management of psychotropic drug-induced dress syndrome: a...
TRANSCRIPT

REVIEW
Management of Psychotropic DrugeInducedDRESS Syndrome: A Systematic Review
Tanner J. Bommersbach, BA; Maria I. Lapid, MD; Jonathan G. Leung, PharmD, RPh;Julie L. Cunningham, PharmD, RPh; Teresa A. Rummans, MD; and Simon Kung, MDAbstract
Drug rash with eosinophilia and systemic symptoms (DRESS) is a severe cutaneous eruption that has beenlinked to several common drugs and drug categories, including antiepileptics, allopurinol, sulfonamides,and various antibiotics; however, because of a number of recent case reports linking psychotropic med-ications to this condition, DRESS is increasingly recognized among psychiatrists. We systematicallyreviewed all psychotropic drugs linked to DRESS syndrome, and this article summarizes the clinicalmanagement relevant to psychiatric professionals. A comprehensive search was performed using OvidMEDLINE, Ovid EMBASE, Ovid Cochrane Database of Systematic Reviews, Web of Science, Scopus, andLitt’s Drug Eruption and Reaction Database for articles published in English during the past 20 years(1996-2015) using the search terms (1) psychotropic drugs OR serotonin uptake inhibitors AND DRESS or (2)psychotropic drugs AND drug reaction (or rash) eosinophilia systemic syndrome, and all article abstracts werescreened for inclusion and exclusion criteria by 3 reviewers. Two independent reviewers examined the fulltext of 163 articles, of which 96 (25 original articles, 12 review articles, 55 case reports, and 4 letters to theeditor) were included in the systematic review. We identified 1072 cases of psychotropic drugeinducedDRESS, with carbamazepine, lamotrigine, phenytoin, valproate, and phenobarbital being the mostimplicated drugs. Based on our review of the literature, we outline management principles that includeprompt withdrawal of the causative drug, hospitalization, corticosteroid therapy, and novel treatments,including intravenous immunoglobulin, cyclophosphamide, and cyclosporine, for corticosteroid-resistantDRESS. Finally, we outline strategies for treating comorbid psychiatric illness after a DRESS reaction to thepsychotropic medication.
ª 2016 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2016;nn(n):1-15
From Mayo MedicalSchool, Mayo ClinicCollege of Medicine(T.J.B.), Department ofPsychiatry and Psychology(M.I.L., T.A.R., S.K.), andPharmacy Services (J.G.L.,J.L.C.), Mayo Clinic,Rochester, MN.
D rug rash with eosinophilia and sys-temic symptoms (DRESS) is a severecutaneous drug eruption that is
characterized by fever, rash, lymphadenopa-thy, internal organ involvement, and hemato-logic abnormalities. The most commonlyaffected organs are the liver, lungs, and kid-neys, and characteristic blood abnormalitiesinclude lymphocytopenia, atypical lympho-cytes, and eosinophilia.1 DRESS syndromecan be difficult to diagnose because of itsnonspecific presentation. Moreover, it oftenis asymptomatic until a considerable amountof time has passed after the initial drug expo-sure.2 The pathogenesis of DRESS is unclear,although several models have been proposed,and it may have a genetic origin.2 Viral reacti-vation may also have a significant role, withseveral studies reporting that reactivation ofhuman herpesvirus 6 and 7, Epstein-Barr
Mayo Clin Proc. n XXX 2016;nn(n):1-15 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org n ª 2016 Mayo Foundation for M
virus, and cytomegalovirus can occur at theonset of DRESS.3 Several common drugs anddrug categories have been associated withthis condition, including antiepileptics, allo-purinol, sulfonamides, and various antibiotics;however, recent case reports have linked psy-chotropic medications to this condition, andDRESS syndrome is becoming increasinglyrecognized among psychiatrists. Although theincidence rate of DRESS syndrome is un-known, prospective studies have estimated itto be about 1 per 1000 to 10,000 individualsexposed to commonly associated drugs. Themortality rate is estimated to be around 10%to 20%.4 Recently implicated psychotropicdrugs include benzodiazepines, bupropion,mirtazapine, and amitriptyline.5-9 Most studieshave focused on aromatic antiepileptics,including phenytoin (PHT), carbamazepine(CBZ), and phenobarbital (PB), but little is
/j.mayocp.2016.03.006edical Education and Research
1

ARTICLE HIGHLIGHTS
n Drug rash with eosinophilia and systemic symptoms (DRESS) isa severe cutaneous eruption that typically presents within 1 or2 months of drug initiation. Common clinical features includemaculopapular rash, elevated liver enzyme levels, lymphade-nopathy, facial edema, and eosinophilia.
n Our systematic review included 1072 cases of psychotropicdrugeinduced DRESS, with carbamazepine, lamotrigine,phenytoin, valproate, and phenobarbital being the most impli-cated drugs.
n The cornerstones of DRESS management include promptwithdrawal of the implicated drug and administration of corti-costeroids. For cases of corticosteroid-resistant DRESS, intra-venous immunoglobulin, cyclophosphamide, cyclosporine, andimmunosuppressants have had efficacy.
n Management of comorbid psychiatric illness includes strictavoidance of the implicated drug and other drugs in the sameclass (eg, aromatic, nonaromatic) and identification of areplacement drug (eg, valproate for carbamazepine-inducedDRESS).
MAYO CLINIC PROCEEDINGS
2
known about psychotropic drugeinducedDRESS syndrome. Moreover, consensus hasnot been established on the management andtreatment of DRESS syndrome. The only man-agement step that appears to be universallyaccepted is cessation of the causative agent.10
The use of corticosteroids for DRESS iscontroversial because of the lack of random-ized controlled trials assessing their efficacy,but they are nevertheless a widely acceptedtreatment.10
Recently, other promising treatments havebeen applied to DRESS, including intravenousimmunoglobulin (IVIG), plasma exchange,cyclosporine, and cyclophosphamide.11
Although these treatment options have beenexplored in individual case reports, little inthe published literature guides psychiatricmanagement of psychotropic drugeinducedDRESS syndrome. The onset of DRESS syn-drome can create a difficult clinical situation,even after the acute symptoms have resolved,because cessation of the causative agent maylead to recurrence and worsening of problem-atic psychiatric symptoms. Evidence-basedrecommendations are needed to guide clinical
Mayo Clin Proc. n XXX 20
decision making for mental health profes-sionals managing patients with DRESS syn-drome. This article provides a systematicreview of all psychotropic drugs linked toDRESS syndrome and summarizes the clinicalmanagement relevant to psychiatric profes-sionals in a multidisciplinary context. To ourknowledge, this is the first systematic reviewof psychotropic drugeinduced DRESS syn-drome and its clinical management.
METHODS
Literature SearchAn experienced medical librarian designed asearch strategy in Ovid MEDLINE and trans-lated the strategy for Ovid EMBASE, OvidCochrane Database of Systematic Reviews,Web of Science, and Scopus. Litt’s Drug Erup-tion and Reaction Database was also searched.The search was limited to articles published inEnglish during the past 20 years (1996-2015;the first report of DRESS was published in1996). The strategy included the US NationalLibrary of Medicine’s medical subject headingsand keywords, including (1) psychotropic drugsOR serotonin uptake inhibitors AND DRESS or(2) psychotropic drugs AND drug reaction (orrash) eosinophilia systemic syndrome. Fromthis search, 394 articles were identified.
ScreeningWe aimed to include articles on DRESS syn-drome involving any psychiatric or psychotro-pic medication such as antipsychotics orneuroleptics, mood stabilizers, antiepileptics,antidepressants, and antianxiety medications.We included pediatric and adult studies. Weexcluded articles that focused primarily onclinical and pathologic features, genotyping,patch testing, or other diagnostics that werenot relevant to psychiatric medications. Wealso excluded articles that focused primarilyon antiepileptic or anticonvulsant drugs exclu-sively for managing seizure disorder (ie,without psychiatric applications).
Article abstracts were screened for inclu-sion and exclusion criteria by 3 authors(S.K., J.L.C., J.G.L.), and disagreements wereresolved by consensus. At this stage, 231 arti-cles were excluded. The full text of the 163remaining articles was reviewed independentlyby 2 authors (M.I.L., T.J.B.). After applying the
16;nn(n):1-15 n http://dx.doi.org/10.1016/j.mayocp.2016.03.006www.mayoclinicproceedings.org

394 Records identifiedthrough database searching
0 Additional records identifiedthrough other sources
394 Records after duplicates removed
Iden
tific
atio
nSc
reen
ing
Elig
ibili
tyIn
clud
ed
394 Records screened
163 Full text of articles assessed for eligibility
96 Studies included in qualitative synthesis
231 Records excluded
• Studies did not include psychotropic medications• Studies did not highlight management of DRESS
• Studies did not include psychotropic medications• Studies did not highlight management of DRESS
67 Articles excluded
FIGURE. Flow diagram of references selected for study inclusion based on the PRISMA (PreferredReporting Items for Systematic Reviews and Meta-Analyses) method.
