meccanismi d’azione dei trattamenti: implicazioni sull ...sm.medicacom.it/2018/clerico.pdf ·...
TRANSCRIPT

Convegno Webinar ECM
Meccanismi d’azione dei trattamenti: implicazioni sull’efficacia e la sicurezza
Marinella ClericoUniversità degli studi di Torino, A.O.U. San Luigi Gonzaga, Orbassano (TO)

aAzathioprine and cyclophosphamide are not approved for the treatment of MS and have been used off-label
IFN, interferon; im, intramuscular; sc, subcutaneous; SmPC, Summary of Product Characteristics
1. Betaferon® EU SmPC, Sep 2017; 2. Avonex® EU SmPC, Jul 2017; 3. Rebif® EU SmPC, Feb 2018; 4. Copaxone® UK SmPC, Jun 2017; 5. Tysabri® EU SmPC, May 2017;
6. Gilenya® EU SmPC, Feb 2018; 7. Lemtrada® EU SmPC, Feb 2018; 8. Aubagio® EU SmPC, Dec 2017; 9. Tecfidera® EU SmPC, Jan 2018; 10. MAVENCLAD® EU SmPC,
Feb 2018; 11. Ocrevus® EU SmPC, Jan 2018
1994
The goal of treatment is to increase efficacy, improve safety and increase selectivity
Immunomodulation/
immunostimulation
Chronic drug administration
resulting in modulation of immune
function without immunosuppression
Clinical efficacy only
during active treatment
Long periods between
administrations
Non-continuous
administration
Clinical efficacy extends
well
beyond period of active
treatment
Broad-spectrum
immunosuppres
sion
Prior to 1990s,
MS treatment
options limited to
broad-spectrum
immunosuppressa
nts
Selective, continuous
immunosuppression
Chronic drug administration
resulting in ongoing
suppression of
immune function
Clinical efficacy only
during active treatment
Cyclophosphami
dea
Azathioprin
ea
sc IFN β-1b1
im IFN β-1a2
sc IFN β-1a3
Glatiramer acetate4
Alemtuzumab7
Ocrelizumab11
Cladribine Tablets10
Natalizumab5
Dimethyl
fumarate9
Teriflunomide8
Fingolimod6
199
6
199
8
200
0200
2200
4
200
6
200
8201
0
201
2201
4
201
6201
8
The current MS treatment landscape

0
10
20
30
40
50
60
OPERA I1
Ocrelizumaba
vs sc IFN β-1a
Sponsored by Genentech
OPERA II1
Ocrelizumaba
vs sc IFN β-1a
Sponsored by Genentech
CLARITY2
Cladribine Tablets
vs placebo
CARE-MS I3
Alemtuzumabvs sc IFN β-1a
Sponsored by Sanofi
AFFIRM4
Natalizumab vs placebo
Sponsored by Biogen
****** ***
* ***
FREEDOMS5
Fingolimodvs placebo
Sponsored by Novartis
**
CARE-MS II6
Alemtuzumab vs sc IFN β-1a
Sponsored by Sanofi
***
DEFINE7
Dimethyl fumarate
vs placebo
Sponsored by Biogen
*
**
TEMSO8
Teriflunomidevs placebo
Sponsored by Sanofi
Pat
ien
ts a
chie
vin
g N
EDA
(%
)
Data cannot be directly compared between trials because of distinct study
designs and/or patient populations
*p<0.05, **p<0.001, ***p<0.0001 study drug vs comparator. aOcrelizumab is approved for the treatment of MS in the US and EU. NEDA defined as no relapses, no 3-month confirmed CDP, and no new T1 Gd+ lesions and no new enlarging or enlarged T2 lesions on cranial MRI (except CLARITY, CARE-MS I and CARE-MS II: based on no 6-month CDP). CDP, confirmed disability progression; Gd+, gadolinium-enhancing; IFN, interferon; MRI,magnetic resonance imaging; NEDA, no evidence of disease activity; sc, subcutaneous.
1. Traboulsee A, et al. Neurology 2016;86 [PL02.004]; 2. Giovannoni G, et al. Lancet Neurol 2011;10:329‒37; 3. Cohen AJ, et al. Lancet 2012;380:1819–28; 4. Havrdova E, et al. Lancet Neurol 2009;8:254‒60; 5. Bevan CJ, Cree BA. JAMA Neurol 2014;71:269‒70; 6. Coles AJ, et al. Lancet 2012;380:1829–39; 7. Giovannoni G, et al. Neurology 2012;78 [PD5.005]; 8. Freedman M, et al. Neurology 2012;78 [PD5.007].
NEDA is achievable with existing MS therapies

The complex therapeutic landscape of DMDs in MS can be
organized through consideration of efficacy, safety and
treatment burden1
1. Coles AJ. Ann Indian Acad Neurol 2015;18(Suppl. 1):S30–34; 2. MAVENCLAD® SmPC, July 2018.
aSuggested placement based on approved indication and monitoring in EU SmPC2.
DMD, disease-modifying drug; DMF, dimethyl fumarate; GA, glatiramer acetate; IFN, interferon; JC, John Cunningham virus.
IFN β
GA
Teriflunomide
DMF
Fingolimod
Alemtuzumab
Natalizumab
in JC–Natalizumab
in JC+
Mitoxantrone
Autologous stem cell
transplantation
Cladribine
Tabletsa
Increasing burden of treatment
(worse safety, more difficult administration)
Figure adapted from Coles AJ.
Ann Indian Acad Neurol
2015;18(Suppl 1):S30–34.
Different therapies provide options across multiple levels of disease activity depending on their benefit:risk profile

IL, interleukin; LTβR, lymphotoxin-β receptor; LTβ, lymphotoxin-β; TNF, tumor necrosis factor.
FORMATION OF ECTOPIC
GERMINAL CENTRESPlasma cellB cell
‘Normal’antibodies
Pathologicalautoantibodies
Antibody-dependent
cell-mediatedcytotoxicity
MacrophageFc
FcC3
Target tissue
CytotoxicT cells
Target tissue
TNFIL-6
IL-1
Cytokines
Macrophage
TNF
Antibody T cell
Dendriticcell
IL-10IL-6
Cytokines
B cell B cell
SECRETION OF ANTIBODY
CytokinesTNF, IL-6, IL-10
B cell
LTR
Meningeal ectopicgerminal centers
Follicular
Dendritic cell
LT
Complement
Toxins
Target tissue
ANTIGEN PRESENTATION
TO T CELLS
CD4 T cell
B cell
CytokinesTNF, IL-6, IL-10
Target tissue
B cell growth Factors
SECRETION
OF CYTOKINE3,4
CD4 T cellhelp
CytokinesIL-4,IL-10, IL-13
CD4 T cell
1. Dalakas MS. Clin Pract Neurol 2008;4:557–67.
Figure reprinted by permission from Macmillan Publishers Ltd: Nat Clin Pract Neurol, Dalakas MC. B cells as therapeutic targets in autoimmune neurological disorders. Volume 4:pp. 557–567, copyright 2008
B & T cells exert different functions in neuroinflammation1,2

B, B cell; BBB, blood–brain barrier; CNS, central nervous system; IFN, interferon; HCA2, hydroxycarboxylic acid receptor 2; MoA, mechanism of action; nrf 2, nuclear factor (erythroid-derived 2)-like 2; S1P1, sphingosine-1-phosphate receptor 1; T, T cell; Th, T-helper cell.
Adapted from: Loleit V, et al. Curr Pharm Biotechnol. 2014;15:276–96; Scannevin R, et al. J Pharmacol Exp Ther. 2012;341:274–84; Chen H, et al. J Clin Invest. 2014;124:2188–92.
Mechanisms of action of distinct MS immunotherapies
Alemtuzumab/Ocrelizumab/Cladribine
CD52Lysis of mature B and T cells
D: Proposed MoA: anti-migratory
FingolimodNatalizumab
Lymph node
BBB
CNS
S1P1
B
T
α4-integrin
A: Proposed MoA: Immunomodulation/pleiotropic effects
Limits pyrimidine availability for rapid cell division
Azathioprine, cyclophosphamide,mitoxanthrone, Teriflunomide
IFNs
Activation of 100+ IFN-response genes
Activation of 700+ nrf 2 responsive genes and HCA2
Glatiramer acetate
Modulation of APC and Th1:Th2 balance
Dimethyl fumarate
C: Proposed MoA: targeted cell lysis
Periphery
B: Proposed MoA: reduced proliferation
T
B
CD20
ALMOST ALL OF THESE TREATMENTS INDUCE TRANSIENT EFFECTS ON THE IMMUNE SYSTEM AND NOT PERMANENT CHANGES

PML
Herpes encephalitis
Rebound on withdrawal
1. Selective adhesion molecule blocker
2. Infusion reactionsa. Anaphylactoidb. Associated with anti-drug
antibodies3. Blocks CNS immune surveillance
a. PMLb. CNS infectionsc. Possible link with CNS
lymphomas4. Rebound activity post-washout
Khatri et al. Neurology 2009;72:402–09.
EXCEMED. Schmierer K. ECF 2017. Available at: https://www.excemed.org/resources/high-efficacy-treatments-management-[Accessed Nov 2018]
Natalizumab

