lip reconstruction - pdfs.semanticscholar.org · this is not an all encompassing presentation of...
TRANSCRIPT

Lip
Reconstruction Steven Taylor, MD
Gregory Renner, MD
September 18, 2013
Overview
History
Anatomy
Causes for reconstruction
Reconstruction goals
Basic reconstructive options
Cases
References

This is not an all encompassing
presentation of repairs of lip
reconstruction.
Thank you Dr Renner for the procurement
of patient pictures and assistance in this
presentation.

History
Earliest known cheiloplasty was around
1000 BC, mentioned in the Indian sacred
texts of Susruta
http://en.wikipedia.org/wiki/File:Shushrut_statue.jpg

History
First mentioned repair in the Western
world was with Celsus in 25 AD.
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.
History
Louis- 1768
Wedge excision with direct closure of margins
von Burrow- 1838
Small triangles removed for flap advancement
Serre- 1842
First to describe repair of the oral commissure
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524. Upper left picture: http://www.lipreconstruction.com/history

History
Robert Abbe- 1898.
Lip switch flap
Actually described by Sabttini 60 yrs earlier
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524. Upper left picture: http://www.lipreconstruction.com/history

History
Jacob Estlander- 1872
Full thickness triangular flap for lateral
defect repair.
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524. Upper left picture: http://www.lipreconstruction.com/history

History
“We can say without exaggeration that
the basis of almost every reconstructive
procedure in use today was established in
the mid-1800’s.”
Ricardo Mazzola
Over 300 options for lip reconstruction
have been described
Mazzola RF, Lupo G. Evolving Concepts in Lip Reconstruction. Clin Plastic Surgery. 11:583-617, 1984.

Anatomy
3 main units Cutaneous
Vermillion
Mucosal
Left: Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524. Right: McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Anatomy Cutaneous
Upper lip Borders
Superior- Nasal sill and columella
Lateral- Nasolabial fold
Inferior- vermilion lip
3 cosmetic units: 2 lateral and 1 medial Lateral units are bordered by the nasolabial groove
laterally and by the philtral crests medially
Medial philtral subunit is composed of the 2 convex philtral crests and the central philtral groove
Cupid's bow - downward projection of the philtral unit
White roll - light linear projection that circumferentially outlines the upper and lower lip Border of the cutaneous and vermilion lip

Anatomy
Cutaneous
Lower lip
Borders
Superior- vermillion
Lateral- Extension of nasolabial folds
Inferior- Mental crease
One aesthetic unit
Left: http://emedicine.medscape.com/article/1127307-overview#showall

Anatomy
Upper: McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380. Lower: http://en.wikipedia.org/wiki/File:Mouth.jpg. Accessed 9/10/2013

Anatomy
Vermillion
Modified mucosal membrane that lacks
pilosebaceous units, eccrine glands, and
salivary glands
Extensive superficial vasculature in this area
gives the vermillion its pink red color
Anatomy
Mucosal lip
Abuts the teeth and contains minor salivary
glands
Red line
Transition zone between the vermilion lip
and the mucosal lip

Anatomy
Muscles
Orbicularis Oris
Primary lip muscle
No bone
attachment
Acts as a sphincter for oral closure
http://emedicine.medscape.com/article/1288447-overview#showall

Anatomy
Lip Elevators
Levator Labii
Superioris Alaeque
Nasi
Levator Labii
Superioris
Zygomaticus major
Zygomaticus minor
Levator anguli oris
http://emedicine.medscape.com/article/1288447-overview#showall

Anatomy Lid depressors
Depressor anguli oris
Depressor labii inferioris
Lip Protrusion
Mentalis
http://emedicine.medscape.com/article/1288447-overview#showall

Anatomy Sensory
CN V Upper lip- infraorbital
nerve Lower lip- Mental
nerve
Motor CN VII
Buccal branch- orbicularis oris and elevators
Marginal branch- Orbicularis oris and depressors
http://emedicine.medscape.com/article/1288447-overview#showall

Anatomy
Blood supply
Superior and
inferior labial
arteries
Branch of Facial
artery
Arteries found
between Orbicularis
oris and submucosa
http://emedicine.medscape.com/article/1288447-overview#showall

Anatomy
Lymphatics
Primarily submental
and submandibular
Ferris RL, Gillman GS. Cancer of the Lip. Expert Consult. Ch 24. Accessed from online source 9/11/2013.

