lessons learned from the us chemical safety and hazard ... · csb investigation approach formal...
TRANSCRIPT

Lessons Learned from the US Chemical Safety
and Hazard Investigations Board
presented at
The IAEA International Conference on Human
and Organizational Aspects of Assuring
Nuclear Safety – Exploring 30 Years of Safety
Culture
Presented by Mark Griffon
Mark Griffon Consulting LLC
February 24, 2016

WHAT IS THE CSB? An independent U.S. federal agency
investigating chemical accidents promoting prevention – public knowledge
Authorized by Congress in 1990 Five Board Members; approximately 45 staff Modeled after NTSB
Intent of CSB investigations are to get to root
cause(s) and make recommendations toward prevention
Not regulatory; no enforcement authority
CSB Investigation Approach
Formal analysis to identify underlying technical, human
factor, management system, organizational and
regulatory causes of the incident.
Beyond immediate technical events and individual actions
Focus is on improving safety NOT assigning blame
Addressing the immediate cause ONLY prevents that
exact accident from occurring again.

CSB, Chevron Report, 2012
19 potential worker fatalities, 6 injuries,
15,000 people sought medical treatment
Oxygen
source
Ignition
source
People
present
“Hot Zone” not
of sufficient size
to protect
personnel
Released
process fluid
autoignitedLeak in
4-Sidecut line
4-Sidecut piping component was extremely thin
No formal method to communicate,
implement, oversee and track to
completion ETC findings and
recommendations
Line constructed of variable
corrosion rate-prone carbon
steel
Turnaround
team relied
on
inspection
data
Flammable
material
released
PHYS
ICAL E
VENT
S AND
CON
DITIO
NSOU
TCOM
ECH
EVRO
NIND
USTR
Y COD
ES
AND S
TAND
ARDS
Increased sulfidation
corrosion rates in low-
silicon carbon steel
Decision to remove insulation to identify
leak location rather than
shut down unit
Essential process safety analyses
not required by regulator
No requirement for ALARP
No Damage
Mechanism
Hazard Review
performed
Thorough
safeguard
evaluation not
conducted in PHA
Refer to Chevron Regulatory Report
Refer to Chevron Interim Investigation Report
Refer to Chevron Final Investigation Report
LEGEND
Chevron reliability
programs not effective
to implement ETC
Sulfidation Failure
Prevention Initiative
No guiding emergency leak
response protocol in place
100% component inspection not in
Richmond Inspection Plan
Consequences of potential
damage mechanisms
were not evaluated
Unit
metallurgists
were not
consulted
Minimal industry
emergency leak response
protocol requirements
Inconsistent API
standards
API does not
require 100%
component
inspection
Regulatory regime
reactive and activity-based
rather than goal-based
Regulators had little input
into safety precautions in
the refinery.
Assumption that
non-inspected
components were
of sufficient
thicknessImportant safety projects not
brought to management rather
than IMPACT team for
approval if outside framing
document requirements
Requests for
replacement or
100% inspection
outside of framing
document
requirements
Low-silicon component
not inspected
Inspection data did
not indicate pipe
was thin
Risk of catastrophic
failure not perceived by
decision makers
Trust in
management
Stop Work
uncommon
for shutting
down plant
“Stop Work”
not called
Past practice is to
keep running with
a small leakRecommendations to
replace or 100% inpect
4-Sidecut line not
implementedT-Min lowered so 4-sidecut
could stay in operation
Chevron
did not
use API
574
default
values
Chevron
allowed
inspector
to lower
alert
thickness
No MOC
performed
to
evaluate
risk of new
T-Min
Thorough inherently safer
systems analysis not
conducted in PHA
Regulator does not require or
oversee safety culture
assessment follow-up action
items

BP Texas City
• March 23, 2005
• 15 deaths and 180 injuries
• During startup, tower and blowdown drum overfilled
• Liquid hydrocarbon released, vapor cloud formed and ignited
• Explosion and fire

CSB Investigation • Most extensive investigation in CSB history
• Conducted 370 interviews
• Reviewed over 30,000 documents
• Assessment of 5-years of electronic data from the
computerized control board system
• Based on human factors framework (Reason, 1997)
and methodologies used in investigations of other
catastrophic incidents, such as Bhopal and Chernobyl
Baker panel findings
BP had not provided effective process safety leadership
BP had not established an open trusting relationship between management and the workplace
Lack of a unifying process safety culture
Personal Safety emphasis; not process safety
Reliance on low LTIR gave misleading risk indicator
Cost cutting pressures seriously degraded infrastructure
Mgmt failed to assess impact of cost and staff reductions on safety

Safety Culture Attributes the degree to which the workforce feels “empowered” as to process
safety
the extent to which the workforce feels free to report safety-related incidents
the process safety awareness, knowledge, and competency of the workforce;
relationships and trust between different workforce / management and contractors
whether deviations from policies and procedures are tolerated;
the extent of information flow at all levels
whether the workforce has a shared belief that safety comes first, regardless of financial, scheduling, or cost objectives; and
the extent to which the workforce is vigilant about process safety risks, continuously tries to reduce them, and seeks to learn from incidents and near misses.
5+ Years Later …..
Lessons Learned??

