mandibular implants and the growing patient
TRANSCRIPT

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Mandibular Implants and the Growing PatientRobert J. Cronin, Jr, DDS, MS/Larry J. Oesterle, DDS, MS/Don M. Ranly, DDS, PhD
The dynamic relation of the anteroposterior and rotational growth of the mandible to the transverse arch width and dental height changes must be understood before placing endosseous implants in actively growing patients. Research models demonstrate that osseointegrated implants lack the compensatory growth mechanism of the natural dentition. Remodeling associated with skeletal growth in the region of the implant placement site could cause the implant to either become unsupported by bone or submerged within it. Implants placed after age 15 in girls and 18 in boys have the most predictable prognosis. When placed in the growing patient, dental implants should be closely monitored and carefully restored with implant prostheses designed to accommodate growth and development. (INT J ORAL MAXILLOFAC IMPLANTS
1994;9:55-62)
Key words: dental implants, growth and development, mandibular growth, osseointegration
There are many indications in the growing individual for implant-supported prosthodontic restorations. However, the literature is lacking in sound justification for implant use in children. Some authors arbitrarily limit their use to fully erupted permanent dentitions1 or a specific age,2 while others report on apparently successful implant use in children with congenital disorders such as ectodermal dysplasia.3 In a previous article, the potential for maxillary implant placement in the growing patient was examined.4 The same concerns for developmental changes in jaw growth and dental