manuscript draft - the faculty of mathematics and …dannyh/downloads/preprint_bodyimag… ·...
TRANSCRIPT

Elsevier Editorial System(tm) for Body Image: An International Journal of Research Manuscript Draft Manuscript Number: Title: Computerized Assessment of Body Image in Anorexia Nervosa and Bulimia Nervosa: Comparison with Standardized Body Image Assessment Tools Article Type: Full Length Research Article Keywords: anorexia nervosa; bulimia nervosa; eating disorder; body image; body image assessment software. Corresponding Author: Dr. Efrat Czerniak, Corresponding Author's Institution: First Author: Asaf Caspi, MD Order of Authors: Asaf Caspi, MD; Revital Amiaz, MD; Noa Davidson, MA; Efrat Czerniak; Eitan Gur, MD; Nahum Kiryati, PhD; Daniel Harari, PhD; Miriam Furst, PhD; Daniel Stein, MD Abstract: Body image disturbances are a prominent feature of eating disorders (EDs). Our aim was to validate a new computerized assessment of body image (CABI), simulating changes in one's own image, For this purpose we administered the Contour Drawing Rating Scale (CDRS), the CABI and the Eating Disorder Inventory-2-Body Dissatisfaction Scale to 22 inpatients with restricting anorexia nervosa (AN), 22 with binge/purge AN, 20 with bulimia nervosa (BN), and 41 healthy controls. All three scales differentiated patients with EDs from controls. Nonetheless, patients with AN and controls were more disturbed than those with BN on the CDRS, whereas a greater disturbance on some CABI dimensions was shown in patients with AN vs. BN. Our findings support the validity of the CABI in the comparison of body image disturbances in patients with EDs, and allow for better understanding of the differences in body image disturbances in different types of EDs.

Covering letter
Computerized Assessment of Body Image in Anorexia Nervosa and Bulimia
Nervosa: Comparison with Standardized Body Image Assessment Tools
Authors:
Asaf Caspi1,2
, MD [email protected]
Revital Amiaz1,2
, MD [email protected]
Noa Davidson3, MA [email protected]
Efrat Czerniak1,2
, MSc [email protected]
Eitan Gur4, MD [email protected]
Nahum Kiryati5, PhD [email protected]
Daniel Harari5, PhD [email protected]
Miriam Furst5, PhD [email protected]
Daniel Stein2,6
*, MD [email protected]
The first two authors equally contributed to the writing of the manuscript
Affiliations:
1 Department of Psychiatry, The Chaim Sheba Medical Center, Tel Hashomer, Israel
2 Sackler Faculty of Medicine, Tel Aviv University, Israel
3 Department of
Psychology, The Hebrew University of Jerusalem, Israel
4The Eating Disorders Department, The Chaim Sheba Medical Center, Tel Hashomer, ,
Israel
5 Electrical Engineering-Systems Department, Faculty of Engineering, Tel-Aviv
University, Israel
6 Pediatric Psychosomatic Department, The Edmond and Lily Safra Children’s Hospital,
The Chaim Sheba Medical Center, Tel Hashomer, Israel
*Corresponding author: Prof. Daniel Stein
Tel: 972-3-5302690 Fax:972-3-5305129 Email: [email protected]
*Title Page (including all author details)

Highlights
Applying a computerized self-image tool to assess body image disturbances in
ED patients.
Comparing it to standardized verbal-affective and perceptual tools.
This computerized tool may be more sensitive in the assessment of body
image in EDs.
Multimodal research strategy enables better understanding of body-image
disturbances.
*Highlights (for review)

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
1
Computerized Assessment of Body Image in Anorexia Nervosa and Bulimia Nervosa:
Comparison with Standardized Body Image Assessment Tools
Dysfunctional body image represents a core feature of both anorexia nervosa (AN)
and bulimia nervosa (BN) (Cash & Deagle, 1997; J. K. Thompson, 1997; Tovee, Benson,
Emery, Mason, & Cohen-Tovee, 2003). Thus, prospective longitudinal studies have shown
that the severity of body-image disturbance is a powerful predictor for the development of
eating-related disturbances in adolescent (Leon, Fulkerson, Perry, & Early-Zald, 1995) and
adult females (Striegel-Moore, Silberstein, Frensch, & Rodin, 1989), for an overall
unfavorable prognosis in the course of AN (Smith, Feldman, Nasserbakht, & Steiner, 1993)
and BN (Trentowska, Bender, & Tuschen-Caffier, 2013), and for the likelihood of relapse in
recovered patients with AN (Keel, Dorer, Franko, Jackson, & Herzog, 2005; Skrzypek,
Wehmeier, & Remschmidt, 2001) and BN (Fairburn, Peveler, Jones, Hope, & Doll, 1993).
An intricate interplay of multi-faceted factors may account for the disturbed body
image seen in patients with eating disorders (EDs). It is firstly associated with a derangement
in visuospatial ability, i.e., in the accuracy of estimation (Skrzypek et al., 2001; Waldman,
Loomes, Mountford, & Tchanturia, 2013) likely leading to perceptual overestimation in both
AN (Skrzypek et al., 2001; Waldman et al., 2013), and BN patients (Mohr et al., 2011). Still,
body image includes also an attitudinal modality (Cash & Deagle, 1997) consisting of
cognitive-evaluative (e.g., body dissatisfaction), cognitive-behavioral (e.g., avoiding mirror
gazing or body checking), and affective (e.g., situational body image-related dysphoria)
dimensions (Cash & Deagle, 1997; Probst, Vandereycken, Van Coppenolle, & Pieters, 1999).
More specifically female patients with an ED tend to overestimate particularly their
own appearance (and to some extent other female figures), whereas only a minimal distortion
is found for non-human figures (Benninghoven, Raykowski, Solzbacher, Kunzendorf, &
*Manuscript (without author identifiers)Click here to view linked References
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
2
Jantschek, 2007; Cash & Deagle, 1997; Probst et al., 1999; Skrzypek et al., 2001). Moreover,
body dissatisfaction has been related to a greater extent to the difference found between ideal
and perceived appearance, than to the difference between ideal appearance and actual weight
(Joiner, Heatherton, Rudd, & Schmidt, 1997). In the same token, subjective distress
associated with body image has been tied more closely than the perceptual accuracy
component of body image to the development of EDs (Cash & Deagle, 1997), although an
association between the two dimensions has been shown in patients with an ED (Cash &
Deagle, 1997; Striegel-Moore et al., 1989; Waldman et al., 2013).
It is difficult to optimize specific tools for the assessment of body image due to its
multi-faceted nature. Today, two main strategies are applied for the assessment of affective
and perceptual aspects. The first, consisting of questionnaires, evaluates body-related
affective aspects; the second focuses on perceptual accuracy and evaluates perceptual
measures (J. K. Thompson, 1997).
Despite extensive use, both strategies may have considerable limitations. Inherently,
questionnaires evaluate body image in an indirect manner, and usually conceptualize body
satisfaction as a uni-dimensional rather than a multi-dimensional construct. The most
significant drawback of perceptual measures is that they do not assess the participant’s own
image, nor do they have the potential to measure the distortion interactively, during the
assessment process.
Several new strategies for the assessment of body image disturbance have been
recently implemented, in an attempt to overcome some of these limitations. One strategy is
based on standardized quantitative assessment software systems, which use biometric data
based on real body shapes. A few studies have previously assessed body image disturbances
in patients with EDs using software measures. Most of these studies (Benninghoven et al.,

