management of status epilepticus in children
TRANSCRIPT
• Definition• EPIDEMIOLOGY• Pathology• Classification• Risk factors• Immediate assessment
• Immediate Treatment• Laboratory studies• Stabilization• Monitoring • PHARMACOLOGIC
AGENTS• Prognosis
Definition
Status Epilepticus: The International League Against Epilepsy (ILAE) and the World
Health Organization currently define SE as a “condition characterized by an epileptic seizure that is
so frequently repeated or so prolonged as to create a fixed and lasting condition”
Definitionpractical definition of SE
has emerged as any seizure that lasts more than 5 minutes
continuous seizure activity or recurrent seizure activity without regaining of consciousness lasting for more than 5 min
Definitionpractical definition of SE
has emerged as any seizure that lasts more than 5 minutes
Nonconvulsive SE (NCSE) refers to ongoing EEG seizure activity without associated clinical
signs.

DefinitionRefractory Status Epilepticus :
failed to respond to therapy, usually with at least 2 (such as a benzodiazepine and another medication) medications.
New-onset refractory status epilepticus (NORSE): refractory status epilepticus in a patient without prior epilepsy
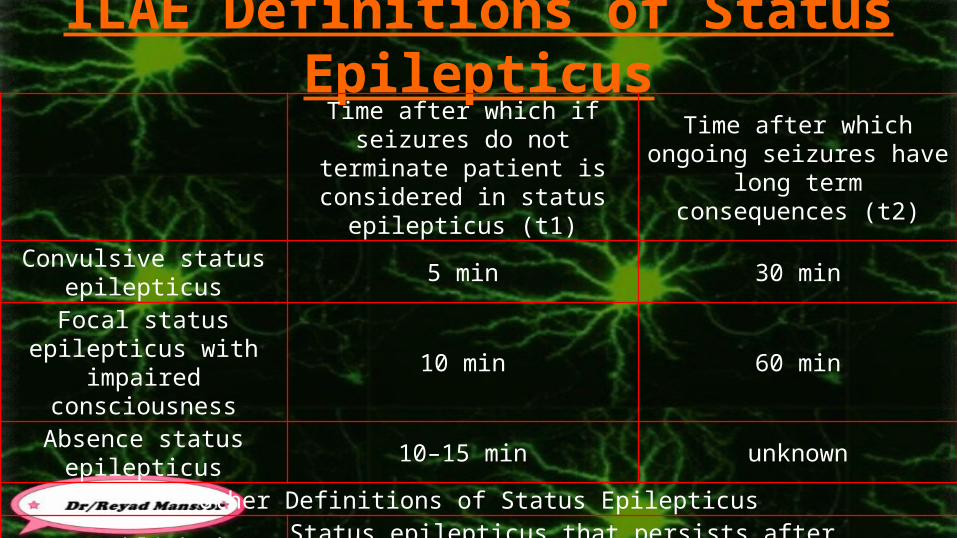
ILAE Definitions of Status EpilepticusTime after which if seizures do not terminate patient is considered in
status epilepticus (t1)
Time after which ongoing seizures have long term
consequences (t2)Convulsive status epilepticus 5 min 30 minFocal status epilepticus with
impaired consciousness 10 min 60 min
Absence status epilepticus 10–15 min unknownOther Definitions of Status Epilepticus
Established statusepilepticus Status epilepticus that persists after treatment with a benzodiazepine (1st line treatment)
Refractory status epilepticus
Status epilepticus that persists after a 1st line agent (benzodiazepine) and 2nd linesagent (additional agent such as levetiracetam, phenytoin, valproic acid) have failed
Definition New-onset refractory status epilepticus (NORSE):
refractory status epilepticus in a patient without prior epilepsy
fever-induced refractory epileptic encephalopathy in school age children
(FIRES)
is a syndrome of refractory status epilepticus that is associated with
acute febrile infections, appears to be parainfectious in nature, and to
be highly drug resistant but responsive to the ketogenic diet.


Definition*
several clinical studies have been published using durations of 5 minutes
More information is needed to clarify and allow acceptance of a standard operational definition for SE.
• incidence of status epilepticus ranges between 10 and 60 per 100,000 population
• Status epilepticus is most common in children younger than 5 yr of age, with an incidence in this age group of >100 per 100,000 children.
EPIDEMIOLOGY

• Approximately 30% of patients presenting with status epilepticus are having their first seizure, and approximately 40% of these later develop epilepsy
EPIDEMIOLOGY

• Febrile status epilepticus is the most common type of status epilepticus in children.
• In the 1950s and 1960s, mortality rates of 6-18% were reported after status epilepticus; currently, with the recognition of status epilepticus as a medical emergency, a lower mortality rate of 4-5% is observed, most of it secondary to the underlying etiology rather than to the seizures.
• Status epilepticus carries an approximately 14% risk of new neurologic deficits, most of this (12.5%) secondary to the underlying pathology.
EPIDEMIOLOGY
1. convulsive SE (CSE)2. nonconvulsive SE (NCSE) : There are
10-20%

1. Neuronal (Cerebral) 2. Systemic Effects.

Cerebral Injury
DISTURBANCE EQUALIBRIMExcitation >inhibitory mechanisms
PROLONGED : SE
Systemic Complications.
+vE
Precipitating factors
+vE

1. Downregulation Of GABAA Receptors May Reduce The Efficacy Of Benzodiazepines In RSE
2. Extrusion Of Anticonvulsants Across The Blood-brain Barrier (BBB) May Limit Anticonvulsant Activity.
3. Over Expression Of The Transporter's Multidrug Resistance Gene
1. Ensure adequate brain oxygenation , cardiorespiratory function2. Terminate clinical , electrical seizure activity as rapidly as possible3. Prevent seizure recurrence4. Identify precipitating factors such as hypoglycemia, electrolyte
imbalance, lowered drug levels, infection, and fever5. Correct metabolic imbalance6. Prevent systemic complications7. Further evaluate and treat the etiology of SE
Out of hospital management – Community education – Patients must be brought to the hospital at the earliest
Hospital emergency management PICU management
– It is helpful to have a protocol in every hospital.


