lesiones del cuello en la infancia
TRANSCRIPT

8 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
Evaluation of neck masses is a com-mon indication for imaging chil-dren. Fortunately, most lesions are
either congenital or inflammatory in ori-gin, and only 5% of all childhood neo-plasms occur in the head and neck. Theprimary goal of imaging is to determinethe extent of the disease and suggest a dif-ferential diagnosis based on the locationand imaging characteristics.
A reasonable differential diagnosiscan usually be made based on location(midline or lateral), clinical history (con-genital or acquired, presence or absenceof fever and tenderness), and imagingcharacteristics (cystic versus solid). Theremainder of this manuscript will focuson the more common cystic and solidmasses that occur in the pediatric neck.
Imaging modalitiesPotential imaging modalities include
conventional radiographs, ultrasound(US), computed tomography (CT), mag-netic resonance imaging (MRI) andnuclear medicine. Conventional radio-graphs are used for evaluation of patientswith stridor, suspected retropharyngealabscess or adenoid hypertrophy. Ultra-sound is ideal for optimally determiningwhether a mass is cystic or solid, as wellas for assessing whether a node is suppu-rative and for guiding abscess drainage.
In addition, it is the imaging modality of choice in children with suspected thy-roglossal duct cyst, not only to prove thecystic nature of the midline neck mass butalso to confirm the presence of a normal-appearing bi-lobed thyroid gland in thelower neck.1 Ultrasound is also ideal forevaluating patients with suspected fibro-matosis colli.2,3 Ultrasound, CT, or MRIcan be used for evaluating jugular veinpatency in patients with suspectedLemierre syndrome (internal jugular veinthrombophlebitis and septic emboli sec-ondary to pharyngotonsillitis).4,5 CT and/or MRI are frequently used to evaluate thetotal extent of more diffuse diseases,including inflammatory, congenital, andneoplastic processes. Since imaging withMRI frequently requires sedation in chil-dren less than 6 or 7 years of age, CT ofthe neck is more frequently performed onthese children. CT of the neck is also fre-quently performed in combination withCT of the chest/abdomen/pelvis in chil-dren with neoplasms such as lymphoma.
CT is ideal for evaluating osseous erosionin children with suspected rhabdomyosar-coma, with MRI frequently performed asan adjunct in patients with suspectedintracranial or intraspinal extension. MRIis the preferred method of imaging in chil-dren with suspected hemangioma ofinfancy, congenital vascular malforma-tions, cervical neuroblastoma, and neu-rofibroma. Nuclear medicine imaging isfrequently used in combination with CTand/or MRI for evaluation of childrenwith neuroblastoma (I-123), lymphoma(gallium-67 citrate or fluorodeoxyglucosepositron emission tomography [FDG-PET]), osteomyelitis (technetium [Tc]-99m-methylene diphosphonate [MDP],gallium-67 citrate) and other neoplasms.
Cystic neck massesThe majority of cystic neck masses in
children are congenital malformationsand include thyroglossal duct cysts, bran-chial apparatus cysts, dermoid cysts, andlymphatic malformations.
The child with a neck mass
Bernadette L. Koch, MD
Dr. Koch is a Staff Radiologist, Neurora-diologist, Associate Professor of Radiol-ogy, and Assistant Professor of Pediatrics,Department of Radiology, CincinnatiChildren’s Hospital Medical Center,Cincinnati, OH.

10 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
CHILD WITH A NECK MASS
Thyroglossal duct cystsThe thyroglossal duct (TGD) is a nor-
mal fetal structure that extends from theforamen cecum at the posterior aspect ofthe tongue to the lower neck in the regionof the thyroid bed. The TGD normallyinvolutes during the 5th or 6th week offetal life. If any portion of the duct doesnot involute, remnant secretory epithe-lium may form a cyst.6,7 Most TGD cystsoccur in the midline. Twenty percent to 25% are in the suprahyoid neck, 15% to
59% are at the hyoid bone, and 25% to 65% are in the infrahyoid neck.7,8
Patients typically present with a midlineneck mass that elevates with swallowingor protrusion of the tongue. If infected,they might present with warmth, ery-thema, and fever. In the past, nuclear med-icine imaging with Tc-99m-pertechnetatewas used to assess for the presence of a bi-lobed thyroid gland in the lower neck andrule out ectopic thyroid in the midlinemass. More recently, US has been used to
evaluate for a normal-appearing bi-lobedthyroid gland in the lower neck and toconfirm the cystic nature of the midlineneck mass.1 Uncomplicated thyroglossalduct cysts may be anechoic, hyperechoic,or heterogeneous on US. The presence ofintralesional echoes does not imply super-imposed infection or hemorrhage (Figure1).9 On CT and MRI, thyroglossal ductcysts will appear as fluid-filled cysts ofvariable attenuation and signal intensity,depending on the protein content of the
FIGURE 1. Thyroglossal duct cyst. (A) Transverse sonographic image shows a hypoechoic well-defined paramidline neck mass with a thinimperceptible wall and increased through-transmission. (B) Transverse sonographic image in the lower neck shows a normal-appearing bi-lobed thyroid gland.
