major depressive disorder: recognition and management in primary care dr. levkovitz y. director...
TRANSCRIPT

Major Depressive Major Depressive Disorder:Disorder:
Recognition and Recognition and Management Management
in Primary Carein Primary CareDr. Levkovitz Y.
Director Day-Hospital & Cognitive and Emotional Laboratory,
Shalvata Mental Health Center,School of Medicine, Tel Aviv University, Israel.

ObjectivesObjectives
To be more knowledgeable about To be more knowledgeable about recognizing and treating depressionrecognizing and treating depression
To increase comfort in managing To increase comfort in managing depression in primary caredepression in primary care

Causes of Disability by Illness Category
United States and Canada15-44 years old
0 5 10 15 20 25 30 35 40
Mental Illness*
Alcohol and drug use
Injuries, including self-inflicted
Respiratory disease
Musculoskeletal disease
Sense organ disease
Cardiovascular disease
Migraine
Infectious disease, excluding HIV
WHO World Health Report 2002
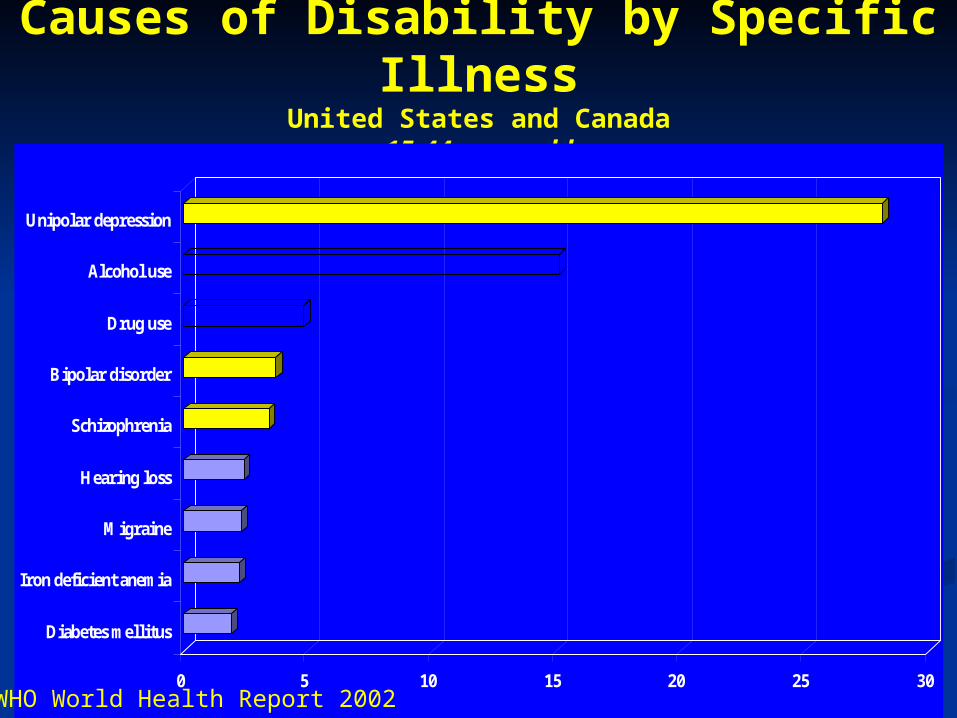
Causes of Disability by Specific Illness
United States and Canada15-44 years old
0 5 10 15 20 25 30
Unipolar depression
Alcohol use
Drug use
Bipolar disorder
Schizophrenia
Hearing loss
Migraine
Iron deficient anemia
Diabetes mellitus
WHO World Health Report 2002

EpidemiologyEpidemiology
Major Depressive Disorder (MDD) is Major Depressive Disorder (MDD) is the one of the the one of the most commonmost common mental mental disorders in primary care settingsdisorders in primary care settings
The The prevalenceprevalence of current MDD in of current MDD in primary care settings has been found primary care settings has been found to range from 9.2% to 13.5%to range from 9.2% to 13.5%
MDD may occur MDD may occur at at any ageany age

