literature review: fitness; social health an overview and ... energy_balance_journal... ·...
TRANSCRIPT
Literature Review: Fitness; Social Health
An Overview and Proposed Framework ofSocial-Environmental Influences on thePhysical-Activity Behavior of WomenJoEllen Vrazel, PhD; Ruth P. Saunders, PhD; Sara Wilcox, PhD
Abstract
Objective. The primary purposes of this review were to identify key social-environmentalinfluences on the physical-activity behavior of women and to propose an organizing frameworkof these influences in the social environment.
Data Sources. Computerized searches of MEDLINE, Science Direct, and CINAHL wereconducted to identify relevant research.
Study Inclusion and Exclusion Criteria. Studies were included if they used a sample ofadult women or included gender-specific analysis, identified or measured some aspect of thesocial environment in relation to physical activity, and were published in English within thelast two decades.
Data Extraction. Characteristics of study design, sample population, and identified social-environmental variables were extracted.
Data Synthesis. Through an iterative review of the data by several researchers, commoninfluences and themes were identified and organized into a social environment framework,which included the following components: social support/social networks, life transitions/multiple roles, and cultural standards/gender role expectations.
Results. Women are exposed to societal messages that indicate physical activity is nota priority and may be inappropriate; they may also lack the social support necessary to adoptand maintain physical activity.
Conclusions. This review reveals the complex range of factors in the social environment thatinfluence women, and it provides support for the importance of the social environment onphysical-activity behavior in women. A social-environmental framework related toBronfenbrenner’s social ecological model is proposed along with recommended strategies to applyin interventions targeting women. (Am J Health Promot 2008;23[1]:2–12.)
Key Words: Physical Activity, Exercise, Social Support, Social Environment, LifeTransitions, Cultural Influence, Women. Manuscript format: literature review;Setting: social environment; Health focus: fitness/physical activity; Strategy:education, culture change, policy, skill building/behavior change; Targetpopulation: adult women; Target population circumstances: race/ethnicity
INTRODUCTION
Regular physical activity providessignificant health benefits to women,including reduced risks for coronaryheart disease,1 some cancers,2,3 stroke,4
type 2 diabetes,5 and other leadingcauses of death and disability.6,7 Com-pared with women who are inactive,women who are physically active havea reduced mortality risk.8 Researchfurther affirms that moderate amountsof daily physical activity can producethese health benefits.9 Even so, na-tional surveys have consistently foundthat women have lower rates of physi-cal activity than men and that women’sparticipation in physical activity de-creases significantly with age.9
Historically, physical activity andhealth research have focused primarilyon men.10,11 However, recent effortshave been directed toward identifyingfactors affecting the health and well-being of women, including physical-activity behavior.11 Current recom-mendations have also called fora greater focus on the role of theenvironment to enhance our under-standing of individual physical-activitybehavior.12,13 In particular, researchershave begun to recognize the significantimpact of the social environment onphysical activity and have called for theidentification and development of in-novative strategies that can assist inshifting social and cultural norms toinfluence individual behavior.12–14 Sev-eral prominent theories, includingSocial Cognitive Theory,15 ecologicalmodels,16 Transactional Model ofStress and Coping,17 and Interdepen-dence Theory,18 recognize the role ofthe social environment on behavior.
JoEllen Vrazel, PhD, is with the Department of Exercise Science, School of Public Health andHealth Services, George Washington University, Washington, District of Columbia. Ruth P.Saunders, PhD, is with the Department of Health Promotion, Education, and Behavior; andSara Wilcox, PhD, is with the Department of Exercise Science, Arnold School of Public Health,University of South Carolina, Columbia, South Carolina.
Send reprint requests to JoEllen Vrazel, PhD, Department of Exercise Science, School of PublicHealth and Health Services, George Washington University, 817 23rd Street NW, Washington, DC20052; [email protected].
This manuscript was submitted July 9, 2006; revisions were requested March 26 and July 30, 2007; the manuscript wasaccepted for publication August 4, 2007.
Copyright E 2008 by American Journal of Health Promotion, Inc.0890-1171/08/$5.00 + 0
2 American Journal of Health Promotion
For individual use only. Duplication or distribution prohibited by law.

The importance of the social environ-ment is recognized, but operationaldefinitions are often limited in scopeand fail to reflect the complexities ofthe social environment. Although dif-ferent aspects of the social environ-ment have been identified in physicalactivity research, most studies focus ona narrowly defined aspect of the socialenvironment, rather than takinga more comprehensive approach. Sim-ilarly, although a growing body of workis emerging in this area, the literaturehas not been reviewed. Therefore, theprimary purposes of this conceptuallyoriented literature review were toidentify key social-environmental in-fluences on the physical-activity behav-ior of women and to propose anorganizing framework of these influ-ences in the social environment.
METHODS
Data Sources
Computerized searches of the Na-tional Library of Medicine MEDLINE,Science Direct, and the CumulativeIndex of Nursing and Allied HealthLiterature (CINAHL) were conductedto identify relevant research for thisreview. Reference lists from identifiedarticles were also used to supplementthe search.
Inclusion and Exclusion CriteriaStudies were included if they used
a sample of adult women or includedgender-specific analysis, identified ormeasured some aspect of the socialenvironment in relation to physicalactivity, and were published in Englishwithin the last two decades (1985–2005). Studies that focused primarilyon adult women aged 20 to 60 yearswere selected; however, some studiesincluded sample populations that ex-tended into slightly younger or olderwomen than this age range. Studieswere excluded if the sample popula-tion included only young-adult women(i.e., 18–20 years old) or older women(i.e., § 60 years old). The searchinvolved all combinations of key wordsrelated to physical activity, the socialenvironment (e.g., social environment,social support, social influence, andsocial norms), and women. This reviewwas intended to identify all potentiallyrelevant constructs pertaining to thesocial environment; therefore, both
quantitative and qualitative studieswere included. Physical activity for thepurpose of this review was defined asany bodily movement that results inenergy expenditure, including exer-cise, leisure-time activity, and lifestyleactivity.
Data Extraction
An extensive literature review wasconducted to identify any conceptuallyrelevant research that reported social-environmental influences on the phys-ical-activity behavior of women. Be-cause of the limited empirical re-search, both quantitative (deductive)and qualitative (inductive) researchstudy designs were included in order tocomprehensively report the state ofresearch in this area. To assist with thisprocess, a form was developed torecord and organize study characteris-tics, such as study design, samplepopulation characteristics, and find-ings from each study specifically re-lated to the social environment.
Data Synthesis
After extraction, a systematic andexhaustive iterative process was used tocomprehend and synthesize the iden-tified social-environmental data. Be-cause of the broad scope of studydesigns and the conceptual nature ofsome of the information, the analysiswas conducted using a qualitative ap-proach. Data were scrutinized by mov-ing back and forth between the iden-tified social-environmental variables tocomprehend and analyze the informa-tion as well as to identify linkages. Thisrigorous iterative process to compre-hend and synthesize the research wasconducted by two researchers. Duringthis in-depth examination, the re-searchers identified common mean-ingful themes that emerged from thedata and used these themes to furtherorganize and conceptualize the infor-mation. Once this process was com-pleted, a preliminary framework wasdeveloped to build on the researchpresented. Finally, a third researcherwas consulted to review the data foraccuracy and to provide further input.
RESULTS
Forty-three studies (25 quantitativeand 18 qualitative) met the inclusioncriteria for this review and are listed in
Table 1; the study design, samplepopulation characteristics, and type ofsocial-environmental influences identi-fied in each study are also included. Ofthe 43 studies identified in this review,23 were conducted with women ofethnic minority populations.
The results of this review yieldedthree major areas that served as theorganization for this paper: socialsupport and social networks, life tran-sitions and multiple roles, and culturalstandards and gender role expecta-tions. Although not applied a priori,these three areas correspond roughlyto three levels of the social environ-ment as described by Bronfenbrenner:the microsystem (interpersonal inter-actions), the mesosystem (interactionsamong various environments, such asfamily settings, acquaintances, andwork groups), and the macrosystem(larger social system that includescultural beliefs and values).16,19–21
Social Support and Social Networks
Social networks are the connectionsbetween people that may provide socialsupport and that may serve otherfunctions.22 Social support includes aidor assistance exchanged by individuals,groups, or organizations (social net-works) through one of four methods:emotional, instrumental, information-al, or appraisal support.22 Emotionalsupport includes situations wherea person or group expresses encour-agement to or acceptance of others.Instrumental or tangible support in-volves providing someone with materi-al aid, direct help, or some type ofservice. Offering advice, suggestions,or information in any form constitutesinformational support, whereas ap-praisal support involves providing an-other person with constructive feed-back and an affirmation of beliefs andvalues.22,23 Social support is the moststudied and understood concept in thesocial environment, and it has beenidentified as a consistent positive cor-relate of physical-activity behavioramong women.24 Thirty-four of the 43studies identified in this reviewaddressed some aspect of socialsupport and social networks (Table 1).Of these 34 studies addressingsocial support, 19 were conductedwith women of ethnic minority popu-lations.
