and sometimes impossible, to treat. They lead to longer hospital stays, increased treatment costs, and in some cases, death. The GARP research estimates that of the approximately 190,000 neonatal deaths in India each year due to sepsis – a bacte-rial infection that overwhelms the bloodstream – over 30 per cent are attributable to antibiotic resistance. Antibiotic resistant hospital infections can be especially deadly because antibiotics are used intensely in hospitals compared with the community, and frequent use drives the development of highly resistant bacteria. “A large proportion of these hospi-tal infections are easily preventable with increased hospital infection control, including stepping up hygiene practices, such as frequent hand-washing,” says Dr Ramanan Laxmi-narayan, Director of CDDEP and vice president for research and policy at the Public Health Foundation of India.
Organisms causing hospital infections in India are similar to those around the world, with S. aureus and P. aerugino-sa among the most common disease-causing pathogens. A prospective study of 71 burn patients at Post Graduate Institute of Medical Education and Research (PGIMER) in Chandigarh found that up to 59 patients (83 per cent) had hospital-acquired infections: 35 per cent of pathogens isolated from wounds and blood were S. aureus, 24 per cent were P. aeruginosa, and 16 per cent were β-haemolytic streptococci. Research on hospital infections in India reveals several concerning trends. In Indian ICUs, the rate of vanco-mycin-resistant enterococcus (VRE), a dangerous hospital infection, is five times the rate in the rest of the world. Rates of methicillin-resistant Staphylococcus aureus in Indian ICUs are also high, with one study finding over 80 per cent of S. aureus samples testing positive for resistance to methi-cillin and closely related antibiotics.Another six-month study conducted in 2001 of the intensive care units (ICUs) at All India Institute of Medical Sciences (AIIMS) in New Delhi, found that 140 of 1,253 patients (11 per cent) had 152 hospital-acquired infections, where P. aeruginosa made up 21 per cent of isolates, 23 per cent were
ICU infections- a scrouge that needs to be controlled
S. aureus, 16 per cent Klebsiella spp., 15 per cent Acinetobacter baumannii and 8 per cent Escherichia coli. Further, a study of 493 patients in a tertiary teaching hospital in Goa also found that 103 people (21 per cent) developed 169 infections.In India, however, hospitals often do not follow infection control practices, and this leads to the spread of disease. In response to the growing burden of HAIs in India, GARP is issuing several key recommendations that aim at reducing the prevalence of HAIs, including increased hand-washing, use of isolation rooms for infected patients, increased availability and uptake of diag-nostic tests, reminders to limit catheter use, and use of gloves and gowns. The ministry of health and family welfare task force also recommends that all hospitals create an infection control plan, committee and team.
“Surveillance of antibiotic resistance, combined with tracking physician prescribing patterns, can be the foundation of success-ful infection control programme in hospitals. But surveillance is a challenge in many places, where microbiology laboratories and trained staff may be unavailable,” says Dr Laxminarayan. Infection control committees may also be met with uncooper-ative hospital staff and administrators. “The greatest challenge is to empower infection control committees and make hospital staff aware of their activities and recommendations,” adds Dr Ramanan Laxminarayan. In all these instances it has been found that existing infection control practices such as Hand washing and judicious use of Disinfectants to clean the equipment is of limited benefit. The
Dr. Anukant Mital