maturation exist when mandibular implant placement is considered. These concerns include jaw growth in relation to static implants, as well as the effects of prosthesis attachment on future growth and development. Without consideration of the dynamic nature of the growing child, a typical diagnosis will not provide the clinician with the knowledge necessary to make valid diagnostic decisions. In this paper, growth of the mandible and its dentition will be examined in the context of implant treatment, and a rationale will be constructed for the implant treatment of the growing patient.
Behavior of ImplantsTo anticipate the behavior that dental implants might exhibit in actively growing mandibles, evidence from several topic areas suggests likely outcomes. These are ankylosed teeth,5-7 metallic implants used in cephalometric growth studies,8-9 and
10

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
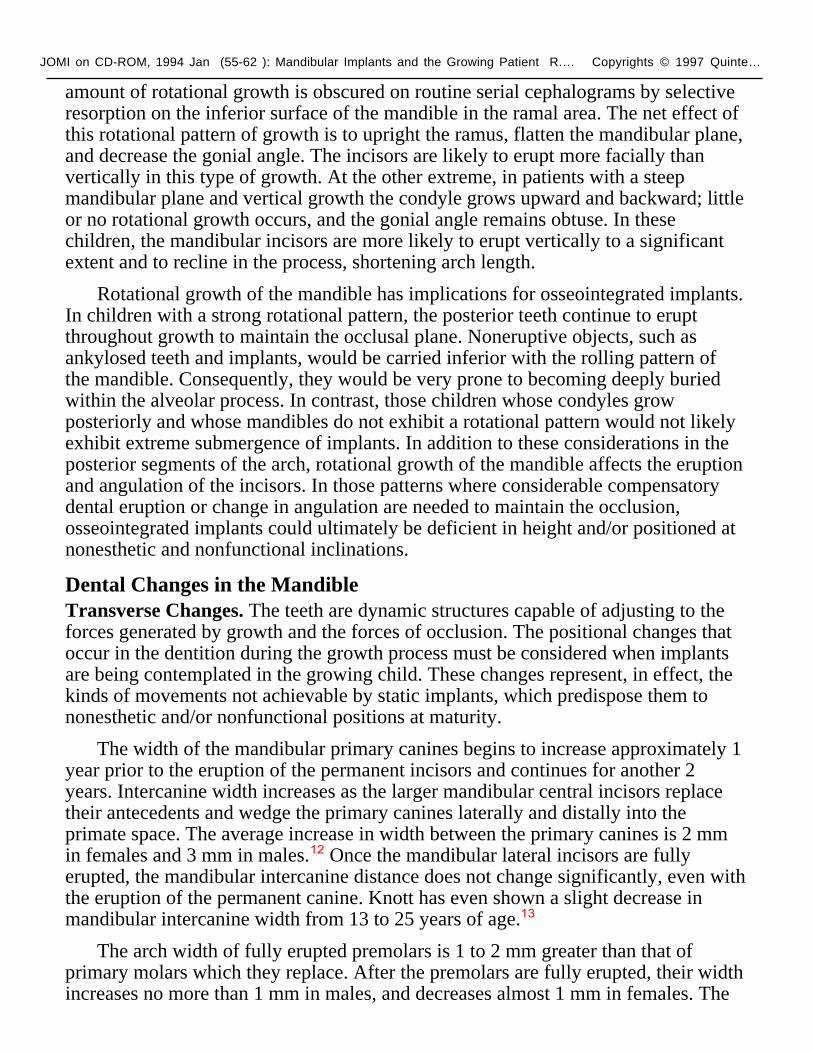
alveolar implants in experimental animals.10 Ankylosed teeth, predominantly a condition of the primary dentition, are characterized by the union of cementum with bone and a "submergence" of the tooth during growth. This apparent submergence results from an inability of the tooth to erupt as needed to compensate for vertical growth of the alveolar process. The static position of the ankylosed tooth can dramatically retard vertical dentoalveolar development (Fig 1).
Metallic implants embedded in bone to ensure stable reference landmarks in longitudinal cephalometric studies have indirectly revealed some of the possible growth-related problems in dental implants.8,9 Unless situated in nongrowing areas, these implants were subject to loosening by resorptive processes or to burial by bone apposition. The younger the recipients, the more likely was the loss of implants. Recent animal studies confirm that implant behavior in growing pigs is similar to the research and ankylosed tooth models.1,10
