max brinsmead mb bs phd may 2015. incidence, types and presentation affects 1:5 women in a lifetime...
TRANSCRIPT
Max Brinsmead MB BS PhDMay 2015
Incidence, Types and PresentationAffects 1:5 women in a lifetimeLichen sclerosis & atrophicus – 25%Lichen planusAssociated with other skin disease
Lichen simplex with dermatitisPsoriasis
PremalignantVulval wartsVulval intraepithelial neoplasia (VIN)
CandidiasisPresents with pruritis and or pain
Taking a HistoryRoutine gynaecological questionsAsk about urinary and bowel incontinenceAny other skin problems?Any other disorders
Especially auto immune diseaseImmune deficiency
Drugs and OTC preparationsSystemicLocal applicationsSmoking & other
Family HistoryAtopy i.e. eczema and allergies, asthma etc.Autoimmune disorders

Common Vulval Irritants
Excessive drying – use of talc etc.Topically applied deodorants, antiseptics , douches
etc.Soaps and detergentsSanitary pads, incontinence pads etc.Lubricants and rubber (condoms)DyesClose fitting clothes especially syntheticsItch and scratching, towel drying, nail polish etc.

Examination
Adequate exposureGood lightMagnification (colposcopy) not mandatoryLower genital tract, Pap and colposcopy
only for suspected VINExamine mouth, scalp, nails and all skin
Especially elbows and knees

InvestigationsExclude diabetes, hypothyroidism & iron
deficiencyGram stain and culture for CandidaTests for STDs when clinically indicatedAutoimmune tests after a diagnosis of
lichen sclerosis or planusBiopsy
Only for suspected VINOr failure to respond to treatmentCan be done with LA as an outpatient
Lichen sclerosis & atrophicusMore common in the postmenopausal
But it does not respond to hormones
Thickened, white skin = hyperkeratosisCauses intense pruritis
Worse at nightScratching leads to secondary skin damage
Other skin becomes atrophic causing stenosis, adhesions and scarring

Lichen sclerosis & atrophicus
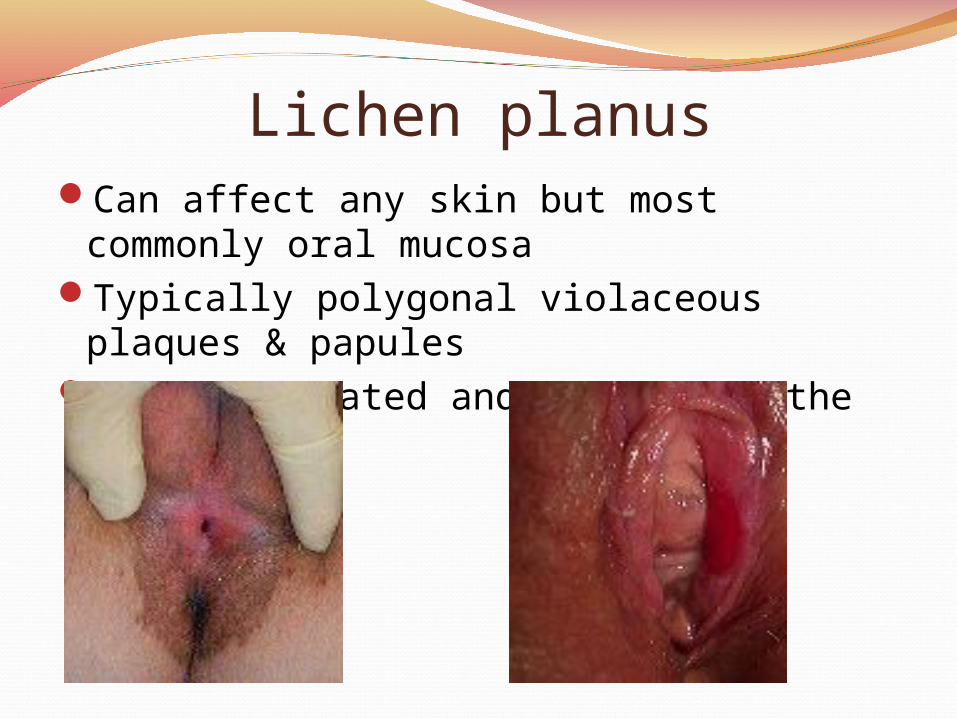
Lichen planusCan affect any skin but most commonly
oral mucosaTypically polygonal violaceous plaques &
papulesOften ulcerated and painful on the vulva
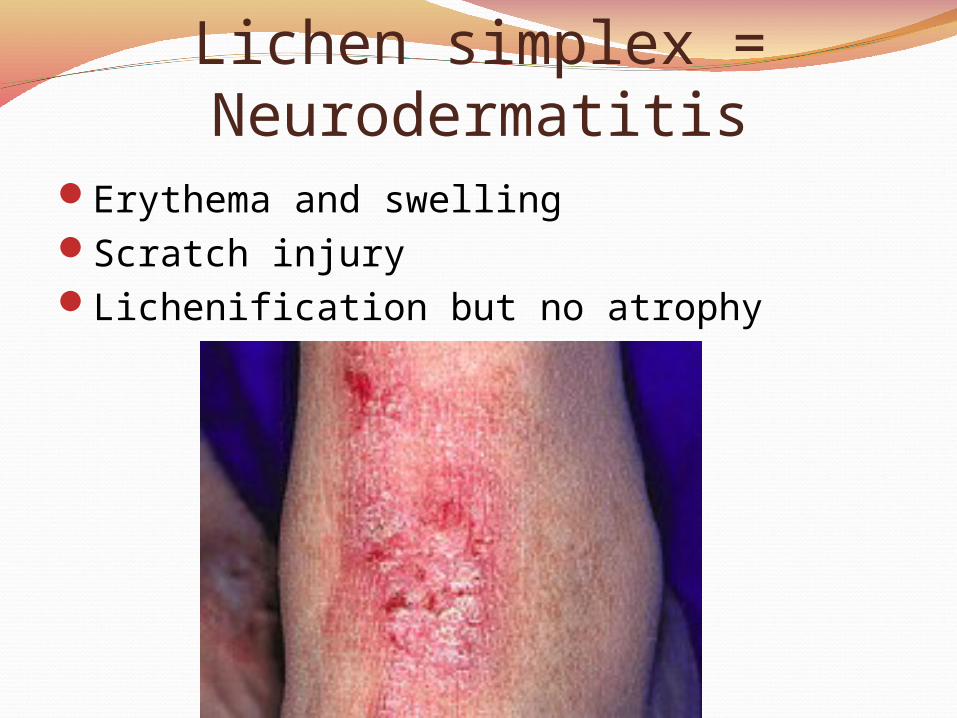
Lichen simplex = NeurodermatitisErythema and swellingScratch injuryLichenification but no atrophy
Vulval Intraepithelial Neoplasia
Comes in two forms:Warty excrescences
Commonly women <55 yearsAssociated with HPV – typically Type 16
Differentiated VINCommonly women >55About 5% of lichen sclerosis will have this as
wellProgresses more quickly to squamous carcinoma
Differential Diagnosis
Not all that important because the treatment for lichen sclerosis, planus and simplex with dermatitis is the same…
Potent topical corticosteroidsBiopsy anything that is clinically suspicious…
Has a raised edgeAbnormal vessels visibleHard to gentle palpation
Or does not respond to treatment

