luhs handbook approval - loyola medicine admissions to the cardiology service: the following are...
TRANSCRIPT

LOYOLACARDIOLOGY
Henri Matisse: © 2015 Succession H. Matisse / Artists Rights Society (ARS), New York

INTRODUCTIONHenri Matisse (1869-1954)
The artwork featured on the front of this reference book was a work created by Henri Matisse titled “Icarus.” The myth arises from the story that Daedalus and his son Icarus, after revealing the secret of the Labarynth to the people of Greece were condemned to die in the Labarynth. They then devised a way to escape the maze by building wings of feathers and wax, but in his hubris and excitement, Icarus, failing to heed the warnings of his father, �ew too close to the sun and the wings melted and fell to his death. Daedalus, having escaped to Siciliy, and his son’s body was found by Heracles who in turn burried him near a small rock promontory in the Aegean Sea.
Matisse’s work is complex, showing Icarus in free fall, his death inevitable, but set against the bursts of sunlight and the surreal calm and peace depicted by the spot of red in place of his heart.
Mike Hushion, MD (PGY 6)Chief Cardiology Fellow
Andrew Chen, MD (PGY 3)Internal Medicine Resident
Shermeen Memon, MD (PGY 6)Chief Cardiology Fellow
Ambrose Panico, DO (PGY 5)General Cardiology Fellow
Contributors
Produced and Edited ByChris Latanich, MD (PGY 5)
General Cardiology Fellow
ADMISSIONSAdmissions to the Cardiology Service: The following are guidelines regarding who is generally appropriate for admission to the cardiology inpatient service (as opposed to a general medicine service or ICU service), each patient must be evaluated respectively and if there is any question about the propriety of an admission, it should be discussed with the fellow on service or on call.
1) Complicated Heart Failure (e.g., severe edema, recurrent admissions or 30 day readmission, inotropic or LVAD support)2) Intermediate Risk ACS3) Severe Valvular Disease4) Pericardial Disease5) Post ACS Complications (chest pain, access problems etc...)6) Non-Sustained Ventricular Tachycardia OR <1 ICD shocks7) Cardiac Syncope8) Hypertensive Urgency9) Adult Congenital Heart Disease10) Clinically Signi�cant Arrhythmias
Required Information For All Consults and Admissions: For any patient seen by the cardiology consult service and or admitted to the CCU / HTU / inpatient cardiology service, it is expected that the following records to have been obtained and in hand within 24 hours of the consultation / patient admission.
Ordering of Echocardiograms / Stress Tests: Before ordering a stress test it is imperative that you can provide some explanation of how the test will change your management of a given patient (don’t order a stress test on a patient who is 95 years old and on hospice for example).
For echocardiograms, if one was done within the last six months, there needs to have been a clear change in clinical status to justify ordering it otherwise the study will not be reimbursed and the hospital or patient will be stuck with the cost.
Name and contact number of the patient’s primary cardiologist
Angiogram (cath report)
Transthoracic echocardiogram
Stress test
Baseline EKGs (or if a patient is admitted / transferred for VT / AT the arrhythmia in question)
Lipid panel and A1c
Open heart operative reports (bare minimum is the graft anatomy)
Device interrogation report with indication for device implantation
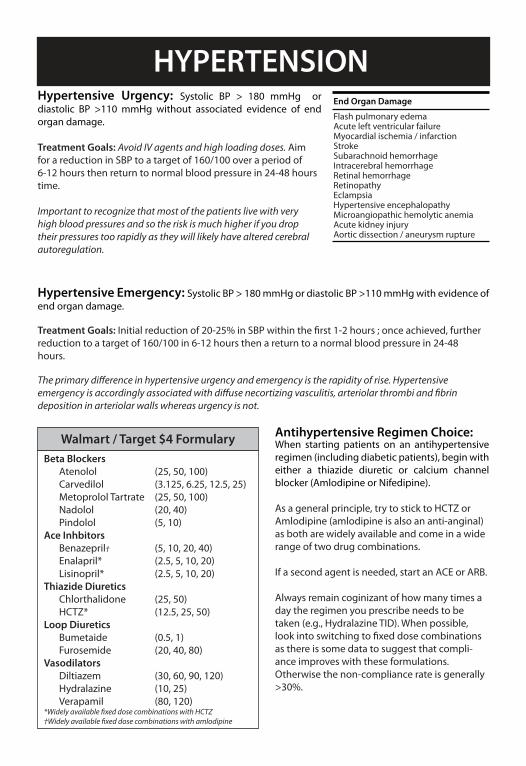
HYPERTENSIONHypertensive Urgency: Systolic BP > 180 mmHg or diastolic BP >110 mmHg without associated evidence of end organ damage.
Treatment Goals: Avoid IV agents and high loading doses. Aim for a reduction in SBP to a target of 160/100 over a period of 6-12 hours then return to normal blood pressure in 24-48 hours time.
Important to recognize that most of the patients live with very high blood pressures and so the risk is much higher if you drop their pressures too rapidly as they will likely have altered cerebral autoregulation.
Hypertensive Emergency: Systolic BP > 180 mmHg or diastolic BP >110 mmHg with evidence of end organ damage.
Treatment Goals: Initial reduction of 20-25% in SBP within the �rst 1-2 hours ; once achieved, further reduction to a target of 160/100 in 6-12 hours then a return to a normal blood pressure in 24-48 hours.
The primary di�erence in hypertensive urgency and emergency is the rapidity of rise. Hypertensive emergency is accordingly associated with di�use necortizing vasculitis, arteriolar thrombi and �brin deposition in arteriolar walls whereas urgency is not.
Antihypertensive Regimen Choice:When starting patients on an antihypertensive regimen (including diabetic patients), begin with either a thiazide diuretic or calcium channel blocker (Amlodipine or Nifedipine).
As a general principle, try to stick to HCTZ or Amlodipine (amlodipine is also an anti-anginal) as both are widely available and come in a wide range of two drug combinations.
If a second agent is needed, start an ACE or ARB.
Always remain coginizant of how many times a day the regimen you prescribe needs to be taken (e.g., Hydralazine TID). When possible, look into switching to �xed dose combinations as there is some data to suggest that compli-ance improves with these formulations. Otherwise the non-compliance rate is generally >30%.
End Organ Damage
Flash pulmonary edemaAcute left ventricular failureMyocardial ischemia / infarctionStrokeSubarachnoid hemorrhageIntracerebral hemorrhageRetinal hemorrhageRetinopathyEclampsiaHypertensive encephalopathyMicroangiopathic hemolytic anemiaAcute kidney injuryAortic dissection / aneurysm rupture
Walmart / Target $4 FormularyBeta Blockers Atenolol (25, 50, 100) Carvedilol (3.125, 6.25, 12.5, 25) Metoprolol Tartrate (25, 50, 100) Nadolol (20, 40) Pindolol (5, 10)Ace Inhbitors Benazepril† (5, 10, 20, 40) Enalapril* (2.5, 5, 10, 20) Lisinopril* (2.5, 5, 10, 20)Thiazide Diuretics Chlorthalidone (25, 50) HCTZ* (12.5, 25, 50)Loop Diuretics Bumetaide (0.5, 1) Furosemide (20, 40, 80)Vasodilators Diltiazem (30, 60, 90, 120) Hydralazine (10, 25) Verapamil (80, 120)*Widely available �xed dose combinations with HCTZ†Widely available �xed dose combinations with amlodipine

Reading an EKG may seem overwhelming at �rst but the following instructions are to help guide your evalua-tion. You should approach an EKG systemically every time, making the potential abundance of information more manageable. Approach them in the following order, even if it appears to be straightforward.
1. Rate. For a regular rhythm, count the large boxes between two QRS complexes.
For an irregular or severely bradycardic rhythm, count the number of QRS complexes on the full 12 lead EKG strip and multiplying by 10 yielding the average beats per minute.
2. Origin of Rhythm. Assess for the presence of a P-wave before every QRS, and upright P-waves in leads I and II – if present, the rhythm is likely normal sinus (60 - 100 bpm).
Inverted or abnormal P-waves suggest an ectopic atrial rhythm (P:QRS is1:1).
No P-wave with a narrow regular QRS complex suggests a junctional rhythm (40 - 60 bpm vs accelerated 60-100 bpm).
No P-wave with a wide QRS complex suggests a ventricular escape rhythm (20-40 bpm).
EKG INTERPRETATION
300 150 100 75 60 50
1 small box = 0.04 s
1 large box = 0.20 s
SA Node
VentricularEscape
AV Node
300 150 100 75 60 50
300 150 100 75 60 50 43
300 150 100 75 60 50 43

EKG INTERPRETATION3. Axis.A normal axis is positive in leads I, II and aVF. Determine the quadrant based upon the orientation of leads I and aVF (to be more precise, then �nd which lead is most isoelectric).
Left Axis Deviation (-30° to -90°):- LVH, inferior MI, WPW, ostium secundum ASD - Left anterior fascicular block (-45° to -90°): qR in aVL, no other cause of left axis deviation. QRS <100 ms unless aberrant conduction present. You cannot code a LAFB if you have an inferior MI.
Right Axis Deviation (90° to 180°): - RVH, PE, COPD, lateral MI, WPW, ostium primum ASD- Left posterior fascicular block: rS in I and aVL and qR in III and aVF, no other causes of R axis deviation - QRS narrow unless aberrant conduction present.
4. Intervals.
Step 1: Quadrant
I Normal
Left Axis
Extre
me Right
Right Ax
is
aVF
aVF
I
aVF
I
aVF
I
I isolectric / -90°
-30° II isolectric
I aVF
aVF I isolectric180°
I isolectric / 90°
aVFI
Normal
Left Axis
Extre
me Right
Right Ax
is
I / 90°
I / -90°
aVF / 180°
II / 150°
III / -150°
aVR / 120°
aVL / -120°
0° / aVF
30° / III
-30° / II
60° / aVL
-60° / aVR
Step 2: Find lead whereQRS is most isoeletric.
RR Interval
ST Interval
QT Interval
PR

