longitudinal variations and predictors of increased perceived impact of multiple sclerosis, a...
TRANSCRIPT

iences 270 (2008) 53–59www.elsevier.com/locate/jns
Journal of the Neurological Sc
Longitudinal variations and predictors of increased perceived impactof multiple sclerosis, a two-year study
Charlotte Ytterberg ⁎, Sverker Johansson, Lotta Widén Holmqvist, Lena von Koch
Department of Clinical Neuroscience, Care Sciences and Society, Karolinska University Hospital, Huddinge, 141 86 Stockholm, SwedenDepartment of Neurobiology, Care Sciences and Society, Karolinska University Hospital, Huddinge, 141 86 Stockholm, Sweden
Received 27 November 2007; received in revised form 23 January 2008; accepted 24 January 2008Available online 4 March 2008
Abstract
Objective: To explore variations and the capacity of selected factors – contextual factors, disease-related characteristics, cognition, fatigue,mood and time – to predict an increase in the perceived physical and psychological impact of multiple sclerosis (MS) over a two-year period.Methods: At an MS specialist clinic, 219 outpatients were included in the study and data were collected every 6 months. The MultipleSclerosis Impact Scale was used for assessment of the perceived physical and psychological impact of MS. For statistical analysis of changesin impact during the study period, Friedman ANOVAwas used and predictors of increased impact were explored with Generalized EstimatingEquations employing proportional odds models.Results: The majority had changes in perceived physical impact of established important magnitude and the psychological impact variedsignificantly. A period of more than 10 years since diagnosis, cognitive disability, fatigue and signs of depression were independentpredictors of increase in physical impact. Weak or moderate sense of coherence, absence of immunomodulatory treatment, fatigue and signsof depression were independent predictors of increase in psychological impact.Conclusion: The fluctuation in perceived impact should be taken into account in clinical decision-making and when designing studies andinterpreting the results. This study identifies the predictors of increased perceived physical and psychological impact that health-relatedservices should pay special attention to, in order to provide interventions aimed at minimizing the perceived impact of MS.© 2008 Elsevier B.V. All rights reserved.
Keywords: Multiple sclerosis; MSIS-29; Perceived impact; Predictors; Prospective; Longitudinal
1. Introduction
Patient-based outcomemeasures of general health status areimportant when evaluating the impact of multiple sclerosis(MS) and may even predict change in disability status [1].Different designations of general health status exist: e.g.,perceived health, quality of life (QOL), health-related qualityof life (HRQOL) and perceived impact of MS but all incor-
⁎ Corresponding author. Division of Neurology R54, Karolinska Uni-versity Hospital, Huddinge, SE-141 86 Stockholm, Sweden. Tel: +46 8 585822 77; fax: +46 8 774 4822.
E-mail address: [email protected] (C. Ytterberg).
0022-510X/$ - see front matter © 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.jns.2008.01.014
porate the perspective of the individual with MS. Severalstudies have shown that people with MS (PwMS) experiencelower HRQOL in comparison with the general population andcompared to those diagnosed with other chronic diseases e.g.,inflammatory bowel disease, and rheumatoid arthritis, evenearly in the disease process [2,3]. Depression has been found tobe strongly associated with low HRQOL in several cross-sectional studies [4–10], whereas results concerning theimpact of disease-related characteristics e.g., duration, courseand severity [4,5,8,9,11,12], fatigue [4,6,8,10], and cognition[7,10], are partially insufficient and contradictory.
The International Classification of Functioning, Disabil-ity and Health (ICF) aims to provide a scientific basis for the

54 C. Ytterberg et al. / Journal of the Neurological Sciences 270 (2008) 53–59
study of health conditions [13]. The ICF has two parts: 1)Functioning, including body functions/body structures, andactivities and participation; 2) Contextual Factors, includingenvironmental and personal factors. An individual's func-tioning is a complex relationship between the health con-dition and contextual factors. Thus, if the full healthexperience is to be described, it is important to collect dataon all components independently and thereafter exploreassociations and causal links between them.
The impact of personal factors e.g., sex and age [5,12,14],and environmental factors e.g., immunomodulatory treat-ment [15,16], on patient-based general health status inPwMS is not fully explored and results are inconsistent.Sense of coherence (SOC) is a personal factor, which can bedescribed as whether stressful situations are experienced ascomprehensible, manageable and meaningful [17]. Anindividual with a strong SOC, for instance, is thought tohave more resources at hand to adjust successfully to livingwith a chronic disease such as MS. An individual's SOC isdetermined through childhood and early adulthood and isbelieved to be relatively stable after age 30 [17]. Weak SOChas recently been found to be associated with low HRQOL inPwMS [9].
