male reproductive system. organs of the urinary system are also shown
TRANSCRIPT

Male reproductive system. Organs of the urinary system are also shown.

Overview of Anatomy and Physiology
Organs of the male reproductive system include:
the testes, the ductal system, the accessory glands and the penis
Functions include: producing and storing sperm, depositing sperm for fertilization and developing the make secondary sex
characteristics
Testes (gonads) - 2 oval structures enclosed in the scrotum ( a sac like structure that lies suspended fro the abdominal wall).
This position keeps the temperature win the testes below
normal body temperature which is necessary for viable
sperm production and storage. - Seminiferous Tubules
-each testis contains 1-3 coiled seminiferous tubules that produce the sperm cells
-Produce testosterone which is responsible for the development of male secondary sex characteristics
Ductal System
-includes the epididymis, rete testes, ductus deferens (vas deferens), ejaculatory duct and
urethra -Process: Sperm produced in the seminiferous
tubules immediately travels through a network of ducts called the rete testes. These passageways contain cilia that sweep sperm out of the testes
into the epididymis (a tightly coiled tube structure).

Epididymis -With sexual stimulation, the walls of the
epididymis contract forcing the sperm along the seminiferous tubules to the vas deferens
Ductus Deferens ( vas deferens) -Approximately 18 inches long
-Rises along the posterior wall of the testes which moves
upward to pass through the inguinal canal into the pelvic
cavity and loops over the bladder -The ductus deferens, nerves and blood vessels are
enclosed in a connective sheath called the spermatic cord. (Vasectomy-severing of the ductus deferens.)

Ejaculatory duct and urethra
-Behind the urinary bladder, the ejaculatory duct
connects with the ductus deferens. It unites with
the urethra to pass through the prostate gland. -Only 1 inch long
-The urethra extends the length of the penis with
the urinary meatus. The urethra carries both sperm and urine but because of the urethral sphincter, it does not do so at the same time.
Accessory Glands
-With each ejaculation (2-5 mL fluid), approximately 200- 500 million sperm are released
-Seminal Vesicles: paired structures that lie at the base of
the bladder and produce 60% of the volume of semen. Fluid is released into the ejaculatory ducts to meet the
sperm -Prostate Gland: surrounds the neck of the bladder and urethra. Composed of muscular and glandular tissue. -Cowper’s Glands: 2 pea sized glands under the male
urethra, provide lubrication during sexual intercourse

Urethra and Penis
-Urethra: conveys urine from the bladder and carries sperm to the outside
-Penis: organ of copulation. The shaft ends with an enlarged tip called the glans penis. The skin covering
the glans penis is called the prepuce or foreskin. -Circumcision: removal of foreskin. Preventative for
phimosis- a tightness of the prepuce (tightness of the prepuce prevents retraction of the foreskin over the
glans). -3 masses of erectile tissue containing numerous sinuses fill the shaft of the penis. These fill with
blood during sexual stimulation causing an erection. After ejaculation, it returns to a flaccid state.
A

Sperm
-3 distinct parts; the head, midpiece and tail -Mature sperm live approximately 48 hours in
the female reproductive system
-If comes in contact with a mature egg, the enzyme on the head of each sperm bombards
the egg in an attempt to breakdown the coating
-Only one sperm enters and causes fertilization.
The remaining sperm disintegrate.

Epididymitis-an infection of the cordlike excretory duct of the testicle
Can be sterile or nonsterile inflammation
-Sterile inflammation can be caused by direct injury, reflux of urine down the vas deferens (reflux is related to
a strain while the bladder is full).
-Nonsterile inflammation can be caused by gonorrhea,
chlamydia, mumps, TB, prostatitis or prolonged use of
a catheter
-Common causative organisms are: Staph. Aureus, E.
Coli, Streptococcus and N. Gonorrhea
INFLAMMATORY DISORDERS
Signs and Symptoms
-Sudden severe pain in the scrotum; radiates
along the spermatic tube; increased sensitivity
and pain with walking -Edema; scrotal area becomes tender
-Chills and fever
Treatment -Diagnostic Tests: UA to check for
pyuria, CBC for WBC check -Epididymis is massaged by the physician, the fluid is expelled and sent to the lab -Bed rest, scrotal support and cold packs
-Antibiotics -If abscess forms, incision and drainage
(I & D)

