mandibular reconstruction after head and neck tumor ...776956/fulltext01.pdf · mandibular...
TRANSCRIPT

Mandibular Reconstruction after Head and Neck Tumor Treatment, a Systematic Review
Jonas Emanuelsson Jonathan Viblom Master thesis 30 ECTS MSc. Dental Surgery Dept. Oral and Maxillofacial Surgery Tutor: Mats Sjöström, Linda Pettersson

- 2 -
ABSTRACT
Objectives
This systematic literature review examined the literature about mandibular
reconstruction after cancer treatment with segmental resection, with focus on
success rate for the reconstruction, patient survival rate, dental rehabilitation
and how this effect the patients QOL, oral function and aesthetics.
Material and methods
A search was performed in Pubmed, a database of scientific articles, based on
four keywords (Mandibular, Reconstruction, Cancer, Segmental). After
screening using our inclusion and exclusion criteria’s, 89 articles were chosen.
A data base in excel was established to sort the information we needed for our
study.
Results
Sixty out of the 89 included articles were in full text and 29 were abstracts. The
median year of publication was 2006 (range 1977 to 2013). A total of 5629
patients were included in the literature review. Of these, 3783 patients were
included in articles that had categorized by gender and we found that 65.4%
were males and 34.6% were females.
The total success rate for reconstruction therapies including plate, vascularized-
and non-vascularized bone transplant was 86.4% in 3219 patients (range from
70.4% in the plate group to 92.3% in the non-vascular group). The mean follow
up time were 46.9 mounts (range 0.2 – 216 months).
Conclusion
This literature review indicates a focus on success rates for different kinds of
reconstruction techniques. The overall success rate for non- and vascularized
bone reconstruction techniques were very high compared to plate
reconstruction only. To evaluate patient-related factors such as function,
aesthetics and quality of life, further prospective randomized studies is required.

3
INTRODUCTION
Primary tumors
The mandible is primarily made of bone which is a highly specialized form of
connective tissue. Tumors that originate from connective tissue are called
sarcomas (Mosby’s Dental Dictionary, 2nd edition (2008)). Several variants of
sarcoma exist but the most common variants are osteosarcoma which
constitutes about 35% of sarcoma cases followed by chondrosarcoma (25.8%),
Ewing´s sarcoma (16%) and chordoma (8.4%). (Dorfman et al., 1995; Coleman
et al., 2012).
The incidence and ratio between these four variants of sarcomas varies in
different age groups. Chondrosarcoma is the most common variant in adults
over the age of 30 years while Ewing’s sarcoma and Osteosarcoma accounts
for more than 90% of the cases in the age group of 0-9 years, and
Osteosarcoma is the most common variant in the age group of 10-19 years.
The primary site for sarcoma differs between the age groups. The proportion of
sarcomas originating in the skull and face is highest in patients between 30-59
years of age. Most cases of osteosarcoma affecting the face and skull area is
seen in persons between 30-39 years of age (Francis et al., 2012).
Benignant bone tumors affecting the mandible does not spread to other tissues
and usually have a relatively good prognosis. Among the benign tumors
affecting the mandible is mainly odontomas and ameloblastomas. (Regezi et al.,
1978).
Secondary tumors
The most common secondary tumors affecting the mandibular bone originate
from epidermoid cells which form the tissue types in the floor of the mouth and
gingiva. Cancer originated from this tissue is for example squamous cell
carcinoma. The most common secondary tumors caused by malignancies
originating outside the head and neck area are spread by metastasis from

4
primary tumors in the breast (women) and lung tissue (men) (Weber et al.
2003). Other primary malignancies that can cause metastasis in the mandible
are adrenal gland, colon, genital, thyroid tissues for women and prostate,
kidney, bone and adrenal gland for men. Most common site for secondary tumor
of the mandible is posteriorly to the wedge starting in the molar region. The
mean age for patients with metastasis in the mandible is 50 to 60 years (N.
Zachariades., 1989; Hirshberg et al., 1994; Jham et al., 2011).
Treatment alternatives
When a patient is afflicted by malignancies in the mandible, you have to plan
the treatment in order to cure the patient. The normal treatment alternatives are
irradiation, chemotherapy and/or resection. This review will focus on the
resection therapy but it will also include the irradiation therapy as these
treatments often are given together (Bak et al., 2010). There are two kinds of
resections of the mandible. The first type is called a “rim resection” a technique
where you leave a base of the mandible meaning that you don’t split the
mandible in sections. The other type of resection is based on a technique where
you split the mandible in to sections during cancer removal, called segmental
resection (Rogers et al., 2004).
One decision is if the treatment should include irradiation therapy and if the
irradiation therapy should be performed before or after resection of the
mandible. However, the literature is inconclusive according the result if the
radiation is given before or after surgery (Choi et al., 2004).
A major side effect of irradiation therapy is the risk for osteoradionecrosis
(ORN). Research on ORN has recently undergone a “shift” from the thought
that the tissue is hypo-cellular, hypo-vascular and hypo-oxygen. Today it is
considered that ORN is caused by the cell damage in the bone due to an acute
inflammation, free radicals and a chronic activation of fibroblasts triggered by a
series of growth hormones. This side effects results in a tissue more vulnerable
to trauma with reduced capacity for healing. For example, dental extractions
performed after irradiation results in higher risk for complications (Koga et al
2008). Previously ORN was treated by a hyperbaric chamber where the high

5
pressure and the high oxygen content of the air would re-oxygenate the tissue
and improve the conditions for healing (Teng and Futran, 2005). Today, the
treatment of ORN with hyperbaric oxygen is questioned. Clayman (1997) have
shown low incidence (5%) of ORN following careful dental extraction on patients
post radiation therapy, without the use of hyperbaric oxygen treatment. New
articles describe the pathogenesis of ORN as radiation-induced fibrosis (Lyons
et al., 2008).
The main goal with mandibular reconstruction is to restore the patient’s function
with focus on speech, range of motion, aesthetics, chewing, swallowing, and
Quality of life (QOL). With today’s techniques the surgeons can restore this to
an acceptable level but there is room for improvement (Hidalgo and Pusic,
2002).
Previous, the main goal of the resection and reconstruction were made in order
to make the patient survive the malignancy, resulting in a suboptimal esthetic
result. Reconstruction was generally made with two methods. The first method
was based on a reconstructing rail or mesh, made of metal (titanium or stainless
steel) filled with bone grafts taken from the hip, or hydroxyapatite (Dumbach et
al., 1994). The second method included endogenous non vascular bone grafts.
The deciding factor in choosing between treatments was mainly patient’s life
expectancy (Kanchanarak et al., 1999). These methods have different treatment
outcomes according to graft survival.
Today’s surgical techniques have progressed further partly in the planning of the
operation with MRI, 3D models, titanium plates and better instruments resulting
in an improving treatment outcome. Today the surgeons uses free bone grafts
taken from the fibula, iliac crest or scapula and transplants it with both the skin,
muscles and bones with its own vascular supply and anastomose it into the
reception site. The selection of donor site is based on access, surgery
technicalities, height in the restored mandible, how much bone and soft tissue
that is needed and so on (Bak et al., 2010).

6
Occlusal rehabilitation is based on factors such as facial height, lip support and
aesthetics. One important factor for the choice of reconstruction is if the
occlusion should be with removable prosthesis or dental implants (Schrag et al.,
2006).
The most common postoperative occlusal rehabilitation for patients undergoing
mandibular reconstruction is dental implants. This technique is fairly new and its
technology have improved over the years and today the success rate is around
85-90% in terms of survival of the implants (Jacobsen et al., 2012).
Complications
The mandible is a very important part in the facial structure. It is not only the
aesthetics that is suffering from the resection and reconstruction, but also the
function. The patient can have functional problems with swallowing, speech and
chewing after the resection and reconstruction (Hidalgo and Pusic, 2002). The
reconstruction itself can be affected with graft detachment, clots and hematoma.
An inevitable complication is numbness, because of the removal of n. alveolaris
inferior during the resection. To improve the sensory function, transplanting
nerve in to the resected area, can regain function of the nerve (Shibahara et al.,
1999; Gennaro et al., 2013).
The literature about the prognosis of mandible reconstruction is comprehensive
but definitive prognosis is difficult to predict (Boyd et al., 1995; Hidalgo and
Pusic, 2002; Virgin et al., 2010). The literature reports about different
techniques, different diagnosis of the malignancy and different measurements
for success. The main focus in the literature is success rate of flap survival
while factors descriebing function, estetic and QOL are neglected.
The aim of this study is to investigate and evaluate the literature which
discusses mandibular reconstruction after cancer treatment including segmental
resection of the mandible.

7
MATERIALS AND METHODS
Objectives for literature review
The aim of this study is to investigate and evaluate the literature describing
mandibular reconstruction after cancer treatment including segmental resection
of the mandible.
Search strategy
A systematic literature review based on four keywords (Mandibular,
Reconstruction, Cancer, Segmental) was performed in PubMed, a database of
scientific articles, October 21, 2013 (See Table 1: Search strategy)
The articles were then entered into Endnote in order to get an easy overview.
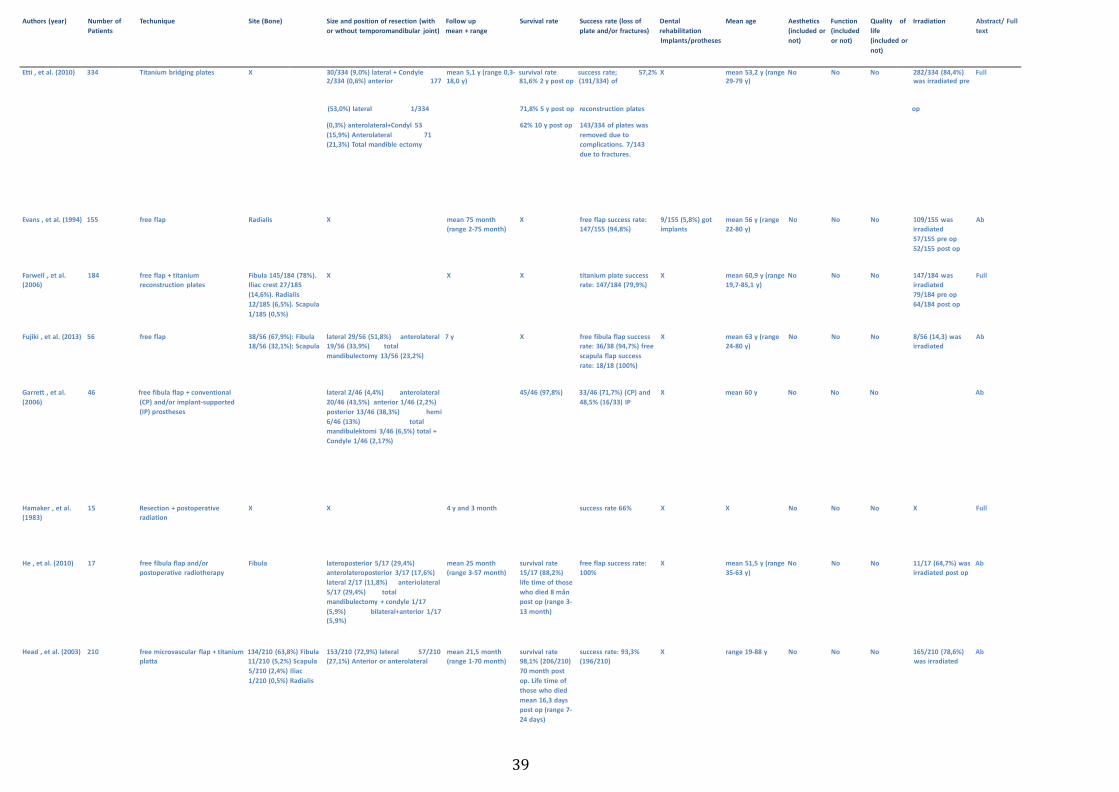
After manual review of the abstracts we sorted out the articles meeting our
exclusion/inclusion criteria. (See Figure 1: Process of selection)
Inclusion criteria
Published and reviewed examined human studies on patients who have
undergone segmental resection of the mandible as part of treatment of cancer
in the head and neck area. The studies needed to be published in scientific
journals with a review system to be included. Articles (at least the abstracts)
must be published in English.
Exclusion criteria
Case reports and articles with less than 10 patients, patients with known
comorbidity, ex. HIV and Diabetes and Rim resections.
Data extraction
One hundred and eight of the 208 articles did not fulfill the inclusion criteria and
were excluded. The 100 remaining articles were reviewed by the two reviewers
independently. During the review, data extraction was performed and data was
placed in a database created in Excel. Data about function, aesthetics and