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
3
2007; Ferrer-Garcia & Gutierrez-Maldonado, 2008; Overas, Kapstad, Brunborg, Landro, &
Lask, 2014; Roy & Forest, 2007) although not all (Tovee et al., 2003), have shown greater
body size overestimation in patients with AN and BN vs. non-ED controls. In addition,
Ferrer-García & Gutiérrez-Maldonado (Ferrer-Garcia & Gutierrez-Maldonado, 2008) have
shown that control individual considered at risk of developing an ED (i.e., showing
pathological scores on the Eating Attitudes Test-26 (EAT-26) and the Eating Disorder
Inventory-2 (EDI-2) reveal greater overestimation of body size in comparison to a not-at-risk
group. Lastly, Roy and Meilleur (Roy, 2010 #91) have shown a decrease in body
image distortion in 70% of patients with AN following inpatient treatment.
Hence, we developed a new instrument for the assessment of body image, the
Computerized Assessment of Body Image (CABI) (Harari, Furst, Kiryati, Caspi, & Davidson,
2001). Our primary aim was to assess the validity of the CABI in comparison to the existing
body assessment methods in particular the widely used perceptual Contour Drawing Rating
Scale (CDRS) (M. A. Thompson & Gray, 1995) and the Body Dissatisfaction scale of the
EDI-2 (EDI-2-BD) (27). The comparison between the CABI, CDRS and EDI-2-BD was
carried out with respect to the perceptual, affective, and ideal-related dimensions of body
image. Our secondary aims were to compare body image disturbances in different ED types,
and to assess the factors affecting body image. We hypothesized that the CABI will be found
a valid tool for the assessment of body image in patients with an ED when compared with
standardized measures. Secondly, although all patients with EDs will show a greater
disturbance in all aspects of body image in comparison to non-ED controls with all tools used,
malnourished AN patients will be more disturbed than normal weight BN patients,
particularly in those measurements taken with the CABI.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
4
METHODS
Participants
The study included 22 inpatients diagnosed with DSM-IV (APA, 1994): restrictive
type AN (AN-R), 22 inpatients diagnosed with binge/purge type AN (AN-B/P), 20 inpatients
diagnosed with BN, and 41 healthy controls. All patients were hospitalized in the adolescent
and adult inpatient ED departments at the Chaim Sheba Medical Center, Tel Hashomer,
Israel. Inclusion criteria comprised of female gender between the ages of 15 to 25; exclusion
criteria comprised of lifetime or current schizophrenic spectrum disorder, bipolar disorder,
organic-brain disorder, mental retardation, and lifetime or current medical illness that could
potentially affect appetite or weight (e.g., diabetes mellitus or thyroid disorders). The patients
did not receive any psychotropic medication for at least two weeks prior to their assessment.
Healthy controls included 41 female volunteers between the ages of 15-25 years.
Adolescent controls were recruited from families of the staff of the hospital, and adult
controls from several universities using advertisements. Healthy controls were matched with
the research patients for age, years of schooling, ethnic origin, and catchment area. Healthy
controls were required to have no lifetime or current psychiatric disorder, medical disorder or
chronic use of medications, and no stigmata indicative of an ED. They were required to have
a body mass index (BMI) between 20-25 kg/m2 (Bray, 1992), and regular menses since
menarche.
All participants and their parents or other legal guardians, in the case of minors under
the age of 18, agreed to participate in the study by signing a written informed consent. The
study was approved by the local IRB committee. Participation was voluntary and anonymous,
and each participant was given coded numbers known only to the principal investigators
(D.S., A.C.). Data was analyzed for the whole sample and not for individual participants.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
5
Instruments
Diagnosis of an ED, according to the DSM-IV (Association, 1994) has been
established using the Eating Disorders Family History Interview (EDFHI) (Strober, 1987).
This is a semi-structured clinical interview designed to gather detailed information on weight
and eating history, previously used in studies of ED patients (Kaye et al., 1998) including in
Israeli samples (Yackobovitch-Gavan et al., 2009). Other lifetime DSM-IV Axis I psychiatric
morbidity was assessed using the Structured Clinical Interview for DSM-IV Axis I Disorders-
Patient Edition (SCID-I/P Version 2.0) (First et al., 1993).
Assessment of body-image
Three tools were used for the assessment of body-image: the Contour Drawing Rating
Scale (CDRS; 20) consists of 9 female contour images sorted from extreme underweight to
extreme overweight. The CDRS has been found to show good validity and test-retest
reliability (r=.78; (M. A. Thompson & Gray, 1995), and is accepted as a standardized tool for
the assessment of body image disturbances in clinical and community populations
(Lombardo, Russo, Lucidi, Iani, & Violani, 2004; M. A. Thompson & Gray, 1995). In the
present study, participants have been asked to choose the image that best fits the way they
think (perceptual), feel (an affective component), and wish they looked like (ideal body
image). Two additional dimensions, assessing the extent of the participants' satisfaction with
their perceived images have been constructed by subtracting the ideal body image from these
perceptual and affective components of body image.
The Computerized Assessment of Body Image (CABI; 19) displays a realistic pictorial
simulation of weight changes, applied to a real source image. The process is based on a
method developed for the representation of biological shape modifications (Harari et al.,
2001). Still pictures of frontal body images are captured using a digital camera in an adjusted