EKG INTERPRETATION4. Intervals.PR Interval (normal 120 - 200 ms):
- Short PR (<120 ms): Wol�-Parkinson-White, AV nodal rhythm, low atrial ectopic rhythms. - Long PR (>200 ms): 1° aV block, higher degree heart block, hypokalemia, rheumatic fever, Lyme disease.
QRS Interval [duration] (normal 60 - 100 ms):
- Narrow QRS (<60 ms): Rarely seen. Hypocalcemia. - Wide QRS (>120 ms): Bundle branch blocks / nonspeci�c conduction delays, VT / VF, hyperkalemia, accessory pathways with preexcitation, ventricular escape rhythms.
QT Interval (normal <450 ms): Varies with heart rate (QTc ). More concerning when QTc >500 ms. - Prolonged QTc (> 450 ms): Medications (see www.qtdrugs.org), hypocalcemia, hypokalemia, hypomagnesaemia, ICH, stroke, carotid endarterectomy, neck dissection, congenital long QT (may not be present on resting EKG), K/Na/Ca channelopathies, CAD, cardiomyopathy, hypothyroidism, hypothermia.
5. Atrioventricular Blocks.1° AV Block (Physiologic): PR > 200 ms and P to QRS is 1:1. - No treatment necessary if seen in isolation
2° AV Block Type I (Wenckebach) (Physiologic): Progressive lengthening of PR interval until impulse not conducted, exhibits “grouped beating.” - No treatment necessary unless severely bradycardic or symptomatic
2° AV Block Type II (Mobitz) (Pathologic): Ocasional or repeatedly non-conducted impulses with consistent PR interval. Level of the block is typically infrahisian. - Requires pacemaker, often worsens to third degree
3° AV Block (Pathologic): Complete AV dissociation, irregular PR intervals, P waves and QRS complexes are both regular but indepentent of one another. - Morphology of QRS complex dependent on origin of escape rhythm - Requires pacemaker

EKG INTERPRETATION5. Hypertrophy and Voltage.Atrial Enlargement.
Ventricular Hypertrophy and Low Voltage. Low Voltage: Requires < 10 mm in all precordial leads and < 5 mm in all limbs. Seen with chronic lung disease ; pericardial / pleural e�usions ; obesity ; cardiomyopathies ; CAD with extensive LV infarction ; myxedema
Left Ventricular HypertrophyCornell: R in aVL + S in V3 greater than 28 mm in men / 20 mm in womenAlternate criteria for precordial and limb leads (one or more): 1) R in V5 or V6 + S in V1 > 35 mm (40 yrs) ; > 40 mm (30-40 yrs) 2) Maximum R wave + S wave in precordial leads > 45 mm 3) R wave in V5 > 26 mm ; in V6 > 20 mm 4) R wave in I + S in II > 25 mm ; R in I > 14 mm ; aVL > 12 mm ; aVF > 21 mm
Right Ventricular HypertrophyRight axis deviation with axis > 100°, downsloping ST depression and T inversions in right precordial leads and one of the following 1) R / S ratio in V1 >1 or R / S ratio in V5 or V6 < 1 2) R in V1 > 7 mm 3) rSR’ in V1 with R’ > 10 mm
6. R Wave Progression.R wave amplitude should increase with the progression of the precordial leads assuming appropriate placement and should be > 3 mm by V3. Poor progression may be caused by anteroseptal MI, LVH, dilated cardiomyopathy.
7. Q Waves.Q Waves: <30 ms common but all Q waves in V1-3 and any in I, II, aVL, aVF and V4-6 lasting over 30 ms are abnormal. For infarct identi�cation, Q waves must be seen in 2 or more contiguous leads.
Isolated Q waves in lead III are not uncommon and do not carry any known prognostic signi�cance.
Terminal portion in V1 >1 deep & 1 wide Notched P > 120 ms in II, III or aVF
LA EnlargementNormal
II
>2.5 mm in II, III & aVF>1.5 mm in V1 or V2
RA Enlargement
II V1 II

EKG INTERPRETATION8. Bundle Branch Blocks.
9. ST Segment Changes.ST Segment Identi�cation: Starting 0.06 s after J point and measure in mm relative to TP segment.
Normal ST Segments: Usually isoelectric but may vary from 0.5 mm depression to 1mm elevation in limb leads and up to 3 mm concave upward elevation in the precor-dial leads in early repolarization.
Diagnosing MI with LBBB (Sgarbossa’s Criteria): Scores ≥ 3 are 80% sensitive and 90% speci�c for AMI
10. Infarct Localization.
ST elevation ≥ 1 mm concordant with QRS in any lead.
≥ 1 mm
QRS
Axi
s
1
5 PointsST elevation ≥ 5 mm disconcordant with QRS in any lead.
≥ 5 mm
QRS
Axi
s
2
2 PointsST depression ≥ 1 mm in V1, V2 or V3.
≥ 1 mm
QRS
Axi
s
3
3 Points
NormalVariation
J point
ST Segment
Septal (LAD)
Lateral (Circ)
Inferior (PDA)
Anterior (LAD)
aVR V1 V4
aVL V2 V5
I
II
III aVF V3 V6
Left Bundle Branch BlockQRS Duration must be > 120 ms (incomplete if QRS is >100 ms but otherwise appears like a LBBB)
Lead 1: Monophasic R & no Q waves.Lead V1: QS or rS patternLead V6: Late intrinsicoid de�ection, Monophasic R & no Q waves.
I V1 V6I V1 V6
Right Bundle Branch BlockQRS Duration must be > 120 ms (incomplete if QRS is >90 ms but otherwise appears like a RBBB)
Lead 1: Wide S wave.Lead V1: Late intrinsicoid de�ection. M-shaped QRS (RSR’). Sometimes wide R or qRLead V6: Early intrinsicoid de�ection with a wide S wave.

AVNRT vs AVRTAV Nodal Reentrant Tachycardia (AVNRT): Initiated with a premature complex (PAC / PVC) and can be divided into one of two varieties: 1) typical AVNRT (antegrade conduction down slow pathand retrograde up fast path): 80-90% of cases and 2) atypical AVNRT (antegrade down fast path and retrograde up slow path): 10-20% of cases.
Rhythm is rapid and regular with normal QRS duration unless there is co-existing conduction system disease (RBBB / LBBB or a rate dependent bundle branch block).
AV Reentrant Tachycardia (AVRT): Initiated with a premature atrial complex (PAC) and can be devided into one of two varieties: 1) typical / orthodromic AVRT (antegrade conduction down fast path and retrograde up accessory path (narrow QRS) 95% of cases and 2) atypical (antidromic) AVRT antegrade down accessory path and retrograde up AV node (wide QRS) 5% of cases.
Sinus impulse conducted down fast path and
accessory path.
PAC
Refractory
SA Node
Slow Fast
Sinus impulse conducted down fast pathway (long
refractory period).
PAC occuring while fast path still refractory and
conducts down slow path.
Impulse from PAC enters ventricles and �nds fast pathway reset, travels retrograde up fast pathway and �nds slow pathway reset and creates a loop.
Termination of AVNRT via Adenosine blockade of AV node (or vagal maneuvers or DCCV). May
terminate in either a ventricular or atrial complex.
PAC
Retrograde P
AdenosineBlock
PAC travels down AV node, through ventricles and retrograde up accessory pathway
establishing loop (orthodromic / typical AVRT).
PAC
Retrograde P
Termination of Orthodromic AVRT via Adenosine blockade of AV node (or vagal maneuvers or DCCV) terminates in an atrial complex. Antidromic AVRT
terminates in a ventricular complex.
Slow Fast
SA Node
AccessoryPathway
PAC
Orthodromic Antidromic
PAC
Ort
hodr
omic
Ant
idro
mic
Orthodromic
AdenosineBlock
Antidromic
AdenosineBlock

ATRIAL TACHYCARDIAS
Sinus Beat 2:1 A Tach
Sinus Beat Focal A Tach
Sinus Beat Multifocal A Tach
P
P1 P1 P1 P1P2 P2 P2 P2P3 P3
Atrial Tachycardia: Broad term used to describe a complex of atrial tachyarrhythmias including atrial �utter. It encopmasses a discrete atrial ectopic focus driving a tachyarrhythmia and re-entrant tachycardias like atrial �utter.
Multifocal Atrial Tachycardia: Rare arrhythmia. Halmark is the identi�cation of 3+ ectoptic atrial foci driving the tachyarrhtyhmia. Treated in a similar fashion as typical focal atrial tachycardia.
Atrial Flutter: Atrial �utter rate 240 - 350 with the ventricular rate dependent upon AV conduction (may be conducting in a set ratio such as 1:4 or have variable AV conduction). Typical atrial �utter has sawtooth pattern with negative �utter waves in the inferior leads and positive �utter waves in V1.
Atrial Fibrillation: Seemingly chaotic atrial activity (mechanism is a matter of debate). Ventricular repsonse typically very irregular but may seem regular if very slow (<70 bpm) which is also indicative of signi�cant conduction system disease. Do not expect to alway see a �brillating baseline.
CHA2DS2-VASc Scoring SystemHeart Failure / L V dysfunction 1Hypertension 1Age 65-74 1 75+ 2Diabetes Mellitus 1Stroke / TIA 2PAD / Old MI / Aortic Plaque 1Female 1
Lip et. al. Chest. 2010;137(2):263-272
CHA2DS2-VASc Annual Stroke Risk0123456789 15.2%
6.7%9.6%9.8%
6.7%4.0%
3.2%2.2%
1.3%