Clearly, foreign or natural bodies that are devoid of surrounding tissue with the attributes of periodontal ligament cannot adjust to growth, and therefore are subject to burial by bone apposition or to loss of bony support by resorption. These examples provide some insight into the fate of osseointegrated implants if the principles of growth and development are ignored. Prior to the establishment of a rationale for the use of dental implants in the mandible of growing patients, an examination of relevant mandibular growth and development is essential.
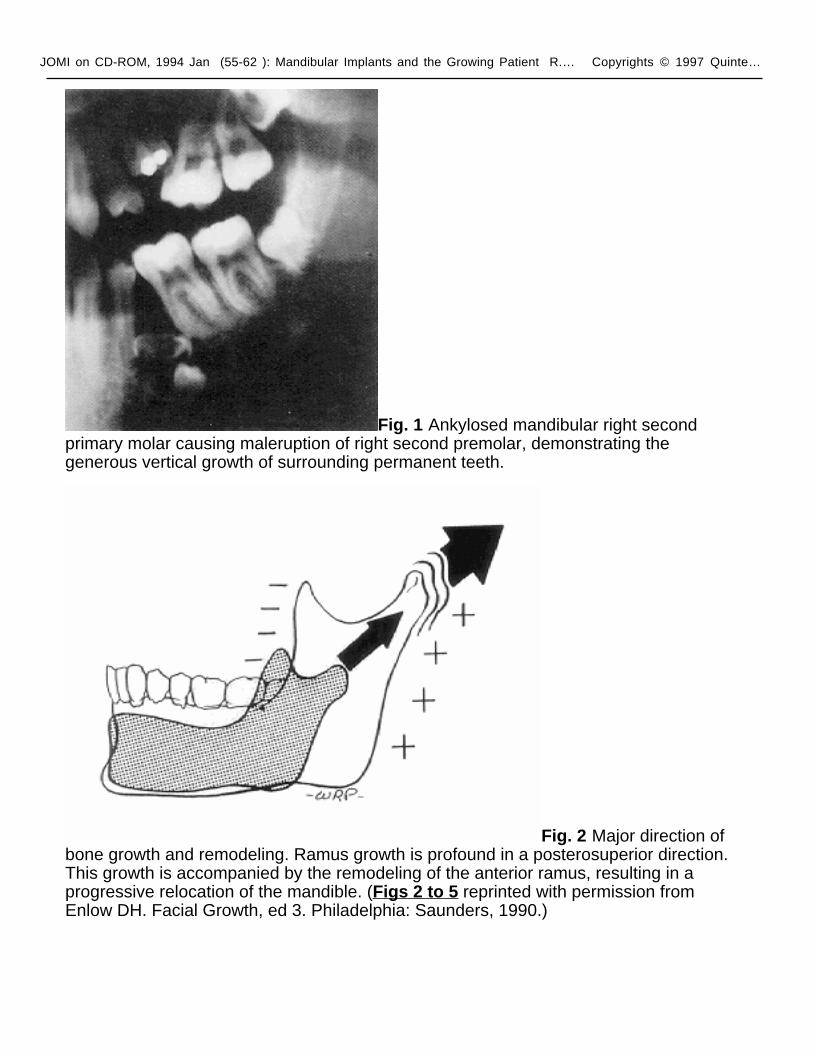
Mandibular Growth ChangesAnteroposterior Growth. The mandible lengthens almost exclusively by posterosuperior growth of the condyle and posterior growth of the ramus (Fig 2). Increasing prominence of the chin during adolescence, seen primarily in males, is not the result as much of appositional growth at the chin as it is of resorption above it. To accommodate eruption of the molars, the body of the mandible increases in length by resorption on the anterior aspect of the ramus and deposition on the posterior. Concurrently, the ramal height is increasing 1 to 2 mm per year.11
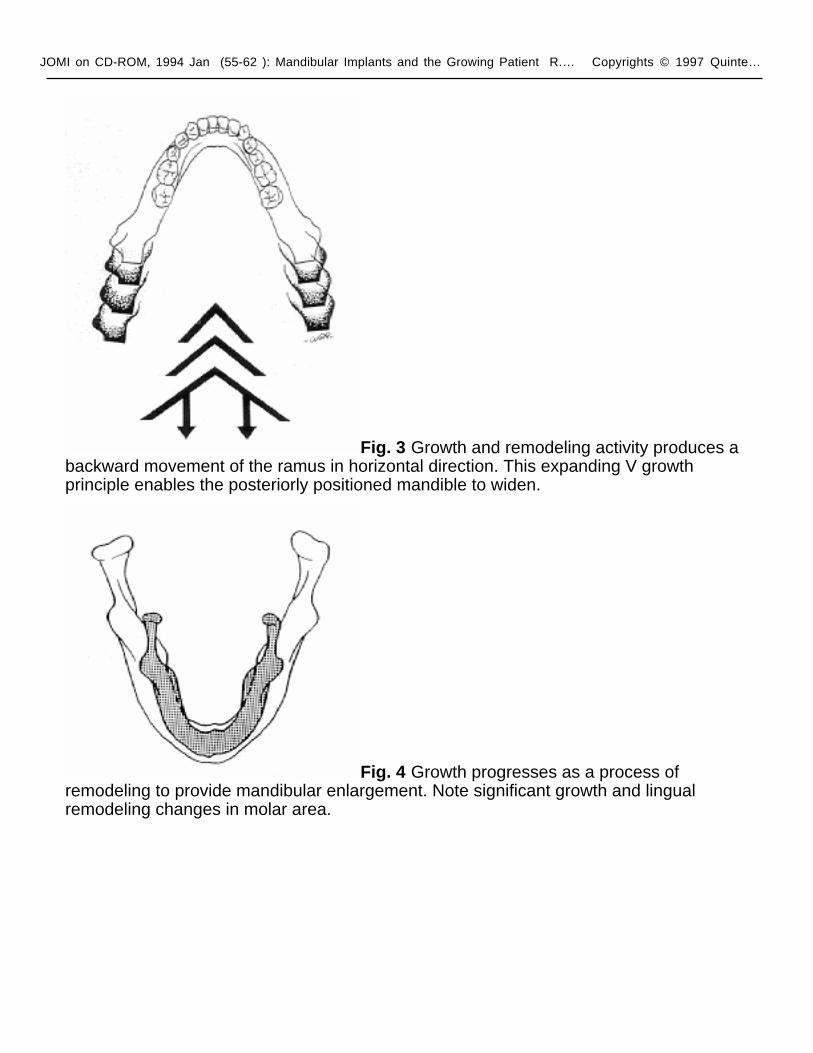
The posterior width of the mandible increases by virtue of its V configuration; the symphyseal suture ceases to be a growth area prior to the eruption of the primary teeth. As a result, mandibular anterior width stabilizes relatively early and only increases slightly by appositional growth (Fig 3).