A B
FIGURE 2. Thyroglossal duct cyst. Axial CT imageshows a low-attenuation nonenhancing midlinemass at the base of the tongue.
FIGURE 3. Diagram of the face shows distribution of first branchial apparatus anom-alies (Figure reprinted with permission from Olsen KD, Maragos NE, Weiland LH. Firstbranchial cleft anomalies. Laryngoscope. 1980;90:423-43611; and from Benson MT,Dalen K, Mancuso AA. Congenital anomalies of the branchial apparatus: Embryologyand pathologic anatomy. RadioGraphics. 1992;12:943.12)

www.appliedradiology.com APPLIED RADIOLOGY©� 11August 2005
CHILD WITH A NECK MASS
A B
FIGURE 4. First branchial apparatus anomaly. Axial fast spin-echo images (A) at the level of the parotid gland and (B) at the level of the lower aspectof the external auditory canal show two hyperintense cystic masses that were connected by a small fluid-filled tract (images of the tract not included).
FIGURE 5. Second branchial apparatus cyst. Axial postcon-trast CT image shows a well-defined, low-attenuation, nonen-hancing left neck mass anterior to the sternocleidomastoidmuscle, lateral to the carotid sheath, and posterior to the sub-mandibular gland.
FIGURE 6. Diagram shows the course of the thymopharyngeal duct. (Figurereprinted with permission from Benson MT, Dalen K, Mancuso AA. Congenitalanomalies of the branchial apparatus: Embryology and pathologic anatomy.RadioGraphics. 1992;12:94312; and from Zarbo RJ, McClatchey KD, AreenRG, et al. Thymopharyngeal duct cyst: A form of cervical thymus. Ann OtolRhinol Laryngol. 1983;92(3 Pt 1):284-289.15)

12 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
CHILD WITH A NECK MASS
cyst (Figure 2). If there is superimposedinfection, there may be edema in the adja-cent soft tissues and peripheral contrastenhancement. Treatment of thyroglossalduct cysts is surgical excision (Sistrunkprocedure) that includes excision of thecyst, the entire remnant tract, and a centralportion of the hyoid bone.10
Branchial apparatus anomaliesNormal branchial apparatus embryol-
ogy is quite complex and beyond thescope of this manuscript. However, ingeneral, the branchial apparatus structuresdevelop between the 4th and 6th week
of gestation and consist of 6 pairs of meso-dermal branchial arches separated by 5 paired endodermal pharyngeal pouchesinternally and 5 paired ectodermal bran-chial clefts externally. Anomalies of thebranchial apparatus may be in the form ofcysts, sinus tracts, or fistulae. Branchialapparatus cysts are the most commonbranchial apparatus anomalies that re-quire imaging.
First branchial anomalies account foronly 8% of all branchial anomalies andare usually cysts or sinuses near the ex-ternal auditory canal, the pinnae, or theregion of the parotid gland (Figure 3).11-13
Patients typically present with masses orsinus tracts, with or without recurrentinfection. The cysts may be imaged withCT, US, or MRI. MR imaging is ideal inevaluating the fluid-filled tract, whichmay extend from the more superficial cystto the external auditory canal (Figure 4).
Second branchial apparatus cysts arethe most common and account for up to95% of all branchial apparatus anomalies.Most are located anterior to the sternoclei-domastoid muscle, posterior to the sub-mandibular gland and lateral to the carotidsheath (Figure 5). Occasionally, cysts mayprotrude between the internal and external
FIGURE 8. Dermoid cyst. Axial postcontrast CT image shows alow-attenuation, nonenhancing right paramidline anterior neckmass deep to the strap muscles. Differential diagnosis includesa thyroglossal duct cyst.
FIGURE 9. Lipoma. Axial postcontrast CT of the lower neck shows a lobu-lated fat-attenuation mass at the cervicothoracic junction.
FIGURE 7. Third branchial apparatus anomaly—thymic cyst. (A) Axial post-contrast CT image at the level of the hyoid bone shows a well-defined, low-attenuation, nonenhancing mass in the region of the carotid sheathdeviating the internal carotid artery anteriorly (arrow) and the jugular vein lat-erally (arrowhead). (B) Axial postcontrast CT image at the level of the uppermediastinum shows extension of the low-attenuation mass to the expectedlevel of the thymus.
