luncheon seminar omni shoreham hotel august 27, 2008 hiv medical case management: addressing the...
TRANSCRIPT

Luncheon SeminarOmni Shoreham Hotel
August 27, 2008
HIV Medical Case Management:
Addressing the Training Needs of Front Line Workers and Ryan White HIV/AIDS Program Grantees

Today we will … Provide an overview of
The concepts underlying the medical case management (MCM) service category in the Ryan White HIV/AIDS Treatment Modernization Act of 2006
HAB’s current requirements regarding medical and non-medical case management (CM)
Approaches used throughout the U.S. to adopt medical CM, with presentations from three metropolitan areas
The Abbott Laboratories and Positive Outcome assessment and curriculum development project

Today we will …Discuss the medical CM training needs of HIV case
managers and CM supervisors in your communities, and the extent to which these needs are being addressed
Conduct a written mini-assessmentGet your feedback about meaningful ways our project
can help you and your colleagues

Defining Medical
CM

HAB’s Medical CM DefinitionMedical CM services (including treatment adherence) A range of client-centered services that link clients with health
care, psychosocial, and other servicesThe coordination and follow-up of medical treatmentsMedical CM includes the provision of treatment adherence
counseling to ensure readiness for, and adherence to, complex HIV/AIDS treatments
These services ensure timely and coordinated access to medically appropriate levels of health and support services and continuity of care
– Through ongoing assessment of the client’s and other key family members’ needs and personal support systems

Key activities include– Initial assessment of service needs – Development of a comprehensive, individualized service
plan – Coordination of services required to implement the plan– Client monitoring to assess the plan’s efficacy and – Periodic re-evaluation and adaptation of the plan as
necessary over the client’s life Includes client-specific advocacy and/or review of utilization of
services Includes all types of CM including face-to-face, phone contact,
and any other forms of communication
HAB’s Medical CM Definition Contd

Provision of advice and assistance in obtaining medical, social, community, legal, financial, and other needed services
Does not involve coordination and follow-up of medical treatments, as medical CM does
HAB’s Non-Medical CM Definition

HAB does not explicitly define treatment adherence responsibilities or roles for medical case managers
Treatment adherence strategies used throughout the U.S. include– Assess factors likely to contribute to poor adherence and
develop individualized care plans to address those factors– Medication, referral, and appointment adherence
interventions– Patient HIV education to expand “health literacy” – HIV medication education, including side effects and their
management
HAB’s CM Treatment Adherence Definition

Attending medical visits to assist patients to understand the information provided by medical provider
Coordinate appointment scheduling to book multiple visits on the same day and arrange transportation to ensure the patient keeps appointments
Home visiting and other methods of case finding for patients that have broken appointments or dropped out of care
Assess and treat mental illness and/or substance abuse
HAB’s CM Treatment Adherence Definition Contd

Environmental Challenges in Operationalizing MCM
Good news: HAB’s MCM definition is not proscriptive Bad news: HAB’s MCM definition does provide a
roadmap in designing or improving MCM and non-medical CM systems
The CM workforce in many (not not all) jurisdictions are in crisis High caseloads, inadequate compensation and training, minimal
supervision, high turnover HAB grantees are re-engineering their CM systems to address
these challenges, as well as to “medicalize” CM practice One missing component to their efforts to medicalize CM
practice is the collateral expectation that clinician embrace the role of MSM on the care team

Medical Case Management Training Strategies:
Approaches Taken by Three Communities

William Green, Broward County Human Services Dept
Adopting Medical Case Management in the Broward County Eligible
Metropolitan Area: Challenges and Opportunities
Adopting Medical Case Management in the Broward County Eligible
Metropolitan Area: Challenges and Opportunities

1980s Late 1980s-Early 1990s Mid to Late 1990s 2000s 2006
20032002 2004
Ft. Lauderdale Broward County EMA
Nationally

HAB/HRSA Project Officer Technical Assistance Training Initiatives


Broward’s Medical Case Management Infrastructure
What components did Broward have to implement medical case management?

