maxillary obturator prosthesis for a hemimaxillectomy patient: a … · 2016-12-11 · bony...
TRANSCRIPT

The Saudi Journal for Dental Research (2016) 7, 153–159
King Saud University
The Saudi Journal for Dental Research
www.ksu.edu.sawww.sciencedirect.com
CASE REPORT
Maxillary obturator prosthesis for a
hemimaxillectomy patient: A clinical case report
* Corresponding author at: Department of Oral Rehabilitation,
Faculty of Dentistry, Khartoum University, Khartoum, Sudan. Tel.:
+249 928978938.
E-mail address: [email protected] (M.N. Alhajj).
Peer review under responsibility of King Saud University.
Production and hosting by Elsevier
http://dx.doi.org/10.1016/j.sjdr.2016.03.0012352-0035 � 2016 The Authors. Production and hosting by Elsevier B.V. on behalf of King Saud University.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Mohammed Nasser Alhajj a,b,*, Ibrahim A. Ismail a, Nadia Khalifa c
aDepartment of Oral Rehabilitation, Faculty of Dentistry, Khartoum University, Khartoum, SudanbDepartment of Prosthodontics, Faculty of Dentistry, Thamar University, Dhamar, YemencDepartment of General and Specialist Dental Practice, College of Dental Medicine, University of Sharjah, Sharjah,United Arab Emirates
Received 28 July 2015; revised 30 January 2016; accepted 22 March 2016Available online 31 March 2016
KEYWORDS
Obturator;
Hemimaxillectomy;
Odontogenic Myxoma;
Clinical report
Abstract This clinical report describes a comprehensive prosthodontic treatment of a young
patient diagnosed with Odontogenic Myxoma. The treatment procedures included surgical removal
of the tumor, immediate surgical plate, interim obturator, orthodontic treatment, and definitive
obturator. The definitive prosthesis was cobalt–chromium removable partial denture gained its sup-
port from the remaining teeth and tissues. The follow-up system revealed satisfactory results with
no deterioration in the prosthesis.� 2016 The Authors. Production and hosting by Elsevier B.V. on behalf of King Saud University. This is
an open access article under the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Treatment modalities of a malignant tumor in the maxilla arevaried according to many factors such as; size, type, severity,etiology and location of the tumor. The most frequent treat-
ment is surgical removal of the affected area which results ina large defect with oro-nasal/antral communication.1,2
Acquired palatal defects resulting from hemimaxillectomymay cause major difficulties with speech, swallowing and
mastication. In turn, these functional problems may affect
the quality of life. Change in appearance resulting from theloss of tissue and underlying structures may also lead to emo-tional stress and depression.3–6 In addition, social phobia andanxiety tend to occur more often in patients who lose part of
their maxillofacial complex than those who lose another partof their body as arm or leg or even both of them.7–9
Rehabilitation of the patient presenting with a malignant
tumor in the maxilla requires a multidisciplinary approachincluding surgical treatment, radio/chemotherapy, phoneticrehabilitation, physiotherapy, and prosthetic treatment.10,11
These defects can be repaired surgically using free micro-vascularized flaps or pedicled flaps. When there are large resec-tions of the maxilla, the defect may be obturated with a dentalor maxillofacial prosthesis. Support for this prosthesis can be
gained either from the remaining teeth and tissues or usingdental implants.12–14
Reconstruction of the maxillectomy with an obturator has
several advantages. Besides replacing the missing soft and hard

