magnetic resonance imaging children with spastic diplegia: correlation with the severity of their...
TRANSCRIPT

MAGNETIC RESONANCE IMAGING IN CHILDREN WITH SPASTIC DIPLEGIA: CORRELATION WITH THE SEVERITY OF THEIR MOTOR AND MENTAL ABNORMALITY
‘A N
m - m 0
18
Kenji Yokochi Kumi Aiba Masayo Horie Kazuhisa Inukai Shinji Fujimoto Mariko Kodama Kazuo Kodama
Spastic diplegia is a type of cerebral palsy that demonstrates bilateral, hypertonic involvement primarily of the lower extremities; it occurs most commonly in preterm infants (Bennett et af . 1981, Veelken et al. 1983). The brain lesions of children with spastic diplegia are not fully understood. On computed tomography (CT) ventriculomegaly, reduced quantity of periventricular white matter, and prominent deep cortical sulci are shown in diplegic children, and lesions are assumed to be in the cerebral white matter (Flodmark el af . 1987, Yokochi et al. 1989). Magnetic resonance imaging (MRI), which is superior in demonstrating the white matter lesions (Nowell et al. 1988), should express these lesions in diplegic children more precisely. We describe the M R I findings of children with spastic diplegia, and investigate the correlation between these findings and the severity of their motor and mental disability.
Subjects The MRIS of 34 children with spastic diplegia (23 males, 11 females) were studied. When last examined, their ages were between three and 10 years. All demonstrated bilateral hypertonic involve- ment of the upper extremities and absence of involuntary movements.
Head circumference measurements were all within the mean values ( f 2 SD) for
age. Three children had birthweights of >2500g, 11 had birthweights of 1500 to 1999g, 17 of lo00 to 14998 and three had birthweights of c 1OOOg. Gestational ages were 237 weeks for three children; for the remaining 31 they were 5 3 6 weeks.
The severity of the children’s motor developmental disability was ranked according to four groupings, evaluated by ability of locomotion without bracing at two and three years of corrected age: six children had walked alone at two years (group 1); eight had not walked at two, but walked alone at three years (group 2); 10 did not walk alone, but had walked sideways with support at three years (group 3); and 10 did not walk with support even at three years of age (group 4). None had undergone any surgical pro- cedure before three years of age.
The children’s intelligence quotients (IQ) were examined by the Tanaka-Binet test, the Wechsler Preschool and Primary Scale of Intelligence, or the Wechsler Intelligence Scale for Children; 13 had IQS of 1 8 0 (‘normal’) and 21 had IQS of 50 to 79 (‘subnormal’). Only one child had epilepsy.
Method MRI was performed between two and 10 years corrected age: eight children were two years of age, 10 children were three, seven were four, one was five, two were
six and the remaining six children were between seven and 10 years of age.
In 25 children, MRI was performed on a Yokogawa Medical 0.5-T Resona system; this included sagittal TZ-weighted spin- echo (SE) images 450/25/4 (TR/TE exci- tations) and axial, proton density- weighted and TZ-weighted SE images 2500/30, 90/2. A slice thickness of 7mm was used, with an intersection gap of 2mm. The axial sections studied were parallel to the orbitomeatal line. Six children had the study performed on a General Electric 1 .5-T Signa system; this included sagittal T1-weighted SE images 600/20/2 and axial and coronal, proton density-weighted and ~2-weighted SE images 2000/20, 80/2. A slice thickness of 5mm was used, with an intersection gap of 2.5mm. For the remaining three children, the study was done on a Siemens 1 * 5 - ~ Magneton system; this included sagittal TI-weighted images 600/15/2 and axial proton density-weighted and Tz- weighted SE images 3000119, 9011. A slice thickness of 8mm was used, with an intersection gap of 2mm.