A B

www.appliedradiology.com APPLIED RADIOLOGY©� 13August 2005
CHILD WITH A NECK MASS
carotid arteries; rarely, they are deep to theplatysma muscle and anterior to the sterno-cleidomastoid muscle or located directlyadjacent to the pharyngeal wall.14 As withother cysts, these lesions will be hyper-echoic or anechoic on US, low in attenua-tion on CT, and fluid in signal intensity onMRI unless there is associated superim-posed infection, which will change the
imaging characteristics on all modalities.The key to making this diagnosis is thelocation of the lesion.
The most common third branchialapparatus anomaly is the thymic cyst.These are rare remnants of the thirdbranchial pouch. In normal embryologicdevelopment, the thymic primordiamigrates from the pharynx caudally and
fuses in the anterior mediastinum along thecourse of the thymopharyngeal duct. Simi-lar to the thyroglossal duct cysts, when theduct fails to involute, a cyst may occuranywhere along the thymopharyngeal ductfrom the angle of the mandible to the uppermediastinum (Figure 6).12,15 There may beintralesional echoes on US with or withoutsuperimposed hemorrhage or infection.
FIGURE 10. Lymphatic malformation. Axial postcontrast CT image shows a low-attenuation nonenhancing left supraclavicular neck mass that extends to theposterior paraspinal soft tissues of the upper back.
FIGURE 11. Lymphatic malformation. Axial fast spin-echoimage of the neck shows a multilocular right neck mass deepto the sternocleidomastoid muscle with several fluid-fluid lev-els consistent with blood products secondary to prior intra-lesional hemorrhage.
FIGURE 12. Mixed lymphatic and venous malformation.Postcontrast axial CT images show an enlarged rightpalatine tonsil without significant contrast enhancement,with multiple intralesional small round calcifications con-sistent with phleboliths.
FIGURE 13. Fibromatosis colli. Longitudinal sonographic image of the right neckshows diffuse enlargement of the right sternocleidomastoid muscle with fairlyhomogeneous echoes.

14 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
Up to 50% of cervical thymic cysts willbe continuous with the mediastinal thy-mus (Figure 7).16 Cervical thymic cystsare intimately associated with thecarotid sheath; they frequently splay thecarotid artery and jugular vein, particu-larly when they involve the suprahyoidneck. As with other branchial apparatusanomalies, the location is the key to suggesting the diagnosis. In a child, anycystic mass that involves the neck andalso extends to the anterior mediastinumshould certainly suggest a cervicalthymic cyst.
Dermoid cysts and epidermoid cystsDermoid cysts may contain squa-
mous epithelium and skin appendagessuch as hair follicles and sebaceousglands. Epidermoid cysts contain onlysquamous epithelium. Both may present
as midline neck masses with variableattenuation, echogenicity, and signalintensity, depending on internal con-tents (Figure 8). If fat globules areidentifiable on CT or MRI, then a der-moid cyst is the most likely diagnosis.If there are associated calcifications,then the lesion is more likely a ter-atoma or venous malformation. If thelesion is entirely composed of fat, thensimple lipoma is the most likely diag-nosis (Figure 9).
Lymphatic malformationsLymphatic malformations (LMs) are
vascular malformations composed ofprimative embryonic lymph sacs ofvarying sizes. Lymphatic malformationstypically increase in size as the childgrows, and they may show rapid increasein size in association with upper respira-
tory tract infection or intralesional hem-orrhage. Although they may be seen ingenetic syndromes such as Turner’s syn-drome, Noonan’s syndrome, and trisomy21 syndrome, most LMs occur in chil-dren with normal karyotype.
Lymphatic malformations can bedivided into microcystic, macrocystic,or mixed lesions. They may be unilocu-lar, multilocular, focal, or diffuse/infil-trative. The fluid-filled spaces areusually anechoic or hypoechoic on USand usually have low attenuation on CTand fluid signal intensity on MRI. Theremay be minimal enhancement of inter-nal septations.17-20 They are the primarycystic malformation to present withtransspatial involvement (Figure 10). Ofall cystic lesions in the neck, LMs arethe most likely to hemorrhage, fre-quently resulting in intralesional fluid-fluid levels (Figure 11). As with othercystic lesions, if there is superimposedinfection, the imaging characteristicswill change accordingly.
Lymphatic malformations are fre-quently part of mixed vascular mal-formations, with the most common
CHILD WITH A NECK MASS
FIGURE 14. Mycobacterium avium intracellulare adenopathy. Axial postcontrast CT imagesreveal multiple intraparotid and periparotid left neck nodes with low-attenuation centers with-out significant edema in the subcutaneous fat.
FIGURE 15. Cat-scratch disease. Axial post-contrast CT of the neck shows right greaterthan left enlarged anterior and posterior cer-vical chain lymph nodes in a toddler withoutfever, erythema, or pain. The boy had arecent history of a cat bite to the tongue.