8
quality of life was excluded in table 2, due to a very large amount of information
that was not suitable to present in that format.
We extracted information out of the articles using the following variables:
Author, article type (full text or abstract), publication year, number of patients,
average age, sex, type of operation, reconstruction technique (Plate,
Vascularized bone graft or non-vascularized bone graft), origin of bone grafts,
size of the resection, success rate of reconstruction, postop follow-up, survival
rate, dental rehabilitation, aesthetics, function, QOL, and radiation or not. If
information could not be contained in an article it was not included in the
summation of the current variable. Along with the data extraction and full text
review, a second exclusion was done and additionally, 11 articles were excluded
as these did not meet the criteria. All variables where later summarized.
Ethical consideration
Since this is a literature study, all data will be reported anonymously. There is no
possibility for personal identification which excludes ethical problems.
RESULTS
Literature review
Out of the 89 included articles, 60 were in full text and 29 were abstracts. The
large numbers of abstracts were the result of articles without full text in English
or articles published back in time before the start of publications on the internet.
The median year of publication was 2006 (range 1977 – 2013).
A total of 5629 patients were included in the study. Of these, 3783 patients were
included in articles that had categorized by gender and we found that 65.4%
were males and 34.6% were females (mean age 52.6 years, range 5 month’s –
88 years of age).

9
The overall success rate (the number of reconstructions with no or minor
complications, that did not need further surgery or to be redesigned) for
reconstruction in the groups; vascular, non-vascular and plate were extracted
from 62 unique articles. The success rate was 86.4% in 3219 patients, with a
range from 70.4% in the plate group to 92.3% in the non-vascular group. Of the
articles included; 59 articles published data about follow up time. The mean
follow up time were 46.9 months (range 0.2 – 216 months).
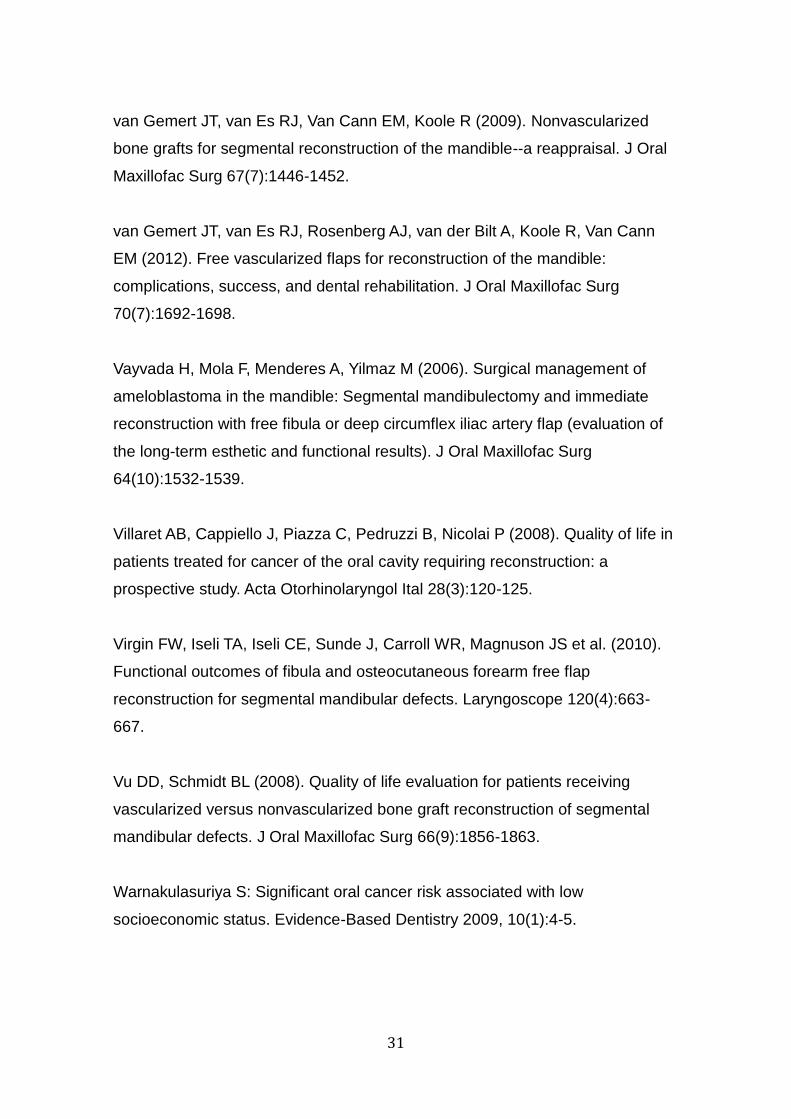
Size and position of the segmental resection of the mandible
Of the included articles; 51 published data about mandibular resection. Two
perspectives on this subject can be recognized. While some of the included
articles report the size of the resection, other articles talk about the location of
the resection. Twenty articles published data about the size and 31 articles
published data about the site of the resection. Three of the included articles
published data of both the size and location of the resection.
The size of resection ranged from 2 to 26 cm with a mean value of
approximately 8.1 cm. The mean values ranged from 6.7 cm in the first quartile
to 8.9 cm in the last quartile, ie half of the participants had a reconstruction size
comprising between these two values.
The site of the resection varies depending on the location of the cancer, but is
also related to the extent of the tumour. The extent of the resection is dependent
on type and size of the malignancy and the approach of the surgeon. Based on
data extracted from the 31 articles (2029 patients), the most commonly found
mandibular site of resection is the lateral part of the mandible with 43.1% of the
cases. Next comes the anterior-lateral part (16.1%) followed by the anterior-
lateral-posterior (11.4%) site of removal. The fourth most common site of
resection is the removal of the anterior part of the mandible which was carried
out in 9.3% of the cases. A resection of the mandibular condyle was performed
in 7.2% of cases. A very small proportion (0.1%) was reported to have the
resection localized lateral-posterior.

10
Reconstruction
After segmental resection of the mandible, a reconstruction of the resected area
is usually performed. Our statistics about the three different reconstruction
methods can be viewed in Tabel 2: Results of reconstruction.
Vascular reconstruction
Of the articles included; 15 unique articles explored the outcome of vascular
reconstruction (some articles investigate 2 or more techniques).
A total of 641 patients were reconstructed with a success rate of 90.6%, with a
range from 83.3% to 94.3%. The most common graft site were Fibula, used in
393 reconstructions. Fibula was also the most publicized graft site with 11
articles. The most successful graft site were Scapula with a success rate of
94.3%.
Non vascular reconstruction
Of the articles included; 31 unique articles explored the outcome of non-
vascular reconstruction (some articles investigate two or more techniques).
A total of 1764 patients were reconstructed with a success rate of 92.3%, with a
range from 89.5% to 100%. The most common graft site in non-vascular
reconstruction was fibula, used in 1195 reconstructions. Fibula was also the
most publicized graft site with 28 articles. The most successful graft site was
Ilium with 100%.
Plate
Of the articles included; 16 unique articles explored the outcome of plate
reconstruction. All plates that did not include a graft of bone were included in the
group plate. A total of 814 patients were reconstructed with a success rate of
70.4%.
Dental rehabilitation
Of the articles included; 29 articles reported about dental rehabilitation.

11
A total of 1425 patients were included. Of these patients, 467 received dental
rehabilitation with removable prosthesis or implants. Implants were the most
common treatment option with 87.6% of the 467 patients.
Irradiation
Of the articles included; 38 articles discussed radiation as an adjuvant therapy
to surgery in the treatment of cancer of the mandible. 62.4%, or 1605 of a total
of 2573 patients received radiotherapy as adjuvant therapy to surgery. Of these
1605, 500 (31%) patients received radiotherapy preoperatively, while 415 (26%)
received radiation therapy postoperatively. For the other 690 (42.9%) patients
who received radiotherapy the time was not specified including a very small
proportion (n = 12, ie, 0.8%) who received radiotherapy, both preoperatively and
postoperatively.
Patient survival rate
We sorted the material from the articles and created three groups. First group; 1
year survival or less; five articles reported a total of 566 patients with a survival
rate of 86.0% (range 74-95%). The patient´s cancer types were: 519 malign
tumors, 0 benign tumors and 47 were undefined.
Second group; 2-4 years of survival; 19 articles reported a total of 1524 patients
with a survival rate of 70.4% (range 50-100%). The patient’s cancer types were:
1033 malign tumors, 138 benign tumors and 283 were undefined.
Third group: 5 years of survival or more; 14 articles reported a total of 1089
patients with a survival rate of 71.8% (range 40-100%). The patient´s cancer
types were: 674 malign tumors, 119 benign tumors and 366 were undefined.
Aesthetics
Of the articles included; 22 articles investigated the aesthetic outcome of
restorations after the treatment of cancer. Thirteen articles featured useful
statistical data with quite varying results regarding the perceived aesthetic level

12
of the patients. This is exemplified by Young et al. (2007) reporting less than
30% of patients have gained an acceptable appearance compared with other
studies in which over 95% were considered to have gained an acceptable
appearance (Patel et al., 1996; Politi et al., 2012).
Function
Of the articles included; 30 articles investigated the functional outcome of
restorations after treatment. Fourteen of these articles presented statistics
about the subject.
The oral function can include many areas, such as the ability to speak and eat.
Three of the 14 articles examined the proportion of patients who had received a
normalized speaking ability. These articles showed that approximately 75% of
patients regained normal speech ability (range 36%-100%).
Nine of the 14 articles examined the proportion of patients who had received a
normalized eating ability, which includes the ability to chew and swallow.
Only seven of these articles presented statistics on both of these functions. Two
of the articles presented statistics only about the ability to chew. The studies
show that half of the patients regained the ability to swallow (58.8%, range 25.8
-81%) and chew (53.1% 25.4 – 81%).
Limitations in the ability to eat mean that the food must be modified in order to
be eaten. Seven of articles have looked at the type of food that patients can eat.
In these studies it can be seen that the patients were divided into four different
groups, those who can eat solid / regular food, those who tolerate soft foods,
those who can only eat liquid food, and those who are dependent on tube
feeding. These studies showed that almost half of the patients (48.6%) regained
the ability to eat a regular diet (Range 25.8 – 65%) and slightly fewer than half
of the patients tolerated soft food (42.9%, range 22.7 – 94%). Ten percent of the
patients could only ingestion liquid food (range 0.9 -27.3%) and 9.8% were
dependent on tube feeding (range 5 -15.9%).