Rotational Growth. When lateral cephalograms are superimposed on the cranial base, the mandible appears to grow downward and forward in a simple linear manner. However, this is not the case in most individuals. Using metallic implants to ensure stable landmarks for serial cephalometric superimposition, Björk8 found that in many cases the mandible exhibits a rotational pattern as it grows. When the condyle grows vertically, or vertically and forward, the vertical growth in the ramus exceeds that of the symphyseal area, and the mandible "rolls" downward and forward. The center of rotation in these cases is situated near the incisal region. The
JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
amount of rotational growth is obscured on routine serial cephalograms by selective resorption on the inferior surface of the mandible in the ramal area. The net effect of this rotational pattern of growth is to upright the ramus, flatten the mandibular plane, and decrease the gonial angle. The incisors are likely to erupt more facially than vertically in this type of growth. At the other extreme, in patients with a steep mandibular plane and vertical growth the condyle grows upward and backward; little or no rotational growth occurs, and the gonial angle remains obtuse. In these children, the mandibular incisors are more likely to erupt vertically to a significant extent and to recline in the process, shortening arch length.
Rotational growth of the mandible has implications for osseointegrated implants. In children with a strong rotational pattern, the posterior teeth continue to erupt throughout growth to maintain the occlusal plane. Noneruptive objects, such as ankylosed teeth and implants, would be carried inferior with the rolling pattern of the mandible. Consequently, they would be very prone to becoming deeply buried within the alveolar process. In contrast, those children whose condyles grow posteriorly and whose mandibles do not exhibit a rotational pattern would not likely exhibit extreme submergence of implants. In addition to these considerations in the posterior segments of the arch, rotational growth of the mandible affects the eruption and angulation of the incisors. In those patterns where considerable compensatory dental eruption or change in angulation are needed to maintain the occlusion, osseointegrated implants could ultimately be deficient in height and/or positioned at nonesthetic and nonfunctional inclinations.
Dental Changes in the MandibleTransverse Changes. The teeth are dynamic structures capable of adjusting to the forces generated by growth and the forces of occlusion. The positional changes that occur in the dentition during the growth process must be considered when implants are being contemplated in the growing child. These changes represent, in effect, the kinds of movements not achievable by static implants, which predispose them to nonesthetic and/or nonfunctional positions at maturity.