154 M.N. Alhajj et al.
tissues, it enables the patient to swallow, masticate, and speakapproximately in the normal way, and forms a barrier betweennasal and oral cavities. Other advantages include that the
obturator can be removed from the patient’s mouth permittingfor a clear vision and early detection of any recurrent tumor;and a better facial appearance can be achieved with the pres-
ence of the obturator where it can provide support for the tis-sues of the face.5,15,16
Odontogenic Myxoma is an uncommon mesenchymal
odontogenic tumor arising from the dental papilla, dental fol-licle, or the periodontal ligament characterized by rounded andangular cells lying in an abundant mucoid stroma that replacesthe cancellous bone and expands the cortex. The presence of
odontogenic epithelium, association with missing or un-erupted teeth and its exclusive location in the tooth-bearingareas of the jaws may be the evidence for its odontogenic ori-
gin. Clinically, it is a painless, invasive, and slowly growingmass causing marked asymmetry of the face. It usually occursin second and third decades of life and causes expansion of
bony cortices, displacement and loosening of teeth.17,18
This present report describes a prosthodontic rehabilitationof a patient with Odontogenic Myxoma in the maxilla.
2. Clinical report
A young male patient aged 18 years presented to the Khar-
toum Dental Teaching Hospital (KDTH) in Sudan complain-ing of a swelling in the left maxillary posterior region (Fig. 1).The involved teeth expressed no pain or mobility.
Clinical and radiographic examination was carried out. A
biopsy was sent for investigation. The histopathologic resultrevealed an Odontogenic Myxoma involving the left maxillaryposterior area. The patient was then referred to the graduate
prosthodontic clinics at the University of Khartoum, Facultyof Dentistry for construction of a surgical obturator/plate.
The pre-operative impression was made using an irre-
versible hydrocolloid material (Hydrogum 5, Zhermack, Italy)in a modified perforated stock tray. The impression waspoured with dental stone (Gyproc, Prevest Denpro, Jammu,
India) to produce the positive template/cast. The cast was sentto the surgeon to delineate area of resection (Fig. 2), and an
Figure 1 Intra-oral pre-operative view.
immediate surgical obturator was fabricated accordingly. Inthe operating room resection of the maxilla was done toremove the tumor (Figs. 3 and 4) and a surgical closure was
attempted using the remaining and neighboring soft tissues.The defect was large and the available tissues were not suffi-cient to completely close the defect. The surgical obturator
was inserted immediately after resection of the maxilla andheld in position using Adam’s clasps on the remaining naturalteeth (Fig. 5).
One week after surgery the patient came for review to ruleout complications, and proper position of the plate wasensured. The patient presented with a hemimaxillectomy defectextending from the midline to the soft palate in the left side.
Clinical intra-oral examination showed a small hollow remain-ing with an oro-nasal communication, while the remainingteeth, gingiva, and palate appeared within the normal limits.
Crowding of the teeth in the canine region was observed andpoor oral hygiene was noticed. Lack of oral hygiene may havebeen due to the inability of the patient to clean his teeth prop-
erly because of the plate in his mouth. Extra-oral examinationshowed a curved profile, an asymmetrical face, no deviation ofthe mandible, no palpable or tender lymph nodes, and a nor-
mal TMJ. Radiographic examination revealed that the sup-porting bone of the remaining teeth was normal and so wasthe crown root ratio. The defect was classified as Aramanyclass I defect. The patient was shown how to remove and
replace the plate and how to maintain a good oral hygiene.Another appointment was arranged for one week later whena tissue conditioning material was applied to improve the fit
and increase the comfort of the patient.After two weeks the clinical intra- and extra-oral
examination revealed a good initial healing at the defect site.
The extra-oral suture was removed at the surgery department.The fabrication of an interim obturator was initialized. Theusual steps in fabricating the conventional acrylic partial
denture were followed (Figs. 6–10). The retention for this typeof obturator was gained from the remaining teeth withwrought wire clasps on the teeth 11, 14, 16. In this stage, a buc-cal canine retractor was incorporated into the acrylic denture
Figure 2 Delineated area of resection.

Figure 3 Surgical removal of the tumor.
Figure 4 Tumor after resection.
Figure 5 Surgical plate in situ.
Figure 6 Final impression for interim prosthesis.