September/October 2008, Vol. 23, No. 1 3
For individual use only. Duplication or distribution prohibited by law.
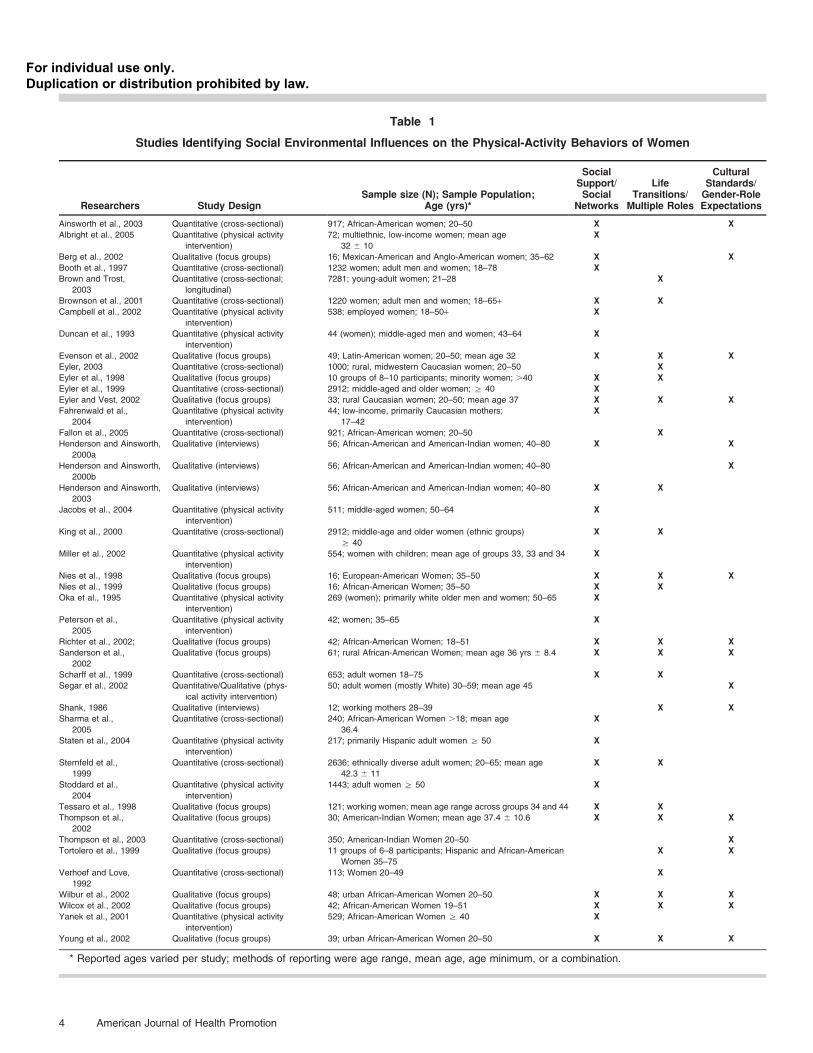
Table 1
Studies Identifying Social Environmental Influences on the Physical-Activity Behaviors of Women
Researchers Study DesignSample size (N); Sample Population;
Age (yrs)*
SocialSupport/Social
Networks
LifeTransitions/Multiple Roles
CulturalStandards/Gender-RoleExpectations
Ainsworth et al., 2003 Quantitative (cross-sectional) 917; African-American women; 20–50 X X
Albright et al., 2005 Quantitative (physical activity
intervention)
72; multiethnic, low-income women; mean age
32 6 10
X
Berg et al., 2002 Qualitative (focus groups) 16; Mexican-American and Anglo-American women; 35–62 X X
Booth et al., 1997 Quantitative (cross-sectional) 1232 women; adult men and women; 18–78 X
Brown and Trost,
2003
Quantitative (cross-sectional;
longitudinal)
7281; young-adult women; 21–28 X
Brownson et al., 2001 Quantitative (cross-sectional) 1220 women; adult men and women; 18–65+ X X
Campbell et al., 2002 Quantitative (physical activity
intervention)
538; employed women; 18–50+ X
Duncan et al., 1993 Quantitative (physical activity
intervention)
44 (women); middle-aged men and women; 43–64 X
Evenson et al., 2002 Qualitative (focus groups) 49; Latin-American women; 20–50; mean age 32 X X X
Eyler, 2003 Quantitative (cross-sectional) 1000; rural, midwestern Caucasian women; 20–50 X
Eyler et al., 1998 Qualitative (focus groups) 10 groups of 8–10 participants; minority women; .40 X X
Eyler et al., 1999 Quantitative (cross-sectional) 2912; middle-aged and older women; § 40 X
Eyler and Vest, 2002 Qualitative (focus groups) 33; rural Caucasian women; 20–50; mean age 37 X X X
Fahrenwald et al.,
2004
Quantitative (physical activity
intervention)
44; low-income, primarily Caucasian mothers;
17–42
X
Fallon et al., 2005 Quantitative (cross-sectional) 921; African-American women; 20–50 X
Henderson and Ainsworth,
2000a
Qualitative (interviews) 56; African-American and American-Indian women; 40–80 X X
Henderson and Ainsworth,
2000b
Qualitative (interviews) 56; African-American and American-Indian women; 40–80 X
Henderson and Ainsworth,
2003
Qualitative (interviews) 56; African-American and American-Indian women; 40–80 X X
Jacobs et al., 2004 Quantitative (physical activity
intervention)
511; middle-aged women; 50–64 X
King et al., 2000 Quantitative (cross-sectional) 2912; middle-age and older women (ethnic groups)
§ 40
X X
Miller et al., 2002 Quantitative (physical activity
intervention)
554; women with children; mean age of groups 33, 33 and 34 X
Nies et al., 1998 Qualitative (focus groups) 16; European-American Women; 35–50 X X X
Nies et al., 1999 Qualitative (focus groups) 16; African-American Women; 35–50 X X
Oka et al., 1995 Quantitative (physical activity
intervention)
269 (women); primarily white older men and women; 50–65 X
Peterson et al.,
2005
Quantitative (physical activity
intervention)
42; women; 35–65 X
Richter et al., 2002; Qualitative (focus groups) 42; African-American Women; 18–51 X X X
Sanderson et al.,
2002
Qualitative (focus groups) 61; rural African-American Women; mean age 36 yrs 6 8.4 X X X
Scharff et al., 1999 Quantitative (cross-sectional) 653; adult women 18–75 X X
Segar et al., 2002 Quantitative/Qualitative (phys-
ical activity intervention)
50; adult women (mostly White) 30–59; mean age 45 X
Shank, 1986 Qualitative (interviews) 12; working mothers 28–39 X X
Sharma et al.,
2005
Quantitative (cross-sectional) 240; African-American Women .18; mean age
36.4
X
Staten et al., 2004 Quantitative (physical activity
intervention)
217; primarily Hispanic adult women § 50 X
Sternfeld et al.,
1999
Quantitative (cross-sectional) 2636; ethnically diverse adult women; 20–65; mean age
42.3 6 11
X X
Stoddard et al.,
2004
Quantitative (physical activity
intervention)
1443; adult women § 50 X
Tessaro et al., 1998 Qualitative (focus groups) 121; working women; mean age range across groups 34 and 44 X X
Thompson et al.,
2002
Qualitative (focus groups) 30; American-Indian Women; mean age 37.4 6 10.6 X X X
Thompson et al., 2003 Quantitative (cross-sectional) 350; American-Indian Women 20–50 X
Tortolero et al., 1999 Qualitative (focus groups) 11 groups of 6–8 participants; Hispanic and African-American
Women 35–75
X X
Verhoef and Love,
1992
Quantitative (cross-sectional) 113; Women 20–49 X
Wilbur et al., 2002 Qualitative (focus groups) 48; urban African-American Women 20–50 X X X
Wilcox et al., 2002 Qualitative (focus groups) 42; African-American Women 19–51 X X X
Yanek et al., 2001 Quantitative (physical activity
intervention)
529; African-American Women § 40 X
Young et al., 2002 Qualitative (focus groups) 39; urban African-American Women 20–50 X X X
* Reported ages varied per study; methods of reporting were age range, mean age, age minimum, or a combination.