Natural History of Major Natural History of Major DepressionDepression
Recurrent, Recurrent, episodicepisodic disorder in disorder in > > 50%50%
Residual Residual symptomssymptoms persist between persist between episodes in 20-35% (partial episodes in 20-35% (partial remission)remission)
Systemic disorderSystemic disorder . . Most serious complication is Most serious complication is suicidesuicide; ;
others include marital, parental, others include marital, parental, social, and vocational difficulties.social, and vocational difficulties.

1מקרה מספר
( . 5 , נשואה ואם לבת )בת 30מורן בת הגיע לרופא המשפחה ומתארת עייפות רבה בחודשיים
האחרונים. מורן עובדת כמזכירה ומתארת כי היא מבצעת שגיאות רבות בעבודתה. המעסיק שלה מעיר לה לאחרונה על שגיאותיה. מרגישה כי לאחרונה קשה לה יותר להתרכז. מדווחת על מריבות ומחלוקות בזמן
האחרון עם בעלה בשל לחץ כלכלי בבית. כשמתעוררת בבוקר מרגישה עייפה ו "לחוצה
מהמחשבה שהיא צריכה ללכת לעבודה". דיווח על התקפי פלפיטציות וכאבים בחזה.
פחות מתעניינת בילדים ומרגישה שפחות משקיעה בהם.

(1מקרה דיון )
איזה שאלות היית רוצה לשאול את •מורן?

)המשך(1מקרה מספר
לאחר שנשאלה מספרת כי מקיצה משנתה בשלוש לפנות בוקר עם מועקה בחזה. לא הולכת לשיעורי "פילאטיס" והתעמלות במועדון השכונתי. מבשלת
למשפחתה אך קיימת ירידה בתאבון . לא בטוחה אם יש שינוי במשקל. מרגישה בטוחה בנישואיה אבל מרגישה כי בעלה פחות מתעניין בה כי היא שווה
פחות במיוחד כי יש לה פחות עניין בקיום יחסי מין עימו. מפחדת כי בעלה יעזוב אותה. מרגישה אשמה
ביחס לילדיה ולבעלה. מרגישה כי צריכה להיענש והתאבדות תפתור את בעיותיה. משתמשת יותר ביין
אדום כדי שתוכל לישון.

(1מקרה דיון )
האם אתה צריך לראות את בעלה?•
מה תעשה אם היא מסרבת לדבר עם •בעלה
כי היא מפחדת שידע כי היא חוששת לנאמנותו?

1מקרה מספר
( . 5 לבת )בת אם , נשואה ו30 בתמורן ( עצב ? )עייפות רבההגיע לרופא המשפחה ומתארת
בחודשיים האחרונים. מורן עובדת כמזכירה ומתארת בעבודתה. המעסיק שלה שגיאות רבותכי היא מבצעת
מעיר לה לאחרונה על שגיאותיה. מרגישה כי לאחרונה ומחלוקות מריבות. מדווחת על להתרכז קשה לה יותר
בזמן האחרון עם בעלה בשל לחץ כלכלי בבית. מרגישה עייפה ו"לחוצה כשמתעוררת בבוקר
מהמחשבה שהיא צריכה ללכת לעבודה". דיווח על וכאבים בחזה. פחות מתעניינת התקפי פלפיטציות
בילדים ומרגישה פחות משקיעה בהם.