O Major, et al. Lancet Neurol 2018,17:467-80
Proposed stages of PML pathogenesis in patients treated with natalizumab

Singer et al. Ther Adv Neurol Disord 2017
Ho et al. Lancet Neurol 2017
Natalizumab: evaluation of risk

Warnke et al. J Neurol Neurosurg Psychiatry 2013
Natalizumab: seroconversion to JCV+

Dong-Si T et al. Ann Clin Transl Neurol 2014;1:755–64.
Figures reprinted from Dong-Si T et al, Outcme and survival of asymptomatic PML in natalizumab-treated MS patients, Ann Clin Transl Neurol, 2014
EXCEMED. Schmierer K. ECF 2017. Available at: https://www.excemed.org/resources/high-efficacy-treatments-management-[Accessed Nov 2018]
Natalizumab: asymptomatic PML

Clerico et al.EODS 2017
Natalizumab: AE other than PML

APC
Lymp
h
node
S1P-RT
Gliosis
S1P-
R
Fingolimod
Fingolimo
d
CNS /
Immune and
Neural
system
Periphery /
Immune
system
Oligo’s
VZV - Chickenpox &
ZosterTB
Cryptococcosis HistoplasmosisKaposi’s PMLBasal Cell
Ca
etc…..
.
Rebound on withdrawal
PRES and other vascular complications
Macular oedema
Conduction Block
Lymphopenia
1. SIP modulatora. Lymphopenia (prolonged)b. Bradycardia/Conduction blockc. Vascular complications
(macular oedema, hypertension, PRES)
d. Bronchoconstriction2. Immunosuppression
a. Opportunistic infectionsb. Secondary malignanciesc. Blunted vaccine response
EXCEMED. Schmierer K. ECF 2017. Available at: https://www.excemed.org/resources/high-efficacy-treatments-management-patients[Accessed Nov 2018]
Fingolimod

Figure adapted from Giovannoni et al, Switching patients at high risk of PML from natalizumab to another disease-modifying therapy, Pract Neurol. 2016
Figures reprinted from Francis G et al, Temporal profile of lymphocyte counts and
relationship with infections with fingolimod therapy, Mult Scler, 2014
1. Francis G et al. Mult Scler 2014;20:471–80; 2. Giovannoni et al. Pract Neurol. 2016 Oct;16:389-93
Fingolimod

Fingolimod

1. Crawford A et al. J Immunol 2006;176:3498–506. 2. Bar-Or A, et al. Ann Neurol 2010;67:452–61. 3. Lisak RP et al. J Neuroimmunol 2012;246:85–95. 4. Weber MS et al. Biochim Biophys Acta 2011;1812:239–45. 5. Serafini B et al. Brain Pathol 2004;14:164–74. 6. Magliozzi R et al. Ann Neurol 2010;68:477–93.cc. 7. EXCEMED. Schmierer K. ECF 2017. Available at: https://www.excemed.org/resources/high-efficacy-treatments-management-patients [Accessed Mar 2018]
Antigen
presenta
tion1,2
Autoantibody
production4
Ectopic lymphoid
follicle-like
aggregates5,6
Cytokine
production2,3
PML Breast CaVZV & herpes
Ocrelizumab

17
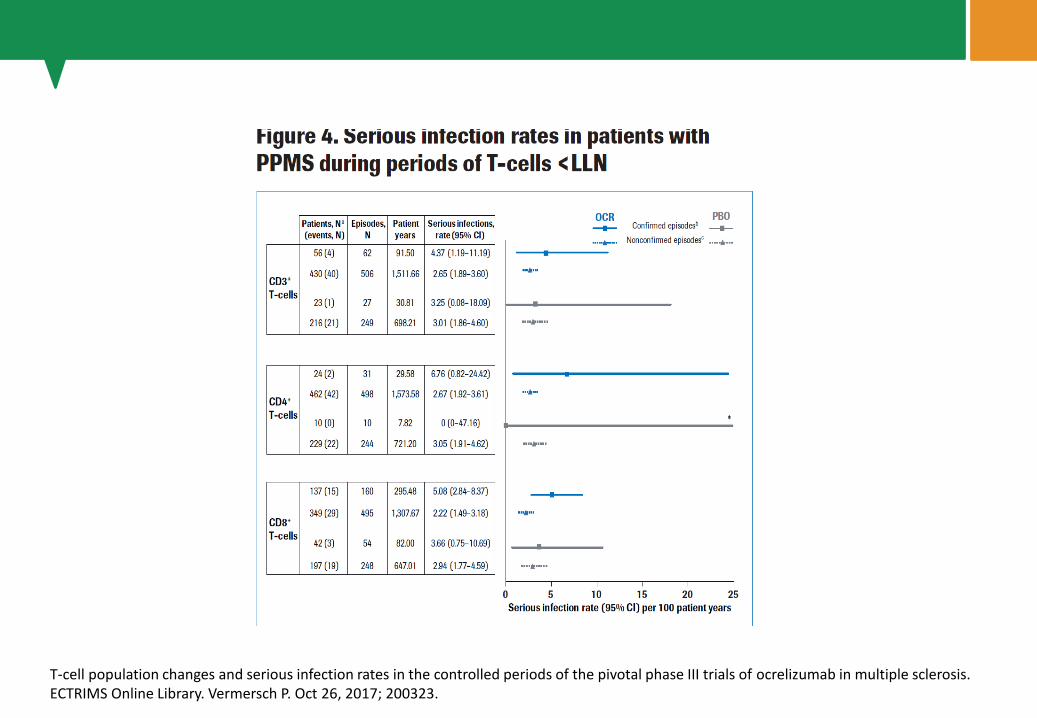
T-cell population changes and serious infection rates in the controlled periods of the pivotal phase III trials of ocrelizumab in multiple sclerosis. ECTRIMS Online Library. Vermersch P. Oct 26, 2017; 200323.

18T-cell population changes and serious infection rates in the controlled periods of the pivotal phase III trials of ocrelizumab in multiple sclerosis. ECTRIMS Online Library. Vermersch P. Oct 26, 2017; 200323.

19
T-cell population changes and serious infection rates in the controlled periods of the pivotal phase III trials of ocrelizumab in multiple sclerosis. ECTRIMS Online Library. Vermersch P. Oct 26, 2017; 200323.
20T-cell population changes and serious infection rates in the controlled periods of the pivotal phase III trials of ocrelizumab in multiple sclerosis. ECTRIMS Online Library. Vermersch P. Oct 26, 2017; 200323.

21ECTRIMS 2017. P668. T-cell population changes and serious infection rates in the controlled periods of the pivotal phase III trials of ocrelizumabin multiple sclerosis

22
Reductions in immunoglobulin levels following natalizumab-to-rituximab crossover in a multiple sclerosis cohort: implications for next generation B cell-targeted therapies
ECTRIMS Online Library. Foley M. Oct 27, 2017; 200872
PML risk is increased in primary hypogammaglobulinemia patients and with anti-CD20 therapy, occurring primarily with concomitant immunosuppressant use.
Further evaluation of chronic hypogammaglobulinemia secondary to anti-CD20 therapy as a risk factor for PML is warranted, especially in high risk populations.

AUC, area under the curve; EDSS, Expanded Disability Status Scale; SPMS, secondary progressive MS; SRD, sustained reduction in disability1. Tuohy O et al. J Neurol Neurosurg Psychiatry 2015;86:208–15; 2. Coles AJ et al. Lancet 1999;354:1691–5; 3. Lemtrada® EU SmPC, Feb 2018; 4. Coles AJ et al. Lancet 2012;380:1829–39
• CD4 and CD8 counts were 30–40% of pre-treatment values 18
months after treatment2
• B cells repopulated more rapidly, with counts reaching 179% of
pre-treatment values by 18 months2
• Adverse reactions included infusion-associated reactions, immune
thrombocytopenia, nephropathies, infection risk and risk of
secondary autoimmune disorders1–4
Durable efficacy with alemtuzumab is demonstrated by a 12-month sustained reduction in disability and
stable/improved EDSS1
Haematological changes after alemtuzumab2
1.61.41.21.00.80.60.40.20.0
0.5
0.4
0.3
0.2
0.1
0.0
T c
ells (
x10
9/L
)
B c
ells (
x10
9/L
)
Pre Post
(Day 2)
3 6 9 12 15 18
Months after alemtuzumab (20 mg x 5)
B cells CD8+ T cells CD4+ T cells
Figure reproduced from Coles AJ et al. Lancet
1999;354:1691–5
Months since first treatment
12-month sustained
reduction in disability2
% S
RD
of
at-
risk p
op
ula
tio
n
60
0 12 24 36 48 60 72 84 96 108 120
50
40
30
20
10
0
ED
SS
-ye
ars
30
20
10
0
-10
-30
-50
-20
-40
Net better
n=43 (50%)
Net unchanged
n=9 (10%)
Net worse
n=35 (40%)
AUC values: EDSS change from
baseline vs follow-up2
Figures adapted from Tuohy O et al. J Neurol Neurosurg Psychiatry
2015;86:208–15
Alemtuzumab reduce MS disease activity through targeting T and B cells