4 American Journal of Health Promotion
For individual use only. Duplication or distribution prohibited by law.

As illustrated in Table 2, three majorthemes emerged from the social sup-port literature and correspondedroughly to three types of social sup-port: emotional, tangible, and infor-mational. Many of the studies do notclearly distinguish between the differ-ent types of social support (i.e., tangi-ble or emotional); this in part may bebecause a given relationship oftenprovides multiple types of support.
Emotional Support. Research consis-tently has revealed that women wantencouragement and support for phys-ical activity from important people intheir lives, such as spouses, family, andfriends.25–40 In fact, survey results fromresearch with minority women confirmthat women with greater levels ofsupport from families or friends weresignificantly more likely to be physi-cally active.41,42
Emotional support from importantothers has also been identified asa positive factor in exercise adherence.Oka et al.43 found that support forexercise received from family andfriends at the midway point of a year-long program was the strongest pre-dictor of exercise adherence for bothmen and women. Similarly, an inter-vention conducted by Duncan et al.44
revealed that women who perceivedhigher levels of reassurance of worthwere more likely to sustain exercisebehaviors.
Other important sources of encour-agement for physical activity for wom-en beyond family and friends includephysicians or other health profes-sionals,33,45–49 others in the work envi-ronment,37,50 and others in a church orfaith-based environment.49,51
Having someone else with whom toexercise25–27,29–32,34,35,37,40,52 or havingthe opportunity to exercise ina group26,34,40,45 have been cited asimportant facilitators of physical activ-ity in women. This type of support isnot easily categorized; it is includedunder emotional support in this re-view, as that appears to be the closestfit.
Tangible Support. Areas of tangiblesupport identified by women includedirect help or assistance with tasks thatare associated with multiple roles, suchas household chores or caring forchildren, in order to have timeto be physically active (seeTable 2).29,30,34,36–39,53 Indeed, one in-tervention that targeted the instru-mental-support needs of women re-vealed that increasing partner supportfor women with young children al-lowed women to increase their physi-cal-activity behavior significantly.53
Informational Support. Informationalsupport may be provided verbally,through advice and suggestion, orthrough print or internet sources.
Examples of informational-supportneeds reported by women includetailored information that focuses onthe health benefits of physical activityfor women33,34,54 and information thatprovides tailored strategies for incor-porating physical activity into women’slives.26,28,37,52 Duncan et al.44 found thatinformational support (i.e., guidance)enhanced exercise adherence amongwomen. Although close relations oftenprovide emotional and tangible sup-port, health professionals have beenidentified as an important source ofinformational support.45,46,55
Previous studies have also revealedthe potential importance of combiningseveral types of support. For example,recent interventions have shown posi-tive changes in physical-activity behav-ior by using tailored messages andinformation combined with some typeof counseling support46,47,52,57 andsupport from group members.48,49,51
Miller et al.53 reported increases inexercise behavior for mothers whoreceived print information and partnersupport (tangible support) as opposedto those who received print informa-tion only. Similarly, Campbell et al.50
discovered improvements in strength-ening and flexibility exercise ina worksite intervention among womenwho received information and emo-tional support compared with thosethat received information only.
Table 2
Overriding Social-Environmental Influences on the Physical-Activity Behavior of Women
Social Support and Social Networks Life Transitions and Multiple RolesCultural Standards andGender-role Expectations
& Emotional support from important others:
support from spouse or significant other, family,
friends, and community; lack of support and
acceptance for women to be active from these
influences
& Increasing responsibilities associated with
life transitions: changing roles through
marriage (or committed relationship),
employment status, parenthood, caregiving
& Acceptance of physical activity for adult
women: perceived lack of acceptance for
adult women participating in physical activity;
without acceptance, women feel guilty or
selfish for taking time to be active
& Tangible support: women need help with
child care and household duties; increased
need due to increased responsibilities tied to
home, work, and community networks;
women need others to exercise with
& Reduced discretionary time and low
priority of physical activity: lack of leisure-time
because of multiple roles and responsibilities
(wife, partner, mother, employee, caregiving,
in addition to being head of household)
& Cultural appropriateness of physical activity
in women: physical activity not seen as being
an appropriate behavior for adult women;
engrained family, household, and caregiving
responsibilities lead women to put the needs
of others first
& Informational support: need for targeted and
tailored physical activity information for women;
information and assistance from health
professionals and important others
& Beliefs about being active enough: being
busy is equated with physical activity;
women may see themselves as being
sufficiently active even though it may
not be enough for health benefits
& Importance of physically active adult female
role models: lack of role models in the
immediate and larger social environment
September/October 2008, Vol. 23, No. 1 5
For individual use only. Duplication or distribution prohibited by law.

Life Transitions and Multiple Roles
Life transitions include key lifeevents, such as marriage, parenthood,and employment, and may be associ-ated with multiple roles, such as wife,mother, employee, caretaker, andhead of household. Twenty-threestudies included in this review ad-dressed some aspect of the influenceof life transitions and multiple roleson the physical-activity behavior ofwomen (Table 1). More than half (14)of these 23 studies included a sampleof women from ethnic minoritygroups. Salient issues related to lifetransitions and multiple roles includeincreasing responsibilities that maycome with life transitions, reduceddiscretionary time related to responsi-bilities, lower priority of physical ac-tivity, and belief that activity involvedin performing role tasks, such ascaregiving, provides sufficient levels ofactivity (Table 2).
Increasing Responsibilities Associated WithLife Transitions. Adulthood, for women,is often marked by significant lifestylechanges associated with shifting rolesand responsibilities and is generallya time when major life events such asmarriage, parenthood, and employ-ment occur. Furthermore, as womentransition into middle-age years, theymay be faced with increased caregivingresponsibilities of older adult rela-tives.32,56 Women’s social roles and theadded responsibilities of those roleshave a profound effect on the physical-activity behavior of women.57–60 Forexample, Fallon et al.58 investigated thedegree to which social-role constraint(e.g., housework, childcare) impactedthe exercise behavior of African-Amer-ican women. Women with more socialrole constraints had lower levels of self-efficacy for physical activity comparedwith those who had fewer social-roleconstraints.
Researchers have begun to examinewhich roles have the most impact onthe physical-activity behavior of wom-en. Brown et al.57 reported that eventssuch as marriage, childbirth and par-enting, and new employment were allassociated with decreased levels ofactivity in young-adult women. Verhoefet al.61 reported that, of three socialroles (parenthood, marital status, andemployment status), only parenthood
had a negative relationship in regardsto whether a woman exercised.
Reduced Discretionary Time and LowPriority of Physical Activity. The issue ofreduced discretionary time is closelyrelated to increasing responsibilitiesassociated with life changes for women.One of the most significant barriersto physical activity identified bywomen is lack of time because ofmultiple roles or caregiving responsi-bilities.28,29,32–34,37–39,40,54,59–61 Minoritywomen in particular have indicatedthat family responsibilities are a priorityand have noted that these responsibil-ities required a great deal of time andare often physically demand-ing.26,28,34,54,62 Results from the Wo-men’s Cardiovascular Health NetworkProject, which was conducted withgroups of African-American, American-Indian, Hispanic, and Caucasian wom-en, revealed that all women, regardlessof race, perceived that family, house-hold, and caregiving responsibilitiespresented a major barrier to leisure-time physical activity.25,28,30,35,36,38,40
Women also reported that they didnot have structured time comparedwith their husbands and that themajority of their time was spent doingintermittent, unstructured activity thatdid not allow for specific structuredactivities, such as exercise.29,64 Similar-ly, women reported that they did notfeel as though they had discretionarytime to engage in leisure-time physicalactivity because of the demands ofothers in their daily lives.60,62 In addi-tion, some women believed that, whenthey did take the time to be active, itwas wasted time that could have beenspent being more productive.29,30,64
Beliefs About Being Active Enough. Anumber of studies have shown that,although many women did not con-sider themselves to be exercisers, theydid consider themselves to be physicallyactive because of their busy schedules,which revolved around social roles andresponsibilities.27,29,30,35,39,40,54,64 In fact,results from research that measureda broad range of activity indicated thatmany women had high levels ofhousehold, work-related, or caregivingactivities. For example, Sternfeld etal.63 found that, although women withchildren perceived themselves as hav-ing little time for exercise, they did have
higher levels of occupational/caregiv-ing activity. Similarly, Scharff et al.59
found that, among women 49 years ofage or younger, having children wasstrongly associated with performingless structured and less intense physicalactivity but also was predictive ofadequate levels of physical activityduring daily living (defined as child-care, work in the home, home repair,and yard work).