Maxillary obturator prosthesis for a hemimaxillectomy patient 155
base to move the canine down and palatally to be realigned in
its correct position on the dental arch (Fig. 10). A follow-upsystem was scheduled for three months later. Tissue condi-tioner was applied as needed and a continuous activation ofthe buccal canine retractor was done. The patient was able
to speak, swallow and maintain good oral health effectively.Six months later the patient presented with good extra-oral
healing. No significant disfigurement on the face was observed.
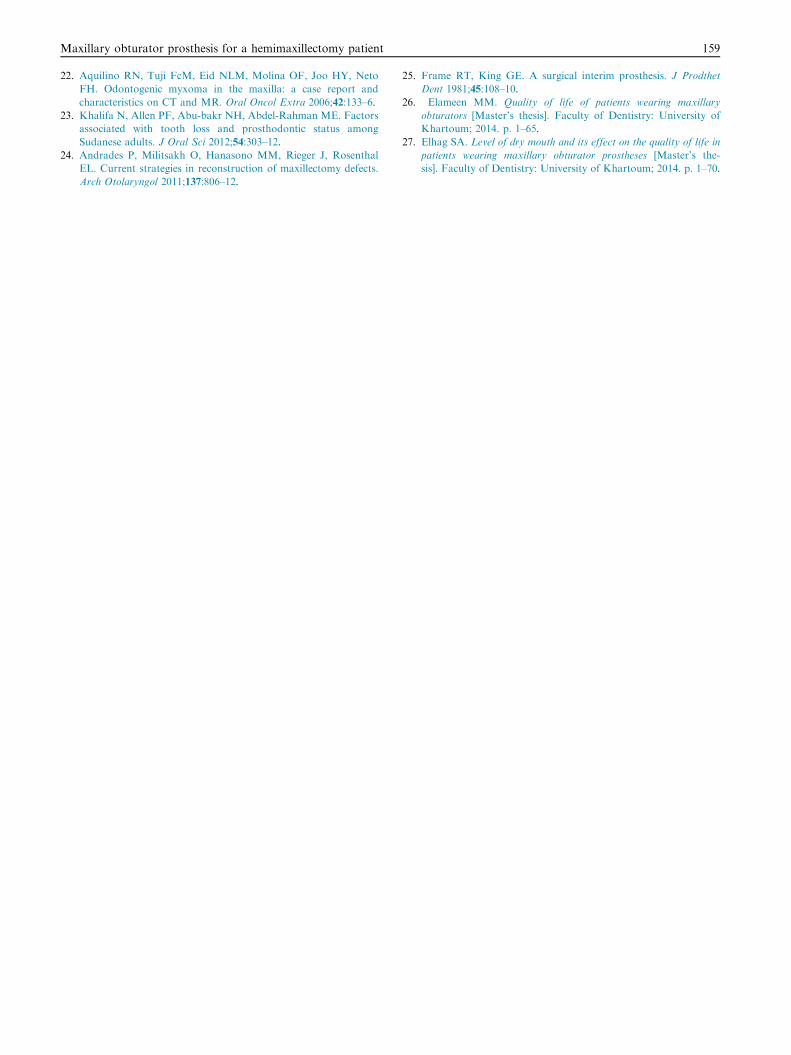
The oral hygiene was obviously improved. After ensuring thatthe healing of the wound had taken place (Fig. 11), the treat-ment plan for the construction of the definitive obturator (a
cast-metal removable dental prosthesis) was rolled out. At thisstage the desired position of the canine was achieved (Fig. 15).The primary impressions were made using irreversible hydro-
colloid material (Hydrogum 5, Zhermack, Italy) and theprimary casts were obtained. The maxillary cast was surveyed,the undercuts were observed and the necessary mouth
preparations were done. For the design of the framework the