The Multiple Sclerosis Impact Scale-29 (MSIS-29) is apatient-based, disease-specific measure of the impact of MS[18]. Unlike many other disease-specific patient-basedoutcome measures of general health status in PwMS, theMSIS-29 has been psychometrically developed for PwMS. Ithas proven to be valid and reliable [18–20] and there isincreasing evidence of responsiveness [21,22]. Althoughgeneric measures make comparisons with the generalpopulation and with other diseases possible, they do notcapture certain disease-specific areas and may have limitedresponsiveness [23].
Few patient-based longitudinal studies on general healthstatus in PwMS have been performed [1,21,22,24,25]. TheMSIS-29 has been scarcely employed in longitudinal studies[21,22,25] and few studies have used the MSIS-29 toidentify predictors of the perceived impact of MS [25,26].Knowledge concerning the longitudinal variation in per-ceived impact of MS has important clinical implications forthose working in the healthcare professions, who see PwMSon a regular basis, as well as scientific implications for studydesign and interpretation of results. Longitudinal studies arealso necessary in order to explore predictors of change in theperceived impact of MS.
The aims of the present study were:
a) to explore variations in the perceived physical andpsychological impact of MS, from the PwMS' perspective,during a two-year period, at an outpatient MS specialistclinic; and
b) to explore the capacity of selected factors – contextualfactors (sex, age, SOC, living with a partner, living withchildren, work status, immunomodulatory treatment),disease-related characteristics, cognition, fatigue, mood
and time – to predict an increase in the perceived physicaland psychological impact of MS, over a period of 2 years.
2. Methods
2.1. Participants and procedures
Those eligible were all PwMS diagnosed according to thePoser criteria [27], who, during the period from February 1,2002 to June 12, 2002, were scheduled for an outpatientappointment with either of two of the senior neurologists atthe MS Centre of the Department of Neurology, KarolinskaUniversity Hospital, Huddinge, in Stockholm, Sweden. ThePwMS received written and oral information regarding thestudy and were included after informed consent. The PwMSwere followed up every 6 months for 2 years, primarily inconjunction with the regular visits to their senior neurologist,or an appointment was made for data-collection on anotherday. During inclusion and at 6, 12, 18 and 24 months, thePwMS met an investigator, one of five research physiothera-pists trained to perform the tests according to a standardizedprocedure, primarily the same investigator and at the sametime of day on all occasions.
The study was approved by the ethical committee of theKarolinska Institutet in Stockholm, Sweden.
2.2. Instruments
Using the ICF [13] as a framework, standardized instru-ments and interviews were employed to collect data.
The neurologist responsible determined disease course,registered occurrence of bouts during the preceding 6 monthsand assessed disease severity by means of the ExpandedDisability Status Scale (EDSS) [28]. The remaining data werecollected by the research physiotherapists. Informationconcerning the time since diagnosis was collected from themedical records or, when not registered, by interview.Contextual factors (sex, age, living with a partner, livingwith children, work status, immunomodulatory treatment)were collected through interviews. To assess SOC the 13-item version of the SOC-scale was used [17]. The SymbolDigit Modalities Test (SDMT) was applied to assesscognition [29]. The SDMT was primarily administered inwritten format, but for PwMS unable to write, the test wasadministered verbally. Enlarged font size was used for PwMSwith visual problems. Perceived level of energy was assessedusing the Fatigue Severity Scale (FSS) [30] and mood, usingthe Beck Depression Inventory (BDI) [31]. Data regardingdisease-related characteristics and contextual factors werecollected at inclusion, except for SOC, which was collected at6 or 12months and occurrence of bouts, which were collectedat each point in time. Data regarding cognition and fatiguewere collected at each point in time and regarding mood, atinclusion and at 12 and 24 months. Criteria for categorizationof the independent variables are presented in Table 1. PwMSwith signs of depression, fatigue or cognitive disability at one

Table 1Criteria for categorization of the independent variables
Independent variable Criteria
Sex Women / menAge b47 years / ≥47 years a
Sense of coherence Sex-related norms: SOC weak or moderate:b76 / SOC strong: ≥76 [32]
Living with a partner Living with a partner ≥18 years of age / livingalone
Living with children Living with children b18 years of age / not livingwith children
Work status Working, full-time or part-time / not working b
Immunomodulatorytreatment
Immunomodulatory treatment /no immunomodulatory treatment
Disease course Relapsing remitting / progressive c
Disease severity EDSS: normal (0) / mild (1.0–3.5) /moderate (4.0–5.5) / severe (6.0–9.5)
Bouts No bouts d / bouts e
Time lapse sincediagnosis
≤10 years since diagnosis / N10 years sincediagnosis
Cognition No cognitive disability d / cognitive disability: age-related norms, written or verbal reply, — 1.5 SD e
[29]Energy No fatigue d / fatigue: FSS≥5 e [33]Mood No signs of depression d / signs of depression:
BDIN13 e [34]a The mean age of the sample.b b65 years of age.c Secondary progressive and primary progressive.d Throughout the study.e At one or more points in time.