The width of the mandibular primary canines begins to increase approximately 1 year prior to the eruption of the permanent incisors and continues for another 2 years. Intercanine width increases as the larger mandibular central incisors replace their antecedents and wedge the primary canines laterally and distally into the primate space. The average increase in width between the primary canines is 2 mm in females and 3 mm in males.12 Once the mandibular lateral incisors are fully erupted, the mandibular intercanine distance does not change significantly, even with the eruption of the permanent canine. Knott has even shown a slight decrease in mandibular intercanine width from 13 to 25 years of age.13
The arch width of fully erupted premolars is 1 to 2 mm greater than that of primary molars which they replace. After the premolars are fully erupted, their width increases no more than 1 mm in males, and decreases almost 1 mm in females. The

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
width of the mandibular first molars increased nearly 3 mm in males and 2 mm in females, with the greatest rate of change seen during eruption. The mandibular second molars showed nearly a 2-mm increase in width in males and no change in females between the ages of 12 and 18.12
The changes in arch width just discussed represent average figures (Fig 4). In fact, the changes in arch width vary greatly from individual to individual, with some arches no wider at 8 years of age than at 4, while in others, intercuspal width increases as much as 3.5 mm in the second premolar area during this time.14 Although stature and statural change have a correlation to intercanine width, it is not strong, and because individual variation has been found to be so great, the accurate prediction of intercanine width at 15 years of age is impossible based on intercanine measurements made at 4 or 5 years of age.15-17
Dental Height Changes. The dental height of the incisors and molars (the distance from the cusp tips to the inferior border of the mandible) increases in a similar pattern throughout growth. The permanent incisors reestablish the dental height of the exfoliated primary teeth by age 9, while at the same time the first permanent molars reach the level of the primary molars. From years 9 to 15 there is a steady increase in height of both teeth. This increase is greater in males than in females. Dental height in males appears to increase beyond 15 years of age, while in females it levels off at 13 to 14 years of age.16 To fully appreciate the magnitude of the compensatory eruptive process, the distance measured on a perpendicular to the mandibular plane from menton (on the mandibular symphysis) to the tip of the incisor increases 12 mm in males and almost 7 mm in females between the ages of 6 and 16.11
Arch Length Changes. Changes in arch length in the mandible differ from those in the maxillary arch. As the permanent incisors erupt, there is generally little or no change in mandibular arch length. Hence, unlike the maxillary anterior teeth, which tend to erupt labially and increase the arch length temporarily, the mandibular incisors erupt closer to their ultimate position. As the primary molars are lost and the premolars erupt, there is almost a 2-mm decrease in arch length as the first permanent molars move mesially.18 Additional arch length changes occur as the mandible grows, the amount of change varying with the direction of growth.
Mandibular Changes and the Osseointegrated ImplantLike the maxilla, the mandible is a dynamic, changing unit during growth. However, because the mandible has a V configuration, posterior teeth naturally erupt at ever-increasing widths. Consequently, there is no need—and no mechanism—to widen the arch, as in the maxilla. The distance between teeth can increase to coordinate with increase in maxillary width, but this occurs by alveolar remodeling, and, as described above, is usually not dramatic. For this reason, an implant is not likely to be esthetically or functionally malpositioned because of transverse movements of adjacent teeth during growth.

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Successful implants in the mandible are also favored by the lack of a complicating suture. Because the symphyseal suture begins to close within months of birth, there is no danger of implant surgery traumatizing a growth site and little possibility that a prosthesis placed across the midline could limit transverse growth. Mandibular midline implants, therefore, have a better prognosis in a young patient than those placed in other areas of the mandible. Prosthesis design must allow for the average increase in dental height of 5 to 6 mm and for the anteroposterior variation caused by the different directions of mandibular growth (Fig 5),16 Figures 6a to 6f demonstrate the utilization of implants in this anterior mandibular area of a 5-year-old partially anodontic ectodermic dysplasia patient. The psychiatric, functional, and esthetic problems associated with ectodermal dysplasia presents the prosthodontist with difficult treatment-planning decisions, and endosseous dental implants have been suggested as a potential aid.19 The implant prosthesis is designed as a detachable frame with denture teeth processed in light-activated acrylic resin. This design facilitates periodic adjustments for future growth and development.
There is, however, one serious concern that limits the utilization of mandibular osseointegrated implants in growing children, and that is the vertical eruption (and in some cases, angular change) required of dental units. The burying of an implant because of occlusal alveolar bone apposition is possible in both the posterior and anterior segments. This condition could be exacerbated in both areas by an unfavorable rotational growth pattern.
