lecture 4 renal handling of sodium, chloride and water “the core of renal physiology”
TRANSCRIPT

Lecture 4RENAL HANDLING OF SODIUM, CHLORIDE AND WATER “the core of renal physiology”

► Maintaining salt (NaCl) and H20 balance is a key function of the kidney.
► Na+, Cl- and H20 are all freely filtered.
AND….huge amounts of these are filtered. AND….most of what’s filtered is
reabsorbed
Note: Na, Cl & H20 are not normally secreted
Some Generalizations:
Na+ Reabsorption is active, via the transcellular route and is powered by thebasolateral Na-K-ATPase.
Cl- Reabsorption is passive (paracellular) and active (transcellular). Regardless of route, it is always coupled somehow to Na+ reabsorption. Indeed, parallel Cl- reabsorption is implied when describing Na+ reabsorption.
H20 Reabsorption is by osmosis and secondary to reabsorption of solute, particularly Na+ and those dependent on Na+ reabsorption.

Overview of Na+ Reabsorption along the Nephron
65% of filtered Na+ is reabsorbed from the proximal tubule.25% of filtered Na+ is reabsorbed from the thick ascending limb.5% of filtered Na+ is reabsorbed from the distal tubule.4-5% of filtered Na+ is reabsorbed from the collecting duct.

Proximal Tubule: Na+ Reabsorption
NaNa++ Reabsorption Stepwise Reabsorption Stepwise::
● 1. Na-K-ATPase keeps intracellular Na level low. This means there is a gradient across apical membrane.
● 2. Filtered Na+ is transported across apical membrane several ways.
● 3. Na+ entering the cell is then moved across basolateral membrane.
Important Points: * Reabsorption of other solutes are linked to Na+ reabsorption.
** Without the Na-K-ATPase, the Na+
gradient that powers reabsorption of Na & other solutes would not exist.
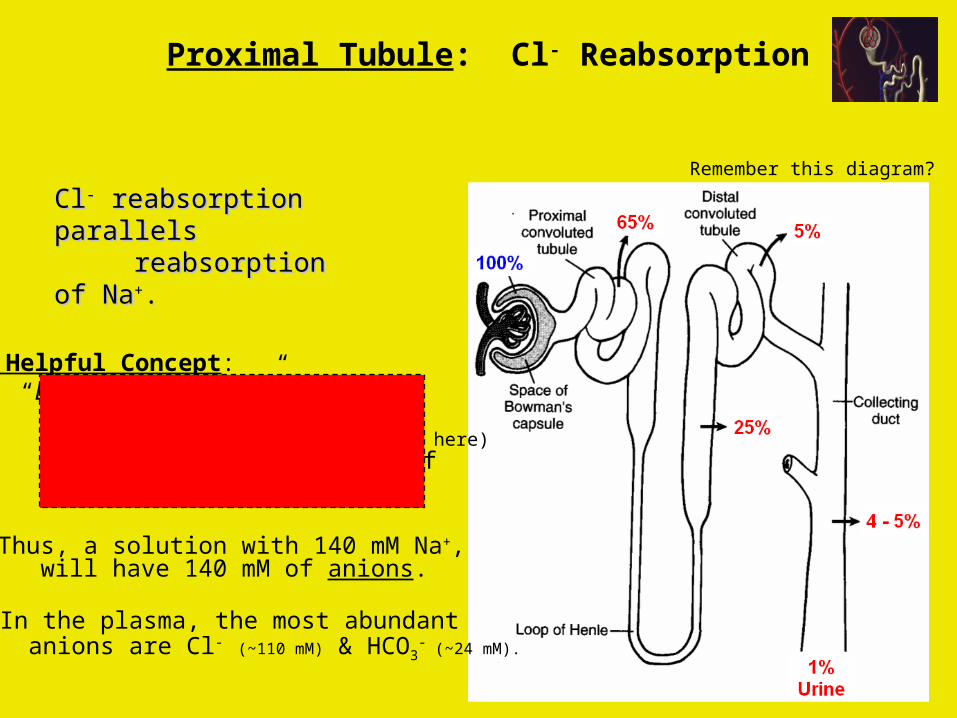
ClCl-- reabsorption parallels reabsorption parallels reabsorption of Nareabsorption of Na++..
Remember this diagram?
A Helpful Concept: “Electronuetrality Rule” any volume of solution (no membranes separating stuff here) will have equal numbers of cations and anions.
►Thus, a solution with 140 mM Na+, will have 140 mM of anions.
► In the plasma, the most abundant anions are Cl- (~110 mM) & HCO3
- (~24 mM).
Proximal Tubule: Cl- Reabsorption