55C. Ytterberg et al. / Journal of the Neurological Sciences 270 (2008) 53–59
or more points in time were categorized as having signs ofdepression, fatigue or cognitive disability respectively.EDSS-scores were categorized according to the SwedishMS-register [35].
The MSIS-29 [18] was used for assessment of theperceived physical and psychological impact of MS from theperspective of the PwMS. The MSIS-29 consists of twoordinal subscales, of which one assesses the physical impactand the other, the psychological impact. The MSIS-29 wasemployed at inclusion and at 12, 18 and 24 months. Theperceived physical and psychological impact of MS,according to the MSIS-29, was categorized according tothe quartiles of its distributions in the sample at inclusion; 1stcategory b25th percentile, 2nd category ≥25th to b50thpercentile, 3rd category ≥50th to b75th percentile, and 4thcategory ≥75th percentile [6]. According to this categoriza-tion, the 1st category represents the lowest perceived impactand the 4th category represents the highest perceived impact.
2.3. Statistical analysis
Descriptive statistics were used to present theMSIS-29. Forstatistical analysis of changes in perceived impact during thestudy period, Friedman ANOVA was used. A p value b0.05was considered statistically significant. Effect size (ES) wascalculated by dividing the mean change in score by the initialstandard deviation [36], using data from inclusion and from24 months. ESs were interpreted using Cohen's arbitrary
criteria (0.2=small, 0.5=moderate and 0.8=large) [37]. Theindividual change in score during the study period wasdetermined for the MSIS-29 physical and psychologicalsubscale respectively. The proportions of PwMS who hadimportant changes in the physical scores were determined byusing established cut-off values i.e., a change in physical scoreof≥7 in PwMS with an EDSS score of 0.0–5.0 and a changein physical score of≥8 in PwMS with an EDSS score of 5.5–8.0 [22]. In the absence of established minimum values forimportant changes in the psychological score, arbitraryintervals of five were used. When an individual experiencedchanges over more than two assessments, the separate changesin scores were recorded. For example: two separate changes inscores were calculated if an individual had different MSIS-29scores at inclusion, and at 12 and 18 months.
Generalized Estimating Equations (GEE) employingproportional odds models were used to explore the predictivecapacity of the independent variables. In the models, theodds for a change in the MSIS-29 physical score and in theMSIS-29 psychological score from the 1st category vs the2nd 3rd 4th categories are equal to the odds for a changebetween the 1st 2nd categories vs the 3rd 4th categories,which are equal to the odds for a change between the 1st 2nd3rd categories vs the 4th category. Stepwise backwardselection criteria were employed, entering all variables andthen removing variables with p values N0.05. In the GEE, itis possible to include persons with missing data, thus theanalyses included PwMS with MSIS-29 data available for atleast one point in time and complete data for the independentvariables. Pair-wise comparisons were adjusted for multiplecomparisons using a p value of b0.01. For each MSIS-29subscale, one model containing all variables except workstatus was created. A second model for each subscale alsocontained the variable work status and only PwMS youngerthan 65 years of age, the customary age for retirement inSweden. Interactions between time and the independentvariables were controlled for, as were interaction betweenSOC and mood; SOC and perceived level of energy; diseaseseverity, disease course and time since diagnosis respec-tively; and between perceived level of energy, cognition andmood respectively. The predictive capacity of the indepen-dent variables are presented as odds ratios (OR) with 95%confidence intervals (CI) and p values for increasedperceived physical and psychological impact respectively.
Descriptive statistics and Friedman ANOVA wereanalysed in Stastistica 7. Software used for analyses withGEE was SAS® System 9.1 (SAS Institute Inc., Cary, NorthCarolina, USA).
