mds 3.0 updates 2018 - arhealthcare.com mds training 2018 .pdf · dressing, using the toilet, or...
TRANSCRIPT

MDS 3.0 Updates 2018
Cassie Crafton R.N., CDP, RAC-CT

Objectives
• Understand new MDS 3.0 items in Sections GG, I, J, M, N and
O that will be effective October 1st, 2018
• Know which MDS 3.0 items that will be removed and language
changes
• Understand and interpret Quality Measures, Quality Reporting
Program (QRP), and Value-based Purchasing (VBP)
• Review Five Star Reports and Nursing Home Compare
Clarifications with Resident Interviews
Timing of Interviews• Section C (BIMS)- to be conducted preferably on the ARD or
the day before• Section D (PHQ-9)- to be conducted preferably on the ARD or
the day before• Section F (Activities/Preferences)- during the 7 day look back
period• Section J (Pain)- to be conducted anytime during the 5 day
lookback period preferably on the ARD or the day before
Clarifications with Resident Interviews• Staff interview should not be completed in place of resident
interview IF the resident interview could have been completed
• B0700 should NOT be coded as “Rarely/Never Understood” if any of the resident interviews were completed
PPS Changes
• Section GG changes
• Admission and Discharge Assessments
• Language Changes

PPS: Admission Assessment
• Admission: The 5 - Day PPS assessment (A0310B =
01) is the first Medicare - required assessment to be
completed when the resident is admitted for a SNF
Part A stay
• This functional assessment must be completed
within the first 3 days (3 calendar days) of the
Medicare Part A stay, starting with the date in
A2400B. Start of Most Recent Medicare Stay, and
the following 2 days, ending at 11:59 p.m. on Day 3
PPS: Discharge Assessment
• The Part A PPS Discharge Assessment is required to be
completed when the resident’s Medicare Part A Stay ends (as
documented in A2400C. End of Most Recent Medicare Stay),
either:
– As a standalone assessment when the resident’s Medicare Part A
stay ends, but the resident remains in the facility, or
– May be combined with an Omnibus Budget Reconciliation Act of
1987 (OBRA) Discharge if the Medicare Part A stay ends on the
day of, or 1 day before the resident’s Discharge Date (A2000)

Coding Tips• Admission Performance and Discharge Goals are coded on
every Admission Assessment (Start of Part A PPS Stay) regardless of length of stay and planned or unplanned discharge
• If the resident has an incomplete stay: – Complete admission performance and goals – Discharge self-care and mobility performance items are not
required

Section GG- Intent• Functional status is assessed based on the need for
assistance when performing self - care and mobility activities
• Residents in SNFs have self - care and mobility limitations and are at risk for further functional decline and complications because of limited mobility