PSYCHOTROPIC DRUGeINDUCED DRESS
inclusion and exclusion criteria, 67 articleswere subsequently eliminated (Figure).
RESULTSWe identified 1072 cases of psychotropicdrugeinduced DRESS, with CBZ, lamotrigine(LTG), PHT, valproate (VPA), and PB beingthe most implicated drugs.
Original ArticlesWe identified 25 original articles that described997 cases of DRESS (Table 1).10,12-35 Theimplicated psychotropic drugs were antiepilep-tics or mood stabilizers. Carbamazepine andPHT were most often associated with DRESS,as were LTG, topiramate, PB, oxcarbazepine,and VPA. No articles specifically mentionedantidepressants, anxiolytics, antipsychotics,sedatives, or hypnotics. The described time topresentation, when reported, was similaramong studies (mean [SD], 24.3 [2.7] days).Management often included corticosteroidsand removal of the suspected agent. One reviewarticle cited a mortality rate as high as 20%.14
Mayo Clin Proc. n XXX 2016;nn(n):1-15 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
Review ArticlesWe identified 12 review articles on DRESS withpsychotropic agents (Table 2).11,36-46 The focusof the articles varied, but they generallyaddressed management recommendations andrisk factors. Treatment recommendations consis-tently included discontinuation of the causativeagent, hospitalization for initial stabilizationand monitoring, and use of corticosteroids,although evidence supporting corticosteroidtreatment is limited and results have been incon-sistent.41,47 Intravenous corticosteroid adminis-tration is recommended when organ damage isevident,1,36 and other common treatment alter-natives included IVIG, cyclosporine, and plasmaexchange.34,37,42,43
The causative agent identified most co-mmonly in the review articles was CBZ.40,41
The genomic allele HLA-A*3101 was identifiedas a risk factor for DRESS when CBZ is used.39
Another risk factor for DRESS development wasa fever preceding cutaneous eruptions.39 Prog-nosis was poor for elderly patients, whereas amore rapid and complete recovery generally
/j.mayocp.2016.03.006 3

TABLE 1. Original Articles on DRESS Associated With Psychotropic Drugsa
Reference, year No. Patient type Medications Results Comment
Time topresentation (d),
mean Presenting symptoms
Sultan et al,12 2015 17 Adults PHT, PB, CBZ, OCBZ, LTG,ALL, LEF, DDS, VAN, NTF
Retrospective studyInjectable dexamethasone as treatmentMajority (76.5%) recovered completely
Systemic corticosteroids usually first-line treatment for DRESS; however,use is controversial because of lackof randomized controlled trials
22.35�5.83 Many differentpresentations
Um et al,13 2010 38 Adults LTG, CBZ, PB, PHT, IBU, ALL,CTX
Retrospective study36 DRESS patients (94.8%) treated
with corticosteroids (n¼16) orantihistamines (n¼22) recoveredcompletely
More information needed to evaluatethe indications for systemiccorticosteroids
25.2 Many differentpresentations
Botelho et al,14
201210 Adults ALL, PHT, CBZ Retrospective study
Systemic corticosteroids as treatment8 Recovered; 2 died of septic shock
None NA Many differentpresentations
Chiou et al,15 2008 29 Adults ALL, PHT, CBZ, INM, VAN,DDS
Retrospective studyTreatment with systemic
corticosteroid (n¼22) or oralantihistamines plus supportive care(n¼7)
High absolute eosinophil counts andmultiple underlying diseases werepoor prognostic factors
23.49 Many differentpresentations
Kardaun et al,16
2013117 Adults CBZ, PHT, LTG, OCBZ, PB,
ALL, VAN, AMX,piperacillin-tazobactam
Early recognition and promptwithdrawal of the drug were themost important steps to avoiddisease progression
None 22 Eosinophilia (95%)Visceral involvement
(91%)High fever (90%)
Karimzadeh andBakrani,17 2013
4 Children PB Retrospective studyOf 70 pediatric patients with AED
reactions, 4 had DRESS
Higher rates of AED reactions witharomatic AEDs than nonaromaticAEDs
NA NA
Sasidharanpillaiet al,18 2014
28 Adults andchildren
PHT, PB, DDS, CBZ, LTG,VPA
Retrospective studyPrednisolone (1 mg/kg) or
dexamethasone was given topatients with >10-fold elevation intransaminase levels,hyperbilirubinemia, or multiorganinvolvement
Full recovery in all patients except 1(nonadherent)
Flare-ups during prednisolonewithdrawal managed successfully byincreasing dose followed by slowtaper
27.2 Many differentpresentations
Peyrière et al,19
2006216 Adults and
childrenCBZ, PHT, LTG, ALL, MNC,NVP, ABC
Retrospective studyClinical presentations of DRESS were
variable
A large prospective study is needed tobetter define DRESS and evaluateprognostic data
NA Fever, cutaneouseruption, hepaticabnormalities,eosinophilia
Continued on next page
MAYO
CLIN
ICPRO
CEED
INGS
4Mayo
ClinProc.
nXXX
2016;nn(n):1-15
nhttp://dx.doi.org/10.1016/j.m
ayocp.2016.03.006www.m
ayoclinicproceedings.org

TABLE 1. Continued
Reference, year No. Patient type Medications Results Comment
Time topresentation (d),
mean Presenting symptoms
Phillips et al,20
2011NA NA NA NA HLA associations might be able to
provide screening for specificdrug-induced DRESS symptoms
NA NA
Santiago et al,21
201056 Adults and
childrenNA Positive patch tests were seen in 18
patients (32.1%), of which 17 wereAEDs
Patch testing was a safe and usefulmethod to confirm the culpritdrug in DRESS induced by AEDs
NA NA
Walsh et al,22 2013 38 Adults andchildren
NA Retrospective study Cutaneous dermatologic signs ofDRESS may have a potentialprognostic value regarding theseverity of visceral involvement
NA NA
Yang et al,23 2013 48 Adults andchildren
NA Retrospective studyTreatments included systemic
corticosteroids alone (n¼40) andboth corticosteroids and IVIG(n¼1); 7 were treatedconservatively
Leukocytosis at presentation was aprognostic factor for prolongedhospitalization
21.5 NA
Heinzerling et al,24
2012107 Adults and
childrenNA Retrospective study
Of 141 cases of suspected cutaneousdrug reactions, 107 were due to adrug (34 [24%] were attributed toother causes)
Clinical assessment overestimates therole of drug allergies in cutaneousreactions
NA NA
Pereira de Silvaet al,25 2011
8b NA CBZ, LTG, PHT Retrospective studyTreatments were diphenhydramine
(n¼4), loratadine (n¼1), prednisone(dose, 30-60 mg/d; n¼6), and bothprednisone and antihistamines(n¼3)
None 28.5 Many differentpresentations
Volcheck,10 2004 NA NA NA Treatment should be supportive(volume replacement, nutritionalsupport, antibiotics, skin care), butcorticosteroids remain controversial
Although case reports have describedefficacy of corticosteroids,randomized controlled trials areneeded to confirm their benefit
NA NA
Lee et al,26 2010 18 Adults andchildren
PHT, ALL Retrospective studyDRESS constituted 18/97 (18.6%) of
the reactions
None NA NA
Continued on next page
PSYCHOTRO
PICDRU
GeINDUCED
DRESS
Mayo
ClinProc.
nXXX
2016;nn(n):1-15
nhttp://dx.doi.org/10.1016/j.m
ayocp.2016.03.006www.m
ayoclinicproceedings.org5

TABLE 1. Continued
Reference, year No. Patient type Medications Results Comment
Time topresentation (d),
mean Presenting symptoms
Boccara et al,27
2006NA NA NA Retrospective study
Hypogammaglobulinemia wassignificantly associated with DRESS
None NA NA
Sasidharanpillaiet al,28 2015
7 Adults VPA Retrospective studyDescribed incidence of adverse drug
reactions on a dermatology wardduring an 11-month period
Rebound or flare-up reactions werenoted for several patients withDRESS during the corticosteroidtaper, which required reinitiation ofhigher doses of corticosteroids
NA DRESS tended topresent with lessmucocutaneousinvolvement than SJSor TEN
Mokhtari et al,29
201418 Adults and
childrenCBZ, VPA, VAN Retrospective study
DRESS reactions accounted for 6.4%of all adverse cutaneous drugreactions in an 8-year period
DRESS should be in the differentialdiagnosis for any adverse drugreaction
NA NA
Grando et al,30
201426 Adults and
childrenNA Retrospective study
DRESS was the most common severecutaneous drug reaction in thissample
Withdrawal of the causative drug is themost important step in management
Corticosteroid use is controversial
NA NA
Wei et al,31 2011 91 Adults andchildren
NA Retrospective studyTachycardia, leukocytosis, tachypnea,
coagulopathy, gastrointestinalbleeding, and SIRS were poorprognostic indicators of DRESS
Early recognition and intervention arekey in avoiding mortality in DRESS
NA NA
Yang et al,32 2011 39 Adults andchildren
CBZ, LTG, OCBZ, PHT Retrospective studyDRESS was more likely to cause organ
involvement, especially liverdysfunction, than SJS or TEN
Corticosteroids (and sometimes IVIG)are frequently used to treat adversecutaneous drug reactions, but thispractice is controversial
NA NA
Continued on next page
MAYO
CLIN
ICPRO
CEED
INGS
6Mayo
ClinProc.