1. Look for medical identification.2. Protect the person from nearby hazards.3. Loosen ties or shirt collars.4. Protect the head from injury.5. Turn the person on his side to keep the airway clear.6. Time record7. Reassure when consciousness returns.8. Ask whether hospital evaluation is wanted, call an ambulance

1. Do not put any hard implement in the mouth.2. Do not try to hold the tongue. It cannot be swallowed.3. Do not try to give liquids during or just after the seizure.4. Do not use artificial respiration unless breathing is absent after muscle
jerks subside, or unless water has been inhaled.5. Do not restrain the person.6. The person should be transferred to a medical center as soon as
possible if their – seizure continues beyond 5 minutes– if after ceasing, it begins again
• The therapeutic window – for most effective treatment with benzodiazepines may have already passed
by the time that hospital treatment starts, which is usually more than 20 min after the onset of GTC-SE.
• administer drugs by 1. Buccal2. Rectal3. Nasal 4. other non-invasive routes
• if appropriately instructed and if proper “rescue medications” are available for emergency use

1. Rectal diazepam (0.5 mg/ kg for children )2. Buccal midazolam (0.4–0.5 mg/kg in children )3. Intranasal midazolam (0.2 mg/Kg in children ) For any of these medications a repeat dose can be
given at least 10 min after the first dose.

1. the seizure has happened in water.2. there's no medical I.D., and no way of knowing whether the seizure is caused
by epilepsy.3. the person is
1. Pregnant2. Injured3. diabetic.
4. the seizure continues for more than five minutes.5. a second seizure starts shortly after the first has ended.6. consciousness does not start to return after the shaking has stopped.
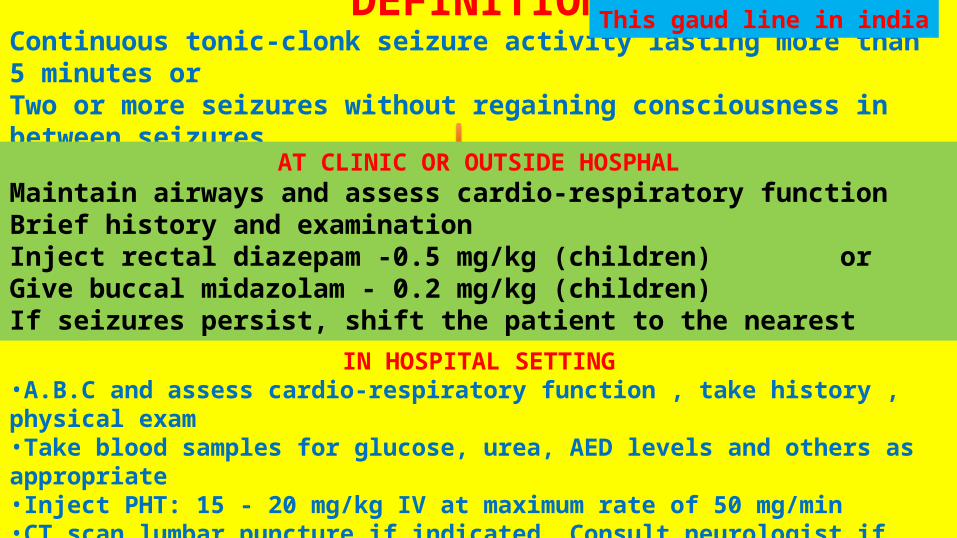
DEFINITIONContinuous tonic-clonk seizure activity lasting more than 5 minutes or Two or more seizures without regaining consciousness in between seizures
This gaud line in india
AT CLINIC OR OUTSIDE HOSPHALMaintain airways and assess cardio-respiratory functionBrief history and examinationInject rectal diazepam -0.5 mg/kg (children) orGive buccal midazolam - 0.2 mg/kg (children)If seizures persist, shift the patient to the nearest hospital
IN HOSPITAL SETTING•A.B.C and assess cardio-respiratory function , take history , physical exam•Take blood samples for glucose, urea, AED levels and others as appropriate•Inject PHT: 15 - 20 mg/kg IV at maximum rate of 50 mg/min•CT scan,lumbar puncture if indicated ,Consult neurologist if seizures persist


OVERVIEW OF ASSESSMENT The evaluation includes:
1. General assessment(ABC); the pediatric assessment triangle
appearance work of breathing circulation
2. Primary assessment: rapid evaluation of 1. Cardiopulmonary 2. Neurologic function
3. Secondary assessment : focused medical history and thorough head to toe physical exam
4. Tertiary assessment :1. Laboratory2. Radiographic3. other ancillary studies
32
Appearance (TICLS)1. Tone : abnormal tone2. Interactiveness : decreased
interactiveness3. Look/gaze : poor color4. Consolability : abnormal stare
Consolability 5. Speech/cry : weak cry.
Breathing:1. Abnormal airway sounds2. position of comfort that
maximizes airway opening3. use of accessory muscles
Circulation Assessment1.Heart rate2.Pulse3.capillary refill4.Blood pressure5.End organ profusion•Urine output•Level of consciousness •Muscle tone
Primary assessmentrapid sequence assess (ABCDE):1.Airway:
Patent patent with maneuvers/adjuncts partially or completely obstructed
2.Breathing: respiratory rate Effort tidal volume lung sounds pulse oximetry
3.Circulation:4)Disability
CNS function Level of conscious ; AVPU pediatric response scale:
Dextrose hypoglycemia :rapid bedside glucose or response to empiric
administration of dextrose6.Exposure :
fever or hypothermia, skin findings, trauma
Has the child ever had a seizure before?
History of :
Trauma?
Fever?
Ingestion?
Was the child his usual self prior to this event?
What medications child take?
Past- History:
Any medical problems?
Any neurologic ?
developmental problems?
If child has known epilepsy
Name and dosage of medications!!! Calculate if this is appropriate dosage.
Has the child missed dosage of medication
If so, consider loading with that medication
Be aware of paradoxical side effects of ACDS
• Phenytoin and carbamazepine toxicity may precipitate SE

1. Serum glucose and a rapid "finger-stick" glucose2. Serum electrolytes, calcium, and magnesium levels3. Arterial blood gases and pH , RFT , LFT4. A complete blood count and general chemical screen5. Urine and blood toxicology6. Serum antiepileptic drug (AED) levels
7. Other testing in specific clinical circumstances may include 1. Blood cultures and lumbar puncture (LP)2. Metabolic studies for inborn errors of
metabolism3. Neuroimaging is generally deferred until the
patient is stabilized.