tripodal design was selected. For this design the rest seats wereprepared on the right first and second molars, first premolar,and on the canine. A custom tray was constructed on the pri-mary cast with cold-cure acrylic resin (Superacryl Plus,
SpofaDental, Markova, Czech). Green stick compound (Trac-ing Sticks, kemdent, UK) was used for border molding and thefinal impression (Fig. 12) was made using polyvinyl siloxane
(PVS) (Oranwash L, Zetaplus, Zhermack, Italy). This waspoured with dental stone type III to produce the secondaryworking cast, which was then duplicated to produce the
refractory cast, on which the wax up of the framework wasperformed (Fig. 13). The framework was casted usingcobalt–chromium alloy. This was tried in the patient’s mouth
to evaluate the fit with the underlining structures, with the helpof pressure indicator paste (PIP, MIZZY Inc. USA). Bite rimblocks were constructed on the framework. Centric jawrelation record was obtained and the casts were mounted on
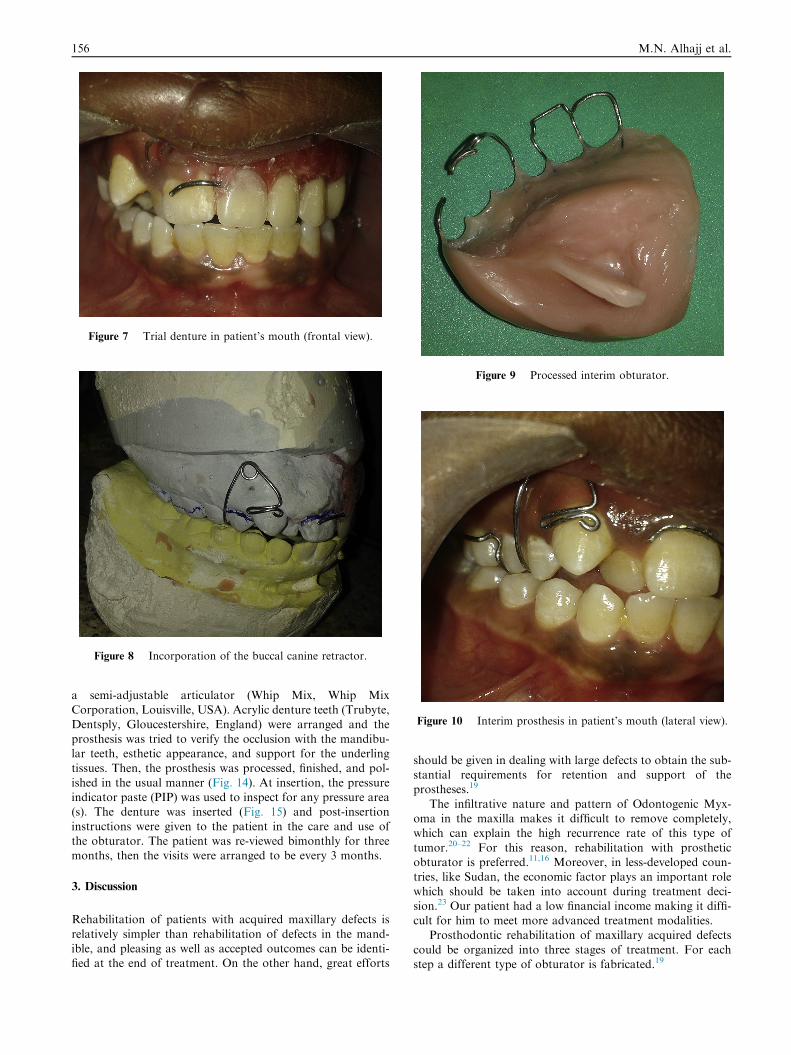
Figure 7 Trial denture in patient’s mouth (frontal view).
Figure 8 Incorporation of the buccal canine retractor.
Figure 9 Processed interim obturator.
Figure 10 Interim prosthesis in patient’s mouth (lateral view).