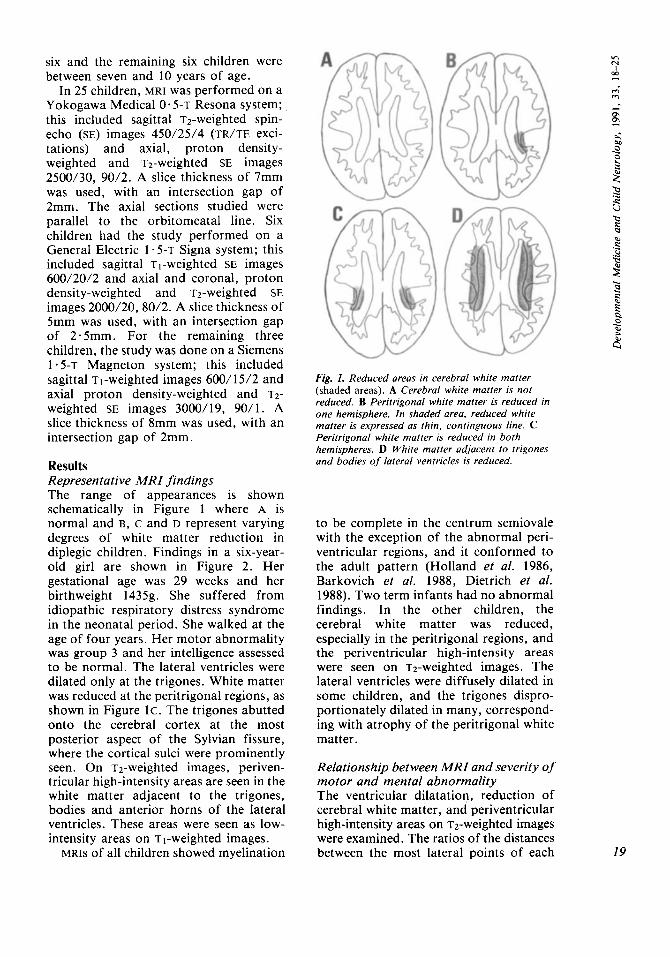
Results Representative MR I findings The range of appearances is shown schematically in Figure 1 where A is normal and B, c and D represent varying degrees of white matter reduction in diplegic children. Findings in a six-year- old girl are shown in Figure 2. Her gestational age was 29 weeks and her birthweight 14358. She suffered from idiopathic respiratory distress syndrome in the neonatal period. She walked at the age of four years. Her motor abnormality was group 3 and her intelligence assessed to be normal. The lateral ventricles were dilated only at the trigones. White matter was reduced at the peritrigonal regions, as shown in Figure lc . The trigones abutted onto the cerebral cortex at the most posterior aspect of the Sylvian fissure, where the cortical sulci were prominently seen. On T2-weighted images, periven- tricular high-intensity areas are seen in the white matter adjacent to the trigones, bodies and anterior horns of the lateral ventricles. These areas were seen as low- intensity areas on TI-weighted images.
MRIS of all children showed myelination
Fig. 1. Reduced areas in cerebral white matter (shaded areas). A Cerebral white matter is not reduced. B Peritrigonal white matter is reduced in one hemisphere. In shaded area, reduced white matter is expressed as thin, continguous line. c Peritrigonal white matter is reduced in both hemispheres. D White matter adjacent to trigones and bodies of lateral ventricles is reduced.
to be complete in the centrum semiovale with the exception of the abnormal peri- ventricular regions, and it conformed to the adult pattern (Holland et al. 1986, Barkovich et al. 1988, Dietrich et al. 1988). Two term infants had no abnormal findings. In the other children, the cerebral white matter was reduced, especially in the peritrigonal regions, and the periventricular high-intensity areas were seen on ~2-weighted images. The lateral ventricles were diffusely dilated in some children, and the trigones dispro- portionately dilated in many, correspond- ing with atrophy of the peritrigonal white matter.