Closely related to the type of day-to-day activity that women describe is theissue of being too tired to exercise.Women have consistently reportedthat traditional household, childcare,caregiving, and work-related activitiesoften leave them feeling too tiredto add regular exercise to theirday.27,32,34–36,38,54,56,59,60,64 These feelingsof being busy and of being on theirfeet all day lead many women tobelieve that they are doing enoughphysical activity.29,65,66
Although some women reportedthat they recognized the importance ofphysical activity to their health, theywere not inclined to add more physicalactivity to their regular schedule.54,60
Furthermore, reports from some stud-ies revealed that, although women didthink they were physically active, theydid not think it was enough to benefittheir health.29,35,66 Research remainsequivocal regarding the health benefitsof occupational and household activi-ties for women.
Cultural Standards and Gender-RoleExpectations
Gender-role expectations are sociallyand culturally determined roles andpatterns of behavior that society viewsas appropriate. Cultural standards in-clude learned and accepted values,beliefs, norms, and practices that aretransferred, directly or indirectly, forgenerations.67 Gender-role expecta-tions and cultural standards are themost complex aspects of the socialenvironment and are possibly the leaststudied. Of the 43 studies identified inthis review, 17 identified cultural andgender-role issues associated with thephysical activity of women. Of the 17studies, 13 were conducted with wom-en in ethnic minority groups. The keyissues that surfaced in this area in-cluded acceptance of physical activity,cultural appropriateness of physical
6 American Journal of Health Promotion
For individual use only. Duplication or distribution prohibited by law.

activity in adult women, and a lack ofrole models (Table 2).
Acceptance of Physical Activity forAdult Women. Results from qualitativeresearch revealed that women per-ceived acceptance for physical-activitybehavior from spouses and significantothers as a necessary and essentialcomponent for allowing them to taketime to participate in physical activi-ty.26,28,30,35,36,38,39 Specifically, Hispanicwomen indicated that it was criticalthat they had consent from theirhusbands to participate in activity,26,28
and some suggested that educationalinformation be directed at theirspouses by providing a supportive,male role model for them to emulate.28
Furthermore, women in a worksite in-tervention stated that it was essentialthat their families understood howimportant it was for them to have timefor themselves in order to add physicalactivity and other health behaviors totheir lifestyles.37 Without this accep-tance, women reported feeling guiltyor selfish for taking personal time to beactive.30,39,60,64
Cultural Appropriateness of Physical Ac-tivity for Adult Women. Some womenhave also reported a social pressurethat implied it was not appropriate forthem to participate in physical activi-ty26,28,36,38,39 or that they were discour-aged from being physical active.56
Women have reported that there weresignificant social and cultural pressuresto conform to their roles as mothersand primary caretakers of the familyand that physical activity was not valuedin their communities.28,36,38,40 Drivenby gender-role expectations and cul-tural standards, as well as by the addedcomplexity of multiple role responsi-bilities, women are often motivated orinfluenced to conform to a caregivingrole and to put family obligations andrelationships with others ahead of theirown needs.26,31,33,38,40,54,62,68 As noted inthe literature, these feelings of re-sponsibility can have a profound im-pact on the decisions made by women,including those related to their healthand behavior.26,28,32,38,40,54,68
Importance of Physically Active, Adult,Female Role Models. One of the mostnotable issues identified from researchwith women was the lack of, and the
need for, positive, physically active rolemodels.30,36,38–40,60 The scarcity of rolemodels for women adds to a perceivedlack of community and social support.Women reported the need for physi-cally active role models to demonstrateways to incorporate activity into theirlives and to make it more sociallyacceptable.38,39 Women in the Wo-men’s Cardiovascular HealthNetwork Project emphasized thathaving role models and open commu-nity support would be essential forthem to feel comfortable and confi-dent about adding activity to theirlifestyles.36,38,39 Women also empha-sized the importance of seeing othersbe active27,32,36,38–40,56,69 and of seeingothers in their social networks (i.e.,family, peers, role models) engage inactivity.32
CONCLUSIONS
This review reveals the wide range offactors in the social environment thatinfluence women, and it providesevidence regarding the important in-fluences that social-environmental fac-tors exert on physical-activity behaviorin women. At the microsystem level,many women report a lack of socialsupport, including emotional, tangi-ble, and informational support, forengaging in physical activity. At themesosystem level, women assume a va-riety of social roles as they transitionfrom early to late adulthood. Managingmultiple roles, including caregivingresponsibilities, may create role strainand overload that make it difficult toinclude physical activity as a priority.Finally, at the macrosystem level,women are exposed to societal mes-sages indicating that physical activity isnot appropriate for women and maynot be accepted within their families,institutions, and communities.
Conceptualizing and Defining Social-Environmental Influences on Physical-Activity Behavior in Women
As noted earlier, many theoriesrecognize the influence of the socialenvironment on health behaviors;however, there is no comprehensiveframework that identifies and definesspecific elements within the socialenvironment, particularly as applicableto adult women. Bronfenbrenner’s
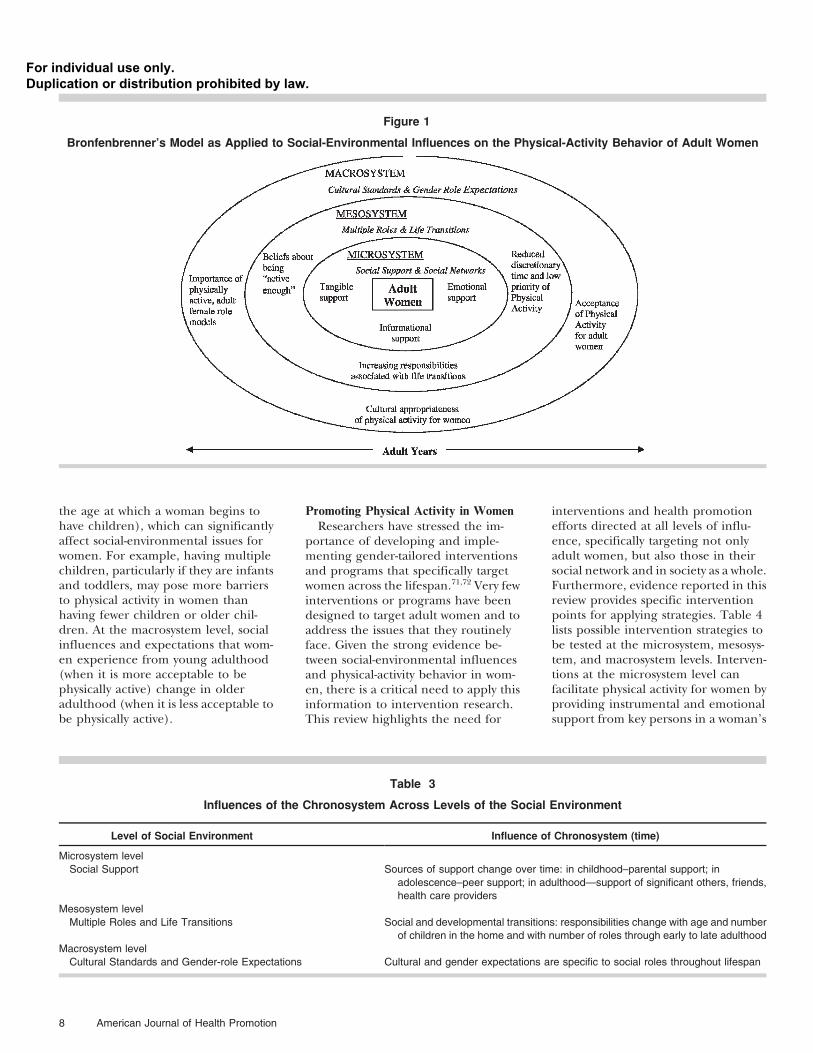
levels of influence (e.g., micro-, meso-,and macrosystems), as further definedand applied to women’s physical activ-ity in this review, may be a plausiblefirst step to developing a social-envi-ronmental framework. Based on thisreview and building from Bronfen-brenner’s ecological model, we presenta preliminary framework that describesthe elements of the social environmentfor physical activity among women(Figure 1). This model also draws fromthe works of Halfon et al.,70 Spence etal.,21 Booth et al.,12 and Renn et al.,20
and it recognizes the importance of lifestages and transitions, cultural andethnic norms, social and gender roles,and social support on physical activity.This model emphasizes relationshipsand interactions among individualswithin a variety of contexts rather thanfocusing on the specific contexts andsettings (e.g., communities, organiza-tions). Similar to ecological models,this model posits that the social envi-ronment exerts both direct and in-direct influences on behavior. Theinfluences of the levels of the modelalso overlap and form what Renn etal.20 describe as a system of nested,interdependent networks. For exam-ple, cultural standards and gender-roleexpectations are broad, social influ-ences; however, these ‘‘messages’’ arecommunicated via socialization pro-cesses with family and peers duringchildhood and are reinforced throughinterpersonal interactions in varioussettings (e.g., workplaces, churches)throughout adulthood.