May – June 2013 43
VIEWSEXPERT
most commonly implicated method of transmission of infection wiyhin such closed environments such as the ICU is the Touch Surface. These Touch Surfaces comprise of all the material in the ICU that is commonly handled by all the medical and Paramedi-cal staff as well as visitors and the patients themselves.Disinfection of these touch surfaces made of conventional ma-terials do not remain sterile for long and in fact act as reservoirs of infection causing Bactria, fungi and viruses. Objects in closest proximity to patients have the highest levels of staphylococcus, MRSA, and VRE. This is why touch surfaces in hospital rooms can serve as abundant sources, or reservoirs, for the spread of bacteria from the hands of healthcare workers and visitors to pa-tients. However if the surfaces are made of the Alloys of Copper containing at least 60% of copper then they automatically elimi-nate all forms of organisms, becoming sterile within few hours.Studies being conducted at the University of Southampton in the United Kingdom are proving that copper and its alloys, brass and bronze, effectively eliminate bacteria and viruses that cause illness. The research has also shown that conventional touch surfaces do nothing to help eradicate germs. Once contaminated, a stainless steel doorknob, faucet or handrail can harbor bacteria and viruses until it is disinfected, usually with harsh chemicals, even then the organisms would survive in the micro Scratches on their surfaces.. However, uncoated copper, including brass and bronze alloys with high copper content, are intrinsically antimi-crobial and begin eliminating pathogens such as streptococcus, staphylococcus and Influenza A on contact. Microorganisms are known to survive on inanimate ‘touch’ surfaces for extended periods of time.[4] This can be especially troublesome in hospital environments where patients with immunodeficiencies are at enhanced risk for contracting nosocomial infections (hospi-tal-borne infections), often with fatal consequences.Touch surfaces commonly found in hospital rooms, such as bed rails, call buttons, touch plates, chairs, door handles, light switches, grab rails, intravenous poles, dispensers (alcohol gel, paper towel, soap), dressing trolleys, and counter and table tops are known to be contaminated with high levels of potentially dangerous bacteria, including Staphylococcus, Methicillin-re-sistant Staphylococcus aureus (MRSA), one of the most virulent strains of antibiotic-resistant bacteria and Vancomycin-resistant Enterococcus (VRE). According to Dr. Harold Michels of the Copper Development Association, which is sponsoring the studies, suggests using copper, brass or bronze for doorknobs and handles, push plates, countertops, sinks and other frequently touched hardware may help cut down on cross-contamination and the spread of infection. Recently, to evaluate their effective-ness as secondary infection control measures, these products have been made from copper and its alloys and deployed in hospital geriatric wards, intensive care units, and general medical wards around the world. Clinical trials are being conducted on microbial strains unique to individual healthcare facilities around the world to evaluate to what extent copper alloys can reduce the incidence of infection in hospital environments. The success of these clinical trials to date, which are summarized here, are prompting hospitals around the world to specify anti-microbial copper touch surfaces as an additional weapon in the fight against infection.
Clinical Trials in the USAIn the USA, a high degree of statistical significance is needed
to provide a convincing argument to U.S. federal government healthcare authorities, such as the Centers for Disease Control and Prevention (CDC), regarding the effectiveness of copper alloys in reducing microbial loads and cross infection in health-care environments. For this reason, clinical trials at three major US hospitals examined environmental bacterial loads, infection rates, and impacts on cross-contamination in intensive care unit (ICU) rooms retrofitted with copper touch surfaces versus rooms without copper surfaces.The trials were funded by the U.S. Department of Defense (DOD) under the Telemedicine and Advanced Technologies Research Center (TATRC), a section of the United States Army Medical Research and Materiel Command (USAMRMC). DOD has extraordinary interests in the potential for antimi-crobial copper surfaces to reduce hospital-acquired infections because it wants to prevent hospital-acquired infections among thousands of its enlisted armed forces servicemen and service-women who have been injured in recent conflicts. TATRC, which funds a Military Infectious Disease Program. The studies are coordinated through the Advanced Technology Institute in Charleston, South Carolina. The clinical studies involve in-tensive care units (ICUs) at Memorial Sloan-Kettering Cancer Center in New York City, one of the world’s most prestigious cancer facilities, the Medical University of South Carolina, and the Ralph H. Johnson VA Medical Center in Charleston, South Carolina. An evaluation of the microbial burden of various objects in the ICU rooms has been documented and is available. Early results disclosed in 2011 indicate that the coppered rooms demonstrated a 97% reduction in surface pathogens versus the non-coppered rooms. This reduction is the same level achieved by “terminal” cleaning regimens conducted after patients vacate their rooms. Furthermore, of critical importance to health care professionals, the preliminary results indicated that patients in the coppered ICU rooms had a 40.4% lower risk of contracting a hospital acquired infection versus patients in non-coppered ICU rooms.. The final analysis indicated that the infection rate in the ICU areas where almost all the targeted bed units and equipment was made from Copper Alloys the Infection rate was lower by as much as 69%. The U.S. Department of Defense investigation contract, which is ongoing, will also evaluate the effectiveness of copper alloy touch surfaces to prevent the transfer of microbes to patients and the transfer of microbes from patients to touch surfaces, as well as the potential efficacy of copper-alloy based components to improve indoor air quality.
Clinical Trials in India Considering that infections in the ICU environment leads to major costs escalation and poor outcomes in treatment in In-dia, in Jan 2013, it was decided to run a Pilot study in the ICU of one of the Major Cancer Hospitals in Mumbai. Retrofitting of the bed units in ICU ward of 4 beds was done for the bed rails, the foot rails, the bedside Table, the overbed table and the IV stand as well as the top surface of the dressing trolley in the ICU. A similar unit of 4 beds across the passage was used as the control where no retrofitting was done. Swab samples from the touched areas were collected and plated to check for colonies that grow. The data collected is now being studied for the total no of Colony Forming Units( CFUs) from both the ICU areas and the results are awaited.