Relationship between MRI and severity of motor and mental abnormality The ventricular dilatation, reduction of cerebral white matter, and periventricular high-intensity areas on ~2-weighted images were examined. The ratios of the distances between the most lateral points of each
In N
m
m m
19

4
a 9
E
cd
.I 0
e 8 u
.- - m 00 .- - .- n n .- u 2 n +a
vl
.- s % c e a .I
6
20
Fig. 2. MR images of diplegic six-year-old girl. T2-weighted images, 0.5T, 2500/90. (Upper) Periventricubr high-intensity areas are seen in white matter adjacent to anterior horns (arrows). (Lower) Lateral ventricle is dilated only at trigone. White matter is reduced in peritrigonal region. showing as thin, contiguous lines (long black arrows), where cortical sulci are prominent (short black arrow). Periventricular high-intensity areas are see in white matter adjacent to trigones (arrowheads) and bodies (white arrows). (Example of pattern C, Fig. 1.)
Fig. 3. MR image of diplegic three-year-old boy. T2-weighted images, 0*5T, 2500190. He was born at term. No abnormal MR findings; amount of cerebral white matter is normal. White matter dorsal and lateral to trigone (arrowheads) and corona radiata (arrows) show homogeneous high- intensity areas. (Example of pattern A, Fig. I.)
anterior horn to the largest transverse width between the inner table were calculated at the plane involving the anterior horn and the quadrigeminal cistern.
Reduction of cerebral white matter was classified into four patterns by axial MRI (Fig. 1). In two cases, the cerebral white matter was not reduced in amount (Figs. l A , 3). In seven cases, the peritrigonal white matter of one hemisphere was expressed as thin contiguous lines, that of the other hemisphere was expressed as wide areas (Figs. l ~ , 4). In six of these seven cases, that of the left hemisphere was reduced more than that of the right hemisphere. In 18 cases, the peritrigonal white matter was bilaterally expressed as thin, contiguous lines, and white matter anterior to the peritrigonal regions was expressed as wide areas (Figs. lc, 2 lower). In these, the trigones were dilated, and abutted onto the cerebral cortex at the most posterior aspect of the Sylvian fissure. In seven cases, the reduction of

m m
Fig. 4. MR image of diplegic three-year-old girl. T2-weighted images, 0.5T, 2500/90. Peritrigonal white matter of left hemisphere is reduced (arrow). High-intensity areas are seen in white matter adjacent to trigones (arrowheads) and bodies (white arrows). (Example of pattern B, Fig. I .)
Fig. 5. MR image of diplegic four-year-old boy. T2-weighted images, O.fiT, 2500/90. Lateral ventricles are dilated, with irregularly shaped lateral borders. White matter adjacent to trigones (arrowheads) and bodies (white arrows) is reduced, with periventricular high-intensity areas. (Example of pattern 0, Fig. I . )
the white matter expanded anteriorly, and the .white matter was expressed as the narrow band at the centrum semiovale anterior to the peritrigonal regions (Figs.
The distribution of periventricular high-intensity areas was studied. On Tz-weighted images of normal children, the white matter dorsal and superior to the trigone and the corona radiata are expressed as homogeneous intensity areas, where the intensity is higher than the surrounding white matter and lower than the cerebral cortex, as shown in Figure 3 (Daniels et al. 1987, Barkovich et al. 1988). The periventricular high-intensity areas were defined as the areas having higher intensity than the cerebral cortex. When they could not be differentiated from the high-intensity areas of the lateral ventricle on Tz-weighted images, the borders of the lateral ventricle were
ID, 5).
judged by the limits of low-intensity areas, meaning the lateral ventricle on proton-density-weighted images. In 32 cases, high-intensity areas were shown bilaterally in white matter adjacent to the trigones and the bodies, including the most posterior parts of the anterior horns. In 10 of these, the high-intensity areas were in white matter adjacent to the posterior horns, and/or anterior horns, on both sides.