Another important aspect to note inrelation to Bronfenbrenner’s modeland the social-environmental frame-work presented here is the influence ofthe chronosystem, which is depicted inTable 3. The chronosystem representsthe passage of time. As noted above,socialization processes, such as thoseconcerning appropriate gender roles,begin very early in life. The passage oftime is particularly relevant for womenacross adulthood. For example, at themicrosystem level, women’s social sup-port needs and sources of supportchange from young adulthood to lateradulthood. At the mesosystem level,one example of the impact of thepassage of time would be the numberand ages of children that a woman hasthroughout the adult years (as well as
September/October 2008, Vol. 23, No. 1 7
For individual use only. Duplication or distribution prohibited by law.
the age at which a woman begins tohave children), which can significantlyaffect social-environmental issues forwomen. For example, having multiplechildren, particularly if they are infantsand toddlers, may pose more barriersto physical activity in women thanhaving fewer children or older chil-dren. At the macrosystem level, socialinfluences and expectations that wom-en experience from young adulthood(when it is more acceptable to bephysically active) change in olderadulthood (when it is less acceptable tobe physically active).
Promoting Physical Activity in Women
Researchers have stressed the im-portance of developing and imple-menting gender-tailored interventionsand programs that specifically targetwomen across the lifespan.71,72 Very fewinterventions or programs have beendesigned to target adult women and toaddress the issues that they routinelyface. Given the strong evidence be-tween social-environmental influencesand physical-activity behavior in wom-en, there is a critical need to apply thisinformation to intervention research.This review highlights the need for
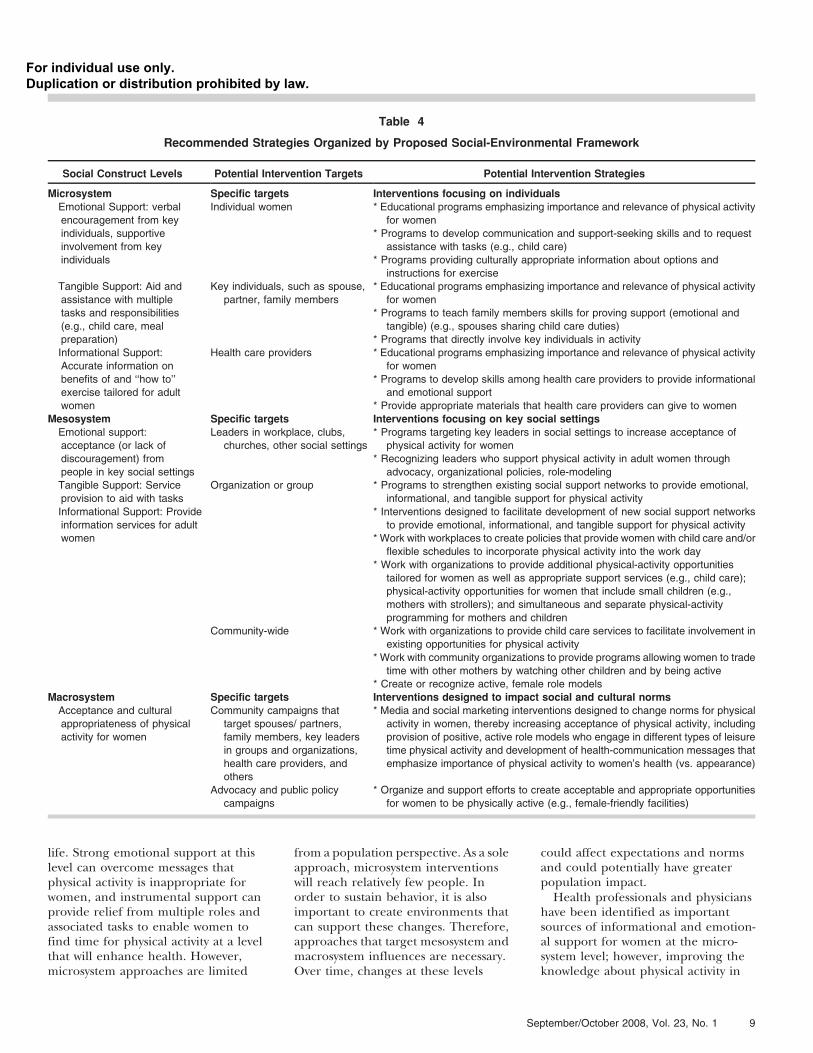
interventions and health promotionefforts directed at all levels of influ-ence, specifically targeting not onlyadult women, but also those in theirsocial network and in society as a whole.Furthermore, evidence reported in thisreview provides specific interventionpoints for applying strategies. Table 4lists possible intervention strategies tobe tested at the microsystem, mesosys-tem, and macrosystem levels. Interven-tions at the microsystem level canfacilitate physical activity for women byproviding instrumental and emotionalsupport from key persons in a woman’s
Figure 1
Bronfenbrenner’s Model as Applied to Social-Environmental Influences on the Physical-Activity Behavior of Adult Women
Table 3
Influences of the Chronosystem Across Levels of the Social Environment
Level of Social Environment Influence of Chronosystem (time)
Microsystem level
Social Support Sources of support change over time: in childhood–parental support; in
adolescence–peer support; in adulthood—support of significant others, friends,
health care providers
Mesosystem level
Multiple Roles and Life Transitions Social and developmental transitions: responsibilities change with age and number
of children in the home and with number of roles through early to late adulthood
Macrosystem level
Cultural Standards and Gender-role Expectations Cultural and gender expectations are specific to social roles throughout lifespan
8 American Journal of Health Promotion
For individual use only. Duplication or distribution prohibited by law.
life. Strong emotional support at thislevel can overcome messages thatphysical activity is inappropriate forwomen, and instrumental support canprovide relief from multiple roles andassociated tasks to enable women tofind time for physical activity at a levelthat will enhance health. However,microsystem approaches are limited
from a population perspective. As a soleapproach, microsystem interventionswill reach relatively few people. Inorder to sustain behavior, it is alsoimportant to create environments thatcan support these changes. Therefore,approaches that target mesosystem andmacrosystem influences are necessary.Over time, changes at these levels
could affect expectations and normsand could potentially have greaterpopulation impact.