)המשך(1מקרה מספר
בשלושלאחר שנשאלה מספרת כי מקיצה בשנתה לשיעורי לא הולכתלפנות בוקר עם מועקה בחזה.
"פילאטיס" והתעמלות במועדון השכונתי. מבשלת . לא בטוחה אם ירידה בתאבוןלמשפחתה אך קימת
יש שינוי במשקל. מרגישה בטוחה בנישואיה אבל מרגישה כי בעלה פחות מתעניין בה כי היא שווה
עניין בקיום יחסי מין פחות פחות במיוחד כי יש לה עימו. מפחדת כי בעלה יעזוב אותה. מרגישה אשמה
ביחס לילדיה ולבעלה. מרגישה כי צריכה להיענש ביין תפתור את בעיותיה. משתמשת יותר והתאבדות
כדי שתוכל לישון. אדום

RecognitionRecognition
Depression is difficult to diagnosis in Depression is difficult to diagnosis in primary care and often goes primary care and often goes undetected:undetected:depressed mood typically depressed mood typically notnot
presenting complaint presenting complaint competing demands (acute and competing demands (acute and
chronic illnesses)chronic illnesses) limitedlimited resources and time resources and time








Major Depression: Four Major Depression: Four HallmarksHallmarks Depressed Mood.Depressed Mood. Anhedonia:Anhedonia: loss of interest or pleasure loss of interest or pleasure Physical Symptoms:Physical Symptoms:
sleep disturbance, low energy, sleep disturbance, low energy, appetite or weight change, appetite or weight change, psychomotor changespsychomotor changes
Psychological Symptoms:Psychological Symptoms: low self-esteem, poor concentration, low self-esteem, poor concentration,
suicidal ideation/obsession suicidal ideation/obsession surrounding death.surrounding death.
Assessing for Depression Assessing for Depression and Anhedoniaand Anhedonia Do not ask patient: “Are you Do not ask patient: “Are you
Depressed?”, INSTEAD, Ask: “Depressed?”, INSTEAD, Ask: “How has How has your mood been?”your mood been?”
Ask about Anhedonia: “What are you Ask about Anhedonia: “What are you doing for fun?” OR: “doing for fun?” OR: “Does your Does your (pain,anxiety, grief, whatever (pain,anxiety, grief, whatever symptoms patient mentions) keep you symptoms patient mentions) keep you from doing all the things you enjoy?”from doing all the things you enjoy?”

(1מקרה דיון )
מה הצעד הבא?•
האם תרצה לדעת פרטים נוספים על •משפחתה ?
האם תרצה לדעת פרטים עליה או על •עברה?
אילו בדיקות דם תרצה להזמין?•

Risk FactorsRisk Factors Prior episodePrior episode of depression of depression Family historyFamily history of depressive disorder of depressive disorder Prior suicide attemptPrior suicide attempt Female genderFemale gender Medical conditionsMedical conditions Lack of social supportLack of social support Stressful life eventsStressful life events Current substance useCurrent substance use

(1מקרה דיון )אבחנה מבדלת
•Substance Induced Disorder ?Substance Induced Disorder ?•Mood Disorder ?Mood Disorder ?•Anxiety Disorder ?Anxiety Disorder ?•Personality Disorder ?Personality Disorder ?•Relationship distress, financial Relationship distress, financial stress related ??stress related ??•Medical Conditions ?Medical Conditions ?•Medications ?Medications ?

Dependence/Withdrawal- 9.2% (Warner, 1995)- 20% (Hall, 1994 )- anger, irritability, aggression- aches, pains, chills- depression
- inability to concentrate- sleep disturbance- slight tremors - decrease in appetite- sweating- craving3 to 7 days, to several weeks after abstinence
(Haney, 1999)

Organic Illnesses Associated with Depression
Rheumatologic - systemic lupus erythematosus, rheumatoid arthritis
Cardiac - mitral valve prolapse.Endocrine - hyperthyroidism,
hypothyroidism, diabetes mellitus, hypercalcemia, Cushing’s syndrome

UniversiUniversityty
of NSWof NSW
Chronic fatigue syndromeChronic fatigue syndrome

UniversiUniversityty
of NSWof NSW
and
What is chronic fatigue syndrome?Definition
• Unexplained, persistent or relapsing fatigue, that is: – of new, definite onset– not due to exertion– not relieved by rest– associated with a
substantial reduction in daily activities
• Four or more of:– impaired short term
memory or concentration
– sore throat– tender lymph nodes– muscle pain– joint pain– headaches– unrefreshing sleep– post-exertional malaise
Fukuda K et al. Ann Intern Med 1994; 121: 953-9.