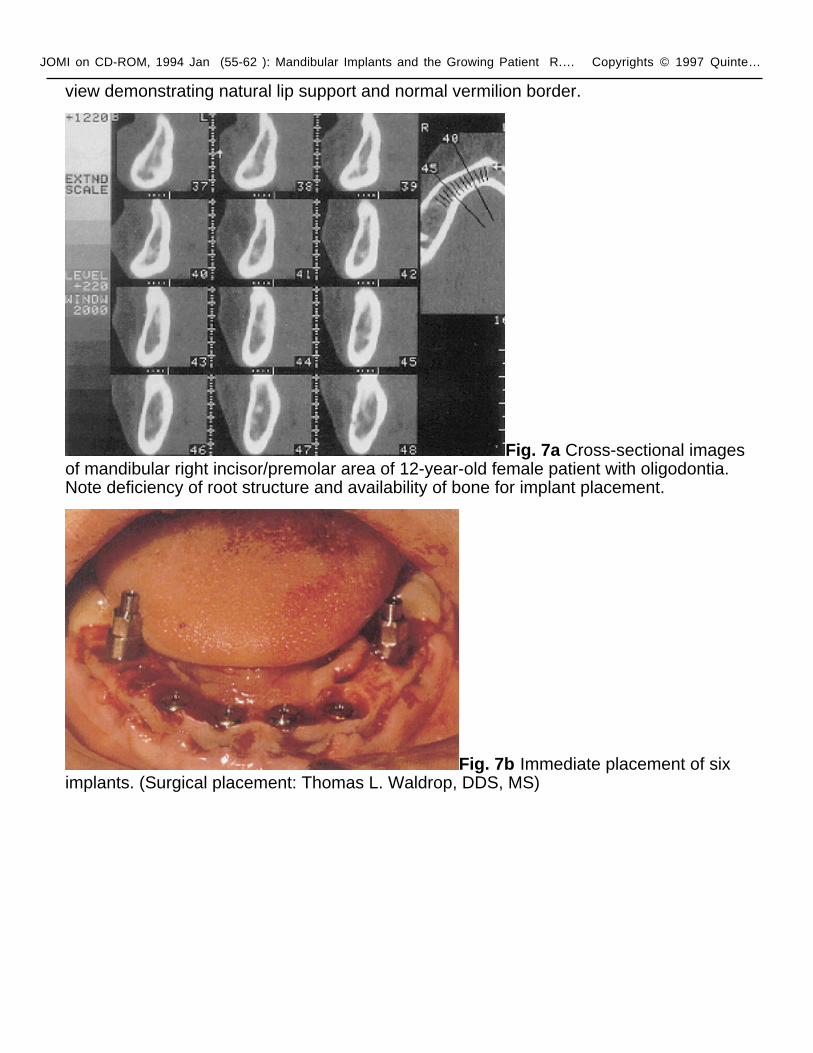
The lack of vertical and angular adjustments by the implant might not be as detrimental to the final outcome in some cases as in others. For instance, in totally anodontic patients, the position of the implants, faulty or otherwise, would not have as much impact on the surrounding alveolar bone as it would in a partially anodontic patient, in whom considerable change with vertical alveolar growth associated with teeth could be expected. There are, however, strong indications for the use of implants early in the development of the anodontic or partially anodontic child. A firmly affixed prosthesis not only allows the restoration of facial height, but improves esthetics and self-image, as well as dental function. However, the use of implants in the primary or early mixed dentition must be done very deliberately. Not only are the growth and dental developmental changes during this time extensive, but the ability to predict the ultimate outcome does not exist. In most cases, the safest treatment plan is to wait until growth slows before placing any implants. Girls grow actively until 14 to 15 years of age, while boys grow longer and more abundantly until 17 to 18 years of age. Figures 7a to 7e show the implant-assisted reconstruction of a 14-year-old female patient in oligodontia. Nonfunctional primary teeth were replaced with dental implants immediately after extraction, preserving alveolar width and height. Extreme care was exercised during the initial healing periods to minimize transepithelial implant-site loading to assure successful osseointegration. A magnetically retained implant prosthesis was then designed to

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
restore esthetic, phonetic, and masticatory function, while maintaining ease of growth and development adjustment.
