macmhb boardworks 2.0 may 20, 2014 · macmhb boardworks 2.0 . may 20, 2014 . dave schneider, ceo ....
TRANSCRIPT

MACMHB Boardworks 2.0 May 20, 2014 Dave Schneider, CEO
Northern Michigan Regional Entity

What are Evidence Based Practices Background – How Did We Get Here Where, Exactly, Is “Here” Sustainability Questions
Intervention with a body of evidence: - rigorous research studies - specified target population - specified client outcomes
Specific implementation criteria A track record showing that the practice can be
implemented in different settings Role for Emerging Promising Practices Evidence-based practices are practices that
integrate best research evidence with clinical expertise and patient values (Institute of Medicine, 2001)
Evidence-based behavioral practice (EBBP) "entails making decisions about how to promote health or provide care by integrating the best available evidence with practitioner expertise and other resources, and with the characteristics, state, needs, values and preferences of those who will be affected
Source: Wikipedia - The Free Encyclopedia

Overall this shift toward the use and development of EBPs in behavioral health services is moving in a positive direction. However, many of these EBPs are tested in urban areas, and are not easily adapted to rural areas without losing key components of the tested practice.
Due to the difficulty of developing and evaluating EBPs, the term, “promising practice,” has been used to refer to behavioral health practices that do not yet have the evidence-base to be considered EBPs, but which appear to be effective based on a less stringent definition of research evidence or preliminary and/or simple data evaluation.
The term, “best practice,” is used to refer to a practice which is generally thought to be effective based upon anecdotal evidence, but for which objective data is lacking.
Rural Behavioral Health Programs and Promising Practices, June 2011, DHHS, HRSA

Practices for which scientific evidence is building
Ongoing research to validate their effectiveness
Address a widely held client need or gap in
service system
Practices for which the research base is currently limited or inconclusive with regard to effectiveness
Approaches that consumers and families
request and find helpful
Common concerns regarding EBP and why they should not be concerns: ◦ EBP is not “person-centered” ◦ Focus should be on outcomes, without defining
how to achieve the outcomes ◦ Innovation is stifled ◦ EBP is not recovery-oriented and may in fact
conflict with a recovery orientation

Links research findings to patient care Links consensus treatment guidelines to
patient care Emphasizes measurable outcomes Encourages the use of science to refine and
advance clinical treatment Sets the stage for a process of continually
and systematically evaluating effectiveness.

Blind application of treatment recommended by researchers
“Cook book care” Ivory tower care Just another name for what clinicians have
been doing all along

Provides a solid foundation from which to help a consumer
More likely to get the results you want Provides evidence of effectiveness Tying treatment to outcome assessment
allows for more informed clinical judgment and clinical decision-making
Much more rewarding experience for both consumer and clinician

Evidence-Based Practice (EBP)
Consumer’s Goals and Strengths
Evidence-Based Practice
Community Resources
Clinical Circumstances
Effective EBP

The new challenge now is to broaden our perspective.
Not just talking about evidence-based behavioral practices – we are moving to integrated care.
Additional new challenges for direct care staff, clinical managers, executive directors and Board members.
EBP Steering Committee Initial Meeting July 21, 2004 Response to Governor’s Cabinet Priority
Initiative Short 2-3 month timeline to document
movement Evolved into ongoing groups Nearly 10 years later….. ◦ Has this lost steam… ◦ Latest draft policy….Trauma Informed Care Policy

Initial Approach Appeared to Be Creation of EBP Institute
Through Dialogue New Approach of Shared Leadership between MDCH, CMHSPs/PIHPs and Universities
Rationale ◦ Cost Savings ◦ Commitment - People Support What They Help to
Create ◦ Expertise Exists Within the State ◦ Need for MACMHB/PIHPs/CMH to take lead

Extensive Discussion of the “levels of EBP” Presentations on unique “EBPs” Extensive discussion on “thwarting
innovation” ◦ Innovation and local adaptation is possible with
expert consensus
Settled on nationally accepted EBPs that met the earlier definition AS THE STARTING POINT
Linkages within state with existing national
experts with the SAMHSA Tool Kits and Parent Management Training Oregon Model
Encourage innovation and development of
other EBP’s

Assertive Community Treatment (ACT) Integrated Dual Disorder Treatment (IDDT) Illness Management and Recovery (IMR) Supported Employment Family Psychoeducation (FPE) (Medication Management Approaches)

Promising Practices ◦ Self Determination
Creation of the Developmental Disabilities
Practice Improvement Team, or DD PIT ◦ Evaluating various practices ◦ Seeking improvements ◦ Group addressing services to persons with a dual
diagnosis of DD and MI – has made recommendations ◦ Autism Benefit – ABA

Cognitive Behavioral Therapy PMTO – Parent Management Training –
Oregon Model Promising Practices ◦ Multi-family Groups for Prevention of Schizophrenia

Institute for Research Education and Training in Addictions (IRETA) – Recovery Model
Stages of Change (Prochaska & DiClemente) Motivational Interviewing (Rollnick & Miller)

