marko turina - policlinico di monza · techniques of optimization of the clinical conditions of...
TRANSCRIPT
TECHNIQUES OF OPTIMIZATION OF THE CLINICAL CONDITIONS OF PATIENTS IN
VIEW OF RECOVERY, TRANSPLANATION, AND/OR DESTINATION THERAPY
MARKO TURINA University Hospital Zurich, Switzerland

Copyright ©2001 The Society of Thoracic Surgeons
Beyersdorf, F.; Ann Thorac Surg 2001;71:192S-194S
Health Care Financing Administration (HCFA) expenditure on heart failure compared with that for cancer and myocardial infarction, according to Medicare in 1991

Optimization of the Patient’s Condition Some introductory statements
• Surgeons are not the primary specialists treating a patient in profound heart failure (except in posto-perative low output syndrome): these are the cardiologist in their ICU.
• Exact diagnosis (although sometimes difficult in cardiogenic shock) is the first, essential part of the decision-making process: insist on echocardio-graphy, coronary angiography, vascular and abdominal ultrasound.
• Effectiveness of non-surgical stabilization (correc-tion of blood chemistry, catecholamines, optimi-zation of PVR, ventilation & oxygenation, haemo-filtration etc.) must be carefully assessed.
SEVERE HEART FAILURE IN NEED OF CIRCULATORY ASSISTANCE
Most common conditions encountered (postoperative LOS excluded)
• Terminal myocardiopathy • End-stage coronary artery disease • Myocarditis • End-stage valvular heart disease • Late-stage congenital heart malformations • Rare conditions: Arrhythmogenic dysplasia,
Uhl’s disease, amyloidosis

HEART TRANSPLANTATION Indications, Zurich 1985-1998
Other indications: • Uhl’s disease • Heart tumors • Amyloidosis • Endomyocardial
fibrosis • Non-compaction
CMP46%
CAD37%
Congenital6%
Valvar6%
Other3%
Pulmonary1% Re-TX
1%

PULMONARY ARTERY CATHETER Obligatory when evaluating patients in heart failure
Full ICU monitoring before any surgical decision!

Checklist For Surgical Consultation In Patients With Profound Heart Failure
• Pharmacologic stabilization (CO, PVR) with preload and afterload adjustment, catecholamines, beta-blockers, ACE and PDE inhibitors, NO, etc.
• Heart rate and rhythm control in tachycardia and in atrial fibrillation.
• Correction of blood chemistry: pH correction, continuous i-v insulin to achieve normoglycaemia, haematocrit elevation to ~ 35%, haemofiltration for control of blood volume and normalization of creatinin and urea.
• Optimization of oxygen delivery (ventilator?) • Resynchronization therapy in cardiomyopathy? • PCI and stenting in coronary ischemia?

Recently elucidated mechanisms of heart failure: advent of molecular biology

Phosphodiesterase Inhibitor (“The Intelligent Drug”): mechanism of action

Reliable TEE, performed by an expert, with a modern machine, is an absolute must in preoperative evaluation

And it can show some previously unsuspected, essential details!
Apical thrombus
ASD

