management of postpartum haemorrhage
TRANSCRIPT

MANAGEMENT
OF PPH

Multidisciplinary team consisting of obstetrician ,
anaesthetist, haemotologist, theatre staff and nursing staff
is ideal.
The patients general condition is evaluated and if he/she
is in shock immediate resuscitative measures are
instituted.
A hand on uterus will confirm atonicity and enable
uterine massage which should be done continuously.

PRINCIPLES OF MANAGEMENT
1. GENERAL MEASURES
* Resuscitative measures
* Investigations
* Monitoring
* Confirm the cause of PPH
2. MEDICAL METHODS
3. MECHANICAL METHODS
4. SURGICAL METHODS
5. RADIOLOGICAL ARTERIAL EMBOLISATION

GENERAL MEASURES
RESUSCITATIVE MEASURESFLUID REPLACEMENT
Two intravenous infusions with large 14 gauge cannulaeare started
Aim is to replace 2-3 times the estimated blood lose
Crystalloids (normal saline or Ringer lactate) infused at the rate of 1L in 15-20 min
Colloids can be given until blood is available (1-2L)
Crossmatch blood should be given as rapidly as possible
A central venous pressure line can be introduced

BLOOD COMPONENT THEORY
Correction of RBC deficit is guided by the rule that each
unit of packed cells will restore Hb concentration by
1gm/dl
If there is evidence of coagulation defects fresh frozen
plasma, platelet concentrates, and cryoprecipitate are
made available

For every 6 units of red cells , 4 units of fresh frozen
plasma can be given
Each adult dose of cryoprecipitate will raise fibrinogen
level by 100mg/dl
Each adult dose of platelet concentrates will raise the
platelet count by 20000/L

OTHER MEASURES
Oxygen can be given by a mask or nasal cannula at rate of 10-15L/min
Patients leg may be elevated in order to increase venous return
If unconscious patient should be turned to one side to minimise aspiration in case of vomiting
Important to keep patient warm as hypothermia will exacerbate poor peripheral circulation

INVESTIGATIONS
LABORATORY TESTS
Hb, haematocrit, bloodgrouping and crossmatching must
be done
Platelet count, fibrinogen assay, partial thromboplastin
time, prothrombin time should be measured .
Electrolytes, urea and creatinine needed in severe
hemorrhage
Bedside tests like clot observation test or clotting time
can be done

MONITORING
Pulse and Blood pressure
Heart rate by ECG monitor
Oxygen saturation by pulse oximetry
Central venous pressure line- to assess adequacy of fluid
replacement
Hourly urine output
Fluids and drugs given

CONFIRMATION OF DIAGNOSIS
Genital tract injuries are looked for and if present,
sutured
If placenta is not yet expelled signs of seperation are
looked for
If there are retained placental fragments , they are
removed
Succenturiate lobe should not be missed
Coagulopathy is checked
MEDICAL METHODS
Oxytocin
20-40 units in 500ml of normal saline
Ergometrine
Ergometrine 0.25mg or methergin 0.2mg given
Prostaglandin derivatives
15 methyl analogue of prostodin- 250microgram given.