V
Z
V
T
B Listeria Nocardia
Molluscum HPVCMVEBV
PCP
Etc...
Thomas et al. Neurol NeuroimmunolNeuroinflamm 2016;3:e228;
AVN
1. Non-selective leukocyte depletiona. Leukopaenia (neutrophils &
monocytes)b. Lymphopaenia (prolonged)c. Infusion reactions (moderate to
severe)d. Complications of corticosteroids
2. Immunosuppressiona. Opportunistic infections
i. Acute bacterial, e.g. Listeriosis
ii. Typical opportunistic, e.g. CMV
3. Aberrant immune reconstitutiona. Secondary autoimmunityb. Anti-drug antibodies
InnateImmunity
AdaptiveImmunity
AVN = avsacular necrosis, HPV = human papiloma virus, PCP = Pneumocystis carinii
pneumonia, VZV = varicella zoster virus
EXCEMED. Schmierer K. ECF 2017. Available at: https://www.excemed.org/resources/high-efficacy-treatments-management-patients[Accessed Nov 2018]

1. Baker D et al. JAMA Neurol 2017; doi:10.1001/jamaneurol.2017.0676; 2. Coles AJ et al. Lancet 1999;354:1691–5
CD4 T cells
Naïve CD4
T cells
Memory CD4
T cells
CD8 T cells
CD4 regulatory
T cells
CD8 regulatory
T cells
CD19 B cells
Mature naïve
B cells
Memory
B cells
Immature B cells
Figure from Coles AJ et al. Lancet
1999;354:1691–5
Figures adapted from Baker D et al. JAMA Neurol 2017;
doi:10.1001/jamaneurol.2017.0676
Figures adapted from
Baker D et al. JAMA
Neurol 2017;
doi:10.1001/jamaneurol.
2017.0676
Alemtuzumab depletes subsets of B and T cells1,2
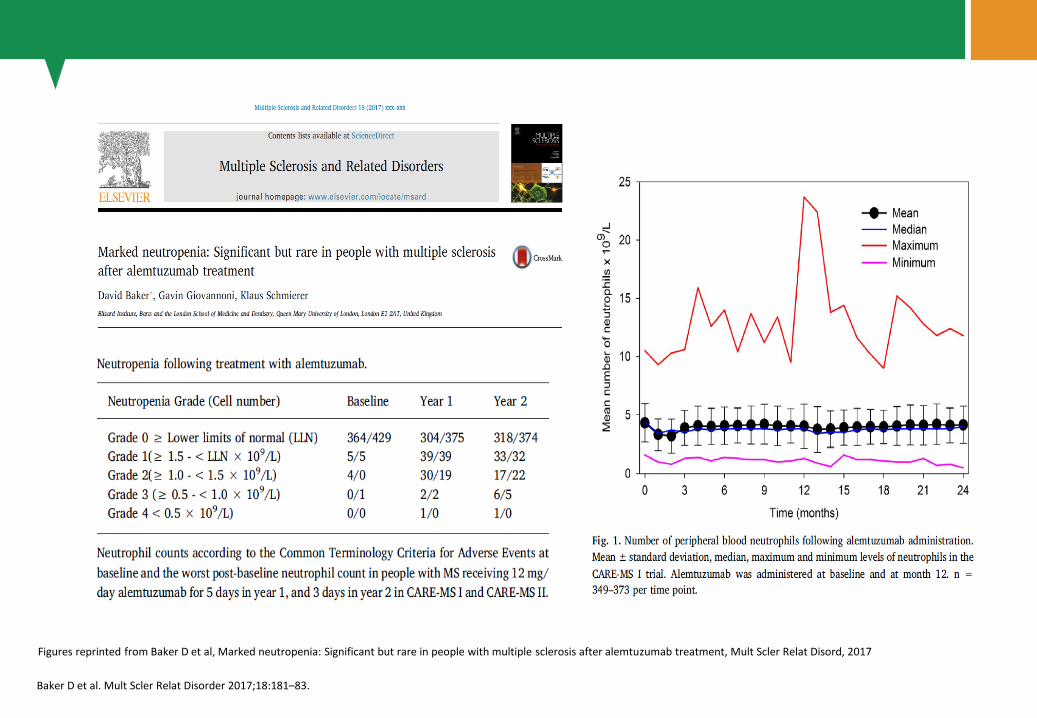
Baker D et al. Mult Scler Relat Disorder 2017;18:181–83.
Figures reprinted from Baker D et al, Marked neutropenia: Significant but rare in people with multiple sclerosis after alemtuzumab treatment, Mult Scler Relat Disord, 2017

Treg
Th17Th1
Treg
Th17
Th1
Treg
Th17
Th1
CD4 T cells
MBP specificcells
Durelli et al.AAN 2016
Clerico et al.AAN 2018

Identified Risk
Rate in Alemtuzumab-
Treated Patients Notes
ITP
Auto-immune Events
~1% (1 fatality
prior
to implementation
of monitoring
program)2
• Onset generally occurred 14-36 mo after first exposure2
• Most cases responded to first-line medical therapy2
0.3%
(anti-GBM n=2)2
• Generally occurred within 39 mo after last administration2
• Responded to timely medical treatment and did not develop
permanent kidney failure3
Nephropath
ies
Thyroid
disorders
(Hypo/hyper)
~36%a
(serious, 1%)2
• Onset occurred 6-61 mo after first Alemtuzumab exposure;
peaked in year 3 and declined thereafter4
• Most mild to moderate, most managed with conventional
medical therapy, however, some patients required surgical
intervention2
• Higher incidence in patients with history of thyroid disorders2
IARs>90%
(serious, 3%)2
• Occurred within 24 h of Alemtuzumab administration2
• Most mild to moderate; rarely led to treatment
discontinuation2
• May be caused by cytokine release following mAb-mediated
cell lysis2
Infections71%
(serious, 2.7%)2
• Incidence highest during first mo after infusion; rate
decreased over time4
• More common with Alemtuzumab; mostly mild to moderate2
• Generally of typical duration; resolved following conventional
medical treatment1
aThrough 48 mo after first exposure. IAR, infusion-associated reaction; ITP, immune thrombocytopenia; GBM, glomerular basement membrane; mAb, monoclonal antibody.1. EXCEMED. Schmierer K. ECF 2017. Available at: https://www.excemed.org/resources/high-efficacy-treatments-management-patients [Accessed Mar 2018];
2. Alemtuzumab SmPC, June 2016; 3. Havrdova, E et al. Ther Clin Risk Manag. 2017;13:1423-1437; 4. Coles A et al. Neurology. 2012;78:1069–78; 5. Willis et al. MSJ 2016;22:1215–23.
Haemolytic anaemia
Goodpasture’s Syn.
ITP Bullous Pemphigoid
Immune neutropenia
Grave’s orbitopathy
Neonatal hyperthyroidism
Acquired Haemophilia
Pernicious Anaemia
Etc...
Cervical dysplasia5 MGUS5
+
10% pre/malignant 6.1 yrsFUp
Alemtuzumab risks identified in clinical trials1

No correlation between lymphocytepharmacodynamics and autoimmune adverse events following alemtuzumabtreatment in patients with relapsing-remitting multiple sclerosisH. Wiendl et al. ECTRIMS Online Library. Oct 11, 2018; 228723

