m. rachel mcdowell, rn, msn, acnp-bc cancer … 2... · cancer supportive care nurse practitioner...
TRANSCRIPT

M. Rachel McDowell, RN, MSN, ACNP-BC Cancer Supportive Care Nurse Practitioner Vanderbilt-Ingram Cancer Center
Goals of presentation � Provide steps for developing treatment plan � Approach to titration (upward and downward) � Patient education � Consent for treatment � Utilization of controlled substance databases � Urine drug screens use and interpretation

Benefits of pain control
� Earlier mobilization � Shortened hospitalization � Reduced cost � Improved QOL � Decrease in patient suffering

Pain Assessment � Location � Character
� Achy � Sharp � Jabbing � Deep or Superficial � Burning, tingling, numbness
� Duration: when did this begin? � Frequency: constant, intermittent, am, pm?

Intensity: Pain Scale
� Lorne B. Yudcovitch, OD, MS, FAAO; College of Optometry, Pacific University; 2043 College Way; Forest Grove, OR 97116 “The Use of Anesthetics, Steroids, Non-Steroidals, and Central-Acting Analgesics in the Management of Ocular Pain” Retrieved from http://www.google.com/imgres?imgurl=http://pacificu.edu/optometry/ce/courses/22746/images/clip_image002.jpg&imgrefurl=http://www.pacificu.edu/optometry/ce/courses/22746/ocularpainpg1.cfm&h=274&w=564&sz=37&tbnid=BdvVnqYJnZHq3M:&tbnh=65&tbnw=134&prev=/images%3Fq%3DPain%2BAssessment%2Bscales&hl=en&usg=__TdhB-pWbp_ouIYHvwQ4FJ1dHzgw=&ei=BBR2S6T_IMGXtgeCnqSlCg&sa=X&oi=image_result&resnum=7&ct=image&ved=0CCEQ9QEwBg

Treatment Plan � Goal of Therapy:
� Decrease pain level � Pain is mostly controlled, most of the time
� Increase level of function � Minimal side effects from regimen � Time frame – acute or chronic

Important Factors � Etiology of pain, prognosis � Stage of disease � What kind of pain or combo do they have? � What medications were trialed in the past?
� Efficacy,side effects, adverse events? � Age, performance status � History or current issue with drug misuse/abuse � Insurance? � How capable is the patient in understanding
plan?

Treatment Options � Treat underlying cause � Non-pharmacological measures � Pharmacological measures
� No single modality done in isolation will be effective for most patients with chronic noncancer pain (CNCP) (Ashburn, Staats, Lancet 1999)

Nonpharmacologic Options � Biofeedback � Relaxation therapy � Physical and occupational therapy � Cognitive/behavioral strategies
� Guided imagery � Acupuncture � Transcutaneous electrical nerve stimulation � Positioning � Rest, activity � Massage � Heat and cold

Treatment for pain � Identify the cause of the pain � Primary treatment if indicated � Radiation � Surgery � Hyperbaric treatment � Interventions: Nerve Block, Kyphoplasty � Medications

Interventional Techniques � Interventional Therapies
� Trigger points � Acupuncture � Nerve blocks � Facet denervation � Intrathecal pumps

Medications � Somatic/Nociceptive Pain
� Opioids � NSAIDS
� Neuropathic Pain � Anticonvulsants � Antidepressants - SNRIs
� Bony Pain � NSAIDS � Steroids

Pharmacotherapeutics and the Nervous System
Brain

Guidelines for opioids � WHO ladder combined with etiology-specific
therapies for syndromes
� pharmacologic and nonpharmacologic interventions
� long-acting + short-acting opioids � adjuvant medications for neuropathic pain � NSAIDs and steroids can be helpful when there is
an inflammatory component to pain

WHO Guidelines for Cancer Pain
� Step 3: Opioids for moderate-to-severe pain +/- non-opioid +/-adjuvant therapy
� Step 2: Opioids for mild- to-moderate pain +/- non-opioid +/- adjuvant therapy
� Step 1: Non-opioid +/- adjuvant therapy
STEP 1
STEP 2
STEP 3
GOAL: Freedom From Pain
Pain Persists
Pain Persists
(Adapted from Portenoy et al, 1997)

Opioid Selection � No perfect opioid � Pre-treat likely side effects � Must recognize individual responses to
opioids may vary � Response and side effects � Hydrocodone vx. Oxycodone
� Sequential trials of different opioids – alone or in combination – may be necessary to optimize therapy