The relationship between MRI appear- ances and the children’s motor and mental severity is shown in Table I. Regarding the ventricular dilatation, the ratios of the distances between the anterior horns to the largest transverse width in the children in group 4 were significantly larger than those of the children in group 1. For the other groups, ratios were not significantly different from each other. The amount of cerebral 21

TABLE I MR findings in children with spastic diplegia
Ventricular White matte? High-intensity areas3 Total dilatation’ A B C D - + + A + P + A P
Motor Group 1 0.26+0.02 1 2 4 0 2 4 0 0 0 6
(;) 2) (2 0 0 2 (0*25+0.01)
Group 2 0 .29 f0 .03 5
Group 3 0.28+0.03 0 0 1 0 0 0 7 2 1 0 10
Group 4 0.29kO-02 1 0 0 3 7 u 0 5 1 1 3 10
Mental Normal 0.27k0.03 2 3 8 1 2 9 2 1 0 14
Subnormal 0.29f0.03 4 10 6 (;A)
1 5 (0.28 * 0.03) c;) (2) cg f )
Total 0 .28 f0 .03 2 I 1 8 7 2 2 2 3 2 5 34 (0- 28 + 0.03) (0) (6) (0) (21) (31)
‘Ratios of distances between anterior horns to largest transverse width on MRI. ’Reduction in amount of cerebral white matter. ’Periventricular high-intensity areas on T2-weighted images: - none; +observed in white matter adjacent to trigones and bodies of lateral ventricle; + A observed additionally in white matter adjacent to anterior horns; +P observed additionally in white matter adjacent to posterior horns; + A P observed additionally in white matter adjacent to anterior and posterior horns. ( ) When term infants are included, figures or numbers shown only for preterm infants. *p<O.OS (F-test for ‘ventricular size’, and Xz-test for ‘white matter’).
white matter correlated with severity of motor disability, and the anterior expan- sion of the area of the white matter reduction from the trigone corresponded to more severe motor disability. However, neither the ratios showing ventricular dilatation nor the amount of white matter corresponded to severity of mental impair- ment. The distribution of periventricular high-intensity areas on Tz-weighted images did not correlate with severity of motor and mental disability.
Discussion Dilatation of the trigone, atrophy of the peritrigonal white matter and prominent deep cortical sulci have been recognized on MRI, as well as on CT, in children with spastic diplegia (Flodmark et al. 1987, Yokochi et al. 1989); the last two findings were more clearly expressed on MRI. The other qualitative abnormality in the white matter was the periventricular high- intensity areas of Tz-weighted images.
The MRI features shown are similar to other reported findings suspicious of periventricular leukomalacia (PVL) (Wilson and Steiner 1986, De Vries et al. 1987, Baker et al. 1988, De Vries et al. 1989,
Flodmark et al. 1989). In infancy, PVL is characterized by delayed myelination (Wilson and Steiner 1986, De Vries et al. 1987, McArdle et al. 1987, De Vries et al. 1989, Van de Bor et al. 1989)-and is demonstrated as the periventricular high- intensity areas on Tz-weighted images-in addition to ventriculomegaly and reduced quantity of periventricular white matter in late infancy and childhood (Wilson and Steiner 1986, De Vries et al. 1987, Baker et al. 1988, De Vries et al. 1989, Flodmark et al. 1989).
Spastic diplegia has been attributed to PVL by pathological study (Banker and Larroche 1962), and the periventricular high-intensity lesions seen on MRI are assumed to represent PVL. Ultrasono- graphic studies have shown that PVL is manifested by lesions with increased echogenicity in the periventricular white matter, followed by cystic changes in neonatal brain, and correlates to later neurodevelopmental disorders, including spastic diplegia (Dubowitz et al. 1985, Fawer et al. 1985, Graziani et al. 1986, Guzzetta et al. 1986). However, PVL confirmed by autopsy has been known to have no abnormal echogenicity in a small

number of cases (DiPietro et al. 1986). PVL is presumed to be caused by the ischaemic process in the watershed zone that exists in the periventricular white matter of the immature brain, and is characterized by involution of cystic lesions, periventricular gliosis, demyelin- ation, and loss of periventricular white matter (Banker and Larroche 1962, DeReuck et al. 1972, Armstrong and Norman 1974, Takashima and Tanaka 1978, Shuman and Selednik 1980). These histological features may be represented by the high-intensity areas on ~2-weighted images, and by the reduction of white matter.