Currently lists following practices: ◦ Assertive Community Treatment ◦ Case Management ◦ Clubhouse – Psychosocial Rehabilitation ◦ Co-occurring Disorder Treatment Integrated Dual Disorders Treatment
◦ Cognitive Behavioral Therapy Dialectic Behavioral Therapy
◦ Family Psychoeducation ◦ Motivational Enhancement/Motivational Interviewing ◦ Supported Employment ◦ Supported Housing ◦ Trauma-Informed Services ◦ Trauma-Specific Treatment Trauma Recovery and Empowerment Model (TREM) and M-TREM Seeking Safety

What Did We Do, and What Are We Doing?
MDCH ◦ Provide Vision and Leadership ◦ Resource Development and Support
Universities ◦ Evaluation and Fidelity Leadership ◦ Consultation to Local Implementation Teams
PIHPs/CMHSPs ◦ Internal System Champions ◦ Supervision and Consultation to Local
MACMHB ◦ Oversee and Provide Ongoing Training and Support
National Experts ◦ In-State Consultation and Training ◦ Assist with Local Modifications
Integrated Healthcare – Learning Collaborative ◦ MDCH providing funding and leadership ◦ Universities providing evaluation ◦ PIHPs/CMHSPs committing staff time to learning
process ◦ MACMHB managing the learning collaborative
activities Potential – Excellent learning opportunity for
staff throughout the system

Learning Collaborative is ongoing, but also…. Data Analytics ◦ Individual care management ◦ Population level analysis ◦ Identification of health disparities
Health Home Pilot Various Integration Projects Statewide

Integration of physical and behavioral health care can be viewed along a continuum: ◦ Universal Screening Screening for other conditions (PH9, Weight/BP/BMI) ◦ Navigators Beyond referral, assist in accessing, moving through
healthcare system ◦ Co-location Capture both in one location ◦ Health Homes ACA offers 90% federal match ◦ System-Level Integration of Care Most advanced level of integration

Need Charge, Sample Work plan and Diagram Follow up Training, Support ◦ Ongoing Learning Communities
Board Support Executive Director Support Local Champions And…..new tools ◦ Data Analytics, Care Management, HIE, etc.

The promise of EBPS is that they pay for themselves via consumer improvement and reduced costs elsewhere
Current funds and staffing are shifted External supports are included – NAMI, family
members, etc. Staff retention is higher Positive consumer outcomes are nearly guaranteed
if practice guidelines are followed Is this what we are seeing?
Assertive Community Treatment (ACT) ◦ We have been doing this for years in Michigan
Multi-Family Psychoeducation (FPE) Integrated Dual Disorders Treatment (IDDT) Parent Management Training, Oregon (PMTO) ◦ Not required, but competitive grant funded
Supported Employment for Adults with SMI Illness Management and Recovery (IMR) Autism Benefit with ABA Health Home pilot sites learning about various EBP and
Promising Practices for integrated care Various Others Around the State
Fidelity Measurement: the extent to which a particular treatment or program is consistent with the model ◦ Can be assessed in various ways; e.g., carefully
developed scales, expert consensus ◦ Effectiveness and fidelity are directly related ◦ Insures that whatever is being measured is related
to the EBP, rather than billing or productivity
Outcome Measurement: allows for a determination of effectiveness ◦ Important to know whether or not a treatment
works This is not without its challenges – ◦ Better outcomes than what? ◦ Generally not delivered in isolation. ◦ Common measures across the state.

Review existing programs for Evidence Base ◦ Is your organization using EBPs? ◦ What are the outcomes for consumers in your
area? ◦ How and when does the Board review them? ◦ In what timeframe are outcomes achieved?
Review all new suggested programs for relationship to Evidence-Based Practice
Create data to generate new EBP

What matters more: Process Fidelity
or Service Outcomes?

In 2006, NAMI gave the State of Michigan a grade of “C” for our mental health services
In 2009, after a few years of striving to
implement multiple evidence-based practices, the State of Michigan received a “D” for our mental health services
What’s wrong with this picture?
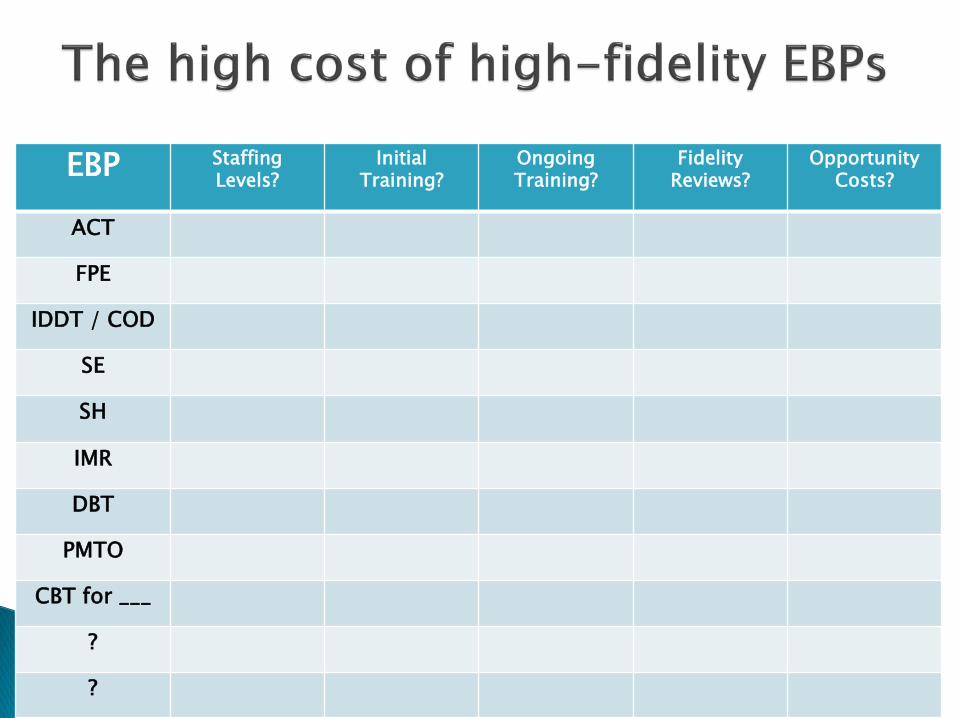
EBP Staffing Levels?
Initial Training?
Ongoing Training?
Fidelity Reviews?
Opportunity Costs?
ACT
FPE
IDDT / COD
SE
SH
IMR
DBT
PMTO
CBT for ___
?
?

