mand-ppt
TRANSCRIPT
Mandibular Mandibular Orthognathic Orthognathic Procedures- Procedures-
Presenter:Dr. saka. Saritha devi3rd yr. MDSDept. of Oral & Maxillofacial Surgery

CONTENTSCONTENTS1.1. IntroductionIntroduction
2.2. Historical aspectsHistorical aspects
3.3. Anatomical & physiological considerations of mandibular Anatomical & physiological considerations of mandibular osteotomies osteotomies
4.4. Timing for the mandibular osteotomiesTiming for the mandibular osteotomies
5.5. Mandibular osteotomiesMandibular osteotomies
6.6. Soft tissue changes after mandibular osteotomiesSoft tissue changes after mandibular osteotomies
7.7. ComplicationsComplications
8.8. Current concepts in mandibular osteotomiesCurrent concepts in mandibular osteotomies

INTRODUCTIONINTRODUCTION
HISTORYHISTORY• Orthognathic surgery was originally developed in the United States of Orthognathic surgery was originally developed in the United States of
America (America (Steinhäuser 1996). Steinhäuser 1996).
• The The first mandibular osteotomy ifirst mandibular osteotomy is considered to be s considered to be Hullihen´s Hullihen´s
procedure in 1849 procedure in 1849 to correct anterior open bite & mandibular to correct anterior open bite & mandibular
dentoalveolar protrusion with an intraoral osteotomy.dentoalveolar protrusion with an intraoral osteotomy.
• Osteotomy of the mandibular bodyOsteotomy of the mandibular body for the correction of for the correction of
mandibular horizontal excess was performed by mandibular horizontal excess was performed by Vilray Blair.Vilray Blair.
• Berger (1897) Berger (1897) described a condylar osteotomy for the correction of described a condylar osteotomy for the correction of
prognathism.prognathism.
• Limberg in 1925 Limberg in 1925 first reported the first reported the subcondylar osteotomysubcondylar osteotomy as an as an
extraoral technique, later it was modified to the intraoral vertical extraoral technique, later it was modified to the intraoral vertical
subcondylar osteotomy.subcondylar osteotomy.
• A variation of the vertical subcondylar osteotomy was suggested by A variation of the vertical subcondylar osteotomy was suggested by
wassmund in 1927,wassmund in 1927,which is similar to the inverted –L-osteotomy.which is similar to the inverted –L-osteotomy.

• Hofer in 1936Hofer in 1936 demonstrated an demonstrated an anterior mandibular alveolar osteotomyanterior mandibular alveolar osteotomy to to
advance anterior teeth in correction of a mandibular dentoalveolar retrusion. advance anterior teeth in correction of a mandibular dentoalveolar retrusion.
• In 1954, Caldwell and Letterman In 1954, Caldwell and Letterman developed developed a a vertical ramus osteotomy vertical ramus osteotomy
techniquetechnique, , which had the advantage of minimizing trauma to the inferior which had the advantage of minimizing trauma to the inferior
alveolar neurovascular bundle. alveolar neurovascular bundle.
• The greatest development in osteotomies of the vertical ramus is the The greatest development in osteotomies of the vertical ramus is the sagittal sagittal
split osteotomysplit osteotomy credited to credited to obwegeser in 1955obwegeser in 1955. The major modifications in the . The major modifications in the
osteotomies design were first made by osteotomies design were first made by Dalpont in 1961Dalpont in 1961.This was further .This was further
discussed by discussed by Hunsuck in 1968 Hunsuck in 1968 inorder to decrease the trauma to overlying soft inorder to decrease the trauma to overlying soft
tissues.tissues.
• Kent & Hinds in 1971 Kent & Hinds in 1971 initially presented the use of single tooth osteotomies of the initially presented the use of single tooth osteotomies of the
mandible.mandible.
• Macintosh Macintosh closely followed with his description of the total mandibular alveolar closely followed with his description of the total mandibular alveolar
osteotomy in osteotomy in 1974.1974.

AIMS OF MANDIBULAR OSTEOTOMIESAIMS OF MANDIBULAR OSTEOTOMIES

PRINCIPLES IN TREATING MANDIBULAR PRINCIPLES IN TREATING MANDIBULAR DEFORMITIESDEFORMITIES
• Patient’s perception of the deformity and expectationsPatient’s perception of the deformity and expectations
• Surgeon’s recognition of the deformitySurgeon’s recognition of the deformity
• Complete Physical examination, model surgery, Complete Physical examination, model surgery,
cephalometric analysiscephalometric analysis
• optimal treatment planoptimal treatment plan
• Counselling of the patientCounselling of the patient
• Informed consentInformed consent