nXXX
2016;nn(n):1-15
nhttp://dx.doi.org/10.1016/j.m
ayocp.2016.03.006www.m
ayoclinicproceedings.org

T LE 1. Continued
ference, year No. Patient type Medications Results Comment
Time topresentation (d),
mean Presenting symptoms
M z andrenner,33 2007
8 Adults CBZ, PHT Retrospective studyWomen tended to present at a
younger age and with a shorter timeto onset of symptoms
None NA NA
C n et al,34 2010 60 Adults andchildren
ALL was the most commonculprit drug (19/60 cases)
Retrospective study75% of patients were treated with
systemic corticosteroids (with IVIGfor 2 patients, 1 of whom died)
10 Patients received only supportivecare
6 Patients (10%) diedCorticosteroid use did not affect
mortality rates
None NA NA
A ncini et al,35
01527 Adults and
childrenPHT, CBZ Retrospective study
All patients were treated withcorticosteroids
Mortality rate was 4%
An association may exist between thepresence of atypical lymphocytesand elevated ALT
NA Maculopapularexanthema (85.1%),fever (96.2%),hepatitis (85.1%)
a ¼ abacavir; AED ¼ antiepileptic drug; ALL ¼ allopurinol; ALT ¼ alanine aminotransferase; AMX ¼ amoxicillin; CBZ ¼ carbamazepine; CTX ¼ ceftriaxone; DDS ¼ dapsone; DRESS ¼ drug rash with eosinophilia andemic symptoms; IBU ¼ ibuprofen; INM ¼ indomethacin; IVIG ¼ intravenous immunoglobulin; LEF ¼ leflunomide; LTG ¼ lamotrigine; MNC ¼ minocycline; NA ¼ not available; NTF ¼ nitrofurantoin; NVP ¼ nevirapine;BZ ¼ oxcarbazepine; PB ¼ phenobarbital; PHT ¼ phenytoin; SIRS ¼ systemic inflammatory response syndrome; SJS ¼ Stevens-Johnson syndrome; TEN ¼ toxic epidermal necrolysis; VAN ¼ vancomycin; VPA ¼ valproate.
b discrepancy between the Number and Results is due to some patients receiving more than one treatment.
PSYCHOTRO
PICDRU
GeINDUCED
DRESS
Mayo
ClinProc.
nXXX
2016;nn(n):1-15
nhttp://dx.doi.org/10.1016/j.m
ayocp.2016.03.006www.m
ayoclinicproceedings.org7
AB
Re
aoB
he
va2
ABCsystOCThe

MAYO CLINIC PROCEEDINGS
8
was seen in children.42 Counseling first-degreerelatives about their increased risk,48 avoidanceof new medication during management ofDRESS,36 and use of alternative medicationswith lower risk48 were additional notablerecommendations.
Case ReportsWe identified 55 case reports of DRESS thatdescribed 75 patients (56 adults, 19 childrenand adolescents). The reports are summarizedin the Supplemental Table (available online athttp://www.mayoclinicproceedings.org).4-9,49-97
Implicated drugs included CBZ (n¼33), LTG(n¼17), PHT (n¼12), VPA (n¼7), PB (n¼4),and oxcarbazepine (n¼2). Medications un-likely to provoke DRESS included armodafinil,bupropion, penicillin, clonazepam, ibuprofen,and ziprasidone (ZIP), with some of thesemedications given in combination with anti-convulsants. The time to presentation of symp-toms ranged from 7 to 120 days (plus anoutlier of 2 years); the mean was 35.6 days,and the median was 21 days. Myocarditis wasa frequent symptom in late presentations ofDRESS. Among the 252 symptoms noted, feverwas most common (n¼38), followed by macu-lopapular rash (n¼32), elevated liver enzymelevels (n¼32), lymphadenopathy (n¼22), facialedema (n¼16), and eosinophilia (n¼16).Discontinuation of medication and cortico-steroid use were the most common treatmentapproaches.
Letters to the EditorWe identified only 4 letters to the editordescribing DRESS: implicated medications werequetiapine (n¼1), VPA (n¼1), and CBZ (n¼2;one case was in combination with cilostazol).
DISCUSSIONThis systematic review underscores the vastamount of literature implicating psychotropicmedication in the development of DRESS syn-drome. Among psychotropic medications, an-ticonvulsants appeared to be most commonlyassociated with DRESS. Our review identified1072 cases of psychotropic drugeinducedDRESS, with CBZ, LTG, PHT, VPA, and PBbeing the most implicated drugs. However,we found very few reports linking antidepres-sants, anxiolytics, antipsychotics, and seda-tives or hypnotics to DRESS syndrome. As
Mayo Clin Proc. n XXX 20
DRESS gains greater recognition, we predictan increase in reports involving other psycho-tropic agents. A summary of evaluation andmanagement recommendations for psychotro-pic drugeinduced DRESS syndrome is pre-sented in Table 3.
Clinicians should continue to report newcases to regulatory bodies and submit casesfor publication because these activities ulti-mately increase patient safety. Recently, theUS Food and Drug Administration (FDA)reexamined ZIP, a second-generation antipsy-chotic medication, because the FDA AdverseEvent Reporting System had received 6 casesof ZIP-associated DRESS. The onset of DRESSranged from 11 days to 1 month after initi-ating ZIP. Three cases were rechallengedwith ZIP, and DRESS recurred in a shorterperiod compared with the initial presentationof DRESS. No deaths were reported, butseveral cases had serious outcomes necessi-tating hospitalization. The prescribing infor-mation for ZIP now highlights a risk ofDRESS.
Even with the extensive literature on psy-chotropic drugeinduced DRESS syndromeand its clinical features, management guide-lines and recommendations vary and arepoorly established. Because mortality ratesfor DRESS of up to 20% have been reported,14
it is important to establish evidence-baseddiagnostic and treatment principles, includingthe management of comorbid psychiatricillness during and after the development ofDRESS syndrome.