Proximal Tubule: Cl- Reabsorption
Two Routes of ClTwo Routes of Cl-- Reabsorption Reabsorption::
1. Paracellular
2. Transcellular

Two Routes of ClTwo Routes of Cl-- Reabsorption Reabsorption::
1. Paracellular Through “not so tight” tight junctions
Passive, down electrochemical gradient Depends indirectly on Na+ transport Most Cl- reabsorption via this route
2. Transcellular
Proximal Tubule: Cl- Reabsorption

Complicated apical process whichdepends directly on Na+ transport
Apical transport is essentiallyCl-Na-symport
Basolateral transport via theCl-K-symporter
Two Routes of ClTwo Routes of Cl-- Reabsorption Reabsorption::
1. Paracellular Through “not so tight” tight junctions
Passive, down electrochemical gradient Depends indirectly on Na+ transport Most Cl- reabsorption via this route
2. Transcellular
Proximal Tubule: Cl- Reabsorption

H20 Reabsorption Overview
HH220 Reabsorption0 Reabsorption is by osmosis and secondary to reabsorption of solute. is by osmosis and secondary to reabsorption of solute.
Kidney’s must be able to “separate salt from H20”. Obvious but important.
If you drink excess H20 (no salt), then your kidneys must excrete the excess H20. If you eat excess salt (no H20), then your kidneys must excrete the excess salt.
Evidence that the kidney’s do this is the body’s capacity to generate dilute or concentrated urine.

Comparison of H20 and Na+ Handling
Four Significant PointsFour Significant Points:: 1. Equal amounts of H20 & Na+ are reabsorbed from proximal tubule. 2. H20 & Na+ are both reabsorbed from loop of Henle, but from different parts of the loop. Overall, the loop reabsorbs more Na+ than H20. 3. Na+ is reabsorbed from the distal tubule. H20 is not. 4. Both Na+ and H20 are reabsorbed from collecting duct. The amounts of each are variable & controlled.

What defines when and where H20 moves along the nephron?
Answer: H20 moves only down osmotic gradients (no H20 pumps here) H20 moves only if it can (a H20 permeable pathway must exist)
The Osmotic Gradients
Proximal Tubule: Na+ & Na-dependent solute reabsorption creates gradient Loop & Collecting Duct: High salt (NaCl) and urea levels in medulla provide gradient
Possible H20 Permeation Pathways
H20 may move through lipid bilayers, aquaporins or tight junctions.
Basolateral membranes: always highly H20 permeable because they containa certain type of aquaporin.
Apical membrane & tight junction: H20 permeability vary along the nephron.
Distal Tubule Zero “Collecting Duct Low, but regulated “
Ascending Limb Zero “Descending Limb High “Proximal Tubule High Apical H20 Permeability

CortexMedulla
HighSoluteLevel
What happens when H20 permeability of collecting duct is very low?
Dilute tubular fluid moves down collecting duct and remains dilute.
H20PermLow
TubularFluid Dilute
Here
Overview of “Urine Concentration” Control

Overview of “Urine Concentration” Control
CortexMedulla
HighSoluteLevel
▼Result
dilute urine
What happens when H20 permeability of collecting duct is very low?
Dilute tubular fluid moves down collecting duct and remains dilute.
H20PermLow
TubularFluid Dilute
Here

CortexMedulla
HighSoluteLevel
H20PermHigh
TubularFluid Dilute
Here
What happens if H20 permeability of collecting duct is high?
High solute level in medulla means there is a large osmotic gradient that favors H20 movement out. H20 moves out of tubular fluid and the fluid becomes more concentrated.
Overview of “Urine Concentration” Control

Preview of “Urine Concentration” Control
CortexMedulla
HighSoluteLevel
H20PermHigh
TubularFluid Dilute
Here
What happens if H20 permeability of collecting duct is high?
High solute level in medulla means there is a large osmotic gradient that favors H20 movement out. H20 moves out of tubular fluid and the fluid becomes more concentrated.
▼Result
Concentrated Urine (H20 was conserved)
Key Points to Remember (so far):1) H20 is moving down osmotic gradient.2) It only moves if there is a H20 permeable
pathway available.3) How much H20 moves will depend on….
- Gradient size - Degree of H20 permeability.