VASCULAR STRUCTURESVASCULAR STRUCTURES
Bell and Levy’s work {1970} Bell and Levy’s work {1970} demonstrated that blood flow demonstrated that blood flow through the mandibular periosteum could easily maintain a through the mandibular periosteum could easily maintain a sufficient blood supply to the teeth of a mobile segment, even sufficient blood supply to the teeth of a mobile segment, even when the labial periosteum was deglovedwhen the labial periosteum was degloved..
subapical osteotomies subapical osteotomies need to be carefully planned to ensure as need to be carefully planned to ensure as large a vascular pedicle as possiblelarge a vascular pedicle as possible. .
The proximal segment of the The proximal segment of the vertical subsigmoid osteotomy vertical subsigmoid osteotomy maintains its blood supply through the temporomandibular joint maintains its blood supply through the temporomandibular joint capsule and the attachment of the lateral pterygoid muscle. But capsule and the attachment of the lateral pterygoid muscle. But the inferior tip of this fragment has undergone vascular necrosis the inferior tip of this fragment has undergone vascular necrosis in some studies. This led to the suggestion that fewer problems in some studies. This led to the suggestion that fewer problems may occur if the cut was made above the angle of the mandible. may occur if the cut was made above the angle of the mandible. And we should minimize the periosteal and muscle attachment And we should minimize the periosteal and muscle attachment stripping on the medial surface of the proximal fragment with stripping on the medial surface of the proximal fragment with either the C or L osteotomy or any of their variations.either the C or L osteotomy or any of their variations.
The greater distance from the apices of the teeth not only The greater distance from the apices of the teeth not only minimizes direct minimizes direct pulpal injury pulpal injury but increases the vascular but increases the vascular pedicle to the mobile segment as well.pedicle to the mobile segment as well.
NERVESNERVES
• In most cases in orthognathic surgery avoiding injury to In most cases in orthognathic surgery avoiding injury to marginal marginal mandibular branch of facial nervemandibular branch of facial nerve is achieved because soft tissue is achieved because soft tissue anatomy in patients undergoing the surgery has not been anatomy in patients undergoing the surgery has not been disturbed by disease or traumadisturbed by disease or trauma. .
• The course of the The course of the inferior alveolar nerveinferior alveolar nerve into the vertical ramus into the vertical ramus and then through the body of the mandible makes it extremely and then through the body of the mandible makes it extremely susceptible to damage from almost every mandibular surgical susceptible to damage from almost every mandibular surgical procedure. In most cases the procedure. In most cases the surgeon’s main goal relative to surgeon’s main goal relative to this nerve is only to minimize the traumathis nerve is only to minimize the trauma because its because its avoidance is almost impossible.avoidance is almost impossible.
MUSCLESMUSCLES
Orthognathic surgery affects muscles in primarily Orthognathic surgery affects muscles in primarily
two ways: two ways:
• It changes the length of a muscle or it changes the It changes the length of a muscle or it changes the
direction of muscle function. direction of muscle function.
• The muscles commonly discussed in orthognathic The muscles commonly discussed in orthognathic
surgery of the mandible have been the muscles of surgery of the mandible have been the muscles of
mastication and the suprahyoid group of muscles .mastication and the suprahyoid group of muscles .

• Evaluation of horizontal osteotomy of Evaluation of horizontal osteotomy of
vertical ramus procedure following vertical ramus procedure following
correction of prognathism found a superior correction of prognathism found a superior
movement of the mandible in the gonial movement of the mandible in the gonial
region as well as a downward and region as well as a downward and
backward movement at the symphysis. backward movement at the symphysis.
This change was attributed to the forces of This change was attributed to the forces of
the pterygomasseteric sling .the pterygomasseteric sling .

TIMING OF OSTEOTOMYTIMING OF OSTEOTOMY
Rule of ThumbRule of Thumb
Union of epiphysis & diaphysisUnion of epiphysis & diaphysis
Indications for mandibular orthognathic surgery during growthIndications for mandibular orthognathic surgery during growth