156 M.N. Alhajj et al.
a semi-adjustable articulator (Whip Mix, Whip MixCorporation, Louisville, USA). Acrylic denture teeth (Trubyte,
Dentsply, Gloucestershire, England) were arranged and theprosthesis was tried to verify the occlusion with the mandibu-lar teeth, esthetic appearance, and support for the underling
tissues. Then, the prosthesis was processed, finished, and pol-ished in the usual manner (Fig. 14). At insertion, the pressureindicator paste (PIP) was used to inspect for any pressure area(s). The denture was inserted (Fig. 15) and post-insertion
instructions were given to the patient in the care and use ofthe obturator. The patient was re-viewed bimonthly for threemonths, then the visits were arranged to be every 3 months.
3. Discussion
Rehabilitation of patients with acquired maxillary defects is
relatively simpler than rehabilitation of defects in the mand-ible, and pleasing as well as accepted outcomes can be identi-fied at the end of treatment. On the other hand, great efforts
should be given in dealing with large defects to obtain the sub-stantial requirements for retention and support of theprostheses.19
The infiltrative nature and pattern of Odontogenic Myx-oma in the maxilla makes it difficult to remove completely,which can explain the high recurrence rate of this type of
tumor.20–22 For this reason, rehabilitation with prostheticobturator is preferred.11,16 Moreover, in less-developed coun-tries, like Sudan, the economic factor plays an important role
which should be taken into account during treatment deci-sion.23 Our patient had a low financial income making it diffi-cult for him to meet more advanced treatment modalities.
Prosthodontic rehabilitation of maxillary acquired defects
could be organized into three stages of treatment. For eachstep a different type of obturator is fabricated.19
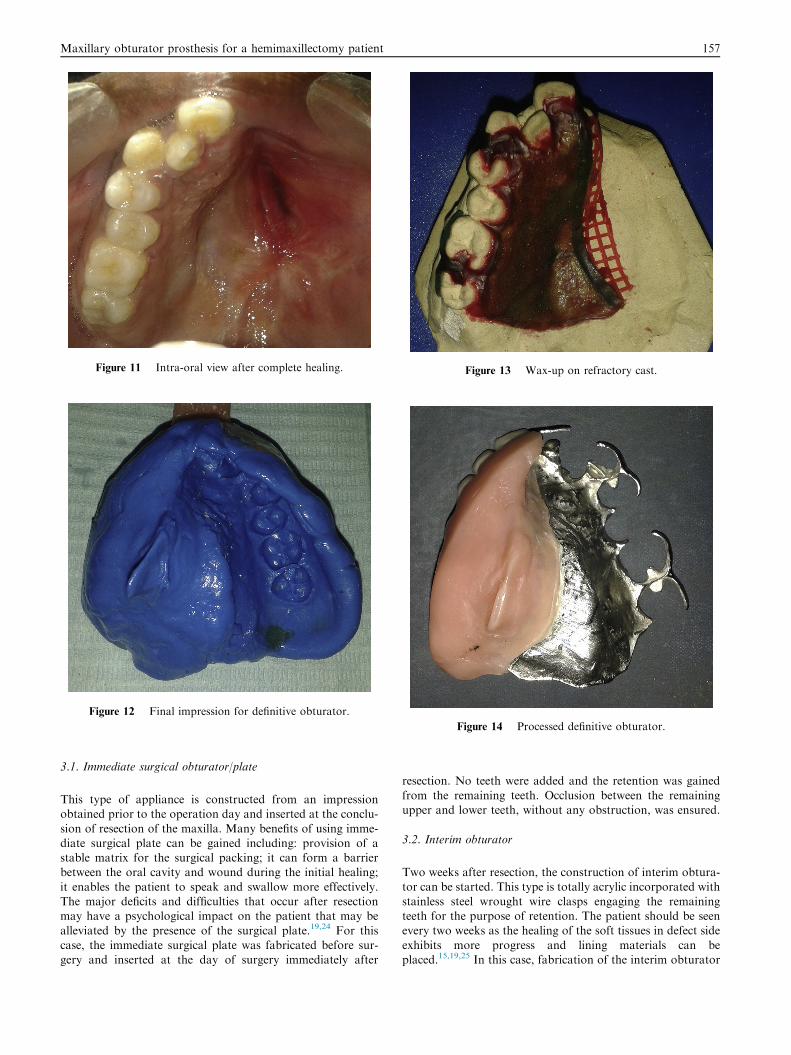
Figure 11 Intra-oral view after complete healing.