3. Results
Of 255 eligible PwMS, 36 declined and 219 wereincluded in the study. During the study period sevenPwMS died and 12 withdrew, leaving 200 to be followedfor 2 years. At inclusion, data were collected within 2 weeksafter the outpatient appointment for 204 of the 219 PwMS

Table 2Disease-related characteristics, contextual factors, cognition, fatigue andmood in the sample
n (%)
People with MS 219Women 149 (68)Age, years 47 (12, 20–75) a
Sense of coherence b
Weak 23 (11)Moderate 125 (61)Strong 58 (28)
Living with a partner 152 (69)Living with children 64 (29)Working full or part-time c 117 (58)Immunomodulatory treatment 182 (83)Disease course
Relapsing remitting 127 (58)Secondary progressive 83 (38)Primary progressive 9 (4)
Disease severityEDSS normal, 0 1 (0.5)EDSS mild, 1–3.5 129 (59)EDSS moderate, 4–5.5 37 (17)EDSS severe, 6–9.5 52 (23.5)
Time lapse since diagnosis, years 14 (10, 0–44) a
Cognition b
No disability 83 (40)Disability 123 (60)
Energy d
No fatigue 65 (31)Fatigue 142 (69)
Mood e
No signs of depression 108 (55)Signs of depression 90 (45)a Mean (SD, range).b 206 PwMS tested.c Working; used only for PwMS b65 years of age, (n=201).d 207 PwMS tested.e 198 PwMS tested.
Table 3aModel 1: Proportional odds for increase in perceived physical impact inPwMS (n=185); odds ratios (OR), 95% confidence intervals (CI) andp values
Independentvariable
Variablecategorization
Increase in perceivedphysical impact, OR (CI)
P value
Years sincediagnosis
N10 yearssince diagnosis
2.01 (1.23 to 3.28) 0.005
≤10 yearssince diagnosis
1
Cognition Cognitivedisability
2.41 (1.49 to 3.90) b0.001
No cognitivedisability
1
Energy Fatigue 10.60 (6.18 to 18.20) b0.001No fatigue 1
Mood Signs ofdepression
2.28 (1.42 to 3.65) b0.001
No signs ofdepression
1
EDSS mild / diseasecourse
Progressive 3.58 (1.23 to 10.46) 0.011Relapsingremitting
1
Relapsing remitting /disease severity
EDSSmoderate
4.83 (1.95 to 11.95) b0.001
EDSS mild 1
56 C. Ytterberg et al. / Journal of the Neurological Sciences 270 (2008) 53–59
and, for the remaining 15, within 5 weeks on average. At24 months, data were collected within 2 years±2 weeks afterinclusion for 147 of the 200 PwMS and for the 53 remainingPwMS within 2 years±4 weeks on average. Data oncontextual factors, disease-related characteristics, cognition,fatigue and mood in the sample are presented in Table 2.
Complete data on the MSIS-29 were collected at all pointsin time from 194 PwMS. Apart from inability due to MS, thereasons for not completing the MSIS-29 were difficulty tounderstand the Swedish language and personal stress.During the two-year study period, there were no statisticallysignificant variations in the physical subscale, p=0.12, butvariations were found in the psychological subscale,pb0.001. The proportions of PwMS in the differentcategories were similar at all points in time. Regarding thephysical subscale 127 (65%) PwMS changed category one ormore times, whereas 67 (35%) remained in the samecategory: 29 in the 1st category, 8 in the 2nd category, 9 inthe 3rd category and 21 in the 4th category. Regarding thepsychological subscale 149 (77%) PwMS changed categoryone or more times, whereas 45 (23%) remained in the same
category: 23 in the 1st category, 8 in the 2nd category, 4 inthe 3rd category and 10 in the 4th category.
The ESs for the whole sample were negligible (b0.2) in bothsubscales but small ESs were found in the EDSS moderatecategory with regard to the physical subscale and in the EDSSmild category with regard to the psychological subscale. InPwMS with an inclusion EDSS of 0.0–5.0, 110 (74%)experienced a change in the MSIS-29 physical score of ≥7.In PwMS with an inclusion EDSS of 5.5–8.0, 35 (80%)experienced a change in the MSIS-29 physical score of ≥8.Regarding the psychological subscale, 139 (72%) PwMSexperienced a change of≥5, 69 (36%)≥10 and 23 (12%)≥15.
