maria e. suarez-almazor, md, phd houston certs using decision aids to enhance shared-decision making
TRANSCRIPT
Maria E. Suarez-Almazor, MD, PhD
Houston CERTs
Using Decision Aids to Enhance Shared-Decision Making
Outline
Overview of decision aids Examples Methods for development Evidence Controversies

Overview
Health Decisions
Good decisions– Informed– Supported by best
evidence– Compatible with patients
values– Considers patients
preferences– Weigh pros and cons– Practical
Poor decisions– Objective data inadequate– Too few options
considered– Alternatives unclear– Values and preferences
unexplored– Roles unclear– Communication is poor
Cornelia Rulandhttp://www.dbmi.columbia.edu/homepages/cmr7001/sdm/html/decision_support.htm

Informed Decision Making
When an individual:1. Understands nature of condition (core knowledge)
2. Understands service, including risks, limitations, benefits, alternatives, uncertainties (core knowledge)
3. Considers preferences and values (values)
4. Chooses desired level of participation in decision (role preferences)
5. Makes (or defers) a decision based on his/her preferences and values (values-based decision)
Briss et al Am J Prev Med 2004

Shared Decision Making
Involvement of patients with their providers in making health care decisions that are informed by the best available evidence about options, potential benefits, and harms, and that consider patient preferences.

Shared Decision Making
2+ participants– Provider– Patient
Information is shared– Knowledge (provider)– Values and preferences (patients)
Participants build consensus Agreement is reached

IDM: Any intervention in communities or healthcare systems intended to promote informed decisions
SDM: The subset of informed decision making interventions that are carried out between one patient and his/her healthcare provider(s) in clinical settings
Briss et al Am J Prev Med 2004.Sheridan et al., Am J Prev Med 2004.
Informed Decision Making vs. Shared Decision Making

Decision Aids
Patient decision aids are tools designed to help people participate in decision making about health care options.
They provide information on the options and help patients clarify and communicate the personal value they associate with different features of the options
International Patient Decision Aids Standards (IPDAS)

Why?
Many decisions have no ‘best choice’ – more than one appropriate option
Evidence uncertain Need to consider
– benefits and harms– values & preferences– practical aspects
Time constraints during medical encounter
Decision Aids
Designed to– Provide information on
options– Help people participate
in decision making– Help clarify and
communicate personal values
NOT designed to– Advise people to choose
one option over another– Not meant to replace
physician consultation
Cornelia Rulandhttp://www.dbmi.columbia.edu/homepages/cmr7001/sdm/html/decision_support.htm
PREPARE PATIENTS TO MAKE INFORMED, VALUES-BASED DECISIONS
WITH THEIR PHYSICIANS
Examples
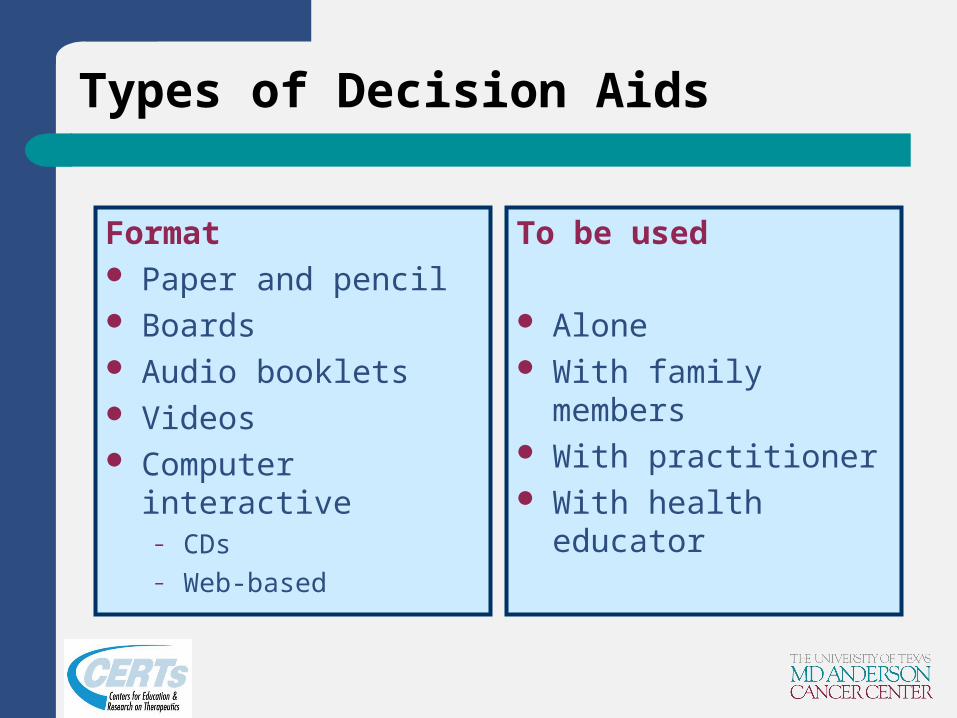
Types of Decision Aids
Format Paper and pencil Boards Audio booklets Videos Computer interactive
– CDs– Web-based
To be used
Alone With family members With practitioner With health educator
Gossey T & Volk R




