lecturer: dr lucy patston [email protected]. girl living with half her
TRANSCRIPT

Week beginningMonday 16 September 2013
Lecture 16
NeuroplasticityLecturer: Dr Lucy Patston

www.youtube.com/watch?v=2MKNsI5CWoU Girl living with half her brain

Lundy: Chapter 4 Tortura: PDF provided on Moodle
Reading
Lundy-Ekman. Neuroscience: Fundamentals for Rehabilitation, 4th Edition. W.B. Saunders Company, 2013.
Kandel et al. Principles of Neural Science, 5th Edition. McGraw Hill, 2012.
Tortura & Derrickson. Principles of anatomy and physiology, 13th Edition. Wiley. 2012.

What is neuroplasticity Central chromatolysis and Wallerian
degeneration Axonal injury in the PNS Mechanisms for recovery in CNS
Overview
Be able to discuss cellular processes after injury (central chromatolysis & Wallerian degeneration)
Be able to name and discuss two mechanisms of sprouting in the PNS
Be able to name and discuss four mechanisms for synaptic recovery in the CNS
Be able to explain why there is no repair of damaged axons in the CNS
Learning Objectives

Capacity of nervous system to adapt to change◦ Learning◦ Injury
Old thinking – cortical representations static upon reaching adulthood, then:
1992: Canadian researchers discovered epidermal growth factor (EGF) stimulated cells from adult mice brains to proliferate into neurons and astrocytes
1998: Human hippocampus seen to show significant number of new neurons
Neuroplasticity Intro

Now we know – brain is dynamic structure, changing constantly through experience◦ Use it or lose it!
Changes: sprouting new dendrites, synthesis of new proteins, changes in synaptic contacts
Despite this, neurons have limited ability to regenerate (replicate and repair themselves)
Change can be anatomical, physiological or pharmacological
Neuroplasticity Intro

Anatomical◦ Studies showing cortical motor maps change upon
learning new skill – piano◦ Recovering from stroke with interventions aimed at
motor movement etc. (fMRI studies) Physiological
◦ Refinement of synaptic connections by experience◦ E.g., music, doing stuff (dancing, swimming),
emotional or social development Pharmacological
◦ Adaptation of synapses after damage, injury or toxic insult Forms basis of addiction/withdrawal
Types of Neuroplasticity

Injuries damaging or severing axons may be recoverable
Injuries to cell bodies, however, usually cause death of the neuron
In PNS damage to dendrites and myelinated axons may be repaired in cell body remains intact and if Schwann cells remain active
In CNS little or no repair of damage occurs (even when cell body intact, a severed axon cannot be repaired or regrown)◦ NB: This is not to say that new neurons/synapses do
not grow
Cellular Recovery from Injury

24-48 hours after injury, cell body undergoes central chromatolysis◦ parts of the cell body
break down/dissolve (Nissl bodies); nucleus moves toward periphery of soma; presynaptic terminals retract
Apoptosis (cell death) may then occur
Central Chromatolysis


By Day 3-5 after an axon is severed, ◦ part connected to cell body is
called proximal segment◦ Part isolated from cell body is
called distal segment Cytoplasm leaks out and
segments retract from each other
Distal segment then undergoes process called Wallerian degeneration
Axonal injury
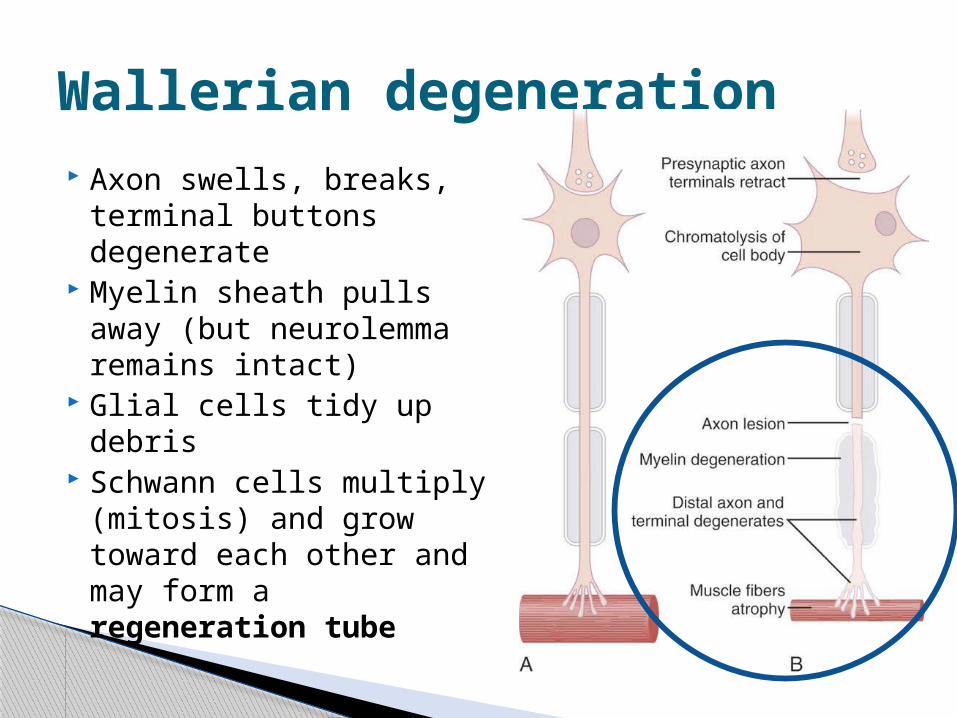
Axon swells, breaks, terminal buttons degenerate
Myelin sheath pulls away (but neurolemma remains intact)
Glial cells tidy up debris Schwann cells multiply
(mitosis) and grow toward each other and may form a regeneration tube
Wallerian degeneration