13
Quality of life
Of the articles included; four articles investigated the quality of life (QOL) after
cancer treatment. Factors examined included the extent to which the mental
and physical well-being had been affected by the cancer treatment. Young et al.
(2007) came to the following; of their patient population (26 patients), 58%
stated that their wellbeing was good. Sixty five percent reported that their mood
was positive and 77% stated that they did not feel physical pain. Boffano et al.
(2011) indicated that 70% of their patients (total 10 patients) had retained the
sensory function of the nervus alveolaris inferior. Dholam et al. (2011) did a
statistical analysis of speech, swallowing parameters and quality of life and
found no significant difference because of the paucity of numbers. Garrett, et al.
(2006) looked at how facial appearance affected the social life and came up
with the following conclusions; the patients satisfaction with facial appearance
was approximately 65% both prior to and after surgery. On the question about if
appearance affect social life, approx. 85% said this was a fact prior to resection.
Postoperatively approximately 75% stated this as a fact.
DISCUSSION
This review examined the literature about mandibular reconstruction after
cancer treatment with segmental resection. Main focus has been to examine
success rate for the reconstructions, patient survival rate, dental rehabilitation
and how this effects the patients QOL, oral function and aesthetics.
Of the 89 articles, 60 articles were in full text. In the remaining 29 articles, only
the abstract could be reviewed due to difficulties in interpreting these on their
original language. Though we cannot evaluate the scientific level of evidence in
these articles, all of the articles have been published in scientific journals and
therefore they have been controlled by a review group. We have chosen to trust
the validity of these review groups, due to the fact that their function is to
evaluate the validity of articles before publication in reputable scientific journals.
We found that there is no major difference in success rate between vascularized

14
bone vs. non- vascularized bone transplants for method of reconstruction. Our
findings with a success rate of 90-92% for bone transplants lies roughly in line
with other research done on the subject. However, recent studies have shown
success rates up to 96% on mandibular reconstructions (Virgin et al., 2010). We
found that the reconstruction method using only plate had a lower frequency of
success than the other two methods using bone transplant. Why plate have a
lower success rate could be explained by the risk of penetration through soft
tissue due to high friction between plate and the mucosa. If radiation is given, it
creates fibrosis making the soft tissue even more sensible. Another known
reason for failure is plate fracture during heavy loading. The plate technique
was more common back in time. Today it is mostly used in patients with spread
cancer with bad prognosis and who have a lateral defect of the mandible. The
plate reconstruction is less invasive for the patient (less blood loss, shorter time
in surgery), why it´s still used in this patient group (Miyamoto et al., 2012).
Some of the patients don’t get any reconstructive therapy at all, mostly due to
bad tumor prognosis.
Fibula is the most common donor site in both the vascularized and non-
vascularized groups. The use of fibula over other bone transplants can be
explained by; easy access and the possibility to reconstruct major resections
due to its length, although the use of Iliac and other donor sites is increasing.
The disadvantage of fibula against Iliac, which is the second most common
donor site, is that Iliac have a more suitable height that can better facilitates
implant placement.
Although we have a large patient material, interpretation of the success rate
should be done with caution because the follow up time varies widely between
the studies, from one week to 216 months.
The average age of the 5629 patients included in our study is 52.6 years. The
age variation is however very great. In some studies exists individuals younger
than a year old, while in other studies exists individuals who are nearly ninety

15
years old. This large variation in age is explained by; the fact that the material
studied is extensive and includes many different types of tumors, which is age
related. As an example, we have studies on children (Benoit et al., 2013) where
the mean age was eight years.
Another study, Boffano et al. (2011) with low average age of the patients, had
odontogenic myxoma as diagnose and this tumor mostly affects young adults
(Barros et al., 1969). Another study (Puxedduet et al., 2004) had a much higher
average age of the participants with a mean age of 62.5 years. All participants
in this study had been diagnosed with squamous cell carcinoma, a form of
tumor that usually affects people over the age of 50 (Chen et al., 1999).
In our study we concluded that 65.4% were males and 34.6% were females.
The fact that the gender distribution looks like this in our study can be supported
by the fact that oral cancer affects more men than women. Rosenquist et al.
(2005) showed that men were over-represented when a total of 91 men,
compared with 41 women were subjected to oral and oropharyngeal squamous
cell carcinoma. This corresponds to 68.9% men and 31.1% women, which is
close to the gender distribution we have seen in our study.
In our study, we have chosen not to include articles in which co-morbidity, such
as Diabetes Mellitus noted to occur in the population studied. We have chosen
to do so because this can be assumed to affect the statistics relating the
survival of patients or the success rate of free flaps and implants. We can,
however not, ignore that there are probably individuals in the studies we have
selected, who have other diseases as well, such as Diabetes Mellitus. This is a
relatively common disease that also appears to increase the risk of oral cancer.
Diabetes can cause inflammatory lesions in the oral mucosa. A correlation
between oral lesions in diabetic patients and a higher risk for premalignant
status is supported by studies, for example, a study of Ujpál et al. (2004) and
Goutzanis et al. (2007). The probability that Diabetes Mellitus is represented
among the individuals in our study is therefore quite high.

16
The degree of malignancy of the tumors shows great diversity in our review.
This is shown in studies discussing the use of radiation therapy as part of
treatment and the size of the mandibular resection performed.
Puxeddu et al. (2004) reported that all participants had squamous cell
carcinoma, the size of the resection was 6.9 cm (range 5.2 to 9 cm), and the
survival rate of the patients was 50% at study end. The proportion that received
adjuvant radiation therapy in this study was 75%. On the other hand, Chaine et
al. (2009) reported a study where all participants had giant mandibular
ameloblastoma. The size of the resection was 12 cm (range 7-16 cm) and the
survival rate was 100% at study end. If radiotherapy was a part of the therapy
was not specified by Chaine et al. However, the patients were probably not
given radiotherapy, as this treatment normally is not used for this type of cancer
(Rosenstein et al., 2001).
The results we found on survival rate were better then we expected but we have
a sprawling patient materiel with various tumors. For example Lindqvist et al.
(1992) reported that patient survival was 20% at five year follow up for patients
with malign cancers stage III or IV. We found that studies with longer follow up
tended to have a higher proportion of patients with benign tumors, which could
explain the good survival rates in these groups. The range between the studies
that presented the best vs. the worst survival rates varied greatly in the groups.
In our data, some studies have been included although their main objective was
to check on implant survival. We believe that these articles probably have
chosen “healthy patients” for their study which results in a much higher survival
rate compared to a article that have a “random” group of reconstructed patients.
Our findings show that dental rehabilitation is not common. The articles that
brought up the subject included a total of 1425 patients. Only one third of these
patients received dental rehabilitation. The reason that so few individuals chose,
for example dental implant treatment can be explained by the fact, it´s a very
expensive treatment that is not state-subsidized in those parts of the world
where these studies where made (Zitzmann et al., 2005). Oral cancer is also
17
more common in people with low socioeconomic status (Warnakulasuriya,
2009). In these patients, it can be assumed that the ability to pay for expensive
dental restorations are lower than average for other patient categories which
explains why so few chose this treatment option. Another explanation for the
low percentage of patients who received implants may be to the fact that
implant treatment is invasive and time consuming.
Regarding QOL and aesthetics we found that more research needs to be done.
These topics are hard to evaluate because of its nature. There should also be
some kind of standardized question formulas and/or indexes so that comparison
between studies can be done. This kind of data should originate from the
patient and not be evaluated by the surgeon. Function is easier to measure in
some cases for example when you measure the ability eating solid food vs. tube
feeding dependent. It is harder to measure the ability to be understood through
speech, because it depends on the ability of the receiver to understand the
conversation. In our study we found that most of the patients regained their
ability to speech but the ability to chew and swallow was more affected, the
latter could be explained by the loss of teeth and loss of masticatory muscles
after segmental resection of the mandible. To strengthen this thesis more
studies needs to be done.
A small number of articles included in this review investigated the opinion about
aesthetic results after mandibular reconstruction. Our study indicates that the
vast majority of patients are satisfied with the aesthetic results after mandibular
reconstruction. However, the numbers of patients are too small to draw any
general conclusions regarding this subject.
ACKNOWLEDGEMENTS
We would like to express our gratitude’s to the following people. A special
thanks to our tutors Mats Sjöström and Linda Pettersson for their help and
guidance during the process of this study. We would also like to thank Lina
Holmström for helping us retrieving full-text studies not available on the internet.

18
REFERENCES
Full-text articles and abstracts (shown in square brackets) from articles
published in journals.
[Abler A, Roser M, Weingart D (2005). On the indications for and morbidity of
segmental resection of the mandible for squamous cell carcinoma in the lower
oral cavity. Mund Kiefer Gesichtschir 9(3):137-142.]
Adekeye EO (1980). Ameloblastoma of the jaws: a survey of 109 Nigerian
patients. J Oral Surg 38(1):36-41.
Anthony JP, Foster RD, Kaplan MJ, Singer MI, Pogrel MA (1997). Fibular free
flap reconstruction of the "true" lateral mandibular defect. Ann Plast Surg
38(2):137-146.
Aramany MA, Myers EN (1977). Intermaxillary fixation following mandibular
resection. J Prosthet Dent 37(4):437-444.
Arden RL, Rachel JD, Marks SC, Dang K (1999). Volume-length impact of
lateral jaw resections on complication rates. Arch Otolaryngol Head Neck Surg
125(1):68-72.
Aydin A, Emekli U, Erer M, Hafiz G (2004). Fibula free flap for mandible
reconstruction. Kulak Burun Bogaz Ihtis Derg 13(3-4):62-66.
Bak M, Jacobson AS, Buchbinder D, Urken ML (2010). Contemporary
reconstruction of the mandible. Oral Oncol 46(2):71-76.
[Barnard NA, Vaughan ED (1991). Osteosynthetic titanium mini-plate fixation of
composite radial forearm flaps in mandibular reconstruction. J Craniomaxillofac
Surg 19(6):243-248.]

19
Barros, R.E., Dominguez, F.V., Cabrini, R.L. Myxoma of the jaws(1969) Oral
Surgery, Oral Medicine, Oral Pathology, 27 (2), pp. 225-236.
Baumann DP, Yu P, Hanasono MM, Skoracki RJ (2011). Free flap
reconstruction of osteoradionecrosis of the mandible: a 10-year review and
defect classification. Head Neck 33(6):800-807.
Beecroft WA, Sako K, Razack MS, Shedd DP (1982). Mandible preservation in
the treatment of cancer of the floor of the mouth. J Surg Oncol 19(3):171-175.
Benoit MM, Vargas SO, Bhattacharyya N, McGill TA, Robson CD, Ferraro N et
al. (2013). The presentation and management of mandibular tumors in the
pediatric population. Laryngoscope. 123(8):2035-2042.
[Bianchi B, Ferri A, Ferrari S, Leporati M, Copelli C, Ferri T et al. (2013).
Mandibular resection and reconstruction in the management of extensive
ameloblastoma. J Oral Maxillofac Surg 71(3):528-537.]
Bilodeau EA, Chiosea S (2011). Oral squamous cell carcinoma with mandibular
bone invasion: intraoperative evaluation of bone margins by routine frozen
section. Head Neck Pathol 5(3):216-220.
Blackwell KE, Buchbinder D, Urken ML (1996). Lateral mandibular
reconstruction using soft-tissue free flaps and plates. Arch Otolaryngol Head
Neck Surg 122(6):672-678.
Blackwell KE, Lacombe V (1999). The bridging lateral mandibular
reconstruction plate revisited. Arch Otolaryngol Head Neck Surg 125(9):988-
993.
Boffano P, Gallesio C, Barreca A, Bianchi FA, Garzino-Demo P, Roccia F
(2011a). Surgical treatment of odontogenic myxoma. J Craniofac Surg