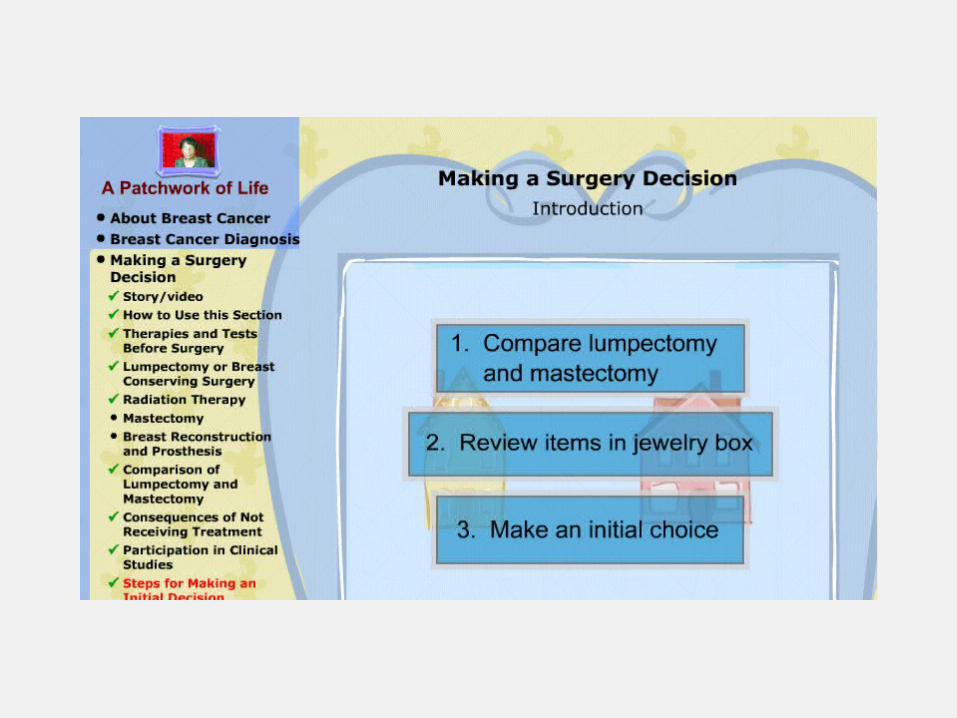
Jibaja-Weiss, Mhttp://www.bcm.edu/patchworkoflife/homepage_en.htm