BRADYCARDIAS Before attempting to treat a patient for symptomatic bradycardia it is imperative that you
understand the pathology driving their bradycardia as medications such as Isoproterenol, Atropine and Epinepherine can paradoxically worsen high grade heart block.
1
23
SA and AV Nodally Mediated Bradycardias
1
1
Pure sinus bradycardia driven by poor intrinsic SA nodal activity or by excess vagal tone (or drug e�ect). Stimulation with Isoroterenol or Epinepherine or disinhibition with Atropine will raise SA nodal rate.
Sinus bradycardia driven by excess vagal tone (e.g. untreated OSA). Progressive RR prolongation before potentially very long sinus pauses (sometimes 6+ seconds) while sleeping. Stimulation with Isoroterenol or Epinepherine or disinhibition with Atropine will raise SA nodal rate and improve AV nodal conduction, but typically the goal is to �x the underlying problem (e.g. CPAP).
2
Second Degree AV Block type I (Wenckebach) driven by intrinsic AV nodal delays, typically physiologic but may also be a manifestation of nodal ischemia or valvular disease. Stimulation with Isproterenol or Epinepherine or disinhibition with Atropine will typically improve AV nodal conduction but this is rarely needed.
2
2
Second Degree AV Block type I (Wenckebach) driven by intrinsic AV nodal delays, typically physiologic but may also be a manifestation of nodal ischemia or valvular disease. Stimulation with Isproterenol or Epinepherine or disinhibition with Atropine will typically improve AV nodal conduction but this is rarely needed.
2
Atrial Fibrillation with Slow Ventricular Response. Slow ventricular rates a manifestation of either high frequency stimulation of the AV node with and longer refractory periods and or of infranodal disease. Stimulation with Isproterenol or Epinepherine or disinhibition with Atropine will probably not have any signi�cant e�ect or may worsen the ventricular response, especially if there is concurrent bundle branch blocks.
Infranodal and Intra-His Mediated Bradycardias
3
Atrial Fibrillation with Slow Ventricular Response and RBBB. Slow ventricular rates likely a manifestation of high frequency stimulation of the AV node compounded by concurrent infranodal disease with hyperpolarization of the his bundles causing longer refractory periods. Stimulation with Isproterenol or Epinepherine or disinhibition with Atropine may worsen the bradycardic response by augmenting the his bundle hyperpolarization and refractoriness.
3
Second Degree AV Block type II (Mobitz) driven by infrahisian conductoin system disese. Stimulation with Isproterenol or Epinepherine or disinhibition with Atropine may worsen the bradycardic response by augmenting the his bundle hyperpolarization and refractoriness.
2
Complete Heart Block. Slow ventricular rate a manifestation of the secondary pacemaker site (narrow QRS junctional, wide QRS may be fascicular or ventricular). Stimulation with Isproterenol or Epinepherine or disinhibition with Atropine may accelerate the secondary pacemaker but if the patient is in any way unstable should have transcutaneous pacing preferentially.
Atropine orIsoproterenol
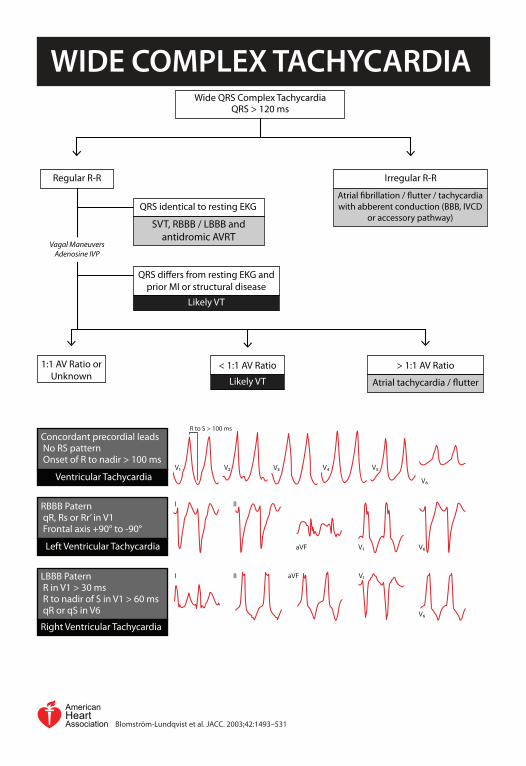
WIDE COMPLEX TACHYCARDIA
Regular R-R
1:1 AV Ratio or Unknown
Wide QRS Complex TachycardiaQRS > 120 ms
Irregular R-R
Atrial �brillation / �utter / tachycardia with abberent conduction (BBB, IVCD
or accessory pathway)
Vagal Maneuvers Adenosine IVP
SVT, RBBB / LBBB and antidromic AVRT
QRS identical to resting EKG
Likely VT
QRS di�ers from resting EKG and prior MI or structural disease
< 1:1 AV Ratio
Likely VT Atrial tachycardia / �utter
> 1:1 AV Ratio
Concordant precordial leads No RS pattern Onset of R to nadir > 100 ms
Ventricular Tachycardia
RBBB Patern qR, Rs or Rr’ in V1 Frontal axis +90° to -90°
Left Ventricular Tachycardia
LBBB Patern R in V1 > 30 ms R to nadir of S in V1 > 60 ms qR or qS in V6
Right Ventricular Tachycardia
V6
V5V4V3V2V1
R to S > 100 ms
I II
aVF V1 V6
I II aVF V1
V6
AmericanHeartAssociation Blomström-Lundqvist et al. JACC. 2003;42:1493–531

CHEST PAIN EVALUATIONDe�nitions of angina:
Typical Angina (De�nite): Substernal chest pain or discomfort that is 1) provoked by
exertion or emotional stress and 2) relieved by rest and/or nitroglycerin.
Atypical Angina (Probable): Chest pain or discomfort that lacks one of the characteristics of de�nite or typical angina.
Nonanginal Chest Pain: Chest pain or discomfort that meets one or none of the typical angina characteristics.
ELECTROCARDIOGRAPHY - LEAD PLACEMENT
4th right intercostal space V1
V2 4th left intercostal space Directly between V2 and V4V3
5th left ICS at the MCLV4
V5 5th left ICS at ant ax line5th left ICS at mid ax lineV6
5th right ICS at the MCLV4r
V5r 5th right ICS at ant ax line5th right ICS at mid ax lineV6r Right ArmRA
LA Left ArmLeft LegLL
Right LegRL
Diamond and Forrester Pre-Test Probability of Coronary Artery Disease
<40 Man 10-90% 10-90% <10%
Woman 10-90% <5% <5%
40-49 Man >90% 10-90% 10-90%
Woman 10-90% <10% <5%
50-59 Man >90% 10-90% 10-90%
Woman 10-90% 10-90% <10%
>60 Man >90% 10-90% 10-90%
Woman >90% 10-90% 10-90%
Age (Years) Sex Typical Angina Atypical Angina Nonanginal Chest Pain
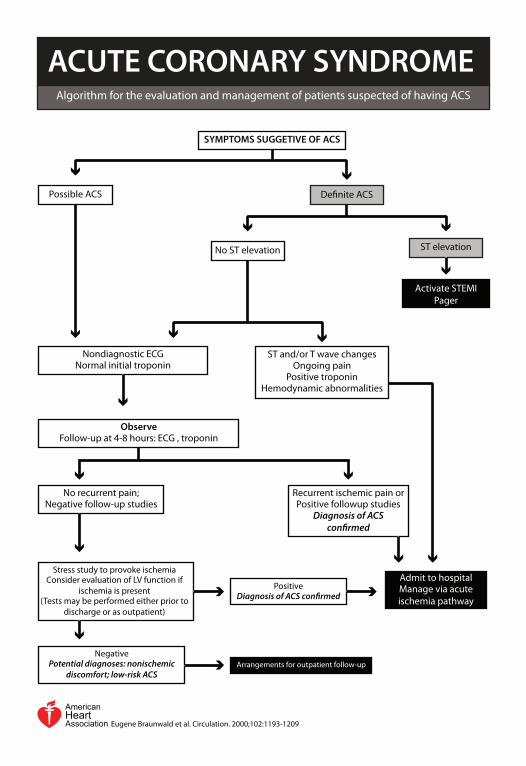
ACUTE CORONARY SYNDROMEAlgorithm for the evaluation and management of patients suspected of having ACS
AmericanHeartAssociation Eugene Braunwald et al. Circulation. 2000;102:1193-1209
SYMPTOMS SUGGETIVE OF ACS
Possible ACS De�nite ACS
No ST elevation ST elevation
Activate STEMI Pager
Nondiagnostic ECGNormal initial troponin
ST and/or T wave changesOngoing pain
Positive troponinHemodynamic abnormalities
Recurrent ischemic pain orPositive followup studies
Diagnosis of ACS con�rmed
ObserveFollow-up at 4-8 hours: ECG , troponin
Admit to hospitalManage via acute ischemia pathway
No recurrent pain; Negative follow-up studies
PositiveDiagnosis of ACS con�rmed
NegativePotential diagnoses: nonischemic
discomfort; low-risk ACSArrangements for outpatient follow-up
Stress study to provoke ischemiaConsider evaluation of LV function if
ischemia is present(Tests may be performed either prior to
discharge or as outpatient)

ACUTE ISCHEMIA PATHWAY
Immediate angiography 12-24 hour angiography Recurrent symptoms/ischemia
Heart failureSerious arrhythmia
Not low risk Low risk
Follow on medical Rx
Recurrent ischemia and / or ST segment shift, or
Deep T-wave inversion, or Positive troponin
AspirinBeta blockers
NitratesAntithrombin Regimen
GP IIb/IIIa inhibitorMonitoring (rhythm and ischemia)
Early invasive strategy Early conservative strategy
Patient stabilizes
Evaluate LV Function
LVEF >40%LVEF <40%
Stress Test
AmericanHeartAssociation Eugene Braunwald et al. Circulation. 2000;102:1193-1209