aOne of the kinases is deoxycitidine kinase (dCK). The phosphatase is 5’-nucleotidase. ADA, adenosine deaminase; CNS, central nervous system.
1. Leist TP, et al. Clin Neuropharmacol 2011;34:28–35; 2. Goodlett CR, et al. Alcohol Res Health 2001;25:175–84; 3. Bredesen DE. Neuroscientist 1996;2:181–190; 4. Charras GT. J Microscopy 2008;231:466–78; 5. Jacobs BM, et al. J Neurol Neurosurg Psychiatry 2018;0:1–6.
❷ Accumulates intracellularly due to protection from
ADA degradation
Slow
degradation
by ADA
Activated cladribine is
inactivated by a
specific phosphatasea
Phosphatase
inactivation
❸ Cladribine is activated by specific kinases
Kinase
activationa
Activated
cladribine
❹ Activated cladribine induces lymphocyte apoptosis
Lymphocyte
reduction
❶ Cladribine enters cell via nucleoside transporterCladribine
Cladribine
Cladribine works by a 4-step
mechanism1:
Apoptosis does not lead to localized
inflammation, unlike cell lysis2–4
In addition to its pro-apoptotic effects,
cladribine promotes immune tolerance
and reduces immune cell infiltration
into the CNS5
Cladribine has to be transported into cells and activated in order to exert its effect
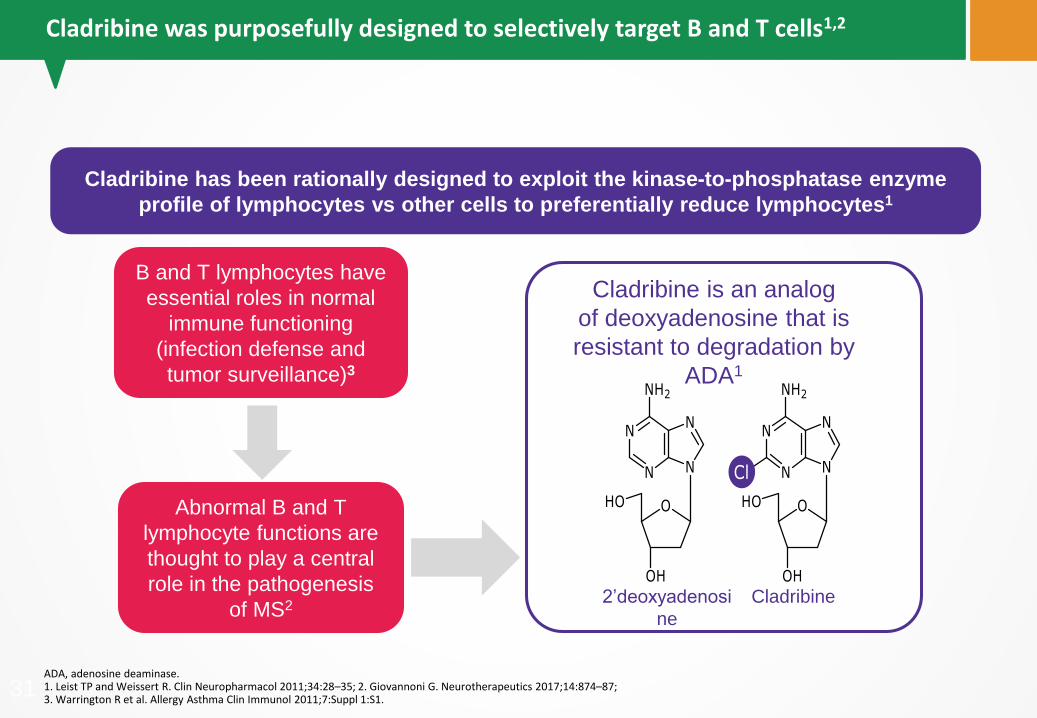
ADA, adenosine deaminase.1. Leist TP and Weissert R. Clin Neuropharmacol 2011;34:28–35; 2. Giovannoni G. Neurotherapeutics 2017;14:874–87; 3. Warrington R et al. Allergy Asthma Clin Immunol 2011;7:Suppl 1:S1.
31
Abnormal B and T
lymphocyte functions are
thought to play a central
role in the pathogenesis
of MS2
B and T lymphocytes have
essential roles in normal
immune functioning
(infection defense and
tumor surveillance)3
B and T lymphocytes have essential
roles in normal immune functioning
(infection resistance and tumour
surveillance)
Cladribine is an analog
of deoxyadenosine that is
resistant to degradation by
ADA1
2’deoxyadenosi
ne
Cladribine
Cladribine has been rationally designed to exploit the kinase-to-phosphatase enzyme
profile of lymphocytes vs other cells to preferentially reduce lymphocytes1
Cladribine was purposefully designed to selectively target B and T cells1,2

B and T lymphocytes have a
higher kinase-to-phosphatase
ratio than other cells4
aThe kinase is deoxycytidine kinase; the phosphatase is 5’-nucleotidase; bData for NT5C, NT5C2L1 and NT5C3 were not available to include as there was no probe set for these genes at the time of analysis. NK, natural killer.
1. Carson D et al. Proc Natl Acad Sci USA 1980;77:6865–9; 2. Carson DA et al. Blood 1983;62:737–43; 3. Salvat C et al. ECTRIMS 2009 [P280]; 4. Leist TP, Weissert R. Clin Neuropharmacol 2011;34:28–35.
Figure adapted from Salvat C et al. ECTRIMS 2009 [P280]
Figure adapted from Leist TP, Weissert R. Clin Neuropharmacol
2011;34:28–35
CD4+ T lymphocytes
CD8+ T lymphocytes
Skin
Heart
Brain
Ovary
Liver
Kidney
Lung
Testis germ cell
Testis
mRNA expression of
activating kinasea
mRNA expression of
inactivating phosphatasea,b
mRNA expression of
inactivating phosphatasea
mRNA expression of
activating kinasea
CD4+ T cells
CD8+ T cells
CD19+ B cells
NK cells
Cladribine selectivity is due to lymphocytes having a higher kinase-to-phosphatase ratio than other cells1–4

Cladribine Tablets
Placebo
BL, baseline; LA, last assessment; Q, quartile.Figures adapted from Soelberg-Sørensen P et al. ECTRIMS 2017 [P655].1. Soelberg-Sørensen P et al. ECTRIMS 2017 [P655]; 2. Soelberg-Sørensen P et al. ENS 2010 [P442]; 3. Bisset LR et al. Eur J Haematol 2004;72:203–12.
Rapid reduction of B
lymphocytes,
followed by reconstitution
Moderate reduction of T
lymphocytes,
followed by reconstitution
CD19+ B lymphocytes1
0
100
50
150
200
300
250
350
400
0 24 48 72 96 120 144 168 192 216 240
Normal range in adults (72–460 cells/µL)3
Weeks
Cladribine Tablets
Placebo
0 24 48 72 96 120 144 168 192 216 240
200
400
600
800
1000
300
500
700
900
Normal range in adults (309–1139 cells/µL)3
Weeks
Me
dia
n (
Q1
–Q
3)
CD
4+
T lym
ph
ocyte
s (
cells
/µL
)
CD4+ T lymphocytes1
79
220
81
203
61
137
74
191
78
195 38 56 68 64 49 33
79
220
81
203
61
137
74
191
78
195 38 56 68 64 49 33
Me
dia
n (
Q1
–Q
3)
CD
19
+ B
lym
ph
ocyte
s (
cells
/µL
)
Cladribine has a selective and transient effect on lymphocyte depletion, followed by a distinct pattern of reconstitution1,2