Ancillary studies in children with status epilepticusPatient
population Studies All patients
Serum electrolytesSerum calcium, phosphate, and magnesiumBrain imaging (CT or MRI)EEG
Patient population Studies
Epilepsy pts on anticonvulsants
Anticonvulsant level
Patient population Studies
Febrile patients
CBC with differential , Blood cultureUrinalysis, urine cultureCSF culture (once seizures stopped and if brain imaging excludes increased intracranial pressure)
Patient population Studies Poisoned patient Urine screen for cocaine, amphetamines,
and PCPAspirin levelVenous or arterial pH and pCO2ECG once seizures stop
Patient Studies Infants <6 months of
age*
Blood gas , Plasma ammonia , Plasma amino acidsPT, PTTSerum AST, ALT, LDH, Alkaline phosphataseBlood lactate and pyruvateUrinalysis ,Urine for reducing substancesUrine organic acids ,Urine amino acidsCheck newborn urine screening results if infant from country where instituted
C. Electrocardiographic (ECG)
D. EEG monitoring

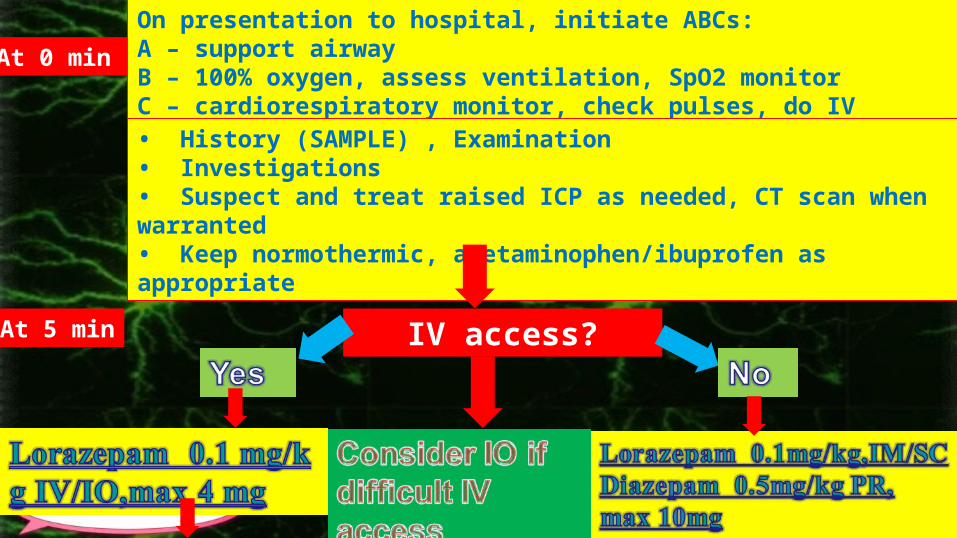
At 0 min On presentation to hospital, initiate ABCs: A – support airway B – 100% oxygen, assess ventilation, SpO2 monitor C – cardiorespiratory monitor, check pulses, do IV access • History (SAMPLE) , Examination• Investigations • Suspect and treat raised ICP as needed, CT scan when warranted • Keep normothermic, acetaminophen/ibuprofen as appropriate
At 5 min IV access?

Mistake Made In The Treatment Of SE
inadequate doses of drugs are given initially
physicians wait for more seizures to occur before administering the necessary total dose
1. Previous response2. Missed medication 3. Paradoxical effects 4. Nonprescription medications5. Alternative routes of administration6. Nonepileptic seizures
1. Rapid Onset Of Action2. Broad Spectrum Of Activity3. Ease Of Administration Including Intravenous (IV) And
Intramuscular (IM) Preparations4. Minimal Redistribution From The CNS5. Wide Therapeutic Safety Margin
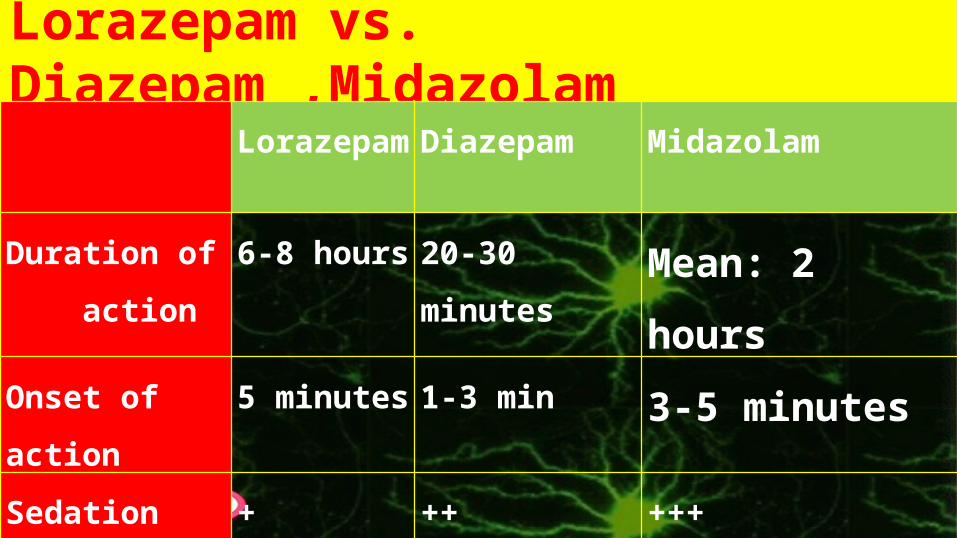
Lorazepam vs. Diazepam ,MidazolamLorazepam Diazepam Midazolam
Duration of
action
6-8 hours 20-30 minutes Mean: 2 hours
Onset of action 5 minutes 1-3 min 3-5 minutes
Sedation + ++ +++
• Mechanism of Action – Depresses all levels of the CNS, including the
limbic and reticular formation, by binding to the benzodiazepine site on the gamma-aminobutyric acid (GABA) receptor complex and modulating GABA, which is a major inhibitory neurotransmitter in the brain