Nursing Interventions
-Monitor bed rest -Scrotal support (elevate on folded towel; use
athletic support when ambulatory) -Cold compresses
-Patient teaching-medications, signs of inflammatory resolution
Orchitis-inflammation of the testes
-May follow from infection of the urinary or
reproductive tract -Most often occurs as a complication of a blood borne infection origination in the
epididymis -Other causes: secondary to mumps of
viral infection of a salivary gland, trauma of
metastasis
Signs and Symptoms -Swelling
-Severe pain -Chills, fever, vomiting
-Hiccoughs -sometimes delirium
Treatment -Bed rest, scrotal support
-Cold compresses -NSAIDS
-Antibiotics
Nursing Interventions- Same as for epididymis
Prostatitis
Common complication of urethritis caused by Chlamydia or Gonorrhea
Bacterial invasion originates in the bloodstream
or from a descending infection from the kidneys
Acute or Chronic
Signs and Symptoms
INFLAMMATORY DISORDERS
Medical: when urethritis suspected
Should not be catheterized
Possible cultures
MEDICAL-SURGICAL MANAGEMENT
• Pharmaceutical– Antibiotics, Procaine: epididymis, orchitis– Antibiotics, analgesics, and stool softeners:
prostatitis

Activity: Treatment for prostatitis
Bed rest
Scrotum elevated
Cold packs to area
Increase fluids
Sitz baths
MEDICAL-SURGICAL
MANAGEMENT
Monitor vital signs, especially temperature and I&OEncourage intake of fluids
Assess painMaintain bed rest
Keep scrotum elevated while in bedUse of athletic support while ambulatory
Cold pack, as ordered
NURSING MANAGEMENT


Benign Prostatic Hyperplasia (BPH)
Early symptoms: hesitancy, nocturia, eventually unable to completely empty bladder which could lead to infection.
BENIGN NEOPLASMS
Medical: digital rectal exam, diagnostic tests, monitor for increased symptoms.
Non-surgical treatment: Balloon dilatation, a prostate urethral stent, and thermotherapy.
These treatments do not correct the problem of incomplete bladder emptying.
Surgical: Transurethral resection of the prostate, or open surgery (suprapubic or retro pubic ) and perineal prostatectomy.
MEDICAL-SURGICAL
MANAGEMENT