MANDIBULAR OSTEOTOMIESMANDIBULAR OSTEOTOMIES
• VERTICAL RAMUS OSTEOTOMIESVERTICAL RAMUS OSTEOTOMIES
• HORIZONTAL RAMUS OSTEOTOMIESHORIZONTAL RAMUS OSTEOTOMIES
• SUB APICAL OSTEOTOMIES[segmental SUB APICAL OSTEOTOMIES[segmental osteotomies]osteotomies]
• TOTAL ALVEOLAR OSTEOTOMIESTOTAL ALVEOLAR OSTEOTOMIES
• HORIZONTAL OSTEOTOMY OF HORIZONTAL OSTEOTOMY OF SYMPHYSIS/ SYMPHYSIS/ GENIOPLASTYGENIOPLASTY
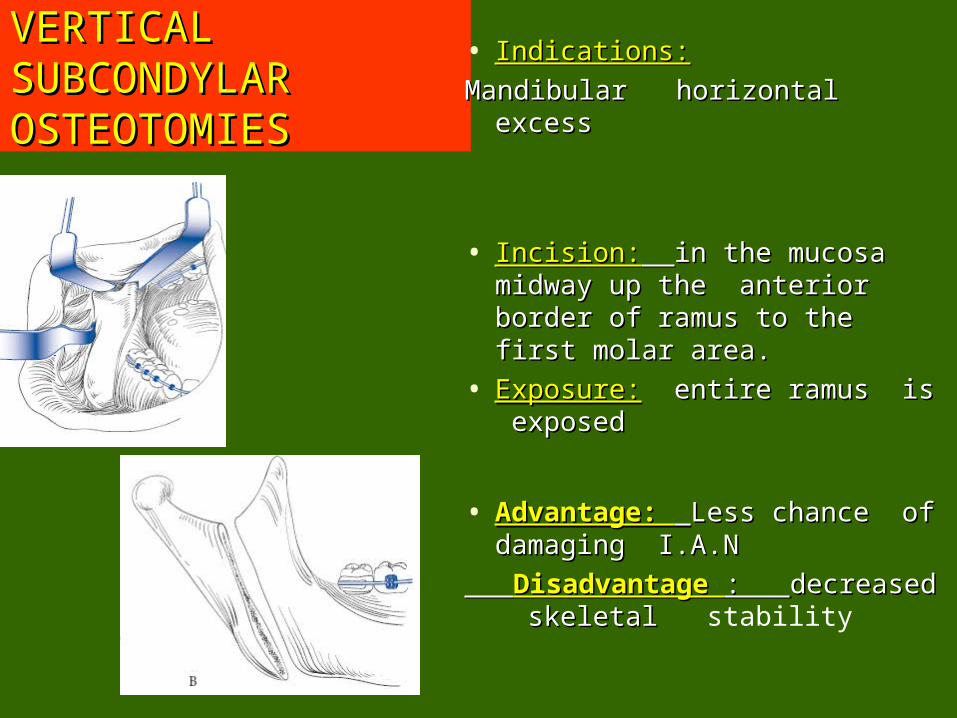
VERTICAL VERTICAL SUBCONDYLAR SUBCONDYLAR OSTEOTOMIESOSTEOTOMIES
• Indications:Indications:
Mandibular horizontal excessMandibular horizontal excess
• Incision:Incision: in the mucosa in the mucosa midway up the anterior midway up the anterior border of ramus to the first border of ramus to the first molar area.molar area.
• Exposure:Exposure: entire ramus is entire ramus is exposedexposed
• Advantage: Advantage: Less chance of Less chance of damaging I.A.Ndamaging I.A.N
Disadvantage Disadvantage : : decreased decreased skeletal skeletal stability
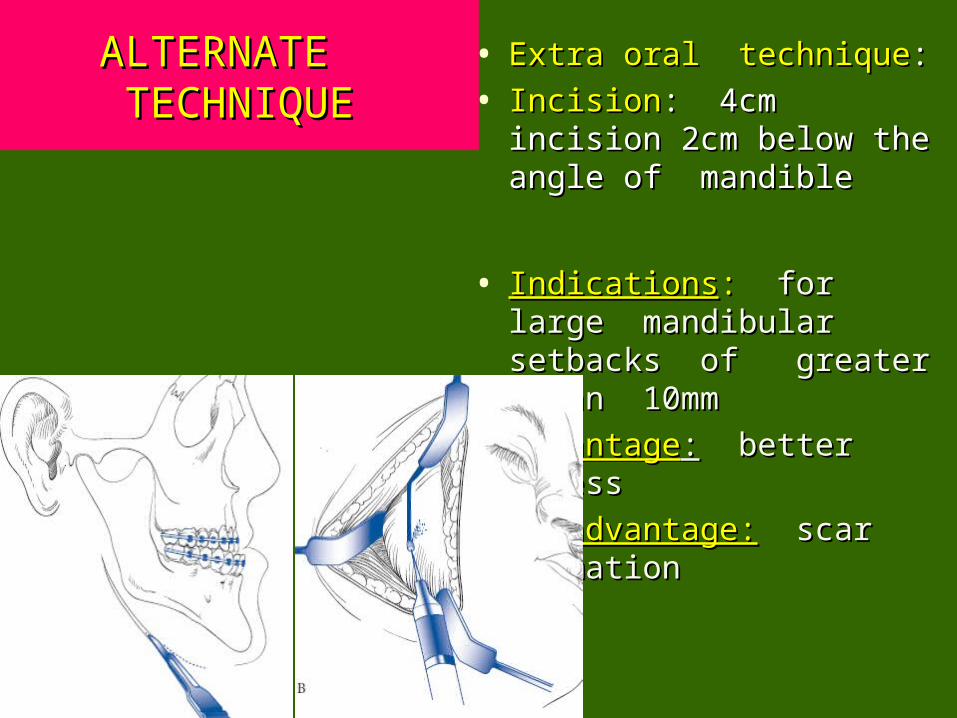
ALTERNATE ALTERNATE TECHNIQUETECHNIQUE
• Extra oral techniqueExtra oral technique::
• IncisionIncision: 4cm incision 2cm : 4cm incision 2cm below the angle of below the angle of mandiblemandible
• IndicationsIndications: : for large for large mandibular setbacks of mandibular setbacks of greater than 10mmgreater than 10mm
• AdvantageAdvantage:: better access better access
• Disadvantage:Disadvantage: scar scar formation formation

INVERTED L & C INVERTED L & C RAMUS RAMUS OSTEOTOMIESOSTEOTOMIES
Trauner and Trauner and Obwegeser in 1957 Obwegeser in 1957
Indications:Indications: horizontal horizontal mandibular mandibular deficiencies.deficiencies.
IncisionIncision:: 6cm 6cm submandibular submandibular incision 2cm below incision 2cm below the angle & inferior the angle & inferior border of mandibleborder of mandible
Exposure:Exposure: entire ramus entire ramus