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
6
room sufficiently illuminated for photography purposes. Body parts are identified and marked
and then the digital picture is processed by the software. Each body part is separately and
independently processed according to its shape-change potential (e.g., arm –cylinder, or
abdomen –sphere); facial simulation was not assessed because of technical limitations.
Following this step, the altered body parts are automatically merged back into a whole body
with an adjustment of joint areas. As a result, the processed images represent lifelike body
shape changes. A single photograph for each individual is taken in uniform conditions related
to clothing (full body leotards), background, lighting and position. Twenty-four simulated
images were processed and introduced to the participants the day after the photograph has
been taken.
The Body-Dissatisfaction Scale of the Eating Disorder Inventory-2 (EDI-2-BD;
(Garner, 1991), assessing the extent of dissatisfaction with different parts of the body. This
scale was used in the present study as an affective body image assessment tool. The EDI-2
has been previously validated in Israeli samples (Yackobovitch-Gavan et al., 2009).
The final results of the image processing steps are a photo series of continuous body
shape change simulation scale (i.e., continuous scale). The series contains a random uniform
sequence displaying original and transformed images. Four of the images are original (non-
simulated, 100% of original weight) whereas the remainder 20 are images with different
levels of simulated weight changes (lowest weight 86% of original weight and highest –
116%, see Figure 1; this range is based on that used in previous studies (Stein et al., 2002). In
the continuous scale, a graphical slider allows the participant to adjust her body shape until it
fits her perceived appearance, while the change in percentage is hidden from her.
A specific non-ordinal pattern of the images has also been applied. Accordingly,
participants are asked to estimate whether each self-image presented is an underweight,

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
7
overweight or unchanged simulation of her. An Identification Index (CABI-ii) is then
constructed, including all identification errors made by the participant, taking into
consideration the magnitude of the distortion. Each picture is scored (0) for correct
estimation, (1) for a minor error (e.g., an overweight estimation when weight is unchanged),
and (2) for a major error (e.g., an overweight estimation when weight is reduced). The CABI-
ii also indicates the error's direction, namely whether the participant perceives herself as
overweight (-ii), or underweight (+ii) versus her actual weight. The CABI-ii scores range
from -48 to +48, when scores closer to zero represent lower body distortion. Following this
non-ordinal presentation, the picture series is presented to the participants once more, this
time as a continuous scale (ordered from 86-116% of original weight). The participants are
asked to choose the picture that best fits their perceptual, affective and ideal body image. This
procedure has been similarly applied when using the CDRS.
Assessment of depression and anxiety
Depression and anxiety have been assessed because of their known influence on body
image in patients with EDs (McCabe, Ricciardelli, Sitaram, & Mikhail, 2006; Overas et al.,
2014). Depression has been evaluated using the self-rating Beck Depression Inventory (BDI)
(Beck, Ward, Mendelson, Mock, & Erbaugh, 1961), and anxiety with the trait scale, i.e. the
general tendency to display anxiety scale) of the State Trait Anxiety Inventory (STAI-Trait)
(Spielberger, Gorsuch, & Lushene, 1970), Both scales have been extensively used in patients
with EDs (Pollice, Kaye, Greeno, & Weltzin, 1997), including in Israeli samples
(Yackobovitch-Gavan et al., 2009).
Procedure
Patients were interviewed on admission with the EDFHI and the SCID-I/P version 2.0
by experienced psychiatrists and child and adolescent psychiatrists. Diagnoses were

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
8
confirmed in clinical meetings of the teams of the two departments. Healthy controls were
similarly interviewed with the EDFHI and the SCID-I/P by a Master's degree psychologist
trained in psychiatric interviewing by one of the study's principal investigators (D.S.). The
EDI-2-BD, BDI, STAI-Trait, CDRS, and CABI were distributed to the patients in random
order by Master's level clinical psychology students within two weeks of admission, upon the
stabilization of their medical condition. These tools were similarly administered to the control
participants. Evaluations took place in a specific research room in the Sheba Medical Center,
which was well illuminated and were carried out individually. All evaluations were performed
in the morning hours, at least one hour after the previous meal, to minimize the variability
related to feeding conditions. Patients’ weight and height are routinely taken in these
departments in the morning hours, using standardized procedures. The weight and height of
the control participants were similarly assessed and were taken last to reduce their influence
on the other findings.
Statistical Analysis
Correlations among the different tools assessing body image disturbance, i.e., the
CABI, CDRS, and EDI-2-BD, as well as the correlations between these parameters and the
demographic, clinical and psychometric measures introduced, were analyzed using Pearson
correlation coefficients for interval parameters and Spearman Rho’s for ordinal parameters.
Due to the large number of measures included in the study, the groups were first
compared with multivariate analysis of variance (MANOVA) and then with univariate
analysis of variance (ANOVA) for each measure. Post hoc Tukey's pairwise comparisons
were used to determine the specific differences among the four groups. Analysis of
covariance (ANCOVA) was used to control for the effect of the between-group differences in
age, education, BMI, depression and anxiety on the CDRS, CABI and EDI-2-BD dimensions.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
9
RESULTS
Significant between-group differences were found for age, education level and BMI
(see Table 1). Patients with AN-R were significantly younger than both AN-B/P and BN
groups, likely resulting in significantly less years of schooling. Healthy controls were not
different from any other group in age and education level. Both groups with AN had a
significantly lower BMI in comparison to patients with BN and healthy controls. No between-
group differences were found for ethnic origin (data not shown).
Using MANOVA we found a significant overall between-group difference for the
CDRS and CABI perceptual/affective dimensions and for EDI-2-BD [F(21,265)=4.25,
p<.0001]. Table 2 summarizes the specific between-group comparisons for all dimensions.
Patients with AN-R, AN-B/P, and BN scored significantly higher on the CABI perceptual and
affective body image dimensions compared with the healthy controls. Whereas no between-
group differences were found for CABI ideal body image, the difference between the CABI
affective and ideal body image dimensions was significantly higher for all ED groups in
comparison to the healthy controls. With regard to the difference between the CABI ideal and
perceptual body image, only the BN group scored higher than the healthy controls.
The assessment of the CABI-ii revealed that patients with AN-R and AN-B/P scored
significantly higher on the perceptual distortion (scores more distant from zero) dimension
compared to the controls. Moreover, the CABI-ii score of the two groups with AN was
negative, namely they perceived themselves as more overweight than they actually were,
compared with the positive score of the controls, who perceived themselves as more
underweight than they really were (see Table 2).
Table 2 also summarizes the between-group differences for the CDRS and the EDI-2-
BD. Patients with BN showed more pathological scores than the two groups with AN, and the