Macondo
April 20th, 2010
11 deaths
> 60 injured
~5 million barrels of oil
spilled in Gulf over 80+ days
Tremendous Economic
Impact

CSB Investigation
Examine specifics of organizational factors Staffing and organizational structure (changes)
Safety Metrics
Awards and Bonuses
Cost and Performance Pressures (cost and production goals)
Human factors analysis of how mistakes occurred Reliance on human intervention
Evidence / Explanations for “inexplicable” decisions leading up to the incident
Control / display panels
Decision making process

Macondo Safety Culture
“Government oversight must be accompanied by
sweeping reforms that accomplish no less
than a fundamental transformation of its safety
culture” (POSC)
“The lack of a strong safety culture resulting from
deficient overall systems approach is evident in
the multiple flawed decisions that led to the
blowout.” (NAE)
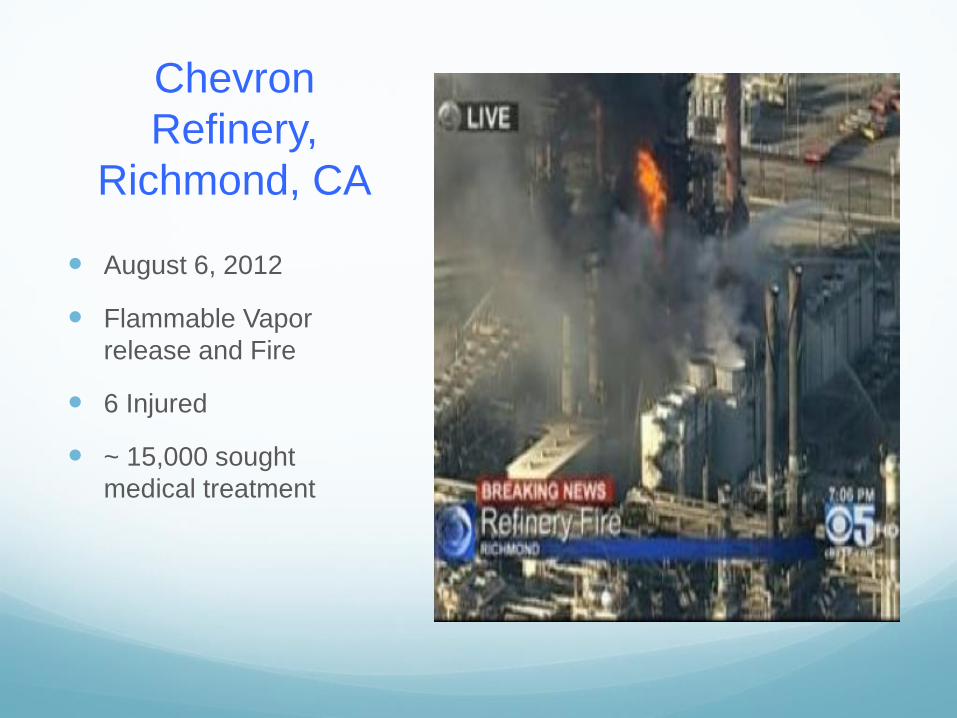
Chevron
Refinery,
Richmond, CA
August 6, 2012
Flammable Vapor
release and Fire
6 Injured
~ 15,000 sought
medical treatment

California PSM Reform
Employee Participation
Process Safety Culture Assessment
Human Factors
Management of Organizational Change

10+ years after BP Texas City ……
How are things going?

Maintaining Safe Production Cut exploration
Reduce manning
Reduce training
Reduce maintenance
Focus on today, not
tomorrow?
UK HSE, S. Mackenzie, 2015
<$50

Safety Performance
Personal
Process
UK HSE, 2015

Cautions / Challenges “the popularity of the concept has been
counterproductive and there is a danger of it becoming meaningless” (M. Fleming, ‘Regulator’s Guide to Safety Culture and Leadership’)
Overemphasis on the sharp end (front line worker) rather than the blunt end (organizational / management)
Risk Tolerance
How is it defined and who defines it
Safety culture study / change must consider inequalities of power and authority

Cautions / Challenges
Unified safety culture vs. understanding different sub-
cultures within an organization and optimizing how they
work together
Focus on Organizational Culture(s) influence on safety
rather then Safety Culture
Trusting and Reporting culture
Look at the real effect of resource limitations on safety

Will Off-Shore Drilling and Refinery Safety
be transformed like the Nuclear Industry?
Nuclear Industry, post TMI, developed a real belief that “if one of us fails, we all fail”
Nuclear Industry agreed to collect and share accident, near miss and indicator data (thru INPO)
Unclear whether same climate exists in Oil and Gas Industry Deepwater was ‘just a rogue operator’
Sharing of ‘lessons learned’, accident data, and near miss data is limited
Reaction to the price of oil
Public Reaction
Thank You