• Dose : – 0.05-0.1 mg/kg
– (maximum: 4 mg/dose)
• Rate : – slow I.V. over 2-5 minutes
– (maximum rate: 2 mg/minute)
• Frequency : – may repeat every 10-15 minutes if needed
• Onset of action: – Oral: Within 60 minutes – I.M.: 30-60 minutes – I.V.: 15-30 minutes
• Duration: – 8-12 hours
• more effective than diazepam• Longer duration of action (6-12 hours vs. <1 hour)• Less respiratory depression than diazepam• Not available rectally
• dose: • Loading dose: 0.15-0.2 mg/kg• Continuous I.V. infusion:
• Initial rate: 0.06-0.12 mg/kg/hour (1-2 mcg/kg/minute); • increase rate every 5-15 minutes in increments of 0.06-0.24
mg/kg/hour (1-4 mcg/kg/minute) until seizure activity ceases• maximum dose: 3 mg/kg/hour (50 mcg/kg/minute)
• Onset of action: – Oral: Children: Within 10-20 minutes – I.M.:
• Children: Within 5 minutes • Adults: Within 15 minutes
– I.V.: Within 1-5 minutes – Intranasal: Within 5 minutes
• Maximum effect: – I.M.:
• Children: 15-30 minutes • Adults: 30-60 minutes
– I.V.: 5-7 minutes – Intranasal: 10 minutes
• Duration: – I.M.: Mean: 2 hours, up to 6 hours – I.V.: 20-30 minutes – Intranasal: 30-60 minutes – Note: Full recovery may take more than 24
hours
– Dose– Children 2-5 years: 0.5 mg/kg– Children 6-11 years: 0.3 mg/kg – Children ≥12 years and Adults: 0.2 mg/kg– Infants >30 days and Children: I.V: 0.1-0.3
mg/kg/dose given over 3-5 minutes, every 5–10 minutes
– (maximum: 10 mg/dose)
– Onset of action: – I.V.: 1-3 minutes – Rectal: 2-10 minutes – Duration: – 15-30 minutes
– Highly effective in rapidly terminating seizures
– However, redistribution into adipose tissue limits
anticonvulsant effect to less than 20 minutes
– Available in rectal gel, which can be given outside
the ED


At 0 min On presentation to hospital, initiate ABCs: A – support airway B – 100% oxygen, assess ventilation, SpO2 monitor C – cardiorespiratory monitor, check pulses, do IV access • History (SAMPLE) , Examination• Investigations • Suspect and treat raised ICP as needed, CT scan when warranted • Keep normothermic, acetaminophen/ibuprofen as appropriate
At 5 min IV access?
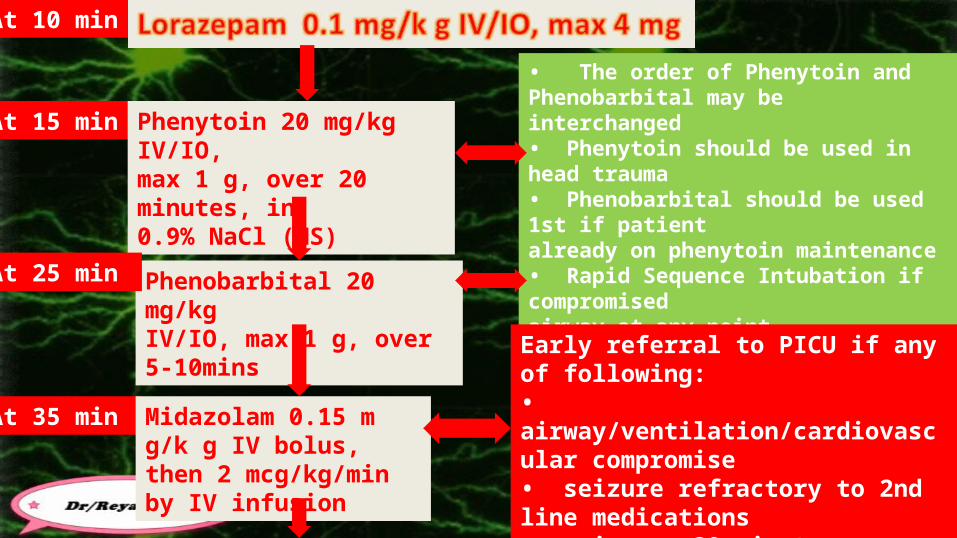
At 10 min
At 15 min Phenytoin 20 mg/kg IV/IO, max 1 g, over 20 minutes, in 0.9% NaCl (NS)
Phenobarbital 20 mg/kg IV/IO, max 1 g, over 5-10mins
At 25 min
• The order of Phenytoin and Phenobarbital may be interchanged • Phenytoin should be used in head trauma • Phenobarbital should be used 1st if patient already on phenytoin maintenance • Rapid Sequence Intubation if compromised airway at any point
• Ventilate to normal parameters • Sedation and muscle relaxants only if necessary to ventilate or protect airway
At 35 min
Early referral to PICU if any of following: • airway/ventilation/cardiovascular compromise• seizure refractory to 2nd line medications • seizure >30 minutes • initiating Midazolam or Thiopental infu
Midazolam 0.15 m g/k g IV bolus, then 2 mcg/kg/min by IV infusion