Based on our review of the literature,prompt diagnosis of DRESS is highly depen-dent on clinical suspicion because its presenta-tion varies and often is nonspecific. In the casereports, the time from drug initiation to pre-sentation of symptoms ranged from 7 to 120days (mean, 35.6 days), and common clinicalfeatures included maculopapular rash,elevated liver enzyme levels, lymphadenopa-thy, facial edema, and eosinophilia. The differ-ential diagnosis of suspected DRESS shouldinclude Stevens-Johnson syndrome (SJS),toxic epidermal necrolysis, acute generalizedexanthematous pustulosis, hypereosinophilicsyndromes, angioimmunoblastic T-cell lym-phoma, Sézary syndrome, and cutaneouslupus erythematosus.99 Clinical suspicion ofDRESS should be augmented by a thorough
16;nn(n):1-15 n http://dx.doi.org/10.1016/j.mayocp.2016.03.006www.mayoclinicproceedings.org

TABLE 2. Review Articles on DRESS Associated With Psychotropic Drugs
Reference, year Clinical recommendations
Chan et al,11 2012 Early identification and prompt withdrawal of the causative agent are key. Patients are hospitalized for careful monitoring.Exclusion of rare symptoms such as myositis, myocarditis, pneumonitis, and pancreatitis is important in DRESS. Moderate- tohigh-dose corticosteroids should be started in patients with internal organ involvement; most commonly, prednisolone(1 mg/kg/d) is initiated and then tapered over 6-8 wk to prevent relapse of organ involvement. Other treatments withreported success have included IV methylprednisolone, IVIG, and plasmapheresis. In corticosteroid-resistant cases,cyclosporine A and cyclophosphamide have been effective
Choudhary et al,36
2013It has been reported that the earlier the drug withdrawal, the better the prognosis. Treatment is largely symptomatic.Corticosteroids are often used, but the evidence regarding their effectiveness is minimal
Jeung et al,37 2010 Corticosteroids are the mainstay of treatment for DRESS, and favorable results have been reported, although the dosage varieswidely across case reports. Primary and secondary prevention have key roles in the management of DRESS
Roujeau et al,38 2014 The authors outline the treatment of DRESS, and prompt withdrawal of the causative drug is the first step. They suggestavoiding introducing new medications during the course of DRESS because of the risk of DRESS flare-up associated withnew medications. Hospitalization is suggested for severe cutaneous manifestations. Fluid and electrolyte replacement andnutritional support are required for those with exfoliative dermatitis, and a warm and humid environment with gentle skincare (eg, warm baths or wet dressings) are suggested. An expert consensus group in France proposed that patients can betreated symptomatically if they have no clinical, laboratory, or imaging evidence of renal or pulmonary involvement and onlymodest elevations of liver enzymes. Relief of pruritus and skin inflammation is obtained with high-potency topicalcorticosteroids, applied 1-3 times per day for 1-2 wk; this treatment should be sufficient for complete recovery in patientswithout severe organ involvement. For patients with organ involvement, use of systemic corticosteroids is very important.Although the optimal dose and duration of corticosteroid therapy is undetermined, an initial prednisone dose of 1-2 mg/kg/dor equivalent is common
Walsh and Creamer,39
2011DRESS can be treated with moderate- or high-dose oral corticosteroids; however, response may be suboptimal. Cyclosporineand other immunosuppressants are sometimes required in corticosteroid-resistant cases. Variation in outcomes of DRESShighlights the need for a clinical tool to define disease severity. Prognostic markers are needed to aid stratification of patientcohorts benefitting from early intervention with potent treatment
Verma et al,40 2013 Oral prednisolone (1-2 mg/kg) is the treatment of choice and should be continued for 2-3 mo. VPA, benzodiazepine, andgabapentin are ideal replacements for drugs causing anticonvulsant hypersensitivity syndrome. Hematologic, hepatic, andrenal parameters must be monitored. Supportive care with fluid and electrolyte balance is important. Topical corticosteroidsand antihistamines are helpful for cutaneous manifestations. Patients should avoid the same or related drugs. First-degreerelatives must be counseled about their increased risk. A lymphocyte toxicity assay can be performed for relatives to confirmincreased susceptibility
Husain et al,41 2013 HLA-A*3101 is associated with an increased risk of DRESS with exposure to CBZ. HLA-DR3 and HLA-DQ2 alleles also areassociated with CBZ-induced DRESS
Kano and Shiohara,42
2009This article reviews the drugs associated with DRESS and DHS and reviews the variable clinical presentations. Drugs includeCBZ, PHT, PB, LTG, ALL, MNC, and DDS
Cacoub et al,43 2011 This article analyzed 172 cases of DRESS in a 12-year period; cases were identified by searching PubMed. All patients werehospitalized, and the causative agent was stopped. Main treatment was corticosteroids. IVIG was combined withcorticosteroids in 10 cases, and the mean (SD) recovery time was 6.4 (9.4) wk. Death occurred in 9 cases (cardiac or hepaticcauses). The patients with fatal DRESS generally were older than those who recovered from DRESS. A total of 44 uniquecausative medications were identified, with CBZ being the most common
Criado et al,44 2012 Prognosis of DRESS is generally worse in the elderly, whereas recovery is often faster and complete in children. Treatment isusually systemic corticosteroids (prednisone or equivalent dose �1-1.5 mg/kg/d). Dose should be tapered slowly over 6-8wk. Abrupt worsening of symptoms is observed when the withdrawal is accidental or with a rapid reduction in dose. Theyrecommend hospitalizing all patients, even when the initial presentation is mild. If symptoms worsen, other options includepulsed methylprednisolone (30 mg/kg IV for 3 d), IVIG, plasmapheresis, or a combination of these treatments. Specialattention should be paid to possible reactivation of cytomegalovirus
Fernando,45 2014 Treatment with oral corticosteroids (1 mg/kg/d) tapered over 6-8 wk to prevent symptom relapse is recommended. Ifsymptoms worsen, IVIG, plasma exchange, rituximab, valganciclovir, or a combination of these treatments can be considered
Tas and Simonart,46
1999The only undisputed treatment for DRESS at the time is prompt withdrawal of the causative agent. Corticosteroid treatment iscontroversial. The authors suggest the potential benefit of N-acetylcysteine. They report treating 2 patients withN-acetylcysteine, but therapy was interrupted because of the development of facial edema with unknown cause
ALL ¼ allopurinol; CBZ ¼ carbamazepine; DDS ¼ dapsone; DHS ¼ drug-induced hypersensitivity syndrome; DRESS ¼ drug rash with eosinophilia and systemic symptoms;IV ¼ intravenous; IVIG ¼ intravenous immunoglobulin; LTG ¼ lamotrigine; MNC ¼ minocycline; PB ¼ phenobarbital; PHT ¼ phenytoin; VPA ¼ valproate.
PSYCHOTROPIC DRUGeINDUCED DRESS
Mayo Clin Proc. n XXX 2016;nn(n):1-15 n http://dx.doi.org/10.1016/j.mayocp.2016.03.006www.mayoclinicproceedings.org
9

TABLE 3. Summary of Evaluation and Management Recommendations for Psychotropic DrugeInduced DRESS Syndrome
1. Immediate withdrawal of the implicated drug through careful history taking
2. If indicated, hospitalization for fluid and electrolyte replacement, skin care, and nutritional supplementation
3. Evaluation with laboratory tests and imaging studies to assess internal organ involvement: complete blood count, 24-hour urine protein andeosinophil count, blood glucose, calcium, parathyroid hormone, C-reactive protein, lactate dehydrogenase, creatine phosphokinase, ferritin,quantitative polymerase chain reaction for human herpesvirus 6 and 7, Epstein-Barr virus and cytomegalovirus, triglycerides, blood culturesa. Hepatic: liver function tests, partial thromboplastin time/prothrombin time/international normalized ratio, hepatitis panelb. Cardiac: electrocardiography, echocardiography, cardiac enzymesc. Pulmonary: chest radiography, pulmonary function testsd. Renal: creatinine, serum urea nitrogen, urinalysis, renal ultrasonographye. Endocrine: thyroid-stimulating hormone/thyroxine (T4)f. Gastrointestinal: lipase levelg. Neurologic: head computed tomography or magnetic resonance imaging, electroencephalography, cerebrospinal fluid analysis
4. For patients without clinical, laboratory, or imaging evidence of internal organ involvement and only modestly elevated liver enzyme levels, no furthertreatment is necessary
5. If any of the measures in step 4 are present, prednisone (1-1.5 mg/kg/d or its equivalent) is recommended (see Table 4 for specific dosinginformation)
6. If improvement is not seen with corticosteroids, several studies have found efficacy with intravenous immunoglobulin or plasma exchange; othertreatment options include cyclophosphamide, cyclosporine, and immunosuppressants (see Table 4 for specific dosing information)
DRESS ¼ drug rash with eosinophilia and systemic symptoms.Adapted from J Am Acad Dermatol,98 with permission.