Figure 12 Final impression for definitive obturator.
Figure 13 Wax-up on refractory cast.
Figure 14 Processed definitive obturator.
Maxillary obturator prosthesis for a hemimaxillectomy patient 157
3.1. Immediate surgical obturator/plate
This type of appliance is constructed from an impressionobtained prior to the operation day and inserted at the conclu-
sion of resection of the maxilla. Many benefits of using imme-diate surgical plate can be gained including: provision of astable matrix for the surgical packing; it can form a barrierbetween the oral cavity and wound during the initial healing;
it enables the patient to speak and swallow more effectively.The major deficits and difficulties that occur after resectionmay have a psychological impact on the patient that may be
alleviated by the presence of the surgical plate.19,24 For thiscase, the immediate surgical plate was fabricated before sur-gery and inserted at the day of surgery immediately after
resection. No teeth were added and the retention was gained
from the remaining teeth. Occlusion between the remainingupper and lower teeth, without any obstruction, was ensured.
3.2. Interim obturator
Two weeks after resection, the construction of interim obtura-tor can be started. This type is totally acrylic incorporated with
stainless steel wrought wire clasps engaging the remainingteeth for the purpose of retention. The patient should be seenevery two weeks as the healing of the soft tissues in defect side
exhibits more progress and lining materials can beplaced.15,19,25 In this case, fabrication of the interim obturator
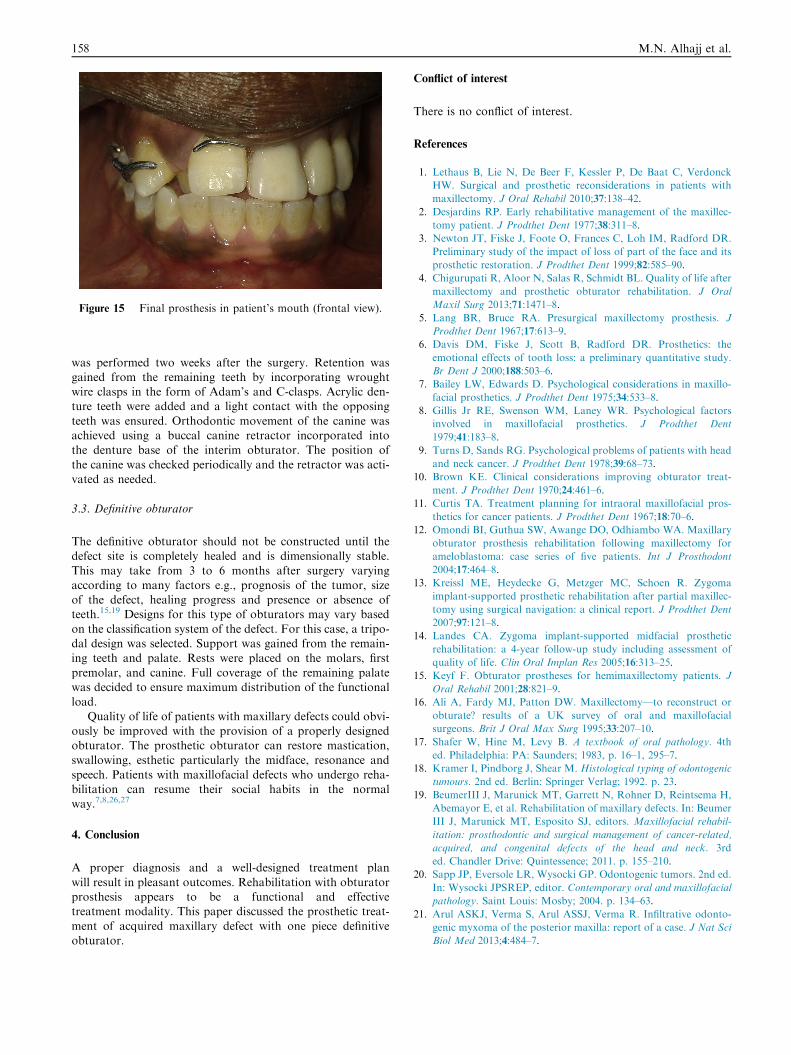
Figure 15 Final prosthesis in patient’s mouth (frontal view).