o seizure refractoryo prevent recurrance If seizures continue for 10 minutes after at least two injections
of lorazepam, begin treatment with fosphenytoin
dose of 20 mg phenytoin equivalents (PE)/kg IV at a rate of 3 mg/kg per minute (maximum rate 150 mg/min). The maximum dose in 24 hours is 1500 mg PE General rule of thumb: for each 1 mg/kg phenytoin (or 1PE/kg
fosphenytoin) expect level to rise by 1)
1. Alternative to second Line drugs Phenobarbital phenytoin4. Third Line medication
1. Valproic acid2. Levetiracetam
Alternative to second Line drugs 1. phenytoin (If fosphenytoin is unavailable)
dose :18 to 20 mg/kg IV , give in large vein, dilute with N/S rate of 1 mg/kg per minute maximum rate 50 mg/min. Maximum dose 1500mg/day onset of action: 10 - 30 min duration of action: 12 - 24 hr
2. Phenobarbital dose : 20 mg/kg rate 2 mg/kg per minute or 50 mg/min followed by repeated increments of approximately 8 to 10 mg/kg
every 30 minutes Maximum dose 1500mg/d
• Loading dose: – 15-18 mg/kg in a single or divided doses
• Maintenance dose : – usually starts 12 hours after the loading dose: – Infants and Children: Initial: 5-10 mg/kg/day in 2-3 divided
doses• onset of action may be delayed for 10 to 30 minutes
• Mechanism of Action• Stabilizes neuronal membranes and decreases seizure
activity by increasing efflux or decreasing influx of sodium ions across cell membranes in the motor cortex during generation of nerve impulses; prolongs effective refractory period and suppresses ventricular pacemaker automaticity, shortens action potential in the heart
• S/E - (most avoided if slower administration)1. hypotension2. arrhythmias - (must monitor)3. respiratory depression4. venous irritation5. extravasation -->tissue injury / necrosis6. “purple glove syndrome”: progressive limb edema,
discoloration and pain 2-12 hr post IV admin
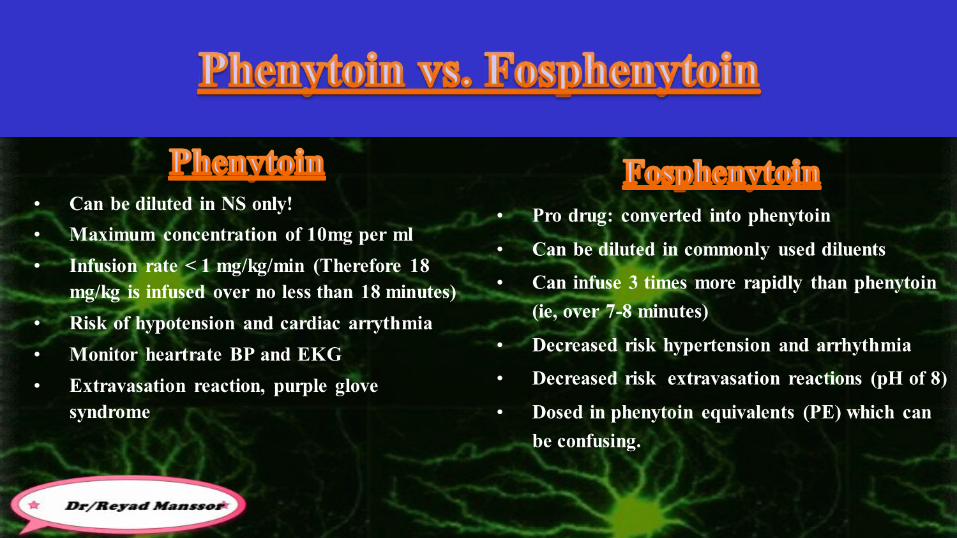
• a prodrug of Phenytoin– it has no anticonvulsant action itself, but is
rapidly converted to Phenytoin– Dosage: in “Phenytoin Equivalents” to
attempt to avoid confusion– can safely give at 3x rate of Phenytoin,
resulting in 2x amount of Phenytoin delivered
• Advantages over Phenytoin:– does not require solvent (Phenytoin is dissolved in
propylene glycol)• can give IM when no IV access• IV: - less potential for irritation - can give faster
- no risk of tissue necrosis if goes interstitial - does not precipitate in IV solutions
– lower risk of hypotension and dysrhythmias

• Negative considerations:– COST Approx 20x that of Phenytoin
Third Line Medication :if necessary
1. Valproic acid2. Levetiracetam
Valproic acid third-line treatment. loading dose of 20 to 40 mg/kg IV (diluted 1:1 with normal
saline or 5 percent dextrose in water) over 5 to 10 minutes may be repeated after 10 to 15 minutes This is followed by an IV infusion of 5 mg/kg per hour

continued seizures after 2 or 3 line antiepileptic drugs have failed Will usually need EEG monitoring at this point The goal is to stop electrographic seizure activity before reducing
the therapyUsually this implies achievement of complete flattening of the
EEG. a burst suppression pattern may be enough, and the periods of
flattening in such a case need to be >8-20 sec

hemodynamically stable1. pentobarbital : Short acting barbiturate with a rapid onset of actionoRequires
1. intubation2. mechanical ventilation3. vasopressor agents.
oDose initial bolus infusion of 5 to 15 mg/kg IV followed by a continuous infusion of 0.5 to 5.0 mg/kg per hour .
• Maintenance of pentobarbital anesthesia is continued for approximately 4 h by an infusion of 1–3 mg/kg/hr.
• The patient is then checked for the seizure activity – If clinical seizures and/or generalized discharges persist on EEG, the
procedure is repeated;– if not, the pentobarbital is tapered over 12–24 hours.
Significant side effects: 1. respiratory depression2. Hypotension3. myocardial depression4. reduced cardiac output5. pulmonary edema6. ileus
2. Midazolam

• Dose: 2-5 mg/kg IV• rapid onset: 30 - 60 sec• short duration: 20 - 30 min• S/E:
– CV depression, hypotension, arrhythmias – resp depression, apnea
• Thiopental - negative aspects:– accumulates in fatty tissues– an active metabolite - Pentobarbital – long recovery time after infusion– hemodynamic instability

hemodynamically unstableMidazolam may be better tolerated Dose
initial bolus infusion of 0.15 to 0.2 mg/kg IV followed by continuous infusion of 1 mcg/kg per min the infusion is increased by 1 mcg/kg per min every 15 minutes until
seizures are controlled or max dose(50 mcg/kg/minute)
3 mg × body wt (in kg), added to diluent to make 50 mL→ 1 mL/h delivers 1 μg/kg/min
hemodynamically unstablePropofol :Intravenous anesthetic
• Dose: 1-2 (3-5) mg/kg• Rate: 5-10 mg/min (1-15 mg/kg/hr)• Onset: 2-4 min• Half-life: 30-60 min• does not accumulate --> rapid recovery• Mechanism:
– stimulates GABA receptors– suppresses CNS metabolism
Risk of 1. Hypotension2. Apnea 3. Bradycardia4. Fatal Acidosis 5. Rhabdomyolysis of the skeletal and cardiac muscles6. Contraindicated in child on ketogenic diet
Advantages over Barbiturates– less hypotension– more rapid onset of action– rapid elimination
• “Pro-convulsant effect” - is now thought to be myoclonus, unlikely a significant problem

Inhalational anesthesia :- isoflorane is preferable because
halothane can increase intracranial pressure enflurane can induce seizures
Valproic acid Levetiracetam Keppra Consider IV pyridoxine if age <18 month
nelson2016• After the emergent therapy usually with a benzodiazepine,
the subsequent urgent therapy medication is usually fosphenytoin,
• The subsequent medication is ofen phenobarbital.• Ideally, emergent and urgent therapies should have been
received within less than 30 min so as to initiate the subsequent therapy soon,
nelson2016• Currently, the level of the evidence for refractory treatment
is strongest for midazolam and valproate, followed by propofol and pentobarbital/thiopental, followed by levetiracetam, phenytoin/fosphenytoin, lacosamide, topiramate, and phenobarbital.