MAYO CLINIC PROCEEDINGS
10
history of exposure to high-risk drugs in theprevious 6 months,54 laboratory and imagingstudies to determine internal organ involve-ment, and a skin biopsy.99 Skin tests (patchand prick) can be important and useful indiagnosing DRESS.49 The lymphocyte trans-formation test also has diagnostic utility (re-ported sensitivity, 60%-70%; specificity,85%). This test has better diagnostic valuethan the patch test and should be performed5 to 8 weeks after the onset of DRESS.4 Impor-tantly, the clinical utility of patch tests and thelymphocyte transformation test are limitedbecause these tests are not widely used andoften are informative only if the test result ispositive.98 Treatment should begin with theprompt withdrawal of the causative drugbecause the prognosis is better with earliercessation.36 The best management practices af-ter withdrawal are still controversial. Recom-mendations from the literature includehospitalization for continued monitoring andsupportive treatment with fluid and electrolytereplacement and nutritional support. A warmand humid environment with gentle skincare (eg, warm baths or wet dressings) also isrecommended.38 For patients without clinical,laboratory, or imaging evidence of internal or-gan involvement and only modestly elevatedliver enzyme levels, no further treatment is
Mayo Clin Proc. n XXX 20
necessary.38 However, if any of these measuresare present, prednisone (1-1.5 mg/kg per dayor its equivalent) is recommended.4 Some pre-fer administering pulsed corticosteroid ther-apy over conventional oral doses becauseliver function returns to normal in a shortertime with pulsed corticosteroids.66 The useof corticosteroids in the treatment of DRESShas been debated because evidence is limitedand results have been inconsistent41,47; how-ever, the literature predominantly recom-mends either oral dosing or pulsed therapy,especially for patients with internal organinvolvement.1,36 Next, if improvement is notseen with corticosteroids, several investigatorshave reported efficacy with IVIG or plasma ex-change.70,77 Other treatment options for themanagement of corticosteroid-resistant DRESSthat have been used with some success includecyclophosphamide, cyclosporine, and immu-nosuppressants.4,81 Suggested dosing strate-gies for these treatments are included inTable 4.5,77,98,100-105
As with other similar drug-induced inflam-matory reactions, prevention is the mostimportant management strategy. When start-ing a new psychotropic medication, especiallyaromatic anticonvulsants (eg, CBZ, PHT, PB,and LTG) and nonaromatic anticonvulsants(eg, VPA, topiramate, and gabapentin), it is
16;nn(n):1-15 n http://dx.doi.org/10.1016/j.mayocp.2016.03.006www.mayoclinicproceedings.org
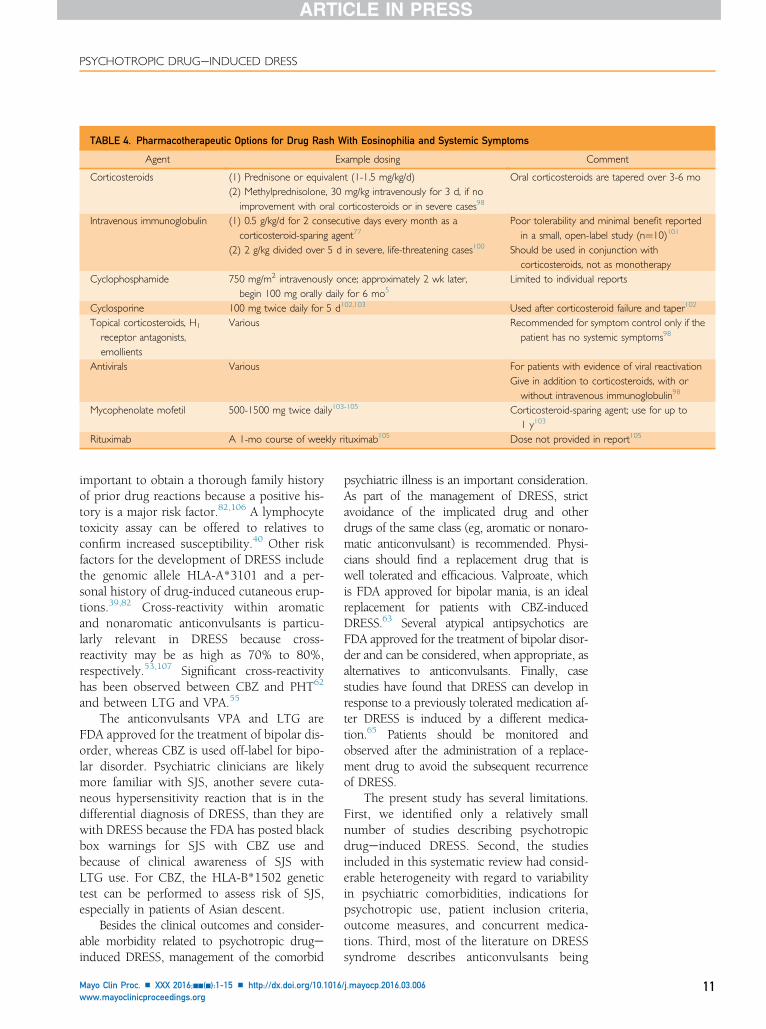
TABLE 4. Pharmacotherapeutic Options for Drug Rash With Eosinophilia and Systemic Symptoms
Agent Example dosing Comment
Corticosteroids (1) Prednisone or equivalent (1-1.5 mg/kg/d)(2) Methylprednisolone, 30 mg/kg intravenously for 3 d, if no
improvement with oral corticosteroids or in severe cases98
Oral corticosteroids are tapered over 3-6 mo
Intravenous immunoglobulin (1) 0.5 g/kg/d for 2 consecutive days every month as acorticosteroid-sparing agent77
(2) 2 g/kg divided over 5 d in severe, life-threatening cases100
Poor tolerability and minimal benefit reportedin a small, open-label study (n¼10)101
Should be used in conjunction withcorticosteroids, not as monotherapy
Cyclophosphamide 750 mg/m2 intravenously once; approximately 2 wk later,begin 100 mg orally daily for 6 mo5
Limited to individual reports
Cyclosporine 100 mg twice daily for 5 d102,103 Used after corticosteroid failure and taper102
Topical corticosteroids, H1
receptor antagonists,emollients
Various Recommended for symptom control only if thepatient has no systemic symptoms98
Antivirals Various For patients with evidence of viral reactivationGive in addition to corticosteroids, with orwithout intravenous immunoglobulin98
Mycophenolate mofetil 500-1500 mg twice daily103-105 Corticosteroid-sparing agent; use for up to1 y103
Rituximab A 1-mo course of weekly rituximab105 Dose not provided in report105
PSYCHOTROPIC DRUGeINDUCED DRESS
important to obtain a thorough family historyof prior drug reactions because a positive his-tory is a major risk factor.82,106 A lymphocytetoxicity assay can be offered to relatives toconfirm increased susceptibility.40 Other riskfactors for the development of DRESS includethe genomic allele HLA-A*3101 and a per-sonal history of drug-induced cutaneous erup-tions.39,82 Cross-reactivity within aromaticand nonaromatic anticonvulsants is particu-larly relevant in DRESS because cross-reactivity may be as high as 70% to 80%,respectively.53,107 Significant cross-reactivityhas been observed between CBZ and PHT62
and between LTG and VPA.55
The anticonvulsants VPA and LTG areFDA approved for the treatment of bipolar dis-order, whereas CBZ is used off-label for bipo-lar disorder. Psychiatric clinicians are likelymore familiar with SJS, another severe cuta-neous hypersensitivity reaction that is in thedifferential diagnosis of DRESS, than they arewith DRESS because the FDA has posted blackbox warnings for SJS with CBZ use andbecause of clinical awareness of SJS withLTG use. For CBZ, the HLA-B*1502 genetictest can be performed to assess risk of SJS,especially in patients of Asian descent.
Besides the clinical outcomes and consider-able morbidity related to psychotropic drugeinduced DRESS, management of the comorbid
Mayo Clin Proc. n XXX 2016;nn(n):1-15 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
psychiatric illness is an important consideration.As part of the management of DRESS, strictavoidance of the implicated drug and otherdrugs of the same class (eg, aromatic or nonaro-matic anticonvulsant) is recommended. Physi-cians should find a replacement drug that iswell tolerated and efficacious. Valproate, whichis FDA approved for bipolar mania, is an idealreplacement for patients with CBZ-inducedDRESS.63 Several atypical antipsychotics areFDA approved for the treatment of bipolar disor-der and can be considered, when appropriate, asalternatives to anticonvulsants. Finally, casestudies have found that DRESS can develop inresponse to a previously tolerated medication af-ter DRESS is induced by a different medica-tion.65 Patients should be monitored andobserved after the administration of a replace-ment drug to avoid the subsequent recurrenceof DRESS.
The present study has several limitations.First, we identified only a relatively smallnumber of studies describing psychotropicdrugeinduced DRESS. Second, the studiesincluded in this systematic review had consid-erable heterogeneity with regard to variabilityin psychiatric comorbidities, indications forpsychotropic use, patient inclusion criteria,outcome measures, and concurrent medica-tions. Third, most of the literature on DRESSsyndrome describes anticonvulsants being
/j.mayocp.2016.03.006 11

MAYO CLINIC PROCEEDINGS
12
used to treat epileptic conditions. Although weattempted to screen for literature that dealtspecifically with psychotropic drugeinducedDRESS, some studies may have included pa-tients receiving medications to treat nonpsy-chiatric illnesses.
CONCLUSIONDRESS is a severe cutaneous eruption thattypically presents within 1 or 2 months ofdrug initiation. Common clinical featuresinclude maculopapular rash, elevated liverenzyme levels, lymphadenopathy, facialedema, and eosinophilia. Common psycho-tropic medications that have been impli-cated in this reaction are CBZ, LTG, PHT,VPA, and PB. Several case reports in theliterature describe various approaches tomanagement, the cornerstones of which areprompt withdrawal of the implicated drugand administration of corticosteroids. Forcases of corticosteroid-resistant DRESS,IVIG, cyclophosphamide, cyclosporine, andimmunosuppressants have had efficacy.Management of comorbid psychiatric illnessincludes strict avoidance of the implicateddrug and other drugs in the same class(eg, aromatic, nonaromatic) and identifica-tion of a replacement drug (eg, VPA forCBZ-induced DRESS).
