measurement of head impacts in collegiate football players - the
TRANSCRIPT

1244 | VOLUME 61 | NUMBER 6 | DECEMBER 2007 www.neurosurgery-online.com
CLINICAL STUDIES
MEASUREMENT OF HEAD IMPACTS IN COLLEGIATEFOOTBALL PLAYERS: RELATIONSHIP BETWEEN HEADIMPACT BIOMECHANICS AND ACUTE CLINICALOUTCOME AFTER CONCUSSION
OBJECTIVE: To determine the relationship between recorded head accelerations andimpact locations and acute clinical outcome of symptomatology, neuropsychological,and postural stability tests after cerebral concussion in Division I collegiate footballplayers.METHODS: A prospective field study was used in which accelerometers were embed-ded in the football helmets of 88 collegiate football players. Linear and rotational accel-erations of all head impacts sustained over the course of 2004 to 2006 National CollegiateAthletic Association football seasons were collected in real-time. Change scores werecalculated on clinical measures from the players’ preseason baseline to postinjury(within 48 h) and regressed against the recorded linear and rotational accelerations ofthe head at the time of the concussion.RESULTS: Thirteen concussions were recorded ranging in impact magnitudes of 60.51to 168.71 g. Linear regression showed no significant relationships between impact mag-nitude (linear or rotational acceleration) or impact location and change scores for symp-tom severity, postural stability, or neurocognitive function (P � 0.05).CONCLUSION: Our findings suggest that football players are concussed by impactsto the head that occur at a wide range of magnitudes and that clinical measures of acutesymptom severity, postural stability, and neuropsychological function all appear to belargely independent of impact magnitude and location. Because of the varying magni-tudes and locations of impacts resulting in concussion as well as other factors such asthe frequency of subconcussive impacts and number of previous concussions, it maybe difficult to establish a threshold for concussive injury that can be applied to all foot-ball players.
KEY WORDS: Acceleration, Helmet, Injury threshold, Mild traumatic brain injury, Neuropsychological func-tion, Postural stability
Neurosurgery 61:1244–1253, 2007 DOI: 10.1227/01.NEU.0000280146.37163.79 www.neurosurgery-online.com
Kevin M. Guskiewicz, Ph.D.Department of Exercise and Sport Science,Curriculum in Human Movement Scienceand Injury Prevention Research Center,The University of North Carolina,Chapel Hill, North Carolina
Jason P. Mihalik, M.S.Department of Exercise and Sport Science,Curriculum in Human Movement Science,The University of North Carolina,Chapel Hill, North Carolina
Viswanathan Shankar, M.Sc.Injury Prevention Research Center, andDepartment of Biostatistics,The University of North Carolina,Chapel Hill, North Carolina
Stephen W. Marshall, Ph.D.Injury Prevention Research Center, andDepartment of Epidemiology,The University of North Carolina,Chapel Hill, North Carolina
Dean H. Crowell, M.A.Division of Sports Medicine,Campus Health Services,The University of North Carolina,Chapel Hill, North Carolina
Scott M. Oliaro, M.A.Division of Sports Medicine,Campus Health Services,The University of North Carolina,Chapel Hill, North Carolina
Mario F. Ciocca, M.D.Division of Sports Medicine,Campus Health Services,The University of North Carolina,Chapel Hill, North Carolina
Daniel N. Hooker, Ph.D., P.T.Division of Sports Medicine,Campus Health Services,The University of North Carolina,Chapel Hill, North Carolina
Reprint requests:Kevin M. Guskiewicz, Ph.D.,University of North Carolina at Chapel Hill,209 Fetzer Gymnasium (CB# 8700),South Road,Chapel Hill, NC 27599.Email: [email protected]
Received, March 30, 2007.
Accepted, August 3, 2007.
Over the past 20 years, playing fields,athletic training rooms, and sportsmedicine clinics have served as work-
ing laboratories in which clinicians andresearchers have learned about mild traumaticbrain injury, often referred to as sport-relatedconcussion. These injuries are now recognizedas a major public health concern (23, 42, 43),and deciding when an athlete can safely returnto participation after a concussion is perhapsthe most challenging task of any sports medi-cine clinician. Previous reports estimated thatnearly 63,000 concussions occur annually in
high school sports (39), whereas a new reportsuggests that an estimated 1.6 to 3.8 millioncases of mild traumatic brain injury occur insports and recreation each year in the UnitedStates (24). A study of high school and colle-giate football players published in 2000 esti-mated that more than 5% of all players sustaina concussion during a single season and thatnearly 15% of those injured players sustain arepeat concussion within the same season (20).More recent National Collegiate Athletic As-sociation Injury Surveillance System data from2000 to 2005 indicate that the game-related

PATIENTS AND METHODS
Eighty-eight Division I collegiate football players (age at start ofenrollment, 20.18 � 1.80 yr) at the University of North Carolina atChapel Hill participated in this study over a 3-year period. The studyperiod included three fall and two spring seasons. Forty participantswere enrolled for one season, 17 were enrolled for at least two seasons,21 participated in three seasons, seven were enrolled for four seasons,and three players participated in all five seasons. Our sample wasrepresentative of many playing positions, including 25 offensive line-men, 15 defensive linemen, 17 defensive backs (including cornerbacksand safeties), 11 linebackers, 14 offensive backs (including fullbacks,running backs, and tailbacks), seven wide receivers, and six otherpositions (including quarterbacks, deep snappers, and kickers). Sevenplayers changed positions over the course of their enrollment in ourstudy, which explains the disparity between the number of playersenrolled in the study and the number of players per position thatappears in our results.
Participants were equipped with a helmet accelerometer telemetrysystem that measured the specific impact locations and magnitude ofacceleration during all practices and games. Before their enrollment inthe study, participants were assessed for baseline postural stability,neuropsychological function, and symptom grading. Participants whowere suspected of sustaining a concussion during the season were firstevaluated by the team physician. This was followed by a reassessmenton the same standardized clinical measures of concussion within thefirst 24 to 48 hours after sustaining the injury, and these data werecompared against preseason measures. Concussion was defined as aninjury resulting from a blow to the head that caused an alteration inmental status and one or more of the following symptoms: headache,nausea, vomiting, dizziness/balance problems, fatigue, trouble sleep-ing, drowsiness, sensitivity to light or noise, blurred vision, difficultyremembering, and difficulty concentrating. Before the start of the study,a detailed explanation of the study was provided for all the participat-ing players. Informed consent documents were approved by the uni-versity’s Institutional Review Board and were signed by each partici-pant before an athlete’s helmet was instrumented.
Instrumentation
Measuring Head Impact MagnitudePlayers wore helmets equipped with the Head Impact Telemetry
(HIT) system (Simbex, Lebanon, NH). The HIT System obtained datafrom accelerometer units comprised of six spring-mounted single-axisaccelerometers embedded in Riddell VSR-4 and Revolution footballhelmets (Riddell Corp., Elyria, OH). The signal transducer was linkedto a laptop computer in the sideline response system throughradiowave transmission (903–927 MHz). The information was storedon an onboard memory system (up to 100 impacts) or was immediatelytransferred to the laptop computer system (eight-bit, 1000 Hz/channel).The downloaded impacts were processed through a validation algo-rithm, and peak head linear and rotational acceleration were com-puted. The HIT System was previously validated in laboratory testingwith hybrid dummies equipped with football helmets (11, 35). Afterconcussive injury, the HIT System data were retrieved and confirmedthrough video observation based on time-stamped footage of the gameor practice.