New Items Section GG• GG 0100 Prior Functioning: Everyday Activities• Intent: To identify resident’s functional status prior to current
illness
Section GG Prior Functioning• Self Care: Code the resident’s need for assistance with bathing,
dressing, using the toilet, or eating prior to the current illness, exacerbation, or injury
• Indoor Mobility (Ambulation): Code the resident’s need for assistance with walking from room to room (with or without a device such as cane, crutch, or walker) prior to the current illness, exacerbation, or injury
• Stairs: Code the resident’s need for assistance with internal or external stairs (with or without a device such as cane, crutch, or walker) prior to the current illness, exacerbation, or injury
• Functional Cognition: Code the resident’s need for assistance with planning regular tasks, such as shopping or remembering to take medication prior to the current illness, exacerbation, or injury
Section GG: Prior Functioning• Coding Instructions:
– Code 3, Independent- no assistance, with/without assistive devices
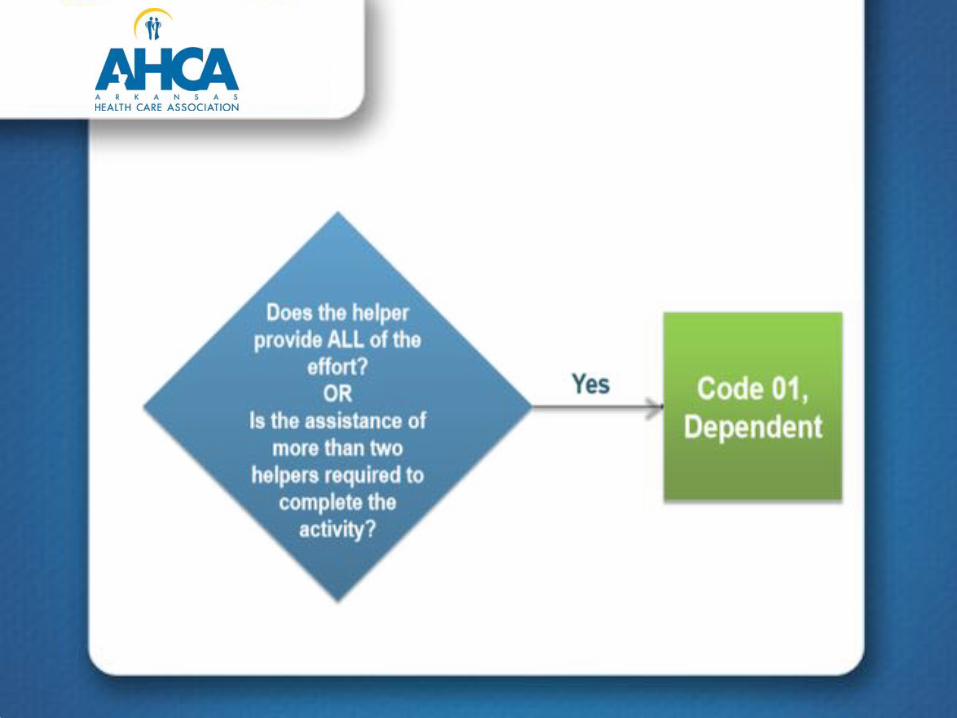
– Code 2, Needed Some Help- needed partial assistance– Code 1, Dependent- helper completed activity; includes
needing 2 person assist– Code 8, Unknown– Code 9, Not Applicable- were not applicable to the
resident’s prior to current illness
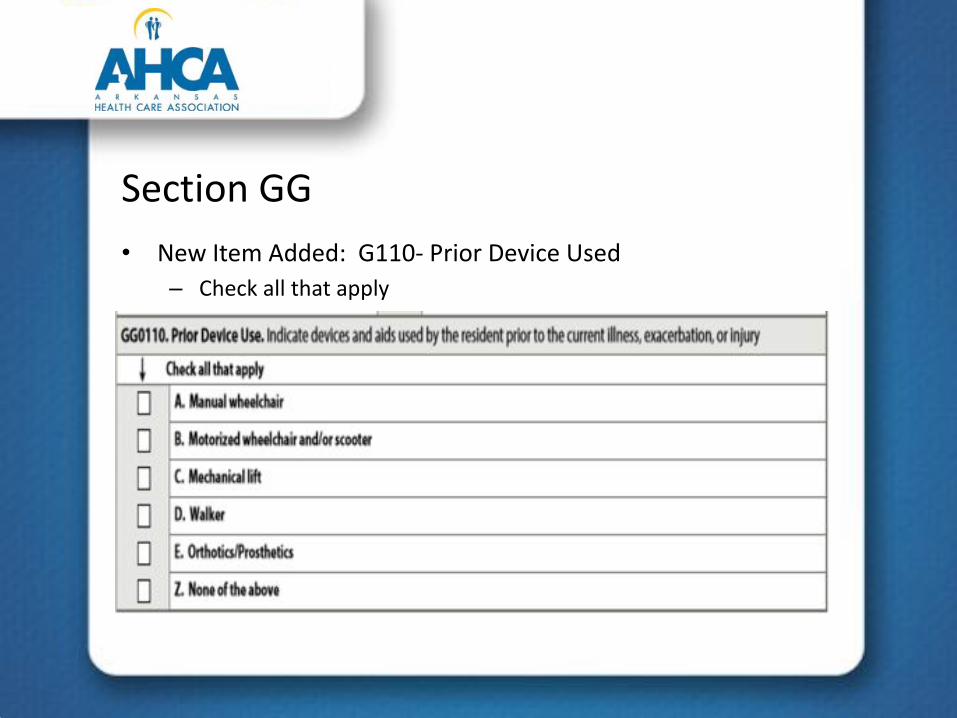
Section GG• New Item Added: G110- Prior Device Used
– Check all that apply

GG0110 Prior Device Used• Clarifications
– Walker: any type of walker (pickup walker, hem-walker, rolling walkers, platform walkers.
– Mechanical Lift: sit-to-stand, stand assist, full body lifts (e.g., Hoyer)

