madurai medical journal march 2011
DESCRIPTION
Madurai Medical Journal is being published by Meenakshi Mission Hospital and Research Centre, Madurai as monthly journalTRANSCRIPT

MADURAI MEDICAL JOURNALISSN. No. 0972-3056 RNI. No. 55383/92
Off ic ia l Journal of IMA Madurai Meenakshi Branch
Price 5.00MMJ
Volume - 20 March 2011 Monthly Issue Issue - 3
(Run by S.R. Trust)
Lake Area, Melur Road, Madurai - 625 107
MMJ REACHING OVER 8500 DOCTORS
www.meenakshimission.org

CME IMA Madurai Meenakshi Branch World Kidney Day
CME Organized by IMA Madurai Meenakshi Branchon 2-3-2011
Dr. Andrew Xavier,Interventional Neurologist, USAStroke Interventions
Speaker : Topic :
World Kidney Day, March 10th 2011 organised by Dept. of
Nephro logy of Meenakshi Mission Hospital and Researc h
Centre, Madurai. Sr. Consultant Nephrologist,
released the Mr. Karmegamani
Managing Director of Solamalai Motors received the first copy.
Dr. K. Sampathkumar,Educational CD on Kidney Disease.
CME - Dindigul CME - Sivagangai
CME Organized by Dindigul Socitey of Obs & Gyanec on 25-02-2011
Jr. Consultant, MMHRC, MaduraiWhat is infertility?
How to proceed in a case of infertility?
Speaker :
Topic :
Dr. K. Thirumagal
CME Organized by IMA Sivagangai Branch andIMA Madurai Meenakshi Branch on 26-02-2011
Paediatric Haematologist & Oncologist, MMHRC, Madurai
Childhood Cancer - early diagnosis and recent advances
Speaker :
Topic :
Dr. S. Jayabose
CME & Unity Meet - Nagercoil
CME Organized by the Joint Action Committee forgrievances of Doctors of Kanyakumari Dist. on 19-03-2011
Sr. Consultant Interventional Cardiologist MMHRC, Madurai
The Recent trends in the management of hypertension
Speaker :
Topic :
Dr. S. Selvamani DNB.(GM), DNB. (Cardio),
Dr. Vinay Agarwal National IMA President, IMA HQRS,
New Delhi & Dr. S. Arul Rhaj, Chairman Common Wealth
Professional Alliance, UK were honoured in the unity meet
at Nagercoil

MaduraiM e d i c a lJ o u r n a lEDITORIAL BOARD
PATRONS
Dr. N. Sethuraman, M.S., M.Ch.(Uro), MNAMS.(Uro), FICS.FOUNDER CHAIRMAN
Dr. S. Gurushankar, M.B.B.S., M.B.A.VICE CHAIRMAN
ADVISORS
Prof. Dr. V.N. Rajasekaran, Ph.D., M.D., DTM&HMEDICAL DIRECTOR
Prof. Dr. N. KrishnamurthyM.S., M.Ch.(Uro), D.H.&HM. BGL, M. Phil(Tamil), M.A(Phi&Rel) PGDIM., PGDHRM.ACADEMIC DIRECTOR
Dr. T.R. Murali, M.S., M.Ch.(Uro),CHAIRMAN ACADEMIC
EDITOR IN CHIEF
Dr. S. Kumar, M.D. (Anaes), D.Diab., (PGHSc).,CONSULTANT CARDIAC ANAESTHESIOLOGIST
MEMBERS
Dr. Ramesh Ardhanari, M.S., M.Ch.(GE), FRCS. (Glasgow)
Dr. K. Sampath Kumar, M.D., DNB., DM.(Nephro)
Dr. A.R. Raghuram, M.S., M.Ch.(CTS), D.N.B., FIACS.
Dr. S. Jayabose, M.B.B.S., D.C.H., A.B(Paed)., A.B(Paed. Hematology - Oncology).,
Dr. P. Krishnamoorthi, M.D., FIAMS., FCGP.,
Dr. T. Mukuntharajan, M.B.B.S., DMRD.
Dr. N. Panchavarnam, M.S., M.Ch. (Plastic)
Dr. S. Lakshmi, M.D., D.A.
Dr. N. Maharajan, M.D., DA.
Dr. K.S. Anand, M.D. (Anaes)
Dr. V. Sathya Narayana, M.S., D.Ortho., DNB
Dr. S. Balasubramanian, M.S.(Ortho),
Dr. S. Padma, M.D., DNB. (OG),
Dr. R. Sivakumar, M.D., DNB.(Cardio)
Dr. S. Selvamani, DNB. (GM), DNB. (Cardio),
Dr. M. Sampthkumar, M.D., DM. (Cardio),
Dr. N. Karunakaran, M.B.B.S., DMRD., DNB.(Radiology),
Dr. K.S. Kirushnakumar, M.D.(RT),
Dr. A. Kannan, M.D. (Paed)
Dr. K. Selva Muthu Kumaran, M.Ch.(Neuro)
Dr. M.S. Senthilnathan, M.D. (Nuc.Med)
Dr. Narendra Nath Jena, M.B.B.S., DFM., PG. Diab., FAEM.
Dr. R. Vijaya Bhaskar, M.S., M.Ch. (Surg. Onco)
Co-ordination & Compilation
Mr. V.M. Pandiarajan, Sr.Manager - Marketing
Mr. R. Saravanan, M.Sc., M.B.A., PGDFRM.,
Mr. P. Madhusudhanan, B.A., PGDHM.,PGDCA., M.B.A., PGDFRM.,
Mr. S. Balaji, M.Com., M.B.A.,
Editorial Address
Meenakshi Mission Hospital and Research Centre(Run by S.R. Trust)
Lake Area, Melur Road, Madurai - 625 107
Tamilnadu, INDIA
Phone : 0452 - 2588741 - 750, 4263000
Fax : 0452 - 2586353
E-mail : [email protected]
Website : http://www.meenakshimission.org
From theEditor’s Desk
About 30% of all deaths worldwide and 10% of all healthy life lost to disease are accounted for Cardio Vascular Disease (CVD) alone. Although there has been some decline in mortality from CVD in developed countries, no such decline has been reported in developing countries, ethnic and socially disadvantaged minority populations or in people with accompanying chronic kidney disease (CKD). Cardiovascular disease is frequently associated with CKD, which is important because individuals with CKD are more likely to die of cardiovascular causes than develop kidney failure. The National Kidney Foundation Task Force issued a report which showed that there was a high prevalence of CVD in chronic kidney disease and that mortality due to cardiovascular disease was 10 to 30 times higher in dialysis patients than in the general population.Diabetes is a major risk factor for chronic kidney disease. Kidney Disease occurs in about one third of people with either type 1 or type 2 diabetes. This is approximately 60 million people worldwide. CVD, diabetes and CKD account for a majority of burden of disease in the world. These three diseases often occur together and share risk factors, such as physical inactivity, smoking, overweight and obesity, and high blood pressure. Renal disease also engenders an environment that promotes cardiovascular injury in ways that are more or less specific to chronic kidney disease. Calcium and phosphorous dysregulation with vascular calcification, anemia, and hyperhomocysteinemia are among the often-cited cardiovascular liabilities of chronic kidney disease.Biomarkers of CKD (proteinuria, eGFR) are easy and relatively inexpensive to detect, and one of these, proteinuria, emerges early in the evolution of generalized vascular disease. Hence, there is an immediate need to stress the importance of early identification and treatment of CKD and its associated comorbid conditions for reduction of unfavourable CVD outcomes. It is now known that albuminuria is a better predictor of renal and cardiovascular events than blood pressure alone, that reducing proteinuria is more renal and cardio protective than lowering blood pressure alone and that identification of CKD can improve CV outcomes. Routine evaluation of patients with CVD or those at high risk for CVD should include measurement of spot urine albumin-to-creatinine ratio or total protein-to-creatinine ratio and estimation of GFR by serum creatinine and prediction equations.World Kidney Day was celebrated on March 11th.The theme for this year was ‘Protect the kidney and Save the heart’. In 2011, World Kidney Day called for attention to the large, and often unappreciated, role played by kidney dysfunction in increasing premature cardiovascular disease, the most common cause of morbidity and mortality worldwide. Celebration of World Kidney Day 2011 will remind and reinforce the message that kidney disease is indeed common, harmful and treatable and that protecting your kidneys is an important health strategy that may save your heart.
Dr. S. KumarEditor in Chief – MMJ, Sr. Consultant Cardiac AnaesthesiologistMobile : 94422 44084, E-mail : [email protected] Classic Printers, 27 Kakathope Street, Madurai - 625 001
& 0452 - 2323819, 2624466, 4381603
Protect the kidney and Save the heart!
Madurai Medical Journal March 20112
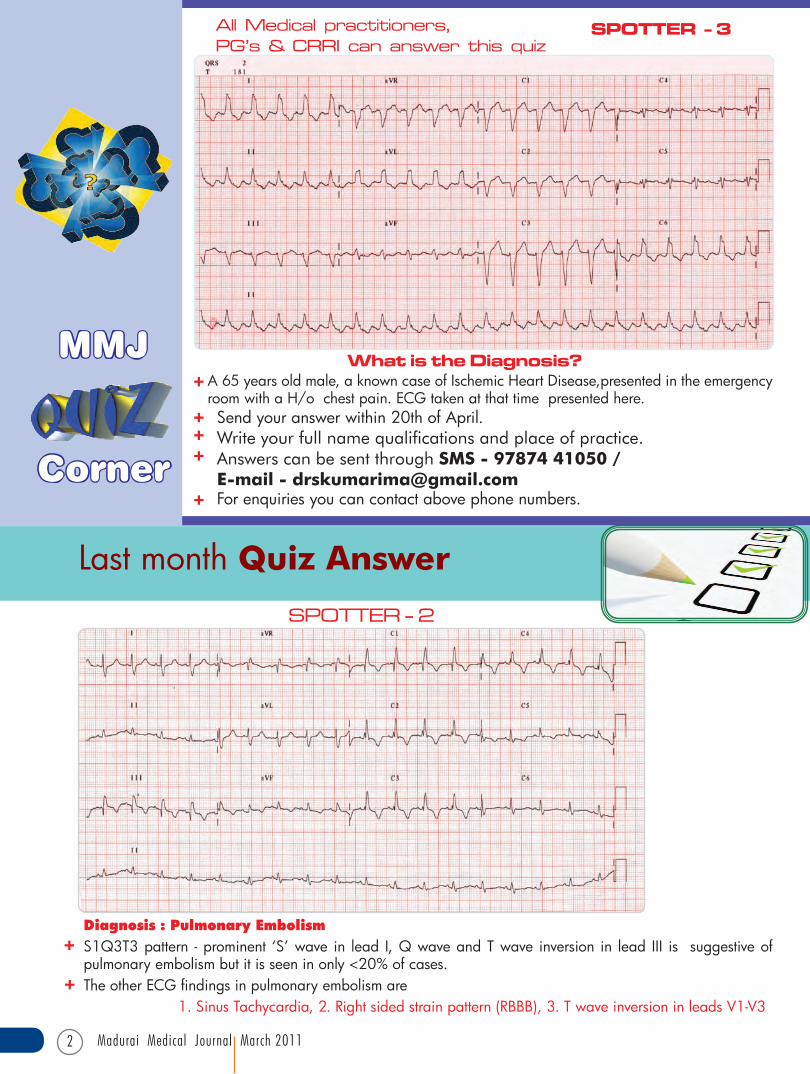
A 65 years old male, a known case of Ischemic Heart Disease,presented in the emergency room with a H/o chest pain. ECG taken at that time presented here.
What is the Diagnosis?
All Medical practitioners,PG’s & CRRI can answer this quiz
SPOTTER - 3
MMJ
Corner
Send your answer within 20th of April.Write your full name qualifications and place of practice.Answers can be sent through SMS - 97874 41050 /E-mail - [email protected] enquiries you can contact above phone numbers.
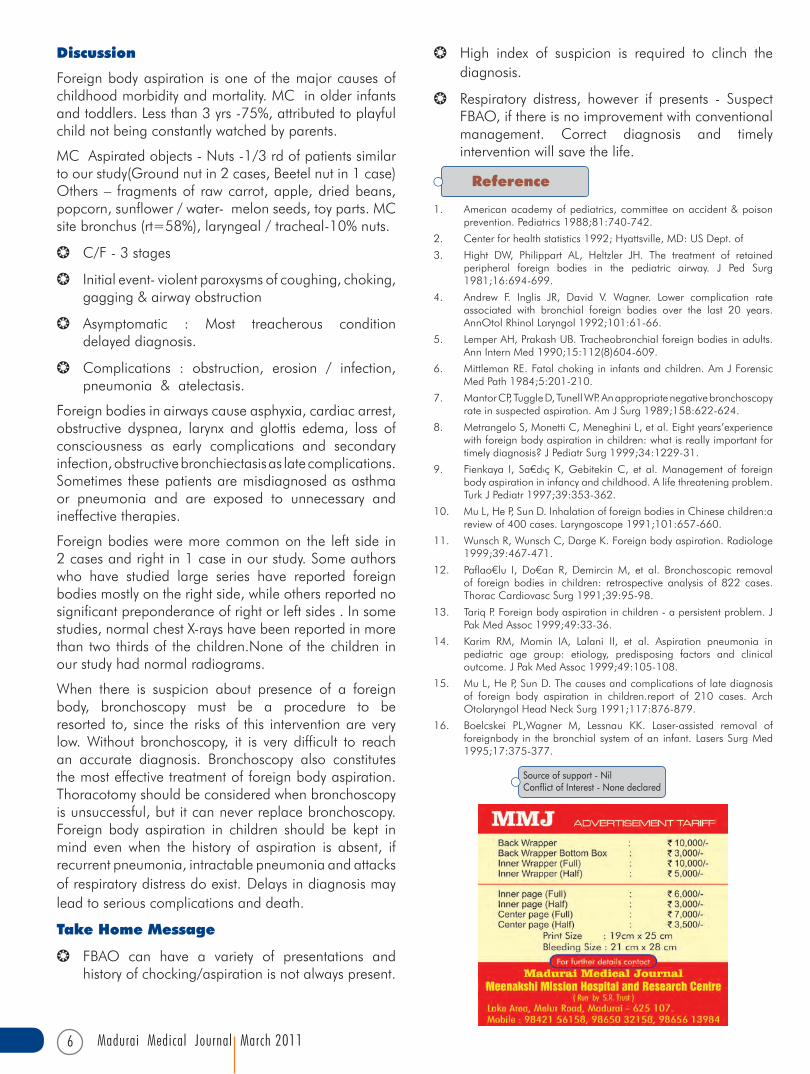
Diagnosis : Pulmonary EmbolismS1Q3T3 pattern - prominent ‘S’ wave in lead I, Q wave and T wave inversion in lead III is suggestive of pulmonary embolism but it is seen in only <20% of cases.The other ECG findings in pulmonary embolism are 1. Sinus Tachycardia, 2. Right sided strain pattern (RBBB), 3. T wave inversion in leads V1-V3
Last month Quiz Answer
SPOTTER - 2