Aesthetic Subunits
Left: http://emedicine.medscape.com/article/1127307-overview#showall Right: J Oral Maxillofac Surg 61:1207-1211, 2003, An overview of facial aesthetic units.

Causes for Reconstruction
Malignancy
SCC most common neoplasm of the lips
>80% lip cancers
Lower Lip>> Upper lip
SCC at commissure or upper lip considered
more aggressive
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Causes for Reconstruction Other malignancies
Basal Cell Carcinoma More common at Upper lip
Melanoma
Microcystic adnexal carcinoma Yellow plaques, paresthesisas (perineural inv)
Locally invasive with high recurrence rate
Merkel cell carcinoma Neural Crest cells
Rapid growth
High rate of recurrence and metastasis
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Causes for Reconstruction
Other etiologies
Granulomatous cheilitis
Infection
Hemangiomas
Trauma
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Functions of the lips
Appearance
Speech
Swallowing/Nutrition
Emotional expression
Tactile information
Whistling, Blowing, Kissing
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Goals of Reconstruction Adequate excision of the lesion
Restore function oral sphincter competency
Minimize microstomia Allows access for dental/medical procedures
Need for dentures
Preserve or restore expressive & sensory functions
Normalize appearance Minimize scarring
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Goals of Reconstruction
Thorough approximation of muscles
Reduce contracture and “notching”
Maintain lip height
Respect aesthetic subunits
Important to properly align the vermillion
and white roll
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Goals of Reconstruction
Scar camoflouage
Mental crease
Philtral ridge
Melolabial fold
Upper: McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.
Lower: http://en.wikipedia.org/wiki/File:Mouth.jpg. Accessed 9/10/2013
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Repair
Over 300 repairs have been described
When possible, use the axiom
“Use of lip to repair the lip defect”

Reconstruction Ladder
Image from http://www.jaaos.org/content/15/5/290/F4.expansion

Repair
3 layer closure (mucosa, muscle, skin)
Mucosa to wet line
Muscle
White roll
Vermillion
Skin

Repair
Vermillion defects
Defects less than 1/3 of either lip
Defects wider than 1/3 of lower lip
Defects wider than 1/3 of upper lip
Commissure defects
_______________________
Total lip defects
Defects beyond the lips
Repair
Vermillion defects
Defects less than 1/3 of either lip
Defects wider than 1/3 of lower lip
Defects wider than 1/3 of upper lip
Commissure defects
_______________________
Total lip defects
Defects beyond the lips

Repair
Muscle Sparing
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Labial Mucosal Advancement Flap
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.
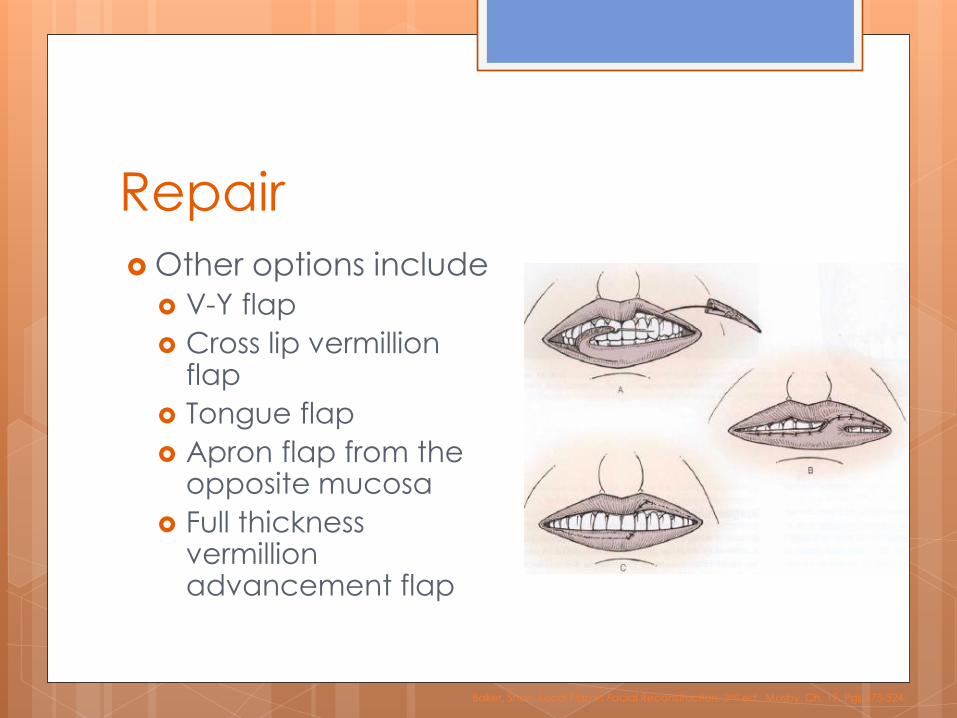
Repair
Other options include
V-Y flap
Cross lip vermillion flap
Tongue flap
Apron flap from the opposite mucosa
Full thickness vermillion advancement flap
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.
Repair
Vermillion defects
Defects less than 1/3 of either lip
Defects wider than 1/3 of lower lip
Defects wider than 1/3 of upper lip
Commissure defects
_______________________
Total lip defects
Defects beyond the lips