Common Analgesics � Demerol � Morphine Sulfate IR � Percocet � Dilaudid � Lortab � Opana IR � Oxycodone � Tramadol
� Butrans � Morphine Sulfate ER � OxyContin � Exalgo � Fentanyl patches � Opana ER � Methadone
Pure Opioid Agonists
� Pure Opioid agonist � No ceiling effect for analgesia � Single-entity for moderate to severe pain � May be a role for combined opioids in certain
subsets of patients

Current Regimen � Opioid Naïve:
� Never been on opioids before � Only been on opioids for a short time period or
intermittently
� Opioid Tolerant � Taking pain medications on a regular basis � Dependent on amount of pain medication

Differences in older adult � Experience higher peak and longer duration of drug
action � Age-related changes in drug distribution and elimination
make more sensitive to sedation and respiratory distress
� Pain perceived differently � Physiologic � Psychological � Cultural changes
� Altered presentations � Aging does NOT increase Pain threshold � Older adults (esp frail and old-old) at risk for too little
or too much

General Approach � Start pt on short acting � Titrate up for pain relief � Once stable convert to long acting
� Add amount of short acting for 24 hours � Convert to long acting
� Continue short acting for breakthrough pain
� 10-15 % of 24 hour total narcotic

Advantages of Long-Acting Opioids
� More predictable serum levels � More predictable pain relief � Avoids mini-withdrawals
� Easier to use; improved compliance � Greater Patient satisfaction � Less reinforcement of drug-taking behavior
Titration of Opioids � Titrate to adequate pain control.
Appropriate dose adjustments are critical to adequate pain control. Adjustments are indicated under the following circumstances � If the patient has been taking more than 4
rescue doses per day � If the patient rates pain as greater than 4/10 � If the patient complains the pain is
inadequately controlled

Dose Titration � Based on two pieces of information:
� Calculation of the 24-hour narcotic total (this should be averaged over several days unless the patient has had a marked increase in pain in the prior 24-hour period of time)
� The stated average pain level (this should be averaged over several days unless the patient has had a marked increase in pain in the prior 24-hour period of time)

24-hour narcotic total: � = 24o fixed dose + 24o rescue doses � a patient is taking MSER 60 mg po bid with MSIR
15 mg po q1-2hrs prn for breakthrough. � On history, he indicates that he is taking the
sustained-release formulation as directed and 8 rescue doses in a 24-hour period of time.

� The 24-hour narcotic total is: (60 mg x 2 doses) + (15 mg x 8 doses) = 120 mg + 120 mg = 240 mg.

Dose Titration � Dose titration by a fixed percentage
� Moderate pain (5/6): � increase 24 hour narcotic total by 25%
� Severe pain (7+): � increase narcotic total by 50%
� Rescue dose: � 10-15% of total dose offered Q 1-2 hours PRN
� Accommodate increase if pt frail, sick, or elderly

Case Study
1. Pt reports 6/10 pain, therefore he requires a 25 % increase in medication.
2. Pt’s 24 hour narcotic total = ___ mg
morphine

Step 1:
Increase dose by 25%
24 NT mg + (24 NT x .25) =
New long acting dose

Step 2: Determine the new fixed dose
New fixed dose / 2 doses per day =
X mg bid

Step 3 Calculate the rescue dose
10% of NT mg = X mg
New rescue order = MSIR X mg q2h prn

Old regimen MSER 60 mg bid MSIR 15 mg q 2 prn
New regimen
MSER 150 mg bid MSIR 30 mg q 2 prn

Case Study
Pt reports 8/10 pain.
What do you do?

Pt reports 8/10 pain, therefore he requires a 50 % increase in his medication.
Pt’s 24 hour narcotic total =
240 mg morphine
Step 1: Increase dose by 50% 24 NT mg + (24 NT x .50) = 240 mg + ___ = ___ mg

Step 2:
� Determine the new fixed dose � ? mg / 2 doses per day = ? mg

Step 3: Calculate the rescue dose 10% of new 24 NT = ___ mg New rescue order =
MSIR ___ mg q2h prn
� Old regimen � MSER 60 mg bid � MSIR 15 mg q 2 prn
New regimen MSER 180 mg bid
MSIR 30 mg q 2 prn

Equianalgesia Opioid Equianalgesic Dose
Morphine 30 mg po
Dilaudid 4-6 mg po
Hydrocodone 30 mg po
Oxycodone 30 mg po
Codeine 180 mg po
Opana Use conversion calculator