In our study, MRI was performed be- tween the ages of two and 10 years, when the brain normally demonstrates an adult pattern of myelination (Holland et al. 1986, Barkovich et al. 1988, Dietrich et al. 1988). At these ages, the children showed an adult pattern of myelination, and the high-intensity areas on ~2-weighted images were limited to the periventricular regions adjacent to the trigones and bodies in many children. Therefore, M R I findings in diplegic children may not be marked in this age-range. The images obtained may not differ notably between machines, since many children have similar abnormal intensity areas on MRI with different machines.
Pathologically, the periventricular white matter at the occipital, parietal, and frontal lobes has been reported to be affected by PVL (Banker and Larroche 1962, DeReuck et al. 1972, Suman and Selednik 1980). On T2-weighted images, the abnormal high-intensity areas were shown in the regions adjacent to the trigones and the bodies in all children who had been preterm, and in the regions adjacent to the anterior and posterior horns in some. The distribution of the periventricular high-intensity areas on MRI coincides with the pathological distribution of PVL (Banker and Larroche 1962, DeReuck et al. 1972, Shuman and Selednik 1980). The periventricular high- intensity areas adjacent to the most anterior part of the body on MRI show the next most frequently PvL-affected site to be white matter dorsal to the internal capsule at the level of the foramen of Monro (Shuman and Selednik 1980).
These lesions may cause spasticity of the lower extremities, by damaging the corticospinal tracts.
The peritrigonal regions, where the abnormal high-intensity areas show re- duction of white matter, are those most severely affected by PVL, both at the occipital radiation and at the more anterior part of the parietal lobe (Banker and Larroche 1962, DeReuck et al. 1972, Shuman and Selednik 1980). Abnormalities here may cause visual problems in diplegic children. Cortical blindness may be a rare complication and was not seen in our subjects. Diplegic children have been known to have perceptual and visuomotor impairment (Abercrombie et al. 1964). The peritrigonal lesions, especially in the parietal lobe, may play some role in this impairment.
Among the M R I findings, ventricular dilatation and white matter reduction reflected t.he severity of motor disability, but not of mental impairment in the diplegic children. Ventricular size, indi- cated by the distance of the anterior horns, was larger than that of normal children (Fukuyama et al. 1979). Ventricu- lar dilatation did not prove to be a useful indicator of severity, for only in the most severely disabled children (group 4) was it significantly greater than in those of group 1.
Otherwise, the amount of cerebral white matter is a useful index reflecting severity of motor developmental dis- ability, as shown previously in our CT study (Yokochi et al. 1989). In the present study, the reduction of white matter was classified into three groups (Figs. 1 ~ - D ) , slightly modifying our CT- study.
Flodmark et al. (1989) described the MRI findings of PVL and divided them into three grades: mild radiological involvement, more severe radiological involvement and almost complete absence of white matter. In our study, Figure I B represents milder changes than their mild radiological involvement, and c and D correspond to their mild and more severe radiological involvement, respectively. As the reduction in white matter extends anteriorly from the trigone, motor developmental disability is more severe.
m m - m 2 5 s 9
Children who have not only high-intensity areas on T2-weighted images, but also 23

d
d *
1 ‘CI
m
c, .- 3 C
cd cl
.- .-a - B u 2 2 n n
.- d
.C
.- V
2 n *
v)
c, .- 3
LI 0
z E:
24
reduction in amount of white matter adjacent to the body of the lateral ventricle are more severely disabled. After 18 months, when myelination in the centrum semiovale is essentially complete, the reduction in amount of cerebral white matter can be identified (Holland el al. 1986, Barkovich el al. 1988, Dietrich el al. 1988) and severity of motor disability predicted.