Repair
Defects less than 1/3 of either lip
Primary Closure
Wedge Excision (V- lip)
W-plasty
Bilateral Advancement flap

Photos courtesy of Gregory Renner, MD

V – Lip Repair
Photos courtesy of Gregory Renner, MD

W – Lip Repair
Photos courtesy of Gregory Renner, MD

W – Lip Repair
Photos courtesy of Gregory Renner, MD
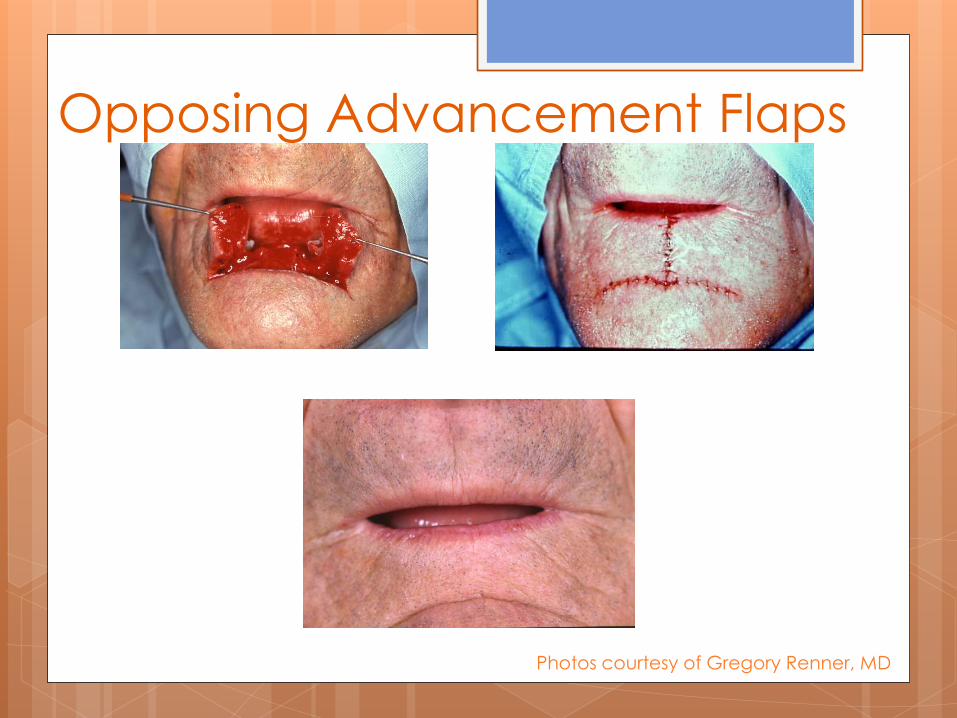
Opposing Advancement Flaps
Photos courtesy of Gregory Renner, MD