Or The ratio is 2:1
2 mg oral morphine per DAY ~ 1 mcq fentanyl patch
24-hour oral morphine dose (mg/day) Transdermal fentanyl dose (mcq/hour)
30-90 25
91-150 50
151-210 75
211-270 100
Every additional 60 mg per day An additional 25 mcq per hour

Fentanyl Patch � In pts currently on opioids, conversion factor for
Morphine to Fentanyl is 2:1 � Fentanyl patch is 2X more potent than morphine
PO � If the 24 hr narcotic total= 180 mg morphine � Fentanyl dose= ___ mg (use nearest fentanyl
patch size)

IV to PO conversion
� Now your patient is ready to go home but need to be converted to PO medication.
� Pt is on a morphine pain pump at a continuous infusion of 7.5 mg/hour and uses the bolus of 1 mg 6 times in the past 24 hours.

Case Study 1. 7.5 mg/hr X 24 = 180 mg morphine IV/24 2. IV Narcotic total = 186 mg IV 3. PO Narcotic total = 558
� Opioid naïve: IV is 6X more potent than PO (1:6) � Currently on opioid: IV is 3X more potent than
PO (1:3)

4. Rescue dose is 10% = 60 mg morphine q 2 hours prn
5. Long acting dose = 280 mg morphine bid

� Old regimen: � 7.5 mg/hour CIV, with 1 mg q 10
minutes prn
� New Regimen: � MSER 280 mg bid � MSIR 60 mg q 2 prn

Case Study � A patient with a pathologic fracture had
satisfactory relief of pain with an IV dilaudid infusion of 3 mg per hour.
� You want to send her home on an equianalgesic dose of sustained release oral morphine (MS Contin or OraMorph SR given q12h, or Kadian q day).
� What is the correct dose?

Calculations
1. 3 mg/hr dilaudid = 72 mg IV dilaudid/24 hrs 2. Convert from dilaudid to morphine:
72 mg dilaudid IV X 5 = 360 mg IV morphine
3. Narcotic total = 360 mg IV morphine/24 hours

3. Narcotic total = 360 mg IV morphine/24 hours 4. Multiply IV by 3 to obtain PO dose
360 x 3 = 1080 mg morphine in 24 hours PO 5. Breakthrough dose = 10 % of 24 hour narcotic
total MSIR 30 mg, 3 tabs po q 2 prn Dilaudid 8 mg, 2 tab po q 2 prn

6. The q12h dose = 500 mg morphine SR PO q12h
MS Contin 100 mg, 5 tabs po BID MS Contin 100 mg, 3 tabs po TID

� Old regimen: � 3 mg/hr dilaudid IV
� New regimen: MS Contin 100 mg, 5 tabs po BID MS Contin 100 mg, 3 tabs po TID
� Rescue dosing MSIR 30 mg, 3 tabs po q 2 prn
or Dilaudid 8 mg, 2 tabs po q 2 prn

NARCAN !!!!! � Narcan is a narcotic antagonist that works by
blocking opiate receptor sites, which reverses or prevents toxic effects of narcotic (opioid) analgesics.
� DANGER: if given too quickly or if too much is given – severe life-threatening side effects can occur

� Cardiovascular: Hyper-/hypotension, tachycardia, ventricular arrhythmia, cardiac arrest
� CNS: Irritability, anxiety, narcotic withdrawal, restlessness, seizure
� Gastrointestinal: Nausea, vomiting, diarrhea � Neuromuscular & skeletal: Tremulousness � Respiratory: Dyspnea, pulmonary edema

Use of Narcan in Narcotic overdose: � I.V. (preferred), I.M., intratracheal, SubQ: 0.4-2 mg
every 2-3 minutes as needed; may need to repeat doses every 20-60 minutes.
� If no response is observed after 10 mg, question the diagnosis.
� Note: Use 0.1-0.2 mg increments in patients who are opioid dependent and in postoperative patients to avoid large cardiovascular changes.