20
22(3):982-987.
Boffano P, Viterbo S, Barreca A, Berrone S (2011b). Pathologic mandibular
fracture as the presenting manifestation of multiple myeloma. J Craniofac Surg
22(4):1312-1315.
[Boyd JB, Mulholland RS, Davidson J, Gullane PJ, Rotstein LE, Brown DH et al.
(1995). The free flap and plate in oromandibular reconstruction: long-term
review and indications. Plast Reconstr Surg 95(6):1018-1028.]
Brown JS, Kalavrezos N, D'Souza J, Lowe D, Magennis P, Woolgar JA (2002).
Factors that influence the method of mandibular resection in the management
of oral squamous cell carcinoma. Br J Oral Maxillofac Surg 40(4):275-284.
Burkey BB, Hoffman HT, Baker SR, Thornton AF, McClatchey KD (1990).
Chondrosarcoma of the head and neck. Laryngoscope 100(12):1301-1305.
Cantu G, Bimbi G, Colombo S, Riccio S, Squadrelli M, Napoli U et al. (2009).
Autologous freeze-treated bone for mandibular reconstruction after malignant
tumor resection: a study of 72 patients. Am J Otolaryngol 30(6):383-389.
Carlson ER (2002). Disarticulation resections of the mandible: a prospective
review of 16 cases. J Oral Maxillofac Surg 60(2):176-181.
Chaine A, Pitak-Arnnop P, Dhanuthai K, Ruhin-Poncet B, Bertrand JC, Bertolus
C (2009). A treatment algorithm for managing giant mandibular ameloblastoma:
5-year experiences in a Paris university hospital. Eur J Surg Oncol 35(9):999-
1005.
[Chana JS, Chang YM, Wei FC, Shen YF, Chan CP, Lin HN et al. (2004).
Segmental mandibulectomy and immediate free fibula osteoseptocutaneous
flap reconstruction with endosteal implants: an ideal treatment method for
21
mandibular ameloblastoma. Plast Reconstr Surg 113(1):80-87.]
Chang SY, Huang JJ, Tsao CK, Nguyen A, Mittakanti K, Lin CY et al. (2010).
Does ischemia time affect the outcome of free fibula flaps for head and neck
reconstruction? A review of 116 cases. Plast Reconstr Surg 126(6):1988-1995.
Chang YM, Santamaria E, Wei FC, Chen HC, Chan CP, Shen YF et al. (1998).
Primary insertion of osseointegrated dental implants into fibula
osteoseptocutaneous free flap for mandible reconstruction. Plast Reconstr Surg
102(3):680-688.
Chen YK, H.C. Huang, L.M. Lin et al. Primary oral squamous cell carcinoma: An
analysis of 703 cases in southern Taiwan Oral Oncol, 35 (1999), p. 173
Choi, S., D. L. Schwartz, D. G. Farwell, M. Austin-Seymour, and N. Futran,2004,
Radiation therapy does not impact local complication rates after free flap
reconstruction for head and neck cancer: Arch Otolaryngol Head Neck Surg, v.
130, p. 1308-12.7
Coleman, H. and S. Sukumar, 2012, Malignant tumours of the jaws: SADJ, v.
67, p. 578-80.
Clayman L. Clinical controversies in oral and maxillofacial surgery: part two.
Management of dental extractions in irradiated jaws: a protocol without
hyperbaric oxygen therapy. J Oral Maxillofac Surg 1997; 55:275-281
Cordeiro PG, Disa JJ, Hidalgo DA, Hu QY (1999). Reconstruction of the
mandible with osseous free flaps: a 10-year experience with 150 consecutive
patients. Plast Reconstr Surg 104(5):1314-1320.
Dholam KP, Bachher GK, Yadav PS, Quazi GA, Pusalkar HA (2011).
Assessment of quality of life after implant-retained prosthetically reconstructed
22
maxillae and mandibles postcancer treatments. Implant Dent 20(1):85-94.
Disa JJ, Winters RM, Hidalgo DA (1997). Long-term evaluation of bone mass in
free fibula flap mandible reconstruction. Am J Surg 174(5):503-506.
[Disa JJ, Hidalgo DA, Cordeiro PG, Winters RM, Thaler H (1999). Evaluation of
bone height in osseous free flap mandible reconstruction: an indirect measure
of bone mass. Plast Reconstr Surg 103(5):1371-1377.]
Dor P (1980). [Complications of post-irradiation radiotherapy mandibular
resection: problems of reconstruction (author's transl)]. Acta Chir Belg 79(1):21-
26.
Dorfman, H. D., and B. Czerniak, 1995, Bone cancers: Cancer, v. 75, p. 203-10
Dumbach, J., H. Rodemer, W. J. Spitzer, and E. W. Steinhäuser, 1994,
Mandibular reconstruction with cancellous bone, hydroxylapatite and titanium
mesh: J Craniomaxillofac Surg, v. 22, p. 151-5.
Ettl T, Driemel O, Dresp BV, Reichert TE, Reuther J, Pistner H (2010).
Feasibility of alloplastic mandibular reconstruction in patients following removal
of oral squamous cell carcinoma. J Craniomaxillofac Surg 38(5):350-354.
[Evans GR, Schusterman MA, Kroll SS, Miller MJ, Reece GP, Robb GL et al.
(1994). The radial forearm free flap for head and neck reconstruction: a review.
Am J Surg 168(5):446-450.]
Farwell DG, Kezirian EJ, Heydt JL, Yueh B, Futran ND (2006). Efficacy of small
reconstruction plates in vascularized bone graft mandibular reconstruction.
Head Neck 28(7):573-579.

23
Francis, M., and G Lawrence , 2012, Bone Sarcoma Incidence and Survival:
NCIN, R12, p. 2-13.
[Fujiki M, Miyamoto S, Sakuraba M, Nagamatsu S, Hayashi R (2013). A
comparison of perioperative complications following transfer of fibular and
scapular flaps for immediate mandibular reconstruction. J Plast Reconstr
Aesthet Surg 66(3):372-375.]
[Garrett N, Roumanas ED, Blackwell KE, Freymiller E, Abemayor E, Wong WK
et al. (2006). Efficacy of conventional and implant-supported mandibular
resection prostheses: study overview and treatment outcomes. J Prosthet Dent
96(1):13-24.]
Gennaro, P., G. Gabriele, M. Della Monaca, A. Facchini, and V. Mitro, 2013,
Mandibular nerve fascicular cross-face for sensitive recovery after
mandibulectomy: A new technique: J Plast Surg Hand Surg, v. 47, p. 228-31.
Goutzanis L, Vairaktaris E, Yapijakis C, Kavantzas, Nkenke E, Derka S,
Vassiliou S, Acil Y, Kessler P, Stavrianeas N, Perrea D, Donta I, Skandalakis P,
Patsouris E: Diabetes may increase risk for oral cancer through the insulin
receptor substrate-1 and focal adhesion kinase pathway. Oral Oncol 43:165–
173, 2007
Group CSoO-HaNSOS (2004). Osteogenic sarcoma of the mandible and
maxilla: a Canadian review (1980-2000). J Otolaryngol 33(3):139-144.
Hamaker RC, Singer MI, Shockley WW, Pugh N, Shidnia H (1983). Irradiated
mandibular autografts. Cancer 52(6):1017-1021.
[He Y, Zhang ZY, Zhu HG, Sader R, He J, Kovacs AF (2010). Free fibula
osteocutaneous flap for primary reconstruction of T3-T4 gingival carcinoma. J

24
Craniofac Surg 21(2):301-305.]
[Head C, Alam D, Sercarz JA, Lee JT, Rawnsley JD, Berke GS et al. (2003).
Microvascular flap reconstruction of the mandible: a comparison of bone grafts
and bridging plates for restoration of mandibular continuity. Otolaryngol Head
Neck Surg 129(1):48-54.]
[Heller KS, Dubner S, Keller A (1995). Long-term evaluation of patients
undergoing immediate mandibular reconstruction. Am J Surg 170(5):517-520.]
[Hidalgo DA (1989). Fibula free flap: a new method of mandible reconstruction.
Plast Reconstr Surg 84(1):71-79.]
Hidalgo, D. A., and A. L. Pusic, 2002, Free-flap mandibular reconstruction: a 10-
year follow-up study: Plast Reconstr Surg, v. 110, p. 438-49; discussion 450-1.
Hirshberg, A., P. Leibovich, and A. Buchner, 1994, Metastatic tumors to the
jawbones: analysis of 390 cases: J Oral Pathol Med, v. 23, p. 337-41.
Hundepool AC, Dumans AG, Hofer SO, Fokkens NJ, Rayat SS, van der Meij EH
et al. (2008). Rehabilitation after mandibular reconstruction with fibula free-flap:
clinical outcome and quality of life assessment. Int J Oral Maxillofac Surg
37(11):1009-1013.
Iino M, Fukuda M, Nagai H, Hamada Y, Yamada H, Nakaoka K et al. (2009).
Evaluation of 15 mandibular reconstructions with Dumbach Titan Mesh-System
and particulate cancellous bone and marrow harvested from bilateral posterior
ilia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107(4):e1-8.
Irjala H, Kinnunen I, Aitasalo K (2012). Mandibular reconstruction using free
bone flap after preoperative chemoradiation. Eur Arch Otorhinolaryngol
269(5):1513-1518.

25
[Jeng SF, Kuo YR, Wei FC, Su CY, Chien CY (2005). Reconstruction of
extensive composite mandibular defects with large lip involvement by using
double free flaps and fascia lata grafts for oral sphincters. Plast Reconstr Surg
115(7):1830-1836.]
Jacobsen, C., A. Kruse, H. T. Lübbers, R. Zwahlen, S. Studer, W. Zemann, B.
Seifert, and K. W. Grätz, 2012, Is Mandibular Reconstruction Using
Vascularized Fibula Flaps and Dental Implants a Reasonable Treatment?: Clin
Implant Dent Relat Res.
Jham, B., A. R. Salama, S. A. McClure, and R. A. Ord, 2011, Metastatic tumors
to the oral cavity: a clinical study of 18 cases: Head Neck Pathol, v. 5, p. 355-8.
[Ji T, Zhang CP (2006). A retrospective study of 541 cases with segmental
resection of mandible. Zhonghua Kou Qiang Yi Xue Za Zhi 41(12):705-708.]
Julieron M, Germain MA, Schwaab G, Margainaud JP, Salvan D, Marandas P et
al. (1996). Free bone flaps in esthetic and functional rehabilitation after
segmental mandibulectomy. Apropos of 38 cases. Ann Otolaryngol Chir
Cervicofac 113(6):353-358.
Kadota C, Sumita YI, Wang Y, Otomaru T, Mukohyama H, Fueki K et al. (2008).
Comparison of food mixing ability among mandibulectomy patients. J Oral
Rehabil 35(6):408-414.
Kanchanarak, C., P. Sittitrai, and R. Charoensil, 1999, Mandibular
reconstruction: free flap vs AO plate: J Med Assoc Thai, v. 82, p. 126-30.
[Kim PD, Blackwell KE (2007). Latissimus-serratus-rib free flap for
oromandibular and maxillary reconstruction. Arch Otolaryngol Head Neck Surg
133(8):791-795.]

26
[Knott PD, Suh JD, Nabili V, Sercarz JA, Head C, Abemayor E et al. (2007).
Evaluation of hardware-related complications in vascularized bone grafts with
locking mandibular reconstruction plate fixation. Arch Otolaryngol Head Neck
Surg 133(12):1302-1306.]
[Koch WM, Yoo GH, Goodstein ML, Eisele DW, Richtsmeier WJ, Price JC
(1994). Advantages of mandibular reconstruction with the titanium hollow screw
osseointegrating reconstruction plate (THORP). Laryngoscope 104(5 Pt 1):545-
552.]
Koga DH, Salvajoli JV, Alves FA (2008). Dental extractions and radiotherapy in
head and neck oncology: review of the literature. Oral Dis 14(1):40-44.
Kovács A, Kiss G, Fehér A, Borbély L, Roszik M (1994). Radial forearm flap in
maxillo-facial surgery. Acta Chir Hung 34(3-4):365-374.
[Kroll SS, Schusterman MA, Reece GP (1992). Costs and complications in
mandibular reconstruction. Ann Plast Surg 29(4):341-347.]
[Kudo K, Shoji M, Yokota M, Fujioka Y (1992). Evaluation of mandibular
reconstruction techniques following resection of malignant tumors in the oral
region. J Oral Maxillofac Surg 50(1):14-21.]
Li L, Blake F, Heiland M, Schmelzle R, Pohlenz P (2007). Long-term evaluation
after mandibular reconstruction with fibular grafts versus microsurgical fibular
flaps. J Oral Maxillofac Surg 65(2):281-286.
[Lindqvist C, Söderholm AL, Laine P, Paatsama J (1992). Rigid reconstruction
plates for immediate reconstruction following mandibular resection for malignant
tumors. J Oral Maxillofac Surg 50(11):1158-1163.]