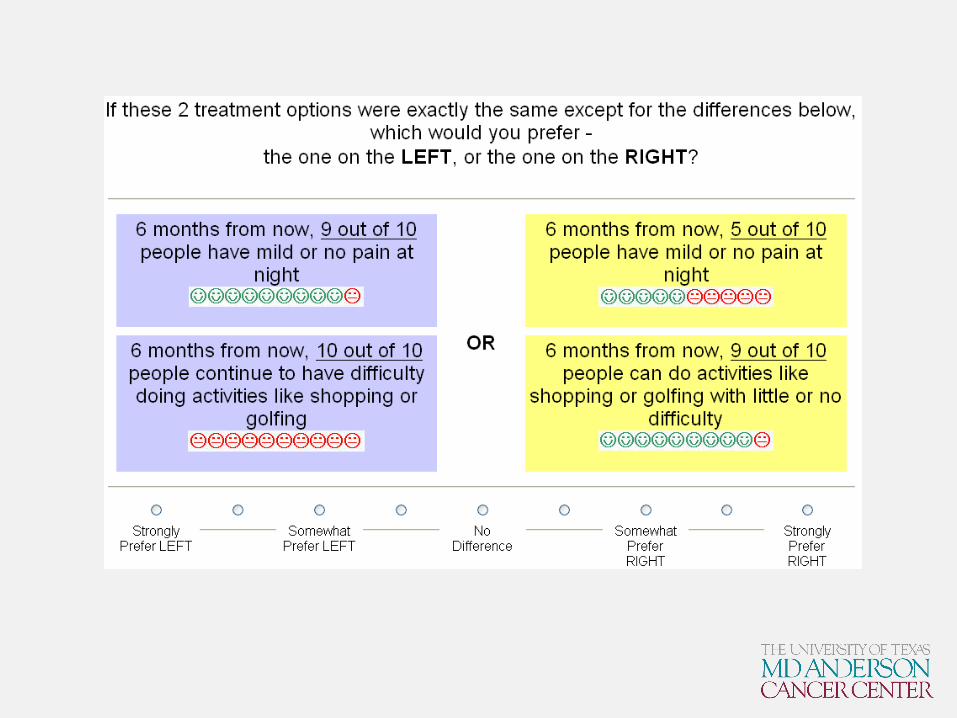
Adaptive Conjoint Analysis
Computer-administered, interactive conjoint method Situations with large number of attributes Exceeds what can reasonably done with other methods Asks respondents to choose between 2 scenarios The scenarios and attributes vary with each screen Avoids information overload by focusing on just a few
attributes at a time Focuses on the attributes that are most relevant to the
respondent

Total Knee Replacement
Surgery vs. no surgery Attributes
– Pain– Function– Complications– Mortality– Surgical revisions– Physical therapy

http://www.sawtoothsoftware.com/products/ssiweb/ssiweb_capi.shtml


Methods

IPDAS
International Patient Decision Aids Standards Collaboration
http://ipdas.ohri.ca/ Over 100 participants from 14 countries Glyn Elwyn, Annette O’Connor, Dawn Stacey, Robert Volk
and others ‘Developing a quality criteria framework for patient
decision aids: online international Delphi consensus process’. BMJ 2006;333:417

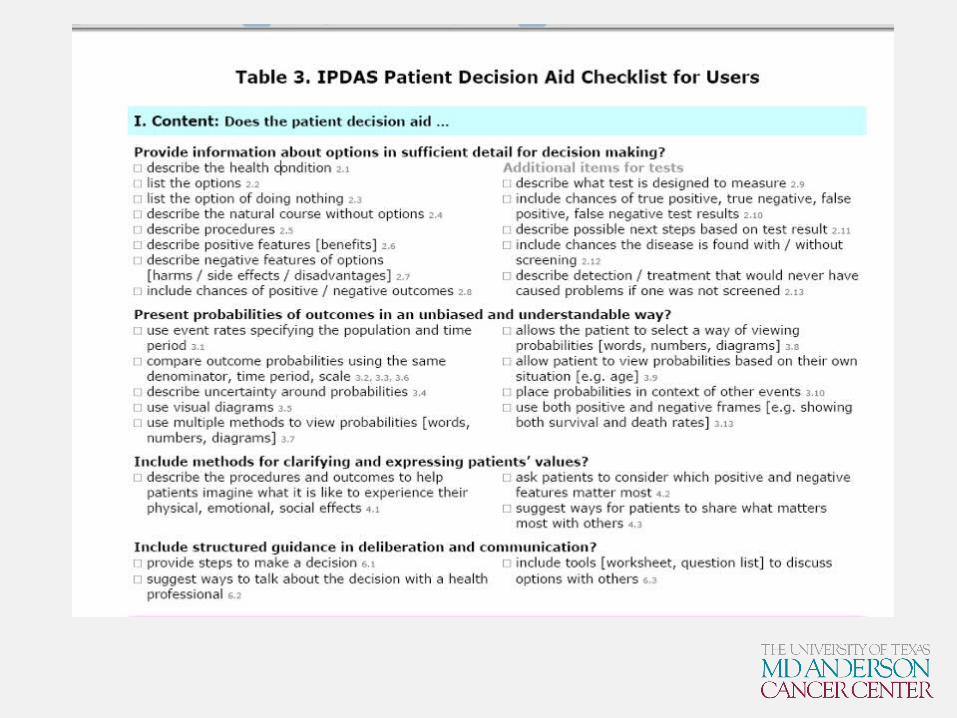
IPDAS criteria for judging the quality of decision aids – checklist
Content
Development Process
Effectiveness