4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0
BL 3 6 9 12 15 18 21 24LA
CD16+/CD56+ NK CELLS
BL, baseline; LA, last assessment; NK, natural killer.1. Baker D et al. Neurol Neuroimmunol Neuroinfamm 2017;4:e360; 2. Giovannoni G et al. N Engl J Med 2010;362:416–26; 3. Soelberg-Sørensen P et al. ENS 2009 [P359]; 4. Soelberg-Sørensen P et al. ENS 2010 [P442]; 5. Rieckmann P et al. ECTRIMS 2009 [P816]; 6. Soelberg-Sørensen P et al. ECTRIMS 2009 [P472]. 7. Bisset LR et al. Eur J Haematol 2004;72:203–12; 8. Soelberg-Sørensen P et al. ECTRIMS 2017 [P1141].
Cladribine has a transient and mild effect on platelets and monocytes1
Normal range in adults (77–427 cells/µL)7250
200
150
100
50
0
BL 3 6 9 12 15 18 21 24LA
Me
dia
n c
ell
co
un
t (c
ells
/µL
)
Study monthsM
edia
n c
ell
count (c
ells
×1
09/ µ
L)
Study months
Threshold
2.03 x 109/L8
Figures adapted from Soelberg Sørensen P et al. ECTRIMS 2009 [P472]Figure adapted from Rieckmann P et al. ECTRIMS 2009 [P816]
Rapid reduction of NK cells,
followed by reconstitution5 Modest effect on neutrophils6
MAVENCLAD®
(n=81)
Placebo (n=79)
MAVENCLAD®
(n=81)
Placebo (n=79)
Cladribine has a minimal impact on innate immune cell counts1–4
1. Baker D, et al. Neurol Neuroimmunol Neuroinflamm 2017;4:e360; 2. Giovannoni G, et al. N Engl J Med 2010;362:416 – 26; 3. Cohen JA, et al. Lancet 2012;380:1819 – 28.
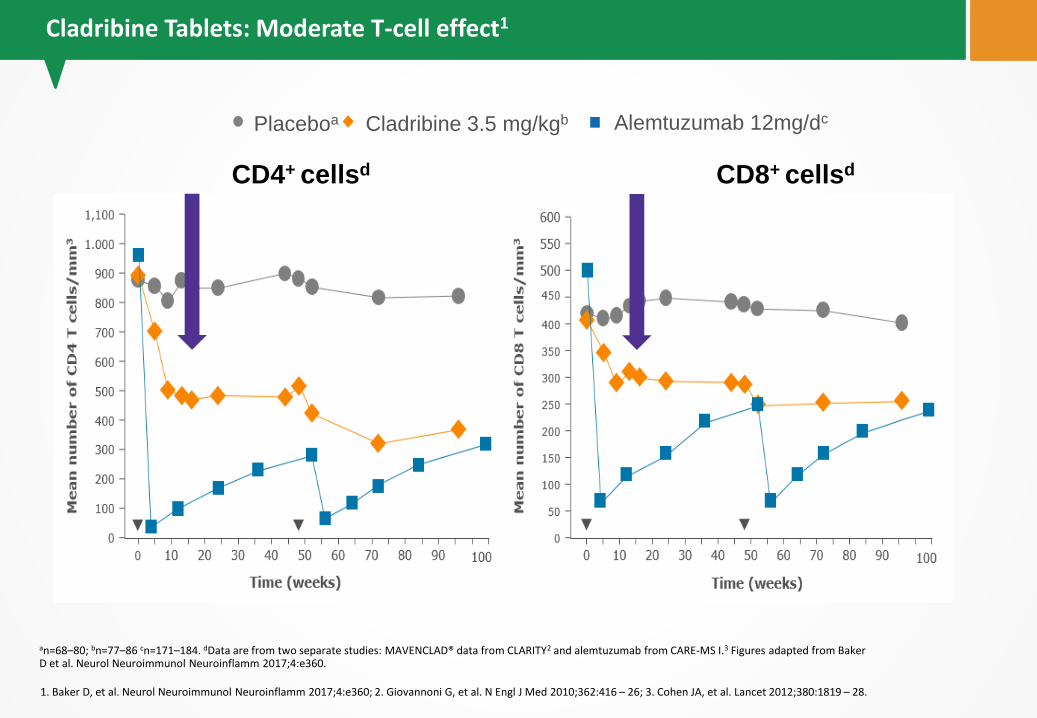
CD4+ cellsd CD8+ cellsd
Cladribine 3.5 mg/kgbPlaceboa Alemtuzumab 12mg/dc
an=68–80; bn=77–86 cn=171–184. dData are from two separate studies: MAVENCLAD® data from CLARITY2 and alemtuzumab from CARE-MS I.3 Figures adapted from Baker D et al. Neurol Neuroimmunol Neuroinflamm 2017;4:e360.
Cladribine Tablets: Moderate T-cell effect1
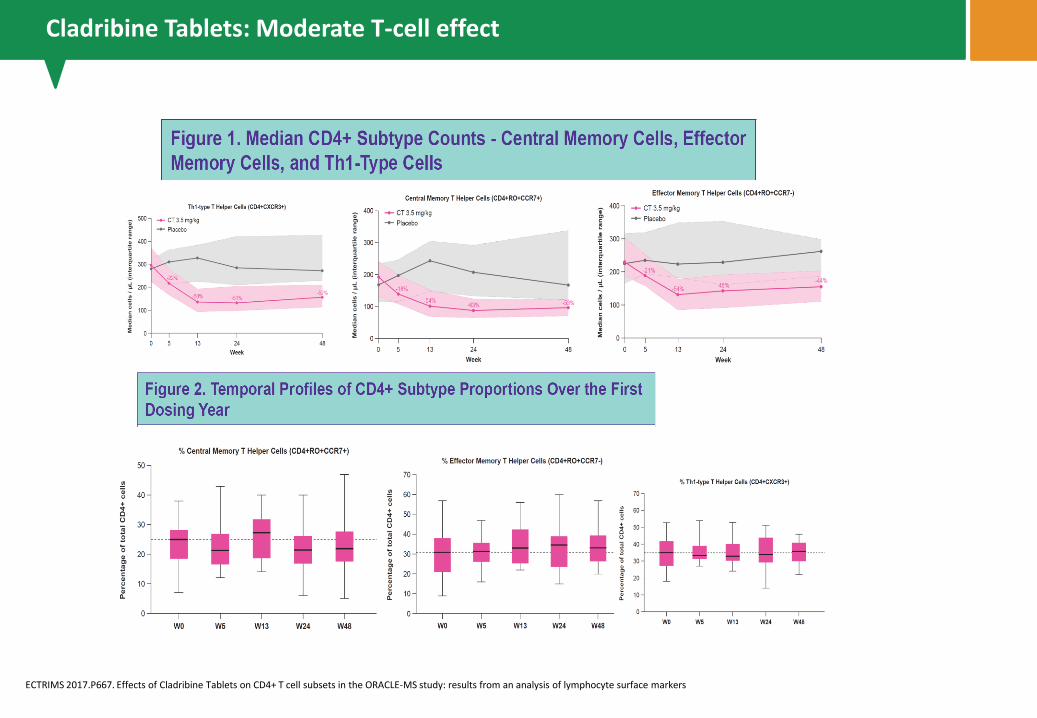
36ECTRIMS 2017.P667. Effects of Cladribine Tablets on CD4+ T cell subsets in the ORACLE-MS study: results from an analysis of lymphocyte surface markers
Cladribine Tablets: Moderate T-cell effect

37ECTRIMS 2017.P667. Effects of Cladribine Tablets on CD4+ T cell subsets in the ORACLE-MS study: results from an analysis of lymphocyte surface markers
Cladribine Tablets: Moderate T-cell effect

38ECTRIMS 2017.P667. Effects of Cladribine Tablets on CD4+ T cell subsets in the ORACLE-MS study: results from an analysis of lymphocyte surface markers

1. Soelberg-Sørensen PS, et al. ACTRIMS 2018 [P084]; 2.Baker D, et al. JAMA neurol 2107;74:961–69; 3. Ceronie B, et al. J. Neurol 2018;265:1199–1209; 4. Baker D, et al. Brain 2108;141:2834–47; 5. Stuve O, et al. ACTRIMS 2018 [P059]; 6.Baker D, et al. Neurol, Neuroimmuno Neuroinflamm 2017;74:961–969.
Figure adapted from Soelberg-Sørensen PS et al. ACTRIMS 2018 [P084]
1200
100
50
150
300
300
250
350
400
0 24 48 72 144 168 192 216 240
LLN
No secondary
autoimmunity
96
CD19+ B lymphocytes
Weeks
CD19+ repopulation is a composite of a number of B cell subsets2-4
Immature B cells repopulate from bone marrow4
• In presence of CD4 T regs5,
• In presence of CD8 T cells5,6
Med
ian
(Q
1 –
Q3 C
D19
+ B
lym
ph
oc
yte
s (
cell
s/µ
l)
79
22
0
81
20
3
61
13
7
74
19
1
78
19
5
38 56 68 64 49 33
Placebo
Cladribine tablets 3.5 mg/kg
Number of
patients
CD19+ B cells were markedly reduced, but on recovery they did not overshoot baseline levels1,2

aIn the clinical study database (1,976 patients, 8,650 patient-years) no case of PML has been reported, accurate at date of creation – Oct 2018. However, a baseline MRI should be considered before initiating MAVENCLAD® (usually within 3 months). This is particularly recommended if patients are switched from other MS agents that have a risk of PML; bCases of PML have been reported for parenteral cladribine in patients treated for hairy cell leukemia with a different treatment regimen. cPatients treated with a cumulative dose of MAVENCLAD® over 2 years as monotherapy; dCladribine can reduce the body’s immune defense and may increase the likelihood of infections2; eMalignancies were observed more frequently in cladribine-treated patients than in patients who received placebo in clinical trials. AE, adverse event. DMD, disease-modifying drug; MoA, mechanism of action; MRI, magnetic resonance imaging; PML, progressive multifocal leukoencephalopathy.
1. PREMIERE, 2009 https://clinicaltrials.gov/ct2/show/NCT01013350 [Accessed Oct 2018]; 2. MAVENCLAD® EU SmPC, July 2018;3. Cook S, et al. Mult Scler 2011;17:578–93; 4. Pakpoor J, et al. Neurol Neuroimmunol Neuroinflamm 2015;2:e158.
LYMPHOPENIA
Transient, mostly mild-to-moderate lymphopenia
was observed2
<1% of patientsc treated developed grade 4 (<200 cells/mm3)
lymphopenia2
MALIGNANCY
No conclusive evidence for an increased risk compared with
the general populatione,3
Cladribine has a malignancy rate comparable to other
DMDs4
INFECTIONS
Overall, risk is
comparable to placebo,
except for
herpes zosterd,2
Herpes zoster-associated
serious or severe events
rare and manageable3
Cladribine has up to 10 years of safety follow-up1
Cladribine had no reported cases of PML in
MSa,b,2
No reported cases of secondary
autoimmunity in MS1
Cladribine has a well-characterized safety profile

aCladribine can reduce the body’s immune defence and may increase the likelihood of infections2 Data shown is from CLARITY trial only. AE, adverse event; URTI, upper respiratory tract infection.
1. Giovannoni G, et al. N Engl J Med 2010;362:416–26; 2. Cook S, et al. ECTRIMS 2017; [P1142].
Most frequently
reported adverse
events
MAVENCLAD®
3.5mg/kg
N=430 (%)
Placebo
N=435 (%)
Any adverse event 80.7 73.3
Most common adverse
eventsa
Headache 24.2 17.2
Lymphocytopenia 21.6 1.8
Nasopharingytis 14.4 12.9
URTI 12.6 9.7
Nausea 10.0 9.0
Any serious adverse
events
8.4 6.4
Infections and
infestations
2.3 1.6
Neoplasmsb 1.4 0.0
Death 0.5 0.5
There was no
incidence of
opportunistic
infectionsa,2
0.7%
Grade 42
<200 cells/μL
24.9%
Grade 32
500–200 cells/μL
74.4%
Grade 0–22
>500 cells/μL
Transient, mostly mild-to-moderate lymphopenia was observed following Cladribine dosing1