27
Louis MY, Rame JP, De Raucourt D, Mayaleh HA (2010). Revascularized free
scapular flaps in mandibular reconstruction. Report of 93 cases (April 1997 -
October 2009). Rev Laryngol Otol Rhinol (Bord) 131(4-5):263-268.
Lyons, A., Ghazali, N (2008). Osteoradionecrosis of the jaws: current
understanding of its pathophysiology and treatment. Br J Oral Maxillofac Surg
46(8):653-660.
[Malata CM, McLean NR, Alvi R, McKiernan MV, Milner RH, Piggot TA (1997).
An evaluation of the Würzburg titanium miniplate osteosynthesis system for
mandibular fixation. Br J Plast Surg 50(1):26-32.]
Maurer P, Pistner H, Schubert J (2006). [Computer assisted chewing power in
patients with segmental resection of the mandible]. Mund Kiefer Gesichtschir
10(1):37-41.
[Millsopp L, Brandom L, Humphris G, Lowe D, Stat C, Rogers S (2006). Facial
appearance after operations for oral and oropharyngeal cancer: a comparison
of casenotes and patient-completed questionnaire. Br J Oral Maxillofac Surg
44(5):358-363.]
Miyamoto S, Sakuraba M, Nagamatsu S, Kamizono K, Hayashi R (2012).
Comparison of reconstruction plate and double flap for reconstruction of an
extensive mandibular defect. Microsurgery 32(6):452-457.
Obiechina AE, Ogunlade SO, Fasola AO, Arotiba JT (2003). Mandibular
segmental reconstruction with iliac crest. West Afr J Med 22(1):46-49.
[Okoturo E, Ogunbanjo O, Akinleye A, Bardi M (2011). Quality of life of patients
with segmental mandibular resection and immediate reconstruction with plates.
J Oral Maxillofac Surg 69(8):2253-2259.]

28
Patel SG, Deshmukh SP, Savant DN, Bhathena HM (1996). Comparative
evaluation of function after surgery for cancer of the alveolobuccal complex. J
Oral Maxillofac Surg 54(6):698-703; discussion 703-694.
[Pellini R, Mercante G, Spriano G (2012). Step-by-step mandibular
reconstruction with free fibula flap modelling. Acta Otorhinolaryngol Ital
32(6):405-409.]
[Politi M, Toro C (2012). Iliac flap versus fibula flap in mandibular reconstruction.
J Craniofac Surg 23(3):774-779.]
Puxeddu R, Ledda GP, Siotto P, Pirri S, Salis G, Pelagatti CL et al. (2004). Free-
flap iliac crest in mandibular reconstruction following segmental
mandibulectomy for squamous cell carcinoma of the oral cavity. Eur Arch
Otorhinolaryngol 261(4):202-207.
Regezi JA, DA Kerr, RM Courtney Odontogenic tumors: an analysis of 706
casesJOralSurg,36(1978),pp.771–778
Rivas B, Carrillo JF, Granados M (2000). Oromandibular reconstruction for
oncologicalpurposes.AnnPlastSurg44(1):29-35.
Robey AB, Spann ML, McAuliff TM, Meza JL, Hollins RR, Johnson PJ (2008).
Comparison of miniplates and reconstruction plates in fibular flap reconstruction
of the mandible. Plast Reconstr Surg 122(6):1733-1738.
Rogers SN, Devine J, Lowe D, Shokar P, Brown JS, Vaugman ED (2004).
Longitudinal health-related quality of life after mandibular resection for oral
cancer: a comparison between rim and segment. Head Neck 26(1):54-62.
29
Rosenstein T, MA Pogrel, RA Smith, JA. Regez.Cystic ameloblastoma-behavior
and treatment of 21 cases. J Oral Maxillofac Surg, 59 (2001), pp. 1311–1316.
Rosenquist K. Risk factors in oral and oropharyngeal squamous cell carcinoma:
a population-based case-control study in southern Sweden. Swed Dent J
Suppl2005; 179: 1–66.
Sarukawa S, Noguchi T, Oh-iwa I, Sunaga A, Uda H, Kusama M et al. (2012).
Bare bone graft with vascularised iliac crest for mandibular reconstruction. J
Craniomaxillofac. Surg. 40(1):61-66.
Schliephake H, Schmelzeisen R, Husstedt H, Schmidt-Wondera LU (1999).
Comparison of the late results of mandibular reconstruction using
nonvascularized or vascularized grafts and dental implants. J Oral Maxillofac
Surg 57(8):944-950; discussion 950-941.
Schrag, C., Y. M. Chang, C. Y. Tsai, and F. C. Wei, 2006, Complete rehabilitation
of the mandible following segmental resection: J Surg Oncol, v. 94, p. 538-45.
Shibahara, T., H. Noma, Y. Takasaki, T. Nomura, and M. Fujikawa, 1999, Repair
of the mandibular nerve by autogenous grafting after ablative surgery of the
mandible: Bull Tokyo Dent Coll, v. 40, p. 1-6.
Shpitzer T, Gullane PJ, Neligan PC, Irish JC, Freeman JE, Van den Brekel M et
al. (2000). The free vascularized flap and the flap plate options: comparative
results of reconstruction of lateral mandibular defects. Laryngoscope
110(12):2056-2060.
Simon EN, Merkx MA, Kalyanyama BM, Shubi FM, Stoelinga PJ (2013).
Immediate reconstruction of the mandible after resection for aggressive
odontogenic tumours: a cohort study. Int J Oral Maxillofac Surg 42(1):106-112.

30
Suh JD, Blackwell KE, Sercarz JA, Cohen M, Liu JH, Tang CG et al. (2010).
Disease relapse after segmental resection and free flap reconstruction for
mandibular osteoradionecrosis. Otolaryngol Head Neck Surg 142(4):586-591.
Söderholm AL, Lindqvist C, Laine P, Kontio R (1988). Primary reconstruction of
the mandible in cancer surgery. A report of 13 reconstructions according to the
principles of rigid internal fixation. Int J Oral Maxillofac Surg 17(3):194-197.
Teng, M. S., and N. D. Futran, 2005, Osteoradionecrosis of the mandible: Curr
Opin Otolaryngol Head Neck Surg, 13:217-21.
[Trignano E, Fallico N, Faenza M, Rubino C, Chen HC (2013). Free fibular flap
with periosteal excess for mandibular reconstruction. Microsurgery. 33(7):527-
533]
Tsuchiya S, Nakatsuka T, Sakuraba M, Kimata Y, Sakurai H, Nakagawa M et al.
(2013). Clinical factors associated with postoperative complications and the
functional outcome in mandibular reconstruction. Microsurgery 33(5):337-341.
[Ueyama Y, Naitoh R, Yamagata A, Matsumura T (1996). Analysis of
reconstruction of mandibular defects using single stainless steel A-O
reconstruction plates. J Oral Maxillofac Surg 54(7):858-862; discussion 862-
853.]
Ujpál M, O. Matos, G. Bíbok, A. Somogyi, G. Szabó, Z. Suba (2004) Diabetes
and oral tumors in Hungary. Epidemiological correlations Diabetes Care, 27:770–
774
Urken ML, Buchbinder D, Weinberg H, Vickery C, Sheiner A, Parker R et al.
(1991). Functional evaluation following microvascular oromandibular
reconstruction of the oral cancer patient: a comparative study of reconstructed
and nonreconstructed patients. Laryngoscope 101(9):935-950.
31
van Gemert JT, van Es RJ, Van Cann EM, Koole R (2009). Nonvascularized
bone grafts for segmental reconstruction of the mandible--a reappraisal. J Oral
Maxillofac Surg 67(7):1446-1452.
van Gemert JT, van Es RJ, Rosenberg AJ, van der Bilt A, Koole R, Van Cann
EM (2012). Free vascularized flaps for reconstruction of the mandible:
complications, success, and dental rehabilitation. J Oral Maxillofac Surg
70(7):1692-1698.
Vayvada H, Mola F, Menderes A, Yilmaz M (2006). Surgical management of
ameloblastoma in the mandible: Segmental mandibulectomy and immediate
reconstruction with free fibula or deep circumflex iliac artery flap (evaluation of
the long-term esthetic and functional results). J Oral Maxillofac Surg
64(10):1532-1539.
Villaret AB, Cappiello J, Piazza C, Pedruzzi B, Nicolai P (2008). Quality of life in
patients treated for cancer of the oral cavity requiring reconstruction: a
prospective study. Acta Otorhinolaryngol Ital 28(3):120-125.
Virgin FW, Iseli TA, Iseli CE, Sunde J, Carroll WR, Magnuson JS et al. (2010).
Functional outcomes of fibula and osteocutaneous forearm free flap
reconstruction for segmental mandibular defects. Laryngoscope 120(4):663-
667.
Vu DD, Schmidt BL (2008). Quality of life evaluation for patients receiving
vascularized versus nonvascularized bone graft reconstruction of segmental
mandibular defects. J Oral Maxillofac Surg 66(9):1856-1863.
Warnakulasuriya S: Significant oral cancer risk associated with low
socioeconomic status. Evidence-Based Dentistry 2009, 10(1):4-5.

32
[Young CW, Pogrel MA, Schmidt BL (2007). Quality of life in patients
undergoing segmental mandibular resection and staged reconstruction with
nonvascularized bone grafts. J Oral Maxillofac Surg 65(4):706-712.]
Zachariades N, 1989, Neoplasm metastatic to the mouth, jaws and surrounding
tissues: J Craniomaxillofac Surg, v. 17, p. 283-90.
Zender CA, Mehta V, Pittman AL, Feustel PJ, Jaber JJ (2012). Etiologic causes
of late osteocutaneous free flap failures in oral cavity cancer reconstruction.
Laryngoscope 122(7):1474-1479.
Zenn MR, Hidalgo DA, Cordeiro PG, Shah JP, Strong EW, Kraus DH (1997).
Current role of the radial forearm free flap in mandibular
reconstruction. Plast Reconstr Surg 99(4):1012-1017.
Zhang Y, Zhang J, Yu G (1999). Long-term complications associated with
immediate plate reconstruction for mandibular defect following tumor-surgery.
Zhonghua Kou Qiang Yi Xue Za Zhi 34(4):205-207.
Zitzmann NU, Sendi P, Marinello CP (2005). An economic evaluation of implant
treatment in edentulous patients - Preliminary results. Int J Prosthodont
18(1):20-27.