Madurai Medical Journal March 2011 3
Contents Page No.
MMJ Quiz Corner ...................................................................................................................................................................................................................................................................... 2
Foreign Body Airway obstruction (FBAO) - Various Presentations - A Review Article ....................................................................................... 4Dr. Vaijananth Dugganikar, Dr. A. Kannan & Dr. N. Edwin
Cervical Cancer Screeing - Current Status - A Brief Communication ..................................................................................................................................... 7Dr. S. Padma
Vertebral column resection - for correction of kyphotic deformity - A Case Report ........................................................................................... 8Dr. S. Balasubramanian
Pituitary disorders in postpartum - A Brief review and case report on Lymphocytic hypophysitis ................................................. 12Dr. R. Subasree, Dr. M. Rajaguru, Dr. T.C. Vijayanand & Dr. N. Karunakaran
PUO with Renal Failure - Unusual Diagnosis - A Case Report ....................................................................................................................................................... 15Dr. A. Prabhakar & Dr. K. Sampathkumar
Post Graduates Corner ....................................................................................................................................................................................................................................................... 18Dr. Krishna Kumar Rathnam
Doctor’s Diary .............................................................................................................................................................................................................................................................................. 20
MMHRC Congratulates the following Doctors whocorrectly answered the last month quiz (Spotter - 2)
Bangalore
Dr. Jumana Afrin
Chennai
Dr. Ahmed Ashar Ali
Dr. S. Vinoth Kanna
Coimbatore
Dr. K. Arun
Dindigul
Dr. Halilur Rahman (Vedasandur)
Dr. Ubaidur Rahman
Dr. P. Vivekanandan (Kodaikanal)
Kanyakumari
Dr. S. Selvakumar (Agastheeswaram)
Madurai
Dr. Andrew Rajiv
Dr. C. Ramesh
Dr. K.R. Santharam
Dr. S.M. Shankar Rajan
MMHRC
Dr. Amuthanilavan
Pudukottai
Dr. M. Periyasamy
Sivagangai
Dr. P. Senkathir (Devakottai)
Tanjore
Dr. Chandra Joseph
Dr. David Baskar
Dr. S. Jayabal (Peravoorani)
Thiruvarur
Dr. M. Chandrasekar
Trichy
Dr. Jayasree (Lalgudi)
Dr. Ramesh (Lalgudi)
Tuticorin
Dr. M. Dhanuskodi
Virudhunagar
Dr. Kesavan (Sattur)
Dr. D. Thiyagarajan (Alangulam)