ACUTE CORONARY SYNDROMENot all troponin leaks are secondary to acute myocardial infarction. THINK is the TROPONIN ELEVATION due to PLAQUE RUPTURE or secondary to another underlying cause.
STEMI: Clinical syndrome de�ned by 1) symptoms of myocardial ischemia in association with 2) persistent ECG ST elevation and 3) subsequent release of biomarkers of myocardial necrosis.
1) New ST elevation at the J point in at least 2 contiguous leads of 2+ mm in men or 1.5+ mm in women in leads V2–V3 and or of 1 mm in other contiguous chest leads or the limb leads.2) New or presumably new LBBB3) ST depression in 2 precordial leads (V1–V4) may indicate transmural posterior injury4) Multilead ST depression with coexistent ST elevation in lead aVR has been described in patients with left main or proximal left anterior descending artery occlusion. 5) Hyperacute T-wave changes may be observed in the very early phase of STEMI, before the development of ST elevation
NSTEMI: Clinical syndrome de�ned by 1) symptoms, 2) absence of persistent ST elevation but can have other ST-T wave changes, and 3) release of cardiac biomarkers (2 of 3 criteria must be met).
Unstable Angina: Clinical syndrome de�ned by 1) symptoms, 2) absence of persistent ST elevation but can have other ST-T wave changes, and 3) release of cardiac biomarkers.
Type 1 Myocardial Infarction
Type 2 Myocardial Infarction(Demand Ischemia)
Vasospasm or endothelial dysfunction
Fixed atherosclerosis andsupply demand imbalance
Supply demand imbalance alone
Plaque rupture with thrombus
Troponin without reperfusionTroponin with reperfusionCKMB without reperfusionCKMB with reperfusion
x U
pper
Lim
it of
Nor
mal
1
2
5
10
20
100
1 2 3 4 5 6 7 80
Days from Onset of Infarction
0

ACUTE CORONARY SYNDROME
Indicator of 35 day composite events risk (mortality, new or repeat MI, severe recurrent ischemia requiring urgent revascularization through 14 days after admission).
1) Age >65 years2) 3+ cardiac risk factors3) Prior coronary stenosis >50%4) ST segment deviation on admission ECG5) >2 anginal events in the last 24 hours6) Aspirin treatment in the prior 7 days7) Prior congestive heart failure, MI, CABG or PCI
TIMI Risk Score (NSTEMI)
0
10
20
30
40
50
0-1 2 3 4 5 6-7
Com
posi
te R
isk
(%)
Medications to be started immediately (these have survival bene�ts) to be administered to all patients (unless clear contraindication).1. Aspirin 325 mg PO once followed by Aspirin 81 mg PO daily2. Heparin drip (intermediate algorithm with bolus)3. Lipitor 40-80 mg PO QHS4. Plavix / E�ent / Brilinta (P2Y12 inhibi-tors) should not be started unless told to do so explicitly by the cardiology fellow or attending. If started before you know if the patient will need CABG it may delay surgery for a week. If they are already taking one of these agents however`, they should be continued.
Medications to be started before discharge (these have survival bene�t but do not need to be started immediately). 5. Beta blocker (typically Metoprolol or Carvedilol)6. Ace inhibitor / ARB if LVEF <40%, comorbid hypertension, diabetes or CKD
Medications for symptomatic relief or minimal if any survival bene�t.7. Nitroglycerin 0.3 - 0.4 mg SL Q5min x 3 PRN for continuing angina and consider starting IV nitroglycerin.8. Supplemental oxygen only if SaO2 <90% or respiratory distress
Ancillary testing to be obtained on all patients admitted with an acute coronary syndrome:1) Lipid panel2) Hemoglobin A1c3) Transthoracic echocardiogram (with de�nity if a large anterior wall MI or concern for aneurysm formation which could predispose to LV thrombus forma-tion.

CARDIAC CATHETERIZATION
Common Angiographic Views
Routine cardiac catheterizations are performed Monday through Friday (7:00 am to 5:00 pm) urgent and emergent cases are performed after hours. Cases typically performed with local anaesthesia and light conscious sedation (Versed and Fentanyl).
Before requesting a procedure be done for a patient, there must be a reasonable risk bene�t assessment and the expectation that the information or therapeutics gleaned from the study will o�set the risks of the procedure.
Pericardiocentesis (30 min): E�usion must be accessible by a subcostal or apical approach.
Right heart catheterization (10-15 min): With shunt run this becomes much longer, usually around 45 minutes to 1 hour.
Left heart catheterization (30 - 60 min): If done as part of an aortic valve study (with or without dobutamine) it will add roughtly another 30 min. Stenting can usually be done at the same time as the angiogram but the time it takes to complete varies greatly with complexity of the intervention.
Balloon Pump Placement (15 - 45 min): If removing a prior balloon pump, add another 30 minutes to the procedure to achieve hemostasis.
Left Main
LAD
Circum�ex
RCA
PDA
Left Main
LAD
Circum�ex
RCA
PDAPDA
Left Main
LAD
Circum�ex
RCA
Contraindications
INR > 2
Platelets < 50
AKI (Angiogram)
Hemodynamically Unstable
Active Hemorrhage
Stroke / CNS Bleed
Preprocedure Checklist
BMP
CBCEKG
INR NPO
Consent
Images courtesy of Patrick J. Lynch

VALVULAR HEART DISEASE
Image courtesy of Patrick J. Lynch
AmericanHeartAssociationNishimura et. al. J Am Coll Cardiol. 2014;63(22):e57-e185
Normal Mild Moderate Severe
Aortic Stenosis Velocity (m/s) <2 2.0 - 2.9 3.0 - 3.9 >4.0 Mean Pressure Gradient (mmHg) <10 <20 20 - 39 >40 Valve Area >2 >1.5 1.0 - 1.5 <1.0 Aortic Regurgitation Vena Contracta (cm) <0.3 0.3 - 0.6 >0.6Mitral Stenosis Planimetry MV Area (cm2) >1.5 1.0 - 1.5 <1.0 DIastolic Pressure Half Time (ms) <150 >150 >220 Mean Pressure Gradient (mmHg) <5 5 - 10 >10Mitral Regurgitation Vena Contracta (cm) <0.3 <0.7 >0.7 ERO (cm2) <0.4 >0.4
American Society for Echocardiography Reference Ranges
Medtronic CoreValve Evolut
Medtronic Mosaic Bovine Pericardial
St. Jude Mechanical

CARDIAC DEVICES
Device Program Coding
Dual Chamber Pacemaker RV & RARV & RA
ShockATPPacing
TherapiesSensing
CSRVRA
Device Type Leads
Single Chamber Pacemaker RVRV
Biventricular Pacemaker (CRT-P) RA / BiVRA / RV / CS
Subcutaneous ICD (SC-ICD) SC Coil
Biventricular De�brillator (CRT-D) RA / BiVRA / RV / CS
Dual Chamber De�brillator (ICD) RV & RARV & RA
Single Chamber De�brillator (ICD) RVRV
Designed to treat tachyarrhythmias (primarily VT / VF) most de�brillators also have the ability to treat bradyarrhythmias via a pacing function (with the exception of subcutaneous ICDs which only de�bril-late).
DEFIBRILLATORSDesigned to treat bradyarrhythmias. They only pace when the patient’s intrinsic heart rate is less than the programmed lower rate limit. They do not treat tachyar-rhythmias.
PACEMAKERS
Right Atrial Lead (RA) (Pace / Sense)
Right Ventricular Lead (RV) (Pace / Sense / De�brillate)
Coronary Sinus Lead (CS) (Pace / Sense)
Pulse Generator
Standard coding involves three letters. 1st denotes which chambers are paced. 2nd denotes which chambers are monitored for intrinsic activation. 3rd denotes the response to a native activation.
Most common modes:DDD - Paces both RA and RV (sometimes BiV). Monitors RA and RV. Detections may trigger a pacing impulse or inhibit depend-ing upon their timing. VVI - Paces RV. Monitors RV. Detections inhibit pacing.
AAI - Paces RA. Monitors RA. Detections inhibit pacing.
AAI <-> DDD - Converts between modes when in AFib or Flutter.

EP PROCEDURESRoutine electrophysiology procedures (device implantations and ablations) are performed Monday through Friday (7:00 am to 5:00 pm) urgent and emergent cases are performed after hours. Pacemak-ers are often performed with local anaesthesia and conscious sedation (Versed and Fentanyl) but more complex procedures will typically be performed with anaesthesia.
Before consulting the electrophysiology service there must be a risk bene�t assessment and a reasonable expectation of quality and life and expected survival of at least one year from any device implantation or upgrade. Similarly if the patient has bradycardia or other arrhythmias due to reversible causes or remediable problems such as electrolye derrangements, sleep apnea or digoxin toxicity, they are generally not appropriate candiates for device implantation.
Single or Dual Chamber Pacemaker Implantation (60 min): Indicated for 1) symptomatic bradycardia or chronotropic incompetence, 2) high grade heart block, 3) alternating bundle branch blocks, 4) sinus pauses while awake of >3 seconds and 5) atrial �brillation conversion pauses while awake of >5 seconds.
Cardiac Resynchronization Therapy (CRT-P / CRT-D) (1 - 3 hours): Indicated for patients with an LVEF <35% and a QRS duration >120 ms in sinus rhythm with class III or ambulatory class IV heart failure despite optimal medical therapy.
De�brillator Implantation (60 min): Indicated for 1) patients who survived a cardiac arrest from VF / VT or sustained VT after exclusion of reversible causes and 2) patients with an LVEF <35% (and at least 40 days post MI if their heart failure is ischemic in nature) and are in NYHA class I-III heart failure.
Atrial Flutter Ablation (1 - 2 hours): Indicated as front line therapy for treatment of typical atrial �utter. If onset of atrial �utter is > 48 hours before the procedure or the patient has not been on anticoagulation, they will usually require a TEE �rst.
Atrial Fibrillation Ablation (4 - 6 hours): Typically this is a very complicated procedure and generally only done as an outpatient.
Ventricular Tachycardia Ablation (4 - 8 hours): Potentially a very complicated procedure and given the length of the procedure usually requires 2-3+ L of IVF being given to prevent thermal burns from the ablation catheters (require continuous �ushing).
Preprocedure Checklist
BMP
Type and Screen
INR
CBC
NPO
Heparins stopped at least 12 hours earlier
NOACs held as directed
Coumadin OK to continue
Post Device Implantation Checklist
Site dressings managed by EP Service
Do NOT restart any heparins or NOACs (this includes DVT prophylaxis) for 1-2 weeks
Coumadin OK to continue Chest XR ( PA / Lateral) in AM
Device interrogation in AM

