major haemorrhage policy for trauma
DESCRIPTION
Major Haemorrhage Policy for Trauma. Rachel Hawes RVI Northern trauma network conference March 2014. Background. Leading cause of traumatic death Advances in haemostatic resuscitation Balanced transfusion 1:1:1:1 Introduction of MHP Questions How many major haemorrhage pt? - PowerPoint PPT PresentationTRANSCRIPT

Rachel HawesRVI
Northern trauma network conference
March 2014
Major Haemorrhage Policy for Trauma

Background
• Leading cause of traumatic death• Advances in haemostatic resuscitation• Balanced transfusion 1:1:1:1• Introduction of MHP
• Questions– How many major haemorrhage pt?– Frequency of Acute Coagulopathy of Trauma (ACoT)– How effective is our MHP?

RVI Major Haemorrhage Policy
• Standardise blood product use
• Reduce logistical delay
• Prehospital initiation • Pre-thawed FFP– avoid delay in receiving
balanced transfusion

Audit • Inclusions
– All trauma patients to RVI– April 2012 - April 2013– >18 yrs– Activation of MHP– Or >4 products in 1 hr
• Exclusions– Children– Preceding medical event– Transfers via Trauma Units
• Data Collection– Injury Severity Score (ISS)– TARN Predicted Survival– Actual 30 day mortality
– Presentation - Hb, PT, Fib– Products Transfused– Post MHP - Hb, PT, Fib

Results - How much trauma do we get?
• April 2012 - April 2013• 935 trauma calls• 899 TARN patients
– RTA– Assault– Fall
• Frequent of major haemorrhage?• 51 MHP Patients (5.6%)

Injury Severity Score v Mortality
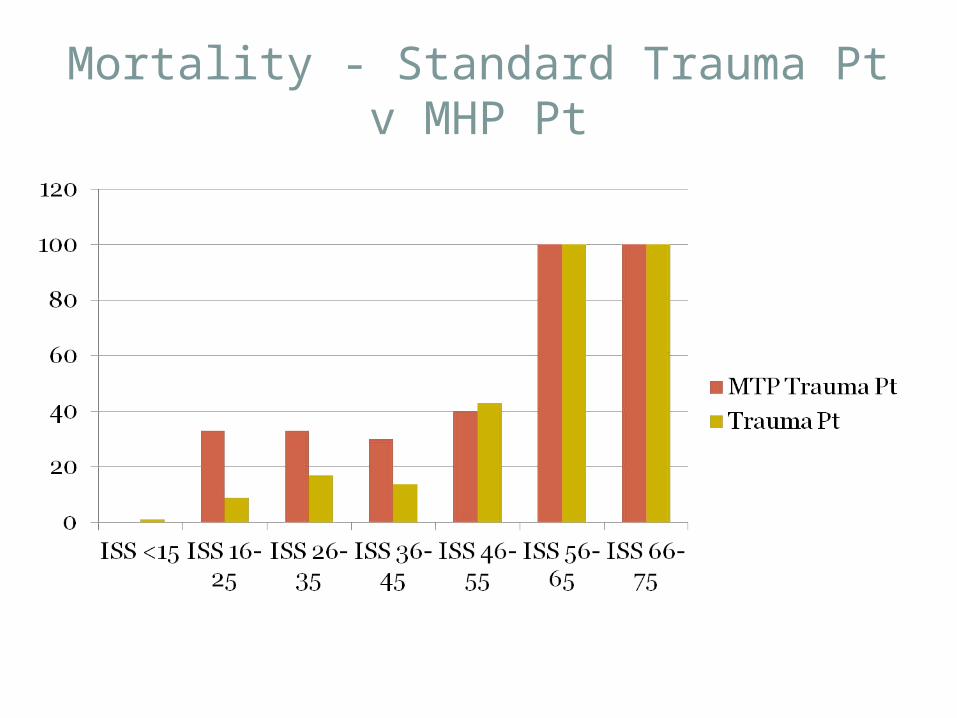
Mortality - Standard Trauma Pt v MHP Pt

ISS versus Predicted & Actual Outcome

Coagulopathy

ACoT on Presentation in ED?
• Fibrinogen on presentation• Fibrinogen <1.5 = 21%
• PT on presentation• PT> 18 = 16%

Is ACoT due to Prehospital Fluid?
• No correlation between fluid volumes given and– Hb on presentation– PT on presentation– Fib on presentation

Presence of Coagulopathy Post MHP
• Post MHP Fib <1.5 = 0%• (Data for 33 Pt)
• Post MHP PT > 18 = 3%• (Data for 29 Pt)

Hb on Arrival v Post MHP
• Hb on arrival <8.0 = 6.8%
• Over and under transfusion
• Hb post MTP <8.0 = 5.8%

The Future
• Over and under transfusion– Deviation from policy– Timing of lab results– Lack of Point of Care testing - guide treatment
• Potential role of ROTEM/ TEG
• Prehospital Transfusion

Limitations
• Early deaths after presentation
• Unable to get bloods
• Included in ISS calculations but excluded for comparison of lab data

Summary• Trauma - Mortality proportional to ISS• 5% of patients have major haemorrhage• Increased mortality ass with major haemorrhage• 20% established ACoT on arrival
– Not related to prehospital fluid administration
• MHP effective in treatment and prevention of ACoT
• Future– POCT – TEG or ROTEM– ‘Blood on Board’ HEMS

Questions?