The results of the GEE including all variables exceptwork status (n=185) are presented in Table 3a – physicalimpact – and Table 3b – psychological impact. Theprobability of belonging to a certain category of the MSIS-29 did not change significantly over time in the GEE models,neither did time interact with the other independent variablesin any model. There were no interactions except betweendisease severity and disease course with regard to physicalimpact. A period of more than 10 years since diagnosis,cognitive disability, fatigue and signs of depression wereindependent predictors of increase in perceived physicalimpact. Mild disease severity in combination with aprogressive disease course compared to a relapsing remittingdisease course predicted increase in physical impact as did arelapsing remitting disease course in combination withmoderate disease severity compared to mild disease severity.No immunomodulatory treatment, fatigue, signs of depres-sion and weak or moderate SOC were independent predictorsof increase in perceived psychological impact. Predictorsand OR were similar in the models with or without the
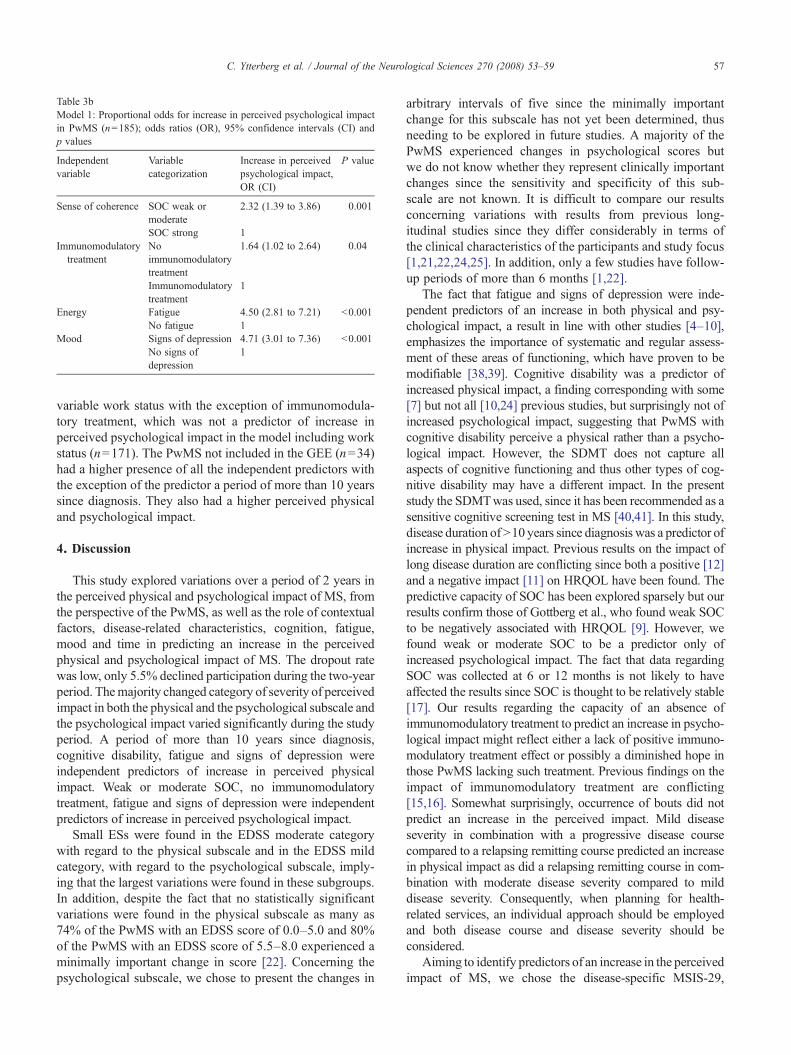
Table 3bModel 1: Proportional odds for increase in perceived psychological impactin PwMS (n=185); odds ratios (OR), 95% confidence intervals (CI) andp values
Independentvariable
Variablecategorization
Increase in perceivedpsychological impact,OR (CI)
P value
Sense of coherence SOC weak ormoderate
2.32 (1.39 to 3.86) 0.001
SOC strong 1Immunomodulatory
treatmentNoimmunomodulatorytreatment
1.64 (1.02 to 2.64) 0.04
Immunomodulatorytreatment
1
Energy Fatigue 4.50 (2.81 to 7.21) b0.001No fatigue 1
Mood Signs of depression 4.71 (3.01 to 7.36) b0.001No signs ofdepression
1
57C. Ytterberg et al. / Journal of the Neurological Sciences 270 (2008) 53–59
variable work status with the exception of immunomodula-tory treatment, which was not a predictor of increase inperceived psychological impact in the model including workstatus (n=171). The PwMS not included in the GEE (n=34)had a higher presence of all the independent predictors withthe exception of the predictor a period of more than 10 yearssince diagnosis. They also had a higher perceived physicaland psychological impact.
4. Discussion
This study explored variations over a period of 2 years inthe perceived physical and psychological impact of MS, fromthe perspective of the PwMS, as well as the role of contextualfactors, disease-related characteristics, cognition, fatigue,mood and time in predicting an increase in the perceivedphysical and psychological impact of MS. The dropout ratewas low, only 5.5% declined participation during the two-yearperiod. Themajority changed category of severity of perceivedimpact in both the physical and the psychological subscale andthe psychological impact varied significantly during the studyperiod. A period of more than 10 years since diagnosis,cognitive disability, fatigue and signs of depression wereindependent predictors of increase in perceived physicalimpact. Weak or moderate SOC, no immunomodulatorytreatment, fatigue and signs of depression were independentpredictors of increase in perceived psychological impact.
