may 28, 2015 links bw ptsd & dv
TRANSCRIPT

Links between PTSD and Domestic Violence in Military Couples
https://learn.extension.org/events/1880

Sign up for webinar email notifications
http://bit.ly/MFLN-Notify
Provide feedback and earn CEU credit with one link:We will provide this link at the end of the webinar

Research and evidenced-based professional development
through engaged online communities.
eXtension.org/militaryfamilies

https://www.facebook.com/MFLNfamilydevelopment https://twitter.com/MFLNFamDev Talk About it Tuesday: #MFLNchat
https://www.youtube.com/user/MILFamLN
https://www.linkedin.com/groups/Military-Families-Learning-Network-6617392
To subscribe to our MFLN Family Development newsletter send an email [email protected]
Subject: Subscribe
Available resources
https://learn.extension.org/events/1880
Find slides and additional resources under ‘event materials’

CE Credit Information• Webinar participants who want to receive 2.0 NASW CE Credits and/or 2.0 Georgia
Marriage and Family Therapy CE Credits (or just want proof participation in the training) need to take the post-test provided at the end of the webinar.
• CE Certificates of completion will be automatically emailed to participants upon completion of the evaluation & post-test. Questions/concerns surrounding the National Association of Social Workers (NASW)
CE credit certificates can be emailed to this address: [email protected]
Sometimes state/professional licensure boards for fields other than social work recognize NASW CE credits, however, you would have to check with your state and/or professional boards if you need CE Credits for your field.
• To learn more about obtaining CE Credits, please visit this website:
http://blogs.extension.org/militaryfamiles/family-development/professionaldevelopment/nasw-ce-credits/

Today’s Presenters:
Casey Taft, Ph.D. Is a staff psychologist at the National Center for PTSD in the VA Boston Healthcare System, and Professor of Psychiatry at Boston University School of Medicine. Dr. Taft was the 2006 Young Professional Award winner from the International Society for Traumatic Stress Studies, and the 2009 Linda Saltzman Memorial Intimate Partner Violence Researcher Award winner. Dr. Taft currently serves as Principal Investigator on funded grants focusing on understanding and preventing partner violence through the National Institute of Mental Health, the Department of Veterans Affairs, the Centers for Disease Control, and the Department of Defense. Dr. Taft is on the Editorial Boards of several journals in the areas of violence, trauma, and the family. Dr. Taft has also chaired an American Psychological Association task force on trauma in the military and has consulted with the United Nations on preventing violence and abuse globally.

Trauma and Intimate
Partner Violence
Casey Taft, Ph.D.
National Center for PTSD, VA Boston
Healthcare System
Boston University School of Medicine
Casey Taft, Ph.D.National Center for PTSD, VA Boston
Healthcare System
Boston University School of Medicine
Links between PTSD and Domestic Violence in Military Couples

Objectives• Contextualize the use of intimate partner violence
(IPV) using the social information processing model
• Review the relationship of PTSD and IPV
• Identify limitations of IPV interventions
• Discuss the Strength at Home programs and strategies for preventing IPV in military families

Social Information Processing Model
• Men who use IPV exhibit cognitive deficits (e.g., faulty attributions, irrational beliefs) that impact interpretation (decoding stage)
• Men who use IPV have difficulty generating a variety of nonviolent responses (decision-making stage)
• Men who use IPV lack the skills to enact a competent response (enactment stage)
• The process is influenced by “transitory factors” such as alcohol use, traumatic brain injury, etc.
Holtzworth-Munroe, 1992

Survival Mode Model• Vigilance to threats in warzone leads combat veteran
to enter into survival mode inappropriately when stateside
• Perceive unrealistic threats
• Exhibit hostile appraisal of events
• Overvalue aggressive responses to threats
• Exhibit lower threshold for responding to the threat
Chemtob et al., 1997

PTSD and IPV
• Service members without PTSD not more violent than civilians (Bradley, 2007)
• Rates in the National Vietnam Veterans Readjustment Study (Kulka et al., 1990)
• Veterans with PTSD = 33%• Veterans without PTSD = 13.5%
• Meta-analytic results (Taft et al., 2011)
• PTSD and physical IPV: r = .42• PTSD and psychological IPV: r = .36