Section GG• New items GG0130 Self-Care 4 new items

Section GG: New items GG0170 • Mobility 7 new items
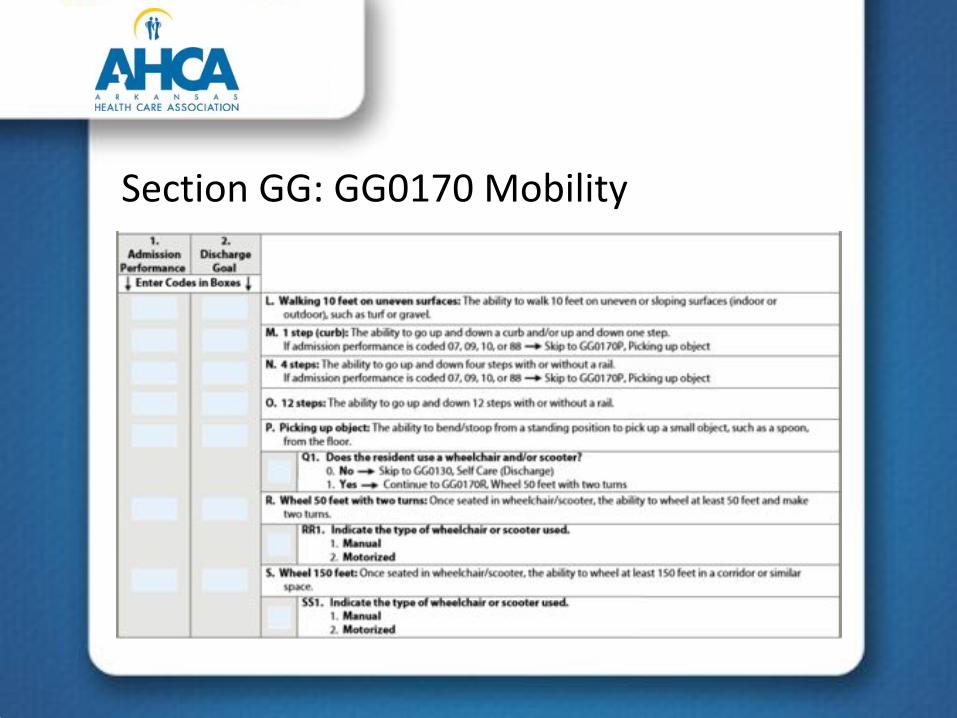
Section GG: GG0170 Mobility
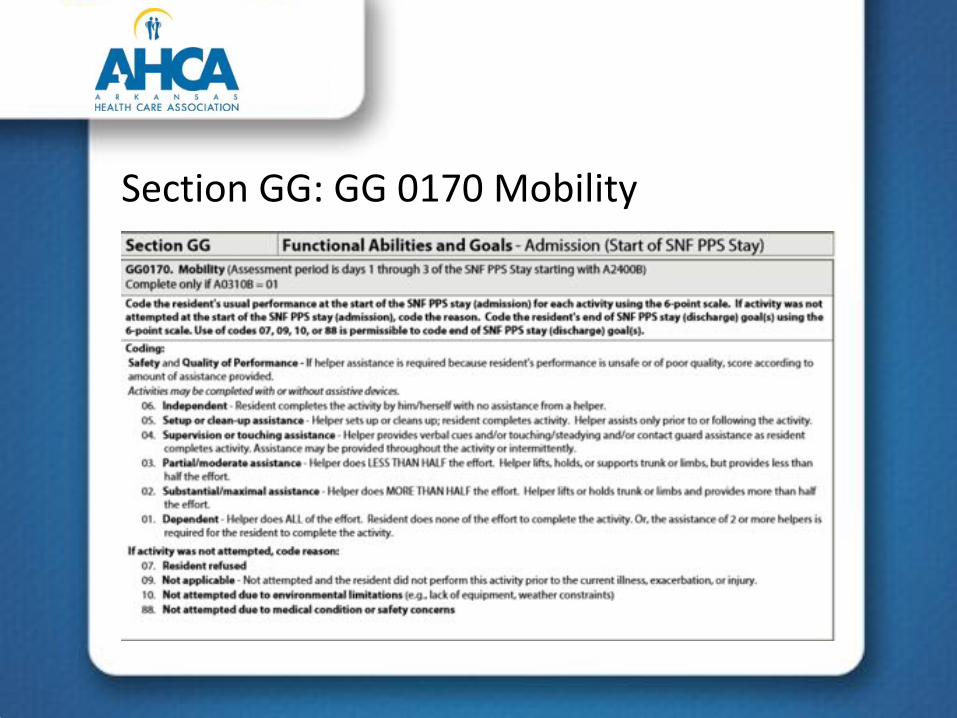
Section GG: GG 0170 Mobility

Section GG• Coding of GG0130 and GG0170• 4 “Not attempted” codes items• 10- Not attempted due to environmental limitations
( NEW)

Section GG: Coding Instructions
• Admission Performance- code based on the first 3 days
of Medicare Part A stay
• Discharge Performance- code based on last 3 days of
Medicare Part A stay
• Coding is based on “usual performance” will require
clinical judgement
• If activity occurs multiple times (e.g., eating, toileting,
dressing, bed mobility activities, bed/chair transfers, do
not code most dependent, do not code most
independent
• Some items may only be assessed once, code that status

Changes to Section GG• Coding and item definitions clarified and aligned:
– “Contact guard” added to definition of code 04, Supervision or touching assistance
– Eating (Item GG0130A) definition clarified to include the ability to bring food and liquid to the mouth and swallow food once the meal is placed before the resident
– Oral hygiene (Item GG0130B) revised to: …The ability to insert and remove dentures into and from the mouth and manage denture soaking and rinsing with use of equipment
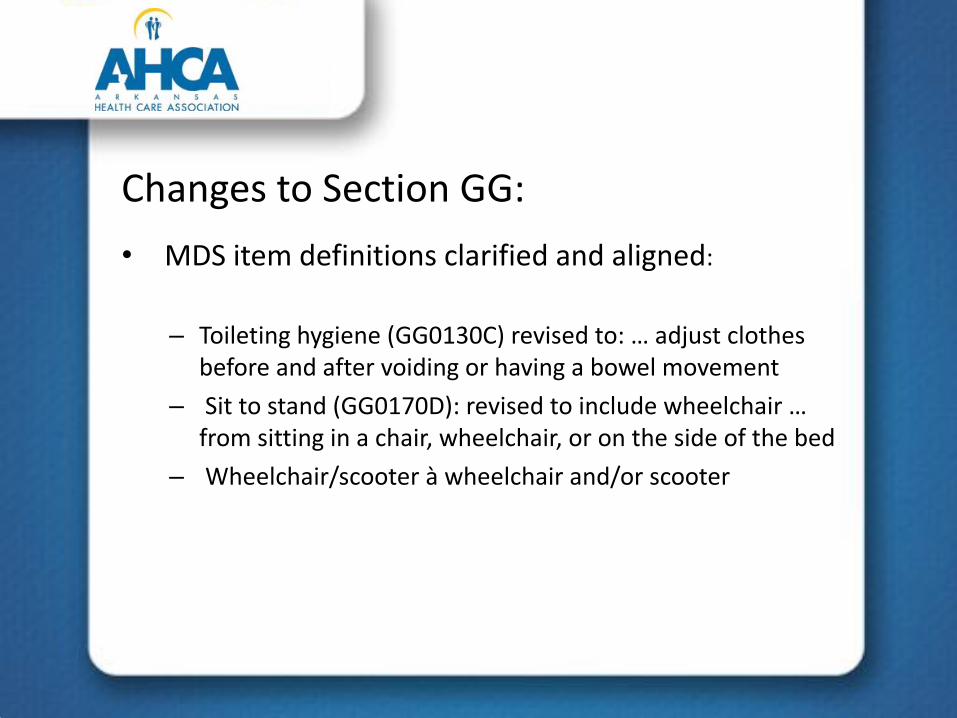
Changes to Section GG:• MDS item definitions clarified and aligned:
– Toileting hygiene (GG0130C) revised to: … adjust clothes before and after voiding or having a bowel movement
– Sit to stand (GG0170D): revised to include wheelchair … from sitting in a chair, wheelchair, or on the side of the bed
– Wheelchair/scooter à wheelchair and/or scooter