16 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
CHILD WITH A NECK MASS
additional component being a venousmalformation. The venous malforma-tion component may appear as a cysticmalformation on precontrast images butwill show postcontrast enhancement andmay contain phleboliths (Figure 12).When LMs are complex and transspatialor when they involve multiple structuresof the neck (eg, airway, tongue, floor ofmouth) or the parotid gland, and inpatients with combined vascular malfor-mations, MR imaging is the preferredmodality.18-20
The preferred treatment of LMs is sur-gical excision. However, complete surgi-cal excision may be difficult when thelesions are microcystic and infiltrative.Macrocystic lesions may also be treatedwith percutaneous sclerotherapy, includ-ing alcohol solution, cyclophosphamide,bleomycin and doxycycline.21-23
Solid neck massesThe remainder of this manuscript will
focus on benign and malignant extra thy-roid solid neck masses in children,
including fibromatosis colli, inflamma-tory adenopathy, hemangioma, neurofi-broma, teratoma, lymphoma, rhabdomyo-sarcoma, neuroblastoma, and metastaticadenopathy.
Fibromatosis colliFibromatosis colli or sternocleido-
mastoid tumor of infancy occurs inneonates. The etiology is uncertain butmay be related to intramuscular hemor-rhage or fibrosis. There is an increasedrisk in neonates with a history of breechpresentation and/or difficult delivery.Patients typically present at 2 to 4 weeksof age with a unilateral neck mass,with or without torticollis. Ultrasoundis the imaging modality of choice,showing focal or diffuse enlargementof the ster-nocleidomastoid muscle(SCM), which may be homogeneousor heterogeneous in echotexture (Fig-ure 13). There may be a rim of de-creased echoes thought to representcompressed normal adjacent stern-ocleidomastoid muscle.2,3,24
Inflammatory adenopathyNonsuppurative adenitis is the most
common non-neoplastic solid neck massin children. The majority of children withuncomplicated cervical adenitis aretreated medically and do not require imag-ing. If they are toxic-appearing or havesymptoms that increase despite adminis-tration of antibiotic therapy, postcontrastCT imaging is frequently performed toassess the extent of the inflammatoryprocess and rule out a focal abscess. Whenimaging children with cervical adenitis,the key questions to be answered are loca-tion of abscess, extent of cellulitis andmyositis, and evaluation of the vascularstructures of the neck to exclude jugularvein compression or thrombosis as well asnarrowing of the internal carotid artery.25
Lymphadenitis may be secondary to viraldisease, bacterial disease, mycobacterialdisease, or fungal disease. Nonsuppura-tive inflammatory adenitis has a typicalappearance on all imaging modalitiesshowing multiple (sometimes conglomer-ate) nodes. Hilar flow is demonstrated on
A B
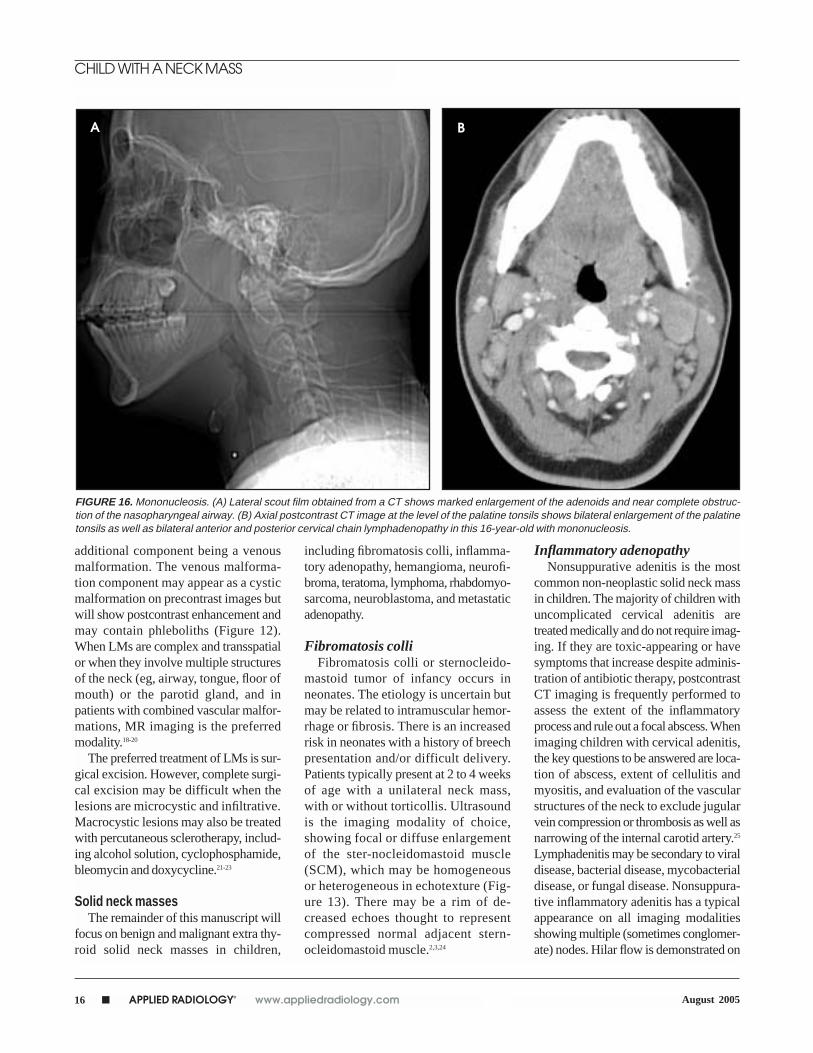
FIGURE 16. Mononucleosis. (A) Lateral scout film obtained from a CT shows marked enlargement of the adenoids and near complete obstruc-tion of the nasopharyngeal airway. (B) Axial postcontrast CT image at the level of the palatine tonsils shows bilateral enlargement of the palatinetonsils as well as bilateral anterior and posterior cervical chain lymphadenopathy in this 16-year-old with mononucleosis.