Postural Stability TestingThe Sensory Organization Test (SOT) (NeuroCom International Inc.,
Clackamas, OR) was used to assess participants’ postural stability dur-
concussion incidence rate in collegiate football has graduallyincreased over this 6-year span from 2.90 to 3.91 concussionsper 1000 athlete-exposures (33).
A follow-up study of collegiate football players reported that,on average, concussed players’ symptoms gradually resolvedwithin 7 days, cognitive functioning improved to baseline lev-els within 5 to 7 days, and balance deficits dissipated within 3to 5 days postinjury. There were no significant symptoms orfunctional impairments at 3 months postinjury (28). Similar tothe earlier study, an association was observed between thereported number of previous concussions and the likelihood ofsustaining an incident concussion. Players reporting a historyof three or more previous concussions were more than threetimes more likely to sustain a concussion than players with nohistory of concussion, and these players experienced a slowerrecovery compared with those with fewer previous concus-sions. Of repeat concussions sustained within the same season,92% occurred within 10 days of the initial injury and 75%occurred within 7 days of the first injury (17).
Despite several significant scientific advancements for vali-dating concussion assessment tools, there has been a lack ofbiomechanical studies to help clinicians better understand themechanisms of injury and to define a threshold for concussiveinjury. Recent studies using a combination of video analysisand dummy reenactments have helped to advance our under-standing of impact biomechanics in football players; however,these have not been combined with clinical measures. Pellmanet al. (36, 37) published a series of studies based on concussiveinjuries occurring during professional football games. Thisgroup used video data to reconstruct the angle, speed, andresultant player kinematics of the injury to propose a potentialinjury threshold of 70 to 75 g (37). Although Pellman et al. sug-gested a 75% injury tolerance level for impacts above 98 g, ourcompanion paper (32) found only a 0.3% injury tolerance levelfor impacts above 80 g. The work of Duma et al. (11) furthersupports this most recent finding because they captured peaklinear accelerations using a newly developed in-helmet six-accelerometer system that measured head impacts in real-timefor a small sample of Division I football players. The authorsreported a mean peak linear acceleration of the head of 32 gand observed one concussive injury with a peak linear acceler-ation of 81 g. The major finding of this study was that the hel-met-mounted accelerometer system proved effective at collect-ing thousands of head impact events in real-time.
The natural course and extent of recovery from concussionis better understood today than it was just 10 years ago; how-ever, significant variability exists with respect to outcomeduring the acute period after injury. Recovery rates may varysignificantly across individual athletes, and the role of impactmagnitude in this equation has yet to be investigated. Thepurpose of our study was to capture real-time head impactsto determine the relationship between the recorded headaccelerations and location and acute clinical outcome ofsymptomatology, neuropsychological and postural stabilitytests during the initial 48 hours after cerebral concussion incollegiate football players.
NEUROSURGERY VOLUME 61 | NUMBER 6 | DECEMBER 2007 | 1245
CONCUSSION RECOVERY AND BIOMECHANICS

ing preseason baseline screening and during the postinjury evaluation.This force plate system measures vertical ground reaction forces pro-duced from the body’s center of gravity (COG) moving around a fixedbase of support. The SOT is designed to systematically disrupt the sen-sory selection process by altering available somatosensory and/orvisual information while measuring a subject’s ability to minimize pos-tural sway. The SOT has been used to assess postural stability after con-cussion in athletes and has proven to be a reliable and valid instrument(18, 19, 38, 40, 41).
The test protocol consists of six 20-second trials of quiet standing inwhich three different visual conditions (eyes open, eyes closed, swayreferenced visual surround) are crossed with two different surface con-ditions (fixed, sway referenced) (Fig. 1). Patients are asked to stand asmotionless as possible in a normal stance with the feet shoulder-widthapart. The term sway referencing involves the tilting of the support sur-face and/or visual surround to directly follow the athlete’s COG sway.During sway reference support surface conditions (Conditions 4–6),the force plate tilts synchronously with the patient’s anteroposterior(AP) COG sway. Similarly, during sway referenced visual surroundconditions (Conditions 3 and 6), the visual surround tilts synchro-nously with AP COG sway. Sway referencing causes orientation of thesupport surface or visual surround to remain constant relative to bodyposition. The SOT can assess the patient’s ability to ignore the inaccu-rate information from the sway referenced senses. A composite equilib-rium score describing a person’s overall level of performance during allof the trials in the SOT is calculated with higher scores being indicativeof better balance performance. The composite score is the average ofthe following 14 scores: the two mean equilibrium scores from each ofthe first two conditions and the equilibrium scores from each of thethree trials in Conditions 3 to 6. The equilibrium scores from each of thetrials represent a nondimensional percentage comparing the subject’speak amplitude of AP sway to the theoretical AP limit of stability.Lower percentages result in a higher (i.e., better) composite score.
Neuropsychological TestingParticipants were tested using the Automated Neuropsychological
Assessment Metrics (ANAM) battery to assess neurocognitive perform-ance. This computerized neuropsychological test battery was devel-oped by researchers at the National Rehabilitation Hospital inWashington, DC over the past 20 years and has been shown to be validand reliable (6, 9). More recent studies have confirmed the ANAM’susefulness in sports settings and have begun to establish normativescores for athletes (5, 7). The battery consists of seven modules thatinclude the following: Simple Reaction Time 1, Math Processing, Matchto Sample, Procedural Reaction Time, Code Substitution, SternbergProcedure, and Simple Reaction Time 2. Although the order by whichthe modules are presented to the participant remain constant, the stim-uli in each of the modules is randomly presented in follow-up test ses-sions to limit practice effects. Scores from the seven modules are com-bined for a composite (average) score.
Instructions for each ANAM subtest appeared on a personal com-puter screen as did stimuli. Data were collected, processed, and storedon a personal computer as the ANAM battery was completed.Throughput scores combining speed and accuracy were calculatedand expressed in milliseconds. One or two button mouse responseswere required for each subtest. To decrease anticipatory responses, avariable interstimulus interval was used for individual stimuli on eachsubtest.
The Simple Reaction Time 1 and Simple Reaction Time 2 modulesare traditional reaction time tests measuring response time to an aster-isk-like symbol (*) stimulus in the center of the computer screen. A
1246 | VOLUME 61 | NUMBER 6 | DECEMBER 2007 www.neurosurgery-online.com
GUSKIEWICZ ET AL.
total of 25 trials were collected with a 9000-ms upper limit in responsetime. The Simple Reaction Time 2 module is a repeat of SimpleReaction Time 1 at the conclusion of the battery, which allows for theassessment of reaction time after acute cognitive fatigue. In the CodeSubstitution subtest, a key with nine different symbols and nine paireddigits was presented in the upper portion of the screen. A singledigit/symbol pairing appeared beneath, and the patients respondedindicating whether or not the single pairing correctly represented thekey above. Thirty-six trials were presented with a maximum of 9500-ms response time. For the Match to Sample scores, a checkerboardmatrix was presented for 3 seconds while the subject memorized it.Two matrices were then presented side by side after a 5-second delay,and the patient indicated which matrix was the initial matrix pre-sented with a right or left mouse button click. The Sternberg Proceduresubtest required the patients to memorize a set of six capital letterspresented on the screen. The letters disappeared when patients indi-cated they had memorized the letters. A series of individual lettersthen appeared on the screen, and the patient decided whether or notthe appearing letters were in the set of the original six. In the MathProcessing subtest, a two-step arithmetic problem involving additionand/or subtraction was presented. Subjects had to solve the problemand then indicate with a right or left click whether the answer was lessthan or greater than five. There was a greater probability of a rightclick compared with a left click for the 20 trials. The ProceduralReaction Time subtest measured reaction time with 20 items. One ofthe numbers 2, 3, 4, or 5 was presented on the screen as the stimulus,and the participant pressed the left mouse key if it was a 2 or a 3 or theright mouse key if it was a 4 or a 5.