IABP should be used early, to facilitate the myocardial recovery

Diastolic Augmentation ↑ Coronary Perfusion
Assisted Aortic End- Diastolic Pressure ↓ MVO2 Demand
Assisted Systole
Unassisted Systole
Balloon Inflation
Unassisted Aortic End-Diastolic
Pressure
140
120
100
80
60
mm Hg
Arterial Waveform Variations During IABP Therapy: Insist On Optimal Timing!
© Datascope Corp.
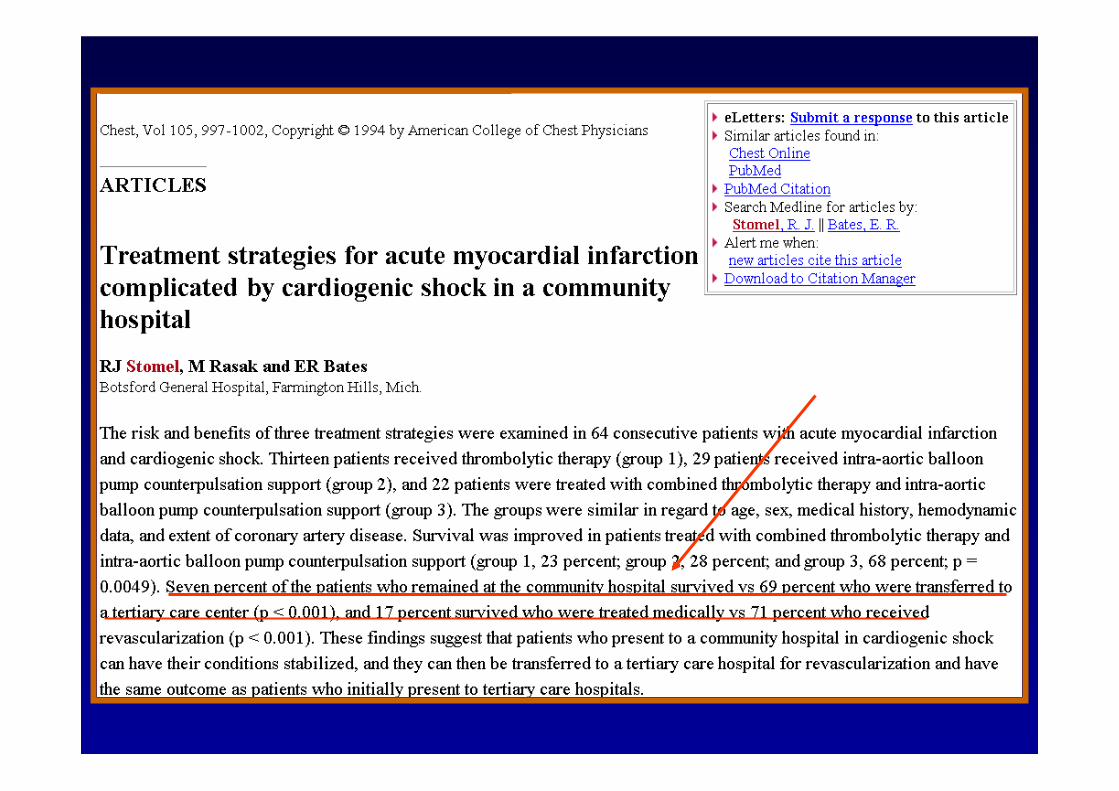

Acute MI and Cardiogenic Shock
23%28%
68%
010203040506070
%
Group I Group II Group III
Survival Rates for AMI and Cardiogenic Shock
Stomel, R, et al; Chest 1994; 105(4):997-1002

PRESENT USE OF IABP
• Unstable angina and acute coronary syndromes
• Preoperative stabilization (heart failure and acute coronaries)
• Postoperative low output syndrome Drawbacks: cannot be used with
incompetent aortic valve; in aorto-iliac disease; ineffective in children; poor efficiency in high-output failure with low PVR.

Resynchronization in heart failure: searching for reduction in QRS width and improvement of dyssynchrony of the LV

Overview of resynchronization trials

Biventricular Resynchronization Pacing In Severe Heart Failure
Caveats
• Inefficient in many heart failure patients. • Difficult placement and poor stability of LV
electrodes. • Need for additional defibrillator (pro-
arrhythmogenic effect of synchronization) • Both QRS width reduction and improvement of LV
dyssynchrony must be demonstrated in echocardiography.
• Effect is not immediate: there can be a delay in clinical improvement.

Quiet revolution in ICU: continuous haemofiltration

SEVERE HEART FAILURE IN NEED OF CIRCULATORY ASSISTANCE
Which direction to take?
• Recovery: very rare, possible in loose indications for LVAD, in acute viral myocarditis and in postop. LOS.
• Destination therapy: contraindications for heart TX (age >70 y; low grade malignancy; chronic rejection; high antibody levels; etc.)
• Bridge to TX: presently a large majority; all patients without heart recovery after 6 -8 weeks.

HEART TRANSPLANTATION Kaplan-Meier Survival (1/1982-6/2003)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Years
Surv
ival
(%)
.
Half-life = 9.6 yearsConditional Half-life = 12 years
N=66,751
ISHLT 2005
N followed at longest time point: 25,908
J Heart Lung Transplant 2005;24: 945-982

NUMBER OF HEART TRANSPLANTS REPORTED BY YEAR
ISHLT 2005
NOTE: This figure includes only the heart transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as evidence that the number of hearts transplanted worldwide has declined in recent years.
J Heart Lung Transplant 2005;24: 945-982