ACKNOWLEDGMENTSWe thank Ms Ann M. Farrell for her work inconducting a literature review on psychotropicdrugeinduced DRESS syndrome.
SUPPLEMENTAL ONLINE MATERIALSupplemental material can be found online at:http://www.mayoclinicproceedings.org. Sup-plemental material attached to journal articleshas not been edited, and the authors takeresponsibility for the accuracy of all data.
Abbreviations and Acronyms: CBZ = carbamazepine;DRESS = drug rash with eosinophilia and systemic symp-toms; FDA = US Food and Drug Administration; IVIG =intravenous immunoglobulin; LTG = lamotrigine; PB =phenobarbital; PHT = phenytoin; SJS = Stevens-Johnsonsyndrome; VPA = valproate; ZIP = ziprasidone
Correspondence: Address to Maria I. Lapid, MD, Depart-ment of Psychiatry and Psychology, Mayo Clinic, 200 FirstSt SW, Rochester, MN 55905 ([email protected]).
Mayo Clin Proc. n XXX 20
REFERENCES1. Chen Y-C, Cho Y-T, Chang C-Y, Chu C-Y. Drug reaction
with eosinophilia and systemic symptoms: a drug-induced hy-persensitivity syndrome with variable clinical features. Derma-tologica Sinica. 2013;31(4):196-204.
2. Camous X, Calbo S, Picard D, Musette P. Drug reaction witheosinophilia and systemic symptoms: an update on pathogen-esis. Curr Opin Immunol. 2012;24(6):730-735.
3. Picard D, Janela B, Descamps V, et al. Drug reaction witheosinophilia and systemic symptoms (DRESS): a multiorganantiviral T cell response. Sci Transl Med. 2010;2(46):46ra62.
4. López-Rocha E, Blancas L, Rodríguez-Mireles K, et al. Preva-lence of DRESS syndrome. Rev Alerg Mex. 2014;61(1):14-23.
5. Laban E, Hainaut-Wierzbicka E, Pourreau F, et al. Cyclophos-phamide therapy for corticoresistant drug reaction with eosin-ophilia and systemic symptoms (DRESS) syndrome in a patientwith severe kidney and eye involvement and Epstein-Barr virusreactivation. Am J Kidney Dis. 2010;55(3):e11-e14.
6. Iacob SA, Sotropa A. DRESS syndrome with hepatic involve-ment in a patient with depressive disorder. Rom J Intern Med.2014;52(3):163-166.
7. Alexander T, Iglesia E, Park Y, et al. Severe DRESS syndromemanaged with therapeutic plasma exchange. Pediatrics. 2013;131(3):e945-e949.
8. Bagshaw SM, Cload B, Gilmour J, Leung ST, Bowen TJ. Drug-induced rash with eosinophilia and systemic symptoms syn-drome with bupropion administration. Ann Allergy AsthmaImmunol. 2003;90(5):572-575.
9. Eppenberger M, Hack D, Ammann P, Rickli H, Maeder MT.Acute eosinophilic myocarditis with dramatic response to ste-roid therapy: the central role of echocardiography in diagnosisand follow-up. Tex Heart Inst J. 2013;40(3):326-330.
10. Volcheck GW. Clinical evaluation and management of drughypersensitivity. Immunol Allergy Clin North Am. 2004;24(3):357-371.
11. Chan JC, Chan HHL, Yeung CK. Drug reaction with eosino-philia and systemic symptoms (DRESS). Hong Kong J DermatolVenereol. 2012;20(4):163-170.
12. Sultan SJ, Sameem F, Ashraf M. Drug reaction with eosino-philia and systemic symptoms: manifestations, treatment,and outcome in 17 patients. Int J Dermatol. 2015;54(5):537-542.
13. Um SJ, Lee SK, Kim YH, et al. Clinical features of drug-inducedhypersensitivity syndrome in 38 patients. J Investig Allergol ClinImmunol. 2010;20(7):556-562.
14. Botelho LF, Higashi VS, Padilha MH, Enokihara MM,Porro AM. DRESS: clinicopathological features of 10 casesfrom an university hospital in São Paulo. An Bras Dermatol.2012;87(5):703-707.
15. Chiou CC, Yang LC, Hung SI, et al. Clinicopathological fea-tures and prognosis of drug rash with eosinophilia and sys-temic symptoms: a study of 30 cases in Taiwan. J Eur AcadDermatol Venereol. 2008;22(9):1044-1049.
16. Kardaun SH, Sekula P, Valeyrie-Allanore L, et al; RegiSCARStudy Group. Drug reaction with eosinophilia and systemicsymptoms (DRESS): an original multisystem adverse drug re-action; results from the prospective RegiSCAR study. Br J Der-matol. 2013;169(5):1071-1080.
17. Karimzadeh P, Bakrani V. Antiepileptic drug-related adversereactions and factors influencing these reactions. Iran J ChildNeurol. 2013;7(3):25-29.
18. Sasidharanpillai S, Riyaz N, Rajan U, et al. Drug reaction witheosinophilia and systemic symptoms: observations from a ter-tiary care institution. Indian J Dermatol Venereol Leprol. 2014;80(3):221-228.
19. Peyrière H, Dereure O, Breton H, et al; Network of theFrench Pharmacovigilance Centers. Variability in the clinicalpattern of cutaneous side-effects of drugs with systemic symp-toms: does a DRESS syndrome really exist? Br J Dermatol.2006;155(2):422-428.
16;nn(n):1-15 n http://dx.doi.org/10.1016/j.mayocp.2016.03.006www.mayoclinicproceedings.org

PSYCHOTROPIC DRUGeINDUCED DRESS
20. Phillips EJ, Chung WH, Mockenhaupt M, Roujeau JC,Mallal SA. Drug hypersensitivity: pharmacogenetics and clinicalsyndromes. J Allergy Clin Immunol. 2011;127(3, suppl):S60-S66.
21. Santiago F, Gonçalo M, Vieira R, Coelho S, Figueiredo A. Epi-cutaneous patch testing in drug hypersensitivity syndrome(DRESS). Contact Dermatitis. 2010;62(1):47-53.
22. Walsh S, Diaz-Cano S, Higgins E, et al. Drug reaction witheosinophilia and systemic symptoms: is cutaneous pheno-type a prognostic marker for outcome? a review of clinico-pathological features of 27 cases. Br J Dermatol. 2013;168(2):391-401.
23. Yang MS, Kang MG, Jung JW, et al. Clinical features and prog-nostic factors in severe cutaneous drug reactions. Int Arch Al-lergy Immunol. 2013;162(4):346-354.
24. Heinzerling LM, Tomsitz D, Anliker MD. Is drug allergy lessprevalent than previously assumed? a 5-year analysis. Br J Der-matol. 2012;166(1):107-114.
25. Pereira de Silva N, Piquioni P, Kochen S, Saidon P. Risk factorsassociated with DRESS syndrome produced by aromatic andnon-aromatic antipiletic drugs. Eur J Clin Pharmacol. 2011;67(5):463-470.
26. Lee HY, Chou D, Pang SM, Thirumoorthy T. Acute general-ized exanthematous pustulosis: analysis of cases managed ina tertiary hospital in Singapore. Int J Dermatol. 2010;49(5):507-512.
27. Boccara O, Valeyrie-Allanore L, Crickx B, Descamps V. Asso-ciation of hypogammaglobulinemia with DRESS (Drug Rashwith Eosinophilia and Systemic Symptoms). Eur J Dermatol.2006;16(6):666-668.
28. Sasidharanpillai S, Riyaz N, Khader A, Rajan U, Binitha MP,Sureshan DN. Severe cutaneous adverse drug reactions: a clin-icoepidemiological study. Indian J Dermatol. 2015;60(1):102.
29. Mokhtari F, Nikyar Z, Naeini BA, Esfahani AA, Rahmani S.Adverse cutaneous drug reactions: eight year assessment inhospitalized patients. J Res Med Sci. 2014;19(8):720-725.
30. Grando LR, Schmitt TA, Bakos RM. Severe cutaneous reac-tions to drugs in the setting of a general hospital. An Bras Der-matol. 2014;89(5):758-762.
31. Wei CH, Chung-Yee Hui R, Chang CJ, et al. Identifying prog-nostic factors for drug rash with eosinophilia and systemicsymptoms (DRESS). Eur J Dermatol. 2011;21(6):930-937.
32. Yang CY, Dao RL, Lee TJ, et al. Severe cutaneous adverse re-actions to antiepileptic drugs in Asians. Neurology. 2011;77(23):2025-2033.
33. Maoz KB, Brenner S. Drug rash with eosinophilia and systemicsymptoms syndrome: sex and the causative agent. Skinmed.2007;6(6):271-273.