Small ESs were found in the EDSS moderate categorywith regard to the physical subscale and in the EDSS mildcategory, with regard to the psychological subscale, imply-ing that the largest variations were found in these subgroups.In addition, despite the fact that no statistically significantvariations were found in the physical subscale as many as74% of the PwMS with an EDSS score of 0.0–5.0 and 80%of the PwMS with an EDSS score of 5.5–8.0 experienced aminimally important change in score [22]. Concerning thepsychological subscale, we chose to present the changes in
arbitrary intervals of five since the minimally importantchange for this subscale has not yet been determined, thusneeding to be explored in future studies. A majority of thePwMS experienced changes in psychological scores butwe do not know whether they represent clinically importantchanges since the sensitivity and specificity of this sub-scale are not known. It is difficult to compare our resultsconcerning variations with results from previous long-itudinal studies since they differ considerably in terms ofthe clinical characteristics of the participants and study focus[1,21,22,24,25]. In addition, only a few studies have follow-up periods of more than 6 months [1,22].
The fact that fatigue and signs of depression were inde-pendent predictors of an increase in both physical and psy-chological impact, a result in line with other studies [4–10],emphasizes the importance of systematic and regular assess-ment of these areas of functioning, which have proven to bemodifiable [38,39]. Cognitive disability was a predictor ofincreased physical impact, a finding corresponding with some[7] but not all [10,24] previous studies, but surprisingly not ofincreased psychological impact, suggesting that PwMS withcognitive disability perceive a physical rather than a psycho-logical impact. However, the SDMT does not capture allaspects of cognitive functioning and thus other types of cog-nitive disability may have a different impact. In the presentstudy the SDMTwas used, since it has been recommended as asensitive cognitive screening test in MS [40,41]. In this study,disease duration ofN10 years since diagnosis was a predictor ofincrease in physical impact. Previous results on the impact oflong disease duration are conflicting since both a positive [12]and a negative impact [11] on HRQOL have been found. Thepredictive capacity of SOC has been explored sparsely but ourresults confirm those of Gottberg et al., who found weak SOCto be negatively associated with HRQOL [9]. However, wefound weak or moderate SOC to be a predictor only ofincreased psychological impact. The fact that data regardingSOC was collected at 6 or 12 months is not likely to haveaffected the results since SOC is thought to be relatively stable[17]. Our results regarding the capacity of an absence ofimmunomodulatory treatment to predict an increase in psycho-logical impact might reflect either a lack of positive immuno-modulatory treatment effect or possibly a diminished hope inthose PwMS lacking such treatment. Previous findings on theimpact of immunomodulatory treatment are conflicting[15,16]. Somewhat surprisingly, occurrence of bouts did notpredict an increase in the perceived impact. Mild diseaseseverity in combination with a progressive disease coursecompared to a relapsing remitting course predicted an increasein physical impact as did a relapsing remitting course in com-bination with moderate disease severity compared to milddisease severity. Consequently, when planning for health-related services, an individual approach should be employedand both disease course and disease severity should beconsidered.
Aiming to identify predictors of an increase in the perceivedimpact of MS, we chose the disease-specific MSIS-29,

58 C. Ytterberg et al. / Journal of the Neurological Sciences 270 (2008) 53–59
consisting of items that are specific and relevant for PwMS.Since the MSIS-29 is a fairly new instrument, it has beenrecommended that it should be used in different cohorts ofPwMS [42] and we believe that the longitudinal design of thepresent study and the fact that several potential predictors wereconcurrently included in the analysis combine to make ourresults important. The fact that some PwMS were excludedfrom the GEE due to incomplete data for the independentvariables is not likely to have biased the results since thesePwMShad an even higher presence ofmost of the independentpredictors and also a higher perceived physical and psycho-logical impact. However, one should keep in mind that a largeproportion of the sample received immunomodulatory treat-ment. Although the absence of immunomodulatory treatmentpredicted an increase in psychological impact, the influence ofsuch treatment and of other health care interventions on theperceived impact of MS is not fully understood. Futureresearch should also study the association between differentpredictors and specific physical and psychological items in theMSIS-29 and also identify individuals with similar patterns inlongitudinal changes.