33
Table 1: Search strategy.
Database Search details Hits Selected
articles
PubMed (“mandibular reconstruction”[MeSH Terms] OR
(“mandibular”[All Fields] AND “reconstruction”[All Fields]) OR
“mandibular reconstruction”[All Fields]) AND segmental[All
Fields] AND (“neoplasms”[MeSH Terms] OR “neoplasms”[All
Fields] OR “cancer”[All Fields])
208 208

34
Table 2: Results of reconstruction.
VASCULAR Patients Success Failure Success rate Number of articles
Fibula 393 355 38 90.33% 11
Radialis 60 50 10 83.33% 7
Iliac 71 66 5 92.95% 7
Scapula 106 100 6 94.33% 3
Rib 11 10 1 90.90% 2
TOTAL 641 581 60 90.63% 15 Unique
NON VASCULAR Patients Success Failure Success rate Number of articles
Fibula 1195 1101 94 92.13% 28
Radialis 315 293 22 93.01% 11
Iliac 172 154 18 89.53% 11
Scapula 46 45 1 97.82% 8
Rib 30 29 1 96.66% 2
Ilium 6 6 0 100,00% 2
TOTAL 1764 1628 136 92.29% 31 Unique
PLATE Patients Success Failure Success rate Number of articles
Plate 814 573 241 70.40% 16
TOTAL 814 573 241 70.40% 16 Unique
OVERALL TOTAL 3219 2782 437 86.42% 62

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
35
Baumann , et al. 63 43/63 (68,3%) of the patients was fibula 37 radial 2 Segmental defect with intact condyle mean 18,2 month 52/63 (82,5%) 32 1/27 (3,7%) segmental X mean 61 y (range No Yes No
(2011)
recontstructed with bone flap iliac 4
27. Posterior or hemi (range 3-72 month) month post op. bony defect lost the
29-88 y) resection with resection of condyle
36
11/63 (17,5%) implant 3/36 died after, mean (8,3%) posterior or hemi
8 month post op resection lost the
(range 3-32 implant
month).
Table 3: The database.Abler , et al. (2005) 152 (112 had
segmental
resection)
Reconstruction plate X X x x x x No No No x Ab
Adekeye , et al. 109 autogenous bone grafts or a X X 8y 67,9% (74/109) 8y The bone transplants x X No No No X Full
(1980)
Bowerman-Conroy prosthesis
post op had 100% succesrate.
Anthony , et al. 17 free flap Fibula mean 6,3 cm (range 2,5-9 cm) 5,5 y 12/17 (70,6%) 21 82,4% (14/17) 3/17 71% dental mean age 54 y Yes Yes No 92% was irradiated Full
(1997) m post op (18%) fracture plate, rehabilitation (35% (range 29-76 y)
malocklusion in form of
osseointegrated
implants.)
Aramany , et al.
(1977)
17 immediate intermaxillary fixation X X X X X X X No No No X Full
Arden , et al. (1999) 31 30 patients; stainless steel plate mean 5,4 cm (range 3-10cm) 7 y X 83,9% (26/31) Success X mean 57 y (range No Yes No 100% was Full
and 1 patient; Vitallium plate
rates. 5/31 (16,1%)
41-76 y)
irradiated preop 6
Complications; fractured
post op 25
plate.
Aydin , et al. (2004) 21 7 patients free osseous flap and
14 patients free osteocutaneous
flap.
Fibula X 5 y 20/21 95,2% 5 y
post op.
95,2% (20/21) success
rate
X mean 41 y (range
22-58 y)
No No No 100% was
irradiated post op
Full
Barnard , et al.
(1991)
30 free flap radial forearm X 4 y X X X X No No No X Ab
Full
Beecroft , et al. 34 marginal mandibula resection X X 15 y 5-year survival: X X X No No 5 X Full
(1982)
84%
Benoit , et al. 13 free tissue transfer 7/13 (53,8%): combined Hemi mandibula ectomy: 9/13 mean 32,8 month Survival rate; X X mean 8 y (range 5 No No No 53,8% was Full
(2013)
musculocutaneous flap (69,2%) Marginal/segmental (range 0,2-124 month) 10/13 (76,9%)
month - 18 y
irradiated
and plate, mandibula ectomy 3/13 (23,1%) 32,8 mån post op.
1/13 (7,7%): regional Total mandibula ectomy 1/13 (7,7%) Mean time alive
tissue + plate
post op of those
5/13 (38,5%):
who died; 47,6

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
36
osteocutaneous free
month
tissue transfer.

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
37
Bianchi , et al. 31 free flap 14/31 (45,2%) Iliac mean 5,6 cm (range 3,5-12,5 cm) mean 53,6 month 31/31 X 25/31 (80,6%) X No No No X Ab (2013)
17/31 (54,8%) Fibula
(range 18-120 month)
endosteal dental
implants. 100%
success rate
Bilodeau , et al.
(2011)
27 Segmental mandibula ectomy X mean 8,5 cm (range 5,3-11 cm) X X X X mean
men/women: 55/66 y
No No No X Full
Blackwell , et al. 15 soft-tissue free flaps + plate 11/15 (73,3%): Radialis X X X success rate; 15/15 X X No No No 100% was Full
(1996)
(titanium (14/15) or stainless 2/15 (13,3%): rectus
(100%) for micro-
irradiated
steel (1/15) abdominis 1/15 (6,7%):
vascular free tissue
scapular and
transfer.
parascapular 1/15
Overall success rate for
(6,7%): lateral arm flap
plate 11/15 (73,3%) 1 y
post op.
Blackwell , et al. 27 free flap + plate radialis free flap: 21/27 x mean 19,5 month survival rate; success rate 25/27 X mean 65 y (range No No No 23/27 was Full
(1999)
(77,8%)
23/27 (85,2%) (92,6%) 19,5 month post
32-88 y)
irradiated Preop
rectus free flap: 6/27
18,7 month post op. With new type of
(n=5) Post
(22,2%)
op. low-profile MRP (plate)
op (n=17) Pre+post
Mean time alive in comparison with the
op (n=1) No
of those who died MRP used by Blackwell
irrradiation (n=4)
17,3 month post 1996 when the success op rate was 73,3%)
Boffano , et al. 10 free flap iliac: 5/10 (50%) Pre-molar region: 2 Molar mean 67,3 month 100% 165 month X X mean 40,1 y (range No No Yes X Full
(2011)
non 3/10 (30%) (lesions region: 7 Paramedian (range 12-165 month) post op
20-55 y)
<3cm), region: 1 mean size 3,85 cm
other: 2/10 (20%) (range 2-5 cm)
(maxilla)
Boyd , et al. (1995) 71 free flap: 31 100% radialis X X X success rate X X No No No X Ab
radial forearm osteocutaneous
total; 78,9% mandibular
flap 15, radial fasciocutaneous
defects anterior
flap 16 free
positioned 65% lateral
flap + Plate: 40 Plate 40
positioned 95%
Brown , et al.
(2002)
65 X X X X X X X X No No No X Full
Burkey , et al. 14 X X X X survival rate; 70% X X X No No No X Full
(1990)
3,5 y post op
Canadian Society of 35 X X X X survival rate 79% X X mean 40 y (range No No No X Full
Otolaryngology-
2 y post op and
14-76 y) Head and Neck
57% 5 y post op
Surgery Oncology Study Group (2004)

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
38
Cantu , et al. (2009) 72 X Autologous freeze- Anterior or Anterior-Lateral: 35/72 14 y survuval rate success rate total; 41/72 X mean 58 y (range 4 Yes No No 26/72 was Full
treated mandibular (48,6%)
32/72 (44,4%) 5 y (56,9%) 1-10 month post 77)
irradiated
bone lateral: 37/72 (51,4%)
post op. op. laterala resections 75,7% anteriora
resections 37,1%
Carlson , et al.
(2002)
16 bone graft (7/16=43,8%) plate +
condylar prosthesis
X 15/16 (93,8%): Disarticulation
resection of mandible
8 y survival rate
14/16 (87,5%)
success rate 15/16
(93,8%)
X X Yes Yes No X Full
Chaine , et al. 44 segmental mandibulectomy + Fibula mean 12 cm (range 7-16 cm) 55,6% mean 53 month survival rate success rate: 88,9% 22,2% got dental mean 35 y (range No No No X Full
(2009)
Free osteocutaneous flap
hemimandible 22,2% total (range 26-73 month) 100% 73 month
implants 18-70 y)
mandibulectomy 22,2%
post op
lateral+frontal mandible
Chana , et al. (2004) 13 free fibula flap + osseointegrated X mean 8,8 cm (range 4,5-13 cm) mean 40,1 month survival rate success rate 13/13 100% 40 month mean 32 y (range No No No X Ab
implants
(range 18-70 month) 100% 70 month (100%) post op (range 18- 17-50 y)
post op
70 month)
Chang , et al. (1998) 12 Fibula osteoseptocutaneous flap Fibula mean 8,1 cm mean 25 month X success rate 12/12 success rate 12/12 mean 36,3 y (range No No No X Full
+ osseointegrated implants (range 1-47 month) (100%) 25 month post
op
(100%) 25 mån post 17-65 y)
op
Chang , et al. (2010) 114 free fibula flap Fibula mean 8,9 cm (range 3-26 cm) 25 month X success rate 98,3% X mean 49,5 y (range No No No X Full
12-85 y)
Cordeiro , et al. 150 free flap + plate and titanium Fibula: 135/150 (90%) 43% hemi mandibular defek t 25% 10 y X free flap success rate: 20/150 (13,3%) mean 50 y (range 3 Yes Yes Yes X Full
(1999)
screws (98% of cases) Radius 6/150 (4%) lateral and 32%
100% osseo-integrated 79 y)
Scapula 6/150 (4%) frontal
dental implants
Ilium 3/150 (2%)
Dholam , et al. 12 free fibular graft Fibula survival rate success rate 63%. Yes Yes Yes 8/12 was Full
(2011)
11/12 (91,7%). 18 month post op
irradiated
Disa , et al. (1997) 27 free fibula flap Fibula 16/27 (59,3%) anterior 11/27 mean 54 month X free flap success rate: 6/27 (22,2%) got mean 43 y (range No No No 10/27 (37%) was Full
(40,7%) lateral. (range 24-104)
93% osseointegrated
dental implants
14-65)
irradiated
6/10 (60%) Preop
4/10 (40%) Post
op.
Disa , et al. (1999) 48 Free osseous flap fibula 35/48 (72,9%) 24/48 (50%) anterior 24/48 mean 47 month X free flap success rate: 17/48 (35,4%) got mean 45 y (range 5 No No No 10/48 (20,8%) was Ab
radius 6/48 (12,5%)
scapula 4/48 (8,3%)
ilium 3/48 (6,3%)
(50%) lateral (range 24-104 month)
97% osseointegrated
dental implants
75 y)
irradiated
6/10 (60%) pre op
4/10 (40%) post op
Dor , et al. (1980) 126 X X X X X X X X No No No X Full
Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
39
Etti , et al. (2010) 334 Titanium bridging plates X 30/334 (9,0%) lateral + Condyle mean 5,1 y (range 0,3- survival rate success rate; 57,2% X mean 53,2 y (range No No No 282/334 (84,4%) Full
2/334 (0,6%) anterior 177 18,0 y) 81,6% 2 y post op (191/334) of
29-79 y)
was irradiated pre
(53,0%) lateral 1/334 71,8% 5 y post op reconstruction plates op
(0,3%) anterolateral+Condyl 53
(15,9%) Anterolateral 71
(21,3%) Total mandible ectomy
62% 10 y post op 143/334 of plates was
removed due to
complications. 7/143
due to fractures.
Evans , et al. (1994) 155 free flap Radialis X mean 75 month X free flap success rate: 9/155 (5,8%) got mean 56 y (range No No No 109/155 was Ab
(range 2-75 month)
147/155 (94,8%) implants 22-80 y)
irradiated
57/155 pre op
52/155 post op
Farwell , et al. 184 free flap + titanium Fibula 145/184 (78%). X X X titanium plate success X mean 60,9 y (range No No No 147/184 was Full
(2006)
reconstruction plates Iliac crest 27/185
rate: 147/184 (79,9%)
19,7-85,1 y)
irradiated
(14,6%). Radialis
79/184 pre op
12/185 (6,5%). Scapula
64/184 post op
1/185 (0,5%)
Fujiki , et al. (2013) 56 free flap 38/56 (67,9%): Fibula lateral 29/56 (51,8%) anterolateral 7 y X free fibula flap success X mean 63 y (range No No No 8/56 (14,3) was Ab
18/56 (32,1%): Scapula 19/56 (33,9%) total
rate: 36/38 (94,7%) free
24-80 y)
irradiated
mandibulectomy 13/56 (23,2%)
scapula flap success
rate: 18/18 (100%)
Garrett , et al.
(2006)
46 free fibula flap + conventional
(CP) and/or implant-supported
(IP) prostheses
lateral 2/46 (4,4%) anterolateral
20/46 (43,5%) anterior 1/46 (2,2%)
posterior 13/46 (38,3%) hemi
6/46 (13%) total
mandibulektomi 3/46 (6,5%) total +
Condyle 1/46 (2,17%)
45/46 (97,8%) 33/46 (71,7%) (CP) and
48,5% (16/33) IP
X mean 60 y No No No Ab
Hamaker , et al. 15 Resection + postoperative X X 4 y and 3 month success rate 66% X X No No No X Full
(1983)
radiation
He , et al. (2010) 17 free fibula flap and/or Fibula lateroposterior 5/17 (29,4%) mean 25 month survival rate free flap success rate: X mean 51,5 y (range No No No 11/17 (64,7%) was Ab
postoperative radiotherapy
anterolateroposterior 3/17 (17,6%) (range 3-57 month) 15/17 (88,2%) 100%
35-63 y)
irradiated post op
lateral 2/17 (11,8%) anteriolateral
life time of those
5/17 (29,4%) total
who died 8 mån
mandibulectomy + condyle 1/17
post op (range 3-
(5,9%) bilateral+anterior 1/17
13 month)
(5,9%)
Head , et al. (2003) 210 free microvascular flap + titanium 134/210 (63,8%) Fibula 153/210 (72,9%) lateral 57/210 mean 21,5 month survival rate success rate: 93,3% X range 19-88 y No No No 165/210 (78,6%) Ab
platta 11/210 (5,2%) Scapula (27,1%) Anterior or anterolateral (range 1-70 month) 98,1% (206/210) (196/210) was irradiated
5/210 (2,4%) Iliac
70 month post
1/210 (0,5%) Radialis
op. Life time of
those who died
mean 16,3 days
post op (range 7-
24 days)