UniversiUniversityty
of NSWof NSWDrugs Commonly Associated with Drugs Commonly Associated with DepressionDepression
• Benzodiazepines• Cimetidine• Beta-blockers• Corticosteriods• Oral contraceptives• Indomethacin

Assessing Risk of SuicideAssessing Risk of Suicide
Assess risk factors:Assess risk factors:PRIOR ATTEMPTSPRIOR ATTEMPTSFamily history of suicideFamily history of suicideHopelessnessHopelessnessDemographics Demographics
Caucasian, male, elderly, lives Caucasian, male, elderly, lives alonealone
Clinical Clinical Substance abuse, psychosis, Substance abuse, psychosis, potentially terminal illnesspotentially terminal illness

Assessing for SuicideAssessing for Suicide Use a gradual, sensitive approach to raise Use a gradual, sensitive approach to raise
the subject:the subject: How does the future look to you?How does the future look to you? Living with (pain/anxiety/patients’ Living with (pain/anxiety/patients’
symptoms) can be very difficult. Do you symptoms) can be very difficult. Do you sometimes wish your life was over?sometimes wish your life was over?
Have you had thoughts that you would Have you had thoughts that you would be better off dead?be better off dead?
Have you had thoughts of hurting Have you had thoughts of hurting yourself?yourself?
Have you thought about how you might Have you thought about how you might hurt yourself?hurt yourself?

When to Consider Involving When to Consider Involving PsychiatryPsychiatry Suicidal ideationSuicidal ideation Psychotic symptomsPsychotic symptoms Manic symptomsManic symptoms Current substance abuseCurrent substance abuse Severe psychosocial problemsSevere psychosocial problems

Interventions: What can be Interventions: What can be done?done? Depression is one of the most Depression is one of the most
treatable mental illnessestreatable mental illnesses• 70% - 75% of all depressed people 70% - 75% of all depressed people
respond to treatmentrespond to treatment• almost all who receive treatment almost all who receive treatment
experience some relief in symptomsexperience some relief in symptoms MedicationMedication PsychotherapyPsychotherapy Electroconvulsive TherapyElectroconvulsive Therapy Watchful waitingWatchful waiting

Management of DepressionManagement of Depression Give an Give an adequate trialadequate trial of treatment of treatment
(therapeutic dose for 6-8 weeks)(therapeutic dose for 6-8 weeks) Follow closelyFollow closely until patient responds until patient responds Change treatmentChange treatment if patient doesn’t if patient doesn’t
respondrespond Continue medication for Continue medication for 6-9 months6-9 months
minimum. minimum. If patient has a history of 2 or more If patient has a history of 2 or more
previous depression episodes, continue previous depression episodes, continue for for 2 years2 years or more. or more.

Overview of AntidepressantsOverview of Antidepressants Selective Serotonin Reuptake Inhibitors Selective Serotonin Reuptake Inhibitors
(SSRIs):(SSRIs): fluoxetine (Prozac), sertraline (Zoloft), fluoxetine (Prozac), sertraline (Zoloft),
paroxetine (Paxet), citalopram (Lustral)paroxetine (Paxet), citalopram (Lustral) Selective Serotonin Norepinepherine Selective Serotonin Norepinepherine
Reuptake Inhibitors (SNRIs):Reuptake Inhibitors (SNRIs): venlafaxine (Effexor), Duloxetine (Cymbalta).venlafaxine (Effexor), Duloxetine (Cymbalta).
Medications With Unique Mechanism of Medications With Unique Mechanism of Actions (MOA):Actions (MOA): bupropion (Wellbutrin), mirtazapine bupropion (Wellbutrin), mirtazapine
(Remeron), nefazodone (Serzone)(Remeron), nefazodone (Serzone) Older Agents (Tricyclic antidepressants or Older Agents (Tricyclic antidepressants or
TCAs):TCAs): desipramine, nortriptyline desipramine, nortriptyline