Madurai Medical Journal March 20114
AbstractForeign body aspiration in the respiratory tract can be encountered at all ages but more frequently in childhood. It is one of the leading causes of accidental death among children under the age 5 years of age. Foreign body aspiration may cause sudden death in some cases or may lead to chronic lung problems. These patients are frequently misdiagnosed and treated for pneumonia or asthma.We had series of 3 cases who were presented with various signs and symptoms of respiratory tract infections. HRCT was the investigation of choice. Bronchoscopy is diagnostic and thereupetic procedure of choice in identifying the foreign body and all the three patients were discharged in stable condition.Key wordsForeign body, aspiration, childhood, bronchopneumonia, asthma.
Corresponding Author
Dr. Vaijanath Dugganikar M.B.B.S., DNB.,
Paediatric Resident, Department of Paediatric & Neonatology
Meenakshi Mission Hospital and Research Centre, Madurai - 625 107 Phone : 0452 2588741, Mobile : 99409 33963E-mail : [email protected]
Foreign Body Airway obstruction (FBAO) –Various Presentations
Case no. 1
1yr 6 months old boy referred to MMHRC as a case of LRI (?Bronchiolitis ) with h/o cough since 2weeks, breathing difficulty since 1 day, received in emergency dept. with cardiorespiratory arrest, revived; intubated and connected to mechanical ventilation. O/E boy was tachypneic, dyspneic, decreased air entry on left side. Other systems were normal. O/I he was anaemic (HB:8gm%), Total counts were elevated (TC:18,000cells/mm3)
Chest X- ray
- A Review Article
1st X-ray
2nd X-ray
HRCT chest:foreign body in left main stem bronhus
Dr.A. Kannan M.D. (Paed),Sr. Consultant
Department of Paediatric & Neonatology, MMHRC
Dr.N. Edwin M.D. (Paed), Professor
Department of Paediatric & Neonatology, MMHRC
Dr.Vaijanath Dugganikar M.B.B.S., DNB.,Paediatric Resident
Department of Paediatric & Neonatology, MMHRC

Madurai Medical Journal March 2011 5
Foreign Body (BEETEL NUT) in left main stem Bronchus with pus collection removed through Flexible Bronchoscopy
Case no. 2
2yrs old boy referred as a case of LRI (?Bronchopneumonia,? Hypereactive airway disease) with h/o cough and breathing difficulty since 15 days, fever since 15 days, treated outside with IV antibiotics. O/E boy was febrile, tachycardic, dyspneic, air entry diminished on the left side. Other systems were normal.
Chest X-ray showed hyperinflation of both lung fields
HRCT Chest showed foreign body in left main stem bronchus
Bronchoscopy removal of Foreign body (Ground nut) from left main stem bronchus.
Case no. 3
1 yr 6months old boy referred to MMHRC as a case of ASTHMA with h/o fever, cough and cold since 11 days, breathing difficulty since 5days.H/o swelling over the neck since 1 day (sudden onset, gradually spread to chest and abdomen). Boy was treated with IV antibiotics and nebulisation for 5 days. O/E Febrile,subcutaneous emphysema over the neck,chest and abdomen +, respiratory distress+, tachpnea+, tachycardia+, air entry decreased on the right side+, crepitations and wheezes +. Other systems were normal.
HRCT Chest showed foreign body in the right main stem bronchus
Bronchoscopic removal of foreign body(Ground nut) from right main stem bronchus
Child developed pneumothorax following bronchoscopy, ICD tube placed.
Madurai Medical Journal March 20116
Reference
Source of support - NilConflict of Interest - None declared
1. American academy of pediatrics, committee on accident & poison prevention. Pediatrics 1988;81:740-742.
2. Center for health statistics 1992; Hyattsville, MD: US Dept. of
3. Hight DW, Philippart AL, Heltzler JH. The treatment of retained peripheral foreign bodies in the pediatric airway. J Ped Surg 1981;16:694-699.
4. Andrew F. Inglis JR, David V. Wagner. Lower complication rate associated with bronchial foreign bodies over the last 20 years. AnnOtol Rhinol Laryngol 1992;101:61-66.
5. Lemper AH, Prakash UB. Tracheobronchial foreign bodies in adults. Ann Intern Med 1990;15:112(8)604-609.
6. Mittleman RE. Fatal choking in infants and children. Am J Forensic Med Path 1984;5:201-210.
7. Mantor CP, Tuggle D, Tunell WP. An appropriate negative bronchoscopy rate in suspected aspiration. Am J Surg 1989;158:622-624.
8. Metrangelo S, Monetti C, Meneghini L, et al. Eight years’experience with foreign body aspiration in children: what is really important for timely diagnosis? J Pediatr Surg 1999;34:1229-31.
9. Fienkaya I, Sa¤d›ç K,GebitekinC, et al.Management of foreignbody aspiration in infancy and childhood. A life threatening problem. Turk J Pediatr 1997;39:353-362.
10. Mu L, He P, Sun D. Inhalation of foreign bodies in Chinese children:a review of 400 cases. Laryngoscope 1991;101:657-660.
11. Wunsch R, Wunsch C, Darge K. Foreign body aspiration. Radiologe 1999;39:467-471.
12. Paflao¤lu I, Do¤an R, DemircinM, et al. Bronchoscopic removalof foreign bodies in children: retrospective analysis of 822 cases. Thorac Cardiovasc Surg 1991;39:95-98.
13. Tariq P. Foreign body aspiration in children - a persistent problem. J Pak Med Assoc 1999;49:33-36.
14. Karim RM, Momin IA, Lalani II, et al. Aspiration pneumonia in pediatric age group: etiology, predisposing factors and clinical outcome. J Pak Med Assoc 1999;49:105-108.
15. Mu L, He P, Sun D. The causes and complications of late diagnosis of foreign body aspiration in children.report of 210 cases. Arch Otolaryngol Head Neck Surg 1991;117:876-879.
16. Boelcskei PL,Wagner M, Lessnau KK. Laser-assisted removal of foreignbody in the bronchial system of an infant. Lasers Surg Med 1995;17:375-377.
Discussion
Foreign body aspiration is one of the major causes of childhood morbidity and mortality. MC in older infants and toddlers. Less than 3 yrs -75%, attributed to playful child not being constantly watched by parents.
MC Aspirated objects - Nuts -1/3 rd of patients similar to our study(Ground nut in 2 cases, Beetel nut in 1 case) Others – fragments of raw carrot, apple, dried beans, popcorn, sunflower / water- melon seeds, toy parts. MC site bronchus (rt=58%), laryngeal / tracheal-10% nuts.
b C/F - 3 stages
b Initial event- violent paroxysms of coughing, choking, gagging & airway obstruction
b Asymptomatic : Most treacherous condition delayed diagnosis.
b Complications : obstruction, erosion / infection, pneumonia & atelectasis.
Foreign bodies in airways cause asphyxia, cardiac arrest, obstructive dyspnea, larynx and glottis edema, loss of consciousness as early complications and secondary infection, obstructive bronchiectasis as late complications. Sometimes these patients are misdiagnosed as asthma or pneumonia and are exposed to unnecessary and ineffective therapies.
Foreign bodies were more common on the left side in 2 cases and right in 1 case in our study. Some authors who have studied large series have reported foreign bodies mostly on the right side, while others reported no significant preponderance of right or left sides . In some studies, normal chest X-rays have been reported in more than two thirds of the children.None of the children in our study had normal radiograms.
When there is suspicion about presence of a foreign body, bronchoscopy must be a procedure to be resorted to, since the risks of this intervention are very low. Without bronchoscopy, it is very difficult to reach an accurate diagnosis. Bronchoscopy also constitutes the most effective treatment of foreign body aspiration. Thoracotomy should be considered when bronchoscopy is unsuccessful, but it can never replace bronchoscopy. Foreign body aspiration in children should be kept in mind even when the history of aspiration is absent, if recurrent pneumonia, intractable pneumonia and attacks of respiratory distress do exist. Delays in diagnosis may lead to serious complications and death.
Take Home Message
b FBAO can have a variety of presentations and history of chocking/aspiration is not always present.
b High index of suspicion is required to clinch the diagnosis.
b Respiratory distress, however if presents - Suspect FBAO, if there is no improvement with conventional management. Correct diagnosis and timely intervention will save the life.