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
40
Heller , et al. (1995) 47 free osseous flap or soft tissue + 18/47 (38,3%) iliac 11/47 (23,4%) anterior
27/47 survival rate 74% free flap success rate: X mean 67 y (range No Yes No 35/47 (74,5%) was Ab
plate 5/47 (10,6%) fibula (57,4%) lateral 9/47
1 y post op 67% 21/23 (91,3%)
13-82 y)
irradiated
2/47 (4,3%) scapula (19,2%) posterior
2 y post op 40% 5 success rate for plate
6/35 (17,1%) pre
1/47 (2,1%) rib.
y post op (mean 14/21 (66,6%)
op 29/35 (82,9%)
8/47 plate + soft tissue
39 month alive
post op
transfer
post op of those
8/47 pectoralis
who died)
5/47 forearm
Hidalgo , et al. 12 free fibula flap el free fibula flap fibula mean 13,5 cm X X free flap success rate: X X No No No 6/12 (50%) was Ab
(1989)
+ miniplates (11/12)
100%
irradiated post op
Hundepool , et al. 70 OFFF fibula 20/70 (28,6%) anterior 31/70 mean 39,5 month survuval rate X total implant mean 53 y (range 6 Yes Yes Yes Full
(2008)
(44,3%) lateral 1/70 (1,4%) (range 6-89 month) 64,3% (45/70) 18
success rate: 97%. 82 y) posterior 16/70 (22,9%) month post op
anterolateral 2/70 (2,9%) lateroposterior
Iino , et al. (2009) 15 Cancellous bone and marrow + Iliac 1/15 (6,7%) anterior 10/15 62,7 month (29-108 X success rate 86,7% Success rate 90,1% mean 58,3 y (range No No No 6/15 (40%) was Full
titanium reconstruction plate
(66,7%) Lateroposterior 4/15 month)
(13/15) (10/11) 23-74 y)
irradiated
(26,7%) lateral
11/15 (73,3%) got
dental
implants/prosthesi s
Irjala , et al. (2012) 10 free osseous flap 9/10 (90%) fibula in X mean 51,5 month survival rate 6/10 free flap success rate: Success rate 100% mean 60 y (range No No No 10/10 (100%) was Full
which 1 of these also
(range 4-142 month) (60%) was alive 90% (9/10) 4/10 (40%) got 48-75 y)
irradiated
included radialis
142 month post dental implants.
1/10 (10%) iliac.
op. Of those who
died, lived for 15,3 month (range 4-26 month)
Jeng , et al. (2005) 10 Double Free Flaps and 10 fibula mean (9.4cm(6-14cm)) 24m 9 of 10 100% x 51.7y (44-64y) Yes Yes No x Ab
Fascia Lata Grafts for Oral
Sphincters
Ji , et al. (2006) 541 The reconstruction methods x x x x x x 40-70y No No No x Ab
included soft flap, reconstruction
plate and bone grafts.
Julieron , et al. 38 free bone grafts 25 fibula 24 anterior 9 x x 36/38 x x Yes Yes No x Full
(1996)
7 scapular laterala 5
3 iliac anterio-laterala
3 forearm free flaps
Kadota , et al. 23 (12) 2 metal plate 2 iliac x x x x x 65.6y (47-74y) No Yes No x Full
(2008)
2 iliac crest free flap
2 scapula
2 scapula osteocutaneous free
flap
6 without reconstrcution

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
41
Kim , et al. (2007) 29 latissimus-serratus-rib free flap 27 latissimus-serratus- 15 anterio-laterala 12 laterala 21m x 28/29 x 68y (21-82y) No No No 22 was irradiated Ab
rib free flap 2 anteriora
preop 13
2 serratus-rib
post op 9
osteomuscular free flap
Knott , et al. (2007) 101 locking mandibular
reconstruction plate and
vascularized bone grafts
93 fibula flaps
8 latissimus-serratus rib
flaps
x (8.1cm (4-23cm)) 14.6m (6-46m) x 86/101 x x No No No 87 was irradiated Ab
29 preop and 56
postop
Koch , et al. (1994) 40 Thorp vs. Metal plate x x 72m x THORP 11/12
Metal plate 14/28 x x No No No x Ab
Kovács , et al.
(1994)
30 Free radial forearm flap Radial 30 x x x 100% x x No No No x Full
Kroll , et al. (1992) 69 A:15 soft tissue x x x x A: 77% B: x x No No Yes x Ab
B:20 immediate reconstruction
50%
with vascularized bone
C: 27%
C:15 metal plate
D: 22%
D:9 plate (bone later)
E: 30%
E:10 no reconstruction (bone
later)
Kudo , et al. (1992) 32 27 seg. Resection 5 A:8 autogenous bone x x 30/32 levde vid A:6 of 8 B: x x No No No x Ab
hemiresection
graft
sista 4 of 7 C:
B:7 pedicled
uppföljningen 2 of 6
myocutaneous flap+
D: 7 of 11
bone graft
C: 6 metalic plate
D: 11 Pedicled
myocutaneous flap and
metallic plate
Li , et al. (2007) 112 fibular grafts Group A (7): x 12-140m x x 239 implantat Group A : 56y No Yes No 19 patients was Full
microvascular bone
sattes på 115 Group B: 55y
irradiated
graft
patienter Group C: 50y
Group B (61):
Group D:54y
microvascular
reconstruction of
Seg.Defects.
Group C (41):Avascular
onlay grafts
Group D (7):avascular
reconstruction
Lindqvist , et al. 34 alloplastic reconstructions x x x 19 of 34 lived at 22 of 34 (64.7%) x x No Yes No x Ab
(1992)
last follow up
Louis , et al. (2010) 93 revascularized free scapular flap 93 scapula x 10-144m x 88/93 (94.6%) x x No No No x Full

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
42
Malata , et al. 100 Würzburg noncompression 92% with vascularised x(10cm (3-19cm)) 47m (12-96m) x 92/100 (92%) x 60y (10-86y) No Yes No 11 was irradiated Ab (1997)
titanium miniplate system bone grafts. (Fibula,
preop 53 was
scapula, radius)
irradiated postop
4 patients having
11 was irradiated
nonvascularised iliac
both pre and post
bone grafts.
Maurer , et al.
(2006)
20 reconstruction plate 16
Iliac 3
miniplate 1
Iliac 3 x x x x x 59y No Yes No x Full
Millsopp , et al. 278 No flap 56 x (not defined) x 24m Group1 (114pat): x x Grupp 65-: 158 Yes No No 110 was irradiated Ab
(2006)
Soft tissue 147
95% 1 year, 89% 2
Grupp 65+: 120
Bone flap 63
year, 81% 3 year.
Bone + soft tissue 7
Gruop 2
(164pat): 75%
1year, 64% 2year,
60% 3year.
Miyamoto , et al. 23 clinical results were compared Double flap : MRP: anterio-lateral 8, lateral 4 22m (1-108m) 5 of 23 lived with MRP: 12 of 12 x 58.4y +- 12y Yes Yes Yes MRP: 1 was Full
(2012)
between mandibular 10 Fibula 1 (1 included the joint)
out disease after Double flap 11 of 11
irradiated
reconstruction plate (MRP) scapula
Double flap: 11 anterio-laterala
108m
Double Flap: 2 was
procedures and double flap
irradiated
transfers.
Obiechina , et al.
(2003)
20 free nonvascularised iliac crest. 20 iliac 5 anterio-lateral 15 laterala x x 19/20 x x Yes Yes No x Full
Okoturo , et al. 13 immediate plate reconstruction x 1 anterior 5 lateral 15m (6-23m) x 11 of 13 plate 2 11 patients had 24y (10-36y) Yes Yes Yes x Ab
(2011)
7 anterio-laterala
removed due to fracture implants
Patel , et al. (1996) 83 Grupp 1: 47 rekonstruerades ej. 8 pectoralis. M. omc. Grupp 1:47 anteriolateralt (47 x x x 12/36 got 32-76y Yes Yes No 25 was irradiated Full
Grupp 2: 21 fick siliastic implants. 7 iliac
8 fick PM-OMC. 7 fick Iliac flap
involved the joint)
Grupp 2: 36 laterla
prosthesis after surgery
Pellini , et al. (2012) 41 x x x x x x x x No No No x Ab
Politi , et al. (2012) 24 Iliac flap vs. Fibula flap 13 iliac 11 x (6-15 cm) 12m x Iliac 13 of 13 Every one had 56y (17-62y) Yes Yes Yes x Ab
fibula
fibula 10 of 11 implants
Puxeddu , et al.
(2004)
12 vascularized
bone-containing free flap
12 iliac 8 laterala 4 anterio-
laterala 6.9cm(5.2-9cm)
21m (6-64m) 6 of 12 survived
50%
11 of 12 no one had
implants
62.5y (57-77y) No No Yes 9 patients was
irradiated after
suregery
Full