As additional evidence-based practices become strongly recommended and/or mandated, but do not come along with additional resources for sustainability, at what point does a limited-resource, public-sector provider reach its limit to implement and sustain multiple EPBs at a high level of model fidelity?
When does the good become the enemy of the
better?

C. 40%
A. 30%
B. 15%
D. 15%
A. Relationship with an agent of change (therapist, doctor, case manager, sponsor, pastor, friend, family member, etc.)
B. Treatment modality (technique, method, model of change)
C. Individual change factors (including willingness and readiness to change)
D. Individual’s belief that change is possible (hope, confidence)
It is a theoretical hypothesis that implementing an evidence-based practice will automatically lead to improved outcomes. There is overwhelming evidence that points to the quality of the treatment relationship being the most significant indicator of beneficial outcomes, twice as significant as the treatment modality being used.
And even if EBPs do result in better outcomes, are
the outcome gains worth the involved costs, as compared/contrasted with other approaches that could be equally or even more efficacious?

The reality is that a number of the EBP models were researched/normed on client populations that are not the same as the SMI consumers that we serve, so high-fidelity implementation may not actually be indicated. Goodness of fit matters, yet local adjustments to EBP models may violate model fidelity and disqualify providers from being considered excellent and effective practitioners.
Additionally the EBP label is gained by demonstrating through duplicated research that the model in question is better than placebo or treatment as usual, NOT that it is better than other alternative models of treatment.
◦ Ex. Is it really surprising that ACT or IDDT shows better results than lower-resourced “treatment as usual” or nothing at all?

There is ongoing interest in the issue of high-fidelity implementation and the outcomes achieved.
This requires the identification of common outcome measures so that changes in fidelity can be evaluated in terms of impact on outcomes.
This effort has been a challenge but is central to the next emerging issue…..
As noted, the MDCH provided grant funding for implementation. But maintaining fidelity is challenging.
How do we ensure sustainability of the evidence based practices that have been implemented?
How do we make additional practice implementation reasonable?
This has been focus of considerable attention from the PISC, with help from Mary Ruffolo, PhD, from U of M

Themes that have emerged from Dr. Ruffolo’s study: ◦ Organizational factors, e.g., turnover, cost, communication ◦ Training, e.g., this takes staff from regular work ◦ Staff involved in multiple EBPs ◦ Consumer knowledge, interest ◦ Environmental issues, such as urban and rural differences ◦ Fidelity – difficult to monitor, what is standard, is this QI or
is this the price to play ◦ Technology – both in terms of EMR and in terms of use of
technology for training ◦ Billing – when can you report EBP, who decides, etc.

Some organizational guidelines for sustainability (Ruffolo) ◦ Initial and permanent funding ◦ Dedicated champions ◦ Training, and technology enhanced training ◦ Continuous internal fidelity monitoring ◦ Ongoing EBP supervision ◦ Leadership support ◦ Low staff turnover ◦ Universities must incorporate into curriculum (at least
common core competencies) ◦ EBPs must be matched to consumers’ needs and desires ◦ Must demonstrate positive recovery outcomes
Dr. Ruffolo addressed training, and the common elements of EBPs. Proposed training modules may include: ◦ Relationship Building and Stages of Change ◦ Cognitive Behavioral Essentials ◦ Behavioral Methods ◦ Acceptance-based Strategies ◦ Motivational Enhancement Skills ◦ Problem Solving ◦ Social Skill and Support Building
Now working to develop modules to then pilot.

As noted previously, the MDCH has created a website for practice improvement.
www.improvingMIpractices.org As healthcare system moves to greater integration
of primary and behavioral healthcare, the public mental health system will need awareness and understanding of a whole new array of EBPs.
Applying experience gained through implementing EBPs to preparing for integrated care.