This study provides an important contribution to theknowledge of the perceived physical and psychologicalimpact of MS from the PwMS perspective, including thecapacity of several factors, of which some have proven to bemodifiable [38,39], to predict an increased impact. Takingthe variations into consideration, it would be appropriateregularly to assess the perceived impact in order to identifythose PwMS in need of special attention. The fluctuation inperceived impact should be taken into account whendesigning studies and interpreting the results. This studyalso highlights predictors of increased perceived physicaland psychological impact that health-related services, usinga multidisciplinary approach, particularly should focus onin order to provide interventions aiming to minimize theperceived impact of MS.
Acknowledgement
The authors wish to express their gratitude to theparticipating people with MS and the staff of the MS Centre,Karolinska University Hospital, Huddinge, to Professor HansLink and to Jakob Bergström, statistician at the Departmentof Learning, Informatics, Management and Ethics, Karolins-ka Institutet. Data collection was supported by an unrestrictedgrant from Biogen Idec. The study was funded by grants fromthe Center for Health Care Sciences, the Health Care SciencesPostgraduate School, Karolinska Institutet, the SwedishAssociation of Persons with Neurological Disabilities, andthe Swedish Research Council.
References
[1] Visschedijk MA, Uitdehaag BM, Klein M, van der Ploeg E, ColletteEH, Vleugels L, et al. Value of health-related quality of life to predictdisability course in multiple sclerosis. Neurology 2004;63:2046–50.
[2] Rudick RA, Miller D, Clough JD, Gragg LA, Farmer RG. Quality oflife in multiple sclerosis. Comparison with inflammatory bowel diseaseand rheumatoid arthritis. Arch Neurol 1992;49:1237–42.
[3] NortvedtMW, Riise T,Myhr KM,NylandHI. Quality of life in multiplesclerosis: measuring the disease effects more broadly. Neurology1999;53:1098-1003.
[4] Amato MP, Ponziani G, Rossi F, Liedl CL, Stefanile C, Rossi L.Quality of life in multiple sclerosis: the impact of depression, fatigueand disability. Mult Scler 2001;7:340–4.
[5] Fruehwald S, Loeffler-Stastka H, Eher R, Saletu B, Baumhackl U.Depression and quality of life in multiple sclerosis. Acta Neurol Scand2001;104:257–61.
[6] Janardhan V, Bakshi R. Quality of life in patients with multiple sclerosis:the impact of fatigue and depression. J Neurol Sci 2002;205:51–8.
[7] Benito-Leon J, Morales JM, Rivera-Navarro J. Health-related qualityof life and its relationship to cognitive and emotional functioning inmultiple sclerosis patients. Eur J Neurol 2002;9:497–502.
[8] Lobentanz IS, Asenbaum S, Vass K, Sauter C, Klösch G, Kollegger H.Factors influencing quality of life in multiple sclerosis patients: disability,depressive mood, fatigue and sleep quality. Acta Neurol Scand2004;10:6–13.
[9] Gottberg K, Einarsson U, Ytterberg C, de Pedro Cuesta J, FredrikssonS, von Koch L, et al. Health-related quality of life in a population-basedsample of people with multiple sclerosis. Mult Scler 2006;12:605–12.
[10] Johansson S, Ytterberg C, Claesson IM, Lindberg J, Hillert J, AnderssonM, et al. High concurrent presence of disability in multiple sclerosis:associations with perceived health. J Neurol 2007;254:767–73.
[11] Pfennings L, Cohen L, Adèr H, Polman C, Lankhorst G, Smits R, et al.Exploring differences between subgroups of multiple sclerosis patientsin health-related quality of life. J Neurol 1999;246:587–91.
[12] FordHL, Gerry E, JohnsonMH, Tennant A. Health status and quality oflife of people with multiple sclerosis. Disabil Rehabil 2001;23:516–21.
[13] The International Classification of Functioning. Disability and health.World Health Organization; 2001. Available at: www.who.int/classification/icf Accessed 12 Nov 2007.
[14] Miller A, Dishon S. Health-related quality of life in multiple sclerosis:psychometric analysis of inventories. Mult Scler 2005;11:450–8.
[15] Vermersch P, de Seze J, Delisse B, Lemaire S, Stojkovic T. Quality oflife in multiple sclerosis: influence of interferon-beta1 a (Avonex)treatment. Mult Scler 2002;8:377–81.
[16] Freeman JA, ThompsonAJ, Fitzpatrick R,HutchinsonM,MiltenburgerC, Beckmann K, et al. Interferon-beta1b in the treatment of secondaryprogressive MS: impact on quality of life. Neurology 2001;57:1870–5.
[17] Antonovsky A. The structure and properties of the sense of coherencescale. Soc Sci Med 1993;36:725–33.
[18] Hobart J, LampingD, Fitzpatrick R, Riazi A, Thompson A. TheMultipleSclerosis Impact Scale (MSIS-29): a new patient-based outcomemeasure. Brain 2001;124:962–73.