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
43
Rivas , et al. (2000) 15 vascularized bone grafts 11 fibula
3 iliac
1 radial
10 laterala 2 hel resection x x 13/15 x x No No No x Full
3 anterio-laterala (tot. 9 involved
the joint)
Robey ,et al. (2008) 117 free fibular flaps. Miniplates Vs. 117 fibula (86 x 29.6m x Mp: 77/86 Mp: 7/86 Mp: 60.4y (21-85y) Yes No No Mp: 53% was Full
Reconstruction plates miniplates 31
RP: 26/31 Rp: 5/31 Rp: 61.1y (21-88y)
irradiated Rp:
reconstruction plates) 16% was irradiated
Rogers , et al.
(2004)
224 123 no resection 44 rim
resection 57 segmental
resektion
26 fibula
7 DCIA
13 radial
6 scapula
5 compination
Of segmentresect. 16% in anterior
sites, 28% in
posterior, and 56% combined
16m (12-36m) 12m: 187/224
36m: 113/224
x x 61y Yes Yes Yes 51% of
segmentalresect.
Patients
Full
Sarukawa , et al.
(2012)
11 vascularised iliac crest Iliac 11 x (4-12cm) 6-44m 81% 81% 2 of 11 58.8y (32-78y) No No No 6 was irradiated
before surgery
Full
Schliephake , et al. 44 21 vascularized grafts VG: iliac: 6 x (6.7cm (2-12cm)) 41.2m 41/44 x (100% on impants 44 x No No No 15/44 was Full
(1999)
23 nonvascularized grafts scapula: 4
after five years 60.3%
irradiated
fibula: 11
after 10years)
Non-VG: iliac 23
Shpitzer , et al. 57 osteocutaneous free flaps, plate + PMMF 27 Lateral defects (16 included the PMMF: 45m(12- x PMMF 20/27 x PMMF 58y FRFF No Yes Yes x Full
(2000)
plate + PMMF , plate + FRFF plate + FRFF 16 joint) 126m)
FRFF 14/16
61y OFF 55y
osteocutaneous free
FRFF:23m (12-53m)
OFF 14/14
flaps 14 (fibula)
OFF: 20m (13-38m)
Simon , et al. (2013) 32 reconstruction plates and an
autogenous particulate bone
graft
x (particulate bone
iliac)
x 27.9m (12-39m) x 31/32 96.8% x (13/32 got
prostehsis)
27.7y No No Yes x Full
Suh , et al. (2010) 40 microvascular free flap Fibula 36 rib 3 x (length 8cm(4- 17.4m x 100% x 62y (38-86y) No No No 40 was irradiated Full
Iliac 1
24cm))
Söderholm , et al.
(1988)
30 rigid internal fixation x x x x 29/30 96.6% x x Yes No No x Full
Trignano , et al.
(2013)
34 fibular osteocutaneous flap vs
free fibular flap with periosteal
excess
Fibula 34 x (length 2-5.7cm) 1.5m x 11/17 free flap x
15/17 free flap PE
No No No 34 was irradiated Ab
Tsuchiya , et al.
126 (114) free flaps Fibula 52 Scapla 7 x 65m x 101/114 88.6%
42.9 (27-55y)
x 62.2 No Yes No x Full

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
44
(2013) Iliac 3
RAMC 43
ALT 5
RF 3
Plate exposure 3
Plate infection 4
Fracture of plate 2
Total flap necrosis 4

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
45
Ueyama , et al. 34 single A-O plate 4st patients x x 47.4 m ( 6-115m) 69.7% 79% x x No No No x Ab (1996)
got ilactrans.
4/34 plate exposure
1/34 screw loosening
2/34 TMJ pain
Urken , et al. (1991) 10 Vascularized bone flaps x x x x x x x Yes Yes No x Full
van Gemert , et al. 83 free forearm flap and Fibula 46 iliac 22 68 (41) lateral 15 anterio- 12-24m 61% after 2 y 100% Fibula 94% 10/83 got implants 63 (25-85 y) No No No 66/83 was Full
(2012) reconstruction plate and free
vascularized bone flaps
Free forearm + plate 15 laterala Iliac 64%
Radial
(After 1 year)
irradiated
van Gemert ,et al. 74 NVBG Iliac 74 X (position) 74 (32) 12m x 76% 11/74 got implants 54.3 (12-73 y) No Yes No 27/74 was Full
(2009) lateral 33/74 got
prosthesis
irradiated
Vayvada , et al. 11 free deep circumflex iliac artery iliac 6 fibula 5 x (position) 11 (2) 29,3m (17m- x 100% 3/11 (due to cost) 25.4 (18-38 y) Yes Yes Yes x Full
(2006)
or fibular flap
lateral
38m)
Villaret ,et al. 92 (35 x x x x x x x x No Yes No x Full
(2008) recsponded)
Virgin ,et al. (2010) 168 free flap reconstruction Radial 51 Fibula 117 x 31m fibula 20m 75% after 5 year 96.6% Fibula 2.3% had implants 63.7 (radial) 59 No No No x Full
fibula
96.1% Radial
(fibula)
VU , et al. (2008) 29 (18 vascularized fibular free flap and Fibula 10 Iliac 8 X (position) 1 anteriora 12m-40m from the x x x 42 Yes Yes Yes 33% were Full
responded) nonvascularized iliac crest
17 (10) lateral
operation
irradiated
Young , et al. (2007) 26 Reconstruction plate x x (position) 2 anteriora
18 (4) laterala 6 (3) anterio-
laterala
12m-72m from the
operation
x x 35% (7/20)
Implants
29,8 Yes Yes Yes 0% Ab
Zender , et al. 65 OCFF Fibula 54 Radial 6 x (position) Lateral 50% 30m 1m- x 90% x 62 No No No 83% irradiated Full
(2012)
Iliac 5 Anterio-Lateral 50% 188m
7/65 flap loss
Zenn , et al. (1997) 17 Free flap Radial forearm mean ~8cm (8.25) 13.5m 1m- 94.1% (16/17) 8 70% 3/17 x 55 No No No >50% irradiated Full
72m days post op fracture plate 2/17
fracture donor site
Zhang , et al. (1999) 97 (68) Reconstruction Plate x x x x 51% x x No No No x Full

Authors (year) Number of
Patients
Techunique Site (Bone) Size and position of resection (with Follow up
or wthout temporomandibular joint) mean + range
Survival rate Success rate (loss of Dental
plate and/or fractures) rehabilitation
Implants/protheses
Mean age Aesthetics Function
(included or (included
Quality of Irradiation
life
(included or
not)
Abstract/ Full
text
not) or not)
46
22/68 detached
6/68 fracture plat
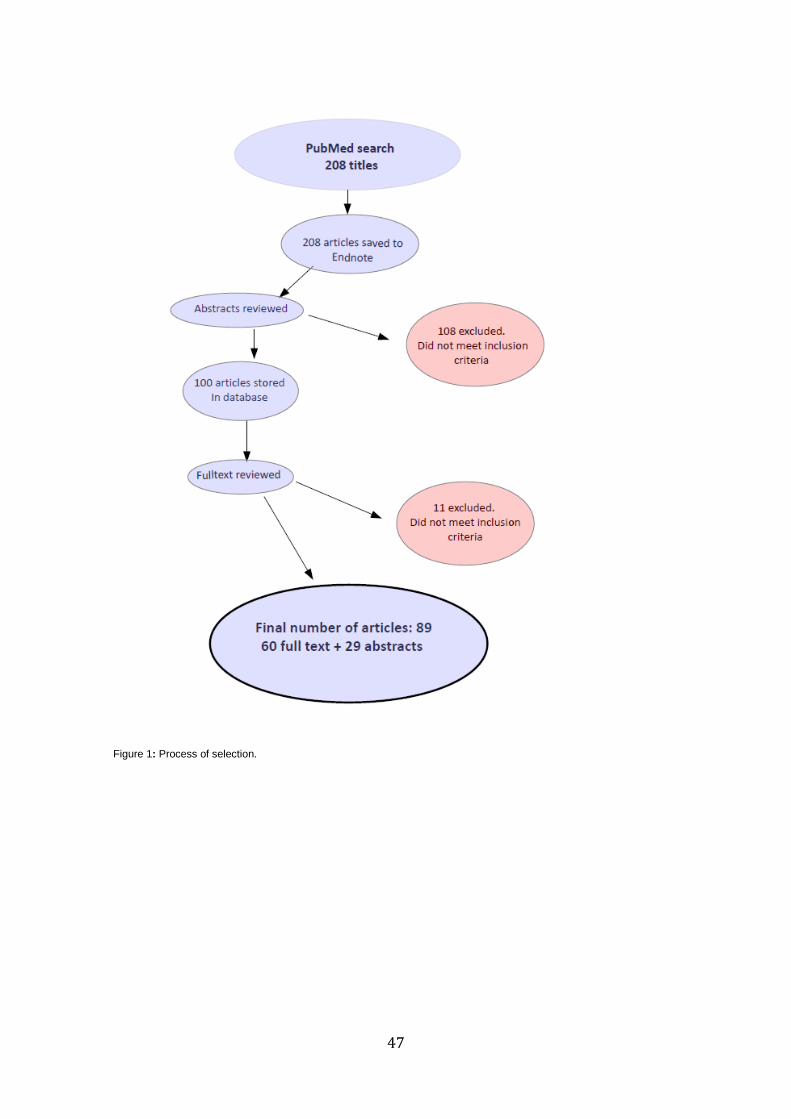
47
Figure 1: Process of selection.
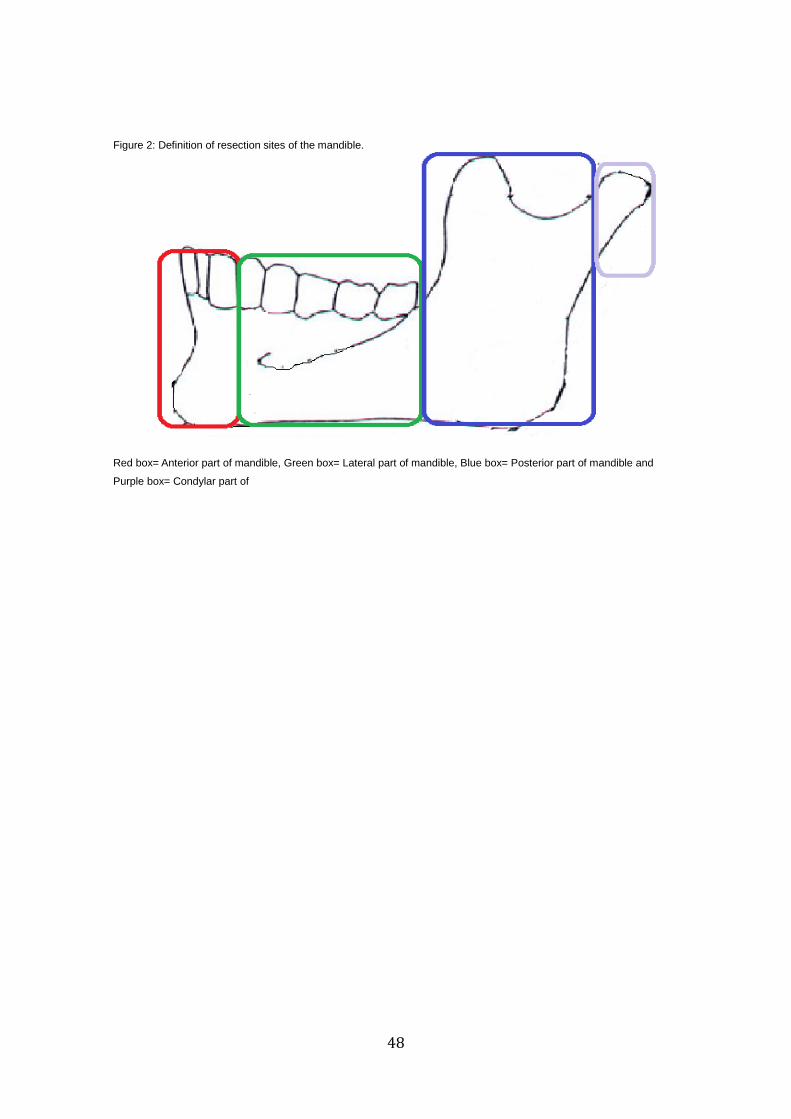
48
Figure 2: Definition of resection sites of the mandible.
Red box= Anterior part of mandible, Green box= Lateral part of mandible, Blue box= Posterior part of mandible and
Purple box= Condylar part of