44 May-June 2013
VIEWSEXPERT
There has been a considerable rise in prevalence of Diabetes across the
world. As per the world health statistics 2012, one in every 10 adults is diabetic with figure increasingly rising among the youth due to unhealthy lifestyle and lack of exercise in their daily routine.The rising trend of weight gain coupled with lack of physical exercise and high level of mental stress in school going children acts as a precursor of future diabetes in them at a younger age particularly in those children who also have a family history of diabetes.
More than 346 million people world-wide are currently suffering from diabetes; and this malady is predicted to become the seventh leading cause of death in the world by the year 2030.Unfortunately, India has one of the largest number of diabetic patients in the world (62.4 million people live with diabetes in India & there are 77.2 million people with pre-diabetes). It is
estimated that every fifth diabetic in the world would be an Indian. The disease is such that it cannot be cured making it all the more important to actively manage it. According to the World Health Orga-nization, every year,35 million people die because of diabetes. 80% of these diabetes deaths worldwide occur in low- and middle-income countries with people aged between 35 and 64 years.While there is one person in the world dying of diabetes every ten seconds, two new diabetic cases in the world are being identified every ten seconds.Additionally, by the year 2025, there will be seven million new diabetic cases in the world.Currently India is facing an epidemic of diabetes, with a high prevalence in urban areas. Over the past 30 years, the prevalence of diabetes has increased to 12-18% in urban India and 3-6% in rural India with significant regional variations. Moreover, IGT (Impaired Glucose Tolerance) is a mounting prob-lem in India and another 14% of the Indian population has pre-diabetes in India, a harbinger of future diabetes. The need to better manage & control the rapid rise of diabetes has led to innovations in Diabetes monitoring and management therapies to help patients & physicians to better manage the chronic disease with more scientific and accurate results.People with type 1 diabetes and many people with type 2 disease require treatment with insulin to control blood sugar and reduce the risks of complica-tions, including blindness, heart disease and nerve damage leading to ampu-tations. The main aim of treatment of diabetes is to achieve blood glucose in order to prevent acute and chronic complications, improve quality of life and avoid premature diabetes associat-ed deaths.
Research in the diabetes field has taken two main directions: innovations aimed at improving current management methods, and exploring radical new approaches. Improvements in current therapy include making glucose moni-
Frequent Diabetes Monitoring & Intensive Management to Rise
Diabetes Management Future Trends
Dr. Shashank R JoshiMD, DM, FRC, FACP, FACE
President, Indian Academy of DiabetesConsultant Endocrinologist, Lilavati and
Bhatia Hospital, Mumbai