Madurai Medical Journal March 2011 7
Cervical Cancer Screening – Current status
Corresponding Author Dr. S. Padma M.D., DNB. (O&G)Sr. Consultant & Head - Dept. of Obst & Gynaec
Meenakshi Mission Hospital and Research Centre, Madurai - 625 107 Phone : 0452 2588741, Mobile : 94430 22046
When should screening be stopped?ACS recommends discontinuing screening1. altogether in women who have undergone, Total
hysterectomy for benign indications (CIN 2,3 is not considered a benign indication )
2. in women older than 70yrs with well documented negative screening histories (i.e at least 3 consecutive satisfactory negative Pap tests in the past 10yrs )
Conventional Vs liquid based cytology While with the conventional Pap smear “ cervical cells “ are transferred directly to a glass slide and fixed, with the liquid based technology, cells scraped from the cervix are suspended in a liquid transport medium and in the laboratory, a thin layer of cells is displayed on a glass slide The liquid based Pap test is marketed as a more sensitive screening test than the conventional smear. In addition, it offers the option of performing reflex HPV-DNA testing for some patients with a Pap report of ASC-US(Atypical squamous cells of uncertain significance)However a RCT conducted at Italy showed that the liquid Pap test resulted in a higher false positive rates, leading to more unnecessary colposcopic examinations without diagnosing more high grade dysplasia or cancerHPV -DNA testing Studies from around the world have been published comparing screening with cytology alone versus. HPV DNA testing alone or HPV in combination with cytology. Compared with cytology alone, HPV DNA testing is more sensitive, less specific and a higher negative predictive value. The combined cytology plus DNA HPV testing has the highest sensitivity, lowest specificity and highest negative predictive value.Currently, in the US, HPV DNA, testing is FDA approved for screening only when used in conjunction with cytology. The American Cancer Society (ACS) and the ACOG have approved this combination as appropriate for use in women aged 30 and older. These professional organizations and the ASCCP (American Society of colposocpy and cervical pathology ) recommend that it screening results on cytology and HPV DNA testing are negative the interval for the next screening should be≥3years.(Tobecontinued)
Pap test is the foundation of cervical cancer screening in the developed countries . The regimen of repeated cytologic screenings, follow up of abnormal results using colposcopy and biopsy, and treatment or continued close follow up has resulted in a dramatic decline in the incidence of and mortality from cervical cancer over the past 50yrs When should a woman begin cervical screening ?The ACOG (American College of Obs & Gyn) and the ACS (American Cancer society) recommend waiting about 3yrs after initiation of sexual activity or age 21 before performing a Pap test. This recommendation is based on the low rate of cancer in this age group, despite high acquisition of HPV infection The causative role of high risk types of HPV (Human Papilloma Virus) in the development of CIN 2,3 and cancer cervix is well established. Most HPV infections are transient with median duration of 6 to 8 months. 70% revert to negative within 12months and 80% within 24months, only the persistence of HPV infection especially of the high risk types leads to CIN 2,3 and invasive cancers.How often to screen with PAP TEST ?ACS and ACOG guidelines recommend a decade of intensive screening once a young women has had her initial Pap test - i.e annual examination until age 30, if conventional Pap smear is used or alternate years until age 30 if liquid based cytology is used (ACS recommendation)After age 30 , a woman who has had 3 consecutive satisfactory negative Pap tests, screening may be done once in 2-3 years
Dr. S. Padma M.D., DNB. (O&G)Sr. Consultant & Head - Dept. of Obst & Gynaec
MMHRC
- A Brief Communication

Madurai Medical Journal March 20118
Case details
This 29 year old male patient came with the complaints of inability to sit, stand or walk comfortably for the past six months. He had a history of fall from a two wheeler following which he developed pain in the thoraco-lumbar junction. There was no neurological deficit initially. He consulted an orthopaedic surgeon who after taking a radiograph diagnosed it as a ‘stable’ wedge compression fracture of twelfth thoracic vertebra. He was advised conservative management in the form of bracing.
(In fact the radiograph actually revealed a ‘Tri-column injury’. Apart from anterior and middle column injury there was also ligamentous disruption posteriorly (posterior column injury) which was seen as a widened interspinous space between D11 and D12).
With the brace treatment the patient’s pain did not come down. The patient also noticed progressively worsening bony prominence (angular kyphosis) at the thoraco-lumbar junction. He also developed a painful callosity over the prominence.
Corresponding Author
Dr. S. Balasubramanian M.S. (Ortho)
Sr. Consultant & Chief Spine Surgeon
Meenakshi Mission Hospital and Research Centre, Madurai - 625 107 Phone : 0452 2588741, Mobile : 98431 49953E-mail : [email protected]
“Vertebral column resection” - For correction of kyphotic deformity - A Case Report
AbstractUnderestimation of sagittal imbalance of the spine (kyphosis) following injury can lead to long lasting morbidity. Kyphosis associated with internal gibbus with spinal cord compression leads to major morbidity. Early recognition and aggressive corrective surgery holds the key to successful outcome. ‘Vertebral column resection’ is one of the most extreme forms of spine surgery which helps to accomplish the goal of ‘Deformity correction, decompression of the spinal cord and a stable painless spine’ at a single go. In this case ‘complete excision of D12 vertebrae, deformity (kyphosis) correction, spinal cord decompression and spinal column reconstruction’ has been done.Key wordsKyphotic deformity, vertebral column resection, spinal deformity correction, unstable thoraco-lumbar fracture.
Dr. S. Balasubramanian MS., (Ortho)Sr. Consultant & Chief Spine Surgeon
MMHRC
The patient decided to go for alternate medicine and he took treatment from a masseur. After the vigorous massaging sessions, he developed ulceration of the callosity over the bony prominence. He also developed gradual weakness of both lower limbs. Now he could not sit without support on either side with his hand. He could not stand without support and started walking by holding the wall for support. He was comfortable only on side lying. He also had hesitancy in passing urine.
On examination he was having upper motor neuron signs in both the lower limbs. His anal tone was preserved. He could not sit, stand or walk without support. A tender angular Kyphosis was present at the thoraco-lumbar junction.
In short
• Thepatienthadsufferedan‘unstable’threecolumninjury of the spine which was initially overlooked.
• Duetotheneglectatthefirstinstancehedevelopedprogressive collapse leading on to severe Kyphosis at the thoraco-lumbar junction.
• ill advised massage therapy further worsened theproblem by adding neurological deficit to the scenario.
By the time the patient came to our care attention the bone (D12) had healed in severe kyphosis. There was a huge bony protrusion into the canal (internal gibbus) stretching and compressing the spinal cord at that level. (Fig 1 & 2).

Madurai Medical Journal March 2011 9
Problems
• Rigid Severe Kyphosis at D12 (Kyphosis angle of450). The normal thoraco-lumbar Kyphosis angle is zero degrees.
• Ahugeinternalgibbus,duetothebucklinginoftheposterior column of the vertebra into the spinal canal compressing and stretching the spinal cord.
• Presence of neurological deficit with the patientunable to do his daily activity.
Procedure
PLAN : “Vertebral column resection” at D12 level, followed by anterior column reconstruction + Deformity correction + Stabilization + Fusion.
The patient was positioned prone after general anaesthesia. After routine posterior midline approach, pedicle screws were inserted two levels above (D10, D11) and two levels below (L1, L2) (Fig).
Fig 1a: Lateral radiograph showing complete wedge collapse of D12 with a kyphosis angle of 450
Fig 1b: Antero-posterior radiograph
showing no coronal plane deformity.
Fig2a: MRI T2WI showing D12 collapse with huge internal gibbus compressing and stretching the spinal cord.
Fig 2b: Axial section T2WI showing gross intrusion
of the gibbus with severe narrowing of the spinal
canal with flattening of the spinal cord.
Fig3: Following posterior exposure of the spine, pedicle screw fixation was done at D10, D11, L1 and L2.
The spinous process of D11, D12 and L1 were excised and later used as bone graft. Total laminectomy of D12 was done with the help of high speed burr. There were extensive adhesions on the under surface of D12 lamina which were released tediously.
Next bilateral twelfth ribs were excised for a distance. The dissection continued along the sides of the D12 vertebral body. The segmental vessels are ligated. The Aorta is identified and dissected away from the D12 vertebral body. Retractors were placed on either side of the D12 vertebra. This isolates the D12 vertebra from the great vessels (Fig 4a,b).
Head
Fig 4a: Posterior elements of D12 have been completely removed with a burr. The exposed dura is covered with a cotton patty. Bilateral lateral dissections done, Aorta and IVC isolated and protected with retractors (arrows).
Fig 4b: Schematic representation of isolation of D12 vertebra from great vessels.
Head

Madurai Medical Journal March 201110
The discs between D11--D12 and D12 –L1 are excised from both sides. Temporary stabilization was achieved on one side to prevent sudden slipping and collapse of the gap. The D12 vertebral body is removed from either side. The bone excised is used for bone grafting later. The internal gibbus is left undisturbed till the end. The anterior longitudinal ligament is excised. This is essential to allow for the Kyphosis correction and to regain the vertebral body height.
Fig 5c: After correction of the kyphosis deformity, the vertebral body is reconstructed with Harm’s type cage (arrow) filled with bone graft. You can appreciate the wrinkling (*) on the posterior surface of the dural sac, which occurred as a result of controlled shortening following correction of kyphosis.
Fig 5b: The suction tube (arrows) is passed underneath the spinal cord (****) from right to the left side to demonstrate the completeness of the vertebral column resection.
Fig 5a: After complete vertebral body excision and removal of internal gibbus, the spinal cord (****) is free on all sides. The vertebral column is now divided into two halves at this level. Only the rod stabilization on the right side is holding the spinal column from collapse at this stage.
The internal gibbus is thinned out using high speed burr. Finally internal gibbus is removed without disturbing the dura (Fig5a,b). This step is very crucial.
A lamina spreader is inserted from one side to jack open the collapsed space of D12 vertebra. A proper sized titanium Harm’s type cage filled with harvested bone graft is inserted under direct vision (Fig 5c). This will take the place of the excised D12 vertebral body anteriorly. Properly contoured rods are inserted on to the pedicle screws on either side and tightened after exerting compression forces. Bone graft pieces are inserted to achieve fusion from D10 to L2 (Fig 6a,b).
Fig 6a: Post operative lateral radiograph showing the correction. The preoperative pathological 45o kyphosis angle is corrected to the normal zero degrees as shown by the parallel red lines.
Fig 6b: Post-operative AP radiograph.
Post operatively, the patient regained good muscle power and bladder control. The patient was given a brace and allowed to walk independently.
Discussion
Underestimation of three column injury of the thoraco-lumbar junctional (TL Jn) injuries can lead to progressive worsening of deformity and development of late neurological sequelae. The posterior column injury can disguise itself as simple widening of the interspinous space or facetal subluxation which could be missed by the untrained eyes. With the conventional routine radiographs, the posterior elements are often overexposed and hence not clearly visible. Unless we look for it specifically, we are likely to miss it. This leads to underestimation of the severity of the injury. The TLICS
Head****
D12 nerve root (Lt)
Head****
Head *