Adjuvant Analgesics � TCAs
� Desipramine � Elavil
� SNRIs � Cymbalta � Savella
� Anticonvulsants � Neurontin/Gabapentin � Lyrica
� Joint/Bone pain: NSAIDS – potentiate opioids � Methadone � Lidoderm patches

TCAs and SNRIs � Desipramine: 25 mg at bedtime, increase
weekly to max dose of 150 mg daily � Elavil: 25 mg at bedtime, max of 150 mg daily � Cymbalta: 20 mg at bedtime, max dose 120 mg

Anticonvulsants � Neurontin/Gabapentin
� Maximum daily dose: 3600 mg � Start low and titrate up to max dose
� 100 mg qid
� Lyrica � Maximum daily dose: 300 mg � Start at 25 or 50 mg tid
� Problematic Side Effect: sedation

Bony or Metastatic pain � NSAIDS
� Ibuprofen 800 mg tid � Naproxen 600 mg bid � Diclofenac 100 mg bid
� Steroids � Medral Dose Pak

Methadone � Possible duel mechanism of action
� Somatic and neuropathic pain relief
� Relatively inexpensive � Available as a liquid � Long half-life
� Accumulates with repeat doses with limited analgesic effect
� Complex pharmacokinetics � No known active metabolites � Conversion tables underestimate potency � Cardiac Toxicity � Recommend specialized training before prescribing as
NP

Lidoderm Patch � Lidocaine 5% in dermal patch � On 12 hours, off 12 hours � FDA approved for shingles � Drug interaction and side effects are unlikely –
most common is skin sensitivity � Mechanical barrier decreases allodynia


Patient Education � How the medication will impact their
pain � How to take medication. � What the medication is treating � Potential side effects, like constipation. � When to call doctor’s office.

Patient Education � How to store/protect their medication.
� Lock box or safe � How to travel with their medication. � What to do if/when medication is
stolen or is lost/missing – CALL POLICE, FILE REPORT
� Consent for treatment

https://tnm.rxportal.sxc.com/rxclaim/TNM/PtMedMngtAgrmt.pdf http://www.painmed.org/Workarea/DownloadAsset.aspx?id=3211
Consent for Treatment Sources

Patient education � Patient’s responsibility � Clinician’s responsibility
� Urine Drug Screen
� Use of drugs other than prescribed, and consequences

Re-evaluation � Changes in pain (level, location, frequency,
character) � Level of function � Average pain level � Worst pain level � Side effects � Benefits � Adherence to medication regimen (missed or
extra doses)

Titrating off Opioids � Indicated if pt unable to take medications
safely � If pt’s level of function is declining � If medication is not effectively decreasing or
controlling their level of pain
� Dose reduce in increments of 25% at a time � No faster than 48-72 hours.


� State Controlled Substance Database Reports � Frequent evaluations, with good documentation � Lost or stolen drugs: Must report to police
department � Check for placement of fentanyl patches � Urine Drug Screens – random, or when there is
aberrant behavior
Monitoring for abuse
Interpretation of UDS Results � Important to understand what the results mean � If question, call lab to check results

Drug Major Cmpds Minor Cmpds
Codeine Codeine Morphine
Morphine Morphine Codeine
Dihydrocodeine Dihydrocodeine Hydrocodone
Hydromorphone
Hydrocodone Hydrocodone Hydromorphone Dihydrocodeine
Hydromorphone Hydromorphone
Oxycodone Oxycodone Oxymorphone
Oxymorphone Oxymorphone
Fentanyl Fentanyl **may not be picked in opiate screen
Heroin/diamorphine Morphine 6MAM by specific assay
Marijuana Carboxy-THC **many false +screen
Cocaine Benzoylecgonine

Results
CANNABINOIDS (SCREEN) Positive Immunoassay(cut-off 20 ng/mL); confirmation to follow
THC CONFIRMATION Positive for Carboxy-THC Cannabis metabolite cut-off 15 ng/mL
COCAINE METAB (SCREEN) Positive Immunoassay(cut-off 300 ng/mL); confirmation to follow
BEG CONFIRMATION Positive for Benzoylecgonine Cocaine metabolite cut-off 150 ng/mL

METHADONE (SCREEN) Negative Immunoassay(cut-off 300 ng/mL)
OPIATE (SCREEN) Positive Immunoassay(cut-off 300 ng/mL); confirmation to follow
GC/MS OPIATE CONFIRM Positive DIHYDROCODEINE Negative CODEINE Negative MORPHINE Negative HYDROCODONE Negative HYDROMORPHONE Negative OXYCODONE Positive OXYMORPHONE Positive OXYCODONE (SCREEN) Positive Immunoassay(cut-
off 300 ng/mL); confirmation to follow

TRICYCLICS (SCREEN) Negative Immunoassay(cut-off 300 ng/mL)
ACETAMINOPHEN METABS Negative SALICYLATES Negative PHENOTHIAZINES Negative PROPOXYPHENE Negative Immunoassay(cut-off
300 ng/mL) METHANOL Negative ETHANOL Negative ACETONE Negative ISO-PROPANOL Negative