Na+, Cl- and H20 Handling Variesin Different Renal Segments
Proximal Tubule … There is “iso-osmotic” reabsorption
Loop of Henle … There is “separation of salt & H20”
Distal Tubule & … Reabsorption is “regulated” (by
hormones)Collecting Duct

“Isosmotic reabsorption” from PROXIMAL TUBULE
→ Proximal Tubule is in the cortex
→ The interstitium of the cortex is iso-osmotic to plasma
This figure was shown earlier.All GlucoseReabsorbed
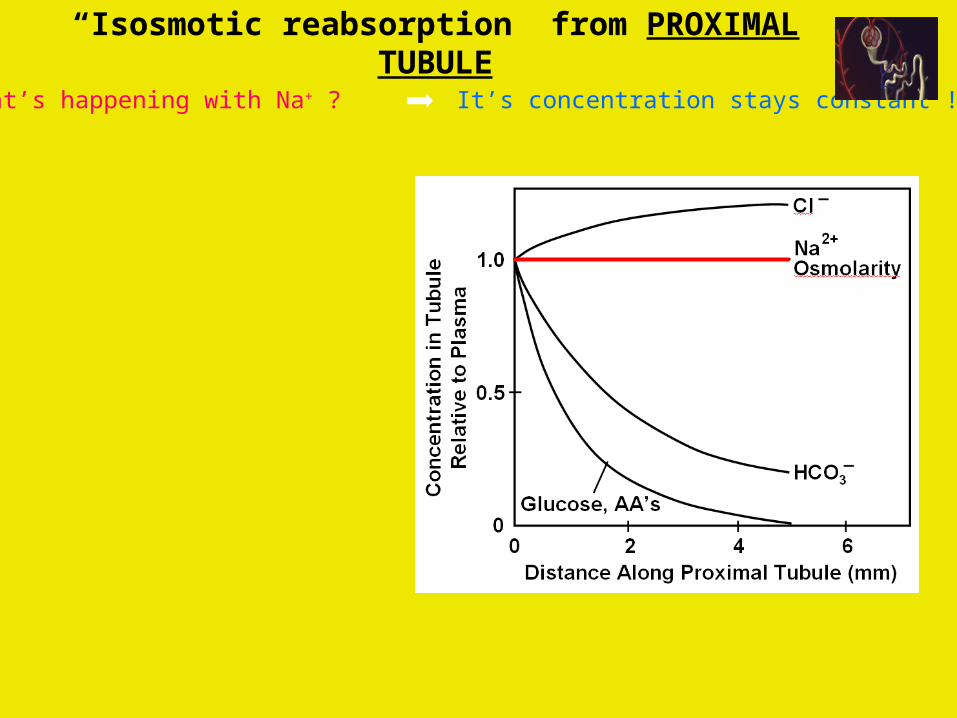
What’s happening with Na+ ? It’s concentration stays constant !
“Isosmotic reabsorption” from PROXIMAL TUBULE

Clearly, Na+ is being reabsorbed.
Na+ reabsorption is what drives reabsorption of HC03
-
and the nutrients.
Na+ concentration inside the tubulestays constant because H20 isalso reabsorbed along the tubule. (i.e. fluid volume decreases)
VOLUME
This is called…. “Isosmotic Volume Reabsorption”
H20 always follows solute….the main extracellular solute is Na+.When ever a little Na+ moves, a little H20 follows it.In other words, Na+ & H20 reabsorption keep pace….osmolarity & [Na+] stay constant
as tubular fluid volume decreases.
What’s happening with Na+ ? It’s concentration stays constant !
“Isosmotic reabsorption” from PROXIMAL TUBULE

Cl- is also being reabsorbed….
So…Why does Cl- level rise?
VOLUME
Cl- level rises because… Early on: HC03
- is the primary anion following the cations.
Later : HC03- levels drop & Cl-
starts following the cations.
►Remember, Cl- is reabsorbedpassively via the paracellular route.
Cl- level levels out later along the proximal tubule.This means Cl- and H20 reabsorption are matching
each other later on in proximal tubule.
What’s happening with Cl- ? It’s concentration rises !
“Isosmotic reabsorption” from PROXIMAL TUBULE