158 M.N. Alhajj et al.
was performed two weeks after the surgery. Retention wasgained from the remaining teeth by incorporating wroughtwire clasps in the form of Adam’s and C-clasps. Acrylic den-ture teeth were added and a light contact with the opposing
teeth was ensured. Orthodontic movement of the canine wasachieved using a buccal canine retractor incorporated intothe denture base of the interim obturator. The position of
the canine was checked periodically and the retractor was acti-vated as needed.
3.3. Definitive obturator
The definitive obturator should not be constructed until thedefect site is completely healed and is dimensionally stable.
This may take from 3 to 6 months after surgery varyingaccording to many factors e.g., prognosis of the tumor, sizeof the defect, healing progress and presence or absence ofteeth.15,19 Designs for this type of obturators may vary based
on the classification system of the defect. For this case, a tripo-dal design was selected. Support was gained from the remain-ing teeth and palate. Rests were placed on the molars, first
premolar, and canine. Full coverage of the remaining palatewas decided to ensure maximum distribution of the functionalload.
Quality of life of patients with maxillary defects could obvi-ously be improved with the provision of a properly designedobturator. The prosthetic obturator can restore mastication,swallowing, esthetic particularly the midface, resonance and
speech. Patients with maxillofacial defects who undergo reha-bilitation can resume their social habits in the normalway.7,8,26,27
4. Conclusion
A proper diagnosis and a well-designed treatment plan
will result in pleasant outcomes. Rehabilitation with obturatorprosthesis appears to be a functional and effectivetreatment modality. This paper discussed the prosthetic treat-
ment of acquired maxillary defect with one piece definitiveobturator.
Conflict of interest
There is no conflict of interest.
References
1. Lethaus B, Lie N, De Beer F, Kessler P, De Baat C, Verdonck
HW. Surgical and prosthetic reconsiderations in patients with
maxillectomy. J Oral Rehabil 2010;37:138–42.
2. Desjardins RP. Early rehabilitative management of the maxillec-
tomy patient. J Prodthet Dent 1977;38:311–8.
3. Newton JT, Fiske J, Foote O, Frances C, Loh IM, Radford DR.
Preliminary study of the impact of loss of part of the face and its
prosthetic restoration. J Prodthet Dent 1999;82:585–90.
4. Chigurupati R, Aloor N, Salas R, Schmidt BL. Quality of life after
maxillectomy and prosthetic obturator rehabilitation. J Oral
Maxil Surg 2013;71:1471–8.
5. Lang BR, Bruce RA. Presurgical maxillectomy prosthesis. J
Prodthet Dent 1967;17:613–9.
6. Davis DM, Fiske J, Scott B, Radford DR. Prosthetics: the
emotional effects of tooth loss: a preliminary quantitative study.
Br Dent J 2000;188:503–6.
7. Bailey LW, Edwards D. Psychological considerations in maxillo-
facial prosthetics. J Prodthet Dent 1975;34:533–8.
8. Gillis Jr RE, Swenson WM, Laney WR. Psychological factors
involved in maxillofacial prosthetics. J Prodthet Dent
1979;41:183–8.