CI, confidence interval; SIR, standardized incidence ratio. aSIR calculated against the GLOBOCAN (2012) reference population; non-melanoma skin cancer excluded due to inconsistent reporting in GLOBOCAN 2012. bThe aim of the GLOBOCAN (2012) project is to provide contemporary estimates of the incidence of, mortality and prevalence from major types of cancer, at national level, for 184 countries of the world. cThis cohort also contains data from combinations/indications that are not approved by the competent authority. However, the safety data have been included in the overall assessment. dIntegrated safety analysis of CLARITY, CLARITY EXT, ORACLE-MS, PREMIERE (oral monotherapy cohort) compared to global malignancy database GLOBOCAN 2012.
1. MAVENCLAD® European Public Assessment Report, June 2017.
8,3 8,0
0
5
10
15
20
25
30
Observed
Monotherapy oral cohortc,d (3.5 mg/kg)
Expected
(GLOBOCAN 2012b)
standardized incidence ratio:
0.97(95% CI 0.44, 1.85)
Expected vs observed malignancies with
Cladribine1
(N=923; 3433 patient years)
Un
iqu
e e
ven
ts o
f m
alig
nan
cy
a
Cladribine had no increased risk of malignancy compared with the general population

aIn the all-exposed cohort, the malignancy rate for cladribine during Years 1–4 (0.38) was identical to the rate during Years 5–8+, demonstrating that the malignancy rate
remained constant over time. PY, patient-years
1. Galazka A et al. ECTRIMS 2017 [P1878].
0,29 0,28
0,00
0,05
0,10
0,15
0,20
0,25
0,30
0,35
0,40
0,45
0,50
Years 1–4 Years 5–8+
No
. o
f m
alig
nan
cie
s p
er
100 P
YIncidence of malignancy per 100 PY
(monotherapy oral cohort)a,1
Patients with events 8 2
Time at risk, years 2715.45 711.84
n = 923
In up to 10 years of follow-up, there was no increase in malignancy incidence1

44
1. EXCEMED. Giovannoni G. EAN 2017 https://www.excemed.org/resources/how-transfer-concept-clinical-practice June 2017 [Accessed Feb 2018]; 2. Baker D et al. Neurol NeuroimmunolNeuroinflamm 2017;4:e360; 3. Massacesi L et al. PLoS One 2014;9:e113371; 4. Cassetta I et al. Cochrane Database Syst Rev 2007;17:CD003982; 5. Kieseier BC. CNS Drugs 2011;25:491–502; 6. Weber MS et al. Neurotherapeutics 2007;4:647–53.
Maintenance/escalation therapythat results in continuous immunosuppression1
Short-course therapythat reconstitutes the immune system
resulting in long-term qualitative changes
in immune function1
Maintenance/escalation therapythat results in continuous immunomodulation1
Maintenance/escalation therapy: Chronic therapy that is maintained and/or
escalated over time resulting in changes in immune function only during active treatment1
Immune reconstitution
therapy1,2
Chronic
immunosuppression3,4 Immunomodulation5,6
New classification pouposed: Immune reconstitution therapy (IRT) is a novel approach that differs from both chronic immunosuppression and immunomodulation1

aApproved in the US and EU.IRT, immune reconstitution therapy.
Giovannoni G. Sequencing workshop treatment algorithm 2018.https://www.slideshare.net/gavingiovannoni/sequencing-workshop-treatment-algorithm [Accessed Nov 2018].
A reduction of the activation or efficacy of the immune system
• This definition refers to short-term (IRTs) and long-term persistent immunosuppression(maintenance)
For a drug to be considered an immunosuppressant, it could cause:
• 1) significant lymphopenia
• 2) be associated with opportunistic infections
• 3) reduce the antibody response to vaccines
• 4) be associated with secondary malignancies
Immunosuppression

BL, baseline; CSF, cerebrospinal fluid; DMD, disease-modifying drug; IFN, interferon;LLN, lower limit of normal; m, Month; ON, on-treatment; OND, other neurological disease;PRE, pre-treatment; W, Week.
1. Ghadiri M, et al. Mult Scler 2017;23:1225–32; 2. Giovannoni G. EXCEMED CME on PIRT, June 2017;
3. Stϋve O, et al. Ann Neurol 2006;59:743–7;4. Spencer CM, et al. Neurol Neuroimmunol Neuroinflamm 2015;2:e76.
Treatment with fingolimod leads to
persistent reduction in peripheral lymphocyte counts with recovery
upon cessation1,a
Ocrelizumabdecreases CD19+ cells to negligible levels by Week 2 of treatment,
with return to LLN more than 1 year after
cessation2
Natalizumab causes reductions in T cells
and B cells in the CSF that persist for up to 6
months after treatment cessation3
Current DMDs are associated with continuous immunosuppression during treatment, with variable rate of lymphocyte recovery upon cessation
DMF causes chronic reductions in lymphocytes4
0.0
0.5
1.0
1.5
2.0
2.5
PRE ON W2 W3–4 M8–9
Tota
l lym
ph
ocy
te c
ou
nt
(x1
09
cells
/L)
LLN
0.0041<0.0001
Time
Lower Limit of Normal
<0.0001
<0.0001
CD
4+
T ce
lls/m
L (C
SF)
0.45<0.0001
0
5000
10,000
15,000
20,000
25,000
Time
Placebo (N=54)Ocrelizumab 1000 mg (N=55)Ocrelizumab 600 mg (N=55)im IFN -1a (N=54)
LLN
Lymphocytes
Month
Tota
l lym
ph
ocy
te c
ou
nt
(x1
09
cells
/L)
N=16
N=16
N=35
N=23
N=14
N=34
N=21
N=15
N=17
Many maintenance/escalation therapies chronically lower lymphocyte levels

1. Winkelmann A et al. Clin Exp Immunol 2014;175:425–38; 2. Dendrou CA et al. Nat Rev Immunol 2015;15:545–58;
3. Nath A, Berger JR. Curr Treat Options Neurol 2012;14:241–55; 4. Stokmaier D et al. EAN 2018 [POD399];
5. Pakpoor J et al. Neurol Neuroimmunol Neuroinflamm 2015;2:e158
The immune
system defends
against infections
and tumours
Neutrophil
deficits
T-cell or
monocyte
abnormalities
Humoral
immunity
disorders
Bacteria, fungi
Bacteria,
parasites, viruses,
fungi
Bacteria
Immunosuppression increases infection risk
Some lymphocyte-targeting therapies are associated with an increased risk of
malignancy,
which varies between therapies and individual studies2,5
Immunosuppression may decrease efficacy of vaccines4
Continual B-cell
suppression
Decreased humoral
response to
vaccination
Potential risks of continuous immunosuppression1–4

Basal Cell
Carcinoma
Zoster
Cumulative Risk
Frontloading Risk
Listeria
TB
Nocardia PCP
Lymphoma
Cryptococcosis
2°autoimmunity
post- Az
Short-termAcute immunosuppression: innate and T-cell
Continuous Chronic immunosuppression
Giovannoni G. Sequencing workshop treatment algorithm 2018.https://www.slideshare.net/gavingiovannoni/sequencing-workshop-treatment-algorithm [Accessed Nov 2018].
aNot licensed; blicensed in the US, Germany, Austria and France; clicensed in Europe, Canada, Argentina, Australia and UAE.BMT, bone marrow transplant; HSCT, hematopoietic stem cell transplant; IFN, interferon; IM, intramuscular; PI, prescribing information; PPMS, primary progressive MS; RMS, relapsing MS;R-SPMS, relapsing secondary progressive MS; SC, subcutaneous; SmPC, summary of product characteristics.
Immunosuppression

Baseline
1. FBC—leukocytes/platelets2. LFTs, U&E, TFTs, urine3. Pregnancy tests4. Immunoglobulin levels5. Serum protein
electrophoresis6. Serology
a. JCVb. HIV-1&2c. Hepatitis B&Cd. VZVe. Syphilisf. TB Elispot
7. Cervical smear8. Vaccinations9. MRI10. LP—CSF analysis
sequencing11. Listeria, PCP prophylaxis
a. Dietb. Prophylactic
antibiotics
Infusion—DMTs & IRTs
1. Infusion reactions
a. Corticosteroid
s
b. Antihistamine
s
c. Antipyretics
2. Antibiotics
a. Anti-herpes
b. Listeria/PCP
prophylaxis
Monitoring
1. Bloods
a. FBC—
leukopenia
b. TFTs, LFTs,
U&E, …..
2. Urine
a. Autoimmune
b. Renal
dysfunction
3. MRI
a. Disease activity
b. PML
4. Infection
a. Serology
b. CSF
5. Disease activity
6. Pregnancy
7. Malignancy
a. Skin, Cervical,
Breast
b. Etc.
12
3
CSF, cerebrospinal fluid; DMT, disease-modifying therapy; FPC, full blood count; HIV, human immunodeficiency virus; IRT, immune reconstitution therapy; JCV, John Cunningham virus; LFT, liver function test; LP, lumbar puncture; MRI, magnetic resonance imaging; PCP, pneumocystis carinii pneumonia; PML, progressive multifocal leukoencephalopathy TB, tuberculosis; TFT, thyroid function test; U&E, urea and electrolytes; VZV, varicella zoster virus
Giovannoni G. Sequencing workshop treatment algorithm 2018.https://www.slideshare.net/gavingiovannoni/sequencing-workshop-treatment-algorithm [Accessed May 2018].
De-risking immunosuppression