May – June 2013 45
VIEWSEXPERT
toring and insulin delivery less invasive and more patient-friendly, and many significant advances have been made in this context in the past two decades. Among these have been the develop-ments of improved glucose monitoring techniques and minimally-invasive techniques for sampling blood. New, fast-acting forms of insulin have also been introduced along with novel, and more accurate, ways of insulin delivery through the use of insulin pumps. There has also been considerable research in non-injection dosage forms for insulin, such as inhalable insulin, although products are not approved and pend-ing more clinical data.Once approved, this could herald a new era in Insulin Therapy.
Recent Trends in Diabetes Monitoring & Diagnosis:Blood sugar of a person without diabetes is maintained by the body within a normal range irrespective of the amount of food that is consumed by a person. In patients having diabe-tes, blood sugar spikes within an hour after any meal. This process goes on throughout the day. So the blood sugar of a person with diabetes is continu-ously changing every minute of the day throughout the person’s life. Patients may use glucometers to check blood sugar, but this gives the value of blood sugar only at the particular time when the test is done. However, since blood sugar levels of a patient are changing from minute to minute, checking sim-ply with Blood Glucose Meters may not be sufficientHowever a more effective way to mon-itor sugar levels to understand how the blood sugar is changing throughout the day is with the help of a technology called Continuous Glucose Monitor-ing System (CGMS), whichis now also available in India. CGMS is done with the monitor (like ipro 2 etc.) which is attached to the abdominal wall. It reads the sugar levels of the person every 10 seconds and keeps a record every five minutes so that we can get 288 readings per day during the CGMS study period. This data is uploaded on a computer
and the data is clearly visible in the form of a graph which any one can understand. The patient gets to see how his or her blood sugar has moved after each and every meal of the day. This gives the person a clear idea as to how much the blood sugar has risen after a partic-ular meal. The patient can then take corrective measures regarding food intake. The doctor can make out how a particular patient’s blood sugar is changing throughout the day. There are plenty of patients who have high blood sugar at odd times of the day which is not detected by the routine tests like Fasting blood sugar and PPBS (blood sugar after food) or who are unaware that they may be experiencing low blood sugars at night. With this information the doctor can modify the treatment to get better control of blood sugar throughout the day.For patients who are suffering from Gestational Diabetes and patients with diabetes who are planning pregnancy, it is absolutely vital that the blood sug-arsare very tightly controlled through-out the pregnancy. The consequences of poor control can be grievous to the mother and fetus. So, in patients with diabetes who are planning pregnancy it is extremely useful to get a CGMS done and get a correct picture of the blood sugar pattern.Low blood sugar especially at night may go unnoticed and this is clearly picked up by a CGMS study. HbA1c (Glycosylated Hemoglobin) is a very useful test to detect how well blood sugar is controlled over the pre-vious three months. HbA1c indicates the average blood sugar and so it does not give a correct picture of how much fluctuation occur. In fact, if a patient has frequent low blood sugar, it could result in low HbA1c (because HbA1c denotes an average value) and a false sense of security to the patient and doctor, even when the blood sugar is often high and is actually poorly con-trolled. CGMS is a useful tool to detect this disease.Another new upcoming diabetes mon-itoring approach is the use of Implant-
able Chips. A microchip can detect the amount of glucose in a person’s blood and will then transmit this information to a wireless scanner where it can be easily read by the patient. All it will require are some basic instructions, and monitoring one’s own glucose level with this product will be simple and accu-rate. This innovative little device serves as an alternate for the aid of glucose monitoring.
Recent Trends in Diabetes Manage-ment:Insulin therapy is one of the corner-stones of diabetes management, and its efficacy in early and in late-stage diabetes is well-established. Yet, the first choice of doctors in India for most diabetics has so far been to attempt sugar control through OADs (Oral An-ti-Diabetics), diet control, exercise and lifestyle changes. One of the key reasons for delaying control through insulin is the resistance and fear in patients, of taking injections daily, particularly self-administering the same. For Type 1 Diabetes where insulin is required to manage the condition, the traditional diabetes management is done by delivering insulin through Multiple Daily Injection (MDI) through devices such as Insulin pens and Insulin Injections are also available for self-management for Diabetes in India. An excellent alternative to multi-ple daily injections is Insulin Pump Therapy. By using an insulin pump, patients can match their insulin to their lifestyle rather than trying to adjust their lifestyle to their body’s response to insulin injections. People of all ages, who require insulin to manage their diabetes, can get benefit from this novel therapy.Insulin pumps are being more com-monly used because of their unique ability to continuously infuse insulin, closely mimicking the behavior of phys-iological secretion from a normal pan-creas.Just as a healthy pancreas delivers insulin automatically, every seven to ten minutes throughout the day, an insulin pump matches the natural rhythm of a healthy pancreas, which is nearly