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
10
controls on the CDRS perceptual and affective dimensions. Patients with AN were not
different from control participants in these dimensions. Both groups with AN showed higher
scores on CDRS ideal body image in comparison to controls. On the other hand, patients with
BN scored significantly higher on the difference between the CDRS ideal and perceptual
body image in comparison to patients with AN-R and controls. Lastly, patients with AN-B/P
and BN showed significantly more body dissatisfaction than controls on the EDI-2 (EDI-2-
BD; see Table 2).
The overall between-group difference for depression (BDI) and anxiety (STAI-Trait)
[F(6,162)=8.28, p<.0001] according to the MANOVA was significant. Table 1 summarizes
the specific between group differences for these dimensions. All three groups with an ED
scored significantly higher than the healthy controls on the BDI. While, only patients with AN
showed significantly higher scores on the STAI-Trait in comparison to the healthy controls.
Finally, a considerable portion of the patients had comorbid disorders. The numbers and
percentages for depressive disorders for patients with AN-R, AN-B/P, and BN were 9 (41%),
16 (73%), and 8 (40%), respectively. The respective distribution for anxiety disorders was 2
(9%), 0, and 0, , for obsessive compulsive disorder 3 (14%), 2 (9%), and 3 (15%), and for no
comorbidity 8 (36%), 4 (18%), and 9 (45%),. No between-group differences were found for
comorbidiy except for depressive disorders (results not shown).
All significant between-group differences for the CDRS were maintained when
controlling for age, years of education, BDI, STAI-Trait, and BMI and for the CABI when
controlling for age, education, and BMI (data not shown). Controlling for BDI and STAI-
Trait maintained the significant between-group differences for the CABI perceptual, affective
and ideal-body image dimensions, but not for the differences between the CABI ideal and
perceptual/affective dimensions (data not shown). Lastly, in the case of the EDI-2-BD, all

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
11
significant between group differences were maintained when controlling for age, education
level and BMI, but not when controlling for BDI and STAI-Trait (data not shown).
DISCUSSION
The aims of this study were threefold. Firstly to establish whether a computerized
assessment of one’s own body image (the CABI) is a valid tool for the assessment of body
image disturbances in patients with EDs by comparing its ability to differentiate between
these patients and non-ED controls to that of accepted standardized verbal (EDI-2-BD) and
perceptual (CDRS) tools. Secondly, including three distinct ED types across several
dimensions of body image enabled us to compare the boy-image disturbances of patients with
restricting vs. B/P behaviors, and of normal weight vs. low-weight patients. Lastly, we aimed
to assess whether different factors would be associated with different dimensions of body
image.
Similarities and differences between the CABI, CDRS and EDI-2-BD
The dimensions of body image assessed using the CABI were in line with the
corresponding dimensions of the well-established CDRS and EDI-2-BD methods. Across the
three groups with EDs, most body-image dimensions were different in comparison to healthy
controls. This relates in particular to the greater overestimation of body size in patients with
EDs with respect to the perceptual and affective dimensions of both the CABI and the CDRS.
These findings, shown also in other studies using different software techniques
(Benninghoven et al., 2007; Ferrer-Garcia & Gutierrez-Maldonado, 2008; Overas et al., 2014;
Roy & Forest, 2007), likely support the validity of the CABI in the assessment of the
perceptual and affective dimensions of body image disturbances in patients with EDs.
Nonetheless, noteworthy differences emerged between the CABI and the CDRS.
Thus, whereas the CABI’s perceptual and affective dimensions differentiated between all
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
12
there groups with ED and controls, in the case of the CDRS, these dimensions distinguished
BN patients from both groups with AN and controls. The greater sensitivity of self-images to
distinguish between patients with EDs and controls in comparison to a neutral female figure
was noted also in other computerized studies (Benninghoven et al., 2007) On the other hand,
in contrast to our findings, other studies using the CDRS demonstrated its ability in
differentiating all ED types from healthy controls (M. A. Thompson & Gray, 1995). To
conclude, we suggest that despite these inconsistencies, our findings add to other
computerized studies in showing superiority in distinguishing patients with EDs from healthy
controls when assessing perceptual overestimation of one’s own body in comparison to
neutral female figures (Overas et al., 2014).
A somewhat puzzling difference between the two tools is the finding of a significant
difference in the ideal body image between both groups with AN and controls when using the
CDRS but not in the CABI. If perceiving one’s own body is considered more sensitive to
perceptual and affective distortion than a neutral figure, this should have been the case also
for one’s desired image. Still, the ideal figures for all groups with the CABI were around the
non-simulated image (i.e., around 100%), suggesting no distortion for self-ideal body image
(see Table 2). By contrast, the ideal figure for all groups with the CDRS was well below the
mean of around 4-5 out of 9 female contour drawings, with the low-weight AN patients and
even normal controls preferring an even skinnier image than the two normal weight groups
(see Table 2). In the same token, discrepancies between patients with EDs and controls in the
differences between the perceptual/affective and ideal body image were greater with the
CDRS than the CABI (see Table 2). Perhaps, there is a greater influence of the societal thin-
body ideal when relating to a general female figure, a procedure putatively allowing for some
distancing from painful contents related to one's own image (Overas et al., 2014).