1. Gilenya® SmPC, 2017; 2. Lemtrada® SmPC, 2016. 3. Tysabri® SmPC, 2017; 4. HSCT NHS guidelines.http://nssg.oxford-haematology.org.uk/bmt/long-term/B-2-13-allograft-and-autograft-immunisation-schedule.pdf; 5. MAVENCLAD® SmPC, July 2018;
IRTsMaintenance
5
1
3
4
natalizu
mab
Vaccines2
It is recommended that patients have completed local immunisation requirements
at least 6 weeks prior to treatment with alemtuzumab. The ability to generate an
immune response to any vaccine following alemtuzumab treatment has not been
studied.
The safety of immunistation with live viral vaccines following a course of
alemtuzumab treatment has not been formally studied in controlled clinical trials in
MS and should not be administered to MS patients who have recently received a
course of alemtuzumab.
Varicella zoster virus antibody testing/vaccination
As for any immune modulation medicinal product, before initiation a course of
alemtuzumab treatment, patients without a history of chickenpox or without
vaccination against varicella zoster virus (VZV) should be tested for antibodies to
VZV. VZV vaccination of antibody-negative patients should be considered prior
to treatment initiation with alemtuzumab. To allow for the full effect of the VZV
vaccination to occur, treatment with alemtuzumab should be postponed for 6
weeks following vaccination
Vaccinations

APPROVED MULTIPLE SCLEROSIS TREATMENTSAFETY
All the following slides are adapted from A Consensus Paper bythe Multiple Sclerosis Coalition updated on March 2017

Drug Side effects Warnings/precautions
Glatiramer acetate (Copaxone®) 20mg SC daily or 40mg SC threetimes weekly
Indication: relapsing forms of MS (Glatopa® - therapeutic equivalent) 20mg SC daily
Indication: relapsing forms of MS
Pregnancy Cat: B
• injection-site reactions• Lipoatrophy• vasodilation, rash, dyspnea -
chest pain• lymphadenopathy
immediate transient post-injectionreaction (flushing, chest pain, palpitations, anxiety, dyspnea, throatconstriction, and/or urticaria) -lipoatrophy and skin necrosis -potential effects on immune response

Drug Side effects Warnings/precautions
interferon beta-1a (Avonex®) 30mcg IM weeklyIndication: relapsing forms of MS Pregnancy Cat: C
• flu-like symptoms• depression • ↑hepatic transaminases
• depression, suicide, psychosis
• hepatic injury• anaphylaxis and other
allergic reactions• CHF • ↓peripheral blood counts• Seizures• other autoimmune
disorders• thrombotic
microangiopathy
Drug Side effects Warnings/precautions
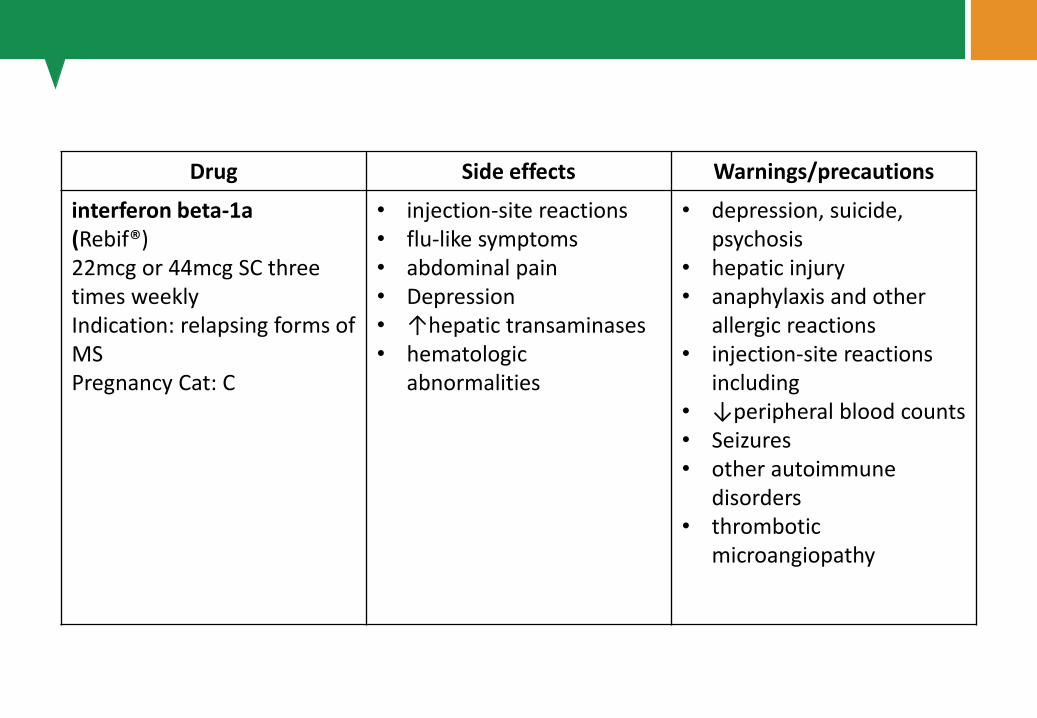
interferon beta-1a(Rebif®) 22mcg or 44mcg SC three times weekly Indication: relapsing forms of MS Pregnancy Cat: C
• injection-site reactions• flu-like symptoms• abdominal pain• Depression• ↑hepatic transaminases• hematologic
abnormalities
• depression, suicide, psychosis
• hepatic injury• anaphylaxis and other
allergic reactions• injection-site reactions
including• ↓peripheral blood counts• Seizures• other autoimmune
disorders• thrombotic
microangiopathy

Drug Side effects Warnings/precautions
interferon beta-1b(Betaseron®) (Extavia®) 0.25mg SC every other day Indication: relapsing forms of MS Pregnancy Cat: C
• flu-like symptoms • injection-site reactions• ↑hepatic transaminases • ↓ WBC
• hepatic injury• anaphylaxis and other
allergic reactions• depression and suicide• CHF• injection-site necrosis• ↓ WBC -flu-like
symptoms• seizures• thrombotic
microangiopathy

Drug Side effects Warnings/precautions
peginterferon beta-1a (Plegridy®) 125mcg SC every two weeks Indication: relapsing forms of MS Pregnancy Cat: C
• flu-like symptoms • injection-site reactions• ↑hepatic transaminases • ↓ WBC
• depression, suicide• hepatic injury• anaphylaxis and other
allergic reactions• CHF• ↓peripheral blood counts• Seizures• other autoimmune
disorders• thrombotic
microangiopathy

Drug Side effects Warnings/precautions
dimethyl fumarate(Tecfidera®) 240mg PO twice dailyIndication: relapsing forms of MS Pregnancy Cat: C
• anaphylaxis and angioedema
• progressive multifocal leukoencephalopathy (PML)
• lymphopenia• elevated AST• liver injury• flushing• GI symptoms -pruritis -
rash
• anaphylaxis and angioedema
• PML• lymphopenia (discontinue
treatment in patientswith persistentlymphopenia (<500) over 6 months) -flushing
• liver injury