Health professionals and physicianshave been identified as importantsources of informational and emotion-al support for women at the micro-system level; however, improving theknowledge about physical activity in
Table 4
Recommended Strategies Organized by Proposed Social-Environmental Framework
Social Construct Levels Potential Intervention Targets Potential Intervention Strategies
Microsystem Specific targets Interventions focusing on individualsEmotional Support: verbal
encouragement from key
individuals, supportive
involvement from key
individuals
Individual women * Educational programs emphasizing importance and relevance of physical activity
for women
* Programs to develop communication and support-seeking skills and to request
assistance with tasks (e.g., child care)
* Programs providing culturally appropriate information about options and
instructions for exercise
Tangible Support: Aid and
assistance with multiple
tasks and responsibilities
(e.g., child care, meal
preparation)
Key individuals, such as spouse,
partner, family members
* Educational programs emphasizing importance and relevance of physical activity
for women
* Programs to teach family members skills for proving support (emotional and
tangible) (e.g., spouses sharing child care duties)
* Programs that directly involve key individuals in activity
Informational Support:
Accurate information on
benefits of and ‘‘how to’’
exercise tailored for adult
women
Health care providers * Educational programs emphasizing importance and relevance of physical activity
for women
* Programs to develop skills among health care providers to provide informational
and emotional support
* Provide appropriate materials that health care providers can give to women
Mesosystem Specific targets Interventions focusing on key social settingsEmotional support:
acceptance (or lack of
discouragement) from
people in key social settings
Leaders in workplace, clubs,
churches, other social settings
* Programs targeting key leaders in social settings to increase acceptance of
physical activity for women
* Recognizing leaders who support physical activity in adult women through
advocacy, organizational policies, role-modeling
Tangible Support: Service
provision to aid with tasks
Organization or group * Programs to strengthen existing social support networks to provide emotional,
informational, and tangible support for physical activity
Informational Support: Provide
information services for adult
women
* Interventions designed to facilitate development of new social support networks
to provide emotional, informational, and tangible support for physical activity
* Work with workplaces to create policies that provide women with child care and/or
flexible schedules to incorporate physical activity into the work day
* Work with organizations to provide additional physical-activity opportunities
tailored for women as well as appropriate support services (e.g., child care);
physical-activity opportunities for women that include small children (e.g.,
mothers with strollers); and simultaneous and separate physical-activity
programming for mothers and children
Community-wide * Work with organizations to provide child care services to facilitate involvement in
existing opportunities for physical activity
* Work with community organizations to provide programs allowing women to trade
time with other mothers by watching other children and by being active
* Create or recognize active, female role models
Macrosystem Specific targets Interventions designed to impact social and cultural normsAcceptance and cultural
appropriateness of physical
activity for women
Community campaigns that
target spouses/ partners,
family members, key leaders
in groups and organizations,
health care providers, and
others
* Media and social marketing interventions designed to change norms for physical
activity in women, thereby increasing acceptance of physical activity, including
provision of positive, active role models who engage in different types of leisure
time physical activity and development of health-communication messages that
emphasize importance of physical activity to women’s health (vs. appearance)
Advocacy and public policy
campaigns
* Organize and support efforts to create acceptable and appropriate opportunities
for women to be physically active (e.g., female-friendly facilities)
September/October 2008, Vol. 23, No. 1 9
For individual use only. Duplication or distribution prohibited by law.

these important sources may also im-pact mesosystem level issues. In orderto have the type of influence necessaryto facilitate behavior change and tocombat many of the issues identified inthis review, it may be important toemploy the expertise of exercise sci-ence and health promotion specialistswithin the health care environment.Researchers have noted that it is in-correct to assume that everyone knowshow to be physically active, especiallywomen who may not have been ex-posed to activity in their youth.11
Trained physical-activity professionalscan ensure that all target populationsreceive accurate, effective, and cultur-ally appropriate information abouthow to incorporate physical activityinto their lives using sound scientificand theoretical principles. Althoughother health professionals may under-stand the importance of a physicallyactive lifestyle, they may not able toprovide the type of expertise andassistance needed to support theirpatients in the initiation and mainte-nance of a physically active lifestylethroughout the lifespan. Althoughmany physician offices, clinics, andhospitals have employed the services ofnutritionist to tackle diet issues, veryfew have integrated exercise andhealth-promotion specialists into thehealth system to combat physical in-activity.
From a macrosystem perspective,women are bombarded with messageseveryday about appearance, motheringand caregiving, and reproductive is-sues; however, few messages are con-veyed to women about the appropri-ateness and benefits of physical activityfor women. The results of this reviewsuggest that women could benefit byreceiving alternative messages andimages to encourage and support theirphysical-activity behavior. Shepard73
stated that, ‘‘hearts must be capturedbefore minds,’’ and emphasized thathealth-promotion specialists musttranslate scientific data into soundbites that are appropriate for thetargeted population and that use sim-ple messages to inform, influence, andmotivate. Another important strategy isto identify alternative images that adultwomen can relate to as role models.
Health communication can increasethe knowledge and awareness of a seg-
mented audience as well as influenceperceptions, beliefs, and attitudes thatmay assist in changing social norms.74
Through this influence and awareness,it may also prompt action from theintended audience, provide a modelfor certain health skills (i.e., physicalactivity), and act to reinforce attitudesand behavior. Overall, health commu-nication can be used to counter mis-perceptions as well as to act as anadvocate for a particular behavior.Information from this review has illu-minated some of the messages thatwomen would like to hear but alsohighlights the critical need for moreresearch with women to inform thedevelopment of health-communicationprograms.
Finally, little research has exploredthe effect of public policy on physicalactivity in general; even less has beenemployed in regards to women. Al-though athletic opportunities for girlsand women have increased signifi-cantly because of the passage of TitleIX, a federal law prohibiting sexdiscrimination in educational environ-ments, and more females are partici-pating in organized sports than everbefore, the number of women whoparticipate in sports or physical activityinto adulthood decreases signifi-cantly.6,7 Title IX is a positive exampleof the effect of public policy; however,few studies have examined the long-term effects of this policy on thephysical-activity behavior in women,especially from the perspective of thesocial environment. Changes in publicpolicy have the potential to influencethe social environment by changingsocial norms.75 Integrating informa-tion identified in this review with thedevelopment of policy in differentsettings, such as the work environment,presents yet another strategy for posi-tively influencing the physical-activitybehavior of women.
In addition to the framework pro-posed here, the structural ecologicalmodel of health75 provides a usefulframework for guiding interventions tochange both the social and physicalenvironments, in order to influencehealth behavior at the populationlevel. Social and physical structurescould affect health behavior directlywithout shifting attitudes or beliefs;they may also work indirectly by medi-
ating changes in social norms andexpectations. This model provides ad-ditional points of intervention by in-corporating aspects of the physicalenvironment that may also enhancechanges in the social environment.Examples of this, reported by womenthroughout the literature, are a per-ceived lack of availability and access toprograms specifically targeting womenand a lack of availability of places toexercise.27–30,38,39,69 Although these arephysical-environmental issues, thepresence or absence of available pro-grams or facilities may convey a mes-sage that positively or negatively influ-ences physical-activity behavior and areadditional areas of influence that needto be explored. In fact, recent researchinvestigating the influence of an urbanpark on the physical-activity behaviorof women revealed that the presence ofothers and chance meetings in thepark provided emotional support andfeelings of safety and enjoyment ofphysical activity among women.76
Although the studies chosen for thisreview varied greatly in design, repre-senting both qualitative and quantita-tive research, an attempt was made toidentify and include any relevant re-search that might provide some insightinto social-environmental influenceson women and their physical-activitybehavior. Although an effort was madeto conduct a methodical search of theliterature, relevant articles may haveinadvertently been omitted.
In conclusion, this literature reviewprovides important evidence regardingthe influence of the social environ-ment on the physical-activity behaviorof women across the adult lifespan(chronosystem), and it provides newavenues for tailoring interventions forwomen. The social-environmentalframework presented here providesa guide for health-promotion practi-tioners and researchers to translateevidence into practice by incorporatingstrategies across the microsystem, me-sosystem, and macrosystem levels. It isencouraging that research identifyingsocial-environmental factors amongwomen, particularly among ethnicwomen, has increased significantly inthe last decade; however, more re-search and interventions applying thisinformation and targeting women areneeded.
10 American Journal of Health Promotion
For individual use only. Duplication or distribution prohibited by law.

References
1. Manson J, Hu F, Rich-Edwards J, et al. Aprospective study of walking comparedwith vigorous exercise in the prevention ofcoronary heart disease in women.N Engl J Med. 1999;341:650–658.
2. Martinez M, Giovannucci E, Spiegelman D,et al. Physical activity, body size, andcolorectal cancer in women [abstract].Am J Epidemiol. 1996;143:S73.
3. McTiernan A, Kooperberg C, White E, etal. Recreational physical activity and therisk of breast cancer in postmenopausalwomen. JAMA. 2003;290(10):1331–1336.
4. Hu F, Manson J, Stampfer M, et al. Aprospective study of physical activity andrisk of stroke in women [abstract].Am J Epidemiol. 1999;149:S39.
5. Hu F, Sigal R, Rich-Edwards J, et al.Walking compared with vigorous physicalactivity and risk of type 2 diabetes mellitusin women. JAMA. 1999;282:1433–1439.
6. Centers for Disease Control andPrevention: Prevalence of recommendedlevels of physical activity among women—Behavioral Risk Factor SurveillanceSystem, United States, 1992. MMWR. 1995Feb;44(6):105–113.
7. US Department of Health Human Services.Physical activity and health: A report of theSurgeon General. Atlanta, GA: Centers forDisease Control and Prevention, NationalCenter for Chronic Disease Prevention andHealth Promotion, 1996.