HEART FAILUREVolume Status vs Perfusion: Volume status: Jugular vein distention (JVD), hepato-jugular re�ux, peripheral edema, orthopnea, PND, rales.
Perfusion: Look for evidence of end organ hypoperfu-sion (cool extremities, renal failure, acidosis, altered mental status etc...).
It is extremely important to remember that these are not problems occuring in isolation and in most patients, there is a mix of both problems at any one given time.
ACC / AHA Stage
High risk for heart failure but without structural heart disease or symptoms. A
Structural heart disease without heart failure.B
Structural heart disease with prior or active heart failure.C
Refractory heart failure requring specialized interventions.D
I Asymptomatic
II Symptoms with moderate exertion
III Symptoms with minimal exertion
IV Symptoms at rest
NYHA Stage1 Year
Mortality
5-10%
15-30%
50-60%
Based on comorbidities
Documentation:Your note must stipulate acute, chronic or acute on chronic systolic or diastolic heart failure. Terms such as HFpEF and HFrEF are not acceptable. After establishing the etiology (if known), you need to note the ACC and NYHA stage as detailed above.
Initial Management:Once you identify the major problem (volume overload and or poor stroke volume) tailor treatment accordingly (diuretics or dialysis for volume overload and inotropes, balloon pumps and LVADs for poor LV function).
Right Heart Catheterization:The use of pulmonary artery catheters to guide heart failure managment was formally evaluated in the ESCAPE trial (PMID 16204662). This study failed to show any bene�t to the use of pulmonary artery catheters to guide therapy over just clinical assessment of volume status. There is currently no well agreed indication for pulmonary artery catheter placement to guide therapy outside of document-ing inotrope dependence.
Measure JVD in CM above sternal notch (measured + 5).Normal is 7-9
45 Degrees
Agent Onset Duration BioavailabilityLasix (40 mg PO) 30-60 min 6-8 hrs 50%Lasix (20 mg IV) 5 min 2 hrs 100%Bumex (1 mg PO) 10 min 4-6 hrs 80%Demedex (10 mg PO) 1 hr 4-6 hrs 90%Metolazone (PO) 60 min >24 hrs
Diuretic Equivalence

HEMODYNAMICS
ECG25
0mmHg
25
0mmHg
25
0mmHg
av
y
c25
0mmHg
x
Aortic ValveOpens
Mitral ValveCloses
Aortic ValveCloses
Mitral ValveOpens
edp
125
100
75
50
25
0mmHg
125
100
75
50mmHgSystole
DDiastole Systole
E
Aortic ValveOpens
Aortic ValveCloses
A
B
C
Native Pressures
With IABP On
RA
RV
PCWP
Ao
LV
IABP
Ao
PAReference Ranges
Right Atrium a wave 2 - 7 mmHg v wave 2 - 7 mmHg Mean 1 - 5 mmHg
Right Ventricle Systolic 15 - 30 mmHg EDP 1 - 7 mmHg
Pulmonary Artery Systolic 15 - 30 mmHg Diastolic 4 - 12 mmHg Mean 9 - 19 mmHg
Pulmonary Capillary Wedge Mean 4 - 12 mmHg
Left Ventricle Systolic 90 - 140 mmHg EDP 5 - 12 mmHg
Aortic Systolic 90 - 140 mmHg Diastolic 60 - 90 mmHg Mean 70 - 105 mmHg
Cardiac Index > 2.5 L/min/m2
Swan Daily Rounds
Chest XR for catheter position
Assessment of insertion site
Pulmonic ValveOpens
Pulmonic ValveCloses
Tricuspid ValveCloses Tricuspid Valve
Opens
a cx
v y

BALLOON PUMPS
Diastole Systole
0 30 60 90 120 150 180 210 240 270 300 330 360 390 420Days after randomisation
p=0·94; log-rank testRelative risk 1·02, 95% CI 0·88–1·19
0
10
20
30
40
50
60
Mor
talit
y (%
)
IABPControl
All Cause Mortality from SHOCK II Trial (IABP Support in ACS with Cardiogenic Shock)
Systole Diastole
125
100
75
50mmHg
Native Pressures
IABP Augm
entation
Coronary PerfusionAugmentation
Bene�t is garnered by a reduction in the work required by the LV during systole (balloon de�ates providing a partial vacuum into the aorta) and an increase in the diastolic pressure (during coronary perfusion).
The use of intraaortic balloon pumps for the treatment of acute cardiogenic shock has mostly been studied in cases of an acute coronary syndrome (such was the subject of the SHOCK II trial). They are also commonly used in cases of cardiogenic shock from other etiologies such as fulminant myocarditis or acute on chronic systolic heart failure. In ACS patients their use has failed to show bene�t as shown above. In the other situations, there is little if any data to assess their value.
Proper placement of IABP with radio-opaque marker just below aortic arch and about the level of the carina.
Balloon Pump (IABP) Daily Rounds
Chest XR to con�rm IABP position
Most recent aPTT and trend
Assessment of IABP insertion site
Assessment of pedal pulses and perfusion
Heparin drip (low dose nomogram)
Balloon Pump (IABP) Anticoagulation
Image redrawn from Jones et. al. J Invasive Cardiol 2012; 24:544-550

LEFT VENTRICULAR ASSIST DEVICES
Inlet (LV) Pressure Outlet (Aortic) Pressure
Pres
sure
(mm
Hg)120
90
60
30
0
Flow
(L/m
in)
8
6
4
2
0
Two models in use are the Heartmate II and HeartWare.
Both have a mechanical pump which draws blood from the LV cavity at the apex and shunts it to the aortic root. This augments the native LV function and there is usually a pulse during systole. Occasionally, the residual LV function is so poor that there is no palpable pulse and the aortic valve does not open.
To measure blood pressure in these patients use a manual cu� and a doppler probe, record the �rst audible sound during de�ation as the MAP (goal is 70-80 mmHg).
Reported Pump Parameters:
Pump Speed (Set)
Power (Measured)
Flow (Estimated)
Pulse Index (Estimated)
Characteristic Electrical Baseline EKG Intereference
Pump Flow
LVAD Flow and Pressure

HEARTWARE LVAD (HVAD)
4.3L/min
2920RPM
4.2Watts
Fixed
Sx O�
1 2 HeartWareHW123456722:43:56
POD: 8
TimeScale
9 8 7 6 5 4 3 2 1Time (s)
12
8
4Pow
er (W
atts
)
9 8 7 6 5 4 3 2 1Time (s)
12
8
4Flow
(L/m
in)
Critical Alarms
Steady Tone
NO MESSAGE - No power to pump / Pump has stopped
VAD STOPPED - Driveline disconnected, fracture or connector malfunction. VAD electrical failure, Controller / VAD Failure. Thrombus or other material in device.
CONTROLLER FAILED - Controller Component Failed
CRITICAL BATTERY - Limited battery life remaining or malfunction.
The nursing sta� has been trained to care for most of these scenarios. In the event of repeated alarms, notify the on call fellow immediately.
Patient System Controller Display(Attached via Driveline)
HeartWare
3000 RPM 5.0 L/min4.8 Watts
Alarm Mute Battery Indicator 2Alarm IndicatorScroll
Battery Indicator 1
Two Tone
Flashing Red
1800 2400 3200 4000
2.5 8.5
103 81.8
Power (Watts)
Set Speed (RPM)
Flow (L/min)
INR 1 2 3 4
HeartWare HVAD Function Reference Ranges
Con�rmation of pump speed
Pump �ow and power trends
Hgb, PLT and LDH trends
Arrhythmia review
Suction event review
INR
HeartWare HVAD Daily Rounds
Aspirin 325 mg PO QD
Coumadin (INR 2-3)
HeartWare HVAD Anticoagulation
Reprinted with the permission of HeartWare ©