ALTERNATE TECHNIQUES FOR ALTERNATE TECHNIQUES FOR INVERTED L OSTEOTOMIESINVERTED L OSTEOTOMIES
• Advantage :to Advantage :to increase the bone increase the bone contact during contact during advancementadvancement
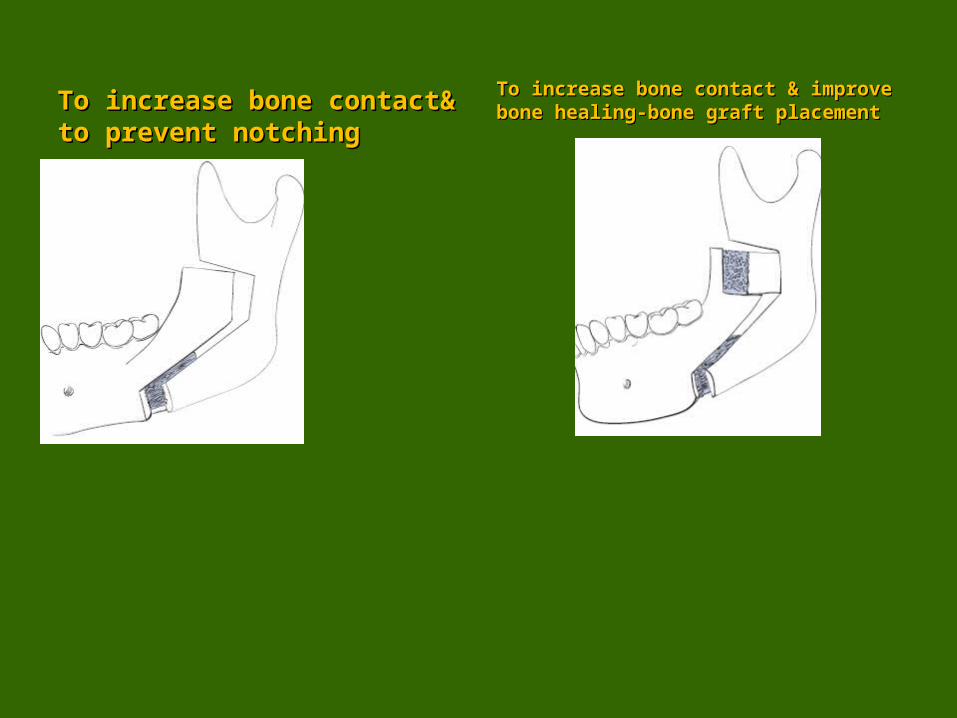
To increase bone contact& To increase bone contact& to prevent notchingto prevent notching
To increase bone contact & improve To increase bone contact & improve bone healing-bone graft placementbone healing-bone graft placement
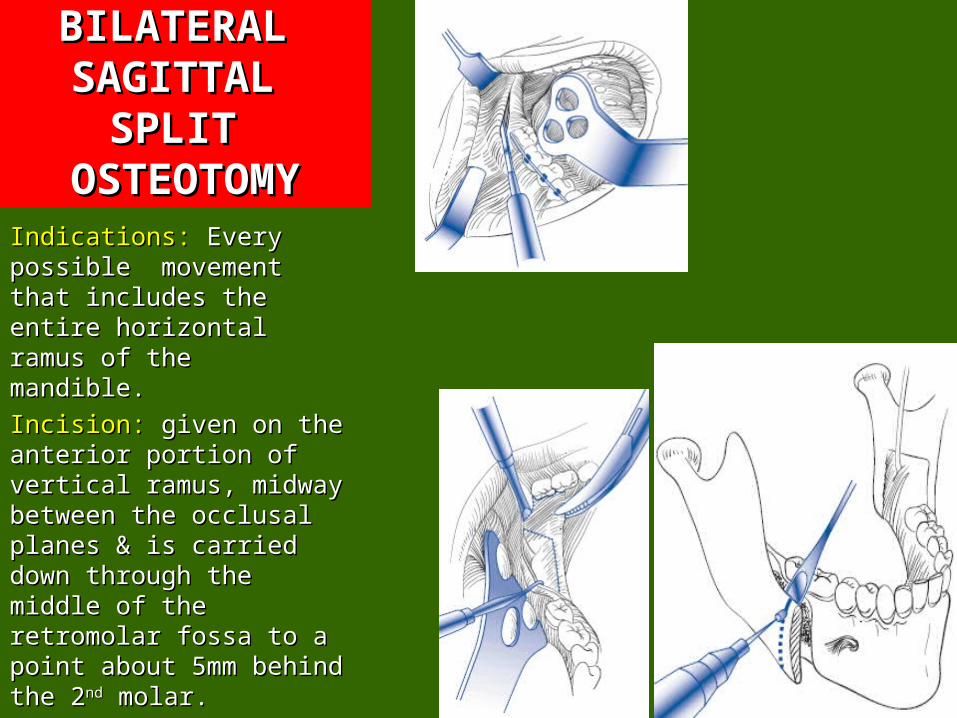
BILATERAL BILATERAL SAGITTAL SAGITTAL
SPLIT SPLIT OSTEOTOMYOSTEOTOMY
Indications: Indications: Every Every possible movement possible movement that includes the entire that includes the entire horizontal ramus of the horizontal ramus of the mandible.mandible.
Incision:Incision: given on the given on the anterior portion of anterior portion of vertical ramus, midway vertical ramus, midway between the occlusal between the occlusal planes & is carried down planes & is carried down through the middle of through the middle of the retromolar fossa to the retromolar fossa to a point about 5mm a point about 5mm behind the 2behind the 2ndnd molar. molar.
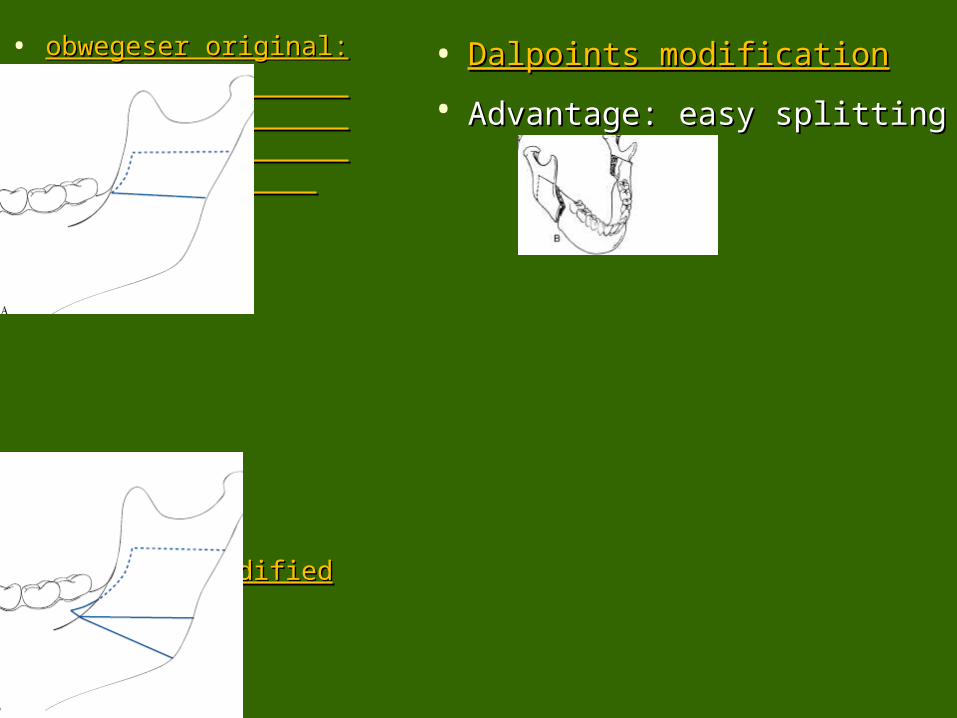
• Dalpoints modificationDalpoints modification
• Advantage: easy splittingAdvantage: easy splitting
• obwegeser original:obwegeser original:
•
• Obwegeser modifiedObwegeser modified