nelson2016• Current evidence for the urgent therapy is strongest for
valproate, followed by phenytoin/fosphenytoin and midazolam continuous infusion, followed by phenobarbital and levetiracetam, the last of which are currently being increasingly used

Tim Assessment Supportive care Seizure treet 0 to 5 minutesprehospital
Obtain initial vital signs, including temperature
Lateral position, Open airwaySuction secretionsAdminister 100 percent O2
Benzodiazepine (first line):Lorazepam 0.05 to 0.1 mg/kg IV or IO, maximum 4 mg IV or IO access not achieved within 3 minutes:Rectal diazepam (Diastat® gel or injection solution given rectally) 0.5 mg/kg, maximum 20 mg OR Buccal midazolam 0.2 mg/kg, maximum 10 mg OR IM midazolam 0.1-0.2 mg/kg, maximum 10 mg
Identify airway obstruction and hypoxemia
Place continuous cardiorespiratory monitors and pulse oximetry
Identify impaired oxygenation or ventilation
Perform bag-valve-mask ventilation, as neededPrepare for RSI*
Obtain rapid bedside blood glucose and other studies
Establish IV or IO access
Evaluate for signs of sepsis/meningitis
Treat hypoglycemia (IV dextrose 0.25 to 0.5 gm/kg)
Evaluate for signs of head trauma
Treat fever (acetaminophen 15 mg/kg rectally)
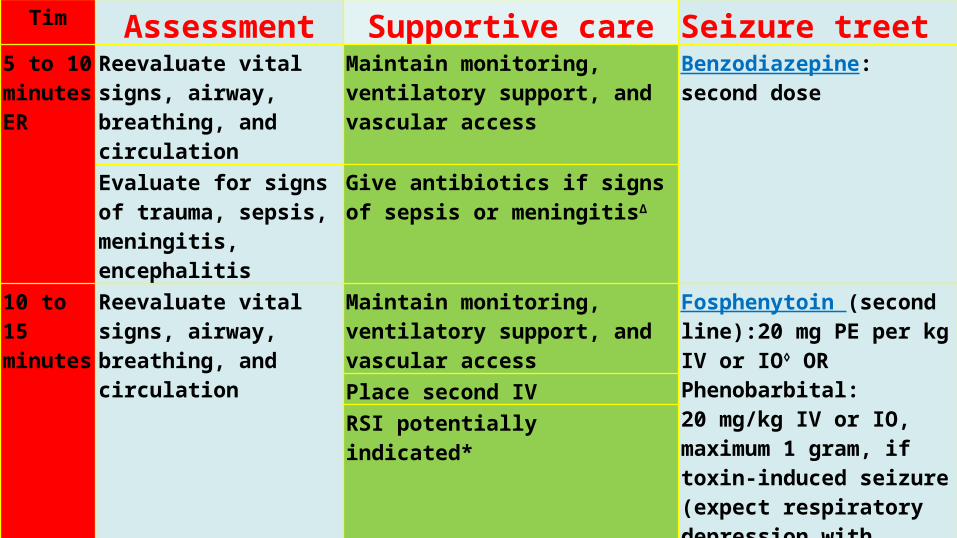
Tim Assessment Supportive care Seizure treet 5 to 10 minutesER
Reevaluate vital signs, airway, breathing, and circulation
Maintain monitoring, ventilatory support, and vascular access
Benzodiazepine: second dose
Evaluate for signs of trauma, sepsis, meningitis, encephalitis
Give antibiotics if signs of sepsis or meningitisΔ
10 to 15 minutes
Reevaluate vital signs, airway, breathing, and circulation
Maintain monitoring, ventilatory support, and vascular access
Fosphenytoin (second line):20 mg PE per kg IV or IO◊ ORPhenobarbital:20 mg/kg IV or IO, maximum 1 gram, if toxin-induced seizure (expect respiratory depression with apnea)§
Place second IVRSI potentially indicated*
Tim Assessment Supportive care
Seizure treet
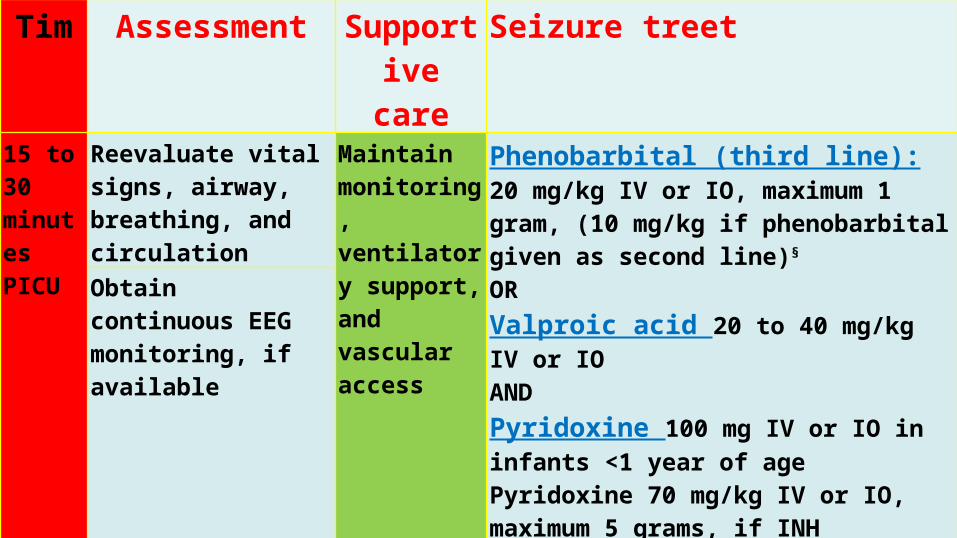
15 to 30 minutesPICU
Reevaluate vital signs, airway, breathing, and circulation