HEARTMATE LVAD (LVAD)Clinical Settings Alarms Save Data History Admin
Pump Flow Pump Speed Pulse Index
Display ON/OFF
9500rpm3.6
Pump Power
5.7w
4.5 lpm
Fixed Mode - Speed Setpoint: 9600 rpm
Test SelectButton
Power Symbol Controller CellSymbol
Red HeartSymbol
Silence AlarmButton
Battery Symbol(yellow & red)
Battery Fuel Gauge
Critical AlarmsRed Heart
Steady Tone
Pump �ow < 2.5 Lpm, pump has stopped, perc lead is disconnected, or pump is not working properly.
Red Battery
Steady Tone
< 5 min battery power remains, voltage too low, or the System Controller is not getting enough power.
Yellow Battery
1 Beep Q4 seconds
< 15 min battery power remains, voltage too low, or the System Controller is not getting enough power.
The nursing sta� has been trained to care for most of these scenarios. In the event of repeated alarms, notify the on call fellow immediately.
Patient System Controller Display(Attached via Driveline)
6K 8K 10K 15K
2.5 10
3 102.5
Power (Watts)
Set Speed (RPM)
Flow (L/min)
INR 1 2 3 4
LVAD Functional Reference Ranges
Con�rmation of pump speed
Pump �ow, PI and power trends
Hgb, PLT and LDH trends
Arrhythmia review
PI / Suction event review
INR
HeartMate II LVAD Daily Rounds
Aspirin 325 mg PO QD
Coumadin (INR 2-3)
HeartMate II LVAD Anticoagulation
Reprinted with the permission of Thoratec Corporation ©
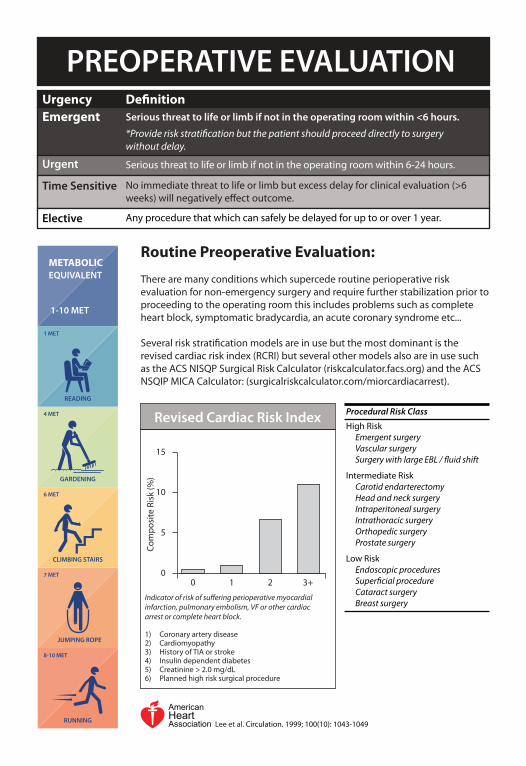
PREOPERATIVE EVALUATION
Routine Preoperative Evaluation:
There are many conditions which supercede routine perioperative risk evaluation for non-emergency surgery and require further stabilization prior to proceeding to the operating room this includes problems such as complete heart block, symptomatic bradycardia, an acute coronary syndrome etc...
Several risk strati�cation models are in use but the most dominant is the revised cardiac risk index (RCRI) but several other models also are in use such as the ACS NISQP Surgical Risk Calculator (riskcalculator.facs.org) and the ACS NSQIP MICA Calculator: (surgicalriskcalculator.com/miorcardiacarrest).
JUMPING ROPE
7 MET
8-10 MET
RUNNING
6 MET
CLIMBING STAIRS
EQUIVALENT
1-10 MET
METABOLIC
4 MET
GARDENING
1 MET
READING
UrgencyEmergent Serious threat to life or limb if not in the operating room within <6 hours.
*Provide risk strati�cation but the patient should proceed directly to surgery without delay.
De�nition
Urgent Serious threat to life or limb if not in the operating room within 6-24 hours.
Time Sensitive No immediate threat to life or limb but excess delay for clinical evaluation (>6 weeks) will negatively e�ect outcome.
Elective Any procedure that which can safely be delayed for up to or over 1 year.
Procedural Risk Class
High Risk Emergent surgery Vascular surgery Surgery with large EBL / �uid shift
Intermediate Risk Carotid endarterectomy Head and neck surgery Intraperitoneal surgery Intrathoracic surgery Orthopedic surgery Prostate surgery
Low Risk Endoscopic procedures Super�cial procedure Cataract surgery Breast surgery
Indicator of risk of su�ering perioperative myocardial infarction, pulmonary embolism, VF or other cardiac arrest or complete heart block.
1) Coronary artery disease2) Cardiomyopathy3) History of TIA or stroke4) Insulin dependent diabetes 5) Creatinine > 2.0 mg/dL6) Planned high risk surgical procedure
Revised Cardiac Risk Index
0 1 2 3+0
5
10
15
Com
posi
te R
isk
(%)
AmericanHeartAssociation Lee et al. Circulation. 1999; 100(10): 1043-1049

PREOPERATIVE EVALUATIONAlgorithm for the risk evaluation of patients prior to surgery
AmericanHeartAssociation
Patient scheduled for surgery with known or risk factors for CAD
Estimated perioperative risk of MACE based on combined clinical / surgical
risk (RCRI etc...)
Functional capacity <4 METs or unknown
Will further testing impact decision making or perioperative care?
Pharmacologic stress testing with angiography and
revascularization as indicated
Proceed to surgery or alternate management
as appropriate
Nonemergent surgical case Emergent surgical case
Clinical risk strati�cation and proceed directly to
surgeryClinically stable Acute coronary syndrome
Evaluate and treat accordingly
Low risk (<1%) Elevated risk (>1%)
Functional capacity >4 METs
No further testing
Proceed to surgeryYesNo

PREOPERATIVE CHECKLISTEKG Should be obtained in patients with known CAD/PAD, arrhythmia, cerebro-
vascular disease, or other signi�cant structural disease except those undergoing low risk surgery.
It should also be considered in patients without above risks factors except those undergoing low risk surgery
Echocardiogram Pre-operative echo should be obtained in patients with dyspnea of unknown origin to assess LV function, known heart failure with change in clinical status, re-assessment of LV function in clinically stable patients with previously documented decreased LV function if there has been no assessment within a year.
Stress Test Reasonable for patients at elevated risk for noncardiac surgery with poor functional capacity to undergo either exercise/dobutamine stress echo or myocardial perfusion scan if it will change management
Please refer to stress testing and ACC pre-operative algorithm.
Angiogram Routine preoperative coronary angiography is not recommended per ACC guidelines
Beta Blockers Continue beta blockers in patients on them chronically. In patients with intermediate or high preoperative test (RCRI>3), it may be reasonable to begin beta blockers prior to surgery.
Do not initiate beta blockers in the immediate pre-operative period (at least 2-7 days prior to surgery).
Statins Continue statins in patients on them chronically. Consider initiating statins before vascular surgery or those with one clinical risk factor. Can consider initiating prior to elevated risk surgery in patients who already meet an indication for statin therapy.
ACE / ARB Reasonable to continue perioperatively if already on them chronically. If held, restart as soon as safe following surgery.
Antiplatelets Continue DAPT in patients undergoing urgent noncardiac surgery in the �rst 4 to 6 weeks after BMS or DES implantation, unless risks of bleeding outweigh risk of stent thrombosis. Patients with stents undergoing surgery that requires discontinuation of P2Y12 inhibitors, continue aspirin and restart P2Y12 inhibitor as soon as possible following surgery. In those undergoing nonurgent surgery and without prior stents, it may be reason-able to continue aspirin if patient at high risk of cardiac events and bene�ts outweighs risk of bleeding.

CARDIAC IMAGINGModality Advantages Limitations / Contraindication
Ideal in low to intermediate risk patients who can exercise enough to get to target heart rate and have an interpretable ECG.
Provides functional capacity.
Cannot use if patient has baseline LBBB or paced rhythm.
Cannot perform in a patient having ACS or recent MI, severe symptomatic AS, aortic dissections, or acute PE.
Exercise ECGExercise should be attempted in any stress modality which its felt the patient can reasonably achieve target heart rate.
Appropriate in wide range of pre-test probability patients.
Can assess viability
Balanced ischemia in triple vessel disease may lead to false negatives.
Cannot use in pregnant patients, with hypotension (SBP<90), high degree AV block, active wheezing.
Myocardial Perfusion ImagingRegadenoson or Adenosine
No radiation exposure
Appropriate in a wide range of pre-test probability patients.
Can assess viability
Can obtain additional hemody-namic data during stress.
Can be limited by poor patient echo windows – obese patients, etc.
Cannot use in symptomatic severe AS, aortic dissection, ACS.
Stress EchoDobutamine
Contraindicated in patients with recent ACS, tachyarrhythmias, uncontrolled hypertension (SBP>200/110), aortic dissections and large aneurysms.
No radiation exposure
Can assess for viability/scar
Excellent structure/anatomy imaging
Appropriate in intermediate and high pretest risk patents.
Requires high technical skill
Needs optimal heart rate and should be able to participate in breath holds.
No functional capacity is obtained.
Stress MRIGFR must be >30
ICD/Pacemakers limit study quality.
Option for low to intermediate risk patients with normal ECG and normal cardiac biomarkers.
Excellent tool for assessing anatomy of coronary arteries.
High negative predictive value
Contrast dye exposure
Limited to larger caliber more proximal vessels.Patient will need to perform breath holds and have a controlled heart rate.
Cannot use in pregnancy
Coronary CTACan potentially end up with double contrast dye exposure if positive.
Functional assessment with CT-FFR.
NOT a stress test
Optimal test for high pretest probability, positive stress tests, and those with acute coronary syndromes.
Invasive with risks of complications such as bleeding
Contrast dye exposure
Cardiac CathGold standard study for CAD.

SYNCOPE
<40 40-60 >60Age (Years)
100%
0%
20%
40%
60%
80%
Etio
logy
of S
ynco
pe (%
)
Structural Disease
Arrhythmia
Orthostatic
Neurally Mediated
Inappropriate Re�ex
CerebralHypoperfusion
Low Vasc
ular
Res
istan
ce Low Cardiac O
utput
Cardiac (Pulmonary)
Poor Venous Return
Autonomic Failure
Norm
al A
uton
oics
Arrhythmia
StructuralO
ther
Secondary ANF
Primary ANF
MixedCard Inhib
Vaso
depressor
Drug
Indu
ced
Dys
auto
nom
ia
Volume LowVenous P
ool
Orthostatic Hypotens
ion
Cardiac Syncope
Re�ex Syncope
Physiologic Basis of Syncope: Any mechanism which causes a transient drop in cerebral blood �ow below 50-60 mL/min for at least 6-8 seconds can result in syncope.
*Syncopized is not a word. Syncopated refers to accentuating the o� beats in music. Neither refers to syncope. Don’t ever say it again.
Orthostatic Hypotension: Drop in CBF because of either volume depletion, excess venous pooling or a failure of compensatory vasoconstriction. Further deliniation requires closer assessment of autonomic function and volume status. -Compression stockings -Fludricortisone -Medication review (may need to stop o�ending drugs like alpha blockers etc...)
Re�ex Syncope: Drop in CBF via sudden changes in e�erent autonomic activity, especially parasympa-thetic, causing bradycardia and a release of sympathetic tone causing a drop in vascular resistance (in other words vasodilation). Look for common triggers like going to the bathroom or around the time of procedures (EGD, C-scope, cystoscopy, carotid massage etc...) or psychologic stress like seeing blood or extreme fear. -Increased salt and water intake -Counterpressure maneuvers -No data to support use of any medications except possibly beta blockers in patients over 40
Cardiac Syncope: Drop in CBF Pretty straight forward subgroup with either structural lesions (HOCM or severe AS) or arrhythmias as the mechanism. -Treatment of underlying process
TelemetryEchocardiogram with dopplerOrthostatic Vital Signs EKG
Initial Diagnostic Evaluation
Clearly documented that patient is restricted from driving if no immediately reversible cause is identi�ed
Driving Restrictions