Converting a non-medical case management system to medical case management
Changing Clinician Attitudes
About Case
Managers
High Turnov
er
Low Case
Manager
Salaries
Psychosocial Model Used by
CBOs and Clinics
High Caseloa
ds

• Treatment Plan Medically Focused
•Incorporate Multi-disciplinary Staffing
•Provide ongoing forums for Continuous
Medical Case Management Training
Medical Staff
Non-Medical Staff

Florida Caribbean/AIDS Educational Training Center (AETC) AIDS Community Research Initiative of America (ACRIA) Grantee Sponsored MCM and MCM Supervisor Training
Continuous Training

Medical Case Management Training Series Training 1-Treatment Adherence Training 2-Lab Tracking 101 Training 3-HIV/AIDS: The Latest Research
and Treatments Training 4-Assessing Client’s Medical/Clinical
Needs Training 5-Cultural Competency

HIV Health Literacy Training Two 8-Hour Days – Offered Twice Required For All Case Managers Optional For Outreach Workers Treatment Adherence Focused

Part A Grantee developed training curriculum and contracted with a training subgrantee to train Medical Case Managers and Medical Case Manager Supervisors Pre-requisite Basic Training (16 hours) Advanced Training (36 hours) Trainings are conducted annually


Imbedded in the SUPPORT model is the 4-1-1 Supervision Format. The 4-1-1 Format specifies that one hour of supervision should include 40 minutes of case review, 10 minutes discussing professional growth, and 10 minutes discussing administrative functions. This model is premised on the belief that the client’s
health is the most important consideration for the MCM and the ability to provide the highest quality of care is directly dependent upon the staff’s performance
and skill level.

HIV Medical Case Management:
Addressing the Training Needs of Frontline Workers and
Ryan White Program Grantees
Evelyn Torres, MBA Philadelphia Department of Public Health Philadelphia EMA

Philadelphia EMA• Nine counties across two states • 70 funded providers • 15,000 consumers• PDPH, AIDS Activities Coordinating Office administers
– Part A– Local Part B - Pennsylvania– CDC Prevention & Surveillance – Local HIV funding

Philadelphia EMA Service System
• Decentralized system
• 24 medical agencies
• 28 edical case management agencies– 6,600 clients receiving case management
services– 1,800 intakes a year completed through the
Client Services Unit

Profile of Medical Case Management (MCM)Services in Philadelphia
• Funding: $7 million (RW A, B, and local)• Services are provided through:
– CBOs – ASOs – Hospital outpatient infectious disease clinics – Stand-alone HIV clinics
• 2/3 of providers are either ASOs or CBOs

MCM Model• Broker model with goals of:
– Facilitating access to and retention in medical care
• Tracked since 2001
– Providing treatment adherence counseling • Standards of care and outcomes established• Educational requirements for case managers and
supervisors • Grantee conducts yearly training and certification of Parts A
and B-funded case managers and supervisors

MCM Training• Annual training and certification process,
coordinated with the local AETC• Core training: nine days on six specific topics for
newly hired case managers and supervisors • Ongoing training: 20 hours of mandated training of
which 6 hours must be medical• Providers are notified of those employees not
completing the annual requirements• 130 case managers and supervisors in the
Philadelphia EMA
Grantee Response to HAB MCM Model
• Fund only MCM • RFP emphasis
– Treatment Adherence – Retention in medical care– Supervision– Case closure
• Mandates policies and procedures for each of above

AACO Medical Case Management Committee
Priority AreasTreatment adherence, clinical supervision, and
linkage/retention in medical careTasks1. Identify responsibilities and roles of MCM providers 2. Identify key implementation activities for the CSU,
ISU, and PSU3. Revise training curriculum to reflect the paradigm
shift