Madurai Medical Journal March 2011 11
scoring system can help to determine the necessity of the need for surgery.
Brace treatment for suitable thoraco-lumbar injuries are advisable only if the patient understands the shortcomings of the method and the importance of strictly adhering to the doctor’s advice. If the patient takes the treatment lightly, there is a high likelihood of worsening of vertebral collapse and attendant complications. It is important to counsel the patient regarding the proper and continued wearing of prescribed braces till further advice is given.
Though massage therapy has a role in some simple soft tissue injuries of the spine, unscientific usage of it in spinal fracture is likely to worsen the problem especially if given prior to adequate healing of the fractures. Patients should be warned about the dangers of massage treatment in the setting of spinal fracture.
Importance of kyphosis
Spinal deformity can occur either in the coronal plane (scoliosis) or in the sagittal plane (Kyphosis). Orthopaedicians are very well aware about the scoliosis deformity. However scant respect is given for the Kyphosis deformity. The normal acceptable Kyphosis angle is very well defined in the literature. Pathologically increased Kyphosis at any spinal level will lead to increased muscular effort to maintain the spine erect. This leads to easy fatigability and unrelenting back pain. This will lead to decreased ability to carry out the ADL.
The TL Jn is the most common site for spinal injury. Most of the spinal injuries at TL Jn lead to increased kyphosis at that level (regional kyphosis).
At the thoraco-lumbar junction (D12-L1), the normal Kyphosis angle is zero degrees. In this case, the patient developed severe rigid kyphosis (450) at D12 level with internal gibbus with neurological deficit.
The goal of surgery is to achieve ‘decompression of the spinal cord, deformity correction and a stable painless spine’. In order to achieve this ‘Vertebral column resection’ of D12 through posterior approach was planned.
Vertebral column resection
A vertebral column resection (VCR) refers to completely resecting one or more vertebral segments. At a minimum, this means the posterior elements, pedicles, and the entire vertebral body with the discs above and below are to be removed. This is followed by reconstruction of both the posterior and the anterior column.
Fig: 7a Fig: 7b Fig: 7c
Conclusion• Itisimportanttoidentifytheunstablespinalinjuryat
the outset. Appropriate measures at this stage are easier.
• Kyphoticdeformityproducesmorespinalpainthanscoliosis.
• Various osteotomies are available to correctKyphotic deformity. Among these, the vertebral column resection (VCR) is the most powerful and the most difficult to do. VCR is followed by deformity correction and reconstruction of anterior and posterior column at a single go, through the posterior approach.
• The morbidity following this technique is muchless compared to double approaches (posterior + anterior). The patient’s rehabilitation proceeds faster as a result of this reduced morbidity.
Among the various spinal osteotomies available, Vertebral column resection is the most powerful tool in terms of deformity correction. However it is to be noted that it is the most difficult of all.
In VCR the spinal column is virtually split into two halves. This is followed by reconstruction of the anterior column using a titanium Harm’s cage filled with bone graft. Compression is applied through the pedicle screws over the rods to correct the kyphosis (Fig 7a,b,c). Throughout this procedure the spinal cord should be protected.
Reference
Source of support - NilConflict of Interest - None declared
1. Zhongqiang Chen, M.D., Yan Zeng, M.D., Weishi Li, M.D., Zhaoqing Guo, M.D., Qiang Qi, M.D., and Chuiguo Sun, M.D.Apical segmental resection osteotomy with dual axial rotation corrective technique for severe focal kyphosis of the thoracolumbar spine. J Neurosurg Spine 14: 106-113, 2011
2. Ian G. Dorward, M.D., and Lawrence G. Lenke, M.D: Osteotomies in the posterior-only treatment of complex adult spinal deformity: a comparative review. Neurosurgery focus 28(3):E4, 2010
3. ROBERT F. HEARY, M.D., AND CHRISTOPHER M. BONO, M.D: Pedicle subtraction osteotomy in the treatment of chronic, posttraumatic kyphotic deformity. J Neurosurg Spine 5:1-8, 2006

Madurai Medical Journal March 201112
Pituitary disorders in postpartum - A Brief reviewand case report on Lymphocytic hypophysitis
Corresponding Author Dr. R. Subasree M.B.B.S., DM. (Neuro),Consultant, Dept. of Neurology
Meenakshi Mission Hospital and Research Centre, Madurai - 625 107 Phone : 0452 2588741, Mobile : 77089 36399E-mail : [email protected]
and adequate symptomatic and supportive measures-antiedema measures, heparin, anti epileptics, antibiotics and inotropic supports were given.
Patient was evaluated with a provisional diagnosis of postpartal CVT versus pituitary apoplexy. Her CT brain showed enlarged pituitary with homogenous enhancement including the stalk. The sella was widened.No contrast enhancement of sphenoid or sella. There was no evidence of haemorrhage / necrosis or pituitary rim sign. The size of pituitary in comparison to the one done outside prior to delivery, inview of headache and vomiting revealed increase in size with enhancement.
During stay, she was found to have one episode of hypoglycemia. She had hypokalemia and hypocalcemia. Her thyroid functions, Growth hormone, FSH(2.45 mIU/ml), LH(2.21mIU/ml) serum cortisol (5.10 IU evening)were normal. Prolactin levels were low (16.9) for her postpartal period. She was given injection hydrocortisone 100mg iv 8 hrly after which patient sensorium improved dramatically. She became conscious and had no focal deficits. Her cardiac status was normal. USG abdomen showed evidence of medical renal disorder.
She also was found to have persistent hypokalemia, hypocalcemia, hypophosphataemia, hypomagnesaemia.Assosciated Renal tubular dysfunction was considered.Parathormone levels were high(107.7pg/ml)and ALP was 240 IU/l. Uric acid levels, bicarbonate,chloride were normal. She also had dyslipidaemia-low HDL,elevated TG and hypoalbuminaemia. Urine protein was 3+. Her ESR was high 75mm. Her vasculitic work up showed that RA factor, Antinuclear antibody were negative.
Case Summary
22 year young lady G2P2L2A0 presented to our Emergency department on day 9 postpartal day with two episodes of seizures followed by altered sensorium, hypotension and shock. She had moderate to severe holocranial headache, recurrent vomiting, fatigue in the preceeding one month prior to delivery. No history of vision loss or field defects.She had anaemia with Hb of 5.6gm%, received 2 pints blood transfusion elsewhere.There was oligohydramnios, mobile head at term and past history of LSCS. She had amniotic fluid index,AFI of 4.Hence patient underwent LSCS 10 days prior to EDD. There was no history of PIH/APH/PPH. There was no history of recurrent venous or arterial thrombosis.She did not have repeated abortions or pregnancy loss. She had not started lactating and the healthy male child born was fed by artificial feeds. There was preceeding history of skin pigmentation over trunk and extremities with multiple large joint pains for past 2 yrs. No history of photosensitivity, rashes, oral ulcers, purpuras.
At presentation, she was in deep altered sensorium, eye opening to pain, groaning to pain, minimally moving limbs to pain and had dilated sluggish reacting pupil on left side. She was intubated and connected to ventilator
Abstract22 year young pospartal lady presented with hypotension, shock, altered mentation, dilated pupil. Evaluation revealed a enlarged enhancing pituitary gland along with the stalk. Approach to pituitary disorders in postpartal period and a brief review on lymphocytic hypophysitis is discussed.Key wordsPostpartum, Hypopituitarism, Lymphocytic hypophysitis, Sheehan necrosis, steroids.
Dr. R. Subasree M.B.B.S., DM. (Neuro)Consultant
Dept. of Neurology, MMHRC
Dr. T.C. Vijay Anand M.D., DNB. (Neuro)Consultant
Dept. of Neurology, MMHRC
Dr. N. Karunakaran M.B.B.S., DMRD., DNB., (Radiology)
ConsultantDept. of Imaging Sciences, MMHRC
Dr. M. Rajaguru M.D., DM. (Neuro)Sr. Consultant
Dept. of Neurology, MMHRC