Drug Side effects Warnings/precautions
fingolimod (Gilenya®) 0.5mg PO dailyIndication: relapsing forms of MS Pregnancy Cat: C
• Headache• Influenza• Diarrhea• back pain• ↑hepatic enzymes• Cough• bradycardia during first dose• macular edema• Lymphopenia• bronchitis/pneumonia
• bradyarrhythmia and/or atrioventricular block following first dose
• risk of infections including serious infections – monitor for infection during treatment and for 2 months after d/c
• avoid live attenuated vaccines during treatment and for 2 months after d/c
• PML • cryptococcal infections• macular edema• posterior reversible encephalopathy
syndrome (PRES)• ↓pulmonary function tests (FEV1)• hepatic injury• ↑BP • basal cell carcinoma• fetal risk: women should avoid
conception for two months aftertreatment d/c
• ↓lymphocyte counts for 2 months afterdrug d/c
Drug Side effects Warnings/precautions
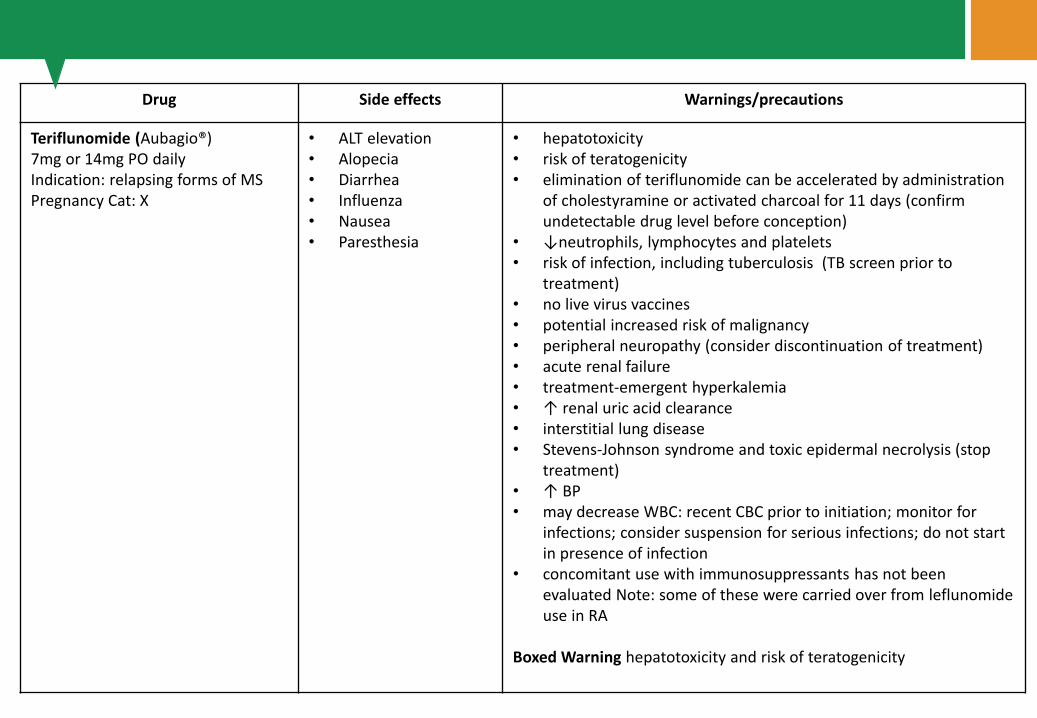
Teriflunomide (Aubagio®) 7mg or 14mg PO daily Indication: relapsing forms of MS Pregnancy Cat: X
• ALT elevation• Alopecia• Diarrhea• Influenza• Nausea• Paresthesia
• hepatotoxicity• risk of teratogenicity• elimination of teriflunomide can be accelerated by administration
of cholestyramine or activated charcoal for 11 days (confirmundetectable drug level before conception)
• ↓neutrophils, lymphocytes and platelets• risk of infection, including tuberculosis (TB screen prior to
treatment)• no live virus vaccines• potential increased risk of malignancy• peripheral neuropathy (consider discontinuation of treatment)• acute renal failure• treatment-emergent hyperkalemia• ↑ renal uric acid clearance • interstitial lung disease• Stevens-Johnson syndrome and toxic epidermal necrolysis (stop
treatment) • ↑ BP• may decrease WBC: recent CBC prior to initiation; monitor for
infections; consider suspension for serious infections; do not start in presence of infection
• concomitant use with immunosuppressants has not been evaluated Note: some of these were carried over from leflunomideuse in RA
Boxed Warning hepatotoxicity and risk of teratogenicity

Drug Side effects Warnings/precautions
Alemtuzumab (Lemtrada®) 12mg/day IV on five consecutive days followed 12 months later by 12mg/day on three consecutive days Indication: relapsing forms of MS – generally for patients who have had an inadequate response to two or more MS therapies Pregnancy Cat: C
->90% of patients in clinical trials experienced infusion reactions: skin rash, fever, headache, muscle aches, temporary reoccurrence of previousneurologic symptoms. More serious butuncommon infusion reactions: anaphylaxis and heart rhythmabnormalities. -serious adversereactions: autoimmunity, infusionreactions, malignancies, immune thrombocytopenia (ITP), glomerularnephropathies, thyroid disorder, otherautoimmune cytopenias, infections, pneumonitis -immediate and significantdepletion of lymphocytes; herpes simplex and zoster infections more common in patients who receivedalemtuzumab in the clinical trials, especially soon after the infusions. Prophylaxis with anti-viral agent isrecommended for at least two months or until CD4 count is >200.
• infusion reactions• autoimmunity (thyroid disorders, immune
thrombocytopenia (ITP), glomerularnephropathies, other cytopenias)
• infections• no live virus vaccinations following infusion• malignancies (thyroid, melanoma,
lymphoproliferative) • pneumonitis
Boxed WarningBecause of the risk of autoimmunity, life threatening infusion reactions, and malignancies, alemtuzumab is available only through restricted distribution under a Risk Evaluation Mitigation Strategy (REMS) program.

Drug Side effects Warnings/precautions
Mitoxantrone(Novantrone®) 12mg/m2 IV every three months; maximum cumulative dose: 140mg/m2 Indication: worsening relapsing-remitting, progressive-relapsing, secondary progressive MS Pregnancy Cat: D
• temporary blue discolorationof sclera and urine
• Nausea• Alopecia• menstrual disorders
including amenorrhea and infertility -infections (URI, UTI, stomatitis)
• cardiac toxicity (arrhythmia, abnormal EKG, congestive heart failure).
• severe local tissue damage if there is extravasation
• Cardiotoxicity• acute myelogenous leukemia• myelosuppression
Boxed Warning cardiotoxicity and secondary leukemia (monitoring required long-term following discontinuation)

Drug Side effects Warnings/precautions
Natalizumab(Tysabri®) 300mg IV every 28 days Indication: relapsing forms of MS Pregnancy Cat: C
• Headache• Fatigue• urinary tract infection• lower respiratory tract infection• Arthralgia• Urticaria• Gastroenteritis• Vaginitis• Depression• Diarrhea
• PML• Hepatotoxicity• herpes encephalitis and meningitis caused by
herpes simplex and varicella zoster viruses• Hypersensitivities• Immunosuppression/infections
Boxed Warning Because of the risk of PML, natalizumab is available only through a restricted distribution program called the TOUCH® Prescribing Program.
Drug Side effects Warnings/precautions
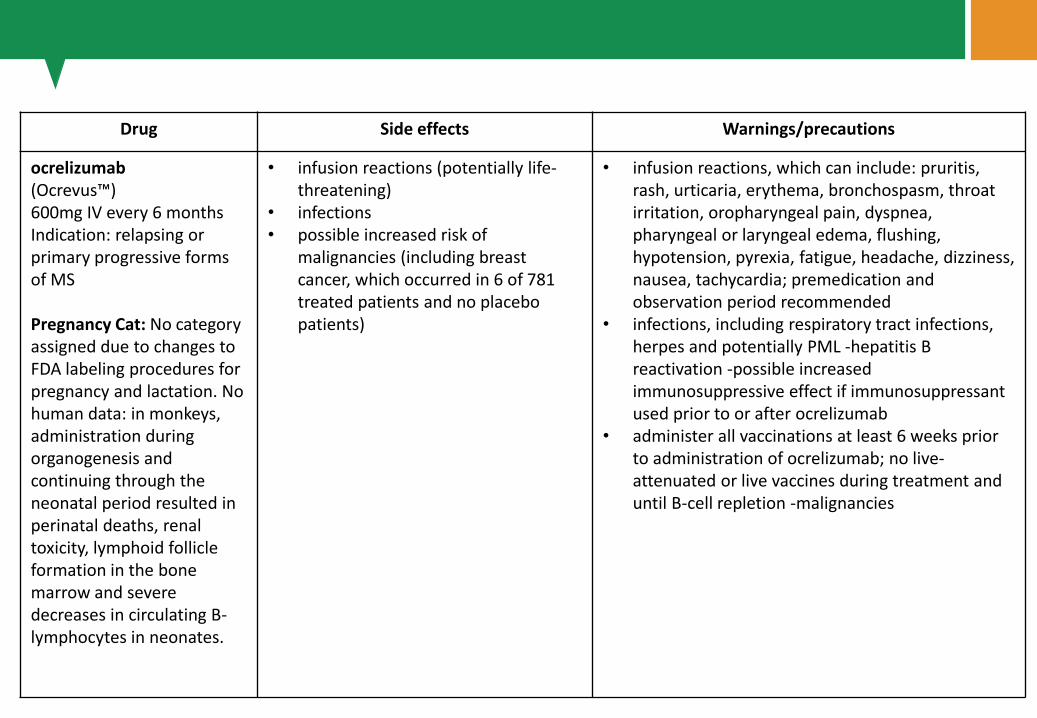
ocrelizumab(Ocrevus™) 600mg IV every 6 months Indication: relapsing or primary progressive forms of MS
Pregnancy Cat: No category assigned due to changes to FDA labeling procedures for pregnancy and lactation. No human data: in monkeys, administration during organogenesis and continuing through the neonatal period resulted in perinatal deaths, renal toxicity, lymphoid follicle formation in the bone marrow and severe decreases in circulating B-lymphocytes in neonates.
• infusion reactions (potentially life-threatening)
• infections• possible increased risk of
malignancies (including breast cancer, which occurred in 6 of 781 treated patients and no placebo patients)
• infusion reactions, which can include: pruritis, rash, urticaria, erythema, bronchospasm, throat irritation, oropharyngeal pain, dyspnea, pharyngeal or laryngeal edema, flushing, hypotension, pyrexia, fatigue, headache, dizziness, nausea, tachycardia; premedication and observation period recommended
• infections, including respiratory tract infections, herpes and potentially PML -hepatitis B reactivation -possible increased immunosuppressive effect if immunosuppressant used prior to or after ocrelizumab
• administer all vaccinations at least 6 weeks prior to administration of ocrelizumab; no live-attenuated or live vaccines during treatment and until B-cell repletion -malignancies

Progetto realizzato con
il contributo non
condizionante di:
Fine