Of our subjects, two term infants had no abnormal MRI findings. The correlation between amount of periventricular white matter and severity of motor disability in the diplegic children may hold true for most of those who are preterm infants. However, term infants with spastic diplegia ma): have some destructive or dysplastic lesions other than PVL. The lesions in term infants with normal MRI
SUMMARY
may be similar to those in genetically inherited diplegia or paraplegia (McKusick 1988); the pathogenesis of spastic diplegia in term infants remains to be studied further.
Accepted for publication 26th July 1990.
Authors’ Appointments *Kenji Yokochi, M.D.; Kumi Aiba, M.D.; Department of Pediatric Neurology; Masayo Horie, M.D.; Kazuhisa Inukai, M.D.; Department of Pediatrics; Seirei-Hamamatsu General Hospital, Mikatabara 3453, Hamamatsu, Shizuoka 433, Japan. Shinji Fujimoto, M.D., Department of Pediatrics, Nagoya City Medical School, Nagoya, Aichi, Japan. Mariko Kodama, M.D.; Kazuo Kodama, M.D.; Department of Pediatrics, National Rehabilitation Center for Disabled Children, Tokyo, Japan.
*Correspondence to first author.
Magnetic resonance imaging (MRI) findings for 34 children with spastic diplegia, examined between two and 10 years of age, were analysed. Dilatation of the trigone, atrophy of the peritrigonal white matter and prominent deep cortical sulci were seen. On T2-weighted images, periventricular high- intensity areas in the white matter adjacent to the trigones and bodies of the lateral ventricles were seen in many children. These MRI features may reflect the pathological changes of periventricular leukomalacia in children with spastic diplegia. Among the MRI findings, only the amount of white matter correlated with severity of disability: white matter reduction corresponded to the more severe motor disabilities.
RESUME Imagerie de resonance magnetique chez les enfants presentant une diplegie spastique: correlation avec la graviti des anomalies mentales et motrices Les donnees de I’imagerie de resonance magnktique (I.R.M.) chez 3 4 enfants atteints de diplkgie spastique, examines entre deux et dix ans d’sge, ont ete analysees. La dilatation du trigone, I’atrophie de la substance blanche peritrigonale et des sillons corticaux saillants et profonds ont ete observees. Sur les images de valeur T2, des aires periventricularies a forte densite dans la substance blanche voisine des trigones et des noyaux des ventricules lateraux ont CtC observees chez de nombreux enfants. Ces donntes I.R.M. peuvent traduire les modifications pathologiques de la leucomalacie pkriventriculaire chez les enfants atteints de diplegie spastique. Parmi les donnkes I.R.M., seule la quantite de substance blanche etait correlee avec la gravite des incapacites: une reduction de la substance blanche correspondait aux plus graves des incapacites.
ZUSAMMENFASSUNG MRI bei Kindern rnit spastischer Diplegie: Gibt es eine Korrelation zur Schwere der motorischen und geistigen Behinderung? Von 34 Kindern mit spastischer Diplegie, die mit zwei bis 10 Jahren untersucht worden waren, wurden die MRI Befunde analysiert. Man fand Trigonurndilatation, Atrophie der peritrigonalen weiljen Substanz und sehr tiefe kortikale Sulci. Auf den T2-weighted images fanden sich bei vielen Kindern periventrikulare Verdichtungszonen in der weiljen Substanz, angrenzend an die Trigoni und die Seitenventrikel. Diese MRI Befunde spiegeln vielleicht die pathologischen Veranderungen der periventrikularen Leukomalazie bei Kindern mit spastischer Diplegie wider. Von den MRI Befunden korrelierte nur die Starke der weiRen Substanz mit der Schwere der Behinderung: eine Verminderung der weiRen Substanz korrespondierte mit schweren motorischen Behinderungen.