HORIZONTAL HORIZONTAL RAMUS RAMUS
OSTEOTOMIESOSTEOTOMIES INDICATIONS:INDICATIONS:
• PrognathismPrognathism
• Incision: Incision: is made 4-is made 4-5mm below the level of 5mm below the level of attached gingiva& is attached gingiva& is carried forward at this carried forward at this level until the canine, level until the canine, where it can be where it can be dropped down 5mm & dropped down 5mm & extended forward to extended forward to the midline.the midline.
SUBAPICAL OSTEOTOMIESSUBAPICAL OSTEOTOMIES
• Anterior subapical Anterior subapical
• Posterior subapicalPosterior subapical
• Total alveolar osteotomyTotal alveolar osteotomy

ANTERIOR SUBAPICAL OSTEOTOMYANTERIOR SUBAPICAL OSTEOTOMY
• Indications: To move the Indications: To move the anterior mandible in every anterior mandible in every desirable desirable direction[direction[ant,post,sup,inf-ant,post,sup,inf-repositioningrepositioning]]
• Incision : is started 1cm Incision : is started 1cm behind the planned behind the planned vertical osteotomy& is vertical osteotomy& is carried 4-5mm below the carried 4-5mm below the attached gingiva & is attached gingiva & is brought to the midline & brought to the midline & connected with the connected with the opposing incision.opposing incision.

POSTERIOR SUBAPICAL OSTEOTOMYPOSTERIOR SUBAPICAL OSTEOTOMY
• Correction of Correction of supraeruption of supraeruption of posterior mandibular posterior mandibular teeth.teeth.
• Ankkylosis of some Ankkylosis of some posterior teeth.posterior teeth.
• Abnormal buccal/lingual Abnormal buccal/lingual position of teeth.position of teeth.
• Incision is made at the Incision is made at the anterior border of anterior border of vertical ramus & is vertical ramus & is carried forward to the carried forward to the caninecanine
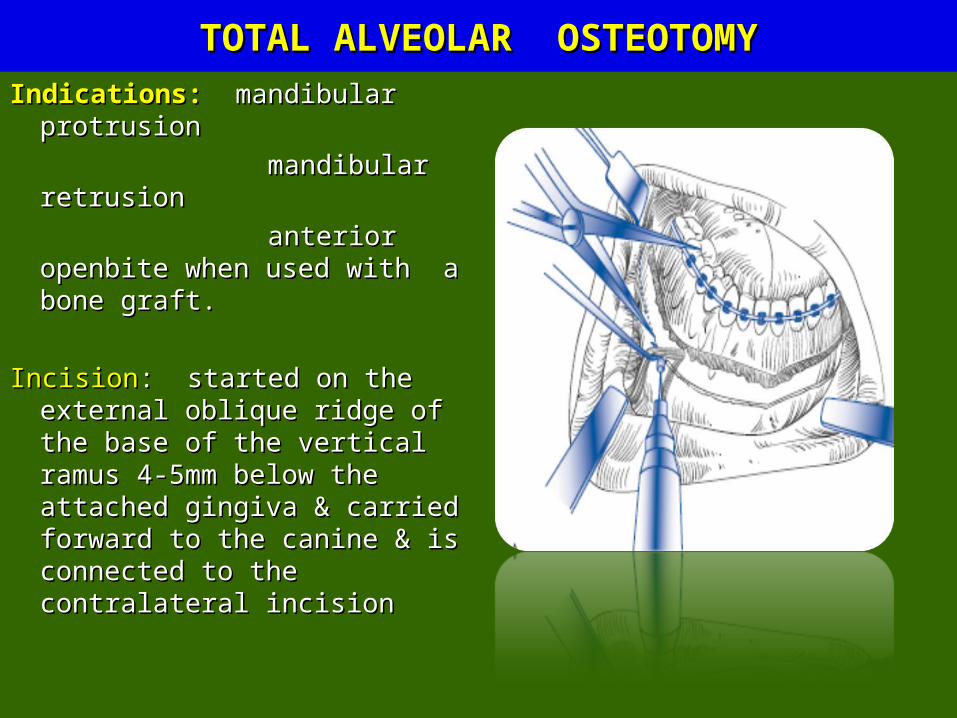
TOTAL ALVEOLAR OSTEOTOMYTOTAL ALVEOLAR OSTEOTOMY
Indications:Indications: mandibular mandibular protrusionprotrusion
mandibular retrusionmandibular retrusion
anterior openbite anterior openbite when used with a bone when used with a bone graft.graft.
IncisionIncision: started on the : started on the external oblique ridge of the external oblique ridge of the base of the vertical ramus 4-base of the vertical ramus 4-5mm below the attached 5mm below the attached gingiva & carried forward to gingiva & carried forward to the canine & is connected to the canine & is connected to the contralateral incisionthe contralateral incision

ALTERNATE ALTERNATE TECHNIQUE-TOTAL TECHNIQUE-TOTAL
ALVEOLAR ALVEOLAR OSTEOTOMYOSTEOTOMY
Total alvoelar Total alvoelar osteotomy+ Sagittal split osteotomy+ Sagittal split osteotomy of vertical osteotomy of vertical ramusramus..
ADVANTAGESADVANTAGES: osteotomy : osteotomy made below the inferior made below the inferior alveolar nerve there by alveolar nerve there by decreasing the risk of decreasing the risk of damaging the damaging the IAN ,apices of the teeth IAN ,apices of the teeth & preserving vascular & preserving vascular supply to the mobile supply to the mobile segment, also sagittal segment, also sagittal part allows a larger bone part allows a larger bone contact area to assist in contact area to assist in healinghealing..