Steps for Assessment Section GG• Assess the resident’s self care and mobility performance
based on direct observation; the resident’s self-report; and reports from clinicians, care staff, or family reports, documented in the resident’s medical record during the 3-day assessment period
• Residents should be allowed to perform activities as independently as possible, as long as they are safe
• If helper assistance is required because a resident’s performance is unsafe or of poor quality, score according to amount of assistance provided
• For Section GG, a “helper” is defined as facility staff who are direct employees and facility - contracted employees (e.g., rehabilitation staff, nursing agency staff)

Steps for Assessment Section GG• Activities may be completed with or without assistive
device(s). Use of assistive device(s) to complete an activity should not affect coding of the activity.
• If the resident’s self-care and mobility performance varies during the assessment period, record the resident’s usual ability to perform each activity.
-Do not record the resident’s most independent performance-Do not record the resident’s most dependent performance
• Refer to facility, Federal, and State policies and procedures to determine which SNF staff members may complete an assessment. Resident assessments are to be done in compliance with facility, Federal, and State requirements.




Activity Not Attempted Codes

Coding scenario

Answer:• Code 02: Substantial or Maximal Assist
• CMS states that when coding bladder and bowel take the lower score. Since the helper had to provide more than HALF of the task then the correct coding would be 02.
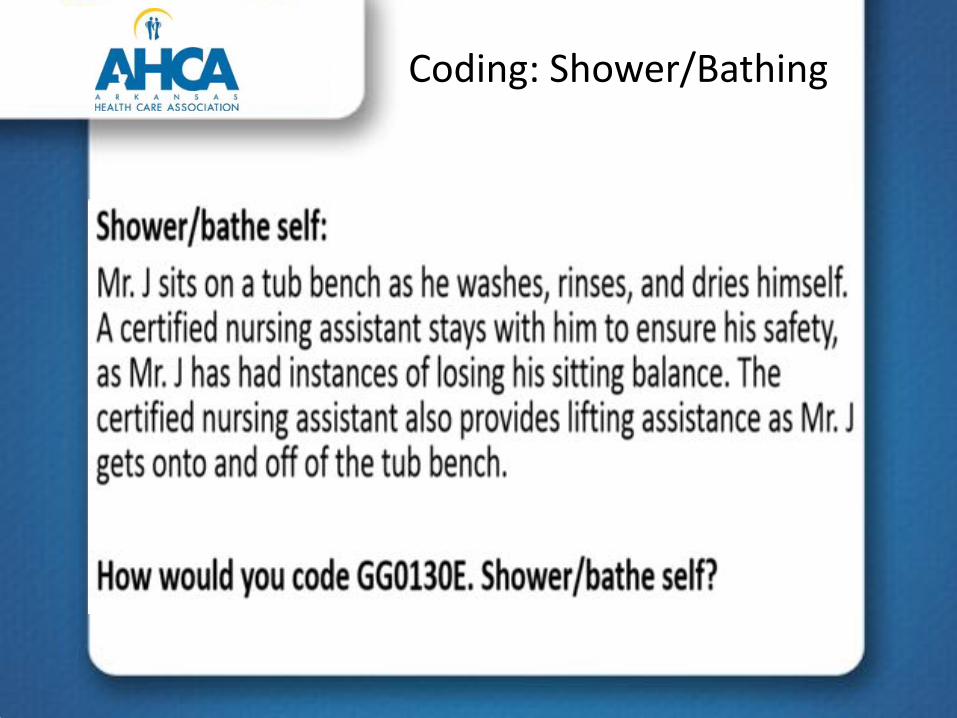
Coding: Shower/Bathing