Repair Primary Closure
Able to use for about defects <3cm stretched lip length
Potential Complications Microstomia
Accomodation for dentures needs to be considered
Sensory deficit May lead to problems with competence
Too much wound tension

Repair
Vermillion defects
Defects less than 1/3 of either lip
Defects wider than 1/3 of lower lip
Defects wider than 1/3 of upper lip
Commissure defects
_______________________
Total lip defects
Defects beyond the lips

Repair
Defects wider than 1/3 of lower lip
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Abbe flap (Sabattini)
Medial lesions
Pedicled off the labial artery
Flap smaller than defect
Division of pedicle after ~3 weeks

Abbe Flap
Photos courtesy of Gregory Renner, MD
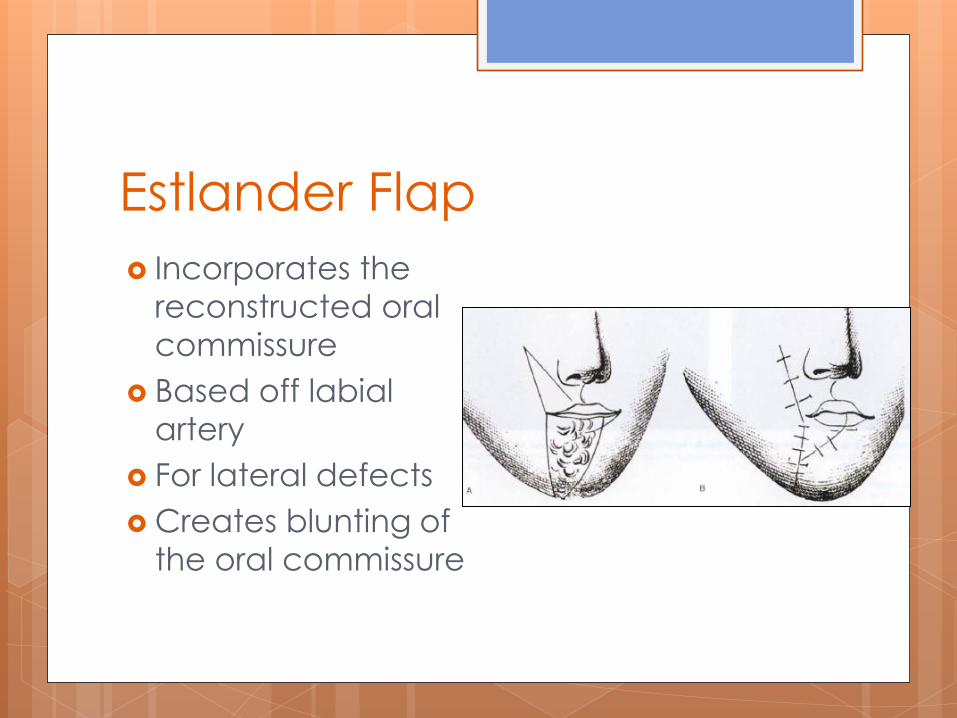
Estlander Flap
Incorporates the
reconstructed oral
commissure
Based off labial
artery
For lateral defects
Creates blunting of
the oral commissure
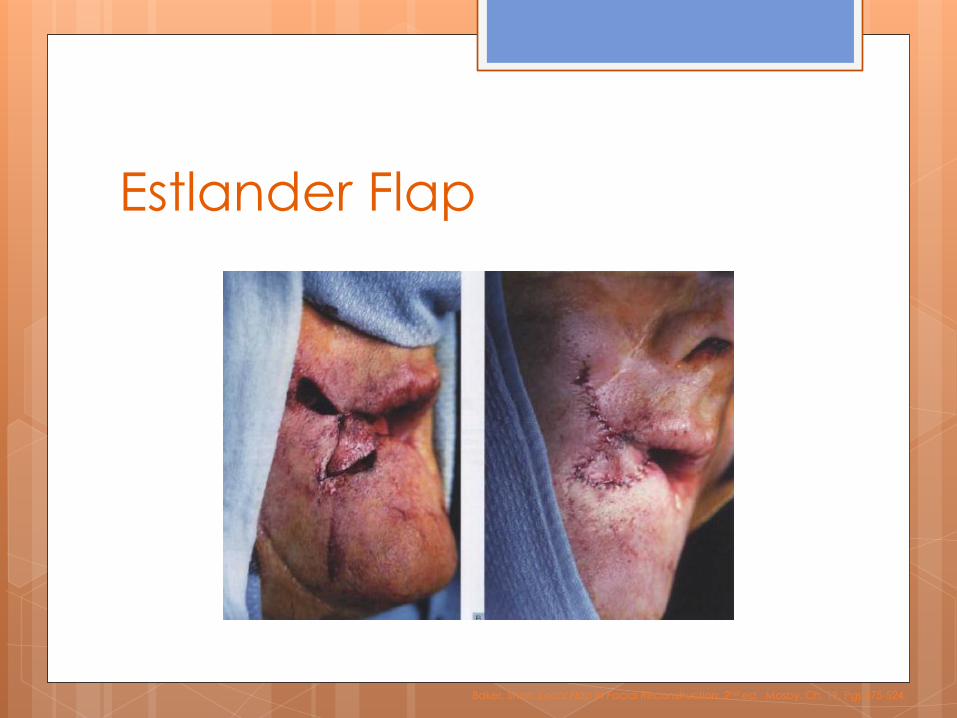
Estlander Flap
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.