Madurai Medical Journal March 2011 13
Her serum, urine osmolarity were normal. Urine spot potassium and spot sodium were normal. Liver functions and Renal functions were normal. HIV, Anti HCV, HbsAg were negative. Coagulation profile was normal.
In view of acute hypopituitarism in postpartal period with assosciated autoimmune dysfunction, hypoprolactinaemia and enlarged enhancing pituitary gland and stalk lymphocytic hyphophysitis is the most likely diagnosis in our patient. Patient gradually showed clinical improvement.
Discussion
Pituitary Disorders in Postpartal period.
Anatomic changes in the pituitary in normal pregnancy
Magnetic resonance imaging (MRI) scans performed during pregnancy demonstrate a gradual increase in maternal pituitary volume over the course of gestation, with an increased final weight (660-760 mg), as well as a volume increase of 30% above the pregestational volume. This enlargement makes the gland reach 12 mm in height a few days postpartum. The pituitary gland achieves its maximum size during the first 3 days of the puerperium in preparation for lactation The pituitary stalk remains unchanged. The posterior pituitary, which is normally visualized as an intense, T1-weighted signal on MRI scans (the so-called pituitary bright spot) is not visualized in the third trimester. These changes usually regress after delivery.
Diverse pathologic conditions affect the central nervous system (CNS)and pituitary gland during pregnancy and the puerperium. Some are specific to the physiologic process of reproduction (eg, eclampsia, postpartum cerebral angiopathy, Sheehan syndrome, lymphocytic adenohypophysitis). Even when imaging changes are nonspecific, knowledge of those entities associated with pregnancy and awareness of the increased likelihood of certain diseases in pregnancy will allow a more informed differential diagnosis.
There is an increased chance of pituitary hemorrhage, infarction, and accelerated prolactinoma growth during the course of pregnancy and the puerperium
Pituitary Apoplexy
Pituitary apoplexy is defined as acute hemorrhagic infarction in an existing pituitary adenoma or otherwise physiologically enlarging pituitary gland. (Fig. 1) Clinically, the patient may present with severe headache, vomiting and visual disturbances including visual field defects and restricted eye movements. Patients may also develop dizziness or altered mental status, thought to be the result of hemodynamic instability presumably due to acute hypopituitarism.
Fig 1 Pituitary apoplexy Sagittal T1-weighted MR image shows Hemorrhage in a prominent pituitary gland
Sheehan Syndrome
Sheehan syndrome is a clinical state of panhypopituitarism due to pituitary infarction that occurs after an obstetrically related hypotensive episode around the time of delivery. Pituitary infarction in the setting of an obstetric hemorrhage should be suspected if hypotension and tachycardia persist after adequate initial treatment of the inciting event. Additional early signs of hypopituitarism may include hypoglycemia and failure of lactation.
Owing to a deficiency of pituitary hormones, patients may subsequently present with chronic fatigue, dizziness, postural hypotension, cold intolerance, hypopigmentation, myxedema, loss of pubic and axillary hair, decreased libido, breast atrophy, and amenorrhea. At imaging, there is usually the appearance of a partial or complete empty sella(Fig 2)
Fig2 Sagittal gadolinium-enhanced T1-weighted MR image shows an empty sella with herniation of the optic chiasma into the sella turcica.
Lymphocytic Adenohypophysitis (LHy)
Lymphocytic adenohypophysitis is a rare inflammatory disorder of the anterior lobe of the pituitary gland that may affect young women in the peripartum. It is associated with other autoimmune diseases such as Hashimoto thyroiditis, pernicious anemia, and type I diabetes mellitus.
The classic presentation of LHy is peripartum hypopituitarism, often with a pituitary mass and visual

Madurai Medical Journal March 201114
failure. The predominant feature appears to be headache out of proportion to the size of the pituitary. Adrenal insufficiency seems to be a common feature, which, if not recognized, can be fatal in as many as 25% of patients. The term lymphocytic infundibuloneurohypophysitis was coined for patients with DI and lymphocytic infiltration of the pituitary stalk (ie, “stalkitis”).
Differentiation from adenoma
Lymphocytic adenohypophysitis results most often in early failure of adrenocorticotropic hormone and thyroid-stimulating hormone, whereas nonfunctioning adenoma causes early failure of growth hormone and gonadotropins A history of infertility is common in patients with adenomas, while nearly all patients with LHy achieve spontaneous pregnancy.Headaches and visual changes are much more common in the LHy group.Postpartum hypoprolactinemia (level less than 150 ng/mL) is seen in the majority of patients with lymphocytic adenohypophysitis.
Plain X-ray films may show reactive sellar bony sclerosis from the inflammatory process. Pituitary adenomas typically have a contrast-enhancing or hypointense area confined to, or compressing, the adjacent normal gland. The picture of LHy is quite different, with the gland appearing diffusely and dramatically enhanced with suprasellar extension in 60%–80%. Also, the presence of a thickened and contrast-enhanced infundibular stalk is nearly pathognomonic of the condition (Fig. 3,4). This enhancement may be homogenous or heterogeneous. Parasellar structures, such as dura mater, sphenoid, and cavernous sinuses, may also enhance in LHy. After recovery, there is regression of the pituitary gland to normal or small size, resulting in the appearance of a partial or total empty sella. Although recovery may occur spontaneously, steroids have been advocated as the main line of treatment.
Figure 3a and b showing enlarged enhancing pituitary in our reported patient
Importantly, a high index of suspicion is necessary to diagnose LHy when only the protean signs of mild headache and malaise are present. This is important, because at least 9 deaths are documented in the literature, most due to a delayed diagnosis of pituitary insufficiency. Patients with LHy need careful endocrinologic follow-up to avoid complications.
The literature is unclear on the correct treatment modality. Visual improvement following decompression via the transsphenoidal route has been reported. Many patients have only headache and radiologic evidence of LHy. Multiple reports exist of these patients improving with glucocorticoid administration alone. Investigators report successful results with dosing in the range of 60 mg of prednisone per day for a period of 1 month to a year, followed by a gradual tapering, with concurrent monitoring for relapse of symptoms.
Acknowledgement
Dr. R. Ganesh, Jr. Consultant, Dept. of Imaging Sciences, MMHRC
Figure 4 a and b Sagittal and Coronal images showing enlarged enhancing pituitary gland with infundibular stalk in our patient.Height of pituitary was 19mm.
Reference
1) Antonio Bellastella, Antonio Bizzarro, Concetta Coronella et al. Lymphocytic hypophysitis: a rare or underestimated disease?European Journal of Endocrinology 2003; 149 :363–376
2) Dineen R, Banks A, Lenthalla R .Imaging of acute neurological conditions in pregnancy and the purperium. Clinical Radiology 2005; 60: 1156–1170
3) Hashimoto K, Takao T, Makino S. Lymphocytic adenohypophysitis and lymphocytic infundibuloneurohypophysitis. Endocr J. 1997; 44(1):1-10.
4) Powrie JK, Powell M, Ayers AB et al. Lymphocytic adenohypophysitis: Magnetic resonance imaging features of two new cases and a review of the literature. Clin Endo 1995;42:315-322.
5) Zak I.T, Dulai H.S, Kish K.K et al.Imaging of Neurologic Disorders Associated with Pregnancy and the Postpartum Period.RadioGraphics 2007; 27:95–108
Source of support - NilConflict of Interest - None declared

Madurai Medical Journal March 2011 15
Abstract13 Years old male admitted with pyrexia of unknown origin with renal failure. Hemodialysis was done without improvement in general condition. Renal biopsy showed focal proliferative glomerulonephritis with interstitial nephritis. All routine microbiological and parasitic investigations were negative. Scrub Typhus was considered in the differential diagnosis and weil felix test was done. It was strongly positive. He was treated with doxycycline. Dramatic all round improvement was noted, the next day.Key wordsPUO, Renal failure, Scrub typhus, Immunohistochemistry, Doxycycline.
Corresponding Author
Dr. K. Sampathkumar M.D., DNB., D.M. (Nephro)
Sr. Consultant & Head, Dept. of Nephrology
Meenakshi Mission Hospital and Research Centre, Madurai - 625 107 Phone : 0452 2588741, Mobile : 99948 72250E-mail : [email protected]
PUO with Renal Failure –Unusual Diagnosis
IntroductionRickettsial illnesses are rarely diagnosed with certainty in our country. Although the presence of spotted fevers and scrub typhus, vector borne illnesses with high mortality, was documented from Tamil Nadu in southern India a few years ago, there are little community based data available from this or any other state in India. Lack of access to reliable testing methods for hospitals functioning at a community level is the main reason. The specific ‘gold standard’ test, microimmunofluorescence test is not available in India. Availability of tests based on ELISA principles is also limited. Therefore, at present, Weil Felix test which utilises antigens prepared from Proteus spp remains the only laboratory test available to investigate these infections occurring in communities in India. Based on hospital data, it was evident that this infection is likely to be prevalent in many parts of TamilNadu. Consideration of Rickettsial illness in the differential diagnosis is crucial for its ultimate diagnosis as exemplified in this case.Case reportA 13 year old boy was admitted to our hospital with a diagnosis of “PUO with Acute Renal failure”. He
- A Case Report
Dr. A. Prabhakar M.D., DNB.,
ResidentDepartment of Nephrology, MMHRC
Dr. K. Sampathkumar M.D., DNB., D.M. (Nephro)Sr. Consultant & Head
Department of Nephrology, MMHRC
complained of fever, nausea,weakness and headache for 20 days duration. Fever was of sudden onset, continuous with chills and rigor, spiking for one to two hours and decreasing with profuse sweating. This boy had been treated at a peripheral hospital with antibiotics and antipyretics without relief before being referred here.
There was no history of vomiting, cough, expectoration, dysuria, neck rigidity, any other drug intake or rashes. On examination the boy looked ill, temperature was 102.9°F, pulse 120/min and BP 100/60 mm of Hg. There was pallor, no icterus,no cyanosis,no clubbing. Liver was palpable 1 cm below the right costal margin, tender on deep palpation with a smooth surface. The spleen was palpable 2cm below the left costal margin and there was no evidence of free fluid in the abdomen. Other systems were normal. The boy was diagnosed as a case of malaria, treated with artesunate inj, injection cefepime and IV fluids. Investigations are given in the Table-1.
H
H Doxycycline was started