MECHANICAL METHODS
BIMANUAL COMPRESSION
Abdominal hand massages the posterior aspect of uterus
and the vaginal hand made into a fist presses the anterior
uterine aspect through anterior fornix.
Should be done continuously to promote uterine
contraction
Aortic compression against sacral promontory to reduce
bleeding.
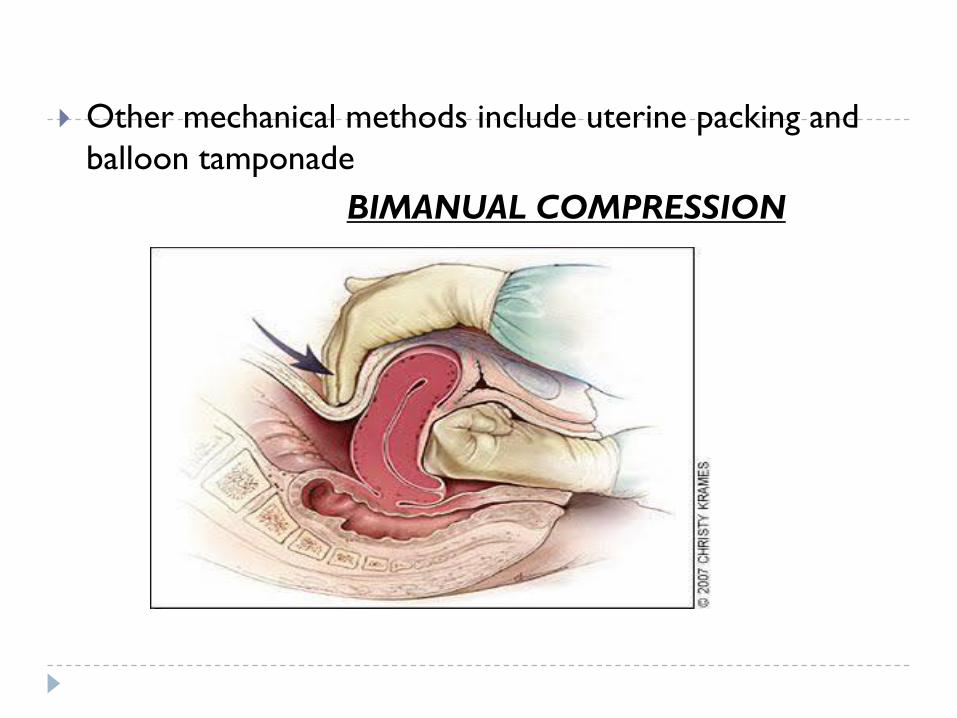
Other mechanical methods include uterine packing and
balloon tamponade
BIMANUAL COMPRESSION
SURGICAL METHODS
UNDER SEWING
CHO’s MULTIPLE BLOCK SUTURES
B LYNCH OR BRACE SUTURE
MODIFIED B LYNCH (HAYMAN)
SYSTEMIC PELVIC DEVASCULARISATION-
HYSTERECTOMY

UNDERSEWING
Undersewing the placental bed with figure of eight or
purse string sutures
Done at caesarean section for placenta praevia
MULTIPLE BLOCK SUTURES
Involve approximation of anterior and posterior uterine
walls with multiple squares until no space is left in uterine
cavity

MULTIPLE BLOCK
SUTURES

BRACE SUTURE
Involves use of vertical brace sutures
Very easy to perform
Commonly performed at caesarean section but can also
be done after vaginal delivery.
MODIFIED B LYNCH(HAYMAN)
Involves use of two vertical compression sutures placed
on either side of fundus
Quicker than brace suture.
Does not require a low transverse incision . Hence it is
useful following a vaginal delivery

BRACE SUTURE
SYSTEMIC PELVIC DEVASCULARISATION
Involve laparotomy and progressive stepwise
devascularisation
Uterine , ovarian and finally the internal iliac arteries are
ligated
Absorbable sutures should be used always
The ascending branch of uterine artery or the anterior
division of internal iliac artery are usually ligated.

UTERINE ARTERY LIGATION

HYSTERECTOMY
Considered as a last resort
Indications include severe atonic hemorrhage, placenta
accreta , placenta praevia and uterine rupture
Subttotal hysterectomy may be easier and quicker but is
inadequate in cases where bleeding is in the lower
segment as in placenta praevia and adherent placenta
Ovaries should be retained
RADIOLOGICAL ARTERIAL
EMBOLISATION
The patient shoud be hemodynamically stable
Under angiographic guidance and percutaneous
transcatheter technique , femoral artery catheterisation is
done
Bleeding vessels are identified
Embolisation carried out with gel foam or microspheres

Management of secondary PPH
High vaginal swab should be taken for culture
Broad spectrum antibiotics should be started
If the ultrasound scan reveals retained products , uterus
should be evacuated
The tissues obtained should be sent for culture and
histopathological studies
If there is evidence of sepsis , evacuation should be
delayed by 12-24 hours to reduce risk of septicemia
If bleeding is severe uterine artery ligation or
hysterectomy is done

THANK YOU