PTSD and IPV
Avoidance/Numbing
Re-experiencing
Hyperarousal
e.g., Taft et al., 2007

Irrational Beliefs
a
-.22**
-.27
Total PTSD Symptoms
Physical IPV
Indices of mediation• ab- indirect effect (90% CI)
• .002 (.000042,.00316**)•percent mediation- ab/(c’ + ab)
•21%
Total PTSD Symptoms
Physical IPV
b
-.01* -.23
c‘ .01*
.21
c .01** .27
Note: unstandardized (top) and standardized (bottom) regression coefficients
* = p < .05; ** = p < .01

Other Contributing Factors
1. Depression
2. Alcohol use problems
3. Traumatic brain injury
4. Power conflicts
5. Trust issues
6. Self-esteem problems

IPV
Intervention

Lack of Empirically Supported Interventions
• No randomized clinical trial has shown treatment effects in military population (e.g., Dunford, 2000)
• Those receiving interventions in other settings average 5% reduction in recidivism relative to untreated groups (Babcock et al., 2004)
• Barriers to examining IPV interventions• Randomizing violent men to no-treatment controls• Arrest and monitoring associated with IPV reduction• Lack of victim contact• IPV practice guidelines
Limitations of Existing Interventions
• Not tailored to military populations
• Are not trauma informed
• Deemphasize psychiatric factors (PTSD) and biological factors (head injury)
• Many are not considered “therapy”
• Large, impersonal groups

Men’s Program

• Department of Defense
• Department of Veterans Affairs
• Goal to develop/evaluate model program for treating IPV in service members/Veterans
• No prior randomized clinical trial has shown treatment effects in a military population
Men’s Program Objectives

Stage 1
Stage 2
Stage 3
Stage 4
Men’s Program Stages

Strength at Home Stages
• Stage I (Sessions 1-2): Psychoeducation
• Pros/cons of abuse
• Forms of IPV and impacts of trauma
• Core themes
• Goals for group

Strength at Home Stages
• Stage II (Sessions 3-4): Conflict Management
• The anger response
• Self-monitor thoughts, feelings, physiological responses
• Assertiveness
• Time Outs to de-escalate difficult situations

Strength at Home Stages
• Stage III (Sessions 5-6): Coping Strategies
• Anger-related thinking
• Realistic appraisals of threat and others’ intentions
• Coping with stress
• Problem-focused versus emotion-focused coping
• Relaxation training for anger

Strength at Home Stages
• Stage IV (Sessions 7-12): Communication Skills
• Roots of communication style
• Active listening
• Assertive messages
• Expressing feelings
• Communication “traps”

• Contacted every three months
• High (>70%) rate of contact
• Safety planning, hotline numbers, mental health services, other support
• Perceptions of IPV
• Program feedback
Intimate Partner Involvement

Sample Characteristics
• 135 enrolled in study (67 to SAH-V intervention, 68 to ETAU)
• Average age = 38.10
• 77% White, 14% Black/African-American
• 34% married, 23% dating, 14% single
• 59% Court-involved
• 57% OEF/OIF/OND, 13% Vietnam, 8% Gulf War
• Treatment Completion (≥9 sessions): 55%

Assessed for eligibility (n=157)
Randomized (n=135)
Excluded (n=22)
Allocated to SAH intervention (n=67)
Allocated to ETAU intervention (n=68)
Completed week 12 follow-up (n=49)
Received SAH intervention (n=57)
Completed week 24 follow-up (n=52)
Received ETAU intervention (n=43)
Completed week 12 follow-up (n=57)
Completed week 24 follow-up (n=57)

Physical IPV
Pre-Tx Post-Tx 3-Month Follow-up
0
0.5
1
1.5
2
2.5
3
Strength at HomeEnhanced Treatment as Usual
Mea
n S
core
B(.061)= -0.135, p=.029, CI [.773, .986]

Psychological IPV (CTS)
Pre-Tx Post-Tx 3-Month Follow-up
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Strength at HomeEnhanced Treatment as Usual
Mea
n S
core
B(.135)= -0.304, p=.026, CI [.565, .964]