ANSWER• CODE: 04 Supervision or touching assistance
• CMS states that transfers on or off tub bench is NOT part of the Shower/bathing assessment
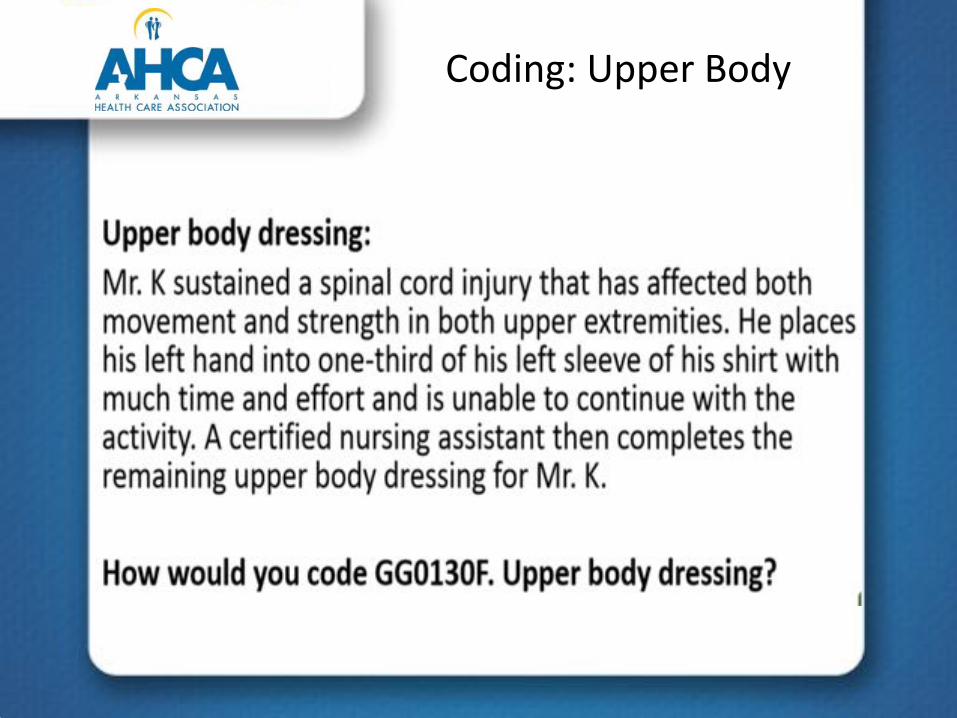
Coding: Upper Body

Answer:• Code: 02 Substantial or maximal assist
• CMS states that Helper is doing more than HALF of the effort

Lower Body Dressing

Answer:• Code 03 Partial/Moderate Assistance
• CMS states prothesis is considered to be part of clothing. Helper is completing less than HALF of the effort

Footwear

Answer:• Code 04: Supervision or Touching Assistance
• CMS states due to occasional loss of balance a helper provides touching assistance while bending over.
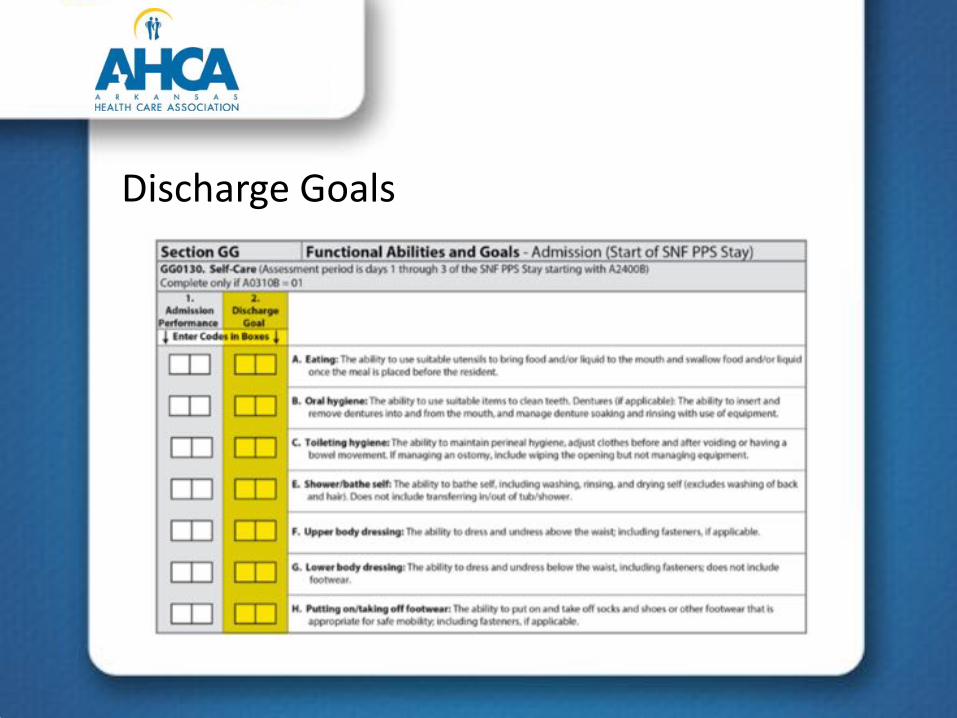
Discharge Goals
Discharge Coding Tips• Use the six-point scale or ‘activity was not attempted” codes
to code the resident’s Discharge Goal(s). Use of codes 07, 09, 10, or 88 is permissible to code discharge goal(s).
• For the SNF QRP, a minimum of one self-care or mobility goal must be coded. However, facilities may choose to complete more than one self-care or mobility discharge goal.
• Use of a dash ( – ) is permissible for any remaining self - care or mobility goals that were not coded.
• Using the dash in this allowed instance after the coding of at least one goal does not affect Annual Payment Update (APU) determination.

Discharge Coding Tips• Licensed qualified clinicians can establish a resident’s
Discharge Goal(s) at the time of admission based on:– Resident’s prior medical condition(s)
• Prior and current self care and mobility status• Discussions with resident and family concerning discharge goals
– Professional’s standard of practice – Expected treatments – Resident motivation to improve – Anticipated length of stay – Resident’s planned discharge setting/home
• Goals should established as part of the resident’s care plan

Discharge: Roll
Answer:• Code: 01 Dependent
• Resident required Two Helpers to compete task
Car Transfers

Answer:• Code 04 Supervision or Touching Assistance
• Guidance states that opening and closing doors and seatbelts are not a part of assessment.