Graded Symptom ChecklistThe Graded Symptom Checklist is a self-report symptom scale that
assesses the presence and severity of 18 concussion-related symptomsusing a seven-point Likert scale ranging from asymptomatic (0), tomild (1), to severe (6). During our baseline evaluation, participants
FIGURE 1. Illustration showing the six conditions of the NeuroComSensory Organization Test.

were instructed to rate the presence and severity of any symptom theyreported feeling at least three times per week over the course of thesummer preceding the baseline test session. During follow-up test ses-sions, the participants were asked to rate the presence and severity oftheir symptoms based on what they felt at the time of testing.Individual symptom scores were recorded and summed for an aggre-gate score on the Graded Symptom Checklist at each assessment point.This instrument has been widely used and validated in the sports con-cussion setting (17, 26, 28).
Data ReductionThe raw head impact data were exported from the Sideline Response
System into Matlab 7 (Mathworks, Inc., Natick, MA), where data wasreduced to include only those impacts that were sustained during prac-tices, scrimmages, and games; only impacts registering a linear accel-eration greater than 10 g were included for the purposes of our analy-ses. Impacts less than 10 g are considered negligible with respect toimpact biomechanics and their relationship to head trauma. Becauseeach impact was linked to a player enrolled in our study by a uniqueidentifier, we were able to easily associate impacts that belonged to aparticular player and categorize those impacts based on positionalinformation we had collected at the start of the season. Linear acceler-ation (g) and rotational acceleration (rads/s2) were the head impactoutcome measures of interest.
Data AnalysisDescriptive statistics and Pearson’s correlation coefficients were cal-
culated to assess the relationship between linear and rotational acceler-ation of head impacts and each outcome measure. Change scores frombaseline to postinjury (within 48 h of injury) were calculated for all out-come variables (Graded Symptom Checklist, SOT composite, andANAM composite). Linear regression was fitted to examine the rela-tionship between linear acceleration magnitudes and change scores foreach dependent variable. For ease of interpretation, linear magnitudewas centered with respect to the median of magnitude and scaleddownward by a factor of 10. This converted magnitude was fittedagainst each response variable: change in symptom score, change inSOT composite, and average ANAM standardized composite changescores, respectively. In addition to the standard linear regression model,we estimated a Jackknife variance to adjust for a small sample sizeand to avoid correlation among cases (45). The point estimates from thestandard linear regression model and the Jackknife model were consis-tent; for some analyses, Jackknife variance estimates were smaller thanstandard linear regression. We report the conservative estimates fromthe standard linear regression. Standard linear regressions were alsocomputed to relate the magnitude of rotational acceleration to eachdependent measure.
RESULTS
We recorded 104,714 total impacts over the course of fiveseasons in the 88 collegiate football players participating in ourstudy. Of these players, 11 sustained one concussive injury andone sustained two concussive injuries, resulting in a total of 13concussions. The average � standard deviation age, height,and mass of concussed players in the study was 19.7 � 1.09years, 185.4 � 4.4 cm, and 104.8 � 14.8 kg, respectively. Theaverage number of impacts experienced by concussed playersduring the session in which they were injured was 27.7 (range,
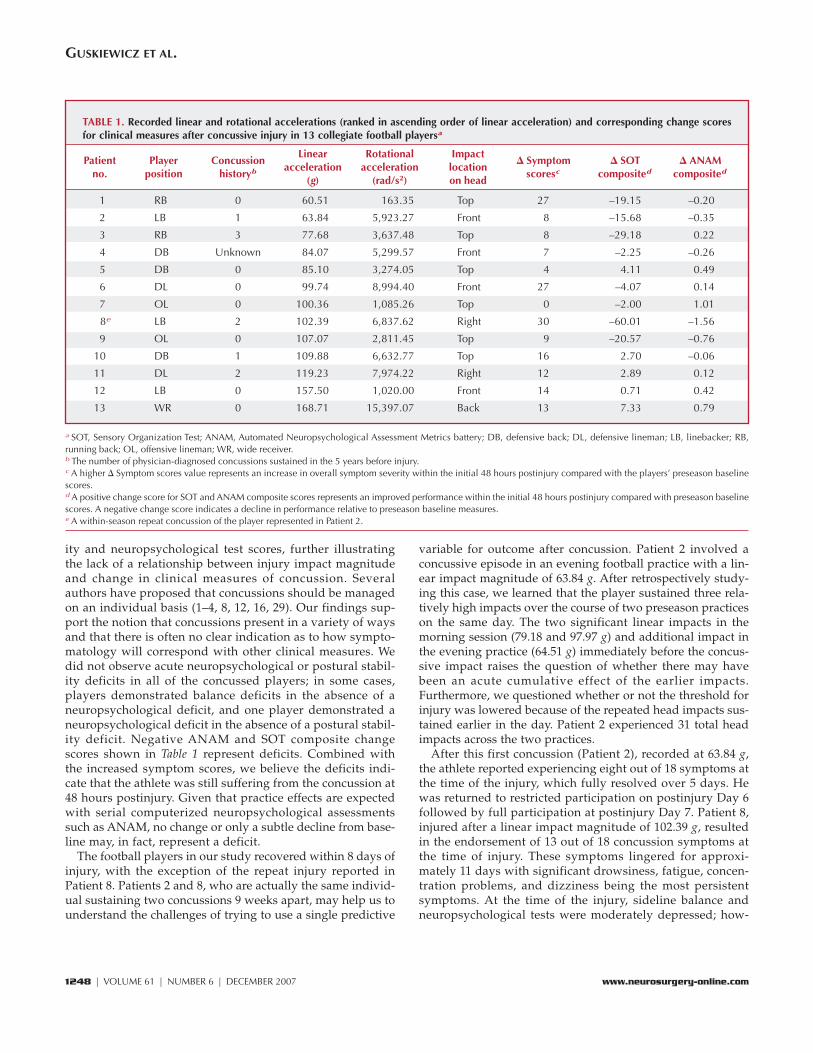
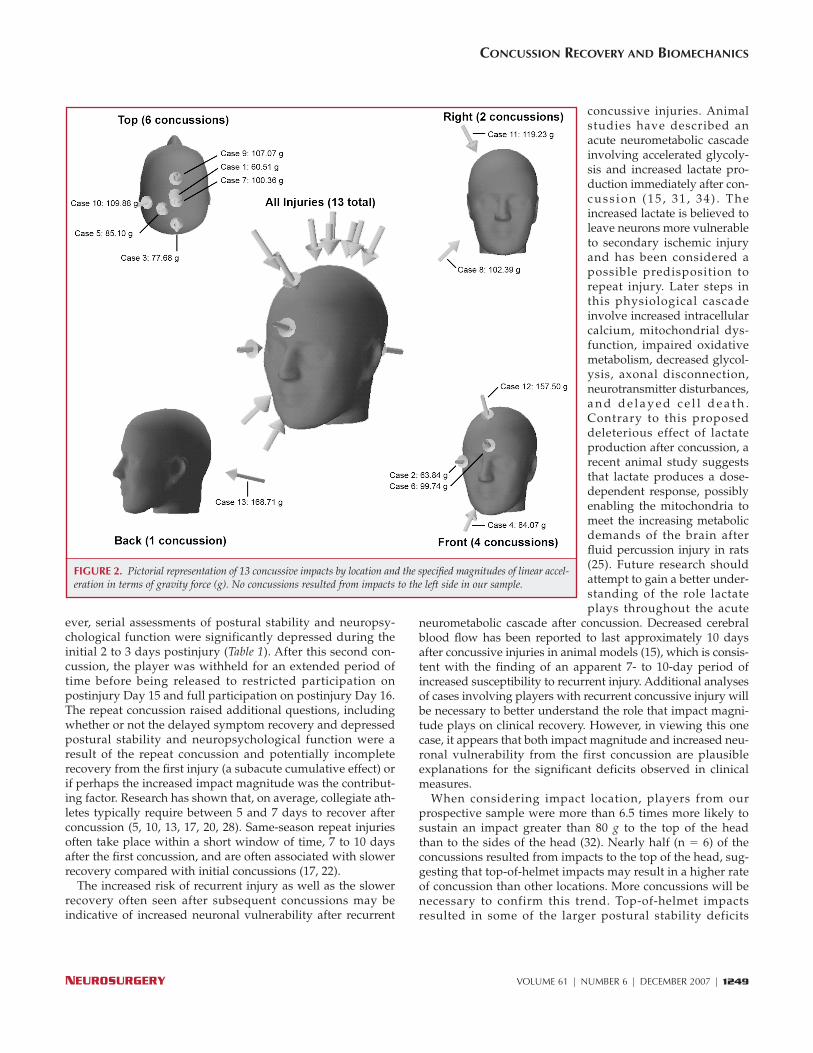
1–121 impacts). The average magnitude of concussive impactswas 102.8 g (range, 60.51–168.71 g). Recorded linear and rota-tional accelerations and corresponding change scores for clini-cal measures after concussive injury in the 13 injured playersare presented in Table 1. Pictorial representation of the concus-sive impacts by location and the specified magnitudes of linearacceleration are presented in Figure 2.