RESUMEN Imagen de Resonancia Magnetica en nifios con diplejia espastica: correlacidn con la gravedad de la anomalia motora y mental Se analizaron 10s hallazgos de las Imagenes por Resonancia Magnetica (IRM) en 34 niflos con diplegia espastica examinados entre dos y 10 aflos de edad. Se observaron dilataciones del trigono, atrofia de la substancia blanca peritrigonal y unos surcos corticales muy rnarcados. En las imAgenes T2, en muchos niflos se observaron areas periventriculares de aka densidad en la substancia blanca adyacente a 10s trigonos y a 10s cuerpos de 10s ventriculos cerebrales. Estas caracteristicas de las

IRM pueden reflejar 10s cambios patologicos d e una leucomalacia periventricular en niflos con diplejia espastica. Entre 10s hallazgos d e la IRM, solo la cantidad d e substancia blanca estaba en correlacion con la gravedad de la discapacidad: la reduccion en la substancia blanca correspondla a unas alteraciones motoras mas graves.
References Abercrombie, M. L. J . , Gardiner, P . A., Hansen,
E., Jonckheere, J . , London, R. L., Solomon, G., Tyson, M. C. (1964) ‘Visual, perceptual and visuomotor impairment in physically handicapped children.’ Perceptual and Motor Skills, 18,
Armstrong, D., Norman, M. G. (1974) ‘Periven- tricular leucomalacia in neonates: complications and sequelae.’ Archives of Disease in Childhood,
Baker, L. L., Stevenson, D. K., Enzmann, D. R. (1988) ‘End-stage periventricular leukomalacia: MR evaluation.’ Radiology, 168, 809-815.
Banker, B. Q., Larroche, J. C. (1962) ‘Periven- tricular leukomalacia of infancy: a form of neonatal anoxic encephalopathy.’ Archives of Neurology, 7, 386-410.
Barkovich, A. J., Kjos, B. O., Jackson, D. E., Norman, D. (1988) ‘Normal maturation of the neonatal and infant brain: MR imaging at 1 .5 T.’ Radiology, 166, 173-180.
Bennett, F. C., Chandler, L. S., Robinson, N. M., Sells, C. J . (1981) ‘Spastic diplegia in premature infants: etiologic and diagnostic considerations.’ American Journal of Diseases of Children, 135,
Daniels, D. L., Haughton, V. M., Naidich, T. P. (1987) Cranial and Spinal Magnetic Resonance Imaging. An Atlas and Guide. New York: Raven Press.
DeReuck, J., Chattha, A. S., Richardson, E. P., Jr. (1972) ‘Pathogenesis and evolution of periven- tricular leucomalacia in infancy.’ Archives of Neurology, 27, 229-236.
De Vries, L. S., Connell, J. A., Dubowitz, L. M. S., Oozeer, R. C., Dubowitz, V., Pennock, J. M. (1987) ‘Neurological, electrophysiological and MRI abnormalities in infants with extensive cystic leucomalacia.’ Neuropediatrics, 18, 61-66.
Dubowitz, L. M. S., Pennock, J . M., Bydder, G. M. (1989) ‘Extensive cystic leucomalacia: correlation of cranial ultrasound, magnetic resonance imaging and clinical findings in sequential studies.’ Clinical Radiology, 40,
Dietrich, R. B., Bradley, W. G., Zaragoza, E. J., Otto, R. J., Taira, R. K., Wilson, G. H. , Kangarloo, H. (1988) ‘MR evaluation of early myelination patterns in normal and develop- mentally delayed infants.’ American Journal of Roentgenology, 150, 889-896.
DiPietro, M. A., Brody, B. A., Teele, R. L. (1986) ‘Peritrigonal echogenic “blush” on cranial sonography: pathologic correlates.’ American Journal of Neuroradiology, 7, 305-3 10.
Dubowitz, L. M. S., Bydder, G. M., Mushin, J . (1985) ‘Developmental sequence of periventricular leukomalacia: correlation of ultrasound, clinical, and nuclear magnetic resonance functions.’ Archives of Disease in Childhood, 60, 349-355.