Karapandzic Flap
Preserves neurovascular bundle
Incisions made are not full thickness
Defects up to 2/3 lip length
May lead to microstomia
Can blunt the oral commissure
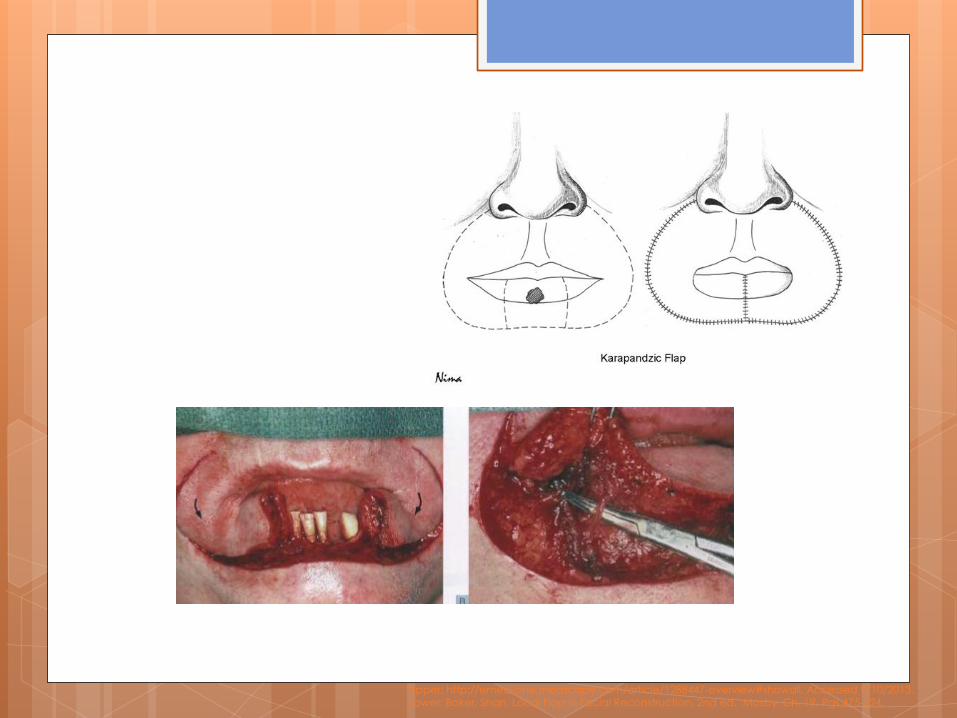
Upper: http://emedicine.medscape.com/article/1288447-overview#showall. Accessed 9/10/2013. Lower: Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.