Section GG: Summary
5-Day Assessment Column 1• All items in column 1
must be completed• Base coding on first 3
days of Med A stay• No dashes• Choose any number
from the 1-6 scale OR• 1 of the 4 “not
attempted” codes
5-day Assessment Column 2• Must have at least one
discharge goal completed (may be in GG0130 or GG0170)
• May use 1 of the 4 “not attempted” as goals
• Dash goals not completed
• Goals may indicate an improvement, maintain, or possible decline
Section GG: Summary
SNF PPS Discharge Assessment• All items in Column 3
must be completed• Base coding on last 3
days of Med A stay• No dashes• Chose any number
from the 1-6 scale or • 1 of the 4 “not
attempted codes
Use of Dashes• Section GG is the
number 1 reason for 2% penalty
• Confusion on coding rules
• Use of dashes• Only items used for
QRP QM calculation are subject to the 2% penalty if dashed

Section I: New item I0020• Resident’s primary medical condition• Provides check boxes for 14 different items

Section I: New item I0020• Select the condition that represents the primary
condition that resulted in resident’s admission to the nursing facility
• If number 14 selected, enter an appropriate ICD-10-CM code in I0020
• If any condition 1-13 selected, then item I0020 is left blank
• Includes the primary medical condition in Section I, Active Diagnoses

Section I• Code 01, Stroke, if the resident’s primary medical condition
category is due to stroke. Example include ischemic stroke, subarachnoid hemorrhage, cerebral vascular accident, and other cerebrovascular disease
• Code 02, Non-Traumatic Brain Dysfunction, if the resident’s primary medical condition category is non-traumatic brain dysfunction. Examples include Alzheimer’s disease, dementia with or without behavioral disturbance, malignant neoplasm of brain, and anoxic brain damage
• Code 03, Traumatic Brain Dysfunction, if the resident’s primary medical condition category is traumatic brain dysfunction. Examples include traumatic brain injury, severe concussion, and cerebral laceration and contusion

Section I• Code 04, Non-Traumatic Spinal Cord Dysfunction, if the
resident’s primary medical condition category is non-traumatic spinal cord injury. Examples include spondylosis with myelopathy, transverse myelitis, spinal cord lesion due to spinal stenosis, and spinal cord lesion due to dissection of aorta
• Code 05, Traumatic Spinal Cord Dysfunction, if the resident’s primary medical condition category is due to traumatic spinal cord dysfunction. Examples include paraplegia and quadriplegia following trauma
• Code 06, Progressive Neurological Conditions, if the resident’s primary medical condition category is a progressive neurological condition. Examples include multiple sclerosis and Parkinson’s disease

Section I• Code 07, Other Neurological Conditions, if the resident’s
primary medical condition category is other neurological condition. Examples include cerebral palsy, polyneuropathy, and myasthenia gravis
• Code 08, Amputation, if the resident’s primary medical condition category is an amputation. An example is acquired absence of limb
• Code 09, Hip and Knee Replacement, if the resident’s primary medical condition is due to a hip or knee replacement. An example is total knee replacement. If hip replacement is secondary to hip fracture, code as fracture.

Section I• Code 10, Fractures and Other Multiple Trauma, if the
resident’s primary medical condition category is fractures and other multiple trauma. Examples include hip fracture, pelvic fracture, and fracture of tibia and fibula
• Code 11, Other Orthopedic Conditions, if the resident’s primary medical condition category is other orthopedic condition. An example is unspecified disorders of joint
• Code 12, Debility, Cardiorespiratory Conditions, if resident’s primary medical condition category is debility or a cardiorespiratory condition. Examples include COPD, asthma, and other malaise and fatigue

Section I• Code 13, Medically Complex Conditions, if the resident’s
primary medical condition category is a medically complex condition. Examples include diabetes, pneumonia, chronic kidney disease, open wounds, pressure ulcer/injury, infection, and disorders of fluid, electrolyte, and acid-base balance
• Code 14, Other Medical Condition, if the resident’s primary medical condition category is not one of the listed categories. Enter the ICD-10 code, including the decimal, in I0020A. If item I0020 is coded 1-13, do not complete I0020A

Section J: New item J2000 Prior Surgery
• Indicate if the resident has had a major surgery in the 100 days prior to admission
Section J: J2000• Examples
– Admitted to SNF after hip replacement surgery 5 days prior. Code 1, Yes, meets criteria
– Cyst removal in outpatient One month prior to admission. Code 0, No, does not meet “major surgery criteria
– Gall bladder surgery performed 6 months prior to admission. Code 0, No, does not meet criteria due to greater than 100 days ago

Section K• Change in Coding Instructions related to K0510 and K0710• CMS no longer requires completion of Column 1 for K0510C or
K0510D. Some states may still require. Arkansas will not

Section K• Change in coding instructions to K0710
– CMS no longer requires completion of Column 1 K0710 A and B. Some states may still require. (Arkansas does not)