8. Rockhill B, Willett W, Manson J, et al.Physical activity and mortality: a prospectivestudy among women. Am J Public Health.2001;91:578–583.
9. Schoenborn C, Adams P, Barnes P,Vickerie J, Schiller J. Health Behaviors ofAdults: United States, 1999–2001. NationalCenter For Health Statistics. Vital Health Stat.2004;10(219):39–54.
10. Eyler A, Brownson R, King A, et al. Physicalactivity and women in the United States: anoverview of health benefits, prevalence,
and intervention opportunities. WomenHealth. 1997;26(3):27–49.
11. Jacobs Institute of Women’s Health,National conference on physical activityand women’s health. Women’s Health Issues.1998;8:69–88.
12. Booth S, Mayer J, Sallis J, et al.Environmental and societal factors affectfood choice and physical activity: rationale,influences, and leverage points. Nutr Rev.2001;59(3):S21–S39.
13. Economos C, Brownson R, DeAngelis M, etal. What lessons have been learned fromother attempts to guide social change?Nutr Rev. 2001;59(3):S40–S56.
14. Kahn E, Ramsey L, Brownson R, et al. Theeffectiveness of interventions to increasephysical activity: a systematic review.Am J Prev Med. 2002;22(4S):73–107.
15. Bandura A. Social Foundations of Thoughtand Action: A Social Cognitive Theory.Englewood Cliffs, NJ: Prentice Hall; 1986.
16. Sallis J, Owen N. Ecological models ofhealth behavior. In: Glanz K, Rimer B,Lewis F, eds. Health Behavior and HealthEducation. 3rd ed. San Francisco: Jossey-Bass; 2002:462–484.
17. Wenzel L, Glanz K, Lerman C. Stress,coping, and health behavior. In: Glanz K,Rimer B, Lewis F, eds. Health Behavior andHealth Education. 3rd ed. San Francisco,CA: Jossey-Bass; 2002:210–239.
18. Lewis M, DeVellis B, Sleath B. Socialinfluence and interpersonalcommunication in health behavior. In:Glanz K, Rimer B, Lewis F, eds. HealthBehavior and Health Education. 3rd ed. SanFrancisco, CA: Jossey-Bass; 2002:240–264.
19. Bronfenbrenner U. Developmentalecology through space and time: A futureperspective. In: Moen P, Elder G Jr, eds.Examining lives in context: Perspectives on theecology of human development. Washington,DC: American Psychological Association;1995:619–647.
20. Renn K, Arnold K. Reconceptualizingresearch on college student peer culture.J Higher Educ. 2003;74(3):261–291.
21. Spence J, Lee R. Toward a comprehensivemodel of physical activity. J Psych Sport.2003;4:7–24.
22. Heaney C, Israel B. Social networks andsocial support. In: Glanz K, Rimer B, LewisF, eds. Health Behavior and Health Education.3rd ed. San Francisco, CA: Jossey-Bass;2002:185–209.
23. Bartholomew L, Parcel G, Kok G, GottliebN. Intervention mapping: Designing theory-based and evidence-based health promotionprograms. Mountain View, CA: MayfieldPublishing Company; 2001.
24. Eyler A, Wilcox S, Matson-Koffman D, et al.Correlates of physical activity amongwomen from diverse racial/ethnic groups:a review. J Womens Health Gend Based Med.2002;11(3):239–253.
25. Ainsworth B, Wilcox S, Thompson W,Richter D, Henderson K. Personal, social,and physical environmental correlates ofphysical activity in African-Americanwomen in South Carolina. Am J Prev Med.2003;25(3Si):23–29.
26. Berg J, Cromwell S, Arnett M. Physicalactivity: perspectives of Mexican Americanand Anglo American midlife women.Health Care Women Int. 2002;23:894–904.
27. Brownson R, Baker E, Housemann R,Brennan L, Bacak S. Environmental andpolicy determinants of physical activity inthe United States. Am J Public Health.2001;91(12):1995–2003.
28. Evenson K, Sarmiento O, Macon L, TawneyK, Ammerman A. Environmental, policy,and cultural factors related to physicalactivity among Latina immigrants. WomenHealth. 2002;36(2):43–57.
29. Eyler A, Baker E, Cromer L, et al. Physicalactivity and minority women: a qualitativestudy. Health Educ Behav. 1998;25(5):640–652.
30. Eyler A, Vest J. Environmental, policy, andcultural factors related to physical activityamong in White women. Women Health.2002;36(2):111–112.
31. Henderson K, Ainsworth B. Theconnections between social support andwomen’s physical activity involvement: thecultural activity participation study. WomenSports Phys Act J. 2000;9(2):27–53.
32. Henderson K, Ainsworth B. A synthesis ofperceptions about physical activity amongolder African American and AmericanIndian women. Am J Public Health.2003;93(2):313–317.
33. Nies M, Vollman M, Cook T. Facilitators,barriers, and strategies for exercise inEuropean American women in thecommunity. Public Health Nurs.1998;15(4):263–272.
34. Nies M, Vollman M, Cook T. African-American women’s experiences withphysical activity in their daily lives. PublicHealth Nurs. 1999;16:23–31.
35. Richter D, Wilcox S, Greaney M,Henderson K, Ainsworth B.Environmental, policy, and cultural factorsrelated to physical activity in AfricanAmerican women. Women Health.2002;36(2):91–109.
36. Sanderson B, Littleton M, Pulley L.Environmental, policy, and cultural factorsrelated to physical activity among rural,African American women. Women Health.2002;36(2):75–90.
37. Tessaro I, Campbell M, Benedict S, et al.Developing a worksite health promotionintervention: health works for women.Am J Health Behavior. 1998;22(6):434–442.
38. Thompson J, Allen P, Cunningham-SaboL, et al. Environmental, policy, andcultural factors related to physical activityin sedentary American Indian women.Women Health. 2002;36(2):59–74.
39. Wilbur J, Chandler P, Dancy B, Choi J,Plonczynski D. Environmental, policy, andcultural factors related to physical activityin urban, African American women.Women Health. 2002;36(2):17–28.
40. Young D, He X, Harris J, Mabry I.Environmental, policy, and cultural factorsrelated to physical activity in well-educatedurban African American women. WomenHealth. 2002;36(2):29–41.
41. Eyler A, Brownson R, Donatelle R, et al.Physical activity social support and middle-
SO WHAT? Implications for Health
Promotion Practitioners and
Researchers
Social-environmental influencesidentified in this review providehealth-promotion specialists andresearchers an organizing frame-work for developing innovativephysical activity interventions thattarget the needs of women acrossthe adult years and provide practi-tioners with specific strategies toaddress social influences acrossmultiple levels. Additional researchis needed to expand and test thesocial-environmental frameworkand strategies based on frameworkcomponents on physical-activity be-havior in women.
September/October 2008, Vol. 23, No. 1 11
For individual use only. Duplication or distribution prohibited by law.
and older-aged minority women: resultsfrom a US survey. Soc Sci Med. 1999;49:781–789.
42. Sharma M, Sargent L, Stacy R. Predictorsof leisure-time physical activity amongAfrican American women. Am J HealthBehavior. 2005;29(4):352–359.
43. Oka R, King A, Young D. Sources of socialsupport as predictors of exerciseadherence in women and men ages 50 to65 years. Women’s Health: Research onGender, Behavior, and Policy. 1995;1(2):161–175.
44. Duncan T, Duncan S, McAuley E. The roleof domain and gender specific provisionsof social relations in adherence toa prescribed exercise regimen. J Sport ExercPsychol. 1993;15:220–231.
45. Booth M, Bauman A, Owen N, Gore C.Physical activity preferences, preferredsources of assistance, and perceivedbarriers to increased activity amongphysically inactive Australians. Prev Med.1997;26:131–137.
46. Fahrenwald N, Atwood J, Walker S,Johnson D, Berg K. A randomized pilottest of ‘‘Moms on the Move:’’ a physicalactivity intervention for WIC mothers. AnnBehav Med. 2004;27(2):82–90.
47. Jacobs A, Ammerman A, Ennett S, et al.Effects of a tailored follow-up interventionon health behaviors, beliefs and attitudes.J Womens Health. 2004;13(5):557–568.
48. Staten L, Gregory-Mercado K, Ranger-Moore J, et al. Provider counseling, healtheducation, and community health workers:the Arizona WISEWOMAN Project.J Womens Health. 2004;13(5):547–556.
