linfoma de hodgkin - sbtmosbtmo.org.br/userfiles/fck/file/aulas_i encontro sbtmo - 2017/aula... ·...
TRANSCRIPT

Linfoma de Hodgkin
Novos medicamentos
Otavio BaiocchiCRM-SP 96.074

Hodgkin Lymphoma
• Unique B-cell lymphoma
• HRS malignant cells
• Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a
background of reactive T-cells infiltrate,.

HRS cells interaction with microenvironment
Aldinucci et al. J Pathol 2010 Jul;221(3):248-63

Hodgkin lymphoma: treatment modalities

Hodgkin lymphoma: treatment modalities

Hodgkin Lymphoma: Depletion of malignant cells
• Chemotherapy and Radiotherapy approach
• Autologous stem-cell transplant
• Antibody-drug conjugate: Brentuximab vedotin
ABVD BEACOPP

Hodgkin Lymphoma: Depletion of malignant cells
• Chemotherapy and Radiotherapy approach
• Autologous stem-cell transplant
• Antibody-drug conjugate: Brentuximab vedotin
ABVDBEACOPP

Hodgkin Lymphoma - treatment
Early favorable
Early
unfavorableAdvanced stages

Current guidelines for HL treatment
Treatment
setting
NCCN guidelines, 2016
Treatment
ESMO guidelines, 2014
Treatment
Frontline
• ABVD + IFRT
• Stanford V
• BEACOPP
• BEACOPP followed by ABVD + RT
• ABVD alone
• Individualized treatment may be necessary for older patients and
patients with concomitant disease (2A)
• ABVD or BEACOPP ± RT (I–II,A)
Second-line • Salvage chemotherapy + ASCT • Salvage chemotherapy + ASCT
Third line therapy
• Brentuximab vedotin
• Allo SCT
• No data to support superior outcomes with any treatment;
individualized therapy recommended
• Clinical trial may be appropriate
• Brentuximab vedotin
• Allo SCT
• No data to support superior outcomes with any
treatment; individualized therapy recommended
• Clinical trial may be appropriate

Current guidelines for HL treatment
Treatment
setting
NCCN guidelines, 2016
Treatment
ESMO guidelines, 2014
Treatment
Frontline
• ABVD + IFRT
• Stanford V
• BEACOPP
• BEACOPP followed by ABVD + RT
• ABVD alone
• Individualized treatment may be necessary for older
patients and patients with concomitant disease (2A)
• ABVD or BEACOPP ± RT (I–II,A)
Second-line• Radiotherapy or second-line chemotherapy ± radiotherapy
followed by high-dose chemotherapy + ASCT/allo-SCT
• Salvage chemotherapy + ASCT
• BEACOPP escalated or salvage radiotherapy alone
Third line therapy
• Brentuximab vedotin
• Allo SCT
• No data to support superior outcomes with any treatment;
individualized therapy recommended
• Clinical trial may be appropriate
• Brentuximab vedotin
• Allo SCT
• No data to support superior outcomes with any
treatment; individualized therapy recommended
• Clinical trial may be appropriate

Current guidelines for HL treatment
Treatment
setting
NCCN guidelines, 2016
Treatment
ESMO guidelines, 2014
Treatment
Frontline
• ABVD + IFRT
• Stanford V
• BEACOPP
• BEACOPP followed by ABVD + RT
• ABVD alone
• Individualized treatment may be necessary for older patients and
patients with concomitant disease (2A)
• ABVD or BEACOPP ± RT (I–II,A)
Second-line • Salvage chemotherapy + ASCT • Salvage chemotherapy + ASCT
Third line therapy
• Brentuximab vedotin
• Allo SCT
• No data to support superior outcomes with any treatment;
individualized therapy recommended
• Clinical trial may be appropriate
• Brentuximab vedotin
• Allo SCT
• No data to support superior outcomes with any
treatment; individualized therapy recommended
• Clinical trial may be appropriate

After 1 month
Tb treatment
Bx: Tuberculosis
Pcte sexo feminino, 34 anos
Stage: IVB After C6 ABVD
PET +
Refractory HL?
Interin PET
After C2 ABVD
PET +
Partial Response
34 y/o white female with fever, night sweats and a newly diagnosed advanced stage HL
After C4 ABVD
PET +
Why a biopsy is mandatory?

2nd line therapy for cHLrelapsed refractory disease
• High dose chemotherapy followed ASCT
• Which salvage chemotherapy?
• How to increase CR rate before ASCT?
• How to improve prognosis in high risk patients after ASCT?

2nd line therapy for cHLrelapsed refractory disease
• High dose chemotherapy followed ASCT
• Which salvage chemotherapy?
• How to increase CR rate before ASCT?
• How to improve prognosis in high risk patients?