Maintain monitoring, ventilatory support, and vascular access
Phenobarbital (third line):20 mg/kg IV or IO, maximum 1 gram, (10 mg/kg if phenobarbital given as second line)§ ORValproic acid 20 to 40 mg/kg IV or IOANDPyridoxine 100 mg IV or IO in infants <1 year of agePyridoxine 70 mg/kg IV or IO, maximum 5 grams, if INH poisoning suspectedObtain pediatric neurology consultation (see Refractory status epilepticus algorithm)
Obtain continuous EEG monitoring, if available
Tim Assessment Supportive care
Seizure treet
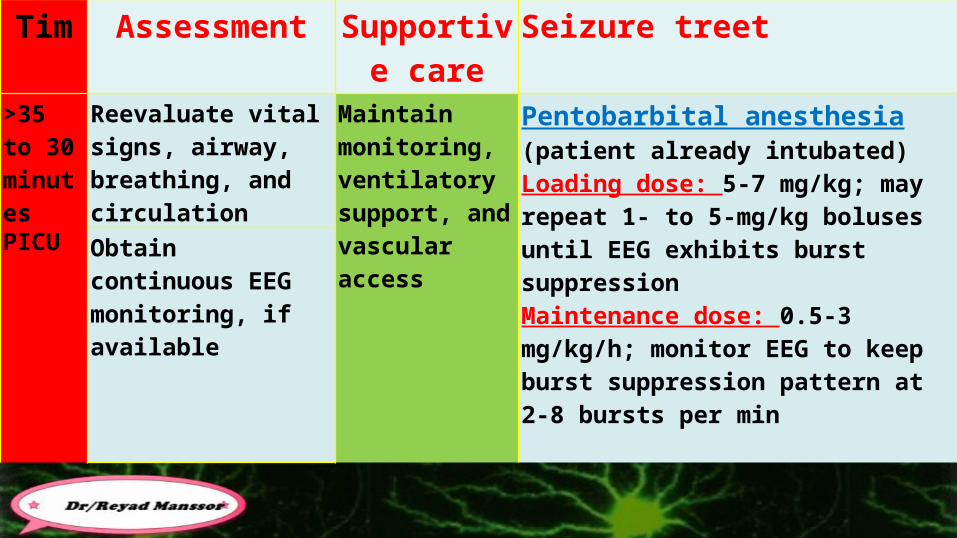
>35 to 30 minutesPICU
Reevaluate vital signs, airway, breathing, and circulation
Maintain monitoring, ventilatory support, and vascular access
Pentobarbital anesthesia (patient already intubated)Loading dose: 5-7 mg/kg; may repeat 1- to 5-mg/kg boluses until EEG exhibits burst suppressionMaintenance dose: 0.5-3 mg/kg/h; monitor EEG to keep burst suppression pattern at 2-8 bursts per min
Obtain continuous EEG monitoring, if available
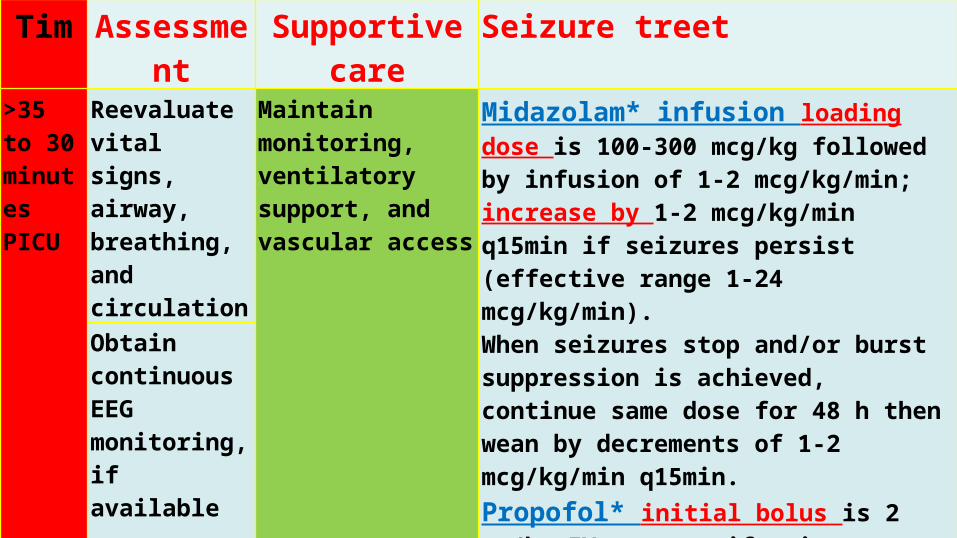
Tim Assessment Supportive care Seizure treet >35 to 30 minutesPICU
Reevaluate vital signs, airway, breathing, and circulation
Maintain monitoring, ventilatory support, and vascular access
Midazolam* infusion loading dose is 100-300 mcg/kg followed by infusion of 1-2 mcg/kg/min; increase by 1-2 mcg/kg/min q15min if seizures persist (effective range 1-24 mcg/kg/min). When seizures stop and/or burst suppression is achieved, continue same dose for 48 h then wean by decrements of 1-2 mcg/kg/min q15min.Propofol* initial bolus is 2 mg/kg IV; repeat if seizures continue and follow by infusion of 5-10 mg/kg/h, if necessary, guided by EEG monitoring. Taper dose 12 h after seizure activity stops.
Obtain continuous EEG monitoring, if available
At 0 min On presentation to hospital, initiate ABCs: A – support airway B – 100% oxygen, assess ventilation, SpO2 monitor C – cardiorespiratory monitor, check pulses, do IV access • History (SAMPLE) , Examination• Investigations • Suspect and treat raised ICP as needed, CT scan when warranted • Keep normothermic, acetaminophen/ibuprofen as appropriate
At 5 min IV access?