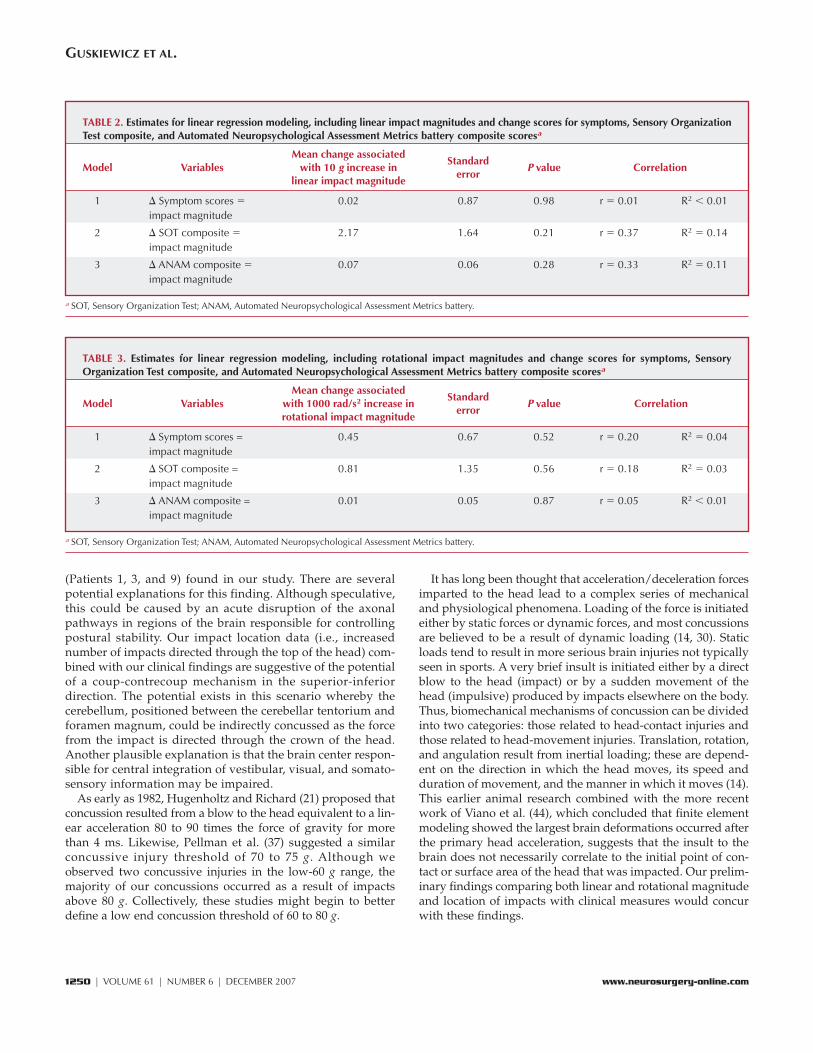
The correlation coefficient between centered scaled impactmagnitude and changed SOT composite, ANAM composite,and symptom score were 0.37, 0.33, and 0.01, respectively. Thethree univariate linear regression models showed no significantrelationships between magnitude and change scores for any ofthe dependent variables (P � 0.05) (Table 2). Likewise, inobserving the impact locations (front, top, and side/back) forthe 13 cases, they were not associated with either the magni-tude of the impact (P � 0.22) or the resultant clinical changescores after injury (SOT composite: P � 0.77; ANAM compos-ite: P � 0.81; symptom score: P � 0.54).
The correlation coefficient between rotational accelerationand changed SOT composite, ANAM composite, and symp-tom score were 0.179, 0.050, and 0.198, respectively. Similar tolinear impact magnitudes, no significant relationships wereobserved between head rotational accelerations and changescores for any of the dependent variables (P � 0.05) (Table 3).
DISCUSSION
There was no observed relationship between linear or rota-tional impact magnitude and acute outcome of symptomatol-ogy, postural stability, and neuropsychological functioning inour 13 cases of concussion in collegiate football players. Ourfindings suggest that football players are concussed by impactsto the head that occur at widely varying magnitudes of accel-eration and that clinical measures of acute symptom severity,postural stability, and neuropsychological function are largelyindependent of both linear and rotational impact magnitudesand location. Obviously, these findings need to be confirmed instudies involving larger samples of concussed athletes, whichwould provide more power to detect significant relationships;however, they do provide a preliminary evaluation of acuteclinical outcome after a wide spectrum of impact magnitudes.If proven, these findings would indicate that there are likelyother contributing factors that influence the occurrence of aconcussion as well as the rate of recovery after the concussion.These factors, which were not controlled for in this prelimi-nary study, may include concussion history and the frequencyof subconcussive impacts sustained in the days leading up tothe concussion. However, players sustaining concussions inour study did not experience an increased number of impactsto the head compared with their noninjured teammates overthe period of this study.