Restrictive Engulfment (MMEA)
Pre-Tx Post-Tx 3-Month Follow-up
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Strength at HomeEnhanced Treatment as Usual
Mea
n S
core
B(.027)= -0.072, p=.01, CI [.882, .983]

Couples Prevention Program

• Centers for Disease Control and Prevention
• Program for preventing IPV in returning service members/Veterans before it begins• Relationship distress but no current violence
Couples’ Program Objectives
• Phase I (Sessions 1-3): Psychoeducation• Education on trauma and impact on relationships• Promoting insight into relationship difficulties• Core themes
• Phase II (Sessions 4-5): Conflict Management• Roots of conflict management style• Assertiveness training• Time Outs to de-escalate difficult situations
• Phase III (Sessions 6-10): Communication Skills• Listening skills • Emotional expression• Communication “traps”
Couples’ Program Phases

Sample Characteristics
• 156 enrolled• 80% Caucasian, 13% African American, and 7% of
another ethnicity
• Age 24-59 years, 41 years on average
• In relationship 6 months – 25 years; 8.1 years on average
• 76% married
• 74% have children
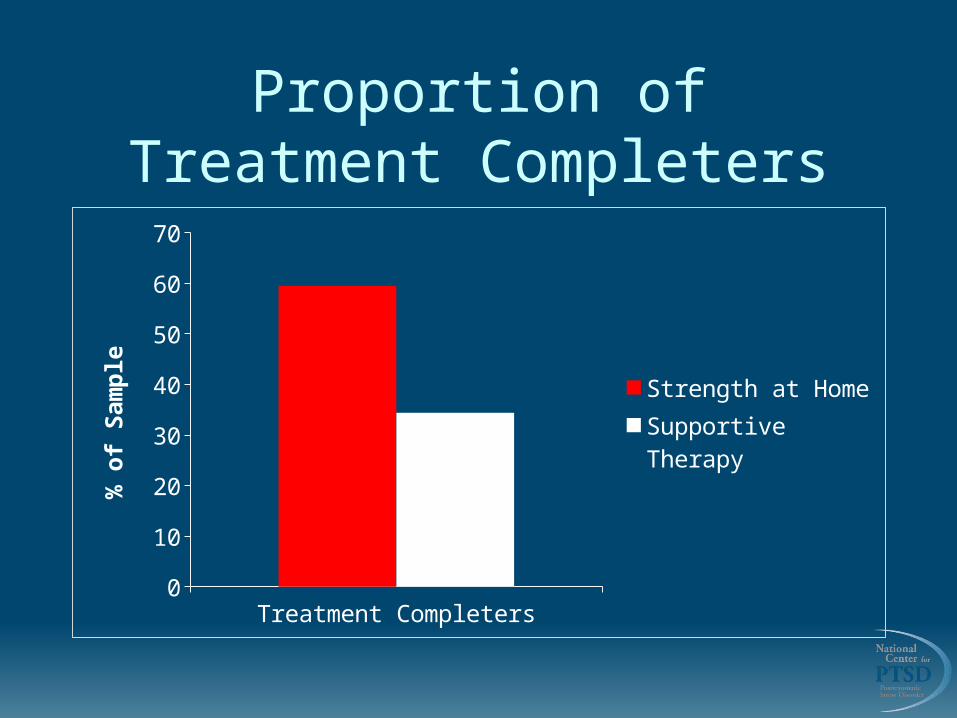
Proportion of Treatment Completers
Treatment Completers0
10
20
30
40
50
60
70
Strength at HomeSupportive Therapy
% o
f S
amp
le

Veteran Physical IPV
Pre-T
x
Post-T
x
6-M
onth
Foll
ow-u
p
12-M
onth
Foll
ow-u
p0
0.20.40.60.8
11.21.41.6
Strength at HomeSupportive Therapy
Mea
n S
core