Therapeutic vs. Side EffectsTherapeutic vs. Side Effects
Effects of Effects of antidepressaantidepressant treatmentnt treatment
Time in weeksTime in weeks0 1 2 3 4
Therapeutic Therapeutic effectseffects
Side effectsSide effects

Side EffectsSide Effects Are relatively commonAre relatively common Are the #1 reason patients give for Are the #1 reason patients give for
stopping medicationsstopping medicationsTherefore:Therefore: TalkTalk to patients about common side to patients about common side
effectseffects WaitWait - many side effects resolve with time - many side effects resolve with time Consider Consider reducing reducing the dose temporarilythe dose temporarily Consider changing to Consider changing to anotheranother type of type of
medicationmedication Consider changing Consider changing timingtiming of medication of medication

Adjunctive MedicationsAdjunctive Medications AnxietyAnxiety
Consider short term use of a Consider short term use of a benzodiazepinebenzodiazepine
InsomniaInsomnia Trazodone – warn about Trazodone – warn about priapismpriapism Antihistamines (hydroxyzine, Antihistamines (hydroxyzine,
diphenhydramine)diphenhydramine) Sexual DysfunctionSexual Dysfunction
sildenafilsildenafil

1מקרה מספר
, סטודנט באוניברסיטת תל אביב.24ליאם, בן מתואר כ "ביישן ומופנם". יש לו קשיים בחברה ואפיזודות של פאניקה באירועים חברתיים.
לאחרונה הבחין בעליה בתדירות התקפי החרדה באירועים בהם היה צריך להציג מעבודותיו.
חודשים האחרונים מדווח על ישנוניות ועייפות. 4ב הוא מאחר לכיתה ונרדם בשיעורים. כשהוא נמצא בכיתה
פעמים 3 הוא מרגיש דחף לספור את חבריו לכיתה ולאחר לספור את התלמידים הלובשים חולצות
כחולות. הוא מוצא את הספירה "מלחיצה". הוא מרגיש חייב לספור כל פרק בספר פעמים.

(1מקרה דיון )
איזה שאלות היית רוצה לשאול את ליאם ?•

)המשך(1מקרה מספר
ליאם מדלג על ארוחות כי איננו רעב. הוא הפסיק לראות את תכנית הטלויזיה האהובה עליו ולצאת עם
הכלב שלו. הוא מדווח על ירידה משמעותית בריכוז וחווה ירידה
בזיכרון. מרגיש כי הוא חייב להפסיק ללמוד כי הוא מבזבז את
כספם של הוריו והוא "כאב ראש" למרצים. הוא משתמש במריחואנה כדי להרגיע את עצמו
, אבל כעת לא מרגיש כי זה עוזר לו. נמאס לו להמשיך ככה.

(1מקרה דיון )אבחנה מבדלת
•Major Depressive Episode with some Atipycal features, with obsessions and compulsions, History of Social Anxiety Disorder ?•Why not just SAD?•Why not Mixed Anxiety and Depression?

Depression Features SpecifiersMelancolia:•Either loss of pleasure or lack of reactivity to usually pleasurable stimuli.>3 of: prevasive non reactive sadness-melancholic, depressionworse in the morning, early morning awakening, marked psychomotor retardation or agitation significant anorexia or weight loss, excessive or inappropriate guilt.Atypical: •Reactivity of mood to positive events. •>2 of: significant weight gain or increased appetite, hypersomnia, “leaden paralysis” or long standing pattern of interpersonal rejection sensitivity.


Thanks !Thanks !