With respect to the symptom change scores, which rangedfrom 0 (no change) to 30, it was interesting that the lower-magnitude impacts resulted in slightly higher symptomchange scores within the initial 48 hours after injury (Table 1).We observed a similar trend in relation to the postural stabil-
NEUROSURGERY VOLUME 61 | NUMBER 6 | DECEMBER 2007 | 1247
CONCUSSION RECOVERY AND BIOMECHANICS
1248 | VOLUME 61 | NUMBER 6 | DECEMBER 2007 www.neurosurgery-online.com
GUSKIEWICZ ET AL.
ity and neuropsychological test scores, further illustratingthe lack of a relationship between injury impact magnitudeand change in clinical measures of concussion. Severalauthors have proposed that concussions should be managedon an individual basis (1–4, 8, 12, 16, 29). Our findings sup-port the notion that concussions present in a variety of waysand that there is often no clear indication as to how sympto-matology will correspond with other clinical measures. Wedid not observe acute neuropsychological or postural stabil-ity deficits in all of the concussed players; in some cases,players demonstrated balance deficits in the absence of aneuropsychological deficit, and one player demonstrated aneuropsychological deficit in the absence of a postural stabil-ity deficit. Negative ANAM and SOT composite changescores shown in Table 1 represent deficits. Combined withthe increased symptom scores, we believe the deficits indi-cate that the athlete was still suffering from the concussion at48 hours postinjury. Given that practice effects are expectedwith serial computerized neuropsychological assessmentssuch as ANAM, no change or only a subtle decline from base-line may, in fact, represent a deficit.
The football players in our study recovered within 8 days ofinjury, with the exception of the repeat injury reported inPatient 8. Patients 2 and 8, who are actually the same individ-ual sustaining two concussions 9 weeks apart, may help us tounderstand the challenges of trying to use a single predictive
variable for outcome after concussion. Patient 2 involved aconcussive episode in an evening football practice with a lin-ear impact magnitude of 63.84 g. After retrospectively study-ing this case, we learned that the player sustained three rela-tively high impacts over the course of two preseason practiceson the same day. The two significant linear impacts in themorning session (79.18 and 97.97 g) and additional impact inthe evening practice (64.51 g) immediately before the concus-sive impact raises the question of whether there may havebeen an acute cumulative effect of the earlier impacts.Furthermore, we questioned whether or not the threshold forinjury was lowered because of the repeated head impacts sus-tained earlier in the day. Patient 2 experienced 31 total headimpacts across the two practices.
After this first concussion (Patient 2), recorded at 63.84 g,the athlete reported experiencing eight out of 18 symptoms atthe time of the injury, which fully resolved over 5 days. Hewas returned to restricted participation on postinjury Day 6followed by full participation at postinjury Day 7. Patient 8,injured after a linear impact magnitude of 102.39 g, resultedin the endorsement of 13 out of 18 concussion symptoms atthe time of injury. These symptoms lingered for approxi-mately 11 days with significant drowsiness, fatigue, concen-tration problems, and dizziness being the most persistentsymptoms. At the time of the injury, sideline balance andneuropsychological tests were moderately depressed; how-
TABLE 1. Recorded linear and rotational accelerations (ranked in ascending order of linear acceleration) and corresponding change scoresfor clinical measures after concussive injury in 13 collegiate football playersa
Linear Rotational ImpactPatient Player Concussion
acceleration acceleration location� Symptom � SOT � ANAM
no. position historyb(g) (rad/s2) on head
scoresc composited composited
1 RB 0 60.51 163.35 Top 27 –19.15 –0.20
2 LB 1 63.84 5,923.27 Front 8 –15.68 –0.35
3 RB 3 77.68 3,637.48 Top 8 –29.18 0.22
4 DB Unknown 84.07 5,299.57 Front 7 –2.25 –0.26
5 DB 0 85.10 3,274.05 Top 4 4.11 0.49
6 DL 0 99.74 8,994.40 Front 27 –4.07 0.14
7 OL 0 100.36 1,085.26 Top 0 –2.00 1.01
8e LB 2 102.39 6,837.62 Right 30 –60.01 –1.56
9 OL 0 107.07 2,811.45 Top 9 –20.57 –0.76
10 DB 1 109.88 6,632.77 Top 16 2.70 –0.06
11 DL 2 119.23 7,974.22 Right 12 2.89 0.12
12 LB 0 157.50 1,020.00 Front 14 0.71 0.42
13 WR 0 168.71 15,397.07 Back 13 7.33 0.79
a SOT, Sensory Organization Test; ANAM, Automated Neuropsychological Assessment Metrics battery; DB, defensive back; DL, defensive lineman; LB, linebacker; RB,running back; OL, offensive lineman; WR, wide receiver.b The number of physician-diagnosed concussions sustained in the 5 years before injury.c A higher � Symptom scores value represents an increase in overall symptom severity within the initial 48 hours postinjury compared with the players’ preseason baselinescores.d A positive change score for SOT and ANAM composite scores represents an improved performance within the initial 48 hours postinjury compared with preseason baselinescores. A negative change score indicates a decline in performance relative to preseason baseline measures.e A within-season repeat concussion of the player represented in Patient 2.
ever, serial assessments of postural stability and neuropsy-chological function were significantly depressed during theinitial 2 to 3 days postinjury (Table 1). After this second con-cussion, the player was withheld for an extended period oftime before being released to restricted participation onpostinjury Day 15 and full participation on postinjury Day 16.The repeat concussion raised additional questions, includingwhether or not the delayed symptom recovery and depressedpostural stability and neuropsychological function were aresult of the repeat concussion and potentially incompleterecovery from the first injury (a subacute cumulative effect) orif perhaps the increased impact magnitude was the contribut-ing factor. Research has shown that, on average, collegiate ath-letes typically require between 5 and 7 days to recover afterconcussion (5, 10, 13, 17, 20, 28). Same-season repeat injuriesoften take place within a short window of time, 7 to 10 daysafter the first concussion, and are often associated with slowerrecovery compared with initial concussions (17, 22).
The increased risk of recurrent injury as well as the slowerrecovery often seen after subsequent concussions may beindicative of increased neuronal vulnerability after recurrent
concussive injuries. Animalstudies have described anacute neurometabolic cascadeinvolving accelerated glycoly-sis and increased lactate pro-duction immediately after con-cuss ion (15 , 31 , 34 ) . Theincreased lactate is believed toleave neurons more vulnerableto secondary ischemic injuryand has been considered apossible predisposition torepeat injury. Later steps inthis physiological cascadeinvolve increased intracellularcalcium, mitochondrial dys-function, impaired oxidativemetabolism, decreased glycol-ysis, axonal disconnection,neurotransmitter disturbances,a n d d e l a y e d c e l l d e a t h .Contrary to this proposeddeleterious effect of lactateproduction after concussion, arecent animal study suggeststhat lactate produces a dose-dependent response, possiblyenabling the mitochondria tomeet the increasing metabolicdemands of the brain afterfluid percussion injury in rats(25). Future research shouldattempt to gain a better under-standing of the role lactateplays throughout the acute
neurometabolic cascade after concussion. Decreased cerebralblood flow has been reported to last approximately 10 daysafter concussive injuries in animal models (15), which is consis-tent with the finding of an apparent 7- to 10-day period ofincreased susceptibility to recurrent injury. Additional analysesof cases involving players with recurrent concussive injury willbe necessary to better understand the role that impact magni-tude plays on clinical recovery. However, in viewing this onecase, it appears that both impact magnitude and increased neu-ronal vulnerability from the first concussion are plausibleexplanations for the significant deficits observed in clinicalmeasures.
When considering impact location, players from ourprospective sample were more than 6.5 times more likely tosustain an impact greater than 80 g to the top of the headthan to the sides of the head (32). Nearly half (n � 6) of theconcussions resulted from impacts to the top of the head, sug-gesting that top-of-helmet impacts may result in a higher rateof concussion than other locations. More concussions will benecessary to confirm this trend. Top-of-helmet impactsresulted in some of the larger postural stability deficits
FIGURE 2. Pictorial representation of 13 concussive impacts by location and the specified magnitudes of linear accel-eration in terms of gravity force (g). No concussions resulted from impacts to the left side in our sample.