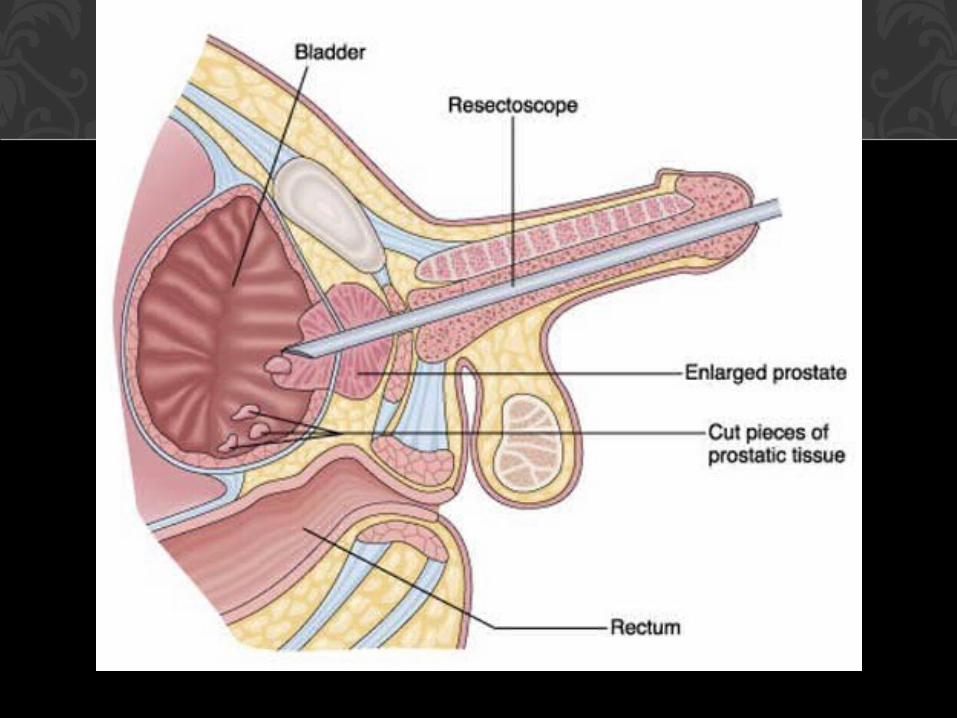
Laser prostatectomy: based on thermal action: transurethral ultrasound-guided laser-induced prostatectomy.
Pharmacological: Finasteride (Procar), Alpha Blockers i.e.. terazosin hydrochloride, doxazocin mesylate, tamulosin
hydrochloride.
Post-op pain: belladonna and opium, and narcotic analgesics.
MED-SURG MANAGEMENT
Foley catheter considerations
Pre-op care as ordered
Monitor and accurately record I&O
Monitor Vital signs and color of urine
Routine post-op care
After catheter removed, encourage voiding at first urge.
NURSING MANAGEMENT
Prostate Cancer:
Second leading cause of cancer deaths in men
Most are adenocarcinomas: slow growing tumors that spread through the lymphatics.
Early symptoms: dysuria, weak urinary stream, increased urinary frequency
Later symptoms: hematuria, urethra obstruction
MALIGNANT NEOPLASMS
Medical: Treatment depends on extent of disease. radiation is alternative to surgery. Not always effective depending on
condition of patient. Also radioactive seed planting is an alternative.
Surgical: Removal of entire prostate gland, including the capsule and adjacent tissue. The urethra is anastomosed to
the bladder neck. Usual approach is perineal.
MED-SURG MANAGEMENT
Medical, con’t: complications of surgery include urinary incontinence, sexual dysfunction, hemorrhage, infection,
thrombosis, and strictures.
Removal of testes (orchiectomy) may be done as palliative measure
Cryosurgery
MED-SURG MANAGEMENT

Pharmacological:
Hormonal agents: diethylstilbestrol, goserelin acetate, or leuprolide acetate
Systemic chemotherapy: not very effective
MED-SURG MANAGEMENT
Encourage all male clients over 40 years of age to have annual rectal exam of the prostate and a PSA serum level.
Monitor vital signs, I&O, signs of bleeding, assess for pain, administer analgesics as ordered
NURSING MANAGEMENT
Testicular Cancer: Most common cancer in young men ages 15-35. Etiology unknown. Usually a small, hard, painless
lump is first sign noticed.
Early intervention is essential: need to teach clients how to perform self testicular exam.
MALIGNANT NEOPLASMS

Medical: Testicular ultrasound, serum acid or alkaline phosphatase test.
Surgical: Biopsy contraindicated
Removal of testis, spermatic cord, and inguinal contents, with exam of nodes
Teaching plan for TSE
MED-SURG MANAGEMENT
• Pharmacological: combination chemotherapy with cisplatin, vinblastine sulfate, and bleomycin sulfate. All in conjunction with a radical inguinal orchiectomy.
ENCOURAGE ALL MALES OVER 15 YEARS OF AGE TO PERFORM TSE!
Post-op: monitor vital signs and incisional drainage. Maintain strict asepsis when changing dressings. Provide client to
voice fears and concerns.
NURSING MANAGEMENT

Penile Cancer: rare; high correlation with poor hygiene or no circumcision, hx of STDs
Symptoms: painless nodular growth on foreskin, fatigue and weight loss.
Metastases common in inguinal nodes and adjacent organs.
MALIGNANT NEOPLASMS
Medical: primary treatment is surgical.
Surgical: If not extensive with no metastases, remaining penis should be long enough for client to void standing.
If penectomy necessary, a suprapubic catheter may be inserted or an ileoconduit may be performed.
MED-SURG MANAGEMENT

Provide emotional support
Monitor vital signs and I&O
Elevate scrotum to prevent edema
Assess pain and administer analgesics as ordered.
NURSING MANAGEMENT