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
13
Differences in body-image disturbances among the different types of ED
Several differences in the various dimensions of body image have been found among
the three groups with ED. Accordingly, patients with AN and healthy controls are more
disturbed than those with BN on the CDRS perceptual, and affective dimensions. Moreover,
in keeping with other studies (Tovee et al., 2003), patients with AN but not BN, have differed
from controls in preferring skinnier ideal body image according to the CDRS, and in having a
greater distortion on the CABI-ii (see Table 2). The greater perceptual overestimation of
patients with AN versus BN, shown also in other studies using software techniques
(Benninghoven et al., 2007), is likely associated with their lower BMI and greater
malnutrition (Bamford, Attoe, Mountford, Morgan, & Sly, 2014). By contrast, despite the
greater body-image overestimation of patients with AN and their preference of thinner ideal
body image, patients with BN do reveal greater discrepancy between the perceptual/affective
and ideal body image dimensions of the CDRS than patients with AN (see Table 2). This may
reflect greater distress in the comparison of ideal and perceived weight in patients with an ED
in the case of normal weight vs. low weight conditions, although it is of note that no
differences have been found between patients with AN and BN in EDI-2-BD. Despite these
inconsistencies, our findings may support the importance of affective dimensions in the
development and maintenance of body image disturbance in patients with an ED above and
beyond the influence of perceptual distortions (Skrzypek et al., 2001; J. K. Thompson, 1997).
Factors influencing body image
The use of MANCOVA has shown that the between group differences in body image
as assessed with all three tools (CDRS, CABI and EDI-2-BD) maintained their significance
when controlling for age, years of schooling, and BMI. In keeping with the findings of Øverås
et al. (Overas et al., 2014), the lack of influence of BMI on the perceptual and affective

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
14
dimensions of body image across all methods, suggests that they represent an inherent trait in
the development and maintenance of an ED further to the influence of reduction of weight.
These findings are also in accordance with studies showing that disturbances in body image in
young females of normal weight may represent a risk factor for the development of later EDs
(Leon et al., 1995; Striegel-Moore et al., 1989). In, in this respect, our findings are consistent
also with studies showing that women recovered from AN (Bachner-Melman, Zohar, &
Ebstein, 2006) and BN (Stein et al., 2003), show more perceptual and affective body image
disturbances in comparison to non-ED controls.
Controlling for depression and anxiety revealed that between-group differences were
still maintained for all CDRS dimensions, most CABI dimensions (except for the differences
between the perceptual/affective and ideal body image dimensions), but not for the EDI-2-BD
scale. These findings suggest that the perceptual design of the CDRS and CABI, potentially
requiring greater precision and attention, may be less subject to the influence of negative
emotions than the verbal EDI-2-BD, which is basically an affective body image tool (Garner,
1991). It is of note that Øverås et al. (Overas et al., 2014) have shown that the differences in
personal images between AN and control participants do persist when controlling for
depression but not for anxiety, suggesting that the overestimation of one’s own figure may be
the result of increased anxiety. In this respect, the association of the difference between the
perceptual/affective and ideal components of one's own image with both depression and
anxiety (Gardner & Bokenkamp, 1996) suggests this discrepancy to be particularly
distressing and anxiety-inducing (Cash & Deagle, 1997; Overas et al., 2014).
Our findings should be interpreted considering the limitations of the study. Firstly, the
number of patients in each of the groups with an ED is relatively small. In addition, as our
sample includes only inpatients, the findings cannot be generalized to patients with less severe

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
15
EDs. Furthermore, although using the definitions of the perceptual (what do you think you
look like) and affective (how do you feel you look like) body image dimensions that are
recommended by Thompson and Gray (M. A. Thompson & Gray, 1995) in the use of the
CDRS, these definitions might be ambiguous to patients with an ED who are likely obsessed
with the way they think and feel they look like. Moreover, although all computerized studies
refer to the participants' own image, they use different assessment techniques, e.g., presumed
BMI (Tovee et al., 2003), percentage of presumed body fat (Benninghoven et al., 2007), or a
full body picture projected onto a wall and a mirror (Overas et al., 2014), or displayed in the
computer (our study). This use of different techniques may limit the likelihood of valid
comparisons among the findings of different computerized studies in the assessment of body
image disturbances.
Our study has, nevertheless, some important advantages. It relates to both the
perceptual and affective aspects of body image, using a computerized-quantified method
versus well-accepted standardized verbal and perceptual measures. Moreover, the CABI
provides 24 pictures in contrast to the standard 9 figures of the CDRS; these are presented in a
random order, increasing the likelihood of a less-biased body-image evaluation. This is
because the presentation of figures in either an upward or downward sequential order, as is
usually the case, may increase the risk of influencing the participant's perception (Gardner,
Jones, & Bokenkamp, 1995). Thirdly, the CABI also enables greater sensitivity in the
assessment of body image, using two different types of measurements: the CABI-ii indicates
error magnitude and directionality, whereas the continuous body shape change simulation
scale reflects the individual's perceived appearance.
Conclusions and future directions