Madurai Medical Journal March 201116
Next day , his condition deteriorated with tachypnoea of 40/min, temperature 104°F, pulse 126/min and blood pressure 90/50mm of Hg. Oliguric acute renal failure was managed by hemodialysis. The blood cultures were sterile. Bedside ultrasound showed hepatosplenomegaly with splenic enlargement of 14 cm and minimal free fluid in the right pleural cavity. The patient’s urine output had decreased and urine was dark coloured. BT, CT and prothrombin time were normal. Platelet count was low. Virological studies and leptospirosis were negative. Blood investigations were suggested. Tumor lysis syndrome and hence bonemarrow aspiration was performed to rule out Acute Leukemia. It showed normal cell lineage. The patient had developed multi-organ failure. Renal biopsy was performed. The Weil Felix test was found to be positive with OX K 1:160 and a diagnosis of Scrub Typhus was made. No eschar or skin rash could be found even in concealed areas such as groin and axilla. Renal Biopsy: Focal proliferative glomerulonephritis with interstitial nephritis.
Fig. 1 - Tubule shows RBC cast.
Fig. 2 - Glomerulus shows mesangial proliferation.
Doxycycline was started at a dose of 100 mg twice a day. Dramatic all round improvement was noted, the next day. He was taken off dialysis in a couple of days and was discharged 5 days later. One month later on follow up he was found to be in normal health.
Discussion
Of the diseases caused by Rickettsia in man, the most widespread is Scrub Typhus. It appears that the disease is active over a very wide area bound by Japan in the
east, through China, the Philippines, tropical Australia in the south and west through India, Pakistan, possibly to Tibet, Afghanistan, and southern parts of Russia in the north. During the decades 1970-90, Scrub Typhus was reported in many countries including China, Japan, India, Indonesia, Malaysia, Thailand and Vietnam. The percentage of positive findings in sera from the general population varied from 2% in India to 40% in Malaysia
Fever, headache, conjunctivitis, lymphadenopathy and a vesicular lesion at the site of bite by larval mite or ‘chiggers’ characterize a severe attack of the disease. The lesion turns into a punched out ulcer covered with a blackened scab (eschar). A macular rash may appear on the body by the 5th to 7th day and last for a few hours to days. It is difficult to perceive in dark skinned individuals. Complications such as pneumonitis, myocarditis, encephalitis and peripheral circulatory failure may occur. Weil Felix fluorescent antibody, complement fixation or microscopic agglutination tests can confirm the diagnosis. The incubation period ranges from 6 to 21 days and averages 12 days. There is no person to person spread hence isolation is not required. On WF test, the highest titers to OXK (1: > 320) were reached by 8 days and titers of IgG had risen after 14 days of onset of symptoms, on MIF.
At present, scrub typhus is rarely diagnosed because of its nonspecific clinical presentation, because of a low index of suspicion and the lack of diagnostic facilities in India. In a study conducted in south India, the sensitivity for OX-K was 30% at a titer breakpoint of 1:80, but the specificity and positive predictive value were 100%.These infections respond well to antimicrobials like doxycycline and chloramphenicol. However, mortality can be high if untreated. The mortality rate in a tertiary care hospital, where patients from this state are referred when complications develop, was found to be about 15 percent.
The preventive measures include DBP application on clothing is the most important single preventive measure while preparing for combat or occupation of an uncontrolled area. Benzyl benzoate is also miticidal and can be utilized to impregnate clothing. Deet (Diethyltoluamide) or permethrin can be used as mite repellent. Deet-based repellents are effective on the skin, whereas permethrin based repellents are for use only on clothing.
However, the availability and the cost of other serological methods are major problems in India and because of current circumstances, it is suggested that the diagnosis of scrub typhus should be largely based on a high index of suspicion and careful clinical, laboratory

Madurai Medical Journal March 2011 17
Reference
Source of support - NilConflict of Interest - None declared
1. SK Mahakam, R Kashia, A Kanga, V Sharma, BS Rasher, LS Pal Relevance ofWeil-FelixTestinDiagnosisofScrubTyphusinIndia.JAPI•VOL.54•AUGUST 2006
2. Lt Col Pushcart Singh Scrub Typhus, a Case Report: Military and Regional Significance -MJAFI 2004; 60 : 89-90
3. Dong-Min Kim, 1 Dae Woong Kang, 1 Jong O Kim, 1 Jong Hoon Chung, 1 Hyun Lee K Acute Renal Failure due to Acute Tubular Necrosis caused by Direct Invasion of Orientia tsutsugamushi J. Clin. Microbiol. doi:10.1128/JCM.01040-07 JCM Accepts, published online ahead of print on 14 November 2007
4. K. Kamarasu, M. Malathi, V. Rajagopal, K. Subramani, D. Jagadeeshramasamy & Elizabeth Mathai Serological evidence for wide distribution of spotted fevers & typhus fever in Tamil Nadu - Indian J Med Res 126, August 2007, pp 128-130
and epidemiological evaluation. Use of empiric treatment should also be considered to reduce the high mortality observed with the disease. Though Weil-Felix agglutination test is not a very sensitive test it is a specific test when positive. ConclusionScrub Typhus should be considered in the differential diagnosis of PUO with renal and hepatic involvement.Treatment with Doxycycline produces prompt improvement.
Form IVStatement about ownership and other particulars
about Newspaper1. Place of Publication : Madurai2. Periodicity of its Publication : Monthly3. Printer’s Name : N. Jayakarthikeyan Nationality : Indian Address : Thee Classic Printers 27, Kakathope Street Madurai - 625 0014. Publisher’s Name : Dr. N. Sethuraman Nationality : Indian Address : Meenakshi Mission Hospital and Research Centre Lake Area, Melur Road Madurai - 625 1075. Editor’s Name : Dr. S. Kumar Nationality : Indian Address : Meenakshi Mission Hospital and Research Centre Lake Area, Melur Road Madurai - 625 1076. Name and addresses of individuals who own Newspaper and Partners of : Single Owner Shareholders holding more than one Percent of the total capitalI, Dr. N. Sethuraman, hereby declare that the particulars given above are true to the best of my knowledge and beliefDate : 01-03-2011 Dr. N. Sethuraman Publisher

Madurai Medical Journal March 201118
Dr. Krishna Kumar Rathnam M.D., (Med.), DM. (Med. Onco.),Consultant, Dept. of Medical Oncology
MMHRC
distant metastasis. On laparotomy she was found to have extensive locally infiltrating disease and small para aortic nodes and diffuse peritoneal nodularity probably metastasis. The patient was termed inoperable and was then referred to our Institute for considering palliative chemotherapy.
Routine examination revealed a soft 1 cm left supraclavicular lymph node, FNAC of which was positive, revealing the advanced nature of disease. She was initiated on palliative chemotherapy.
Case 3
56 year old smoker, was evaluated for hemoptysis and chest pain, CT chest revealed a suspicios mass lesion in the right lung. He underwent FNAC from the mass lesion (see picture 1), which was unremarkable and revealed few groups of degenerate cells. Following the procedure patients became progressively dyspnoeic and he was referred to our hospital for further management.
In last 2 editions , in PG corner, we saw some of the simple and correct ways of approaching diagnosis of haematological and gynaecological malignancies. In this edition we will discuss how a simple but careful examination of left supraclavicular lymph node can aid not only in easy diagnosis but also make a mammoth difference in management of common cancers. The discussion will be in the form of few case scenarios.
Case 1
A 39 year old lady was referred for treating lump in her left breast-infiltrating ductal carcinoma grade III ( T2N1 – clinical status ). All staging work up was negative. At first sight, this was a straight forward case of operable breast cancer, which would need adjuvant treatment based on the post op status.
However on careful examination, the left supraclavicular area appeared granular, with doubtful lymph node <1.0 cm. She underwent a left supraclavicular fat pad biopsy which revealed 3 nodes, 1 of which was positive for metastatic carcinoma. The plan was immediately revised. This case was defined as N3 status with INOPERABLE LOCALLY ADVANCED BREAST CANCER and needed neoadjuvant chemotherapy ± radiotherapy to left supraclavicular area prior to considering any mastectomy.
Case 2
56 year old lady was evaluated for a growth in the stomach, biopsy of which was a poorly differentiated adencarcinoma. Initial imaging did not reveal any
Corresponding Author
Dr. Krishna Kumar Rathnam MD.(Med.), DM.(Med. Onco.),Consultant, Medical Oncologist
Meenakshi Mission Hospital and Research Centre, Madurai - 625 107 Phone : 0452 2588741, Mobile : 93804 17299 E-mail : [email protected]
Post Graduates Corner“ Supraclavicular Lymph Node ” – the Gateway to cancer diagnosis
Pic 1 – Mass lesion in the right lung
Pic 2 – Right sided pneumothorax
DiscussionSupraclavicular lymph node belongs to the cervical group of lymph nodes, which drains the head and neck area, lung, deep axillary nodes and terminal drainage from most of the abdominal organs including pelvis also. Virchow’s node (or signal node) is a lymph node in the left supraclavicular fossa (the area above the left clavicle). It takes its supply from lymph vessels in the abdominal