At 10 min
At 15 min Phenytoin 20 mg/kg IV/IO, max 1 g, over 20 minutes, in 0.9% NaCl (NS)
Phenobarbital 20 mg/kg IV/IO, max 1 g, over 5-10mins
At 25 min
• The order of Phenytoin and Phenobarbital may be interchanged • Phenytoin should be used in head trauma • Phenobarbital should be used 1st if patient already on phenytoin maintenance • Rapid Sequence Intubation if compromised airway at any point
• Ventilate to normal parameters • Sedation and muscle relaxants only if necessary to ventilate or protect airway
At 35 min
Early referral to PICU if any of following: • airway/ventilation/cardiovascular compromise• seizure refractory to 2nd line medications • seizure >30 minutes • initiating Midazolam or Thiopental infu
Midazolam 0.15 m g/k g IV bolus, then 2 mcg/kg/min by IV infusion

Midazolam increase by 2 mcg/kg/min q 5 min,0.15 mg/kg bolus as needed, Max50 mcg/kg/min
If stops x 48 hrs
Midazolam taper by 1 mcg/kg/min q 30 minAt 90 min
Thiopental 4 mg/kg IV bolus, then 1 mg/kg/hr IV infusion Discontinue Midazolam Infusion
Thiopental increase by 1 mg/kg/hr q 30 min, 2 mg/kg bolus as needed, max 6 mg/kg/hr
Thiopental taper by 25% q 12 hrs
If stops x 48 hrs
At 35 min

Initial assessmentNeurologic examinationGeneral evaluation with attention to
respiratory and circulatory status02 *-/- mechanical ventilation PRNIV catheters inserted (at least two)Blood work: electrolytes, glucose, toxicology, CBC, LFTS, Ca, Mg, ABG, Flngerstfck glucoseCardiac monitoring with pulse oximetryFrequent vital signsConsider glucose + thiamine IV
Initial therapyIn first IV:
Lorazepam 0.02-0.03 mg/kg IVAlternatives: Diazepam 0.1 mg/kg IVMidazolam 0.05 mg/kg IVWait l minute for response then additionalLorazepam PRN: max dose 0.1 mg/kg;max rate 2 mg/min
in second IV:Phenytoin 20 mg/kg at 25-50 mg/min* ORFosphenytoin 20 mg/kg PE at 50-125 mg PE/min*
Correct metabolic abnormalities if presentSecond-line therapy Phenytoin or Fosphenytoin dose: 10 mg/kg PEintubate, mechanical ventilation ,Continuous blood pressure, cardiac monitoring
Risk for prolonged ventilation Propofol infusion l to 2 mg/kg per hour, titrated to seizure free state. Rates may be as high as 10 to 12 mg/kg per hour After seizures controlled, maintain for 24 hours, then taper at 5 percent per hour If seizures persist after 45 to 60 minutes, then pentobarbital infusion Maintain therapeutic levels of phenytoin and/or phénobarbital
• Patients who are at high risk for prolonged mechanical ventilation (eg, those with severe COPD, severe debilitation, or cancer) should be treated with propofol in an attempt to minimize the duration of sedation
• The term "malignant" status epilepticus has been introduced to refer to status epilepticus that either fails to respond to the therapies discussed above or recurs quickly on tapering these medications
• It has been reported that as many as 20 percent of patients with refractory status epilepticus evolve into malignant status epilepticus, a transition that is associated with a very poor prognosis

• SE can be 1. fatal ( mortality)2. Morbidity associated with long-term morbidity,
including:seizure recurrence neurologic problems.
PrognosisOUTCOME
Depend onAge, etiology, and duration correlate directly
with mortalityThe highest mortality is seen in the elderly;
fortunately, children have a far lower mortality rate than do adults
Prognosis

OUTCOMEMortality :can result from
1. Underlying condition 2. Respiratory3. Cardiovascular4. metabolic complications of SE
mortality rates of SE in children varies between 3 and 9 percent The underlying etiology is the main predictor of mortality
mortality rates of SE in adult 20 percent

OUTCOME Morbidity Neurologic sequelae of SE include;
1. focal motor deficits2. mental retardation3. behavioral disorders4. chronic epilepsy.
morbidity other than epilepsy occurred in 15 percent of patients Neurologic sequelae are usually caused by the underlying condition rather than the seizures
rates of neurologic sequelae are increased in younger patients with a longer duration of seizures, Patients with cryptogenic SE and those with febrile SE do not have an increased
incidence of recurrent seizures or other neurologic sequelae over baseline
OUTCOME-Morbidity Recurrent seizures
The risk for having future seizures of any type : Is high when SE is the child's first seizure, up to 50 percent in two reports Recurrent SE also was more likely to occur in children who presented with
SE (21 versus 1 percent in those with a brief initial seizure. Other risk factors for recurrence include :
1. Remote symptomatic etiology2. Abnormal electroencephalogram3. Seizure during sleep4. History of prior febrile seizures5. Focal post-ictal deficits, including Todd's paresis
OUTCOMENeurologic sequelae more with :
prolonged inadequately treated

OUTCOME Refractory status epilepticus high mortality and morbidity. mortality ; 33% to 52% More in :
Younger patients (<5 years) multifocal abnormalities on EEG generalized abnormalities on EEG
Morbidity In survivors, recurrent seizures were common (31 to 97 percent) new neurologic deficits (71 to 100 percent).

Treatmentposttreatment subtle SE isidentical to that of refractory SEcentral theme to improving outcome is early
recognition intensive EEG monitoring.

Neonatal Status EpilepticusTreatment• Phenobarbital
– Usually used first– Prolonged half life—100 hours after day 5-7; therefore watch for toxicity– 20 mg/kg IV (up to 40 mg); repeat 10/kg every 15-30 minutes times two
• Phenytoin/Fosphenytoin– 20 mg/kg (over 30-45 minutes)– Half-life 100 hours– Nonlinear kinetics; redistribution, variable rate hepatic metabolism require
individuallization of maintenance dosing• Benzodiazepine
– Diazepam• 0.25mg/kg IV bolus or 0.5 mg/kg PR
– Lorazepam• 0.05 mg/kg IV over2-5 minutes
• Midazolam infusion

References1. UpToDate 21.62. Text book of pediatric_epilepsy-diagnosis_and_therapy_3rd
3. CLINICAL PEDIATRIC NEUROLOGY: A SIGNS AND SYMPTOMS APPROACH ; 20094. Pediatric Neurology ;20105. Neurocrit Care society6. EPILEPSY: GLOBAL ISSUES FOR THE PRACTICING NEUROLOGIST7. Atlas of Pediatric EEG8. eMedicine Medical 9. A Clinical Guide to Epileptic Syndromes and their Treatment10. Current Management in Child Neurology, Third Edition11. Nelson_Textbook_of_Pediatrics__19th_Edition12. Rudolph's Pediatrics13. epilepsyfoundation.org14. Nelson_Textbook_of_Pediatrics__20th_Edition15. Child Neurology 6th edition : by John H. Menkes (Editor), Harvey B. Sarnat, Samat By
Lippincott, Williams & Wilkins