HORIZONTAL OSTEOTOMY OF SYMPHYSIS/ GENIOPLASTYHORIZONTAL OSTEOTOMY OF SYMPHYSIS/ GENIOPLASTY
• Indications: Indications: All types of All types of skeletal abnormalities of skeletal abnormalities of chinchin
• Incision;Incision; labial vestibule labial vestibule to its depth & extends to its depth & extends posteriorly to the 1posteriorly to the 1stst premolar.premolar.

Obwegesser modificationObwegesser modification
• Midsagittal osteotomy of Midsagittal osteotomy of inferior fragment is inferior fragment is helpful in preventing the helpful in preventing the prominence of the prominence of the posterior ends of the posterior ends of the fragment,relative to fragment,relative to mandible as fragment is mandible as fragment is advancedadvanced
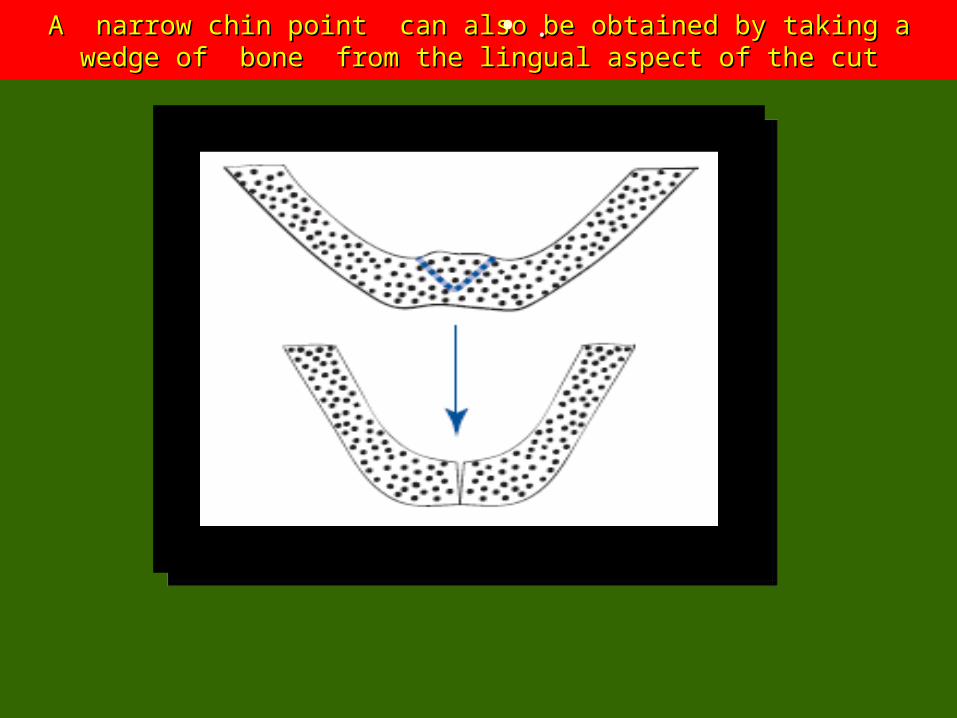
A narrow chin point can also be obtained by taking a wedge of bone A narrow chin point can also be obtained by taking a wedge of bone from the lingual aspect of the cut from the lingual aspect of the cut
• ..