RecommendationsThis review illustrates the dynamic aspect of occlusion in the growing child, as well as the diversity in developmental trends among individuals. A discussion of average growth trends and average dental change during development affords the clinician a concept of normal development. However, extrapolating average data to an individual and predicting growth is almost impossible.
Because of the changes that occur in both the dentition and growing jaws, extreme caution must be used in placing implants in children. Orthognathic surgery for the maxilla or mandible is usually delayed until after puberty, lest adolescent growth reestablish the adverse pattern. Likewise, if implants are placed during active growth, they may be displaced or malpositioned by continued growth and may require removal and replacement. Whenever possible, implant placement should be delayed until age 15 for girls and age 18 for boys. Implants placed after these ages have the most predictable prognosis. The parents and patient must be fully informed that implants placed before these ages may not be "permanent" and may have to be reimplanted. If implants are deemed necessary in a child, care must be taken during implant placement and subsequent prosthesis design. Although the primary area of concern is the midpalatal suture of the maxilla, the growing patient who has received an implant in either arch must still be monitored closely to assure that the implant remains functional and does not disturb growth.
Submerging implants, like ankylosed teeth, could interfere with tooth-to-tooth relationships and affect occlusal force distribution, total jaw-growth patterns, and long-term occlusal relationships. If an implant is adversely affected by growth or contrarily is causing adverse growth, it should be removed while the surgery is still uncomplicated.
Further research must be done in the area of implants in growing children. Anecdotal evidence of implant success in children must be cautiously judged. Since the amount and direction of growth varies greatly from individual to individual, success in a few individuals cannot be extrapolated to the general population. Growing patients treated with dental implants should have adequate follow-up, including cephalometric radiographs. Well-controlled animal studies, particularly on primates, could provide further insight into the use of implants in children.

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
1. Ödman J, Gröndahl K, Lekholm U, Thilander B. The effect of osseointegrated implants on the dento-alveolar development. A clinical and radiographic study in growing pigs. Eur J Orthod 1991;13:279-286.
2. Schulte W. Suitability of Patients. Proceedings of a Consensus Conference on Implantology, October 18, 1989, Mainz, West Germany. Int J Oral Maxillofac Implants 1990;5:182-187.
3. Bergendal T, Eckerdal O, Hallonsten AL, Koch G, Kurol J, Kvint S. Osseointegrated implants in the oral habilitation of a boy with ectodermal dysplasia: A case report. Int Dent J 1991;41:149-156.
4. Oesterle L, Cronin R, Ranley D. Maxillary implants and the growing patient. Int J Oral Maxillofac Implants 1993;8:377-387.
5. Rubin PH, Weisman EJ, Bisk F. Experimental tooth ankylosis in the monkey. Angle Orthod 1984;54:67-72.
6. Kurol J. Infraocclusion of primary molars: An epidemiological and familial study. Community Dent Oral Epidemiol 1981 ;9:94-102.
7. Kurol J, Koch G. The effect of extraction of infraoccluded deciduous molars: A longitudinal study. Am J Orthod 1985;87:46-55.
8. Björk A. Variations in the growth pattern of the human mandible: A longitudinal radiographic study by the implant method. J Dent Res 1963;42:400-411.
9. Shaw WC. Problems of accuracy and reliability in cephalometric studies with implants in infants with cleft lip and palate. Br J Orthod 1977;4:93-100.
10. Thilander B, Ödman J, Gröndahl J, Lekholm U. Aspects on osseointegrated implants inserted in growing jaws. A biometric and radiographic study in young pigs. Eur J Orthod 1992;14:99-109.
11. Rilo ML, Moyers RE, McNamara JA Jr, Hunter WS. An Atlas of Craniofacial Growth, monograph 2, Craniofacial Growth Series. Ann Arbor, MI: Univ of Michigan Press, 1979.