Training Curriculum Changes • Emphasis on treatment adherence
– Assessment of client’s adherence to HIV treatment
– Treatment adherence activities – Documentation
• Health literacy • Continue focus on medical follow-up by
fostering collaboration between community-based case managers and medical providers

Pearls of Wisdom• Do not re-invent the wheel
– Look at what is out there
• Take an integrated approach– Training cannot be done in a vacuum
• Highlight best practices • Stress the benefit• Get input from key stakeholders
– Surveys– CQI Meetings– Focus Groups

Implications for Training and Service Implementation
Pat Balducci, LCSW
Medical Case Management

Presentation OverviewPresentation Overview
I.I. Historical PerspectiveHistorical Perspective
II.II. The Baltimore ExperienceThe Baltimore Experience
III.III. Training StrategiesTraining Strategies

Section I:Section I:Historical PerspectiveHistorical Perspective
Historically, Case Managers focused on Historically, Case Managers focused on helping HIV+ patients and their loved helping HIV+ patients and their loved ones grapple with issues such as ones grapple with issues such as chronic disease management with few chronic disease management with few medications, limited entitlements, medications, limited entitlements, lifestyle issues, and too often, death lifestyle issues, and too often, death and dyingand dying

HIV – In the HIV – In the BeginningBeginning
Few tools Few tools Evolving understanding of disease Evolving understanding of disease Limited medicationsLimited medications Limited entitlementsLimited entitlements Limited staff trainingLimited staff training Developing Standards of CareDeveloping Standards of Care

Section II:Section II:
The Baltimore ExperienceThe Baltimore Experience

Baltimore EMA Standards of Baltimore EMA Standards of CareCare Part A (formerly Title I) Standards of Care were Part A (formerly Title I) Standards of Care were
ratified November 1998 and revised October 2003ratified November 1998 and revised October 2003 Case Management (CM) Standards evolved as a Case Management (CM) Standards evolved as a
Medical ModelMedical Model Addressed:Addressed:
AssessmentAssessment Care Plan DevelopmentCare Plan Development Plan ImplementationPlan Implementation Monitoring and EvaluationMonitoring and Evaluation Case ClosureCase Closure Qualifications (RN or licensed SW with a minimum 3 years Qualifications (RN or licensed SW with a minimum 3 years
experience)experience)

Standards of Care Standards of Care ContdContd Delineated CM ServicesDelineated CM Services
Ensure timely and coordinated access to medical Ensure timely and coordinated access to medical care and support servicescare and support services
Timeline for intake and Care Plan development Timeline for intake and Care Plan development addressedaddressed
Provision of comprehensive forms and related CM Provision of comprehensive forms and related CM toolstools
Levels of care definedLevels of care defined Emphasis on care coordination, appointment Emphasis on care coordination, appointment
tracking, and access to medicationtracking, and access to medication Technical Assistance/CQITechnical Assistance/CQI