How to protect yourself � Documentation � UDS � Consent for treatment � Controlled Substance Database Report � Frequent re-evaluation � Communication (with your team and other
providers) � Patient Education � Consistency

Addressing Aberrant Drug-Related Behavior � General Management Principles
– know laws and regulations – structure therapy to match perceived risk
� Proactive Strategies – communicate goals of therapy – provide written guidelines (treatment contract) – assess often
� Reactive Strategies – require frequent visits and small quantities of drug – use of urine toxicologies – long-acting drugs with no rescue doses – refer to addiction-medicine community (sponsor,
program, addiction-medicine specialist, psychotherapist)
(Mironer et al, 2000; Portenoy et al, 1997; Passik et al, 2000)

Promoting Pain Relief and Preventing Abuse of Pain Medications: A Critical Balancing Act
A joint statement from 21 health care organizations and the Drug Enforcement Agency, October 23, 2001
� Undertreatment of pain is a serious problem in the US, including pain among patients with chronic conditions and those who are critically ill or near death
� Effective pain management is an integral and important aspect of quality medical care, and pain should be treated aggressively
� For many patients, opioid analgesics, when used as recommended by established pain management guidelines, are the most effective way to treat their pain, and often the only treatment option that provides significant relief
� http://www.usdoj.gov/dea/presrel/pr102301.html


Considerations for the Nurse Practitioner � Regulations – State law, Boards of Nursing and
Medicine � Safe Practice � Requirements by the State Board of Nursing and
Board of Medicine
� Prescriptions

Evaluation of Quantity and Chronicity
� Documented appropriate diagnosis � Treatment of recognized medical indication � Documented persistence of recognized
medical indication � Properly documented follow-up evaluation with
appropriate continuing care

Writing Prescriptions � Prescriptive authority varies state by state
� NPs denied any prescriptive authority � Limited prescriptive authority – i.e. NP can only write 72
hours worth of pain medication � Full prescriptive authority granted to NPs.
� For specifics visit: http://www.medscape.com/viewarticle/439917
� http://www.bartonassociates.com/nurse-practitioners/nurse-practitioner-scope-of-practice-laws/

Safe Prescription Writing Pt’s Name, DOB, Current date Medication name Dose (mg, mcg) SIG: instructions about how medication is to be
taken, how often, how many tablets, what route, frequency.
DISP: amount of tablets or liquid to be dispensed.
Should write it both as number and spelled out.
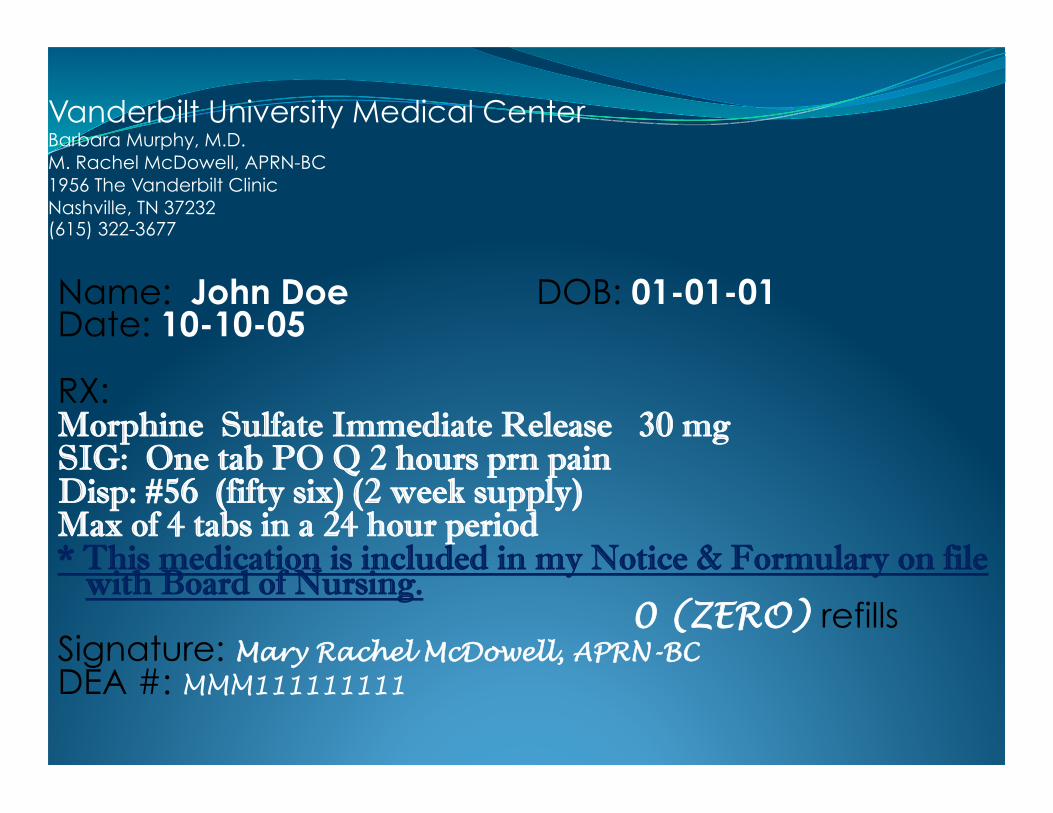
Vanderbilt University Medical Center Barbara Murphy, M.D. M. Rachel McDowell, APRN-BC 1956 The Vanderbilt Clinic Nashville, TN 37232 (615) 322-3677
Name: John Doe DOB: 01-01-01 Date: 10-10-05 RX: Morphine Sulfate Immediate Release 30 mg SIG: One tab PO Q 2 hours prn pain Disp: #56 (fifty six) (2 week supply) Max of 4 tabs in a 24 hour period * This medication is included in my Notice & Formulary on file
with Board of Nursing. 0 (ZERO) refills
Signature: Mary Rachel McDowell, APRN-BC DEA #: MMM111111111
Recent Changes in TN Law � Requirement to run Controlled Substance
Database Report prior to initiation of regimen with controlled substance
� Limitation of PA/NPs – can only write 30 day supply of controlled substances, and med must be on Notice and Formulary � Pharmacies are required to verify that controlled
substance is on Notice and Formulary or that the medication was prescribed after authorization given by supervising physician.