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
16
The primary aim of the study was to assess the validity and utility of a computerized
evaluation of body image disturbances in patients with an ED, the Computerized Assessment
of Body Image (CABI), against well-accepted standardized verbal-affective (EDI-2-Body
Dissatisfaction) and perceptual (perceptual Contour Drawing Rating Scale; CDRS) tools. The
findings of the present study provide, to our understanding, validation to the use of the self-
image assessment method of the CABI as an additional, and perhaps more sensitive tool in
addressing the role of perceptual and affective/attitudinal dimensions and their interactions in
body image disturbances in patients with different types of EDs. Secondly, the use of a
multidimensional assessment strategy enabled a better understanding of the differences in the
various dimensions of body image in patients with AN vs. BN. Future studies implementing
the CABI in larger samples, both in naturalistic follow-up studies and following treatment,
may improve the choice of the treatment strategies best tailored for reducing body image
disturbance, and the understanding of the role of these disturbances in the outcome of an ED.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
17
References
Association, A. P. (1994). Diagnostic and Statistical Manual of Mental Health Disorders (4th
ed.). Washington DC.
Bachner-Melman, R., Zohar, A. H., & Ebstein, R. P. (2006). An examination of cognitive
versus behavioral components of recovery from anorexia nervosa. J Nerv Ment Dis,
194(9), 697-703. doi: 10.1097/01.nmd.0000235795.51683.9900005053-200609000-
00010 [pii]
Bamford, B. H., Attoe, C., Mountford, V. A., Morgan, J. F., & Sly, R. (2014). Body checking
and avoidance in low weight and weight restored individuals with anorexia nervosa
and non-clinical females. Eat Behav, 15(1), 5-8. doi:
10.1016/j.eatbeh.2013.10.011S1471-0153(13)00118-9 [pii]
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for
measuring depression. Arch Gen Psychiatry, 4, 561-571.
Benninghoven, D., Raykowski, L., Solzbacher, S., Kunzendorf, S., & Jantschek, G. (2007).
Body images of patients with anorexia nervosa, bulimia nervosa and female control
subjects: a comparison with male ideals of female attractiveness. Body Image, 4(1),
51-59. doi: S1740-1445(06)00114-8 [pii]10.1016/j.bodyim.2006.12.002
Bray, G. A. (1992). Pathophysiology of obesity. Am J Clin Nutr, 55(2 Suppl), 488S-494S.
Cash, T. F., & Deagle, E. A., 3rd. (1997). The nature and extent of body-image disturbances
in anorexia nervosa and bulimia nervosa: a meta-analysis. Int J Eat Disord, 22(2),
107-125. doi: 10.1002/(SICI)1098-108X(199709)22:2<107::AID-EAT1>3.0.CO;2-J
[pii]
Fairburn, C. G., Peveler, R. C., Jones, R., Hope, R. A., & Doll, H. A. (1993). Predictors of 12-
month outcome in bulimia nervosa and the influence of attitudes to shape and weight.
J Consult Clin Psychol, 61(4), 696-698.
Ferrer-Garcia, M., & Gutierrez-Maldonado, J. (2008). Body Image Assessment Software:
psychometric data. Behav Res Methods, 40(2), 394-407.
First, M. B., Opler, L. A., Hamilton, R. M., Linder, J., Linfield, L. S., Silver, J. M., . . .
Spitzer, R. L. (1993). Evaluation in an inpatient setting of DTREE, a computer-
assisted diagnostic assessment procedure. Compr Psychiatry, 34(3), 171-175. doi:
0010-440X(93)90043-4 [pii]
Gardner, R. M., & Bokenkamp, E. D. (1996). The role of sensory and nonsensory factors in
body size estimations of eating disorder subjects. J Clin Psychol, 52(1), 3-15. doi:
10.1002/(SICI)1097-4679(199601)52:1<3::AID-JCLP1>3.0.CO;2-X
Gardner, R. M., Jones, L. C., & Bokenkamp, E. D. (1995). Comparison of three
psychophysical techniques for estimating body-size perception. Percept Mot Skills,
80(3 Pt 2), 1379-1390. doi: 10.2466/pms.1995.80.3c.1379
Garner, D. M. (1991). Eating Disorder Inventory-2. Professional Manual. Odessa, FL, USA:
Psychological Assessment Research, Inc.
Harari, D., Furst, M., Kiryati, N., Caspi, A., & Davidson, M. (2001). A computer-based
method for the assessment of body-image distortions in anorexia-nervosa patients.
IEEE Trans Inf Technol Biomed, 5(4), 311-319.
Joiner, T. E., Jr., Heatherton, T. F., Rudd, M. D., & Schmidt, N. B. (1997). Perfectionism,
perceived weight status, and bulimic symptoms: two studies testing a diathesis-stress
model. J Abnorm Psychol, 106(1), 145-153.
Kaye, W. H., Greeno, C. G., Moss, H., Fernstrom, J., Fernstrom, M., Lilenfeld, L. R., . . .
Mann, J. J. (1998). Alterations in serotonin activity and psychiatric symptoms after
recovery from bulimia nervosa. Arch Gen Psychiatry, 55(10), 927-935.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
18
Keel, P. K., Dorer, D. J., Franko, D. L., Jackson, S. C., & Herzog, D. B. (2005).
Postremission predictors of relapse in women with eating disorders. Am J Psychiatry,
162(12), 2263-2268. doi: 162/12/2263 [pii]10.1176/appi.ajp.162.12.2263
Leon, G. R., Fulkerson, J. A., Perry, C. L., & Early-Zald, M. B. (1995). Prospective analysis
of personality and behavioral vulnerabilities and gender influences in the later
development of disordered eating. J Abnorm Psychol, 104(1), 140-149.
Lombardo, C., Russo, P. M., Lucidi, F., Iani, L., & Violani, C. (2004). Internal consistency,
convergent validity and reliability of a brief questionnaire on disordered eating (DEQ).
Eat Weight Disord, 9(2), 91-98.
McCabe, M. P., Ricciardelli, L. A., Sitaram, G., & Mikhail, K. (2006). Accuracy of body size
estimation: Role of biopsychosocial variables. Body Image, 3(2), 163-171. doi: S1740-
1445(06)00005-2 [pii]10.1016/j.bodyim.2006.01.004
Mohr, H. M., Roder, C., Zimmermann, J., Hummel, D., Negele, A., & Grabhorn, R. (2011).
Body image distortions in bulimia nervosa: investigating body size overestimation and
body size satisfaction by fMRI. Neuroimage, 56(3), 1822-1831. doi:
10.1016/j.neuroimage.2011.02.069S1053-8119(11)00225-4 [pii]
Overas, M., Kapstad, H., Brunborg, C., Landro, N. I., & Lask, B. (2014). Memory versus
perception of body size in patients with anorexia nervosa and healthy controls. Eur
Eat Disord Rev, 22(2), 109-115. doi: 10.1002/erv.2276
Pollice, C., Kaye, W. H., Greeno, C. G., & Weltzin, T. E. (1997). Relationship of depression,
anxiety, and obsessionality to state of illness in anorexia nervosa. Int J Eat Disord,
21(4), 367-376. doi: 10.1002/(SICI)1098-108X(1997)21:4<367::AID-
EAT10>3.0.CO;2-W [pii]
Probst, M., Vandereycken, W., Van Coppenolle, H., & Pieters, G. (1999). Body experience in
eating disorders before and after treatment: a follow-up study. Eur Psychiatry, 14(6),
333-340. doi: S0924-9338(99)00159-5 [pii]
Roy, M., & Forest, F. (2007). Assessment of body image distortion in eating and weight
disorders: the validation of a computer-based tool (Q-BID). Eat Weight Disord, 12(1),
1-11. doi: 3450 [pii]
Skrzypek, S., Wehmeier, P. M., & Remschmidt, H. (2001). Body image assessment using
body size estimation in recent studies on anorexia nervosa. A brief review. Eur Child
Adolesc Psychiatry, 10(4), 215-221.
Smith, C., Feldman, S. S., Nasserbakht, A., & Steiner, H. (1993). Psychological
characteristics and DSM-III-R diagnoses at 6-year follow-up of adolescent anorexia
nervosa. J Am Acad Child Adolesc Psychiatry, 32(6), 1237-1245. doi: S0890-
8567(09)64524-X [pii]10.1097/00004583-199311000-00018
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970). Manual for the State-Trait
Anxiety Inventory (STAI). Palo Alto, CA, USA: Consulting Psychologists Press.
Stein, D., Kaye, W. H., Matsunaga, H., Myers, D., Orbach, I., Har-Even, D., . . . Rao, R.
(2003). Pain perception in recovered bulimia nervosa patients. Int J Eat Disord, 34(3),
331-336. doi: 10.1002/eat.10164
Stein, D., Kaye, W. H., Matsunaga, H., Orbach, I., Har-Even, D., Frank, G., . . . Rao, R.
(2002). Eating-related concerns, mood, and personality traits in recovered bulimia
nervosa subjects: a replication study. Int J Eat Disord, 32(2), 225-229. doi:
10.1002/eat.10025
Striegel-Moore, R. H., Silberstein, L. R., Frensch, P., & Rodin, J. (1989). A prospective study
of disordered eating among college students. International Journal of Eating
Disorders, 8(5), 499-509. doi: 10.1002/1098-108x(198909)8:5<499::aid-
eat2260080502>3.0.co;2-a