2nd line therapy for cHLrelapsed refractory disease
• High dose chemotherapy followed ASCT
Salvage chemotherapy - UNIFESP
1. ICE Moskowitz et al. (2001)
2. DHAP Josting et al. (2005)
3. IGEV Santoro et al. (2007)
4. GDP Bartlett et al. (2007)
Do not delay cycles – DHAP14, ICE15 have shown the best
results
CR rate ICE, DHAP, IGEV, GDP - 45 – 60%

Response to salvage therapy predicts post-ASCT
survival
17% in patients with resistant disease (p<0.0001)1
1. Sirohi B et al. Ann Oncol 2008;19:1312–9; 2. Majhail N et al. Biol Blood Marrow Transplant 2006;12:1065–72;;
100
80
60
40
20
0 5 10 15 20
n
Complete response 53
Partial response 96
Resistant 46
Pro
ba
bili
ty o
f O
S (
%)
Time since transplant (years)
Survival correlates with depth of response prior to ASCT1
5-year OS: 79% for patients in CR pre-ASCT
59% in patients with PR
Complete remission is good, but not a pre-requisite!

2nd line therapy for cHLrelapsed refractory disease
• High dose chemotherapy followed ASCT
• Which salvage chemotherapy?
• How to increase CR rate before ASCT?
• How to improve prognosis in high risk patients?
The role of Brentuximab vedotin

BV-bendamustine
Brentuximab vedotin 1.8 mg/kg D1 with bendamustine 90 mg/m2 on
D1-2 q3w for 3 cycles
ORR 92%
76 patients, 80% CR30% used plerixafor
LaCasce, et al. ASH 2016
Brentuximab Vedotin Plus ESHAP (BRESHAP)
GELTAMO
ORR 94%
39 patients, 85% CR
Garcia-Sans, et al. EBMT 2016 (poster)
Use brentuximab vedotin (BV) with salvage chemotherapy
CR rate ICE, DHAP, IGEV, GDP - 45 – 60%
Is it possible to increase CR rate without increasing
toxicity? The role of BV in savage therapy

Brentuximab monotherapy
60 patients
ORR 88%
CR 65% Excellent stem-cell harvest
Chen et al, EBMT 2016 (poster)
B-ICE – ASH 2017 preliminary results
B-DHAP – ISHL 2016 – preliminary results CR 85%
Is it possible to increase CR rate without increasing
toxicity? The role of BV in savage therapy
Hagenbeck et al, Oral ISHL 2016

2nd line therapy for cHLrelapsed refractory disease
• High dose chemotherapy followed ASCT
• Which salvage chemotherapy?
• How to increase CR rate before ASCT?
• How to improve prognosis in high risk patients after ASCT?

AETHERA phase III trial of brentuximab vedotin vs placebo in
relapsed or refractory HL pts at risk of relapse post ASCT
Dose and schedule: Pts were randomized 1:1 to receive 16 21-day cycles of
brentuximab vedotin 1.8 mg/kg IV day 1 or placebo
• Pts who progressed on placebo could receive brentuximab vedotin
Moskowitz C et al. Lancet Oncology 2016
HL, Hodgkin lymphoma; PFS, progression free survival; IRF, independent review facility; OS,
overall survival; mos, months; CR, complete response; PR, partial response; SD, stable disease;
PD, progressive disease; ASCT, autologous stem cell transplantation; BV, brentuximab vedotin;
pts, patients ; R/R, relapsed refractory

AETHERA phase III trial of brentuximab vedotin vs placebo in
relapsed or refractory HL pts at risk of relapse post ASCT
PFS outcome
Brentuximab
vedotin (n=165)
Placebo
(n=164)
Median PFS NR 16 mos
HR (95% CI) 0.50 (0.36, 0.70)
p-value NR
2-year PFS 65% 45%
Moskowitz C et al. Lancet Oncology 2016
Moskowitz C et al. Lancet Oncology 2016

• Consolidation after ASCT with brentuximab vedotin (BV)
demonstrated improved PFS in patients with HL and risk factors for
relapse or disease progression (HR = 0.57, p = 0.001)
• PFS benefit was sustained after 3 years f/u (EHA 2016)
• Consistent benefit observed across subgroups
• Analysis of overall survival did not show a significant difference
between treatment arms.
AETHERA phase III trial of brentuximab vedotin vs placebo in
relapsed or refractory HL pts at risk of relapse post ASCT
Moskowitz C et al. Lancet Oncology 2016