Section M: Intent• The items in this section document the risk,
presence, appearance, and change of pressure ulcers/injuries. This section also notes other skin ulcers, wounds, or lesions, and documents some treatment categories related to skin injury or avoiding injury.
• It is important to recognize and evaluate each resident’s risk factors and to identify and evaluate all areas at risk of constant pressure.
Section M: Intent• A complete assessment of skin is essential to an
effective pressure ulcer prevention and skin treatment program. Be certain to include in the assessment process a holistic approach.
• It is imperative to determine the etiology of all wounds and lesions, as this will determine and direct the proper treatment and management of the wound.
Section M: Intent • CMS adheres to the following guidelines:
– Stage 1 pressure injuries and deep tissue injuries (DTIs) are termed “pressure injuries” because they are closed wounds
– Stage 2, 3, or 4 pressure ulcers, or unstageable ulcers due to slough or eschar, are termed “pressure ulcers” because they are usually open wounds
– Unstageable ulcers/injuries due to non - removable dressing/device are termed “pressure ulcers/injuries” because they may be open or closed wounds

Section M: Definitions• New: The term “device” was added to items: M0300E–
M0300E2
Section M: Definitions• New: – Removed the term “suspected deep tissue injury
in evolution” and replaced with “deep tissue injury” to items M0300G and M0300G1
Section M: Definitions
• Pressure Ulcer/Injury Risk Factor – Examples of risk factors include immobility and decreased
functional ability; co-morbid conditions such as end-stage renal disease, thyroid disease, or diabetes; drugs such as steroids; impaired diffuse or localized blood flow; resident refusal of care and treatment; cognitive impairment; exposure of skin to urinary and fecal incontinence; microclimate, malnutrition, and hydration deficits; and a healed ulcer

Section M: Definitions• Pressure Ulcer/Injury– A pressure ulcer/injury is localized injury to the
skin and/or underlying tissue, usually over a bony prominence, as a result of intense and/or prolonged pressure, or pressure in combination with shear. The pressure ulcer/injury can present as intact skin or an open ulcer and may be painful.

Section M: Deletions• Items Retiring October 1, 2018
– M0300B3 Date of Oldest Stage 2 Pressure Ulcer – M0610 Dimensions of Unhealed Stage 3 or 4 Pressure
Ulcers or Eschar – M0700 Most Severe Tissue Type for Any Pressure Ulcer – M0800 Worsening in Pressure Ulcer Since Prior
Assessment (Omnibus Budget Reconciliation Act (OBRA) or Scheduled PPS) or Last Admission/Entry or Reentry
– M0900 Healed Pressure Ulcers

Section M: Coding• Steps for completing M0300A–G1. Determine Deepest Anatomical Stage2. Identify Unstageable Pressure Ulcers/Injuries 3. Determine “Present on Admission”
On the Admission Assessment, “on admission” means as close to the actual time of admission as possible
On each assessment determine the number of pressure ulcers/injuries present and determine the number of these that were present on admission Manual instruction 9 under Step 3: If a pressure ulcer was numerically staged, then became unstageable, and is subsequently debrided sufficiently to be numerically staged, compare its numerical stage before and after it was unstageable. If the numerical stage has increased, code this pressure ulcer as not present on admission.
Coding Scenario 1• A resident develops a Stage 2 pressure ulcer while
at the nursing facility. The resident is hospitalized due to pneumonia for 8 days and returns with a Stage 3 pressure ulcer in the same location. How would you code M0300C1 and M0300C2 on the 5Day PPS assessment?

Answer:
• Stage 3
• Present on admission
Coding Scenario 2• A resident is admitted to a nursing facility with a short
leg cast to the right lower extremity. He has no visible wounds on admission but arrives with documentation that a pressure ulcer exists under the cast. Two weeks after admission to the nursing facility, the cast is removed by the physician. Following the removal of the cast, the right heel is observed and assessed as a Stage 3 pressure ulcer, which remains until the subsequent assessment.
• How would you code M0300C1 on the subsequent assessment?

Answer
• Stage 3
• Present on admission

Coding Scenario 3• Mr. H was admitted with a known pressure
ulcer/injury due to a non-removable dressing. Ten days after admission, the surgeon removes the dressing, and a Stage 2 pressure ulcer is identified. Two weeks later the pressure ulcer is determined to be a full thickness ulcer and is at that point Stage 3. It remains Stage 3 at the time of the next assessment.
• How would you code M0300C1?

Answer
• Stage 3
• Not present upon admission
Section M: Summary• Wording revisions due to Ulcer vs Injury
– Injury is used for closed wounds (Stage 1, Deep Tissue Injury)– Ulcer is used for open wounds (Stage 2-4, Unstageable due to
slough/eschar• Significant Change in Definition related to “Present on
Admission”– If the pressure ulcer/injury was present on admission/entry or
reentry and becomes unstageable due to slough or eschar, during the resident’s stay, the pressure ulcer/injury is coded at M0300F and should not be coded as “present on admission”

Section M: Summary• If two pressure ulcer/injuries occur on the same bony
prominence and are separated, at least superficially, by skin, then count them as two separate pressure ulcer/injuries. Stage and measure each pressure ulcer/injury separately.
• M1040D-open lesions that develop as part of a disease or condition and are not coded elsewhere on the MDS, such as wounds, boils, cysts, and vesicles, should be coded in this item.
• M1040G-do not code cuts/lacerations or abrasions here. Although not recorded on the MDS, these skin conditions should be considered in the plan of care
Section M: Summary• Deleted Items:
– M0610 (Wound Measurements)
– M0700 (Most Severe Tissue Type Present)
– M0800 (New or Worsened Pressure Ulcer)
– M0900 (Healed Pressure Ulcers)