NEUROSURGERY VOLUME 61 | NUMBER 6 | DECEMBER 2007 | 1249
CONCUSSION RECOVERY AND BIOMECHANICS
1250 | VOLUME 61 | NUMBER 6 | DECEMBER 2007 www.neurosurgery-online.com
GUSKIEWICZ ET AL.
(Patients 1, 3, and 9) found in our study. There are severalpotential explanations for this finding. Although speculative,this could be caused by an acute disruption of the axonalpathways in regions of the brain responsible for controllingpostural stability. Our impact location data (i.e., increasednumber of impacts directed through the top of the head) com-bined with our clinical findings are suggestive of the potentialof a coup-contrecoup mechanism in the superior-inferiordirection. The potential exists in this scenario whereby thecerebellum, positioned between the cerebellar tentorium andforamen magnum, could be indirectly concussed as the forcefrom the impact is directed through the crown of the head.Another plausible explanation is that the brain center respon-sible for central integration of vestibular, visual, and somato-sensory information may be impaired.
As early as 1982, Hugenholtz and Richard (21) proposed thatconcussion resulted from a blow to the head equivalent to a lin-ear acceleration 80 to 90 times the force of gravity for morethan 4 ms. Likewise, Pellman et al. (37) suggested a similarconcussive injury threshold of 70 to 75 g. Although weobserved two concussive injuries in the low-60 g range, themajority of our concussions occurred as a result of impactsabove 80 g. Collectively, these studies might begin to betterdefine a low end concussion threshold of 60 to 80 g.
It has long been thought that acceleration/deceleration forcesimparted to the head lead to a complex series of mechanicaland physiological phenomena. Loading of the force is initiatedeither by static forces or dynamic forces, and most concussionsare believed to be a result of dynamic loading (14, 30). Staticloads tend to result in more serious brain injuries not typicallyseen in sports. A very brief insult is initiated either by a directblow to the head (impact) or by a sudden movement of thehead (impulsive) produced by impacts elsewhere on the body.Thus, biomechanical mechanisms of concussion can be dividedinto two categories: those related to head-contact injuries andthose related to head-movement injuries. Translation, rotation,and angulation result from inertial loading; these are depend-ent on the direction in which the head moves, its speed andduration of movement, and the manner in which it moves (14).This earlier animal research combined with the more recentwork of Viano et al. (44), which concluded that finite elementmodeling showed the largest brain deformations occurred afterthe primary head acceleration, suggests that the insult to thebrain does not necessarily correlate to the initial point of con-tact or surface area of the head that was impacted. Our prelim-inary findings comparing both linear and rotational magnitudeand location of impacts with clinical measures would concurwith these findings.
TABLE 3. Estimates for linear regression modeling, including rotational impact magnitudes and change scores for symptoms, SensoryOrganization Test composite, and Automated Neuropsychological Assessment Metrics battery composite scoresa
Mean change associatedModel Variables with 1000 rad/s2 increase in
StandardP value Correlation
rotational impact magnitudeerror
1 � Symptom scores = 0.45 0.67 0.52 r � 0.20 R2 � 0.04impact magnitude
2 � SOT composite = 0.81 1.35 0.56 r � 0.18 R2 � 0.03impact magnitude
3 � ANAM composite = 0.01 0.05 0.87 r � 0.05 R2 � 0.01impact magnitude
a SOT, Sensory Organization Test; ANAM, Automated Neuropsychological Assessment Metrics battery.
TABLE 2. Estimates for linear regression modeling, including linear impact magnitudes and change scores for symptoms, Sensory OrganizationTest composite, and Automated Neuropsychological Assessment Metrics battery composite scoresa
Mean change associatedModel Variables with 10 g increase in
StandardP value Correlation
linear impact magnitudeerror
1 � Symptom scores � 0.02 0.87 0.98 r � 0.01 R2 � 0.01impact magnitude
2 � SOT composite � 2.17 1.64 0.21 r � 0.37 R2 � 0.14impact magnitude
3 � ANAM composite � 0.07 0.06 0.28 r � 0.33 R2 � 0.11impact magnitude
a SOT, Sensory Organization Test; ANAM, Automated Neuropsychological Assessment Metrics battery.

9. Daniel JC, Olesniewicz MH, Reeves DL, Tam D, Bleiberg J, Thatcher R,Salazar A: Repeated measures of cognitive processing efficiency in adolescentathletes: Implications for monitoring recovery from concussion. Neuro-psychiatry Neuropsychol Behav Neurol 12:167–169, 1999.
10. Delaney JS, Lacroix VJ, Leclerc S, Johnston KM: Concussions among univer-sity football and soccer players. Clin J Sport Med 12:331–338, 2002.
11. Duma SM, Manoogian SJ, Bussone WR, Brolinson PG, Goforth MW,Donnenwerth JJ, Greenwald RM, Chu JJ, Crisco JJ: Analysis of real-time headaccelerations in collegiate football players. Clin J Sport Med 15:3–8, 2005.
12. Echemendia RJ, Cantu RC: Return to play following sports-related mild trau-matic brain injury: The role for neuropsychology. Appl Neuropsychol10:48–55, 2003.
13. Echemendia RJ, Putukian M, Mackin RS, Julian L, Shoss N: Neuro-psychological test performance prior to and following sports-related mildtraumatic brain injury. Clin J Sport Med 11:23–31, 2001.
14. Gennarelli TA: Mechanisms of brain injury. J Emerg Med 11 [Suppl 1]:5–11, 1993.
15. Giza CC, Hovda DA: The neurometabolic cascade of concussion. J Athl Train36:228–235, 2001.
16. Guskiewicz KM, Bruce SL, Cantu RC, Ferrara MS, Kelly JP, McCrea M,Putukian M, Valovich McLeod TC: National Athletic Trainers’ AssociationPosition Statement: Management of sport-related concussion. J Athl Train39:280–297, 2004.
17. Guskiewicz KM, McCrea M, Marshall SW, Cantu RC, Randolph C, Barr W,Onate JA, Kelly JP: Cumulative effects associated with recurrent concussionin collegiate football players: The NCAA Concussion Study. JAMA290:2549–2555, 2003.
18. Guskiewicz KM, Riemann BL, Perrin DH, Nashner LM: Alternativeapproaches to the assessment of mild head injury in athletes. Med Sci SportsExerc 29 [Suppl 7]:S213–S221, 1997.
19. Guskiewicz KM, Ross SE, Marshall SW: Postural stability and neuropsy-chological deficits after concussion in collegiate athletes. J Athl Train36:263–273, 2001.
20. Guskiewicz KM, Weaver NL, Padua DA, Garrett WE Jr: Epidemiology ofconcussion in collegiate and high school football players. Am J Sports Med28:643–650, 2000.
21. Hugenholtz H, Richard MT: Return to athletic competition following concus-sion. Can Med Assoc J 127:827–829, 1982.
22. Iverson GL, Gaetz M, Lovell MR, Collins MW: Cumulative effects of concus-sion in amateur athletes. Brain Inj 18:433–443, 2004.
23. Kelly JP: Traumatic brain injury and concussion in sports. JAMA282:989–991, 1999.
24. Langlois JA, Rutland-Brown W, Wald MM: The epidemiology and impactof traumatic brain injury: A brief overview. J Head Trauma Rehabil21:375–378, 2006.