3rd line therapy for cHLrelapsed after ASCT

Current guidelines for HL treatment
Treatment
setting
NCCN guidelines, 2016
Treatment
ESMO guidelines, 2014
Treatment
Frontline
• ABVD + IFRT
• Stanford V
• BEACOPP
• BEACOPP followed by ABVD + RT
• ABVD alone
• Individualized treatment may be necessary for older patients and
patients with concomitant disease (2A)
• ABVD or BEACOPP ± RT (I–II,A)
Second-line• Radiotherapy or second-line chemotherapy ± radiotherapy
followed by high-dose chemotherapy + ASCT/allo-SCT
• Salvage chemotherapy + ASCT
• BEACOPP escalated or salvage radiotherapy alone
Third line
therapy
• Brentuximab vedotin• Allo SCT
• Clinical trial may be appropriate
• Brentuximab vedotin• Allo SCT
• Clinical trial may be appropriate

Five-year survival and durability results of brentuximab vedotin in
patients with relapsed or refractory Hodgkin lymphomaChen et al, Blood 2016
• Single agent brentuximab vedotin can induce durable remissions
• 5-year overall survival rate was 41% and 70% for those who achieved CR

Current guidelines for HL treatment
Treatment
setting
NCCN guidelines, 2016
Treatment
ESMO guidelines, 2014
Treatment
Frontline
• ABVD + IFRT
• Stanford V
• BEACOPP
• BEACOPP followed by ABVD + RT
• ABVD alone
• Individualized treatment may be necessary for older patients and
patients with concomitant disease (2A)
• ABVD or BEACOPP ± RT (I–II,A)
Second-line• Radiotherapy or second-line chemotherapy ± radiotherapy
followed by high-dose chemotherapy + ASCT/allo-SCT
• Salvage chemotherapy + ASCT
• BEACOPP escalated or salvage radiotherapy alone
Third line
therapy
• Brentuximab vedotin
• Allo SCT• Clinical trial may be appropriate
• Brentuximab vedotin
• Allo SCT• Clinical trial may be appropriate

Hodgkin lymphoma: treatment modalities

29
New medications: Cancer immunotherapy

WHEN A T-LYMPHOCYTE MEETS AN ANTIGEN…
CD4 LymphocyteAPC
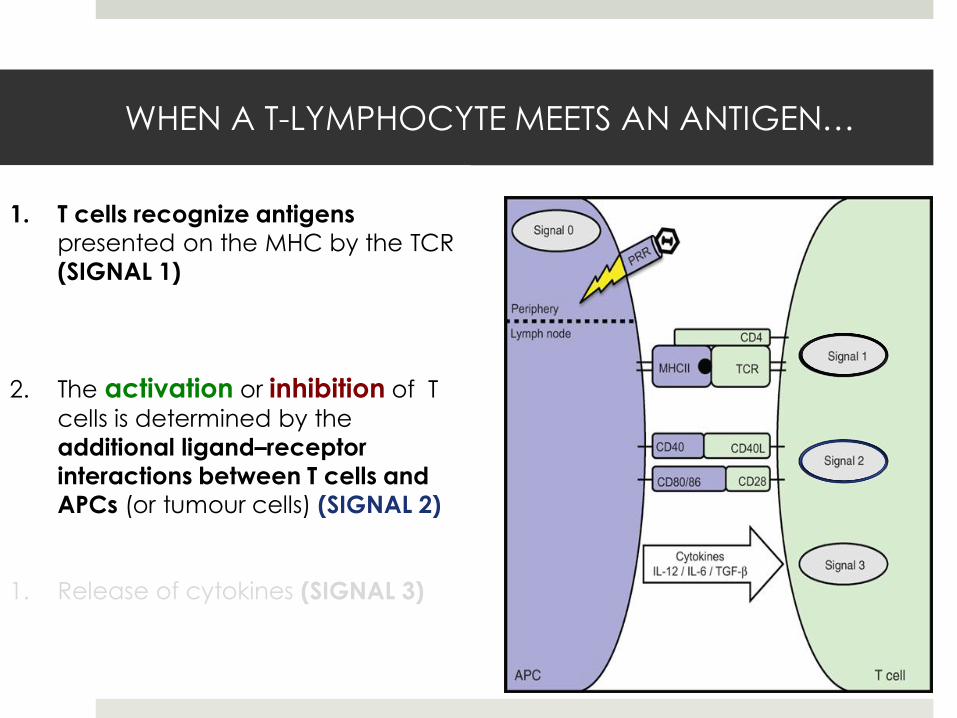
1. T cells recognize antigens
presented on the MHC by the TCR
(SIGNAL 1)
WHEN A T-LYMPHOCYTE MEETS AN ANTIGEN…
1. T cells recognize antigens
presented on the MHC by the TCR
(SIGNAL 1)
2. The activation or inhibition of T
cells is determined by the
additional ligand–receptor
interactions between T cells and
APCs (or tumour cells) (SIGNAL 2)
1. Release of cytokines (SIGNAL 3)
CD4 LymphocyteAPC