Recruitment of Community-Based Recruitment of Community-Based ProvidersProviders
Recognition early on in the Baltimore EMA that Recognition early on in the Baltimore EMA that consumers and community partners needed to play a consumers and community partners needed to play a greater role in care development and service deliverygreater role in care development and service delivery
Demand for culturally competent HIV CM services grew Demand for culturally competent HIV CM services grew in conjunction with targeted outreach and care retention in conjunction with targeted outreach and care retention strategiesstrategies
Non-medical, community-based providers were Non-medical, community-based providers were identified through capacity building resulted in identified through capacity building resulted in additional training needsadditional training needs
HAB requirements further define MCMHAB requirements further define MCM Care linkage role broadens to include care Care linkage role broadens to include care
coordination and management of medical care plancoordination and management of medical care plan
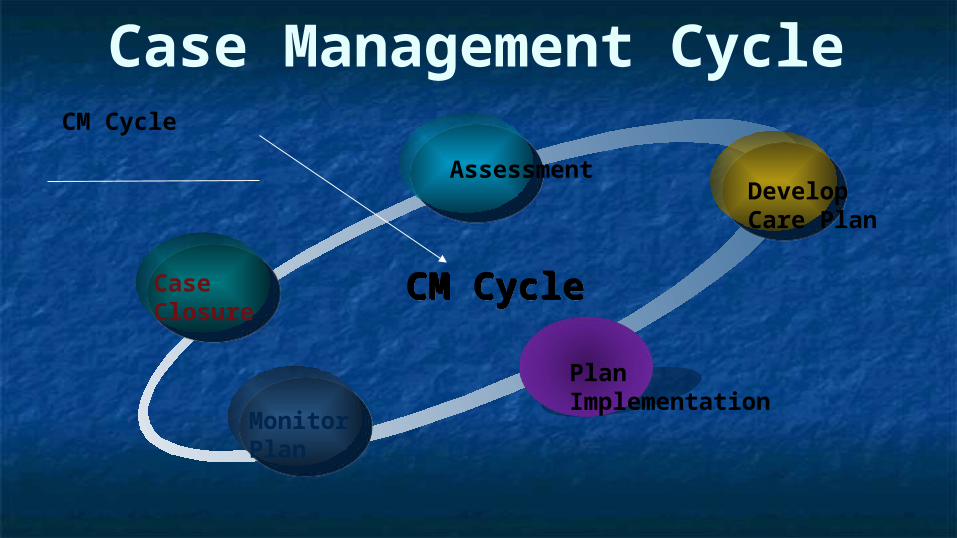
Case Management Cycle
CaseClosure
AssessmentDevelopCare Plan
Plan Implementation
Monitor Plan
CM CycleCM Cycle
CM Cycle


Section III:Section III:
Training Tools & StrategiesTraining Tools & Strategies
For Front Line Case ManagersFor Front Line Case Managers


CM TrainingCM Training Diagnostic AssessmentDiagnostic Assessment
Review local CM Standards and relevant Review local CM Standards and relevant Performance MeasuresPerformance Measures
Conduct individual provider meetingsConduct individual provider meetings Perform chart reviewsPerform chart reviews Offer Corrective Action Plans that Offer Corrective Action Plans that
emphasize MCM practices and emphasize MCM practices and documentationdocumentation
CM Training CM Training ContdContd Comprehensive TA offered by multi-Comprehensive TA offered by multi-
disciplinary training teams in multiple disciplinary training teams in multiple sessionssessions Provider engagement/rapport buildingProvider engagement/rapport building Encouragement of provider collaboration and Encouragement of provider collaboration and
sharing of expertise and experiencesharing of expertise and experience Integration of documentation training emphasizing Integration of documentation training emphasizing
CM indicatorsCM indicators Quality indicators/measurements reviewQuality indicators/measurements review Use of detailed case conferences as mechanism to Use of detailed case conferences as mechanism to
discuss/learn MCM interventionsdiscuss/learn MCM interventions

Comprehensive Training Comprehensive Training ContdContd Practice Care Plan development, emphasizing SMART Practice Care Plan development, emphasizing SMART
goals (Specific, Measurable, Attainable, Realistic, goals (Specific, Measurable, Attainable, Realistic, Time-Limited)Time-Limited)
Facilitated dialogue with other care providers Facilitated dialogue with other care providers (Medicaid, VA, Social Security, homeless services, etc.) (Medicaid, VA, Social Security, homeless services, etc.) to create linkages and seamless service integrationto create linkages and seamless service integration
Provision of CM tools:Provision of CM tools: Chart and forms templatesChart and forms templates EMA specific benefits gridEMA specific benefits grid Web-based tools, online resources, trainings, Web-based tools, online resources, trainings,
virtual learning lab, ongoing provider-specific virtual learning lab, ongoing provider-specific technical supporttechnical support
Training/Updates on available insurance programs Training/Updates on available insurance programs and entitlementsand entitlements