TreatmentGeneral measures to protect vulval skinPotent fluorinated corticosteroid applications
Advantan = MethylprednisoneDiprosone = Betamethasone propionateElocon = MometasoneClobetasol = the most potent available
Use ointment rather than creamProlonged use results in skin atrophy
Daily for a month2nd daily for a monthTwice weekly for a monthWeekly for a monthThen as required
A 30g tube should last 3 months
General Measures to Protect Vulval SkinShower rather than bathUse neutral soap substitutesHands only – no flannels or spongesPat or blow dry – no towellingUse water with inert emollient cream other timesWear loose fitting silk or cottonRemove underwaer whenever possibleWash clothes in neutral soap or gel - avoid all
biological (enzymes) detergents and bleaches Avoid dyes – in dark clothes & toilet paperMinimal use of vulval pads of any typeAvoid all OTC applicationsKeep aqueous cream in the fridge for soothing

Treatment (2)About 10% fail to respond to topical
corticosteroidsTopical Tacrolimus, an immunodifier , is a second
line treatment for lichen sclerosisUsually occurs with supervision from a Dermatlogy
ClinicBecause there is a small risk of malignant
transformationWarts can be treated with Imiquimod cream =
Aldara15 – 80% response rateCompliance is an issue
Some 15% of VIN will have unrecognised invasive disease disclosed by excision biopsy
Follow Up
40 – 60% 0f VIN progresses to Ca over 8+ yearsCan be reduced to <5% by adequate biopsy
excisionAnd reconstructive surgery when requiredFollow up with colposcopy and cytologyAnd encourage self examinationRelapse of lichen sclerosis is common
Up to 80% within 4 yearsBut it has a much smaller potential for malignant
change so follow up can be with a GP

Some Rare Vulval LesionsBeçhet’s Disease
Recurrent oral and genital ulcers
Extramammary Paget’s DiseaseFlorid eczema and lichenificationBiopsy to exclude underlying adenoCa & look for
primary in breasts, GI or urinary tracts
Zoon’s VulvitisInfiltrated with plasma cells and haemosiderin
Vulval Crohn’s DiseaseGranulomas, abscess, ulcers and sinusesUsually associated with small gut pathology
Recurrent CandidiasisFirst confirm the diagnosis
Requires swab and culture >48 hrs after fungicidal application
Exclude imidazole-resistant organismsThis requires the use of borates for treatment
Exclude diabetesAvoid broad spectrum antibiotics
Recolonization of vaginal Acidophilus with natural yoghurt?
Use systemic antifungal = Oral DiflucanMost respond to recurrent and intermittent
Imidazole Use Canesten PRN
There are many “natural therapies” Try Tea Tree oil (Melaleuca alterniflora) 2 -3 drops in
sweet almond oil on a tampon 8-hourlyThere may be a role for immune boosting by
transfusions with Transfer Factor

Please leave a note on the Welcome Page to this website