www.appliedradiology.com APPLIED RADIOLOGY©� 17August 2005
CHILD WITH A NECK MASS
FIGURE 17. Abscess. Axial postcontrast CT image of the neckshows a low-attenuation left submandibular collection with avery irregular, mildly enhancing wall and associated edema ofthe adjacent subcutaneous fat and several small lymph nodesat the periphery.
FIGURE 18. Hemangioma. Axial postcontrast CT image shows diffuseenhancement of a large neck mass that replaces the deep and superficialportions of the right parotid gland in an infant.
FIGURE 19. Hemangioma. Axial postcontrast T1-weighted image shows diffuse homogenous contrastenhancement of a left parotid gland mass with multi-ple intralesional high-flow vessels.
FIGURE 20. Neurofibroma. Axial fast spin-echo image at the level of the epiglottisshows large bilateral symmetric carotidsheath masses and elongated serpiginoussuboccipital masses. The right suboccipitallesions show focal central areas ofhypointensity typical of a target sign, whichis consistent with neurofibroma.
FIGURE 21. Teratoma. Axial postcontrastCT image of the upper neck shows a largeheterogeneous neck mass in this neonate.There are multiple areas of fat attenuationas well as multifocal areas of calcification.

18 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
CHILD WITH A NECK MASS
US. Nontuberculous mycobacterial dis-ease may lack evidence of surroundingcellulitis and myositis and may containsmall calcifications or low-attenuationcenters (Figure 14).26-28 Cat-scratch diseaseis not uncommon in children and may alsopresent with cervical adenopathy, withoutsignificant associated cellulitis (Figure15). This diagnosis should be consideredin any child with a history of exposure tocats. If a child without evidence of celluli-
tis presents with significant cervicaladenopathy and associated enlargementof the palatine and adenoid tonsils, mono-nucleosis should be considered (Figure16). A well-defined or irregularly shapedfluid collection with an enhancing rim iscertainly suggestive of an abscess (Fig-ure 17). However, these imaging charac-teristics are not 100% specific, and theappearance of phlegmon without truedrainable pus can be similar.29
Hemangioma of infancyHemangioma of infancy is a benign
neoplasm resulting from endothelial pro-liferation, which usually presents in chil-dren less than 6 months of age, graduallyincreases over the next 2 years, and spon-taneously involutes over the next 5 to 7 years. In the proliferative phase, theydemonstrate diffuse intense contrastenhancement (Figure 18). High-flowintralesional flow voids will be demon-
FIGURE 22. Lymphoma. (A) Axial postcontrast CT image of the neck showsbulky left anterior and posterior cervical chain lymph nodes, as well as conglom-erate nodes posterior to the trachea deviating the trachea and thyroid anteriorlyand to the right. (B) Gallium-67 citrate scintigraphy shows uptake in the leftsupraclavicular region and anterior neck in this child with Hodgkin’s disease.
A B
FIGURE 23. Lymphoma. (A) Axial postcontrast CT image shows conglomerate lymph nodes compressing the jugular vein in the left lower neck.(B) Corresponding fluorodeoxyglucose positron emission tomographic image shows abnormal uptake in the left supraclavicular region, as wellas in the left mediastinum.
A B

20 � APPLIED RADIOLOGY© www.appliedradiology.com August 2005
CHILD WITH A NECK MASS
strated on MRI (Figure 19). During theinvolutional phase, they show evidenceof fatty infiltration and decrease insize.30,31 Attention to the age of the patientwith a significantly enhancing neck massis extremely important. In an older childwithout a prior history of a neck mass ininfancy, similar imaging characteristicsshould raise the question of sarcomarather than of benign hemangioma.Treatment of hemangioma occurring inan infant is usually expectant waiting.Steroids, interferon, and, rarely, surgeryare reserved for lesions that compromisethe airway or are associated with signifi-cant loss of skin integrity.