Ongoing Training/TAVirtual LearningLab
Case ManagementTraining
Direct TA
Virtual LearningLab-OnlineResource forproviders
MonthlyCase ConferenceWeb-castand Web-Tools
MultipleTrainingSessions For AllCase Managers
Technical Support24-7 via e-mail and Virtual Learning LabPhone supportas needed
Web-castCase Conference

SummarySummary Case managers need support and comprehensive Case managers need support and comprehensive
technical assistance to shift to a MCM Modeltechnical assistance to shift to a MCM Model Facilitation of the initial commitment and “buy-in” of Facilitation of the initial commitment and “buy-in” of
front-line staff must occurfront-line staff must occur Requires multiple contacts via face-to-face meetings, Requires multiple contacts via face-to-face meetings,
web support, and individual telephone contactweb support, and individual telephone contact Multi-disciplinary, multi-session trainingMulti-disciplinary, multi-session training Creation of training tools for case managers that are Creation of training tools for case managers that are
linked to medical CM performance measures and linked to medical CM performance measures and Standards of CareStandards of Care
Creation of web-based tools that include chart Creation of web-based tools that include chart templates, TA presentations pertaining to specific templates, TA presentations pertaining to specific EMA needs, and ongoing supportEMA needs, and ongoing support

SourcesSources Greater Baltimore HIV Health Services Greater Baltimore HIV Health Services
Planning Council, Planning Council, Case Management Case Management Standards of CareStandards of Care, , http://www.baltimorepc.org/v2/main/page.php?page_id=64
HAB, HIV Case Management HAB, HIV Case Management Standards of Care, Standards of Care, http://hab.hrsa.gov/
http://www.taylor-wilksgroup.com/

HIV Medical Case Management Project

Project Objectives Conduct a national assessment of the training needs
of HIV case managers in adopting MCM techniques Identify HIV MCM training efforts being undertaken
by the AETCs, other HAB-funded grantees, or subgrantees
Develop and test an HIV MCM curriculum that can easily be used by trainers or supervisors and that can be adopted by Part A and B grantees and AETCs

Project Activities Steering committee is being formed now Several jurisdictions will be selected to participate in the
assessment of training needs of HIV case managers and their supervisors The assessment tool was field tested at the HIV and Social Work
Conference and several local CM training conferences Participating jurisdictions will receive a report summarizing
assessment results The HIV MCM training efforts undertaken by the AETCs, other
HAB-funded grantees, or subgrantees will be identified and materials gathered Please share your materials
The curriculum will be developed based on results of the training needs assessment

Project Activities Steering committee is being formed now Several jurisdictions will be selected to participate in
the assessment of training needs of HIV case managers and their supervisors Assessment tool was field tested at the HIV and Social Work
Conference and several local CM training conferences Participating jurisdictions will receive a report summarizing
assessment results The HIV MCM training efforts undertaken by the
AETCs, other HAB-funded grantees, or subgrantees will be identified and materials gathered Please share your materials
Project Activities The curriculum will be developed based on results of
the training needs assessment The curriculum will be design using the train-of the-
trainer (ToT) approach for introductory, intermediate, and advanced HIV MCM topics
One module will focus on how to integrate HIV medical case managers into staffing and care models. The ToT approach will be used so that case management supervisors can easily use the training modules for in-service training sessions.

Project Activities Two cities will be selected to participate in a series
of four workshops to test the curriculum: beginning, intermediate, and advanced medical CM topics and how to integrate HIV medical case managers into staffing and care models– To ensure the workshops are relevant to the audience,
information will be gathered from RWHAP grantees in the jurisdiction to ensure an understanding of the organization, delivery, and financing of HIV medical and other CM services
The curriculum will be disseminated to grantees, AETCs, and other interested groups

Discussion
HIV Medical Case Management:
Addressing the Training Needs of Front Line Workers and Ryan White HIV/AIDS Program Grantees