Content -- Decision aid…..
Provides information about options in sufficient detail
Presents probabilities of outcomes in an unbised and understandable way
Includes methods for clarifying and expressing patients’ values
Include structured guidance in deliberation and communication
Development process – Decision aid…
Presents information in a balanced manner Has a systematic development process Uses up-to-date evidence (cited) Discloses conflict of interes Uses plain language Additional criteria to be met if decision aid is:
– Internet-based– Uses stories

Effectiveness (1) – Decision aid….
DECISION
Improves the match between the chosen option and the features that matter most to the informed patient.

DECISION PROCESSHelps patients: recognize that a decision needs to be made know options and their features understand that values affect the decision be clear about the option features that matter
most discuss values with their practitioner become involved in preferred ways.
Effectiveness (2) -- Decision aid….
O'Connor A. Cochrane Collaboration 2009

Evidence

Cochrane Systematic Review
Last update 2006 55 RCTs Comparison to usual care ‘True’ decisions – not hypothetical Excluded ‘education only’ programs not leading
to a decision Mapping to IPDAS criteria
O’Connor et al., Cochrane Library, 2009

Primary outcomes (IPDAS criteria)
Attributes of decision Attributes of decision making process Other decision making process variables
• Decisional conflict• Patient practitioner communication• Participation in decision making• Satisfaction
Behaviour• Decisions (proportion undecided, option selected).• Adherence to chosen option.
Health outcomes• Health status and quality of life (generic and conditionspecific).• Anxiety, depression, emotional distress, regret, confidence.
Healthcare system• Patients’ and physicians’ satisfaction.• Costs, cost effectiveness.• Consultation length.• Litigation rates.
Secondary outcomes (IPDAS criteria)

Results
Decision aids performed better in terms of:– Greater knowledge (MD 15.2 out of 100)– Lower decisional conflict related to feeling
uninformed (MD -8.3 out of 100)– Lower decisional conflict related to feeling unclear
about personal values (MD -6.4– Reduced the proportion of people who were passive
in decision making (RR 0.6)– Reduced proportion of people who remained
undecided post-intervention (RR 0.5)
Results
Higher proportion of people with accurate risk perceptions (RR 1.6)
Reduced rates of: elective invasive surgery in favour of conservative options (RR 0.8)
Reduced use of menopausal hormones (RR 0.7) Reduced PSA screening (RR:0.8)

Results
Decision aids were no better for: – Satisfaction with decision making– Anxiety– Health outcomes
Inconclusive:– Patient-practitioner communication– Consultation length– Continuance– Resource use

Controversies

Controversies
Patient-practitioner communication Effects on health outcomes Uncertainty is real – decisional conflict should
not be avoided Best decisions based on ‘gist’ ‘Loaded’ choices

Acknowledgements
Robert Volk Maria Jibaja-Weiss Travis Gossey Carol Looney Liana Frankel Annette O’Connor Rick Street