Depression in Primary CareDepression in Primary Care Depression In Western Industrialized Nations Depression In Western Industrialized Nations
(DSM-IV):(DSM-IV): Males: 2-3% of population at any given time, Males: 2-3% of population at any given time,
and 5-12% for population in lifetime. and 5-12% for population in lifetime. Females:5-9% of population at any given Females:5-9% of population at any given
time, and 10-25% for population in lifetime. time, and 10-25% for population in lifetime. Percent of mental disorders accounted for by Percent of mental disorders accounted for by
depression: Males (up to) 15%, Females (up to) depression: Males (up to) 15%, Females (up to) 45% (rough estimate).45% (rough estimate).
In primary care practices 5-9% patients at any In primary care practices 5-9% patients at any given time have Major Depression (it is given time have Major Depression (it is estimated that only one third to one half are estimated that only one third to one half are recognized by practitioners).recognized by practitioners).
Consequences of Untreated Consequences of Untreated DepressionDepression Depression is the Depression is the 2nd2nd leading cause leading cause
of disability in industrialized of disability in industrialized countriescountries
Depression associated with:Depression associated with:2x2x increased risk of death overall increased risk of death overall26x26x increased risk of suicide increased risk of suicide
Impaired social functioningImpaired social functioning

Consequences of Untreated Consequences of Untreated Depression (continued)Depression (continued) Depressed patients visit primary care Depressed patients visit primary care
provider provider 3x3x more than non- more than non-depressed patientsdepressed patients
2-5x2-5x increase in days absent from increase in days absent from workwork
Cost of depression in US in 1990 Cost of depression in US in 1990 estimated to be estimated to be $44 billion$44 billion

Making the DiagnosisMaking the Diagnosis
Depression DisordersDepression DisordersMajor depressive disorder Major depressive disorder (MDD)(MDD)
Minor (subthreshold) Minor (subthreshold) depressiondepression
Adjustment disorder with Adjustment disorder with depressed mooddepressed mood
DysthymiaDysthymia

Diagnostic Criteria for Diagnostic Criteria for Major Depression (DSM-IV)Major Depression (DSM-IV)
Major depression is present when the Major depression is present when the patient has had at least 5 of the 9 patient has had at least 5 of the 9 following symptoms for following symptoms for a minimum of a minimum of two weekstwo weeks. One of the symptoms must . One of the symptoms must be either:be either:
1.1. Depressed moodDepressed mood -- or ---- or --2.2. Loss of interest or pleasure -- Loss of interest or pleasure --
and --and --

Diagnostic Criteria (Diagnostic Criteria (continuedcontinued))
3. 3. Significant change in weight or Significant change in weight or appetiteappetite
4. 4. Insomnia or hypersomniaInsomnia or hypersomnia5. 5. Psychomotor agitation or Psychomotor agitation or
retardationretardation6. 6. Fatigue or loss of energyFatigue or loss of energy7. 7. Feelings of worthlessness or Feelings of worthlessness or
guiltguilt8. 8. Impaired concentration or ability Impaired concentration or ability
to to make decisions make decisions9. 9. Thoughts of suicide or self-harmThoughts of suicide or self-harm

Diagnostic Criteria (Diagnostic Criteria (continuedcontinued))
Symptoms must be accompanied by Symptoms must be accompanied by functional impairment in one or more of functional impairment in one or more of the following domains:the following domains:
work/schoolwork/school doing things at homedoing things at home relationships with other peoplerelationships with other people
PHQ9 includes 10PHQ9 includes 10thth question addressing question addressing functional impairmentfunctional impairment

Depression Coexisting with Depression Coexisting with Other Behavioral DisordersOther Behavioral Disorders
Alcohol DependencyAlcohol Dependency Anxiety Disorders (panic attacks, Anxiety Disorders (panic attacks,
phobias)phobias) Eating DisordersEating Disorders Obsessive Compulsive DisorderObsessive Compulsive Disorder Somatization DisordersSomatization Disorders Personality DisordersPersonality Disorders Grief and Adjustment ReactionsGrief and Adjustment Reactions

