leveraging health systems strengthening for prevention...
TRANSCRIPT

Leveraging Health Systems
Strengthening for Prevention
and Control of NCD in India:

Vision of the National Health
Mission….
“Attainment of Universal Access to Equitable, Affordable and Quality health
care services, accountable and responsive to people’s needs, with effective inter-
sectoral convergent action to address the wider social determinants of health”.

Key Features Strengthening public health infrastructure
Focus on primary health care
Expanding access and coverage: poor and vulnerable; urban underserved.
Strengthening community based health care services –
ASHA (Community Health Volunteer),
outreach and facility based services
addressing social and environmental determinants
Augmenting HR: capacity and capability, facilitated by innovations in selection, support and payments

Key Features –contd.
Nationwide network of ambulances,
Improved quality of care:
Expanding access to free drugs,diagnostics,
HMIS for planning and monitoring,
Improved governance
Effective public-private partnerships with a focus on equity

91
126
43 49
0
20
40
60
80
100
120
140
2011-13 2011-
13
1990 1990
GLOBAL INDIA
India’s Progress on MDG 4 – Under 5 Mortality Rate
53%
decline
61%
decline
U5MR in India declined 15 % faster than
the global U5MR
• In 1990, India carried a 40 %
higher burden of child mortality
compared to the global average
• Rate of decline more than
doubled from 3.3% in 1990-
2008 to 6.6 % in 2008-2013
• Decline equal to or better than
the national average in states
with low indicators at baseline
Source: Global – MMEIG Estimates, India MMEIG Estimates & SRS 2011-13

385
556
216 167
0
100
200
300
400
500
600
1990 2011-
13
1990 2011-
13
GLOBAL INDIA
India’s Progress on MDG 5 – Maternal Mortality Ratio
MMR in India declined 59 % faster than
the global MMR
44%
decline
70%
decline
• In 1990, India carried a 47 % higher
burden of maternal mortality compared to
the global average
• MMR declined at an accelerated pace &
reached a figure lower than the global
average
• Projected to reach MDG 140/ 100,000 live
births
Source: Global – MMEIG Estimates, India MMEIG Estimates & SRS 2011-13

• TFR reduced from 2.9 (2005) to 2.3 (2013)
• 61% acceleration in average annual rate of
decline
• 24 States/UTs achieved replacement level of
less than 2.1
Infant Mortality Rate (IMR) Total Fertility Rate (TFR)
• IMR reduced from 58 (2005) to 40
(2013)
• Average annual rate of decline more
than doubled post National Rural
Health Mission
Reduction Rates
Decline
2.1%
Decline
4.5%
Decline
2.9% Decline
1.8%

Malaria MDG 6 to halt and begin to reverse the incidence of Malaria by 2015
achieved
44.4% reduction in mortality and 38% reduction in incidence of
Malaria in 2015 as against 2005.
Tuberculosis Prevalence, Incidence and Mortality due to TB significantly reduced.
MDG Goal achieved.
88% Cure rate.
Leprosy
Prevalence
Reduced from 1.3 per 10000 in 2005 to 0.74 per 10000 population
Disease Control Programmes

2004-05 2014
1162 872
4137
8128
Public Private
•Increase in childbirths in public health
facilities by 131.63% compared to 2004
•Reduction in average medical expenditure
in public health facilities, costs about 1/10th of
private sector costs
•Private sector has a larger share in health care
delivery, but over 80% of preventive and
promotive care by public health system
Findings from NSSO – 71st Round (Jan-June, 2014)
Average medical expenditure in Child
Birth in Rural areas
70
%
30
%
Rural Areas
Public
Private
47
%
53
%
Urban Areas
Institutional Deliveries