INO
TRO
PIC
AG
ENTS
Age
nt (M
OA
)D
ose
Rang
e
Milr
inon
e (c
GM
P / P
DE3
)0.
20 -
0.50
mcg
/ kg
/ m
in
Clea
ranc
e (t
½)
Rena
l ~80
% (2
.3 h
rs)
PDE3
- cG
MP
med
iate
d in
crea
se in
in
trac
ellu
lar i
ntra
cellu
lar C
a++
conc
entr
atio
n an
d co
nseq
uent
rise
in
con
trac
tility
and
CI.
Dec
reas
es
SVR
/ PVR
.
Prim
ary
Act
ivit
y
Dob
utam
ine
(β1 +
+ / β
2 +)
2.5
- 10
mcg
/ kg
/ m
inRe
nal (
2 m
inut
es)
Beta
1 re
cept
or m
edia
ted
incr
ease
in
car
diac
con
trac
tility
and
HR.
D
ecre
ase
in S
VR v
ia B
eta
2 m
edi-
ated
vas
odila
tion.
Epin
ephe
rine
(β1
/ β2 /
α1)
1 - 2
0 m
cg /
min
Rena
l 100
% (1
min
)Be
ta 1
rece
ptor
med
iate
d in
crea
se
in c
ardi
ac c
ontr
actil
ity a
nd H
R.
Incr
ease
s SV
R vi
a po
tent
Alp
ha
activ
ity.
Nor
epin
ephe
rine
(β1
/ α1)
0.02
- 1.
0 m
cg /
kg /
min
Rena
l 100
% (1
min
)Be
ta 1
rece
ptor
med
iate
d in
crea
se
in c
ardi
ac c
ontr
actil
ity a
nd H
R.
Incr
ease
s SV
R vi
a po
tent
Alp
ha
activ
ity.
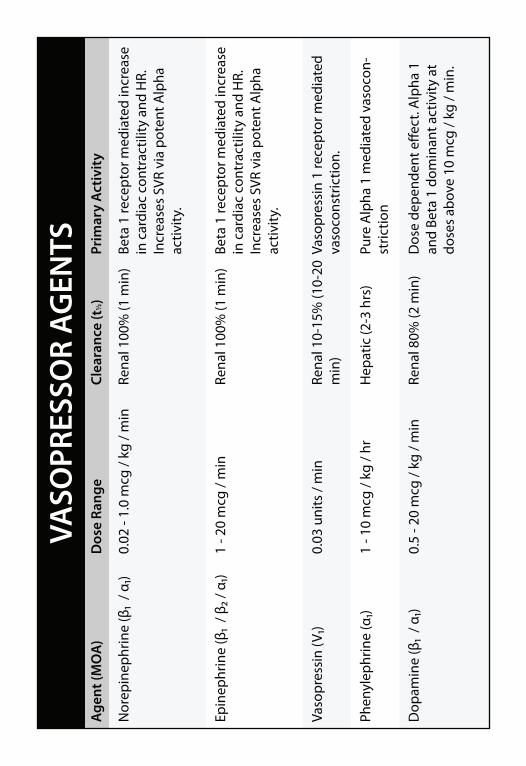
VASO
PRES
SOR
AG
ENTS
Age
nt (M
OA
)D
ose
Rang
e
Nor
epin
ephr
ine
(β1
/ α1)
0.02
- 1.
0 m
cg /
kg /
min
Clea
ranc
e (t
½)
Rena
l 100
% (1
min
)Be
ta 1
rece
ptor
med
iate
d in
crea
se
in c
ardi
ac c
ontr
actil
ity a
nd H
R.
Incr
ease
s SV
R vi
a po
tent
Alp
ha
activ
ity.
Prim
ary
Act
ivit
y
Epin
ephr
ine
(β1
/ β2 /
α1)
1 - 2
0 m
cg /
min
Rena
l 100
% (1
min
)Be
ta 1
rece
ptor
med
iate
d in
crea
se
in c
ardi
ac c
ontr
actil
ity a
nd H
R.
Incr
ease
s SV
R vi
a po
tent
Alp
ha
activ
ity.
Vaso
pres
sin
(V1)
0.03
uni
ts /
min
Rena
l 10-
15%
(10-
20
min
)Va
sopr
essi
n 1
rece
ptor
med
iate
d va
soco
nstr
ictio
n.
Dop
amin
e (β
1 / α
1) 0.
5 - 2
0 m
cg /
kg /
min
Rena
l 80%
(2 m
in)
Dos
e de
pend
ent e
�ect
. Alp
ha 1
an
d Be
ta 1
dom
inan
t act
ivity
at
dose
s ab
ove
10 m
cg /
kg /
min
.
Phen
ylep
hrin
e (α
1)1
- 10
mcg
/ kg
/ hr
Hep
atic
(2-3
hrs
)Pu
re A
lpha
1 m
edia
ted
vaso
con-
stric
tion
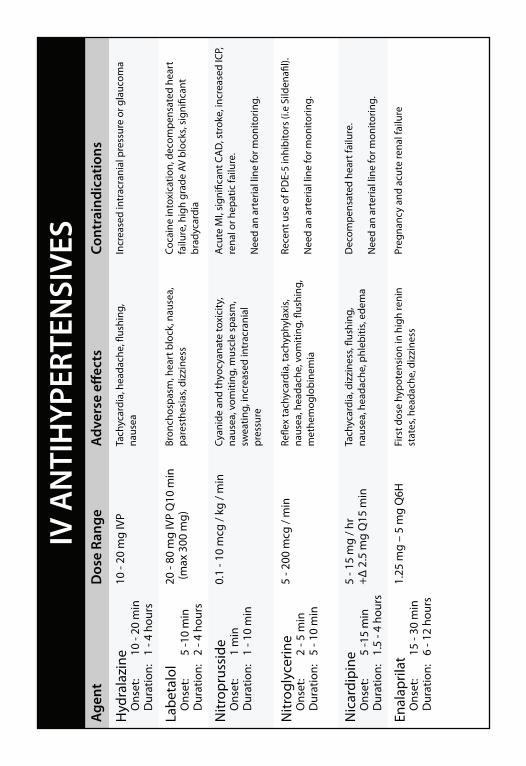
Age
ntD
ose
Rang
e
Hyd
rala
zine
O
nset
: 10
- 20
min
D
urat
ion:
1
- 4 h
ours
10 -
20 m
g IV
P
Adv
erse
e�e
cts
Tach
ycar
dia,
hea
dach
e, �
ushi
ng,
naus
eaIn
crea
sed
intr
acra
nial
pre
ssur
e or
gla
ucom
a
Cont
rain
dica
tions
Labe
talo
l
Ons
et:
5 -1
0 m
in
Dur
atio
n:
2 - 4
hou
rs
20 -
80 m
g IV
P Q
10 m
in (
max
300
mg)
Bron
chos
pasm
, hea
rt b
lock
, nau
sea,
pa
rest
hesi
as, d
izzi
ness
Coca
ine
into
xica
tion,
dec
ompe
nsat
ed h
eart
fa
ilure
, hig
h gr
ade
AV b
lock
s, si
gni�
cant
br
adyc
ardi
a
Nitr
opru
ssid
e
Ons
et:
1 m
in
Dur
atio
n:
1 - 1
0 m
in
0.1
- 10
mcg
/ kg
/ m
inCy
anid
e an
d th
yocy
anat
e to
xici
ty,
naus
ea, v
omiti
ng, m
uscl
e sp
asm
, sw
eatin
g, in
crea
sed
intr
acra
nial
pr
essu
re
Acut
e M
I, si
gni�
cant
CA
D, s
trok
e, in
crea
sed
ICP,
rena
l or h
epat
ic fa
ilure
.
Nee
d an
art
eria
l lin
e fo
r mon
itorin
g.
Nitr
ogly
cerin
e
Ons
et:
2 - 5
min
D
urat
ion:
5
- 10
min
5 - 2
00 m
cg /
min
Re�e
x ta
chyc
ardi
a, ta
chyp
hyla
xis,
naus
ea, h
eada
che,
vom
iting
, �us
hing
, m
ethe
mog
lobi
nem
ia
Rece
nt u
se o
f PD
E-5
inhi
bito
rs (i
.e S
ilden
a�l).
Nee
d an
art
eria
l lin
e fo
r mon
itorin
g.
Nic
ardi
pine
O
nset
: 5
-15
min
D
urat
ion:
1.
5 - 4
hou
rs
5 - 1
5 m
g / h
r +Δ
2.5
mg
Q15
min
Tach
ycar
dia,
diz
zine
ss, �
ushi
ng,
naus
ea, h
eada
che,
phl
ebiti
s, ed
ema
Dec
ompe
nsat
ed h
eart
failu
re.
Nee
d an
art
eria
l lin
e fo
r mon
itorin
g.
Enal
april
at
Ons
et:
15 -
30 m
in
Dur
atio
n:
6 - 1
2 ho
urs
1.25
mg
– 5
mg
Q6H
Firs
t dos
e hy
pote
nsio
n in
hig
h re
nin
stat
es, h
eada
che,
diz
zine
ssPr
egna
ncy
and
acut
e re
nal f
ailu
re
IV A
NTI
HYP
ERTE
NSI
VES