25. Levasseur JE, Alessandri B, Reinert M, Clausen T, Zhou Z, Altememi N,Bullock MR: Lactate, not glucose, up-regulates mitochondrial oxygen con-sumption both in sham and lateral fluid percussed rat brains. Neurosurgery59:1122–1131, 2006.
26. Lovell MR, Collins MW: Neuropsychological assessment of the college foot-ball player. J Head Trauma Rehabil 13:9–26, 1998.
27. McCaffrey MA, Mihalik JP, Crowell DH, Shields EW, Guskiewicz KM:Measurement of head impacts in Division I football players: Clinical meas-ures of concussion after high- and low-magnitude impacts. Neurosurgery61:1236–1243, 2007.
28. McCrea M, Guskiewicz KM, Marshall SW, Barr W, Randolph C, Cantu RC,Onate JA, Yang J, Kelly JP: Acute effects and recovery time following concus-sion in collegiate football players: The NCAA Concussion Study. JAMA290:2556–2563, 2003.
29. McCrory P, Johnston K, Meeuwisse W, Aubry M, Cantu R, Dvorak J, Graf-Baumann T, Kelly J, Lovell M, Schamasch P; International Symposium onConcussion in Sport: Summary and agreement statement of the 2ndInternational Conference on Concussion in Sport, Prague 2004. Clin J SportMed 15:48–58, 2005.
30. McIntosh T, Vink R: Biomechanical and pathophysiologic mechanisms inexperimental mild to moderate traumatic brain injury, in Hoff J, Anderson T,Cole T (eds): Mild to Moderate Head Injury. Boston, Blackwell ScientificPublications, 1989, pp 35–45.
CONCLUSION
The uniqueness of our study is that it combines impact bio-mechanics captured in real-time with clinical measures of symp-tom severity, neurocognitive function, and postural stabilitycaptured within the acute period after concussive injury. In asmall sample of concussed athletes, our findings underscorethat concussions can occur at varying magnitudes and loca-tions, and that acute concussion symptoms are unrelated toboth linear or rotational magnitude and impact location. Thefindings further suggest that the threshold for injury may belower than originally predicted. To the contrary, the argumentcould be made that the threshold for concussive injury could behigher than previously predicted. This notion is supported bythe findings of our companion studies in which impacts greaterthan 90 g, in the absence of self-reported concussion symptoms,did not result in a diagnosed concussive episode (27) and inwhich fewer than a half percent (� 0.35%) of all impacts greaterthan 80 g in our 2-year study resulted in a diagnosed concussion(32). Because of the varying magnitudes and locations ofimpacts resulting in concussion, as well as other factors such asthe number of sustained subconcussive impacts and number ofprevious concussions, it may be difficult to establish a thresholdfor concussive injury that can be applied to all football players.
Finally, many sports medicine clinicians have anecdotallysuggested that acceleration/deceleration magnitudes, partic-ularly rotational acceleration, play a role in predicting injuryseverity. Our preliminary findings suggest that this may notbe the case and calls for more research to be conducted toinvestigate how linear and rotational acceleration relate tomeasures of symptom severity, neurocognitive function, andpostural stability in larger sample sizes across the entirerecovery period.
REFERENCES1. Anonymous: Concussion (mild traumatic brain injury) and the team physi-
cian: A consensus statement. Med Sci Sports Exerc 38:395–399, 2006.2. Anonymous: Practice parameter: The management of concussion in sports
(summary statement). Report of the Quality Standards Subcommittee.Neurology 48:581–585, 1997.
3. Aubry M, Cantu R, Dvorak J, Graf-Baumann T, Johnston K, Kelly J, Lovell M,McCrory P, Meeuwisse W, Schamasch P; Concussion in Sport Group:Summary and agreement statement of the First International Conference onConcussion in Sport, Vienna 2001. Recommendations for the improvement ofsafety and health of athletes who may suffer concussive injuries. Br J SportsMed 36:6–10, 2002.
4. Bailes JE, Hudson V: Classification of sport-related head trauma: A spectrumof mild to severe injury. J Athl Train 36:236–243, 2001.
5. Bleiberg J, Cernich AN, Cameron K, Sun W, Peck K, Ecklund PJ, Reeves D,Uhorchak J, Sparling MB, Warden DL: Duration of cognitive impairmentafter sports concussion. Neurosurgery 54:1073–1080, 2004.
6. Bleiberg J, Garmoe WS, Halpern EL, Reeves DL, Nadler JD: Consistency ofwithin-day and across-day performance after mild brain injury. Neuro-psychiatry Neuropsychol Behav Neurol 10:247–253, 1997.
7. Brown CN, Guskiewicz KM, Bleiberg J: Athlete characteristics and outcomescores for computerized neuropsychological assessment: A preliminary analy-sis. J Athl Train 42:515–523, 2007.
8. Cantu RC: Posttraumatic retrograde and anterograde amnesia: Patho-physiology and implications in grading and safe return to play. J Athl Train36:244–248, 2001.
NEUROSURGERY VOLUME 61 | NUMBER 6 | DECEMBER 2007 | 1251
CONCUSSION RECOVERY AND BIOMECHANICS

1252 | VOLUME 61 | NUMBER 6 | DECEMBER 2007 www.neurosurgery-online.com
GUSKIEWICZ ET AL.
31. Meyer JS, Kondo A, Nomura F, Sakamoto K, Teraura T: Cerebral hemody-namics and metabolism following experimental head injury. J Neurosurg32:304–319, 1970.
32. Mihalik JP, Bell DR, Marshall SW, Guskiewicz KM: Measurement of headimpacts in Division I football players: An investigation of positional andevent-type differences. Neurosurgery 61:1229–1235, 2007.
33. NCAA Injury Surveillance System (ISS): http://www.ncaa.org/iss. Accessed6/10/07.
34. Nilsson B, Nordstrom CH: Rate of cerebral energy consumption in concussivehead injury in the rat. J Neurosurg 47:274–281, 1977.
35. Padgaonkar AJ, Krieger KW, King AI: Measurement of angular accelerationof a rigid body using linear accelerometers. J Appl Mech 42:552–556, 1975.
36. Pellman EJ, Viano DC, Tucker AM, Casson IR; Committee on MildTraumatic Brain Injury, National Football League: Concussion in profes-sional football: Location and direction of helmet impacts-Part 2.Neurosurgery 53:1328–1341, 2003.
37. Pellman EJ, Viano DC, Tucker AM, Casson IR, Waeckerle JF: Concussion inprofessional football: Reconstruction of game impacts and injuries.Neurosurgery 53:799–814, 2003.
38. Peterson CL, Ferrara MS, Mrazik M, Piland S, Elliott R: Evaluation of neu-ropsychological domain scores and postural stability following cerebral con-cussion in sports. Clin J Sport Med 13:230–237, 2003.
39. Powell JW, Barber-Foss KD: Traumatic brain injury in high school athletes.JAMA 282:958–963, 1999.
40. Riemann BL, Guskiewicz KM: Effects of mild head injury on postural stabil-ity as measured through clinical balance testing. J Athl Train 35:19–25, 2000.
41. Riemann BL, Guskiewicz KM, Shields EW: Relationship between clinical andforceplate measures of postural stability. J Sport Rehabil 8:71–82, 1999.
42. Thurman DJ, Alverson C, Browne D, Dunn KA, Guerrero J, Johnson R,Johnson V, Langlois J, Pikey D, Sniezek JE, Toal S: Traumatic Brain Injury in theUnited States: A Report to Congress. Atlanta, National Center for InjuryPrevention and Control, Centers for Disease Control and Prevention, USDepartment of Health and Human Services, 1999.