Partner Physical IPV
Pre-T
x
Post-T
x
6-M
onth
Foll
ow-u
p
12-M
onth
Foll
ow-u
p0
0.5
1
1.5
2
2.5
Strength at HomeSupportive Therapy
Mea
n S
core
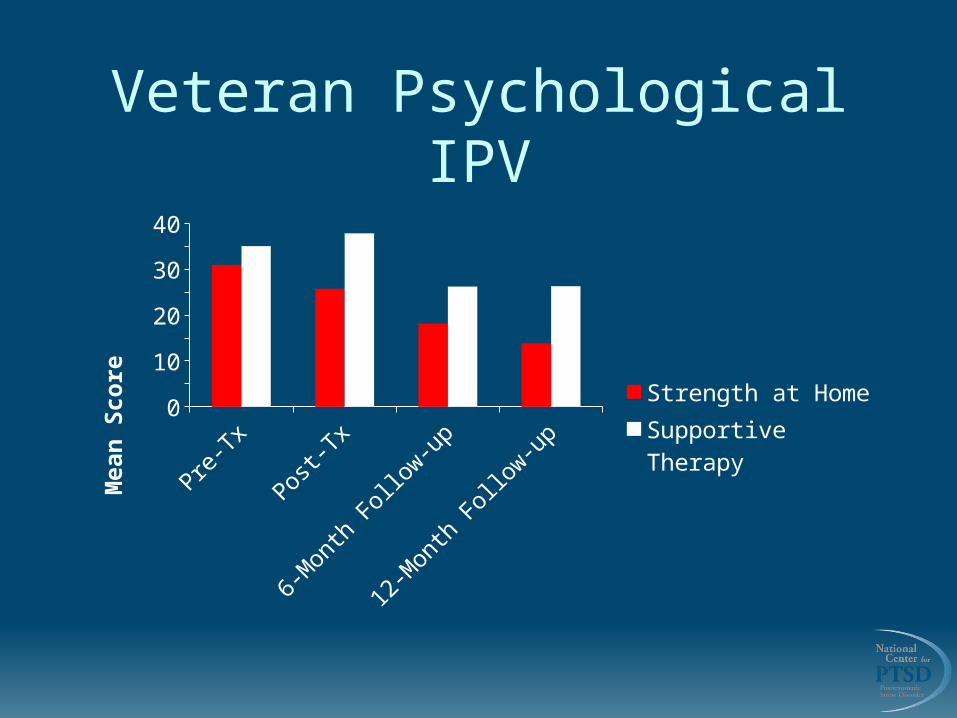
Veteran Psychological IPV
Pre-T
x
Post-T
x
6-M
onth
Foll
ow-u
p
12-M
onth
Foll
ow-u
p05
10152025303540
Strength at HomeSupportive Therapy
Mea
n S
core

Partner Psychological IPV
Pre-T
x
Post-T
x
6-M
onth
Foll
ow-u
p
12-M
onth
Foll
ow-u
p05
101520253035
Strength at HomeSupportive Therapy
Mea
n S
core
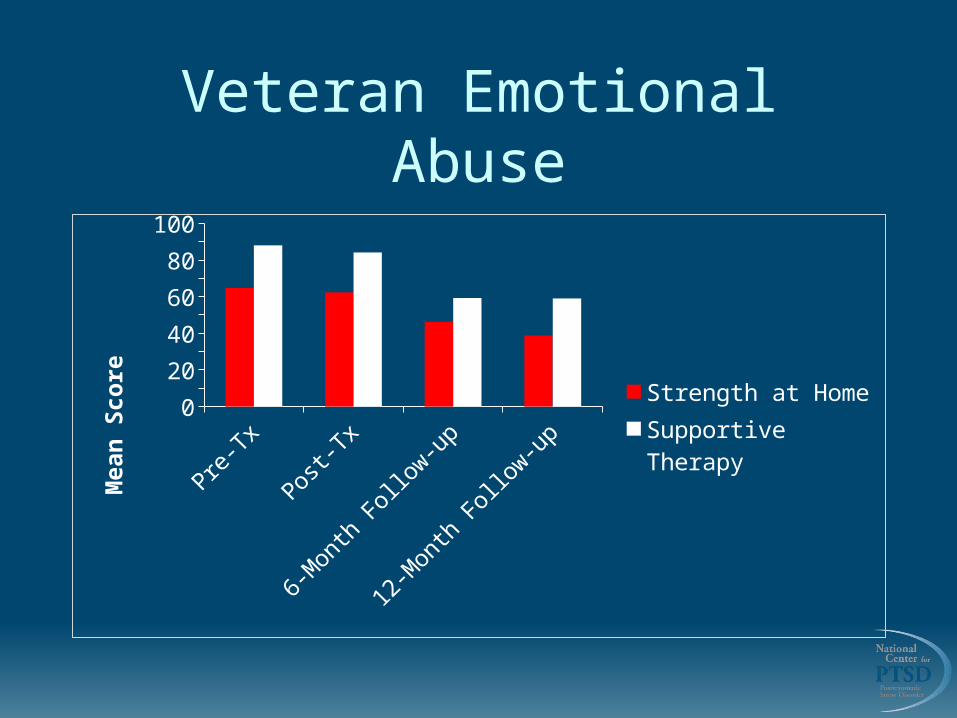
Veteran Emotional Abuse
Pre-T
x
Post-T
x
6-M
onth
Foll
ow-u
p
12-M
onth
Foll
ow-u
p0
20
40
60
80
100
Strength at HomeSupportive Therapy
Mea
n S
core