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
19
Strober, M. (1987). The Eating Disorders Family History Interview. Los Angeles: University
of California.
Thompson, J. K. (Ed.). (1997). Body Image, Eating Disorders and Obesity. Washington DC:
American Psychological Association.
Thompson, M. A., & Gray, J. J. (1995). Development and validation of a new body-image
assessment scale. J Pers Assess, 64(2), 258-269. doi: 10.1207/s15327752jpa6402_6
Tovee, M. J., Benson, P. J., Emery, J. L., Mason, S. M., & Cohen-Tovee, E. M. (2003).
Measurement of body size and shape perception in eating-disordered and control
observers using body-shape software. Br J Psychol, 94(Pt 4), 501-516. doi:
10.1348/000712603322503060
Trentowska, M., Bender, C., & Tuschen-Caffier, B. (2013). Mirror exposure in women with
bulimic symptoms: how do thoughts and emotions change in body image treatment?
Behav Res Ther, 51(1), 1-6. doi: 10.1016/j.brat.2012.03.012
Waldman, A., Loomes, R., Mountford, V. A., & Tchanturia, K. (2013). Attitudinal and
perceptual factors in body image distortion: an exploratory study in patients with
anorexia nervosa. J Eat Disord, 1, 17. doi: 10.1186/2050-2974-1-172050-2974-1-17
[pii]
Yackobovitch-Gavan, M., Golan, M., Valevski, A., Kreitler, S., Bachar, E., Lieblich, A., . . .
Stein, D. (2009). An integrative quantitative model of factors influencing the course of
anorexia nervosa over time. Int J Eat Disord, 42(4), 306-317. doi: 10.1002/eat.20624

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
20
Figure Captions
Figure 1. Four simulated figures using the Computerized Assessment of Body Image (CABI)
software
An example of the discriminating potential of the CABI software: a figure of original body
weight (100%), non-simulated (a); figures simulating 104% (b), 110% (c) and 114% (d) of
body weight.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
21
Acknowledgements: We thank Prof. Edith Mitrani and Dr. Amit Yaroslavsky from the
Adolescent and Adult inpatient ED departments at the Sheba Medical Center, Tel Hashomer,
for their valuable comments.
Disclosure of conflict: No conflict of interest in this work.