Regeneration tube acts as protection and guidance for axon to regrow across injury site (if small enough)

Common due to long-range axons not sheltered by skull or vertebral column
Axons may be severed by knives, machines etc.
Axons may undergo repair if:◦ 1. cell body is intact◦ 2. Schwann cells are functional◦ 3. Scar tissue has not occurred
Regrowth of damaged axons called sprouting1. Collateral (presynaptic death)2. Regenerative (postsynaptic death)
Axonal injury in the PNS

1. Collateral sprouting

2. Regenerative sprouting

Functional regeneration of axons occurs more frequently in PNS than CNS
Nearly complete lack of neurogenesis in CNS due to ◦ (1) inhibitory influences from glial cells (oligodendrocytes)
Possibly mechanism that stops axonal growth in development once target region is reached? (see Development lecture)
◦ (2) absence of nerve growth factor (NGF) by Schwann cells 1-1.5mm growth per day Problematic when new innervation is inappropriate
(e.g., wrong muscle)◦ Unintended movements named synkinesis usually short-
lived
Regeneration

Same processes after SCI and TBI◦ Axonal retraction◦ Wallerian degeneration (WD)◦ Central chromatolysis
In CNS most damage occurs hours/days afterwards, due to cellular cascade:◦ Increased permeability of axons◦ Dysregulation of Na+-Ca2+ channels
causing influx of Ca2+
Ca2+ influx -> swelling/breaking/chromatolysis/WD This causes diffuse axonal injury/disconnection
Axonal Injury in the CNS
SCI: Spinal cord injuryTBI: Traumatic brain injury

Glial scars form physically preventing axonal regeneration
Astrocytes and microglia release growth-inhibiting factors (Nogo)
Oligodendrocytes have no NGF, but Nogo instead!
Animal tests have shown that administering a Nogo inhibitor after injury improves sprouting and functioning
There is no regeneration in CNS!

Mechanisms for recovery in CNS:1. Recovery of synaptic effectiveness2. Denervation hypersensitivity3. Synaptic hypereffectiveness4. Unmasking of silent synapses
Synaptic changes after injury

Swelling that produced pressure on presynaptic cell resolves and normal transmission is resumed
1. Recovery of Synaptic Effectiveness
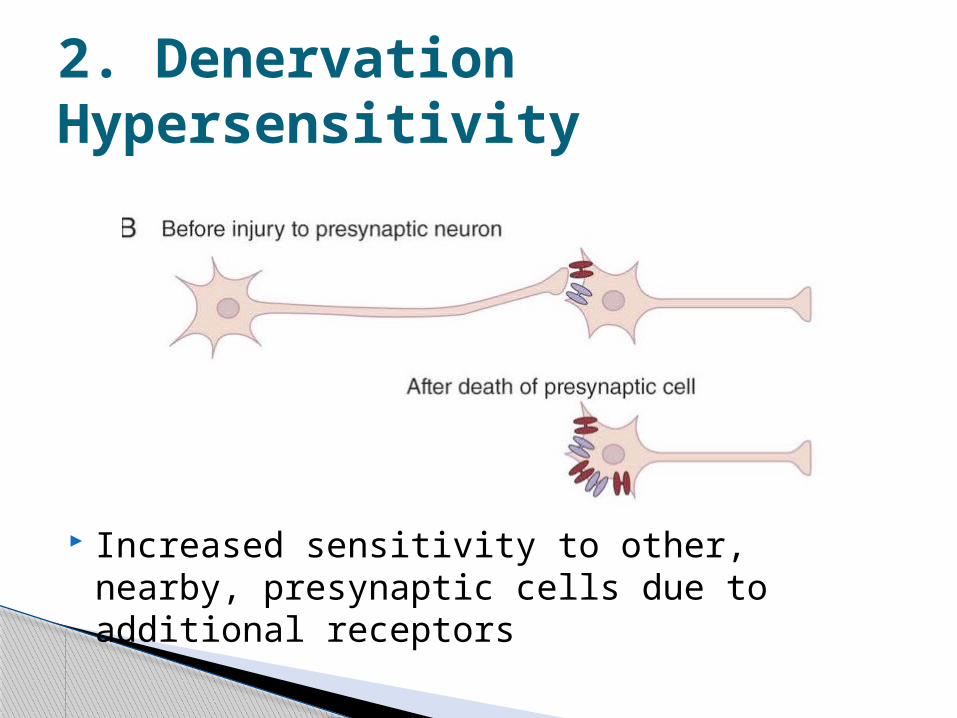
Increased sensitivity to other, nearby, presynaptic cells due to additional receptors
2. Denervation Hypersensitivity

Larger than normal amounts of neurotransmitter released to remaining synapse
3. Synaptic Hypereffectiveness

Unused synapses are lurched into action!
4. Unmasking of Silent Synapses

Cortical maps can be modified by experience◦ E.g., violinists have enlarged finger representations for
the left hand fMRI studies document functional recovery after
stroke. ◦ Activity in somatosensory cortex shifts to more bilateral
after stroke and then back to lateralised as recovery progresses
Reorganisation seen in deaf and blind individuals. ◦ Cochlear implants after age 7 activate non-usual
cortical areas. ◦ Congenitally blind ppl use occipital cortex for reading
Braille and memory
Functional Reorganisation

Intensity and time between injury and rehab influence recovery
Prolonged inaction promotes adjacent loss of cells/function◦ Rat study: “rehab” 5 or 30 days post lesion◦ 5 day group used impaired forelimb twice as well
as 30 day group Task-specific rehab better
◦ Constraint-induced movement therapy (functional arm constrained in sling) shown to be better behaviourally and through imaging
Effects of Rehabilitation