34. Chen YC, Chiu HC, Chu CY. Drug reaction with eosinophiliaand systemic symptoms: a retrospective study of 60 cases.Arch Dermatol. 2010;146(12):1373-1379.
35. Avancini J, Maragno L, Santi CG, Criado PR. Drug reactionwith eosinophilia and systemic symptoms/drug-induced hy-persensitivity syndrome: clinical features of 27 patients. ClinExp Dermatol. 2015;40(8):851-859.
36. Choudhary S, McLeod M, Torchia D, Romanelli P. Drug reac-tion with eosinophilia and systemic symptoms (DRESS) syn-drome. J Clin Aesthet Dermatol. 2013;6(6):31-37.
37. Jeung YJ, Lee JY, Oh MJ, Choi DC, Lee BJ. Comparison of thecauses and clinical features of drug rash with eosinophilia andsystemic symptoms and Stevens-Johnson syndrome. AllergyAsthma Immunol Res. 2010;2(2):123-126.
38. Roujeau JC, Haddad C, Paulmann M, Mockenhaupt M. Man-agement of nonimmediate hypersensitivity reactions to drugs.Immunol Allergy Clin North Am. 2014;34(3):473-487.
39. Walsh SA, Creamer D. Drug reaction with eosinophilia andsystemic symptoms (DRESS): a clinical update and review ofcurrent thinking. Clin Exp Dermatol. 2011;36(1):6-11.
40. Verma R, Vasudevan B, Pragasam V. Severe cutaneousadverse drug reactions. Med J Armed Forces India. 2013;69(4):375-383.
Mayo Clin Proc. n XXX 2016;nn(n):1-15 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
41. Husain Z, Reddy BY, Schwartz RA. DRESS syndrome, part I:clinical perspectives. J Am Acad Dermatol. 2013;68(5):693.e1-693.e14.
42. Kano Y, Shiohara T. The variable clinical picture of drug-induced hypersensitivity syndrome/drug rash with eosinophiliaand systemic symptoms in relation to the eliciting drug. Immu-nol Allergy Clin North Am. 2009;29(3):481-501.
43. Cacoub P, Musette P, Descamps V, et al. The DRESS syn-drome: a literature review. Am J Med. 2011;124(7):588-597.
44. Criado PR, Criado RF, Avancini JM, Santi CG. Drug reactionwith Eosinophilia and Systemic Symptoms (DRESS)/Drug-induced Hypersensitivity Syndrome (DIHS): a review of cur-rent concepts. An Bras Dermatol. 2012;87(3):435-449.
45. Fernando SL. Drug-reaction eosinophilia and systemic symp-toms and drug-induced hypersensitivity syndrome. Australas JDermatol. 2014;55(1):15-23.
46. Tas S, Simonart T. Drug rash with eosinophilia and systemicsymptoms (DRESS syndrome). Acta Clin Belg. 1999;54(4):197-200.
47. Su HH, Hsu CC, Fang CK. Suspected drug reaction witheosinophilia and systemic symptoms (DRESS) secondaryto quetiapine in an elderly patient. Int J Gerontol. 2014;8(1):45.
48. Roujeau J-C, Allanore L, Liss Y, Mockenhaupt M. Severe cuta-neous adverse reactions to drugs (SCAR): definitions, diag-nostic criteria, genetic predisposition. Dermatologica Sinica.2009;27:203-209.
49. Aouam K, Bel Hadj Ali H, Youssef M, et al. Carbamazepine-induced DRESS and HHV6 primary infection: the importanceof skin tests. Epilepsia. 2008;49(9):1630-1633.
50. Bakker CV, Hegt VN, Praag MC. Lamotrigine hypersensitivitysyndrome and spiking fever. Indian J Dermatol. 2012;57(6):504.
51. Bamanikar A, Dhobale S, Lokwani S. Pregabalin hypersensitiv-ity in a patient treated for postherpetic neuralgia. Indian J Phar-macol. 2013;45(5):522-523.
52. Didenko I, Ferreira F, Tomaz E, Salgado M, de Sousa AV,Inacio F. Carbamazepine-induced DRESS/DIHS: case report[in Portuguese]. Rev Portuguesa Imunoalergol. 2009;17(6):539-547.
53. Ginory A, Chaney-Catchpole M, Demetree JM, MayolSabatier LM, Nguyen M. Drug reaction with eosinophiliaand systemic symptoms (DRESS) in an adolescent treatedwith lamotrigine. J Pediatr Pharmacol Ther. 2013;18(3):236-240.
54. Oelze LL, Pillow MT. Phenytoin-induced drug reaction witheosinophilia and systemic symptoms (DRESS) syndrome: acase report from the emergency department. J Emerg Med.2013;44(1):75-78.
55. Özaydin E, Çayir A, Gürler T, Cengizlier R, Köse G,Vidinlisan S. Lamotrigine-induced hypersensitivity syndrome:case report. Gazi Med J. 2009;20(3):135-138.
56. Roquin G, Peres M, Lerolle N, et al. First report of lamotrigine-induced drug rash with eosinophilia and systemic symptomssyndrome with pancreatitis. Ann Pharmacother. 2010;44(12):1998-2000.
57. Teng P, Tan B. Carbamazepine-induced DRESS syndrome in achild: rapid response to pulsed corticosteroids. Dermatol On-line J. 2013;19(5):18170.
58. Turcu G, Ioana NR, Forsea D. Drug Rash with Eosinophiliaand Systemic Symptoms (DRESS) caused by lamotrigine: acase report and brief review. Therapeut Pharmacol Clin Toxicol.2012;16(1):66-69.
59. Albayrak F, Cerrah S, Albayrak A, Dursun H, Yildirim R,Uyanik A. DRESS syndrome with fatal results induced by so-dium valproate in a patient with brucellosis and a positivecytoplasmic antineutrophilic cytoplasmic antibody test result.Rheumatol Int. 2012;32(7):2181-2184.
60. Bourgeois GP, Cafardi JA, Groysman V, et al. Fulminantmyocarditis as a late sequela of DRESS: two cases. J AmAcad Dermatol. 2011;65(4):889-890.
/j.mayocp.2016.03.006 13
MAYO CLINIC PROCEEDINGS
14
61. Do-Pham G, Charachon A, Duong TA, et al. Drug reactionwith eosinophilia and systemic symptoms and severe involve-ment of digestive tract: description of two cases. Br J Dermatol.2011;165(1):207-209.
62. Fsadni C, Fsadni P, Piscopo T, Mallia Azzopardi C. Carbamaz-epine-induced drug reaction with eosinophilia and systemicsymptoms syndrome in a 35-year-old man with epilepsy.Clin Neuropharmacol. 2008;31(5):295-298.
63. Ganeva M, Gancheva T, Lazarova R, et al. Carbamazepine-induced drug reaction with eosinophilia and systemic symp-toms (DRESS) syndrome: report of four cases and briefreview. Int J Dermatol. 2008;47(8):853-860.
64. Halink DA, Marijnissen RM, Schut AA, Oude Voshaar RC.Drug reaction with eosinophilia and systemic symptomsinduced by carbamazepine: DRESSed to kill. Gen Hosp Psychi-atry. 2011;33(4):412.e5-412.e8.
65. Kim CW, Choi GS, Yun CH, Kim DI. Drug hypersensitivity topreviously tolerated phenytoin by carbamazepine-inducedDRESS syndrome. J Korean Med Sci. 2006;21(4):768-772.
66. Kocaoglu C, Cilasun C, Solak ES, Kurtipek GS, Arslan S. Suc-cessful treatment of antiepileptic drug-induced DRESS syn-drome with pulse methylprednisolone. Case Rep Pediatr.2013;2013:928910.
67. Lo MH, Huang CF, Chang LS, et al. Drug reaction with eosin-ophilia and systemic symptoms syndrome associated myocar-ditis: a survival experience after extracorporeal membraneoxygenation support. J Clin Pharm Ther. 2013;38(2):172-174.
68. Mehta M, Shah J, Khakhkhar T, Shah R, Hemavathi KG. Anti-convulsant hypersensitivity syndrome associated with carba-mazepine administration: case series. J PharmacolPharmacother. 2014;5(1):59-62.
69. Mendiratta V, Bhushan P. Phenytoin-induced DRESS withcross-reactivity to carbamazepine in a 10-year-old Indian child.Clin Exp Dermatol. 2006;31(5):720-721.
70. El Omairi N, Abourazzak S, Chaouki S, Atmani S, Hida M.Drug Reaction with Eosinophilia and Systemic Symptom(DRESS) induced by carbamazepine: a case report and litera-ture review. Pan Afr Med J. 2014;18:9.