Table 1: Between-group differences in demographic and psychometric variables
AN-R
(n=22)
AN-B/P
(n=22)
BN
(n=20)
Controls
(n=41)
F (3,102) p-value
Age (years) 18.05±3.3a
22.02±5.0b
22.40±4.0b
19.98±4.9a,b
4.434 .006
Education (years) 10.64±1.9a
12.82±2.3b
12.70±1.9b
12.02±3.0a,b
3.659 .02
BMI (kg/m2) 16.01±1.8
a 17.16±2.1
a 20.96±1.9
b 21.17±2.5
b 35.365 <.001
BDI 21.44±13.7a 21.72±12.4
a 18.40±6.7
a 5.64±7.8
b 16.540 <.001
STAI-Trait 53.20±12.8a
50.33±13.8a
45.67±11.8a,b
37.46±8.5b
10.062 <.001
Legend: AN-R: anorexia nervosa, restricting type; AN-B/P: anorexia nervosa, binge purge type;
BN: bulimia nervosa; BMI: body mass index; BDI: Beck Depression Inventory, STAI-Trait: State
Trait Anxiety Inventory-Trait.
Scores with superscripts indicate the findings according to Tukey. Scores with different
superscripts differ significantly from each other in the respective row at p≤.05. Scores with the
same superscript do not differ significantly from each other in the respective row.
Table(s)

Table 2. Between-group differences in the CDRS, CABI and EDI-2-BD body image tools
AN-R
(n=22)
AN-B/P
(n=22) BN (n=20)
Controls
(n=41) F (3,102) p-value
CDRS Perceptual 3.91±1.9a
4.05±2.0a
6.15±1.6b 4.88±1.3
a 7.949 <.001
CDRS Affective 4.67±2.3a
5.10±2.3a
7.15±1.6b 4.98±1.2
a 8.653 <.001
CDRS Ideal 2.67±1.2a
2.50±1.1 a
3.25±1.0a,b
3.93±1.1b
10.634 <.001
CDRS
Perceptual – Ideal 1.24±2.4
a 1.55±2.4
a,b 2.90±1.8
b .95±1.3
a 4.971 .003
CDRS
Affective – Ideal 2.00±2.7
a,c 2.60±2.8
a,b 3.90±1.9
b 1.05±1.3
c 8.832 <.001
CABI Perceptual 105.36±4.9a
105.34±6.0a
105.40±3.7a
101.64±2.6b
6.590 <.001
CABI Affective 107.83±6.4a
108.86±7.0a
109.68±4.3a
102.73±3.3b
11.925 <.001
CABI Ideal 98.01±6.7a
98.18±7.5a
96.28±5.6a
98.67±5.2a
0.697 .56
CABI
Perceptual – Ideal 7.42±8.5
a,b 7.16±11.6
a,b 9.13±6.8
a 2.97± 4.6
b 3.567 .02
CABI
Affective – Ideal 10.00±9.9
a,b 10.68±12.1
a 13.4±7.0
a 4.06±4.6
b 7.049 <.001
CABI-ii -3.95±7.4a
-3.82±7.4a
-1.80±5.6 a,b
2.46±5.1b
7.416 <.001
EDI-2-BD 10.89±7.5a,b
14.11±9.2a 17.31±7.9
a 7.61±6.2
b 7.832 <.001
Legend: AN-R: anorexia nervosa, restricting type; AN-B/P: anorexia nervosa, bingeing purging
type; BN: bulimia nervosa; CDRS: Contour Drawing Rating Scale; CABI: Computerized
Assessment of Body Image; CABI-ii: CABI identification index; EDI-2-BD – Eating Disorder
Inventory-2- Body Dissatisfaction Scale.
Scores with superscripts indicate the findings according to Tukey. Scores with different
superscripts differ significantly from each other in the respective row at p≤.05. Scores with the
same superscript do not differ significantly from each other in the respective row.
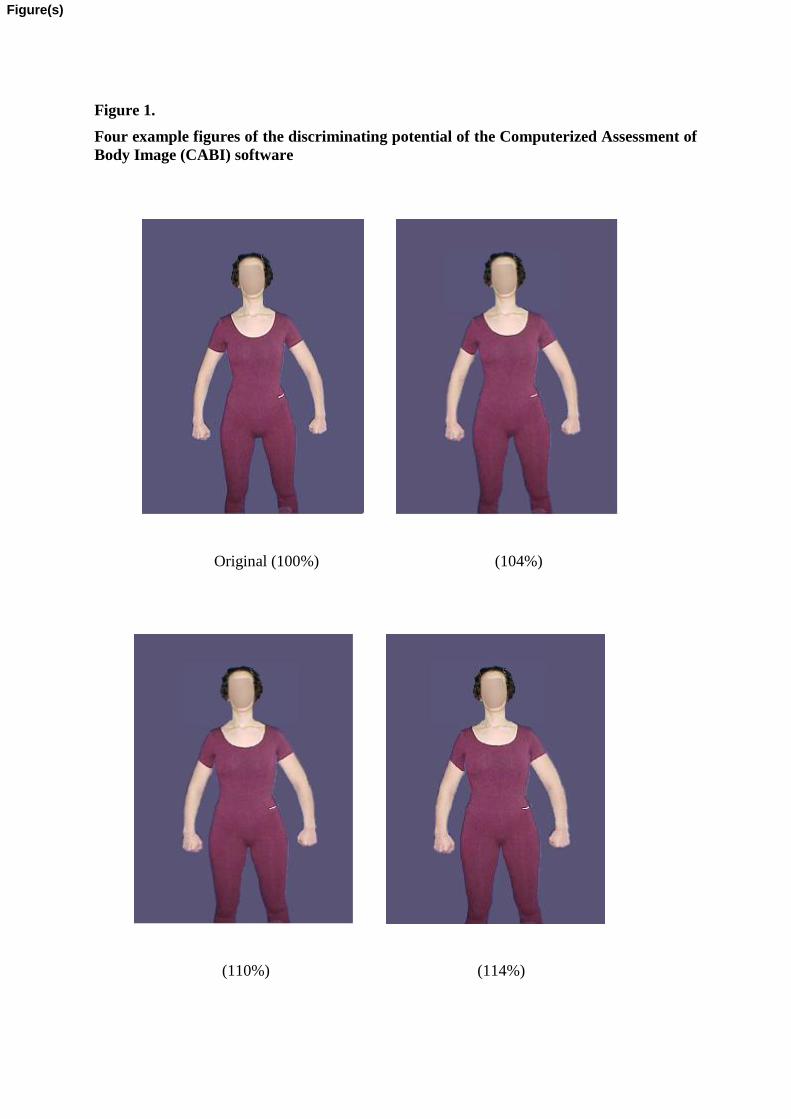
Figure 1.
Four example figures of the discriminating potential of the Computerized Assessment of
Body Image (CABI) software
Original (100%) (104%)
(110%) (114%)
Figure(s)