Minor depressionMinor depression
Patient has 2 to 4 of the 9 symptoms Patient has 2 to 4 of the 9 symptoms listed above listed above
Symptoms present for at least two Symptoms present for at least two weeksweeks
One of the symptoms must be either One of the symptoms must be either item 1 (depressed mood) or item 2 item 1 (depressed mood) or item 2 (loss of interest or pleasure)(loss of interest or pleasure)

Selective Serotonin Reuptake Selective Serotonin Reuptake Inhibitors (SSRIs)Inhibitors (SSRIs) fluoxetine (Prozac), sertraline (Zoloft), fluoxetine (Prozac), sertraline (Zoloft),
paroxetine (Paxil), citalopram (Celexa)paroxetine (Paxil), citalopram (Celexa) Side effects:Side effects:
Insomnia or sedation, agitation/restlessness, GI Insomnia or sedation, agitation/restlessness, GI distress, sexual dysfunction, headachedistress, sexual dysfunction, headache
Absolute contraindication:Absolute contraindication: MAOI (not selegiline)MAOI (not selegiline)
Relative contraindication:Relative contraindication: Mania history (manic depression)Mania history (manic depression)
DysthymiaDysthymia
Depression present more days than Depression present more days than not, for 2 years or morenot, for 2 years or more
Well period can not last more than 2 Well period can not last more than 2 months during this timemonths during this time

Depression Coexisting with Depression Coexisting with Other Medical DisordersOther Medical Disorders
StrokeStroke DementiaDementia DiabetesDiabetes Coronary Artery DiseaseCoronary Artery Disease Cancer Cancer Chronic Fatigue SyndromeChronic Fatigue Syndrome FibromyalgiaFibromyalgia

Response and Remission Response and Remission defineddefined
Hamilton Depression Rating Scale (HAM-D): 17 Items, Total Score 0 - 52
15
7
Response 50% reduction from
baseline HAM-D score
Remission: HAM-D Score 7
Depression (Major Depressive Disorder)
References:1. Frank E. Conceptualization and rationale for consensus definition terms in MDD, Arch Gen Psych. 1991; 48:851-855.
HAM-D17 Scores

Drug InteractionsDrug Interactions Sertraline and citalopram have no Sertraline and citalopram have no
clinically significant drug interactions clinically significant drug interactions through the CYP450 systemthrough the CYP450 system
Fluoxetine and paroxetine are potent Fluoxetine and paroxetine are potent 2D6 inhibitors2D6 inhibitors
Nefazodone is a potent 3A4 inhibitorNefazodone is a potent 3A4 inhibitor

Common Barriers to TreatmentCommon Barriers to Treatment Practical BarriersPractical Barriers Ethnic/Cultural barriersEthnic/Cultural barriers Patient doesn’t agree with diagnosis Patient doesn’t agree with diagnosis
or planor plan Patient doesn’t understand Patient doesn’t understand
treatment plantreatment plan Patient is afraid of becoming Patient is afraid of becoming
addicted to antidepressantsaddicted to antidepressants

Common Barriers to Treatment (Continued) Side effects Patient forgets to take medications
or runs out early
Formulary restrictions Friends or family are not supportive Treatment is ‘not working’; patient
feels hopeless Treatment ‘is working’; patient is
better and wants off

AdherenceAdherence 20-50% of patients “drop out” in the 20-50% of patients “drop out” in the
first month of treatmentfirst month of treatment 30-50% of patients don’t have a 30-50% of patients don’t have a
complete response to the initial complete response to the initial treatmenttreatment
If patient is not better at 8 weeks, If patient is not better at 8 weeks, consider changing medication, consider changing medication, adding psychotherapy, or getting a adding psychotherapy, or getting a psychiatric consultationpsychiatric consultation
Improving Medication AdherenceImproving Medication Adherence Tell patients:Tell patients:
Medications take time to workMedications take time to work Medications are not addictiveMedications are not addictive Take medications every day as orderedTake medications every day as ordered Take medications even if you feel Take medications even if you feel
betterbetter Do not stop medication before first Do not stop medication before first
contacting your physiciancontacting your physician Engage in pleasant activitiesEngage in pleasant activities Call your provider if you have questionsCall your provider if you have questions