Moving from Selective
to Comprehensive
Primary Health Care
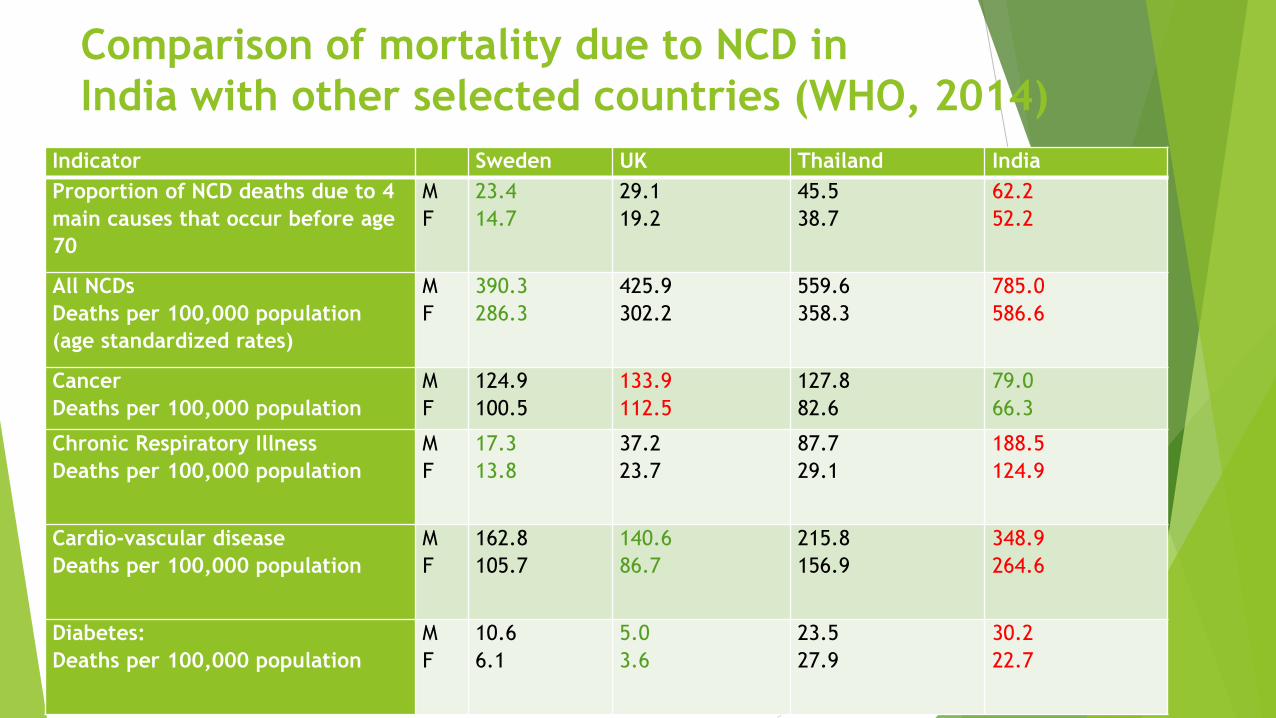
Comparison of mortality due to NCD in
India with other selected countries (WHO, 2014)
Indicator Sweden UK Thailand India
Proportion of NCD deaths due to 4
main causes that occur before age
70
M
F
23.4
14.7
29.1
19.2
45.5
38.7
62.2
52.2
All NCDs
Deaths per 100,000 population
(age standardized rates)
M
F
390.3
286.3
425.9
302.2
559.6
358.3
785.0
586.6
Cancer
Deaths per 100,000 population
M
F
124.9
100.5
133.9
112.5
127.8
82.6
79.0
66.3
Chronic Respiratory Illness
Deaths per 100,000 population
M
F
17.3
13.8
37.2
23.7
87.7
29.1
188.5
124.9
Cardio-vascular disease
Deaths per 100,000 population
M
F
162.8
105.7
140.6
86.7
215.8
156.9
348.9
264.6
Diabetes:
Deaths per 100,000 population
M
F
10.6
6.1
5.0
3.6
23.5
27.9
30.2
22.7

