maternal pregnancy complications
TRANSCRIPT
Maternal Pregnancy ComplicationsJason Ryan, MD, MPH
• Nausea and/or vomiting common in early pregnancy • Mild cases: “morning sickness”• Severe cases: hyperemesis gravidarum
• Vomiting causing hypovolemia• May lead to weight loss
• Check electrolytes and urinalysis• May see alkalosis or hypokalemia• Urinary ketones may be present
Hyperemesis Gravidarum
Shutterstock
• Intravenous fluids• Thiamine
• Rare cases of maternal Wernicke’s encephalopathy reported
• Correct magnesium, calcium and phosphorus if low
Hyperemesis GravidarumTreatment
• Lifestyle changes• Eat when hungry – avoid empty stomach• Avoid triggers: odors, lying down after eating
• Usual first-line medical treatment: doxylamine-pyridoxine• Doxylamine: anti-histamine• Pyridoxine: vitamin B6 (improves nausea through unknown mechanism)
• Severe cases: other antihistamines, dopamine agonists, ondansetron
Hyperemesis GravidarumTreatment
Diabetes in Pregnancy
• Pregnancy is an insulin-resistant state• Decreased maternal response to insulin• Diabetes mellitus: worsened by pregnancy• Gestational diabetes: onset of diabetes during pregnancy• May adversely affect fetus• Screening with serum glucose testing• Glycosuria occurs in normal pregnancy• Hemoglobin A1c limited use in pregnancy
Zapyon/Wikipedia
C-peptide
α chain
β chain
Insulin
Diabetes in PregnancyAdverse effects
• Many potential adverse effects for mother and baby• Large for gestational age• Macrosomia • Birth trauma (shoulder dystocia)• Cesarean delivery• Polyhydramnios• Spontaneous abortion or stillbirth• Preeclampsia • Neonatal hypoglycemia
Shutterstock
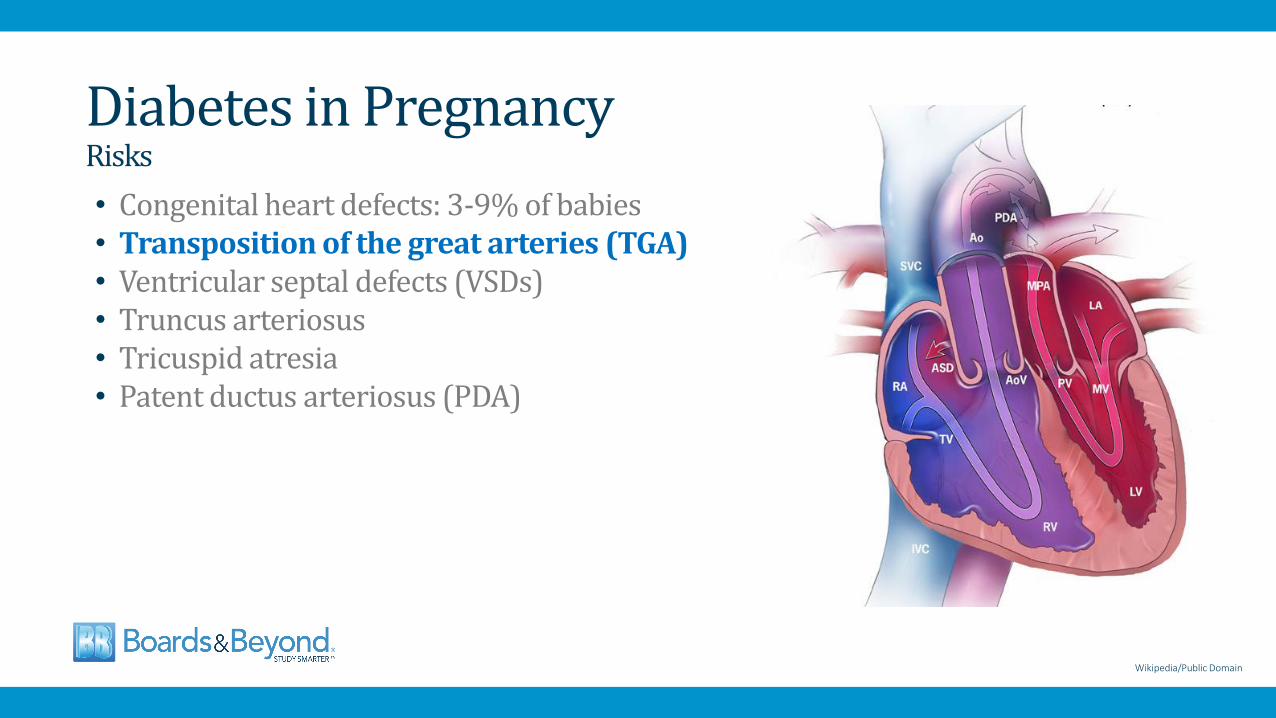
Diabetes in PregnancyRisks
• Congenital heart defects: 3-9% of babies• Transposition of the great arteries (TGA)• Ventricular septal defects (VSDs)• Truncus arteriosus• Tricuspid atresia• Patent ductus arteriosus (PDA)
Wikipedia/Public Domain
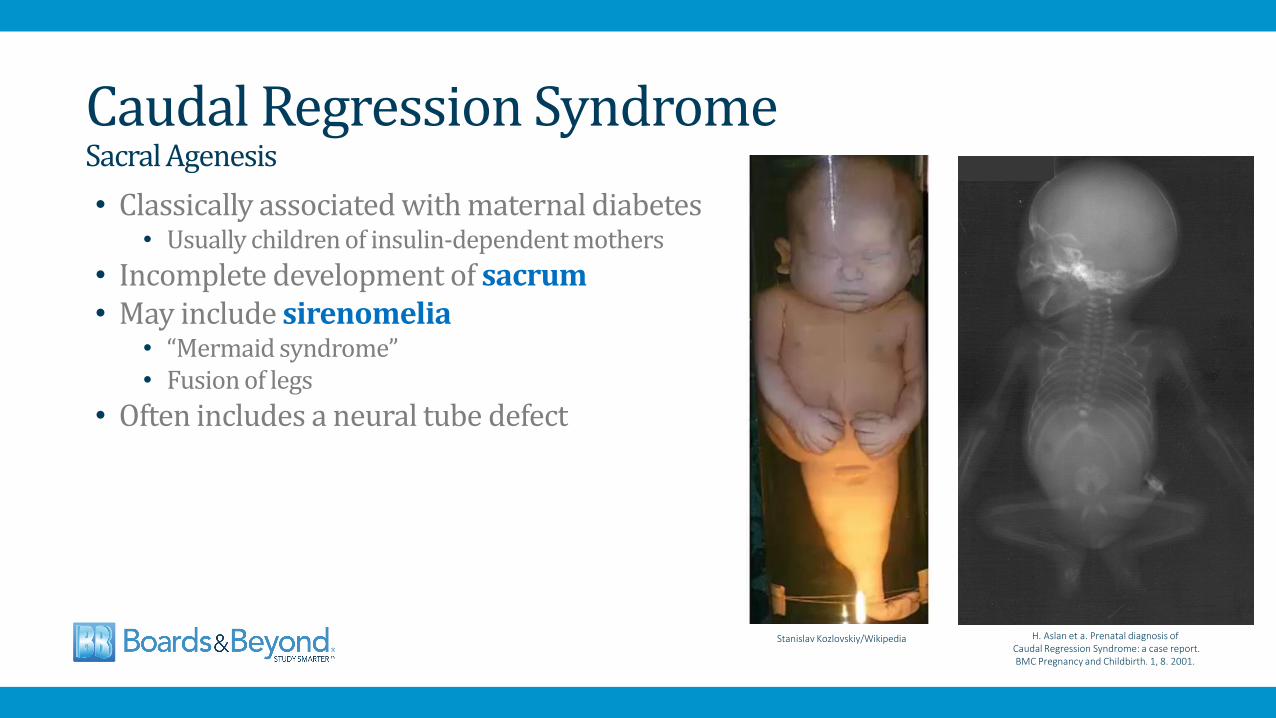
Caudal Regression SyndromeSacral Agenesis
• Classically associated with maternal diabetes• Usually children of insulin-dependent mothers