VASO
DIL
ATO
RS A
GEN
TSA
gent
(MO
A)
Dos
e Ra
nge
Nitr
ogly
cerin
e5
- 200
mcg
/ m
in
Clea
ranc
e (t
½)
Hep
atic
/ RB
Cs (1
- 3
min
)Co
nver
ted
to N
O p
rom
otin
g ve
nous
(pre
load
) rel
axat
ion.
Sm
all a
fter
load
redu
cing
e�e
ct.
Prim
ary
Act
ivit
yCo
ntra
indi
catio
ns
Acut
e in
ferio
r MI
HO
CM
Nitr
opru
ssid
e0.
1 - 1
0 m
cg /
kg /
min
Hep
atic
/ RB
Cs (1
- 3
min
)Sm
all v
esse
l vas
odila
tion
prim
ar-
ily a
fter
load
redu
ctio
n.St
roke
/ TI
ACo
arct
atio
nVS
D
HEA
RT F
AIL
URE
AG
ENTS
Age
nt (M
OA
)
ACE
Inhi
bito
rs
Capt
opril
En
alap
ril
Lisi
nopr
il
50 m
g PO
TID
10 m
g PO
BID
40 m
g PO
QD
Vaso
dila
tors
H
ydra
lazi
ne
Isor
dil
Im
dur
50-7
5 m
g PO
TID
20-8
0 m
g PO
TID
60-1
20 m
g PO
QD
Targ
et D
ose
Age
nt (M
OA
)Ta
rget
Dos
e
Beta
Blo
cker
s
Carv
edilo
l
Met
opro
lol X
L (n
ot L
opre
ssor
)25
mg
PO B
ID20
0 m
g PO
QD
Ald
oste
rone
Ant
agon
ist
Sp
irono
lact
one
25 m
g PO
QD
Ang
iote
nsin
Rec
epto
r Blo
cker
s V
alsa
rtan
80-1
60 m
g Q
D -
BID

NO
VEL
ORA
L A
NTI
COA
GU
LAN
TS
Dab
igat
ran
(Pra
daxa
)
Dire
ct T
hrom
bin
Inhi
bito
r
Ons
et:
90 m
in
Clea
ranc
e: R
enal
(12-
27 h
rs)
Re
vers
al:
Prax
bind
Non
-Val
vula
r AF
G
FR >
30:
150
mg
PO B
ID
GFR
15-
30:
75 m
g PO
BID
DVT
/ PE
Tre
atm
ent
G
FR >
30:
150
mg
PO B
ID
Mus
t not
ope
n ca
psul
es.
Avoi
d us
ing
with
am
ioda
rone
, dro
nade
rone
, ve
rapa
mil,
ket
ocon
azle
, cla
rithr
omyc
in, q
uini
dine
.
Cons
ider
atio
ns
Ok
to c
rush
tabl
ets
and
mix
with
app
le s
auce
.
Avoi
d us
ing
in p
atie
nts
with
mod
erat
e to
sev
ere
liver
dy
sfun
ctio
n.
Api
xaba
n (E
liqui
s)
Fact
or X
a In
hibi
tor
O
nset
: 3-
4 ho
urs
Cl
eara
nce:
Hep
atic
(12
hrs)
Re
vers
al:
KCen
tra
Non
-Val
vula
r AF:
5 m
g PO
BID
but
if tw
o or
mor
e co
nditi
ons
appl
y
(C
r >1.
5, A
ge >
80, w
t< 6
0 kg
) the
n 2.
5 m
g PO
BID
DVT
/ PE
Tre
atm
ent
10
mg
PO B
ID x
7 d
ays
then
5 m
g PO
BID
Ok
to c
rush
and
sus
pend
in D
5W 6
0 m
L if
give
n im
med
iate
ly.
Avoi
d in
sev
ere
hepa
tic im
pairm
ent.
Edox
aban
(Sav
aysa
)
Fact
or X
a In
hibi
tor
O
nset
: 1-
2 ho
urs
Cl
eara
nce:
Ren
al 5
0% (1
2 hr
s)
Reve
rsal
: KC
entr
a
Non
-Val
vula
r AF
G
FR 9
5-50
: 60
mg
PO Q
D
GFR
50-
15:
30 m
g PO
QD
Avoi
d in
pat
ient
s w
ith v
ery
high
func
tioni
ng k
idne
ys
due
to e
xces
sivl
y ra
pid
clea
ranc
e.
Avoi
d us
ing
in p
atie
nts
with
mod
erat
e to
sev
ere
liver
dy
sfun
ctio
n.
Age
nt (M
OA
)D
osin
g
Riva
roxa
ban
(Xar
elto
)
Fact
or X
a In
hibi
tor
O
nset
: 2-
3 ho
urs
Cl
eara
nce:
Ren
al 6
6% (5
-9 h
rs)
Re
vers
al:
KCen
tra
Non
-Val
vula
r AF
G
FR >
15:
20 m
g PO
QD
DVT
/ PE
Tre
atm
ent
G
FR >
15:
15 m
g PO
BID
x 2
1d th
en 2
0 m
g Q
D

LANDMARK CLINICAL TRIALSTopic Trial Name (PMID) Brief FindingsAtrial Fibrillation Anticoalguation Apixiban (Eliquis) ARISTOTLE (21870978) Apixiban superior to coumadin for stroke prevention (NNT 300) Dabigatran (Pradaxa) RE-LY (19717844) Dabigatran non-inferior to coumadin for stroke prevention Rivaroxiban (Xarelto) ROCKET-AF (21830957) Rivaroxiban non-inferior to coumnadin for stroke prevention Rate Control Threshold RACE-II (20231232) Lenient HR control (<110) non-inferior to strict (<80 bpm) for risk of MACE Rate vs Rhythm Control AFFIRM (12466507) Rate control non-inferior to rhythm control for risk of MACE
Ischemic Heart Disease Antiplatelet and Anticoagulant Therapy ASA ISIS-2 (2899772) ASA reduces reinfarct and death [very old study] (NNT 20) Clopidogrel CURE (11519503) Addition of Clopidogrel to ASA reduces MACE (NNT 50) Prasugrel TRITON TIMI 38 (17982182) Prasugrel superior to clopidogrel with PCI (NNT 50) Ticagrelor PLATO (20079528) Ticagrelor superior to clopidogrel with PCI (NNT 60) Revascularization Paclitaxel DES in STEMI HORIZONS AMI (19420364) DES in STEMI reduced TVR but not MACE (NNT 35) Compl. Revasc STEMI PRAMI (23991625) Non-infarct artery PCI reduces death / MI (NNT 7) PCI in UA / NSTEMI RITA-3 (16154018) PCI in high risk pts over OMT alone reduces 5 yr MACE (NNT 30) DES PCI vs CABG SYNTAX (19228612) CABG in LM or 3v CAD superior to PCI (e�ect rises with SYNTAX score) FREEDOM (23121323) CABG superior to PCI in diabetic pts to reduce MACE at 5 years (NNT 12) PCI vs OMT COURAGE (17387127) OMT non-inferior to BMS PCI for stable CAD for 5 year MACE FAME-2 (22924638) FFR guided PCI v OMT in stable CAD reduced urg revasc but not MI or death Access Radial vs Femoral RIVAL (21470671) Radial approach reduced hemorrhagic complications (NNT 500)
Heart failure Enalapril CONSENSUS (2883575) Enalapril in NYHA class IV reduced death(NNT 6) SOLVD (1463530) Enalapril in NYHA class II+ reduced hospitalization, not death (NNT 25) Valsartan ValHeFT (11759645) Valsartan in NYHA class II+ reduced hospitalizatoin (NNT 25) Spironolactone RALES (10471456) Spironolactone in NYHA class III+ reduced death(NNT 9) Carvedilol COMET (12853193) Carvedilol superior to Mortality in NYHA class II+ in reducing death (NNT 18) Digoxin Dig (9036306) Digoxin in Systolic HF reduced hospitalization but not death. Ivabradine BEAUTIFUL (18757088) Ivadribine in stable CAD + HR >70 reduced ACS admits (NNT 50) SHIFT (20801500) Ivadribine in stable CAD + HR >70 reduced ACS and Death (NNT 20 / 50) Dialysis with UF CARRESS-HF (23131078) Ultra�ltration “inferior” really equivalent to diuresis in NYHA class IV
Hypertension Benazepril + Amlodipine ACCOMPLISH (19052124) Benazepril+CCB reduced death / MI v Benazepril+HCTZ (NNT 50) Benazepril + HCTZ ACCOMPLISH (19052124) See above Lisinopril ALLHAT (12479763) Amlodipine v Chlorthalidone v Lisinopril all equal for ACS risk Amlodipine ALLHAT (12479763) See above VALUE (15207952) Amlodipine reduced MI but not mortality compared to Valsartan (NNT 140) Chlorthalidone ALLHAT (12479763) See above Losartan LIFE (11937178) Losartan reduced risk of stroke but not death or MI vs atenolol (NNNT 50) Valsartan VALUE (15207952) See above Trans-Catheter Aortic Valve Implantation (TAVI) TAVI in Surg High Risk PARTNER (22443479) Stroke and MI similar in both arms at 2 years.
Dyslipidemia Primary prevention Rosuvastatin JUPITER (18997196) Rosuvastatin in patients with CRP >2 mg/L reduced MACE (NNT 150) Secondary Prevention Rosuvastatin SATURN (22085316) Rosuvastatin 40 and Atorvastatin 80 both promoted atheroma regression Atorvastatin PROVE-IT (15007110) Atorvastatin reduced death / repeat ACS compared to Pravastatin (NNT 25) Ezetimibe IMPROVE-IT (18376000) Ezetimibe +Simvastatin in FHL did not reduce CIMT over Simvastatin alone. Niacin AIM-HIGH (22085343) No bene�t to addition of Niacin to Statin, trend toward increase stroke.
*The above information is only an extremely condensed version of the full trial details. Please see the full paper for further details.

AmericanHeartAssociation
AM
ERICAN COLLEGE
OF CARDIOLOGY