ELECTRICALLY DRIVEN LVAD Novacor device

THE NASA DE BAKEY LVADTM
OUTFLOW GRAFT
LVAD
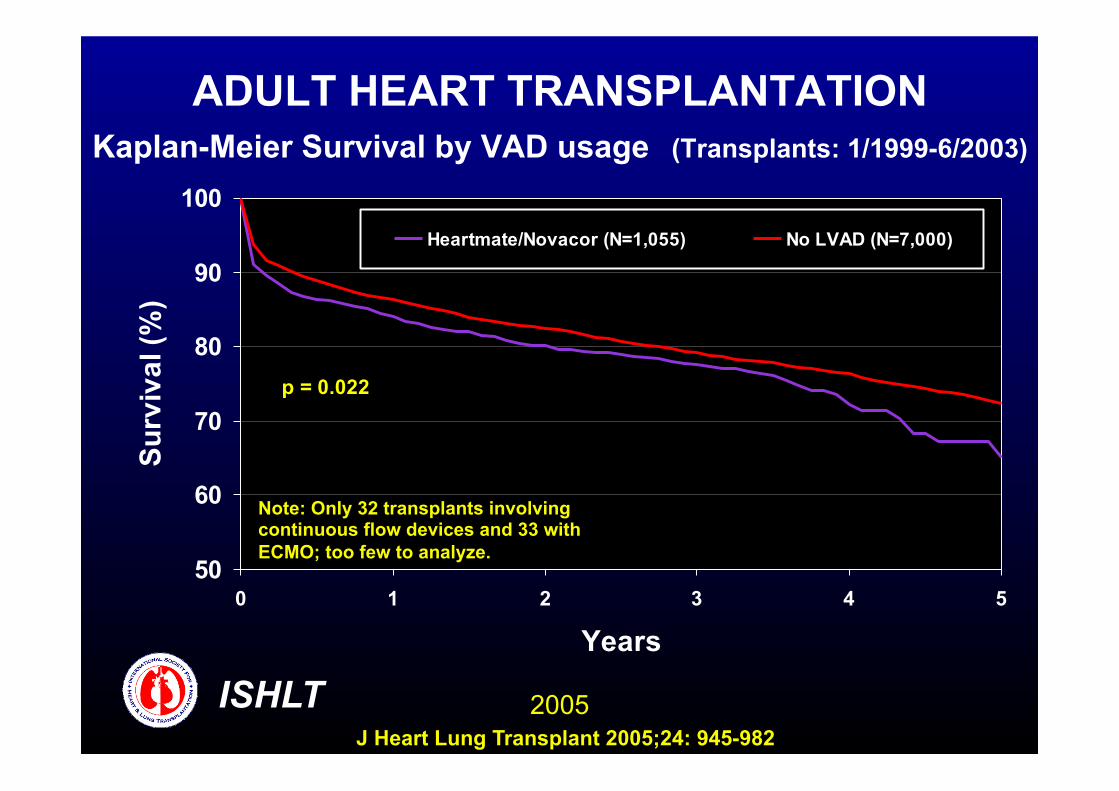
ADULT HEART TRANSPLANTATION Kaplan-Meier Survival by VAD usage (Transplants: 1/1999-6/2003)
50
60
70
80
90
100
0 1 2 3 4 5
Years
Surv
ival
(%)
Heartmate/Novacor (N=1,055) No LVAD (N=7,000)
p = 0.022
ISHLT 2005
Note: Only 32 transplants involving continuous flow devices and 33 with ECMO; too few to analyze.
J Heart Lung Transplant 2005;24: 945-982

Prolonged assist with LVAD is essential for normalization of patient’s condition


MECHANICAL CIRCULATORY ASSISTANCE AS BRIDGE TO TRANSPLANTATION
Meta-analysis: odds ratio for non-survival


Heart Transplantation: Age of recipient as the determinant of survival
Heidelberg Databank, 2000 (Prof. Opelz)


ELECTRICALLY DRIVEN LVAD

MICROMED LVAD ACTION

Patient in massive heart failure When should one abstain from active surgical help?
• Profound vasoplegia in spite of adequate
pharmacologic support and pH correction. • Septic shock not responding to antibiotics. • Cirrhosis Childs A or higher. • Multiple organ failure • Massive cerebrovascular incident or intracranial
bleeding (anticoagulation not possible). • End stage malignancy. • Established dementia (Alzheimer, cerebro-
vascular disorder). • Known patient’s objection (“living will”).