Section N• Three New items added• New QRP QM (drug regimen review)• Drug Regimen Review
– Upon admission medications reviewed– Significant clinical issues reported to provider
(physician or NP) and follow up orders/recommendations implemented by midnight of the following day
– Upon discharge any clinically significant issues were reported to provider and orders/recommendations implemented by midnight the next day

Section N: N2001 and N2003• To be completed on 5 day PPS assessment• Two questions related to resident admission (drug
regimen review)

Section N: N2001 and N2003• Coding N2001
0- No, no issue found (Go to Section O)1- Yes, Issue found (continue to N2003)9- NA, Resident not taking medications (skip to O)
• Coding N2003 (Only completed if answered YES to N2001)0- No1- yes

Section N- N2005• Covers entire stay- from Admission throughout stay• If N2003 us coded as “No”, then N2005 must also be
“No”

Drug Regimen Review• If the physician prescribes an action that will take longer than
midnight of the next calendar day to complete, then code 1, YES, should still be entered, if by midnight of the next calendar day, the clinician has taken the appropriate steps to comply with the recommended action.
• Example of a physician-recommended action that would take longer than midnight of the next calendar day to complete.– The physician writes an order instructing the clinician to monitor
the medication issue over the next three days and call if the problem persists.
Drug Regimen Review• Includes all medications
– Prescribed and over the counter medications– Administered by an route (including oral, topical, inhalant,
injection, sublingual, parenteral, and by infusion– Includes total parenteral nutrition (TPN) and oxygen
• A clinical significant medication issue is a potential or actual issue that, in the clinician’s professional judgement, warrants:– Physician (or physician-designee) communication and – Completion of prescribed/recommended action by midnight of
the next calendar day

Drug Regimen Review• Clinically Significant Issues
– Medication prescribed despite medication allergies– Adverse reactions to medications– Duplicate therapy– Wrong patient, drug, dose, route, and time errors– Omissions– Drug interactions– Ineffective drug therapy– Nonadherence to drug therapy
Drug Regimen Review• Who can perform the Drug Regimen Review?
– CMS does not provide guidance on who can or cannot code the DRR items
– Each facility determines their own policies and procedures for completing the assessments
– Each facility provides patient care according to their unique characteristics and standards
– Not strictly a pharmacy function• Communication Methods
– In person– Telephone, voicemail– Electronic means– Fax– Any means that appropriately conveys messages of patient status
Drug Regimen Review• Drug Regimen Review performed:– Upon admission or as close to Admission as
possible (per CMS)– Should be completed within first 24 hours– Drug Regimen Review is ongoing throughout stay• Each new drug order• Each revision or change in drug order• Change in clinical status

Drug Regimen Review• Medication Reconciliation
– Compare admission orders with medications received in hospital, prior to hospitalizations
– Review Diagnosis and Allergies
– Review Labs and ongoing lab monitoring (coumadin, etc.)

Drug Regimen Review• Operational Changes
– Develop and review current processes– Involve consultant pharmacist– Need to educate nursing staff on drug regimen
review and requirements– Educate providers on new regulations and
requirements– Documentation:
• Nurse document DRR upon admission (review, physician notification, and recommendation)

Section O• Chemotherapy Clarification– Hormonal and other agents administered to prevent
the recurrence or slow the growth of cancer should NOT be coded in this item, as they are not considered chemotherapy for the purpose of coding the MDS
– Examples: Tamoxifen, Evista, Fareston, Arimidex, Aromasin, Femara, Lupron, Eligard, Lupron Depot, Viadur

Section O• Clarifications for O0100F and O0200G
– O0100F now defined as an invasive mechanical ventilator (ventilator or respirator)
– O0100G now named a non-invasive mechanical ventilator (BiPAP/CPAP)
• Pneumococcal– Removed old CDC diagram
– Follow guidance at :• https://www.cdc.gov/vaccines/vpd/pneumo/downloads/
pneumo-vaccine-timing.pdf


Care Area Assessments• Opioids have been added to the care areas
– Delirium– Visual Function– Communication– Activities of Daily Living– Incontinence– Mood State– Falls– Dental Care– Pressure Ulcer/Injury
Care Area Assessments• Updates to CAAs
– Behavioral Review of Indicators updated with inclusion of Section E items • Potential Indicators of Psychosis• Behavioral Symptoms
– Alarm use has been added as a factor to can cause or exacerbate behavior

Summary• Resident Interviews
– Updated to day of ARD or day before• Section GG
– Updated items– Addition of prior functioning– Self care– Mobility
• Section I– New item I0020 (Primary Medical Condition)
• Section J– Prior Surgery
Summary• Section K
– K0510C (Mechanically altered diet)– K0510D (Therapeutic Diet)– K0710A (Proportion of total calories)– K0710B (Average fluid intake)
• Section M– Language changes– Deleted items (M0300B3, M0610A-C, M0700, M0800A-F,
M0900A-D)– Clarification “present upon admission”
Summary• Section N
– Drug Regimen Review• Medication Review• Medication Follow-up• Medication Intervention
• Section O– Chemotherapy medication clarification– Invasive mechanical ventilator separated from non invasive
mechanical ventilator• Updates to Care Area Assessments worksheets
– Opioids added to care areas
Questions or Comments?
Thank You.Cassie Crafton RN, CDP, RAC-CT