Madurai Medical Journal March 2011 19
Reference
Source of support - NilConflict of Interest - None declared
1. Virchow R (1848). “Zur Diagnose der Krebse in Unterleibe”. Med. Reform. 45: 248.
2. Troisier CE (1889). “L’adénopathie sus-claviculaire dans les cancers de l’abdomen”. Arch. Gen. de Med. 1: 129–138 and 297–309.
3. Mizutani M, Nawata S, Hirai I, Murakami G, Kimura W (December 2005). “Anatomy and histology of Virchow’s node” . Anat Sci Int 80 (4): 193–8
Pic 3 – Lymphatic drainage of breast
cavity. The finding of an enlarged, hard node (also referred to as Troisier’s sign) has long been regarded as strongly indicative of the presence of cancer in the gastro intestinal tract, more specifically gastric cancer, that has spread through the lymph vessels. It is sometimes called the signal node or sentinel node for the same reason, although it is not directly related to the sentinel node procedure sometimes used in cancer surgery nor to the “sentinel gland” of the greater omentum. It is named after Rudolf Virchow (1821-1902), the German pathologist who first described the gland and its association with gastric cancer in 1848[1]. The French pathologist Charles Emile Troisier noted in 1889 that other abdominal cancers, too, could spread to the node[2].Malignancies of the internal organs can reach an advanced stage before giving symptoms. One of the first visible spots where these tumors metastatise is the left supraclavicular lymph node, because it is on the left side of the neck where the the thoracic duct enters the venous circulation via the left subclavian vein. The metastasis blocks the thoracic duct leading to regurgitation into the surrounding nodes ie. virchow’s node. Another concept is that one of the supraclavicular nodes corresponds to the end node along the thoracic duct and hence the enlargement[3].Picking up an involved supraclavicular lymph node is helpful to the clinician in many ways. It aids in easy diagnosis ( histopathology ).Its involvement can make a huge difference in management also.Let us discuss the above case scenarios one at a time, in which picking up involved supraclavicular lymph nodes would make major differences in management.Case 1 - DiscussionBreast has rich lymphatic drainage ( see picture - 3 ). Cancer of breast is notorious for lymph nodal spread, irrespective of it’s primary size. It is the biology of the disease (like tumor grade and receptor and Her 2 amplification status ) which decides the initial presentation of the disease. On clinical examination, one clue which post graduates can follow is to see 2 things – the size of primary tumor and Nodal status in the axilla. If the patient presents with a primary T4 status , or if she has a matted or fixed node in the axilla, one should be careful
in picking up a supraclavicular lymph node.In case of any doubt , one can subject the patient for a supraclavicular fat pad biopsy, which can then clearly pick up any occult involvement.The difference obviously would mean a lot to the patient. Upfront surgery is clearly not the ideal treatment option in this case and neoadjuvant treatment and reassessment for the supraclavicular node before proceeding with mastectomy, would be the way to go about.Case 2 - DiscussionCarcinoma stomach, as already termed in literature can be a very silent disease, till advance stages. Many times a CT scan abdomen does not reveal the locally advanced nature of the tumor or the small peritoneal disease. A proper clinical examination, especially for supraclavicular lymph node is a must on day 1, which can save a patient from unnecessary open and closure procedures.One other similar, but rare lymph nodal metastasis is the “ IRISH NODE ”, that is left anterior axillary lymph nodal metastasis in a case of cancer esophagus and gastric cancer, which may be clinically missed on routine clinical examination.Case 3 - DiscussionThe right lung and most of the left lower lobe drain into the right supraclavicular node and the rest finally into the left supraclavicular node. Inaccessible lung lesions pose a challenge to tissue diagnosis. For such a case, before posting for any invasive needle biopsy tests, careful examination of the neck nodes is a must. Many times a simple FNAC of a small supraclavicular lymph node can clinch the diagnosis and save the patient from an invasive needle biopsy or risk of pneumothorax.The differential diagnosis of enlarged supra clavicular lymph nodes could be either a primary nodal pathology like Tuberculous node or lymphoma. Other causes of secondary involvement from – lung, thyroid, breast, gastro intestinal tract and hepato biliary cancers, pelvis primary and genital cancers should be excluded.When a primary cancer is apparently very localised, rarely the left supraclavicular node could be enlarged due to a different co existing systemic problem like tuberculosis, in developing countries, which is one more reason for such nodes to be biopsied early on during treatment.

Madurai Medical Journal March 201120
( A Page to serve)Doctor’s Diaryoctor’s DiaryDContactThe EditorMadurai Medical JournalMeenakshi Mission Hospital and Research CentreLake Area, Melur Road, Madurai - 625 107
MMHRC Wishes the following Couple a Happy and Prosperous Wedded life
M. Sulthan Sheik Thamby B.E.,S/o. Dr. S. Mohamed Kaleel M.B.B.S., DCH.,
Devipattinam, Ramnad Dist.
withS.A. Howra B.Com.,
04-04-2011
WANTED
Sonologist • Salary negotiable
Contact
Managing DirectorsSivagami X-Rays & Scan Centre
Chinnamanur, Theni Dist. - 625 515Mobile : 98425 42000, 97888 55359
WANTEDFull time Orthopaedician
for 150 bedded Multispeciality Hospital in
Tirunelveli
Contact
Mobile : 93644 55003
ATTENTIONAre you changing your Clinic?Please send usyour new postal address withpincode to deliver MMJ regularly
ATTENTIONAre you changing your Clinic?Please send usyour new postal address withpincode to deliver MMJ regularly
by Editor

Dr. Krishnakumar Rathnam Consultant Medical Oncologist, MMHRC, Maduraiatt ended BREAST CANCER SPECIALISTS FORUM 2011, conducted atNottin gham Univers ity, Nottin gham, UK on March 10th and 11th 2011.Dr. John F Robertson, convener of the Breast cancer Forum.
At Australia presentation of "SINGLE STAGE AESTHETIC CORRECTION OF BILATERALCLEFT LIP" as a new innovation in "AUSTRALIAN CLEFT LIP AND PALATE ASSOCIATION
AND ASIAN PACIFIC CLEFT LIP" on March 2011, by HODPlastic Surgery, Project Director The Smile Train, MMHRC
Dr. N. Panchavarnam,
MMHRC Consultants in International Forum
Up Coming Event...
Regional Academy of Cardiovascular Intervention (RACI)Regional Academy of Cardiovascular Intervention (RACI)Dear Sir,
on Behalf of RACI you are cordially invited to attend the "Percutaneous Intervention 2011"on 30th April & 1st May 2011 at Madurai.
Venue : Hotel Sangam, Alagarkovil Road, Madurai
30-04-2011 : 6-00 p.m onwards Interesting Interventions - CDs presentation Endovascular Therapy for Aortic Aneurysm Rotablation - Practical Tips & TricksGala Dinner
01-05-2011 : 07-30 a.m 8-30 a.m Live Demonstration - Case 1 Lectures - Role of IVUS Role of FFR10-30 a.m Live Demonstration - Case 2 Lecture - Approach to CTO12-00 noon Inaugural address - Evolution of PCI01-00 p.m to 02-00 p.m 02-00 p.m Live Demonstration - Case 3 Lecture - BMV - Practical Tips & Tricks03-30 p.m Live Demonstration - Case 4 Lecture - PDA closure - Practical Tips & Tricks
Breakfast
Lunch
Organizing Committee, MaduraiFor Further Details :
90251 35271, 98421 58870, 98421 58868
Registration Free
Invited Deligates
Cardiologist &
Cardio Thoracic Surgeons
only

30-03-11MA 99 / 2010-2012
Printed by N. Jayakarthikeyan at Thee Classic Printers, 27, Kakathope Street, Madurai - 625 001 Phone : 0452 - 2624466, 2323819, 4381603E-mail : [email protected]
Postage paid in cash at Madurai HPO & Posted at Madurai BPC
(Run by S.R. Trust)
Lake Area, Melur Road, Madurai - 625 107
Free Corrective Operation for
Cleft Lip & Palate at MMHRC....
SurgeryMedicineAccommodationFood andTo & Fro ChargesFREE
We have performed5900 operations successfullyso far.....
For Cleft Lip and Palate below 40 years of age group of any category
Before Surgery After Surgery
This Programme organized by SMILE TRAIN (USA) & Meenakshi Mission Hospitaland Research Centre
TheThe TrainTrainSmileSmileChanging The World One Smile At A Time.Changing The World One Smile At A Time.The TrainSmileChanging The World One Smile At A Time.