12. Moyers RE, Van der Linden FP, Riolo ML, McNamara JA Jr. Standards of Human Occlusal Development. Monograph No. 5, Craniofacial Growth Series. Ann Arbor, Ml: Center for Human Growth and Development, The University of Michigan, 1976.
13. Knott V. Longitudinal study of dental arch widths at four stages of dentition. Angle Orthod 1972;42:387-394.
14. Meredith HV, Hopp WM. A longitudinal study of dental arch width at the deciduous second molars on children 4-8 years of age. J Dent Res

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
1956;35:879-889.
15. Lavelle CL. A study of dental arch and body growth. Angle Orthod 1976;46:361-364.
16. Jones B, Meredith H. Vertical changes in osseous and odontic portions of the human face between the ages of 5 and 15 years. Am J Orthod 1966;52:902-921.
17. Holcomb AE, Meredith HV. Width of the dental arches at the deciduous canines in white children 4 to 8 years of age. Growth 1956;20:159-177.
18. Moorrees CFA, Reed RB. Changes in dental arch dimensions expressed on the basis of tooth eruption as a measure of biological age. J Dent Res 1965;44:129-141.
19. Guckes AD, Brahim WS, McCarthy GR, Rudy SF, Cooper LF. Using endosseous dental implants for patients with ectodermal dysplasia. J Am Dent Assoc 1991;122:59-62.
JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Fig. 1 Ankylosed mandibular right second primary molar causing maleruption of right second premolar, demonstrating the generous vertical growth of surrounding permanent teeth.
Fig. 2 Major direction of bone growth and remodeling. Ramus growth is profound in a posterosuperior direction. This growth is accompanied by the remodeling of the anterior ramus, resulting in a progressive relocation of the mandible. (Figs 2 to 5 reprinted with permission from Enlow DH. Facial Growth, ed 3. Philadelphia: Saunders, 1990.)
JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Fig. 3 Growth and remodeling activity produces a backward movement of the ramus in horizontal direction. This expanding V growth principle enables the posteriorly positioned mandible to widen.
Fig. 4 Growth progresses as a process of remodeling to provide mandibular enlargement. Note significant growth and lingual remodeling changes in molar area.

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Fig. 5 Typical remodeling pattern seen at the mandibular midline. Bone deposition occurs at the basal area, while resorption is seen on the labial cortical plate, resulting in the maturation of the chin.
Fig. 6a Five-year-old ectodermal dysplasia patient with implants placed bilaterally to the mandibular symphysis (impression copings in place).

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Fig. 6b Diagrammatic depletion of tooth movement and remodeling process occurring in anterior mandibular area. Broken line depicts early childhood position and solid line depicts mature position. (Reprinted with permission from Enlow DH. Facial Growth, ed 3. Philadelphia: Saunders, 1990.)
Fig. 6c Implant-supported prosthesis must be designed to easily accommodate changes in tooth position secondary to growth and development. The retrievable metal frame with acrylic resin-retained denture teeth allows easy removal and laboratory tooth replacement.

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Fig. 6d Implant prosthesis in place replacing mandibular incisors.
Fig. 6e Lateral pretreatment view depicting deficient mandibular lip support.
Fig. 6f Lateral posttreatment
JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
view demonstrating natural lip support and normal vermilion border.
Fig. 7a Cross-sectional images of mandibular right incisor/premolar area of 12-year-old female patient with oligodontia. Note deficiency of root structure and availability of bone for implant placement.
Fig. 7b Immediate placement of six implants. (Surgical placement: Thomas L. Waldrop, DDS, MS)

JOMI on CD-ROM, 1994 Jan (55-62 ): Mandibular Implants and the Growing Patient R.… Copyrights © 1997 Quinte…
Fig. 7c After stage 2 surgery with healing abutments in place.
Fig. 7d Implant-supported magnetically retained overdentures.
Fig. 7e Implant-retained prosthesis restoring function and esthetics at an optimal vertical dimension of occlusion.