Partner Emotional Abuse
Pre-T
x
Post-T
x
6-M
onth
Foll
ow-u
p
12-M
onth
Foll
ow-u
p0
20
40
60
80
Strength at HomeSupportive Therapy
Mea
n s
core

Process and Clinical Considerations

Rationale for Group Focus
• Group cohesion a predictor of violence reduction (Taft et al., 2003)
• Camaraderie among service members
• Sense of shared experience
• Enhances support
• Group members provide each other feedback
• Increase empathy from relating to other group members

Therapeutic Factors(Yalom, 1995)
1) Instillation of hope
2) Universality of experience
3) Imparting information
4) Altruism
5) Socialization techniques
6) Imitative behavior
7) Group cohesiveness
8) Catharsis
9) Existential factors

Leader Tasks and Techniques• Role model empathy and supportive listening
• Encourage self-disclosure
• Promote healthy relationship norms
• Make the group a safe place for exploration of personal and interpersonal problems
• Comment on process
• Accountability emphasized throughout group

Reviewing Practice Assignments
• Comment on positive work done before exploring problem areas
• Highlight use of new skills by asking “How is this different than what you’ve done in the past?”
• “If you could do it over again, how would you do it differently?”
Key Take-Away Applications
Examine IPV using the
Social Information
Processing Model
Discover tips to implement in work with military families.
Review relationship between PTSD
and domestic violence.
Explore Effectiveness of
Strengths at Home model.

CE Credit Information• Webinar participants who want to receive 2.0 NASW CE Credits and/or 2.0 Georgia
Marriage and Family Therapy CE Credits (or just want proof participation in the training) need to take this evaluation AND post-test:
https://vte.co1.qualtrics.com/SE/?SID=SV_6EHzErvYOKbkbKR
• CE Certificates of completion will be automatically emailed to participants upon completion of the evaluation & post-test. Questions/concerns surrounding the National Association of Social Workers
(NASW) CE credit certificates can be emailed to this address: [email protected]
Sometimes state/professional licensure boards for fields other than social work recognize NASW CE credits, however, you would have to check with your state and/or professional boards if you need CE Credits for your field.
• To learn more about obtaining CE Credits, please visit this website: http
://blogs.extension.org/militaryfamilies/family-development/professional-development/nasw-ce-credits/
Upcoming Webinars: Social Emotional Development in the Early Years: Understanding Social Emotional Development
Thursday, June 18, 2015 11:00 am- 12:30pm Eastern
Social Emotional Development in the Early Years: Promoting Positive Relationships
Thursday, August 13, 2015 11:00 am- 12:30pm Eastern

Find all upcoming and recorded webinars covering:
http://www.extension.org/62581
Personal FinanceMilitary Caregiving
Family Development
Family TransitionsNetwork Literacy
Nutrition & Wellness Community Capacity Building