WHEN A T-LYMPHOCYTE MEETS AN ANTIGEN…
1. T cells recognize antigens
presented on the MHC by the TCR
(SIGNAL 1)
2. The activation or inhibition of T
cells is determined by the
additional ligand–receptor
interactions between T cells and
APCs (or tumour cells) (SIGNAL 2)
1. Release of cytokines (SIGNAL 3)
CD4 LymphocyteAPC

Hodgkin Lymphoma: Immune activation
• Allogeneic SCT
• Immune checkpoint inhibitors (inhibitory effect)
• Immune checkpoint activators (activation effect)

34
Activating or inhibitory receptors

Hodgkin Lymphoma: Immune activation
• Immune checkpoint inhibitors (inhibitory effect)
• Immune checkpoint activators (activation effect)

Immune checkpoints in HL
Teach your body to fight tumor
Haematologica cover July 2016

37
Inhibitory receptors

• Regulatory T-cells surround HRS cells(Assis et al, Med Oncol, 2012)
• EBV increases Tregs in tumor
microenvironment(Assis et al, Leukemia & Lymphoma, 2014)
• Increased Tregs in peripheral blood
of patients with cHL at diagnosis.(Silva et al, Clin Leuk, Lymph and Myel, 2015)
Regulatory T-cells in Hodgkin Lymphoma

• Regulatory T-cells downregulate anti-tumor immune response
Regulatory T-cells in Hodgkin Lymphoma

CTLA-4 Inhibitors: Ipililumabmechanism of action

41
Activating or inhibitory receptors

PD-1 Inhibitors in Hodgkin Lymphoma:Pembrolizumab and nivolumab

PD-1 Inhibitors in Hodgkin Lymphoma:Pembrolizumab and nivolumab

Results of PD1 Blocking Antibodies in
Relapsed HL (all pts received BV)
Drug Dose/Schedule
N % ORR % CR ORR in BV treated HL
1st Author
Pembrolizumab(humanized IgG4)
10 mg/kg IV Q 2wks
15 53% 20% 53% (n=15) Moskowitz C
Nivolumab(Fully human IgG4)
3 mg/kg IV Q 2wks
23 87% 17% 89% (n=18) Armand P
Phase 2 trials on going

45
Preliminary Safety and Efficacy of the Combination of Brentuximab Vedotin
and Ipilimumab in Relapsed / Refractory Hodgkin Lymphoma: A Trial of the ECOG-ACRIN Cancer Research Group (E4412)
Stephen Ansell et al, Poster, ASH 2016
• E4412 is a phase 1 study of the combination of BV and the checkpoint
inhibitors ipilimumab (anti-CTLA-4) (IPI) and nivolumab (NIVO)
• 23 patients have been treated with BV + IPI (first cohort)
• BV + IPI was well tolerated
• Overall response BV + IPI was 87% with a CR rate of 62%
• Optimization of this combination strategy is planned with ongoing accrual
to cohorts receiving BV + NIVO and BV + IPI + NIVO.

PD1 Blocking Antibodies:
potential serious side effects

PD1 Blocking Antibodies:
potential serious side effects
• Fulminant type 1 diabetes mellitus with Nivolumab
• Fatal GVHD following Pembrolizumab
• AIHA after nivolumab treatment
• Vitiligo induced by nivolumab
• Myasthenia gravis induced by nivolumab
J Diabetes, 2016
Bone Marrow Transplant. 2016
Oncotarget, 2016
Cancer reviews, 2016
JAMA Oncol, 2016

Single agent activity of novel agents in relapsed
cHL: update 2016
0
25
50
75
100
CR
PR

BrentuximabVedo nn
HDACi
PI3Ki/mTORi
Chemotherapy
PD1/PDL1an bodies
BrentuximabVedo nn
HDACi
PI3Ki/mTORi
Chemotherapy
PD1/PDL1an body
+
Strategy A Strategy B
Courtesy: Prof. Anas Younes
Current and Future Treatment Paradigms
of Hodgkin Lymphoma


Current and Future Treatment Paradigms of
Hodgkin Lymphoma
ABVD
Platinum-based salvage
Gemcitabine-based salvage
ASCT
No response/relapse
And/or
No response/relapse
?
2002 - 2012 ABVD
Platinum-based salvage
Gemcitabine-based salvage
ASCT
No response/relapse
And/or
No response/relapse
BrentuximabAlloSCT
2012 - 2016 ?
?
?
?
No response/relapse
No response/relapse
2020
?
And/or