NeurofibromasNeurofibromas are unencapsulated
benign nerve sheath tumors of Schwanncell origin. They may be single or multi-ple; when multiple or plexiform, theyalmost always occur in children with neu-rofibromatosis Type 1. Solitary lesions
may be very well defined; plexiformlesions are ill defined and infiltrative. Fre-quently, neurofibromas will show vari-able contrast enhancement, with orwithout a “target sign” composed of acentral area of decreased T2 signal inten-sity and decreased contrast enhancement(Figure 20).32
TeratomasTeratomas are neoplasms composed
of multiple tissues that are foreign to thepart of the body in which the lesionarises.33 Teratomas in children are mostcommonly sacrococcygeal, and 5% to14% occur in the head and neck region;most of these children are less than 1 year of age at the time of diagnosis.These lesions contain all 3 germ layers,originate from pleuripotential cells, andmay be composed of mature or immatureelements. In the neonate, the presence ofimmature elements does not correlatewith malignant potential, and most ter-
FIGURE 24. Rhabdomyosarcoma. Axial postcontrastCT image of the neck shows a large heterogeneousright neck mass. This mass surrounds the carotidartery and deviates it anteriorly and medially. The jugu-lar vein is not identified.
FIGURE 25. Neuroblastoma. Axial proton-density–weighted image of the neck shows awell-defined right neck mass in the carotid sheath deviating the carotid artery and jugularvein anteriorly and mildly deviating the trachea to the left.
FIGURE 26. Neuroblastoma. Posterior I-123-metaiodobenzylguanidine image of thechest reveals focal areas of abnormalincreased radiopharmaceutical uptake inthe left shoulder and midthoracic spine inthis patient with known neuroblastoma. Notenormal uptake in the salivary glands.

www.appliedradiology.com APPLIED RADIOLOGY©� 21August 2005
CHILD WITH A NECK MASS
atomas are benign. Most are very large and complexlesions containing solid and cystic components, fre-quently with fat and calcification (Figure 21). Treatmentis surgical excision.
Malignant solid massesLymphoma
Malignant lymphoma accounts for approximately 50%of head and neck malignancies in children. Approximately50% of cervical involvement with lymphoma is due toHodgkin’s disease and 50% due to non-Hodgkin’s lym-phoma. Imaging characteristics cannot distinguishbetween the two. Patients may present with unilateral orbilateral disease in both Hodgkin’s and non-Hodgkin’slymphoma. Lymphomatous nodes have a similar appear-ance to inflammatory and metastatic nodes from other pri-mary malignancies. However, lymphomatous nodes arefrequently larger and more extensive than inflammatoryadenopathy. The differential diagnosis in children withbulky cervical adenopathy includes mononucleosis (partic-ularly if there is associated enlargement of the adenoidsand palatine tonsil), metastatic disease (rarely, from pri-mary malignancy such as nasopharyngeal carcinoma,rhabdomyosarcoma, or neuroblastoma), and lymphopro-liferative disease (particularly in the posttransplantpatients). Imaging of patients with head and neck lym-phoma should include CT of the involved area and adja-cent lymph nodes as well as the chest, abdomen, andpelvis. In addition, gallium-67 citrate scintigraphy is fre-quently used for initial staging and follow-up (Figure 22).Increasingly, FDG-PET is being used in evaluation ofthese patients (Figure 23).
RhabdomyosarcomaRhabdomyosarcoma is the most common childhood
soft-tissue sarcoma and involves the head and neck in upto 40% of patients.34,35 Rhabdomyosarcoma is divided bysites of origin into orbit, parameningeal (middle ear,paranasal sinus, nasopharynx), and all other sites. Up to55% of parameningeal rhabdomyosarcomas have intra-cranial extension. In these patients, CT is helpful to assessbony destruction and MRI is complimentary to evaluatefor intracranial extension. Rhabdomyosarcoma is typi-cally heterogeneous on all imaging modalities (Figure24), with or without osseous erosion.34
NeuroblastomaNeuroblastoma is the most common malignant tumor in
children <1 year of age; primary lesions are usually locatedin the adrenal gland and retroperitoneum. Cervical lym-phadenopathy from neuroblastoma is most often metasta-tic disease. Less than 5% of primary lesions are located inthe neck. In addition to presenting with a palpable neckmass, patients may present with feeding difficulties,
FIGURE 27. Metastatic adenopathy. (A) Axial postcontrast CT of the neckshows a heterogeneous left supraclavicular mass deviating the trachea to theright in a patient with metastatic hepatoblastoma. (B) Axial postcontrast CTimage of the neck shows large heterogeneous left neck mass deviating andcompressing the jugular vein in a teenager with metastatic testicular carci-noma. (C) Axial postcontrast CT image of the neck shows a heterogeneouslow-attenuation left lower neck mass with an irregular enhancing wall in ateenager with metastatic nasopharyngeal carcinoma.