Karapandzic Flap
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.
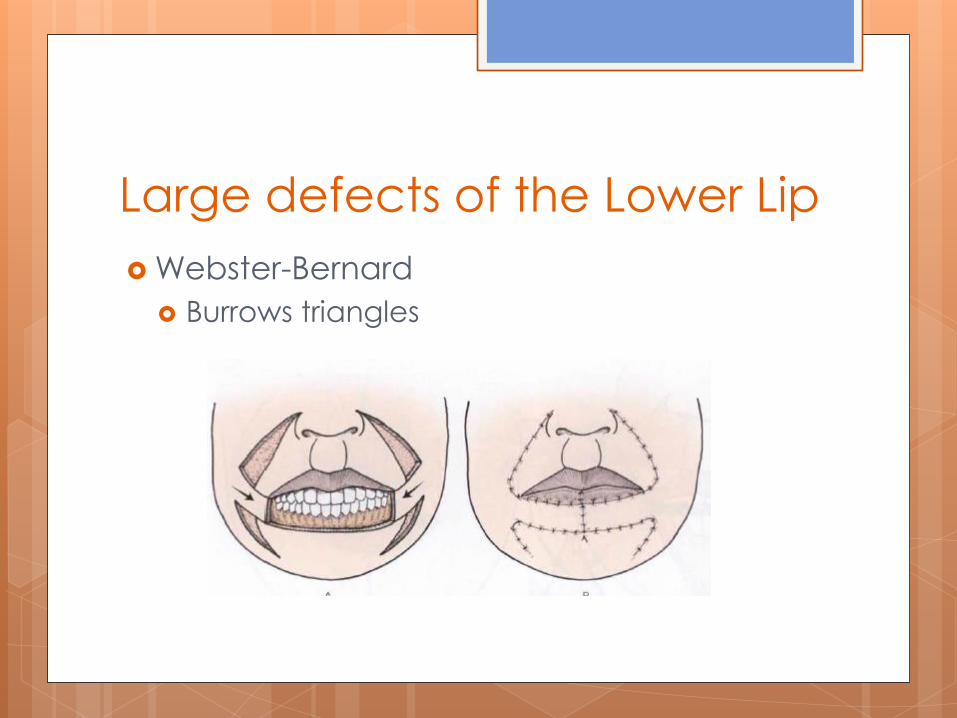
Large defects of the Lower Lip
Webster-Bernard
Burrows triangles

Lower Lip
Melolabial flap
Photos courtesy of Gregory Renner, MD

Repair
Vermillion defects
Defects less than 1/3 of either lip
Defects wider than 1/3 of lower lip
Defects wider than 1/3 of upper lip
Commissure defects
_______________________
Total lip defects
Defects beyond the lips

Upper Lip
May use Cross lip flaps
Estlander
Abbe flap
Melolabial flaps
Temporoparietal Flap

Melolabial Flap
Photos courtesy of Gregory Renner, MD

Upper Lip
Temporoparietal Flap
No muscle, but gravity aids in competence
Anticipate contraction and make the flap
slightly larger.
May use skin graft underneath the flap to
recreate the oral mucosa.
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.

Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.

Repair
Vermillion defects
Defects less than 1/3 of either lip
Defects wider than 1/3 of lower lip
Defects wider than 1/3 of upper lip
Commissure defects
_______________________
Total lip defects
Defects beyond the lips