• Incomplete development of sacrum• May include sirenomelia
• “Mermaid syndrome”• Fusion of legs
• Often includes a neural tube defect
H. Aslan et a. Prenatal diagnosis ofCaudal Regression Syndrome: a case report. BMC Pregnancy and Childbirth. 1, 8. 2001.
Stanislav Kozlovskiy/Wikipedia
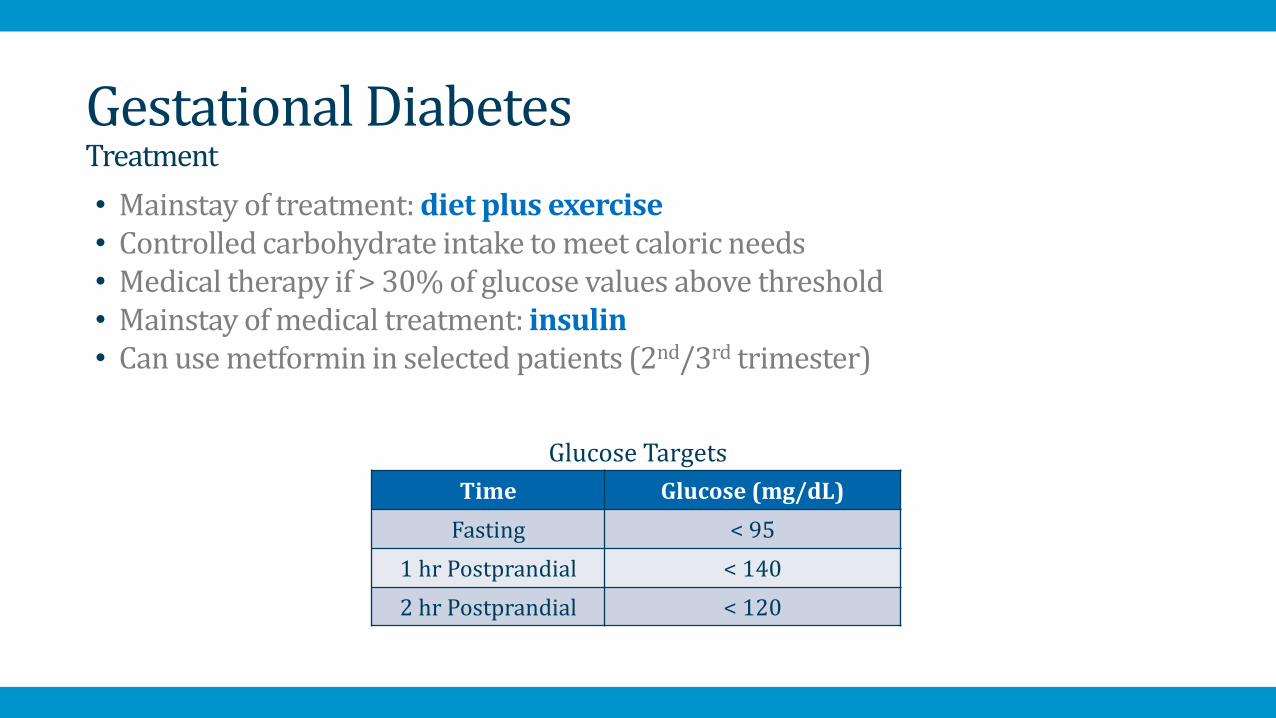
• Mainstay of treatment: diet plus exercise• Controlled carbohydrate intake to meet caloric needs• Medical therapy if > 30% of glucose values above threshold• Mainstay of medical treatment: insulin• Can use metformin in selected patients (2nd/3rd trimester)
Gestational DiabetesTreatment
Time Glucose (mg/dL)
Fasting < 95
1 hr Postprandial < 140
2 hr Postprandial < 120
Glucose Targets
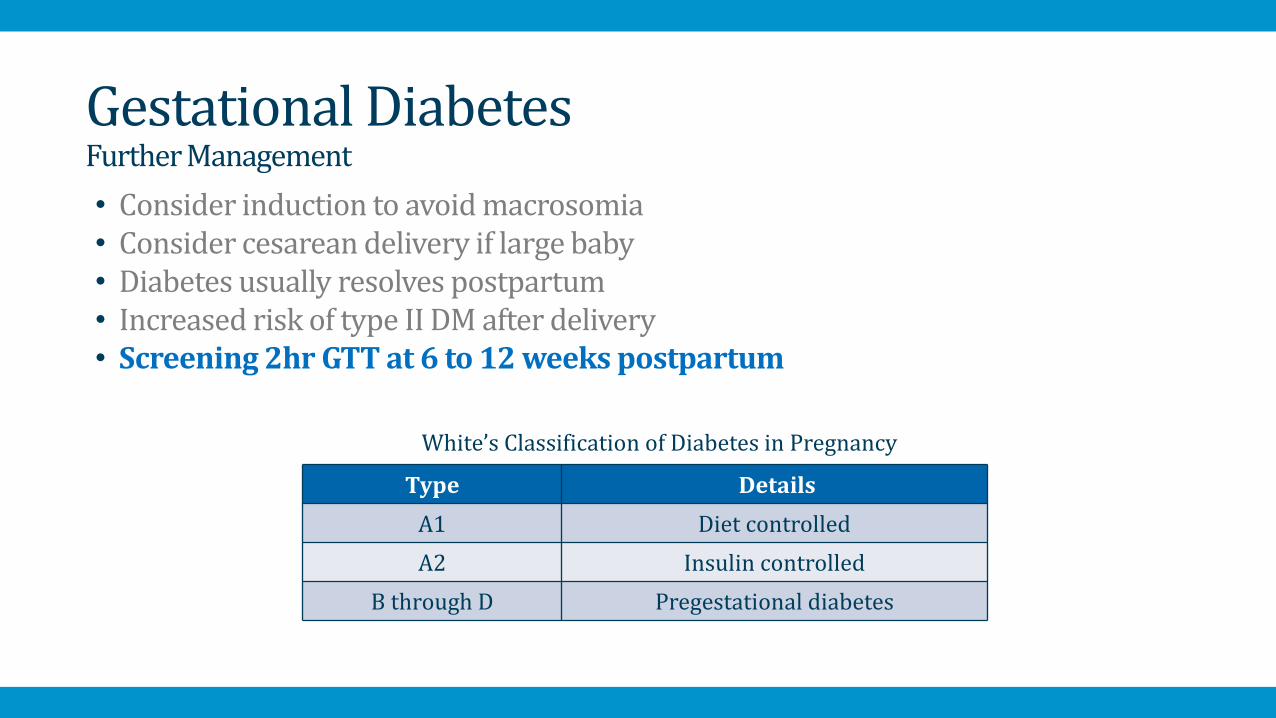
• Consider induction to avoid macrosomia • Consider cesarean delivery if large baby• Diabetes usually resolves postpartum • Increased risk of type II DM after delivery• Screening 2hr GTT at 6 to 12 weeks postpartum
Gestational DiabetesFurther Management
Type Details
A1 Diet controlled
A2 Insulin controlled
B through D Pregestational diabetes
White’s Classification of Diabetes in Pregnancy