49. Yanek L, Becker D, Moy T, Gittlesohn J,Koffman D. Project Joy: faith basedcardiovascular health promotion forAfrican American women. Public HealthRep. 2001;116(S1):68–81.
50. Campbell M, Tessaro I, DeVellis B, et al.Effects of a tailored health promotionprogram for female blue-collar workers:health works for women. Prev Med.2002;34:313–323.
51. Peterson J, Yates B, Atwood J, Hertzog M.Effects of a physical activity interventionfor women. West J Nur Res. 2005;27(1):93–110.
52. Stoddard A, Palombo R, Troped P,Sorenson G, Will J. Cardiovascular diseaserisk reduction: the MassachusettsWISEWOMEN Project. J Womens Health.2004;13(5):539–546.
53. Miller Y. Trost S, Brown W. Mediators ofphysical activity behavior change amongwomen with young children. Am J Prev Med.2002;23(2S):98–103.
54. Wilcox S, Richter D, Henderson K,Greaney M, Ainsworth B. Perceptions ofphysical activity and personal barriers andenablers in African American women. EthnDis. 2002;12:353–362.
55. Albright C, Pruitt L, Castro C, et al.Modifying physical activity in amultiethnic sample of low-incomewomen: one-year results from the IMPACT(Increasing Motivation for PhysicalACTivity) Project. Ann Behav Med.2005;30(3):191–200.
56. King A, Castro C, Wilcox S, et al. Personaland environmental factors associated withphysical inactivity among different racial-ethnic groups of U.S. middle-aged andolder-aged women. Health Psychol.2000;19(4):354–364.
57. Brown W, Trost A. Life transitions andchanging physical activity patterns inyoung women. Am J Prev Med. 2003;25(2):140–143.
58. Fallon E, Wilcox S, Ainsworth B. Correlatesof self-efficacy for physical activity inAfrican-American women. Women Health.2005;41(3):47–62.
59. Scharff D, Homan S, Kreuter M, BrennanL. Factors associated with physical activityacross the life span: implications forprogram development. Women Health.1999;29(2):115–134.
60. Shank J. An exploration of leisure in thelives of dual career women. Journal ofLeisure Research. 1986;18(4):300–319.
61. Verhoef M, Love E. Women’s exerciseparticipation: the relevance of social rolescompared with non-role relateddeterminants. Can J Public Health.1992;83(5):367–370.
62. Henderson K, Ainsworth B. Socioculturalperspectives on physical activity in the livesof older African American and AmericanIndian women: a cross cultural activityparticipation study. Women Health.2000;31(1):1–20.
63. Sternfeld B, Ainsworth B, Quesenberry C.Physical activity patterns in a diversepopulation or women. Prev Med.1999;28:313–323.
64. Tortolero S, Masse L, Fulton J, Torres I,Kohl H. Assessing physical activity amongminority women: focus group results.Womens Health Issues. 1999;9(3):135–142.
65. Eyler A. Personal, social andenvironmental correlates of physicalactivity in rural midwestern white women.Am J Prev Med. 2003;25(3Si):86–92.
66. Eyler A, Matson-Koffman D, Vest J, et al.Environmental, policy, and cultural factorsrelated to physical activity in a diversesample of women: the women’scardiovascular health network project:summary and discussion. Women Health.2002;36(2):123–134.
67. Kreuter M, McClure S. The role of culturein health communication. Ann ReviewPublic Health. 2004;25:439–455.
68. Segar M, Jayaratne T, Hanlon J,Richardson C. Fitting fitness into women’slives: effects of a gender-tailored physicalactivity intervention. Womens Health Issues.2002;12(6):338–347.
69. Thompson J, Wolfe V, Wilson N, PardillaM, Perez G. Personal, social, andenvironmental correlates of physicalactivity in Native American women.Am J Prev Med. 2003;25(3Si):53–60.
70. Halfon N, Hochstein M. Life course healthdevelopment: an integrated framework fordeveloping health, policy, and research.Milbank Q. 2002;80(3):433–478.
71. Marcus B, Forsyth L. Tailoringinterventions to promote physically activelifestyles in women. Womens Health Issues.1998;8(2):104–110.
72. Krummel D, Koffman D, Bronner Y, et al.Cardiovascular health interventions inwomen: what works? J Womens Health GendBased Med. 2001;10(2):117–136.
73. Shepard R. Whistler 2001: a HealthCanada/CDC conference oncommunicating physical activity andhealth messages—science into practice.Am J Prev Med. 2002;23(3):221–225.
74. US Department of Health and HumanServices. Making Health CommunicationsPrograms Work. Washington, DC: NationalCancer Institute, National Institutes ofHealth, Available at: http://www.nci.nih.gov/pinkbook. Accessed March 28, 2004.2004.
75. Cohen D, Scribner R, Farley T. Astructural model of health behaviors:a pragmatic approach to explain andinfluence health behaviors at thepopulation level. Prev Med. 2000;30:146–154.
76. Krenichyn K. Women and physical activityin an urban park: enrichment and supportthrough an ethic of care. J Environ Psychol.2004;24:117–130.
12 American Journal of Health Promotion
For individual use only. Duplication or distribution prohibited by law.

A fusion of the best of science and the best of practice —
together, to produce the greatest impact.
Stay on top of the science and art of health promotion withyour own subscription to the American Journal ofHealth Promotion.
“ The American Journal of Health Promotion provides a forum for that rare commodity— practical and intellectual exchange between researchers and practitioners. ”
Kenneth E. Warner, PhDAvedis Donabedian Distinguished University Professor of Public HealthSchool of Public Health, University of Michigan
“ The contents of the American Journal of Health Promotion are timely, relevant, andmost important, written and reviewed by the most respected researchers in our field. ”
David R. Anderson, PhDVice Programs and Technology, StayWell Health Management
Definition of Health Promotion“Health Promotion is the art and science of helping peoplediscover the synergies between their core passions and optimalhealth, enhancing their motivation to strive for optimal health,and supporting them in changing lifestyle to move toward a stateof optimal health. Optimal health is a dynamic balance ofphysical, emotional, social, spiritual and intellectual health.Lifestyle change can be facilitated through a combination oflearning experiences that enhance awareness, increase motivation,and build skills and most importantly, through creatingopportunities that open access to environments that make positivehealth practices the easiest choice.”
(O’Donnell, American Journal of Health Promotion, 2009, 24,1,iv)
DIMENSIONS OFOPTIMAL HEALTH
Subscribe today...ANNUAL SUBSCRIPTION RATES: (Availalble 1/1/10. Good through 12/31/10)
Individual Institution Institution InstitutionPrint & Online Print Only Online Only Print & Online
U.S. $139 $177 $359 $359
Canada and Mexico $148 $186 $359 $368
Other Countries $157 $195 $359 $377
CALL 800-783-9913 (U.S. ONLY) or 818-760-8520OR FIND US ON THE WEB AThttp://www.HealthPromotionJournal.com
Editor in ChiefMichael P. O’Donnell, PhD, MBA, MPHAssociate Editors in ChiefMargaret Schneider, PhDJennie Jacobs Kronenfeld, PhDShirley A. Musich, PhDKerry J. Redican, MPH, PhD, CHES
SECTION EDITORSInterventionsFitness
Barry A. Franklin, PhDMedical Self-Care
Donald M. Vickery, MDNutrition
Karen Glanz, PhD, MPHSmoking Control
Michael P. Eriksen, ScDWeight Control
Kelly D. Brownell, PhDStress Management
Cary Cooper, CBEMind-Body Health
Kenneth R. Pelletier, PhD, MD (hc)Social Health
Kenneth R. McLeroy, PhDSpiritual Health
Larry S. Chapman, MPH
StrategiesBehavior Change
James F. Prochaska, PhDCulture Change
Daniel Stokols, PhDHealth Policy
Kenneth E. Warner, PhDPopulation Health
David R. Anderson, PhD
ApplicationsUnderserved Populations
Ronald L. Braithwaite, PhDHealth Promoting Community Design
Bradley J. Cardinal, PhDThe Art of Health Promotion
Larry S. Chapman, MPH
ResearchData Base
Troy Adams, PhDFinancial Analysis
Ron Z. Goetzel, PhDFrom Evidence-Based Practice toPractice-Based Evidence
Lawrence W. Green, DrPHQualitative Research
Marjorie MacDonald, BN, PhDMeasurement Issues
Shawna L. Mercer, MSc, PhD
fOnline
subscriptionsnow available