46 May-June 2013
VIEWSEXPERT
impossible for people using tradition-al injection therapy. In brief, insulin pumps consist of: (a) the pump (com-puterized battery operated device); (b) a disposable reservoir to hold insulin; (c) a disposable infusion set, including a soft plastic cannula to be inserted just below the skin). The insulin pump is a small mechanical device that is worn outside the body, often on a belt or in a pocket. The pump delivers insulin directly into the body through the soft, flexible cannula under the skin. Patients generally refill their pump with insulin every two to three days. Scientific evidences from published studies have also proven added ben-efit of insulin pumps in improving quality of life, normalizing sugars in recalcitrant diabetes, improving sexual function, and relieving the intractable pain of neuropathyPump therapy allows people with dia-betes to adjust insulin intake easily to keep glucose levels within a near-nor-mal range. An insulin pump is an excellent tool for helping improve gly-cemic control. Tight glycemic control is central to good health, as proven by nu-merous studies, including the landmark Diabetes Control and Complications Trials (DCCT). In that study, patients who maintained near-normal glycemic control significantly reduced their risk of long-term complications. The risk of diabetic eye disease decreased by up to
76 per cent, nerve disease was reduced by up to 60 per cent, and kidney com-plications were reduced by up to 56 per cent. A pump can help patients avoid hyperglycemia (high blood sugar), which can cause long-term complica-tions and lead to ketoacidosis (causing coma or death if left untreated), and hy-poglycemia (low blood sugar), an acute condition that can be very dangerous, particularly while sleeping.
With a pump, people can also be more flexible. Patients using longer-acting insulin with injection therapy must follow rigid schedules of insulin injections, meals and snacks, whereas patients using an insulin pump can programme insulin delivery when they eat, and adjust or stop insulin delivery for exercise or other needs. Patients using pump therapy can eat what they want, when they want - something almost unheard of in patients treating their condition with traditional insulin injections. Pumps are also beneficial for patients who are unable to manage their diabetes or related complications.Currently, approximately 500,000 people worldwide are using insulin pump to manage diabetes; however, despite India’s claim of educational achievement and economic progress, the benefits of insulin pump therapy have reached only a fraction of people with diabetes, who rightly deserve such
innovative therapy. Advanced Insulin Pump technology like MiniMed VEO, is the world’s one of the new insulin pump which can automatically shut-off the supply of insulin, if the patient’s glucose levels drop too low, protecting against dangerous, and potentially life threatening, hypoglycemia(Low Glu-cose Suspend). The Insulin pump, when used with an integrated glucose sensing technology, monitors the patient’s glucose levels 24 hours a day and can actively protect the patient against the risk of a hypoglycemic event becoming severe, even while the person is asleep. This new therapyalso has a range of simple alerts to help patients act to keep their glucose level stable, providing the best possible chance of staying safe and avoiding highs and lows. This new technology, which is now also available in India, gives greater freedom in eating and sleeping. At the same time it takes the stress and fear out of diabetes management for its capacity to protect against the dangers of hypogly-cemia.The reasons for the poor utilization of insulin pump therapy in India include lack of awareness among doctors and patients, affordability concerns, lack of proper diagnostic infrastructure, and lack of reimbursement. As a greater number of doctors in India begin to be more aware of such advance thera-pies, they will be able to educate more Indians on the causes, prevention and management of diabetes. The success of insulin pump therapy depends on selec-tion of the right candidate, extensive ed-ucation, motivation, and implementing the sophisticated programs with skill. So far, while diabetes does not have a cure, diabetes management with the help of education, correct diet and ex-ercise, medication (oral hypoglycaemic agents and/or insulin), glucose monitor-ing, and modern technology have made managing diabetes better and simpler. However, finding a permanent cure for the disease will be one of the greatest breakthroughs in medical science. Some animal studies have shown promising results and there seems to be hope for curing diabetes in the future.