Rationale
NSSO data (71st Round. 2014) : Only 11.5% and about 4% in rural and
urban areas respectively sought any form of OP care - at or below the
CHC (except for Childbirth)
Sub centre and Primary Health centre- currently provide largely
preventive care related to maternal and child health
Epidemiologic Transition: Death from the four major NCDs for nearly
60% of all mortality
The sequelae of NCD impose a high fiscal cost – need to focus on
primary and secondary prevention.
Lack of Primary Health Care close to communities, increases the burden
on secondary and tertiary facilities; consequences on quality of care

Reorganizing work processes
Family/Household and Community Level: by community level workers- ASHA,
Anganwadi Workers, community volunteers, school teachers, etc. with active support of
VHSNC.
Health and Wellness Centres - one per 5000 population - Existing sub centres to be
converted to Health and Wellness Centers (HWC) – with a Primary Health Care Team- led
by a trained mid level health care providers (MLP) (Community Health Officer- a BSc.
Community Health or a Nurse Practitioner (NP) or an Ayurvedic doctor)
Other team members : all ASHAs and AWW in the villages in sub centre area, an ANM
and an MPW (Male) or two ANMs
First Referral Level - Referral support includes general medical and specialist
consultation as relevant and the first level of hospitalization at FRU

Comprehensive Primary Health Care- Package of Services
1. Care in pregnancy and child-birth. (the latter would be provided in specific facilities based on state
context).
2. Neonatal and infant health care services
3. Childhood and adolescent health care services.
4. Family planning, Contraceptive services and Other Reproductive Health Care services
5. Management of Communicable diseases: National Health Programmes
6. Management of Common Communicable Diseases and General Out-patient care for acute simple
illnesses and minor ailments
7. Screening and Management of Non-Communicable diseases
8. Screening and Basic management of Mental health ailments
9. Care for Common Ophthalmic and ENT problems
10. Basic Dental health care
11. Geriatric and palliative health care services
12. Trauma Care (that can be managed at this level) and Emergency Medical services

Leveraging NHM led Health System Strengthening
Systems for registration, tracking and follow up of target/high risk groups for MNCH and FP,
Expanding workforce- particularly frontline workers
ASHA – to expand outreach, promote mobilization and provide home care, including counselling
Mechanisms for Referral and transport established for MNCH
Free Drugs Service Initiative/Free Diagnostics Service Initiative - strengthening of attendant components- Procurement and Logistics, Standard Treatment Guidelines, use of IT.
Social protection for the poor and vulnerable including elderly
Strengthening District Hospitals/Secondary care – CVD/CKD

Screening for Non Communicable Diseases-
Hypertension, Diabetes, Common Cancers
Builds on programmes for NCD prevention and control from several states
and NGO led pilots.
Population Enumeration: use of Family Health Folders
Targeted Population Based Screening
Essential Drug List for primary care- also recognize the complementary
practices of Ayurveda and other Indian Systems of Medicine.
IEC for behaviour modification;

Screening for Non Communicable Diseases-
Hypertension, Diabetes, Common Cancers Performance monitoring – through the use of IT and periodic external verification
Population based information- on the prevalence of hypertension, the level of successful control and incidence of complications (stroke, renal failure) that reflect primary care failures.
Team incentives based on annual performance assessment
Strengthen Continuity of care
Systems for referral to Medical Officer at PHC and an annual specialist consultation
Family folders designed to phase into Electronic Medical Records
Drug refills and compliance monitoring
Promotion of positive heath behaviours by ASHA and ANM
Patient support groups in the community

Anticipated Challenges Work processes to move from RCH/ID oriented systems to management
of chronic illnesses
Use of varying cadres of service providers: maintaining standards.
Creating training systems to accelerate scaling up.
Strengthen systems for monitoring, measurement and accountability
Ensure reach to the marginalized and elderly; eliminate disparities
Reduce fragmented care and maintain continuity of care.
Not being limited to care for diabetes and hypertension- focus on other
NCDs: COPD, CKD, Mental Health, musculoskeletal disorders
Ensuring universal access to secondary and tertiary care where needed
Close watch on out of pocket expenditures
Coordinated, inter-sectoral action

Thank You