What To Do If Patients Don’t Get What To Do If Patients Don’t Get BetterBetter Wrong diagnosis?Wrong diagnosis? Insufficient dose?Insufficient dose? Insufficient length of treatment?Insufficient length of treatment? Problems with barriers to Problems with barriers to
adherence?adherence? Side effects?Side effects? Other complicating factors?Other complicating factors? Wrong treatment?Wrong treatment?

Continue Medication for 6-9 Months or Continue Medication for 6-9 Months or MoreMore Medications should be continued for 6-9 Medications should be continued for 6-9
months months after the patient gets betterafter the patient gets better People at high risk for relapse (those with People at high risk for relapse (those with
at least two prior episodes of major at least two prior episodes of major depression, dysthymia, or residual depression, dysthymia, or residual depressive symptoms) should get a full depressive symptoms) should get a full dose of medication for 2 years or more to dose of medication for 2 years or more to prevent recurrencesprevent recurrences
See patients at least every 3 monthsSee patients at least every 3 months

What To Do If Patients RelapseWhat To Do If Patients Relapse Assess adherence to medication Assess adherence to medication
regimenregimen Examine for new stressorsExamine for new stressors Restart treatment at the last Restart treatment at the last
effective dose of antidepressants effective dose of antidepressants or consider an increase in dose if or consider an increase in dose if patient is still taking medicationpatient is still taking medication
Consider adding psychotherapyConsider adding psychotherapy Consider psychiatric consultationConsider psychiatric consultation
Preparing the Patient for a Mental Preparing the Patient for a Mental Health ReferralHealth Referral Bring up the possibility of a mental Bring up the possibility of a mental
health consultation when first health consultation when first presenting the diagnosis of presenting the diagnosis of depression to the patient.depression to the patient.
The request for a mental health The request for a mental health consultation is simply a matter of consultation is simply a matter of obtaining another professional obtaining another professional opinion.opinion.
Draw the analogy of referrals made Draw the analogy of referrals made to other medical specialist, like to other medical specialist, like cardiologists, endocrinologists, etc.cardiologists, endocrinologists, etc.

Side Effects of Other Side Effects of Other AntidepressantsAntidepressants bupropion (Wellbutrin)bupropion (Wellbutrin)
Main contraindication is seizure disorder or Main contraindication is seizure disorder or eating disordereating disorder
Also effective for smoking cessation Also effective for smoking cessation Less sexual dysfunction than othersLess sexual dysfunction than others
mirtazapine (Remeron)mirtazapine (Remeron) SedationSedation Weight gainWeight gain
venlafaxine (Effexor):venlafaxine (Effexor): Relative Relative contraindication if HTN is presentcontraindication if HTN is present
nefazodone (Serzone):nefazodone (Serzone): Carries a black box Carries a black box warning for liver failurewarning for liver failure

Antidepressant DosingAntidepressant Dosing Once a day dosing:Once a day dosing:
Give sedating meds at bedtime Give sedating meds at bedtime (paroxetine, mirtazapine, nefazodone)(paroxetine, mirtazapine, nefazodone)
Activating meds (fluoxetine) in the Activating meds (fluoxetine) in the morningmorning
Starting dose is lower with the elderly, Starting dose is lower with the elderly, with the medically ill, and if there is a with the medically ill, and if there is a comorbid panic disorder.comorbid panic disorder.
Titrate to therapeutic dose as tolerated Titrate to therapeutic dose as tolerated by side effectsby side effects