43. Thurman DJ, Branche CM, Sniezek JE: The epidemiology of sports-relatedtraumatic brain injuries in the United States: Recent developments. J HeadTrauma Rehabil 13:1–8, 1998.
44. Viano DC, Casson IR, Pellman EJ, Zhang L, King AI, Yang KH: Concussion inprofessional football: Brain responses by finite element analysis. Part 9.Neurosurgery 57:891–916, 2005.
45. Zhu W: Making bootstrap statistical inferences: A tutorial. Res Q Exerc Sport68:44–55, 1997.
AcknowledgmentsWe thank Richard Greenwald, Ph.D., and his colleagues at Simbex, Inc.,
Lebanon, NH, for their assistance in the processing and interpretation of datacollected by the Head Impact Telemetry System. This study was supported inpart by a grant from the Center for Disease Control and Prevention to theUniversity of North Carolina at Chapel Hill Injury Prevention Research Center,number 5-R49-CE000196.
COMMENTS
I appreciate how this study was designed because thorough baselineand postinjury testing were performed. We use very similar (if not the
same) test batteries at the University of Southern California. The labo-ratory was brought to the field of play in practice and games to deter-mine impacts using the Head Impact Telemetry (HIT) system. Thestudy’s main limitation was that the sample size was small and limitedto one college football program. Whether the results of this study rep-resent high school, collegiate, or professional football players remainsto be seen. Additional study is needed. Publishing this study allowsother researchers to gain a clearer understanding of this complicateddiagnosis. Because the conclusions of this study did not show a rela-tionship between impact magnitude and symptom severity, posturalstability, or neuropsychological function, it further supports how diffi-
cult and complex sport-related concussions are to identify and effec-tively manage. This study shows that even if you measure impactseverity sustained during practice and games, you still must rely onclinical judgment and experience to determine whether a player shouldreturn to competition or whether an injury even occurred.
Russ RomanoAthletic TrainerLos Angeles, California
Guskiewicz et al. gathered data from more than 100,000 headimpacts sustained by 88 college football players over a 3-year
period. They conclude that clinical measures of concussion are unre-lated to measured magnitudes of impact and to locations of impact onthe head. These conclusions run counter to the conventional wisdomabout impact thresholds for concussion and are therefore interesting.However, the very small number of players with concussions is a majorlimitation of this work that can be addressed only by ongoing collectionof carefully documented cases.
Alex B. ValadkaHouston, Texas
I agree with the authors that every concussed athlete needs to betreated on an individual case-by-case basis. I am glad that
Guskiewicz et al. reiterate this important point, as it bolsters the argu-ment that standardized concussion management guidelines are not asubstitute for the clinical judgment and medical expertise of the treat-ing physician in the evaluation and treatment of the concussed athlete.This article, however, has a number of serious flaws. The small samplesize of 13 concussions is a major limitation that renders the resultsextremely preliminary and the conclusions drawn from them highlyspeculative. These results are not so earth-shattering or revolutionaryas to justify the rush to publish. I believe that science would have beenbetter served if the authors had patiently waited until they had col-lected a larger number of cases before presenting their (more conclusiveand definitive) results. I also cannot understand how an article aboutclinical outcomes does not include the results of neurological historiesand clinical examinations of the concussed athletes. Fancy balance test-ing, neuropsychological testing, and filling out a symptom question-naire are not substitutes for clinical history and examination. Based onthis article, I do not see any indication that the HITS system differenti-ates between the striking player and the struck player in a helmet-to-helmet collision. Because the struck player is far more likely than thestriking player to sustain a clinical concussion from the same collision,this implies that a large number of the HITS-detected impacts (regard-less of magnitude or direction) will never be associated with clinicalconcussion, thereby seriously skewing the results of studies like thisone. It is also curious that there were no concussion-producing impactsto the left side of the helmet in any of these 13 cases. I presume that thisis some type of statistical aberration, but it does raise questions aboutthe accuracy and reliability of the HITS technology.
Ira R. CassonNeurologistForest Hills, New York
This is a unique and excellent study that sheds important light on thesubject of concussion and on sports injuries in general.
Although the findings are counterintuitive and change our beliefstructure with respect to concussion, this is extremely important. Thelack of good correlation between the force of impact and the clinicalseverity of the concussion argues that innate human head/brain differ-

ences are important. This in turn supports the contention that someathletes may be “concussion prone,” as data from this same group ofauthors and the sports news media have previously shown. The studyis well performed in a large cohort of football players using state-of-the-art modern telemetric physics: biomechanical techniques in the realworld! The data are, therefore, unique.
Clearly, the implication is that a similar study needs to be done in theAmerican Football League or National Football League to follow thisimportant lead and determine whether magnitudes of concussion arehigher or in some way different in more-experienced players who areprobably better athletes and who are larger. Moreover, the exquisitefilming of modern games with slow-motion replays will allow closercorrelation between the forces, biomechanics, and head motions.
Helmet design can surely be much improved by these studies, as hashappened with race car drivers’ helmets using these same accelerom-eter studies.
Ross BullockMiami, Florida
Sport-related concussion is a common problem with potentially long-term neurological consequences, particularly for those athletes who
suffer repeat injury. Our understanding of the mechanistic factors thatcontribute to clinical outcomes has been hampered by lack of reliableinformation about the biophysics of impacts sustained by concussedathletes. Guskiewicz et al. have begun to address this issue with theirinvestigation of head impact and concussion in collegiate football play-ers. The authors followed 88 athletes using an innovative helmet-embedded accelerometer device that allowed real-time measurementsof head-impact location and linear and rotational accelerations.Athletes were assessed at baseline and after concussion using tests ofsymptom severity, neuropsychological performance, and postural sta-bility. During the study period, over 100,000 impacts and a total of 13concussions were documented.
Analyses that focused on the 13 episodes of concussion did not revealassociations between magnitude of impact and concussion syndromes.The finding that impact characteristics did not predict clinical severity in
this study should be interpreted with caution. The small number ofobserved concussions limited the power to detect an association if onetruly exists. Additional potentially contributory factors, such as historyof prior head injury or concussion and characteristics of subconcussiveimpacts preceding the actual injury, were not assessed. Thus, as theauthors note, these results should be considered preliminary, and addi-tional study is warranted before management conclusions can be drawn.
Despite these limitations, this article makes an important contribu-tion to the field of sport-related concussion. The strength of this worklies in its demonstration that detailed data about head-impact physicscan be successfully gathered in the course of athletic competition. Theexpanded use of this investigative approach will permit larger-scalestudies comparing impacts that result in concussion with those that donot. By including additional patient and impact variables, and lookingat both acute and chronic outcomes, future work with this techniqueshould shed additional light on the predictors of injury and its sever-ity. Guskiewicz et al. have thus introduced a tool that ultimately mayprove valuable for both prevention and management of sport-relatedconcussion. Whether continuous monitoring of acceleration-forceparameters is practical remains to be seen.
Todd L. HarshbargerJulian E. BailesMorgantown, West Virginia
This article is part of three articles designed to evaluate variousaspects of head collisions using the HITS system. This represents a
new and exciting area of research, and the authors should be com-mended for their efforts. However, although very interesting, theresults are limited and are based on inclusion of a very small samplesize (13 subjects). This makes any real statistical exploration of the datadifficult, and the article must be regarded as 13 case studies. Therefore,at best, the study provided food for thought.
Mark R. LovellNeuropsychologistPittsburgh, Pennsylvania
CONCUSSION RECOVERY AND BIOMECHANICS