Fawer, C. L., Calame, A., Perentes, E. , Anderegg, A. (1985) ‘Periventricular leukomalacia: a corre- lation study between real-time ultrasound and autopsy findings. Periventricular leukomalacia in the neonate.’ Neuroradiology, 27, 292-300.
561-625.
49, 367-375.
732-737.
-
1 58- 166.
Flodmark, O., Roland, E. H., Hill, A., Whitfield, M. F. (1987) ‘Periventricular leukomalacia: radiologic diagnosis.’ Radiology, 162, 119-124.
Lupton, B., Li, D., Stimac, G. K., Roland, E. H., Hill, A, , Whitfield, M. F., Norman, M. G. (1989) ‘MR imaging of periventricular leuko- malacia in childhood.’ American Journal of Roentgenology, 152, 583-590.
Fukuyama, Y., Miyao, M., Ishizu, T., Maruyama, H. (1979) ‘Developmental changes in norma! cranial measurements by computed tomography. Developmental Medicine and Child Neurology, 21, 425-432.
Graziani, L. J . , Pasto, M., Stanley, C . , Pidcock, F., Desai, H.. Desai, S., Branca, P. , Goldberg, B. (1986) ‘Neonatal neurosonographic correlates of cerebral palsy in preterm infants.’ Pediatrics, 78,
Guzzetta, F., Shackelford, 0 . D., Volpe, S., Perlman, J. M., Volpe, J. J . (1986) ‘Periven- ricular intraparenchymal echodensities in the premature newborn: critical determinant of neurologic outcome.’ Pediatrics, 78, 995-1006.
Holland, B. A., Haas, D. K., Norman, D., Brant- Zawadzki, M., Newton, T. H. (1986) ‘MRI of normal brain maturation.’ American Journal of Neuroradiology, 7, 201-208.
McArdle, C. B., Richardson, C. J . , Hayden, C. K., Nicholas, D. A., Amparo, E. G. (1987) ‘Abnormalities of the neonatal brain: MR imaging. Part 11: Hypoxic-ischemic brain injury.’ Radiology, 163, 395-403.
McKusick, V. A. (1988) Mendelian Inheritance in Man. 8th Edn. Baltimore: Johns Hopkins University Press.
Nowell, M. A., Grossman, R. I . , Hackney, D. B., Zimmerman, R. A, , Goldberg, H. I . , Bilaniuk, L. T. (1988) ‘MR imaging of white matter disease in children.’ American Journal of Roentgenology, 151, 359-365.
Shuman, R. M., Selednik, L. J. (1980) ‘Periven- tricular leukomalacia. A one-year autopsy study.’ Archives of Neurology, 37, 231-235.
Takashima, S., Tanaka, K. (1978) ‘Development of cerebrovascular architecture and its relationship to periventricular leukomalacia.’ Archives of Neurology, 35, 11-16.
Van de Bor, M., Guit, G. L., Schreuder, A. M., Wondergem, J . , Vielvoye, J . (1989) ‘Early detection of delayed myelination in preterm infants.’ Pediatrics, 84, 407-41 1.
Veelken, N., Hagberg, B., Hagberg, G., Olow, I . (1983) ‘Diplegic cerebral palsy in Swedish term and preterm children: differences in reduced optimality, relations to neurology and patho- genetic factors.’ Neuropediatrics, 14, 20-28.
Wilson, D. A., Steiner, R. E. (1986) ‘Periventricular leukomalacia: evaluation with MR imaging.’ Radiology, 160, 507-5 11.
Yokochi, K . , Horie, M., Inukai, K., Kito, H., Shimabukuro, S., Kodama, K. (1989) ‘Computed tomographic findings in children with spastic diplegia: correlation with the severity of their motor abnormality.’ Brain and Development, 11, 23 6-240.
-
88-95.
m N
“0 m m
25