• Overlapping an Overlapping an advanced inferior advanced inferior fragment on the fragment on the lateral cortex of lateral cortex of the symphysis the symphysis allows both an allows both an increase in increase in horizontal horizontal prominence as prominence as well as a decrease well as a decrease in the anterior in the anterior mandibular mandibular vertical heightvertical height
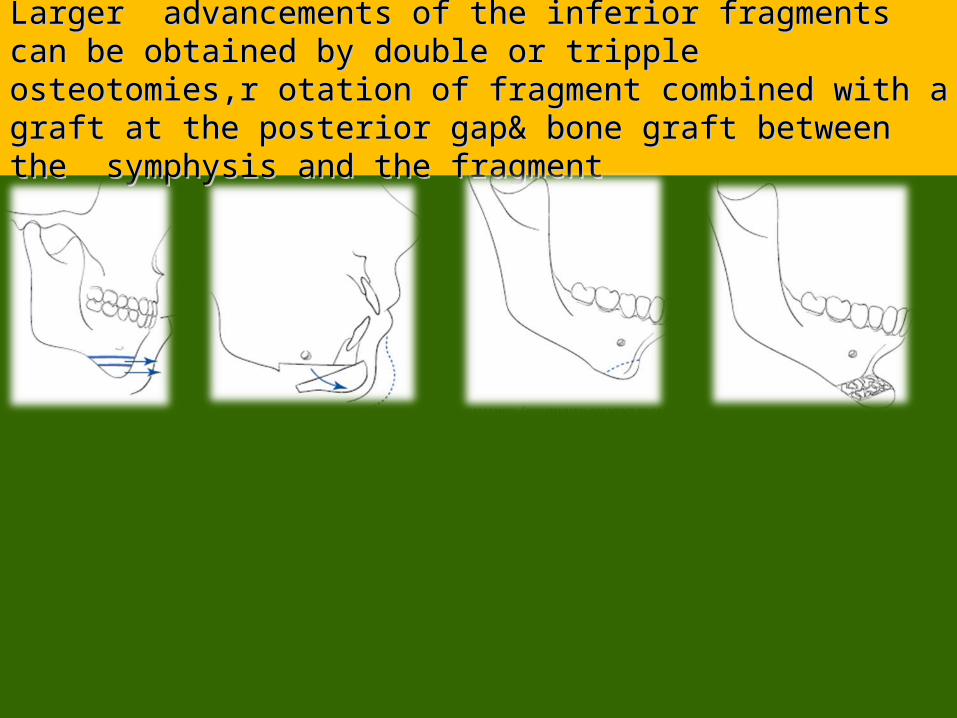
Larger advancements of the inferior fragments can be Larger advancements of the inferior fragments can be obtained by double or tripple osteotomies,r otation of obtained by double or tripple osteotomies,r otation of fragment combined with a graft at the posterior gap& fragment combined with a graft at the posterior gap& bone graft between the symphysis and the fragmentbone graft between the symphysis and the fragment
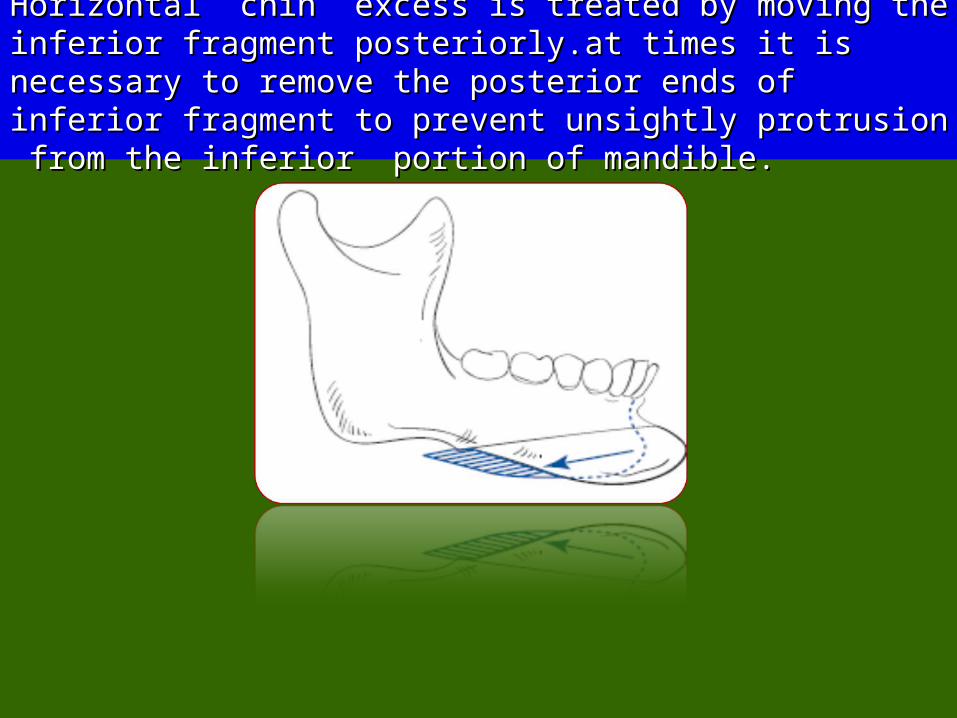
Horizontal chin excess is treated by moving the inferior Horizontal chin excess is treated by moving the inferior fragment posteriorly.at times it is necessary to remove fragment posteriorly.at times it is necessary to remove the posterior ends of inferior fragment to prevent the posterior ends of inferior fragment to prevent unsightly protrusion from the inferior portion of unsightly protrusion from the inferior portion of mandible.mandible.

When the patient has normal facial height,the plane of When the patient has normal facial height,the plane of the osteotomy should parallel the F-H plane,then the osteotomy should parallel the F-H plane,then anterior chin projection can be reduced by parallel/ v-anterior chin projection can be reduced by parallel/ v-shaped osteotomies in vertical plane,with middle segment shaped osteotomies in vertical plane,with middle segment removed.removed.

Vertical symphysis excess can be reduced by removing Vertical symphysis excess can be reduced by removing middle segment of bone when the plane of 2 parallel middle segment of bone when the plane of 2 parallel osteotomies is more horizontalosteotomies is more horizontal
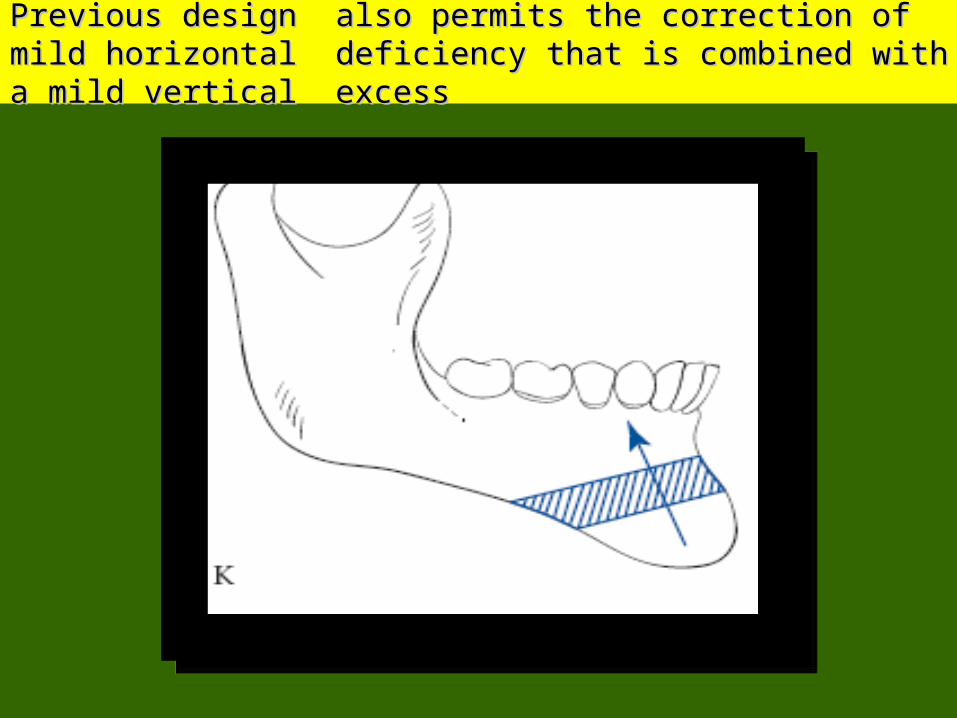
Previous design also permits the correction of mild Previous design also permits the correction of mild horizontal deficiency that is combined with a mild vertical horizontal deficiency that is combined with a mild vertical excess excess