71. Brizendine CE, Naik PJ. Drug rash with eosinophilia and sys-temic symptoms syndrome associated with use of phenytoin,divalproex sodium, and phenobarbital. Am J Health Syst Pharm.2013;70(6):507-510.
72. Gupta A, Srivastava VK, Rizvi I, Aziz A. DRESS syndrome. BMJCase Rep. doi:10.1136/bcr-03-2012-6128.
73. Matsuda H, Saito K, Takayanagi Y, et al. Pustular-type drug-induced hypersensitivity syndrome/drug reaction with eosino-philia and systemic symptoms due to carbamazepine withsystemic muscle involvement. J Dermatol. 2013;40(2):118-122.
74. Neri I, Virdi A, Piccolo V, Patrizi A. Drug rash with eosinophiliaand systemic symptoms (DRESS) due to lamotrigine in a 12-year-old girl. Eur J Pediatr Dermatol. 2011;21:7-10.
75. Saha S, Sengupta M. A rare cause of eosinophilia-anticonvulsant hypersensitivity syndrome. Indian J Pract Pediatr.2012;14(3):366-369.
76. Seth D, Kamat D, Montejo J. DRESS syndrome: a practicalapproach for primary care practitioners. Clin Pediatr (Phila).2008;47(9):947-952.
77. Singer EM, Wanat KA, Rosenbach MA. A case of recalcitrantDRESS syndrome with multiple autoimmune sequelae treatedwith intravenous immunoglobulins. JAMA Dermatol. 2013;149(4):494-495.
78. Swanson EA, Low L, Naini BV. Severe enterocolitis associatedwith antiepileptic-induced drug reaction with eosinophilia andsystemic symptoms. Hum Pathol. 2014;45(9):1973-1977.
79. Valencak J, Ortiz-Urda S, Heere-Ress E, Kunstfeld R, Base W.Carbamazepine-induced DRESS syndrome with recurrent fe-ver and exanthema. Int J Dermatol. 2004;43(1):51-54.
80. Suzuki Y, Fukuda M, Tohyama M, Ishikawa M, Yasukawa M,Ishii E. Carbamazepine-induced drug-induced hypersensitivity
Mayo Clin Proc. n XXX 20
syndrome in a 14-year-old Japanese boy. Epilepsia. 2008;49(12):2118-2121.
81. Syn WK, Naisbitt DJ, Holt AP, Pirmohamed M, Mutimer DJ.Carbamazepine-induced acute liver failure as part of theDRESS syndrome [published correction appears in Int J ClinPract. 2005;59(11):1371]. Int J Clin Pract. 2005;59(8):988-991.
82. Anjum N, Polak ME, Ardern-Jones M, Cooper HL. Presenceof the HLA-A*3101 allele in a familial case of drug reactionwith eosinophilia and systemic symptoms, secondary to carba-mazepine. Clin Exp Dermatol. 2014;39(3):307-309.
83. Aplyn M. Rash, organ dysfunction, and eosinophiles: it is aDRESS [letter]. Intensive Care Med. 2013;39(9):1666-1667.
84. Ben Salem C, Slim R, Denguezli M, Nouira R, Hmouda H,Bouraoui K. A recurrent drug rash with eosinophilia and sys-temic symptoms. Pediatr Dermatol. 2007;24(6):666-668.
85. Bonaci-Nikolic B, Jeremic I, Nikolic M, Andrejevic S,Lavadinovic L. High procalcitonin in a patient with drug hyper-sensitivity syndrome. Intern Med. 2009;48(16):1471-1474.
86. Chang JY, Kim SC. Anticonvulsant hypersensitivity syndromeassociated with Epstein-Barr virus reactivation. Yonsei Med J.2007;48(2):317-320.
87. Naveen KN, Ravindra MS, Pai VV, Rai V, Athanikar SB,Girish M. Lamotrigine induced DRESS syndrome. Indian J Phar-macol. 2012;44(6):798-800.
88. Gordon JS, Neyman KM, Wells RD, Chen SC. Drug rash witheosinophilia and systemic symptoms (DRESS syndrome).Cutis. 2012;89(4):180-182.
89. Kang SY, Kim JY, Kim MY, et al. Drug-induced hypersensitivitysyndrome/drug reaction with eosinophilia and systemic symp-toms syndrome induced by cilostazol and carbamazepine.J Dermatol. 2012;39(8):723-724.
90. Allam JP, Paus T, Reichel C, Bieber T, Novak N. DRESS syn-drome associated with carbamazepine and phenytoin. Eur JDermatol. 2004;14(5):339-342.
91. Cornell SL, DiBlasi D, Arora NS. Drug reaction with eosino-philia and systemic symptoms: DRESS following initiation ofoxcarbazepine with elevated human herpesvirus-6 titer. CaseRep Dermatol Med. 2014;2014:853281.
92. Yun SJ, Lee JB, Kim EJ, et al. Drug rash with eosinophilia andsystemic symptoms induced by valproate and carbamazepine:formation of circulating auto-antibody against 190-kDa anti-gen. Acta Derm Venereol. 2006;86(3):241-244.
93. D’Orazio JL. Oxcarbazepine-induced Drug Reaction withEosinophilia and Systemic Symptoms (DRESS). Clin Toxicol(Phila). 2008;46(10):1093-1094.
94. Bicknell LT, Sanches M, Schatte DJ. Erythema multiforme vs.DRESS syndrome associated with the combined use of lamo-trigine and cyclobenzaprine: a case report. Int J Psychiatry Med.2012;44(4):305-314.
95. Amante MF, Filippini AV, Cejas N, Lendoire J, Imventarza O,Parisi C. DRESS syndrome and fulminant hepatic failureinduced by lamotrigine. Ann Hepatol. 2009;8(1):75-77.
96. Chauhan A, Anand S, Thomas S, Subramanya HC, Pradhan G.Carbamazepine induced DRESS syndrome. J Assoc PhysiciansIndia. 2010;58:634-636.
97. Gaig P, García-Ortega P, Baltasar M, Bartra J. Drug neosensiti-zation during anticonvulsant hypersensitivity syndrome.J Investig Allergol Clin Immunol. 2006;16(5):321-326.
98. Husain Z, Reddy BY, Schwartz RA. DRESS syndrome, part II:management and therapeutics. J Am Acad Dermatol. 2013;68(5):709.e1-709.e9.
99. Roujeau JC. Drug reaction with eosinophilia and systemicsymptoms (DRESS). UpToDate website. http://www.uptodate.com/contents/drug-reaction-with-eosinophilia-and-systemic-symptoms-dress. Updated September 30, 2015.Accessed December 14, 2015.
100. Spriet S, Banks TA. Drug reaction with eosinophilia and sys-temic symptoms syndrome. Allergy Asthma Proc. 2015;36(6):501-505.
16;nn(n):1-15 n http://dx.doi.org/10.1016/j.mayocp.2016.03.006www.mayoclinicproceedings.org

PSYCHOTROPIC DRUGeINDUCED DRESS
101. Joly P, Janela B, Tetart F, et al. Poor benefit/risk balance ofintravenous immunoglobulins in DRESS. Arch Dermatol.2012;148(4):543-544.
102. Zuliani E, Zwahlen H, Gilliet F, Marone C. Vancomycin-induced hypersensitivity reaction with acute renal failure: res-olution following cyclosporine treatment. Clin Nephrol. 2005;64(2):155-158.
103. Bourgeois GP, Cafardi JA, Hughey LC, Groysman V.Fulminant myocarditis as a late sequelae of DRESSsyndrome [abstract]. J Am Acad Dermatol. 2009;60(3,suppl 1):AB123-AB124.
104. Mortezavi M, Lomas JM, Looney RJ. Treatment of Drug Reac-tion with Eosinophilia and Systemic Symptoms (DRESS) with
Mayo Clin Proc. n XXX 2016;nn(n):1-15 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
mycophenolate mofetil as a steroid-sparing agent [abstract].Ann Allergy Asthma Immunol. 2014;113(5, suppl):A29.
105. Shaughnessy KK, Bouchard SM, Mohr MR, Herre JM, Salkey KS.Minocycline-induced drug reaction with eosinophilia and sys-temic symptoms (DRESS) syndrome with persistent myocar-ditis. J Am Acad Dermatol. 2010;62(2):315-318.
106. van Zoelen MA, de Graaf M, van Dijk MR, et al. Valproic acid-induced DRESS syndrome with acute liver failure [letter]. NethJ Med. 2012;70(3):155.
107. Aouam K, Ben Romdhane F, Loussaief C, et al. Hypersensitiv-ity syndrome induced by anticonvulsants: possible cross-reactivity between carbamazepine and lamotrigine. J ClinPharmacol. 2009;49(12):1488-1491.
/j.mayocp.2016.03.006 15