9. Turns D, Sands RG. Psychological problems of patients with head
and neck cancer. J Prodthet Dent 1978;39:68–73.
10. Brown KE. Clinical considerations improving obturator treat-
ment. J Prodthet Dent 1970;24:461–6.
11. Curtis TA. Treatment planning for intraoral maxillofacial pros-
thetics for cancer patients. J Prodthet Dent 1967;18:70–6.
12. Omondi BI, Guthua SW, Awange DO, Odhiambo WA. Maxillary
obturator prosthesis rehabilitation following maxillectomy for
ameloblastoma: case series of five patients. Int J Prosthodont
2004;17:464–8.
13. Kreissl ME, Heydecke G, Metzger MC, Schoen R. Zygoma
implant-supported prosthetic rehabilitation after partial maxillec-
tomy using surgical navigation: a clinical report. J Prodthet Dent
2007;97:121–8.
14. Landes CA. Zygoma implant-supported midfacial prosthetic
rehabilitation: a 4-year follow-up study including assessment of
quality of life. Clin Oral Implan Res 2005;16:313–25.
15. Keyf F. Obturator prostheses for hemimaxillectomy patients. J
Oral Rehabil 2001;28:821–9.
16. Ali A, Fardy MJ, Patton DW. Maxillectomy—to reconstruct or
obturate? results of a UK survey of oral and maxillofacial
surgeons. Brit J Oral Max Surg 1995;33:207–10.
17. Shafer W, Hine M, Levy B. A textbook of oral pathology. 4th
ed. Philadelphia: PA: Saunders; 1983, p. 16–1, 295–7.
18. Kramer I, Pindborg J, Shear M. Histological typing of odontogenic
tumours. 2nd ed. Berlin: Springer Verlag; 1992. p. 23.
19. BeumerIII J, Marunick MT, Garrett N, Rohner D, Reintsema H,
Abemayor E, et al. Rehabilitation of maxillary defects. In: Beumer
III J, Marunick MT, Esposito SJ, editors. Maxillofacial rehabil-
itation: prosthodontic and surgical management of cancer-related,
acquired, and congenital defects of the head and neck. 3rd
ed. Chandler Drive: Quintessence; 2011. p. 155–210.
20. Sapp JP, Eversole LR, Wysocki GP. Odontogenic tumors. 2nd ed.
In: Wysocki JPSREP, editor. Contemporary oral and maxillofacial
pathology. Saint Louis: Mosby; 2004. p. 134–63.
21. Arul ASKJ, Verma S, Arul ASSJ, Verma R. Infiltrative odonto-
genic myxoma of the posterior maxilla: report of a case. J Nat Sci
Biol Med 2013;4:484–7.
Maxillary obturator prosthesis for a hemimaxillectomy patient 159
22. Aquilino RN, Tuji FcM, Eid NLM, Molina OF, Joo HY, Neto
FH. Odontogenic myxoma in the maxilla: a case report and
characteristics on CT and MR. Oral Oncol Extra 2006;42:133–6.
23. Khalifa N, Allen PF, Abu-bakr NH, Abdel-Rahman ME. Factors
associated with tooth loss and prosthodontic status among
Sudanese adults. J Oral Sci 2012;54:303–12.
24. Andrades P, Militsakh O, Hanasono MM, Rieger J, Rosenthal
EL. Current strategies in reconstruction of maxillectomy defects.
Arch Otolaryngol 2011;137:806–12.
25. Frame RT, King GE. A surgical interim prosthesis. J Prodthet
Dent 1981;45:108–10.
26. Elameen MM. Quality of life of patients wearing maxillary
obturators [Master’s thesis]. Faculty of Dentistry: University of
Khartoum; 2014. p. 1–65.
27. Elhag SA. Level of dry mouth and its effect on the quality of life in
patients wearing maxillary obturator prostheses [Master’s the-
sis]. Faculty of Dentistry: University of Khartoum; 2014. p. 1–70.