May – June 2013 47
Apple iPhone/iPad/Android/Windows 8 and WebIs now available on
Magazine
Download and read it on
Magzter
From your Apple iPad please go toApp store and search for
Magzter
From your Android Tablet please go toGoogle Play and search for
Magzter
From your Windows8 device please go toWindows Store and search for
Magzter
48 May-June 201348 May-june 2013
TENDERS
Ref Number: 8116136 Tender Number: Buyer/Seller: Military Engineer Services Requirement: Provision of Deficient intensive care facility of 04 beds at INHS JeevantiLocation: Goa - Goa - India Document Fees: Rs.2,000 EMD: Rs.396,000 Estimated Cost: Rs.32,100,000 Closing Date: 28/06/2013 at 00:00 Hrs. Contact Details: Military Engineer ServicesMumbai, Maharashtra, India Document Sale From: 13-5-2013________________________________________
Ref Number: 8128948 Tender Number: Buyer/Seller: Rajasthan Medicare Relief Society Requirement: Supply of High Pressure noise suction machine, Air Compressor for pneumatic drill ma-chine, Surgeons Stool, Bipolar non sticking forceps & Pulse Oximeter.Location: Udaipur - Rajasthan - India Document Fees: Rs.200 EMD: Rs.6,000 Estimated Cost: Rs.300,000 Closing Date: 22/06/2013 at 12:30 Hrs. Contact Details: Rajasthan Medi-care Relief Society, Udaipur, Rajas-thanIndia Document Sale To: 21-6-2013________________________________________
Ref Number:8039290 Tender Number: Tender Prod. No: IS2130004 Buyer/Seller:Ordnance Factory Board Requirement: Supply of Operation Theatre Table for OFAJ Hospital.
Location: Nagpur - Maharashtra - India Document Fees: INR100
EMD: INR8,700 Estimated Cost: INR290,000 Closing Date: 21/06/2013 at 14:00 Hrs. Document Sale To: 21-6-2013 at 14:00 Hrs________________________________________
Ref Number:7956310 Tender Number: Tender Prod. No: 06/13/OT/5015 Buyer/Seller: Southern Railway Requirement: Supply Of Electric Icu/Ccu Bed (As Per Specification Enclosed)-5 NosLocation: Perambalur - Tamil Nadu - India Document Fees: INR1,000 EMD: INR35,800 Estimated Cost: INR1,785,000 Closing Date: 19/06/2013 at 14:00 Hrs. Contact Details: Southern Railway Document Sale To: 19-6-2013 at 14:00 Hrs________________________________________
Ref Number:8154858 Tender Number: Buyer/Seller: Employees State In-surance Corporation Requirement: Supply of hospital furniture, surgical consumables, suture materials, X ray chemicals, custom made itemsLocation: Tirunelveli - Tamil Nadu India Closing Date: 17/06/2013 at 13:00 Hrs.E-mail: [email protected]: www.esic.nic.inO.0462 2502199F.0462 2502399________________________________________
Ref Number:8111540 Tender Number: Tender Prod. No: 2013-14/3560-65 Buyer/Seller: Rajasthan Medicare Relief Society Requirement:

May – June 2013 49May-June 2013 49
1. Repair & Painting of Furniture. 2. Supply of biomedical waste, Fruit,Vegetable, Spine instrument, ECG machine, Table, Stationery, General items & Head Surgery instrument. 3. Annual Maintenance Section mchine & Centrifugal machine. 4. Printing work. 5. Providing of Computer with man. 6. Contract Cycle stand. 7. Operation of STD/PSO & Xerox machine. 8. Sale of waste fixture solutions &X-ray film.
Location: Kota - Rajasthan - India Document Fees: Rs.200 EMD: Rs.40,000 Estimated Cost: Rs.2,000,000 Closing Date: 15/06/2013 at 13:00 Hrs. Add to Calendar Contact Details: Rajasthan Medi-care Relief Society, Kota, RajasthanIndia Document Sale From: 5-6-2013 Document Sale To: 14-6-2013________________________________________
Ref Number: 8079017 Tender Number: Buyer/Seller: Ahmednagar Munici-pal Corporation Requirement: Repair of Sluice valve, PVC pipe. 2. Supply of Alum, TCL powder, Liquid chlorine gas, Pesticide pow-der, Malaria oil, Hydro choric acid,Medicine, Chemical, Plasticcontainer, Gumboot, Hand gloves,Rubber hosepipe, Metal roof, GI pipe, Broom, Fiber dustbin, Wheel barrow, Tree guard, Bench, Tiles, Murrum, Sand, Metal, RCC Slab, Manhole cover, Hume pipe with Collar, Tube, Starter, Lock holder, Chock, Tube patti, Sodium bulb, Sodium chock, Igniter, Copper cable, Motor pump, Main switch starter, UPS, Tubular battery, Office & Computer stationery item, Paper, Register, Duplicate book, Carbon paper, Stamp pad, Pin, Sutali,Cartridge, Toner, Ribbon, Floppy,Calculator, Diary, Computer paper,
Office furniture, Chair, Table,Computer table, Revolving chair,Wheel chairLocation: Ahmednagar - Maharash-tra - India Document Fees: Rs.2,000 EMD: Rs.50,000 Estimated Cost: Rs.5,000,000 Closing Date: 3/06/2013 at 11:00 Hrs. Add to Calendar Contact Details: AhmednagarMunicipal CorporationAhmednagar, Maharashtra, India Document Sale To: 30-5-2013 at 11:00 Hrs________________________________________
Ref Number: 8091558 Tender Number: Tender Prod. No: PUR/1/13-14/EOI/UTF/GDT Buyer/Seller: Indian Institute Of Petroleum Requirement: Expression of interest for Procurement & installation of Ultra thin film measurement sys-tem, modular laboratory furniture, surface profiler.Location: Dehradun - Uttaranchal - India Closing Date: 5/06/2013 at 14:30 Hrs e-mail: [email protected], [email protected] 2525762F.0135 - 2660072 URL: www.iip.res.in______________________________________
Ref Number:8118656 Tender Number: Buyer/Seller: Medical And Health Department Requirement: Supply of Medicines, Machinery Equipment, Hospital furniture, Pathology Chemical Reagent etcLocation: Seoni - Madhya Pradesh - India Document Fees: Rs.1,000 EMD: Rs.50,000 Closing Date: 10/06/2013 at 00:00 Hrs.
Contact Details: Medical And Health Department, Seoni, Madhya PradeshIndia Document Sale From: 20-5-2013 Document Sale To: 24-5-2013________________________________________
Ref Number:8078252 Tender Number: Tender Prod. No: GMCH-PB-I-PA-V-PA-IV-13/3131 Buyer/Seller: Medical Education And Research Requirement: Supply of Patient Trolley with Oxygen Cylinder Case & IV Rod.Location: Chandigarh - Punjab - India EMD: INR16,000 Closing Date: 7/06/2013 at 14:00 Hrs. Document Sale To: 7-6-2013 at 14:00 Hrs
TENDERS

50 May-June 2013
TENDER

May – June 2013 5151
SECTIONBUSINESS

52 May-June 2013

May – June 2013 53
Join this Summit and participate inthe most important discussion on
Clinical Trials
Media Sponsor
Be a part of the
REGISTER TODAY!
Organised by
To Book Your Place ContactTIKENDERJIT SINGHE: [email protected]: +91 20 6727 6403 F +91 20 6607 0061W: www.fleminggulf.com/Healthcareitindia2013
Clinical Trials Asia Summit 26 – 27 September 2013, Hyderabad, India
Scan theQR Code
to Know More

54 May-June 2013
th 20 InternationalExhibition and Conference
India's No. 1Trade Fairfor Hospitals, Health Centresand Clinics
14-16 March 2014Bombay Convention &Exhibition CentreGoregaon (East), Mumbai/India
www.medicalfair-india.com

May – June 2013 55
56 May-June 2013

May – June 2013 57

58 May-June 2013

May – June 2013 59

60 May-June 2013

May – June 2013 61
Name: ................................................................................Last Name:.........................................................................Designation:.......................................................................Organisation:.....................................................................Address:...........................................................................................................................................................................City:................................... Pin Code:...............................State:.................................Mobile No.:.............................. Fax:..................................Email:...................................................................................
Enclose Cheque No.:............................................................................Drawn On:.............................................................................................Dated:.....................................................................................................towards subscription for Medgate Today Magazine in favour of Medgate Today
Sign.:................................................... Date:...............................
Mail this form with payment to:Medgate Today 92/17, Zakir Nagar, opp New Friends Colony, Okhla New Delhi-110025Mobile:+91 9212366351, email: [email protected], [email protected]: www.medgatetoday.com
Tick Terms
1 year (6 issues)
2 years (12 issues)
Subscription Rate
Rs.625/-
Rs.1200/-

62 May-June 2013


RNI No. DElENG/2010/33833