Helpful Websites � American Pain Society
� http://www.ampainsoc.org/
� Partners against Pain � http://www.partnersagainstpain.com/index.aspx?sid=27
� International Association for the Study of Pain � http://www.iasp-pain.org//AM/Template.cfm?Section=Home
� The Joint Commission � http://www.jointcommission.org/
� American Academy of Pain � http://www.aapainmanage.org/Management

The following resources can provide important information on prescription pain medications, such as DEA schedule, appropriate prescribing and use, and information on how to prevent drug abuse and diversion:
� The American Pain Society (APS) http://www.ampainsoc.org
� American Academy of Pain Medicine (AAPM) http://www.painmed.org
� American Society of Addiction Medicine (ASAM) http://www.asam.org
� Pain and Policy Studies Group for the University of Wisconsin Comprehensive Cancer Center http://www.medsch.wisc.edu/painpolicy
� United States Drug Enforcement Administration http://www.dea.gov
� Taken from Partners Against Pain Web site

� Food and Drug Administration http://www.fda.gov
� The Substance Abuse and Mental Health Services Administration (SAMHSA) http://www.samhsa.gov
� The National Association of Drug Diversion Investigators (NADDI) http://www.NADDI.org
� Local law enforcement � Local addiction treatment specialists/centers � Taken from Partners Against Pain Web site

References � Katz, Warren, Rothenberg, Russell, 2005, Section 3:
The Nature of Pain: Pathophysiology, JCR: Journal of Clinical Rheumatology, volume 11 (2) Supplement, April 2005, pp S11-S15, http://gateway.ut.ovid.com/gw1/ovidweb.cgi, (Oct. 3, 2005)
� Cancer: principles and practice of oncology [edited by] Vincent T. DeVita, Jr., Samuel Hellman, Steven A. Rosenberg; 319 contributors.—6th
� Nicholson, B.D., Neuropathic Pain: New Strategies to Improve Clinical Outcome, January 31, 2005 http://www.medscape.com/viewprogram/3765_pnt, (Sept. 30, 2005)

� Passik SD, Portenoy RK. Substance abuse issues in palliative care. In Berger A, Portenoy RK, Weissman D, eds. Principles and Practice of Supportive Oncology. 2nd ed. Philadelphia, PA: Lippincott-Raven Publishers; 1998.
� Passik SD, Portenoy RK: Substance abuse issues in psycho-oncology. In Holland J, et al. Handbook of Psycho-oncology. 2nd ed. Oxford: Oxford University Press; 1998:576-586.
� Loeser et al, 2001; Portenoy et al, 1996)
� Besson, JM. The neurobiology of pain. Lancet. 1999;353:1610-1615 .