A
B
C

airway symptoms, or opsomyoclonus(opsoclonus, myoclonus, and cerebellarataxia), which is thought to be a paraneo-plastic syndrome. Most patients with cervi-cal primary lesions present with a well-defined mass posterior to the carotid sheathvessels with or without intraspinal exten-sion and with or without calcification.36-38
CT and MRI nicely show the primary mass(Figure 25), occasionally with intraspinalextension. In addition to CT or MRI, I-123-metaiodobenzylguanidine (MIBG) is in-dicated in the workup of these children toassess for metastatic disease (Figure 26).
Metastatic adenopathyMetastatic cervical adenopathy un-
related to lymphoma is very uncommonin children. Potential etiologies includeneuroblastoma, rhabdomyosarcoma, naso-pharyngeal carcinoma, and thyroid carci-noma (Figure 27).
ConclusionThe majority of cystic neck masses in
children are congenital. When midline orparamidline in position, thyroglossal ductcyst and dermoid cyst are the primary dif-ferential considerations. When off mid-line, branchial apparatus cysts andlymphatic malformations should be con-sidered. Based on location and appear-ance, the majority of branchial apparatuscysts can be differentiated from lym-phatic malformations.
Most solid neck masses in children arebenign, including fibromatosis colli, in-flammatory adenopathy, hemangioma ofinfancy, neurofibroma, and benign ter-atoma. Using the clinical history, physicalexamination and imaging characteristics,most of these can be diagnosed withsome certainty. Malignant lesions includelymphoma, rhabdomyosarcoma, neurob-lastoma, and, rarely, metastatic adenopa-thy. Although it may be more difficult tomake a definitive diagnosis in these chil-dren, with the above-mentioned imagingcharacteristics and clinical history, a rea-sonable differential diagnosis should beachievable.
REFERENCES1. Lim-Dunham JE, Feinstein KA, Yousefzadeh DK, etal. Sonographic demonstration of a normal thyroid
gland excludes ectopic thyroid in patients with thy-roglossal duct cyst. AJR Am J Roentgenol. 1995;164:1489-1491.2. Youkilis RA, Koch B, Myer CMI. Ultrasonographicimaging of sternocleidomastoid tumor of infancy. AnnOtol Rhinol Laryngol. 1995;104:323-325.3. Chan YL, Cheng JC, Metreweli C. Ultrasonographyof congenital muscular torticollis. Pediatr Radiology.1992;22:356-360.4. Screaton NJ, Ravenel JG, Lehner PJ, et al. Lemierresyndrome: Forgotten but not extinct––report of fourcases. Radiology. 1999;213:369-374.5. Ramirez S, Hild TG, Rudolph CN, et al. Increaseddiagnosis of Lemierre syndrome and other Fusobac-terium necrophorum infections at a Children’s Hospital.Pediatrics. 2003;112:e380.6. Thomas JR. Thyroglossal-duct cysts. Ear NoseThroat J. 1979;58:510-514.7. Pounds LA. Neck masses of congenital origin. Pedi-atr Clin North Am. 1981;28:841-844.8. Solomon JR, Rangecroft L. Thyroglossal-ductlesions in childhood. J Pediatr Surg. 1984;19:555-561.9. Wadsworth DT, Siegel MJ. Thyroglossal duct cysts:Variability of sonographic findings. AJR Am J Roentgenol.1994;163:1475-1477.10. Sistrunk WE. The surgical treatment of cysts of thethyroglossal tract. Ann Surg. 1920;71:121-123.11. Olsen KD, Maragos NE, Weiland LH. First branch-ial cleft anomalies. Laryngoscope. 1980;90:423-436.12. Benson MT, Dalen K, Mancuso AA, et al. Congen-ital anomalies of the branchial apparatus: Embryologyand pathologic anatomy. RadioGraphics. 1992;12:943-960.13. Mukherji SK, Fatterpekar G, Castillo M, et al. Imag-ing of congenital anomalies of the branchial apparatus.Neuroimaging Clin N Am. 2000;10:75-93, viii.14. Bailey H. Branchial Cysts and Other Essays on Sur-gical Subjects in the Faciocervical Region. London, UK:HK Lewis & Co.; 1929.15. Zarbo RJ, McClatchey KD, Areen RG, Baker SB.Thymopharyngeal duct cyst: A form of cervical thymus.Ann Otol Rhinol Laryngol. 1983;92(3 Pt 1):284-289. 16. Guba AM, Adam AE, Jaques DA, Chambers RG.Cervical presentation of thymic cysts. Am J Surg.1978;136:430-436.17. Burrows PE, Fellows KE. Techniques for manage-ment of pediatric vascular anomalies. In Cope E, ed.Current Techniques in Interventional Radiology.Philadelphia, PA: Current Medicine; 1995:12.18. Baker LL, Dillon WP, Hieshima GB, et al. Heman-giomas and vascular malformations of the head andneck: MR characterization. AJNR Am J Neuroradiol.1993;14:307-314.19. Fordham LA, Chung CJ, Donnelly LF. Imaging ofcongenital vascular and lymphatic anomalies of thehead and neck. Neuroimaging Clin N Am. 2000;10:117-136, viii.20. Meyer JS, Hoffer FA, Barnes PD, Mulliken JB. Biological classification of soft-tissue vascular anom-alies: MR correlation. AJR Am J Roentgenol. 1991;157:559-564.21. Dubois J, Garel L, Abela A, et al. Lymphangiomasin children: Percutaneous sclerotherapy with an alco-holic solution of zein. Radiology. 1997;204:651-654.22. Turner C, Gross S. Treatment of recurrent suprahy-oid cervicofacial lymphangioma with intravenouscyclophosphamide. Am J Pediatr Hematol Oncol.1994;16:325-328.23. Molitch HI, Unger EC, Witte CL, vanSonnenberg E.Percutaneous sclerotherapy of lymphangiomas. Radi-ology. 1995;194:343-347.