Commissure defects
Difficult to recreate
Estlander
Karapandzic
Zisser Flap
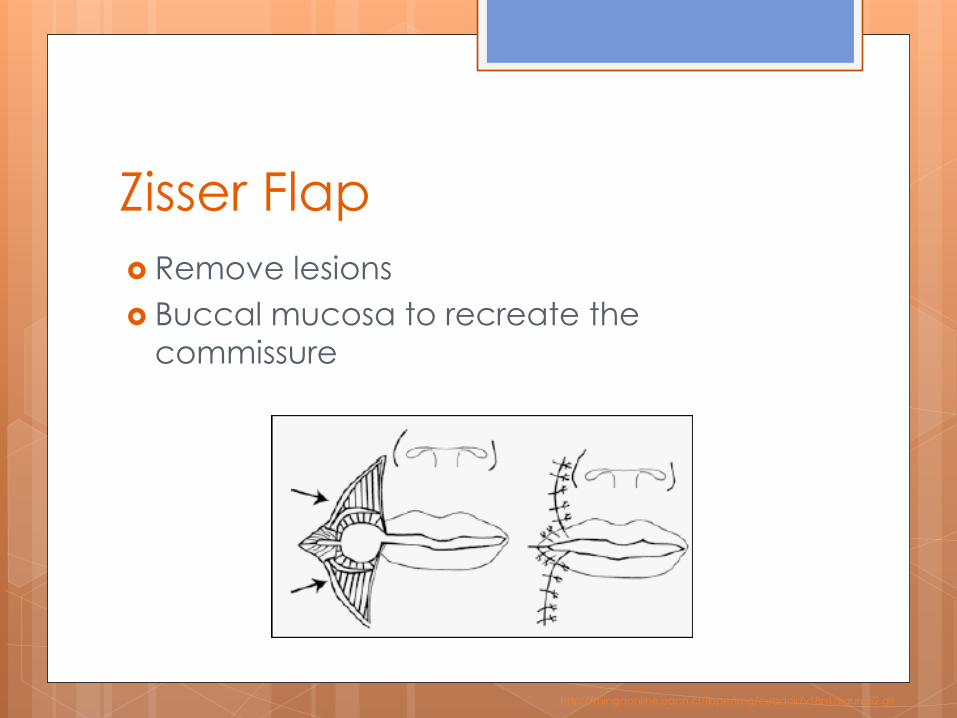
Zisser Flap
Remove lesions
Buccal mucosa to recreate the
commissure
http://mingaonline.uach.cl/fbpe/img/cuadcir/v18n1/figura52.gif

Cases

Case #1
Recurrent SCC invading lower lip
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.
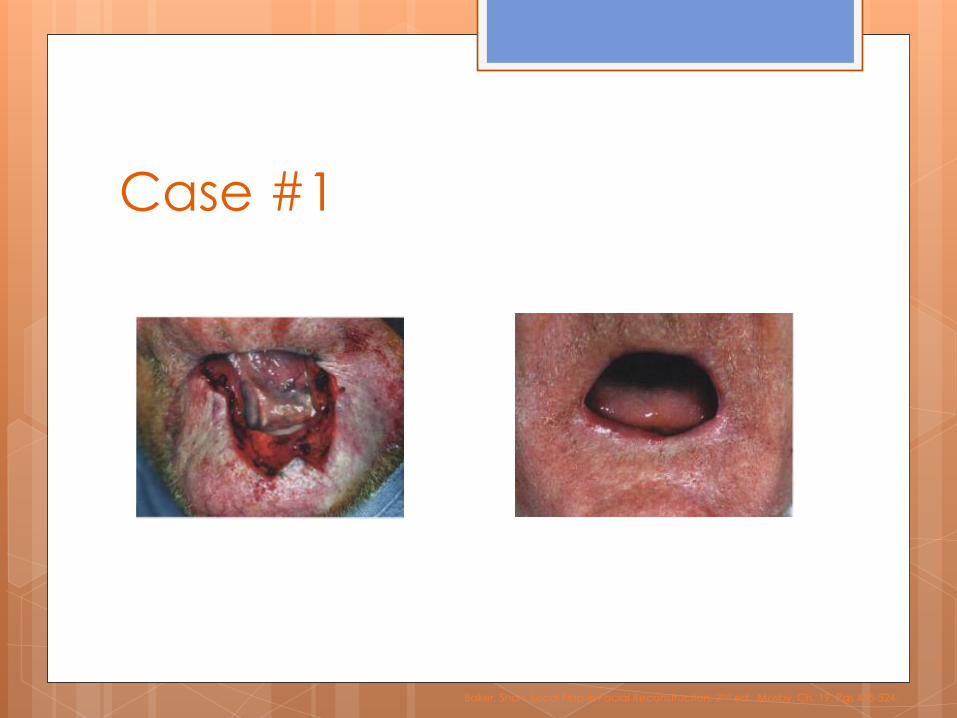
Case #1
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.

Case #2
Closmann JJ, et al. Reconstruction of Perioral Defects Following Resection for Oral Squamous Cell Carcinoma. J Oral Maxillofac Surg 64:367-374, 2006.