[19] Riazi A, Hobart J, Lamping D, Fitzpatrick R, Thompson AJ. MultipleSclerosis Impact Scale (MSIS-29): reliability and validity in hospitalbased samples. J Neurol Neurosurg Psychiatry 2002;73:701–4.
[20] Hoogervorst EL, Zwemmer JN, Jelles B, Polman CH, Uitdehaag BM.Multiple Sclerosis Impact Scale (MSIS-29): relation to establishedmeasures of impairment and disability. Mult Scler 2004;10:569–74.
[21] Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ. Howresponsive is the Multiple Sclerosis Impact Scale (MSIS-29)?A comparison with some other self report scales. J Neurol NeurosurgPsychiatry 2005;76:1539–43.
[22] Costelloe L, O'rourke K, Kearney H, McGuigan C, Gribbin L DugganM, et al. The patient knows best; significant change in the physicalcomponent of the Multiple Sclerosis Impact Scale (MSIS-29 physical).J Neurol Neurosurg Psychiatry 2007;78:841–4.
[23] PatrickDL,DeyoRA.Generic and disease-specificmeasures in assessinghealth status and quality of life. Med Care 1989;27(suppl 3):217–32.
[24] O'Connor P, Lee L, Ng PT, Narayana P, Wolinsky JS. Determinants ofoverall quality of life in secondary progressive MS: a longitudinalstudy. Neurology 2001;57:889–91.

59C. Ytterberg et al. / Journal of the Neurological Sciences 270 (2008) 53–59
[25] Riazi A, Thompson AJ, Hobart JC. Self-efficacy predicts self-reportedhealth status in multiple sclerosis. Mult Scler 2004;10:61–6.
[26] Ayatollahi P, Nafissi S, Eshraghian MR, Kaviani H, Tarazi A. Impactof depression and disability on quality of life in Iranian patients withmultiple sclerosis. Mult Scler 2007;13:275–7.
[27] Poser C, PatyD, Scheinberg L,McDonaldWI,Davis FA, EbersGC, et al.New diagnostic criteria for multiple sclerosis: guidelines for researchprotocols. Ann Neurol 1983;13:227–31.
[28] Kurtzke JF. Rating neurologic impairment in multiple sclerosis: anexpanded disability status scale (EDSS). Neurology 1983;77:1444–52.
[29] Smith A. Symbol Digit Modalities Test (SDMT). In: Lezak M, editor.Neuropsychological assessment. 3rd ed. New York: Oxford UniversityPress; 1995. p. 379–81.
[30] Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigueseverity scale. Application to patients with multiple sclerosis andsystemic lupus erythematosus. Arch Neurol 1989;46:1121–3.
[31] Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventoryfor measuring depression. Arch Gen Psychiatry 1961;4:561–71.
[32] Larsson G, Kallenberg KO. Sense of coherence, socioeconomicconditions and health. Eur J Public Health 1996;6:175–80.
[33] Bakshi R, Shaikh ZA, Miletich RS, Csarnecki D, Dmochowski J,Henschel K, et al. Fatigue in multiple sclerosis and its relationship todepression and neurologic disability. Mult Scler 2000;6:181–5.
[34] Goldman Consensus Group. The Goldman Consensus statement ondepression in multiple sclerosis. Mult Scler 2005;11:328–37.
[35] The SwedishMS-register. Available at: http://www.msreg.net Accessed12 Nov 2007.
[36] Kazis LE, Anderson JJ, Meenan R. Effect sizes for interpreting changesin health status. Med Care 1989;27(suppl 3):178–89.
[37] Cohen J. A power primer. Psychol Bull 1992;112:155–9.[38] Mathiowetz VG, Finlayson ML, Matuska KM, Chen HY, Luo P.
Randomized controlled trial of an energy conservation course forpersons with multiple sclerosis. Mult Scler 2005;11:592–601.
[39] Thomas PW, Thomas S, Hillier C, Galvin K Baker R. Psychologicalinterventions for multiple sclerosis. Cochrane Database Syst Rev2006(Issue 1).
[40] Dent A, Lincoln NB. Screening for memory problems in multiplesclerosis. Br J Clin Psychol 2000;39:311–5.
[41] Rudick R, Antel J, Confavreux C, Cutter G, Ellison G, Fischer J, et al.Recommendations from the National Multiple Sclerosis Society ClinicalOutcomes Assessment Task Force. Ann Neurol 1997;42:379–82.
[42] Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.Improving the evaluation of therapeutic interventions in multiplesclerosis: development of a patient-based measure of outcome. HealthTechnol Assess 2004;8:1–48.