• Rare cause of acute liver failure in 3rd trimester of pregnancy• Fatty infiltration of hepatocytes• Classic presentation: persistent nausea and vomiting• Other features: jaundice or encephalopathy• Abnormal labs: LFTs, bilirubin• Treatment: immediate delivery plus supportive care
• Progression of pregnancy may lead to fulminant liver failure
• Most cases recover after delivery
Acute Fatty Liver of Pregnancy
Shutterstock
• Diffuse pruritus with elevated serum bile acids• Occurs in 2nd half of pregnancy due to unknown cause• Diagnosis: ↑ serum total bile acids• Mild abnormalities LFTs or bilirubin • Treatment: ursodeoxycholic acid • Risk to fetus: fetal demise, preterm delivery • Deliver at term
Intrahepatic Cholestasis of Pregnancy
Shutterstock
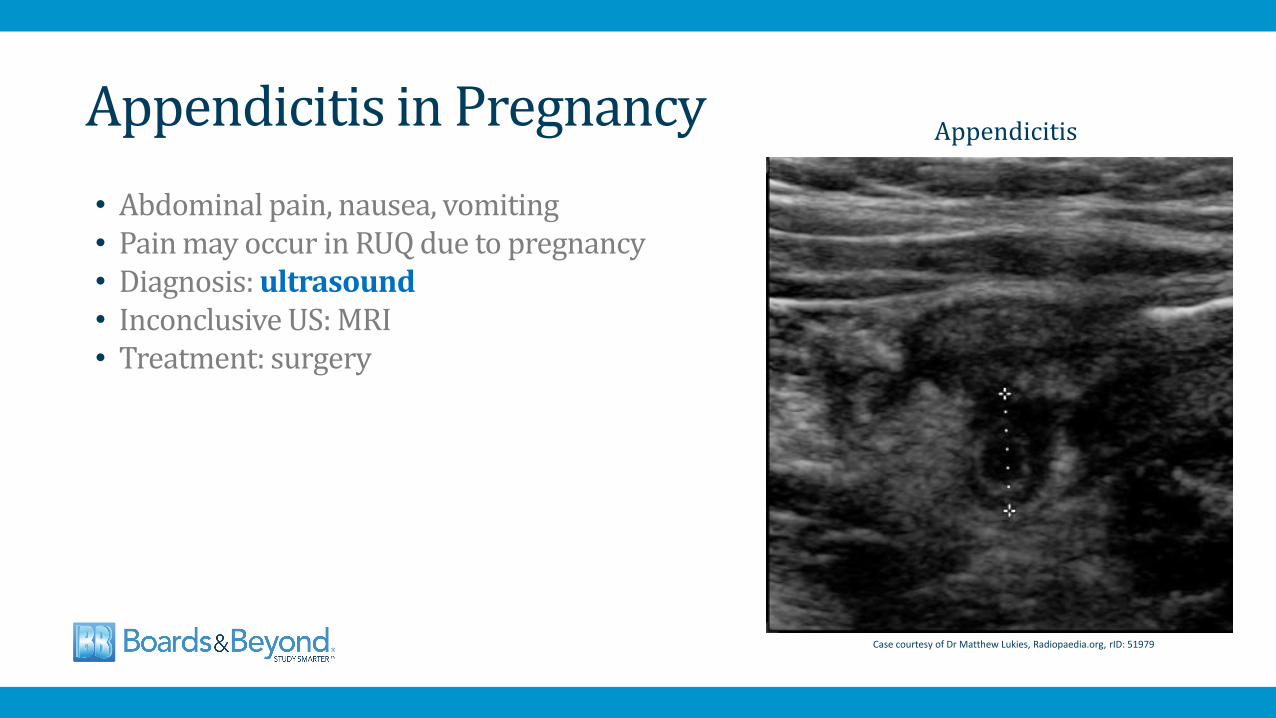
• Abdominal pain, nausea, vomiting• Pain may occur in RUQ due to pregnancy• Diagnosis: ultrasound • Inconclusive US: MRI• Treatment: surgery
Appendicitis in Pregnancy
Case courtesy of Dr Matthew Lukies, Radiopaedia.org, rID: 51979
Appendicitis
• Progesterone → urinary stasis• Relaxation of smooth muscle in urinary tract• Asymptomatic bacteriuria, cystitis, or pyelonephritis• Most common bacteria: E. coli• Others: S. saprophyticus, GBS, enterococcus
Urinary Infections
Public Domain
E. Coli
• Asymptomatic bacteriuria • Screening at first prenatal visit with urine culture• High risk of pyelonephritis and preterm birth• Treat positive culture with antibiotics for 7 days• Drug choice based on bacteria sensitivity• Up to 30% do not clear bacteriuria after antibiotics• Repeat culture is usually done for test of cure
• Acute cystitis: empiric antibiotics• Nitrofurantoin• Fosfomycin • Modify when culture results available
Urinary Infections
Wikipedia/Public Domain
• Pyelonephritis• Occurs in 2% of pregnancies• Common indication for hospitalization
• Treatment:• IV fluids• Parenteral, broad spectrum antibiotics• Ceftriaxone, Cefepime, ampicillin-gentamicin
• Recurrence common• Suppressive antibiotics often used until delivery
Urinary Infections
Shutterstock
• Hyperthyroidism or hypothyroidism may complicate pregnancy• Routine screening not recommended• Hyperemesis gravidum
• Associated with high hCG→ stimulates thyroid• Low TSH and possibly high T4• Thyroid studies avoided in HG patients
Thyroid Disease
Shutterstock