24. Yamaguchi M, Takeuchi S, Matsuo S. Ultrasonicevaluation of pediatric superficial masses. J Clin Ultra-sound. 1987;15:107-113.25. Hudgins PA, Dorey JH, Jacobs IN. Internal carotidartery narrowing in children with retropharyngeal lym-phadenitis and abscess. AJNR Am J Neuroradiol.1998;19:1841-1843.26. Nadel DM, Bilaniuk L, Handler SD. Imaging of gran-ulomatous neck masses in children. Int J PediatrOtorhinolaryngol. 1996;37:151-62.27. Hazra R, Robson CD, Perez-Atayde AR, HussonRN. Lymphadenitis due to nontuberculous mycobac-teria in children: Presentation and response to ther-apy. Clin Infect Dis. 1999;28:123-129.28. Robson CD, Hazra R, Barnes PD, et al. Nontu-berculous mycobacterial infection of the head and neck in immunocompetent children: CT and MR findings. AJNR Am J Neuroradiol. 1999;20:1829-1835.29. Stone ME, Walner DL, Koch BL, et al. Correlationbetween computed tomography and surgical find-ings in retropharyngeal inflammatory processes in children. Int J Pediatr Otorhinolaryngol. 1999;49:121-125.30. Mulliken JB, Glowacki J. Hemangiomas and vascu-lar malformations in infants and children: A classifica-tion based on endothelial characteristics. PlastReconstr Surg. 1982;69:412-422.31. Burrows PE, Mulliken JB, Fellows KE, et al. Child-hood hemangiomas and vascular malformation: Angio-graphic differentiation. AJR Am J Roentgenol. 1983;141:483-488.32. Suh JS, Abenoza P, Galloway HR, et al. Peri-pheral (extracranial) nerve tumors: Correlation of MRimaging and histologic findings. Radiology. 1992;183:341-346.33. Batsakis JG. Tumors of the Head and Neck: Clinicaland Pathological Considerations. Baltimore, MD:Williams & Wilkins; 1979.34. Castillo M, Pillsbury HC 3rd. Rhabdomyosarcomaof the middle ear: Imaging features in two children.AJNR Am J Neuroradiol. 1993;14:730-733.35. Latack JT, Hutchinson RJ, Heyn RM. Imaging ofrhabdomyosarcomas of the head and neck. AJNR AmJ Neuroradiol. 1987;8:353-359.36. Abrahmson SJ, Berdon WE, Ruzal-Shapiro C. Cer-vical neuroblastoma in eleven infants: A tumor withfavorable prognosis. Clinical and radiologic findings.Pediatr Radiol. 1993;23:253-257.37. Casselman JW, Smet MH, Van Damme B, LemahieuSF. Primary cervical neuroblastoma: CT and MR find-ings. J Comput Assist Tomogr. 1988;12:684-686.38. Smith MC, Smith RJ, Bailey CM. Primary cervicalneuroblastoma in infants. J Laryngol Otol. 1985;99:209-214.
Products used• 1.5T GE Signa MRI unit (GE Healthcare,
Waukesha, WI)• LightSpeed (4-detector) CT scanner (GE
Healthcare)• Acuson ultrasound scanner (Siemens Medical
Solutions, Malvern, PA)• Optiray CT contrast (Tyco Healthcare/
Mallinckrodt, St. Louis, MO) • Magnevist MR contrast (Berlex Laboratories,
Wayne, NJ)
CHILD WITH A NECK MASS
August 200522 � APPLIED RADIOLOGY© www.appliedradiology.com