Closmann JJ, et al. Reconstruction of Perioral Defects Following Resection for Oral Squamous Cell Carcinoma. J Oral Maxillofac Surg 64:367-374, 2006.
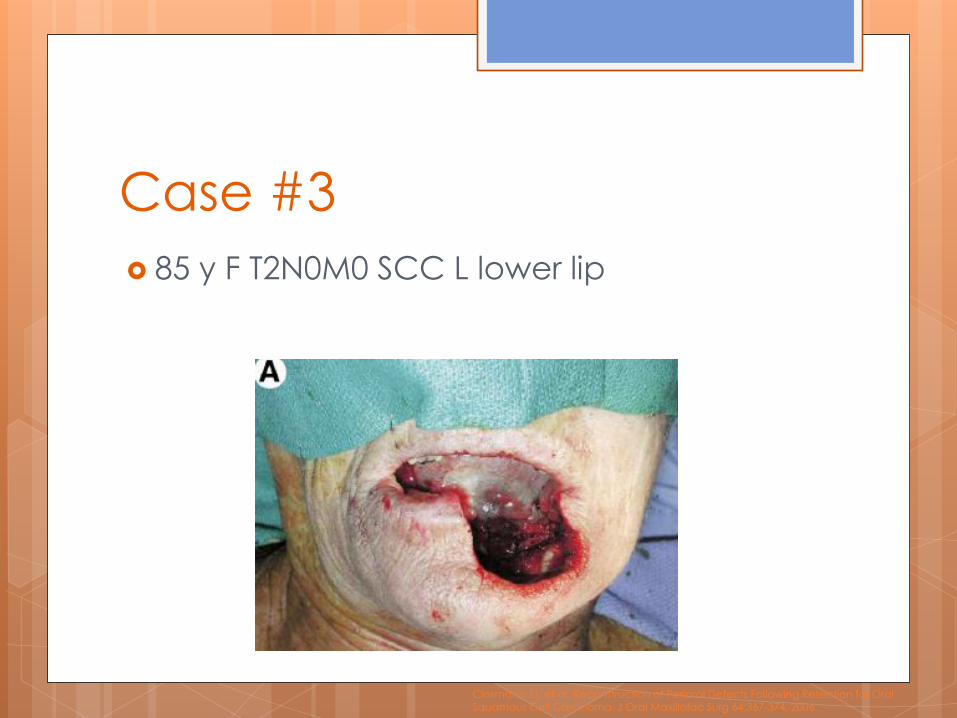
Case #3
85 y F T2N0M0 SCC L lower lip
Closmann JJ, et al. Reconstruction of Perioral Defects Following Resection for Oral Squamous Cell Carcinoma. J Oral Maxillofac Surg 64:367-374, 2006.

Closmann JJ, et al. Reconstruction of Perioral Defects Following Resection for Oral Squamous Cell Carcinoma. J Oral Maxillofac Surg 64:367-374, 2006.

Case #4
2 cm defect of upper lip
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.

Conclusions
There are multiple techniques for
managing lip reconstruction.
Abbe, Estlander and primary closure are
most common.
As much as possible, use lip to repair lip.
References Mona Lisa picture from
http://en.wikipedia.org/wiki/File:Mona_Lisa.jpg. Accessed 9/11/2013.
www.Lipreconstruction.com
http://www.slideshare.net/ronaldagador/lip-reconstruction
Baker, Shan. Local Flap in Facial Reconstruction. 2nd ed. Mosby. Ch. 19. Pgs 475-524.
Mazzola RF, Lupo G. Evolving Concepts in Lip Reconstruction. Clin Plastic Surgery. 11:583-617, 1984.
McCarn KE, Park SS. Lip Reconstruction. Otolaryngol Clin N Am. 40 (2007) 361–380.
http://emedicine.medscape.com/article/1288447-overview#showall. Accessed 9/10/2013.
Closmann JJ, et al. Reconstruction of Perioral Defects Following Resection for Oral Squamous Cell Carcinoma. J Oral Maxillofac Surg 64:367-374, 2006.