Above mentioned skeletal problem can also be corrected Above mentioned skeletal problem can also be corrected by making a single osteotomy more vertical& moving the by making a single osteotomy more vertical& moving the segment anteriorly& forwardsegment anteriorly& forward

Vertical symphyseal deficiency managed only by some Vertical symphyseal deficiency managed only by some type of interpositional material with either bone grafts type of interpositional material with either bone grafts or implantsor implants

SOFT TISSUE CHANGES INDUCED BY SOFT TISSUE CHANGES INDUCED BY SURGERYSURGERYAdvancement of the mandibleAdvancement of the mandible: increase in lower lip protrusion: increase in lower lip protrusion
chin prominenecechin prominenece
enhanced chin neck definitionenhanced chin neck definition
decreased prominence of labiomental decreased prominence of labiomental foldfold
decreased lower lip eversiondecreased lower lip eversion
increased lower third facial heightincreased lower third facial height
Total subapical surgery for dentoalveolar horizontal Total subapical surgery for dentoalveolar horizontal deficiency:deficiency:
• Increased lower lip prominence,I ncreased lower facial Increased lower lip prominence,I ncreased lower facial height,decreased depth of labiomental fold.height,decreased depth of labiomental fold.
Correction of Mandibular horizontal excess:Correction of Mandibular horizontal excess: reduced chin reduced chin prominence & lower lip eversion, decrased lower facial height, prominence & lower lip eversion, decrased lower facial height, increased prominence of angles.increased prominence of angles.
Excessive setbacks in older & obese individuals:Excessive setbacks in older & obese individuals: increased increased fullness in the submental region & produce poor chin & neck fullness in the submental region & produce poor chin & neck contour.contour.
COMPLICATIONSCOMPLICATIONS
• Bleeding.Bleeding.
• Hematoma formation- Hematoma formation- condylar resections and genioplasties.condylar resections and genioplasties.
• post-operative dysfunction of inferior alveolar nerve post-operative dysfunction of inferior alveolar nerve is greatest in is greatest in body osteotomies, but it is seen to a lesser degree in sagittal split.body osteotomies, but it is seen to a lesser degree in sagittal split.
• In extra-oral approach, injury to the In extra-oral approach, injury to the main trunk or marginal main trunk or marginal mandibular branch of facial nervemandibular branch of facial nerve..
The neurosensory disturbances are usually transient, lasting for The neurosensory disturbances are usually transient, lasting for weeks to months. The duration and severity of the problem is weeks to months. The duration and severity of the problem is directly related to the degree of trauma inflicted on the nerves. directly related to the degree of trauma inflicted on the nerves. Direct nerve injury, such as transection, requires immediate Direct nerve injury, such as transection, requires immediate microneuronal repair for optimal recovery.microneuronal repair for optimal recovery.
• unfavourable splits may cause unfavourable splits may cause fractures of the proximal or distal fractures of the proximal or distal segmentsegment. The most common factor causing a proximal segment . The most common factor causing a proximal segment fracture is the failure to cut the inferior border prior to applying fracture is the failure to cut the inferior border prior to applying chisels to the osteotomy. When this occurs, the fracture line chisels to the osteotomy. When this occurs, the fracture line propagates along the buccal a Adverse distal segment fractures propagates along the buccal a Adverse distal segment fractures may be splits that are short of the lingula, medial splits up the may be splits that are short of the lingula, medial splits up the condyle and those occurring just distal to the second molar. condyle and those occurring just distal to the second molar.

REFERENCESREFERENCES
• Peterson s- principles of oral and maxillofacial Peterson s- principles of oral and maxillofacial surgery-2surgery-2ndnd edition edition
• Historical developments of orthognathic surgery. Historical developments of orthognathic surgery. E. W. E. W. SteinhauserSteinhauser. Journal of cranio-Maxillofacial surgery. . Journal of cranio-Maxillofacial surgery. 1996: 24 : 195 – 204.1996: 24 : 195 – 204.
• Mandibular procedures. Fonseca . Orthognathic Mandibular procedures. Fonseca . Orthognathic surgery. Text book of oral and maxillofacial surgery.surgery. Text book of oral and maxillofacial surgery.

• Mandibular prognathism. Mandibular prognathism. David Hall, Ronald HathawayDavid Hall, Ronald Hathaway. . Mandibular deficiency. Mandibular deficiency. David J. Darab. David J. Darab. Modern practice Modern practice of orthognathic and reconstructive surgery. of orthognathic and reconstructive surgery. William H. William H. Bell.Bell. W. B. Saunders company. 1992. Vol. III. 2110 – W. B. Saunders company. 1992. Vol. III. 2110 –2140, 2334-2517.2140, 2334-2517.
• Orthognathic Surgery. Orthognathic Surgery. edited byedited by N. J. Betts, T. A. N. J. Betts, T. A. Turvey.Turvey. In Oral and Maxillofacial Surgery. In Oral and Maxillofacial Surgery. edited byedited by R. J. R. J. Fonseca.Fonseca. W. B. Saunders company. 1992. Vol II. W. B. Saunders company. 1992. Vol II.
• Surgical Correction of Dentofacial Deformities. Surgical Correction of Dentofacial Deformities. Bell, Bell, Profitt and White.Profitt and White.
• Aesthetic Surgery of the face. Aesthetic Surgery of the face. Varghese Mani Varghese Mani
• Textbook of Oral and Maxillofacial Surgery. Textbook of Oral and Maxillofacial Surgery. Gustav O. Gustav O. KrugerKruger