Important Fact: The The LoopLoop ( ( the loop overall the loop overall ) ) alwaysalways reabsorbs more Na reabsorbs more Na++ than H than H220.0. This means that the fluid leaving the loop is always more dilute
than the fluid that entered it.
Same diagram as before:
1. Na+ & H20 reabsorption physically separated (in different loop segments)
2. H20 reabsorbed from descending limb.
3. Na+ reabsorbed from ascending limb (thick
ascending limb)
Loop of Henle Separates Salt & H20
1st
2nd
3rd
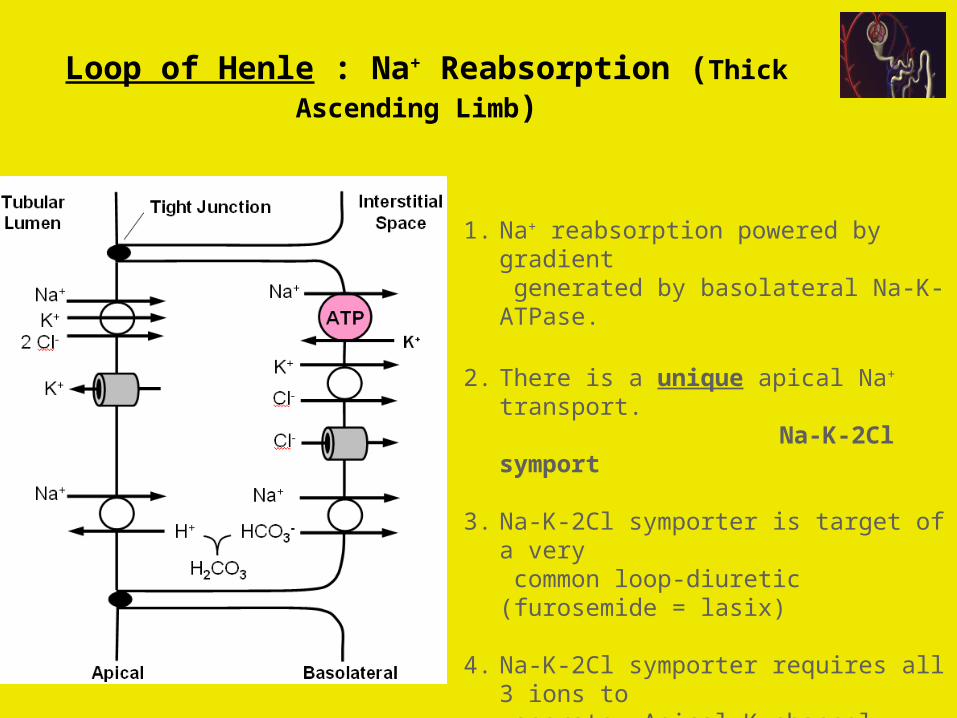
1. Na+ reabsorption powered by gradient generated by basolateral Na-K-ATPase.
2. There is a unique apical Na+ transport. Na-K-2Cl symport
3. Na-K-2Cl symporter is target of a very common loop-diuretic (furosemide = lasix)
4. Na-K-2Cl symporter requires all 3 ions to operate. Apical K channel assures there will be lumenal K available to keep it going.
Loop of Henle : Na+ Reabsorption (Thick Ascending Limb)

*Like ascending limb of loop, distal tubule is not permeable to H20 but Na+ reabsorption occurs
Distal Tubule : Na+ Reabsorption
1. Na+ reabsorption powered by gradient generated by basolateral Na-K-ATPase.
2. Another unique apical Na+ transport. Na-Cl symport
3. Na-Cl symporter is the target of another type of diuretic (thiazide)
4. Note presence of apical Ca channels.Parathyroid hormone regulates these.
(more later about this)

Two Types of Cells Present
→→ Principal cellsPrincipal cells (70% of total cells present) are specialized to handle Na+ & H20.
→→ Intercalated cellsIntercalated cells (2 subtypes called / or A/B) are specialized to handle Cl- & pH.
1. Again…Na+ reabsorption powered by the basolateral Na-K-ATPase.
2. Another unique apical Na+ transport a Na+ channel(These are not like the Na
channels associated with the AP.)
3. This Na+ channel is regulated by thehormone aldosterone.
4. Several diuretics also target this Na+
channel or its aldosterone regulation. (more about this later)
Collecting Duct : Na+ Reabsorption
Now a closer look

Here is another view of the Principal Cell.
1. The H20 permeability of collectingduct is inherently very low but can bevery high if Antidiuretic Hormone (ADH) is present. (ADH = vasopressin)
2. ADH is a peptide hormone released from posterior pituitary. It acts on the
apical membranes of principal cells. (again, more about this later)
Collecting Duct : Na+ & H20 Reabsorption

FirstFirst…… Collecting duct is only site in the nephronwhere H20 permeability is hormonally regulated.ADH increases H20 permability. (normally its very low)
SecondSecond……Collecting duct of inner medulla is a little bitdifferent. Even in absence of ADH, it has somesmall amount of H20 permeability. So, some H20will always be reabsorbed there.
ThirdThird…… ADH action is not all-or-none. A little ADH increasesH20 permeability a little. More ADH increases it more.
FourthFourth…… ADH increases apical H20 permeability by stimulating fusion of aquaporin-containingmembrane vesicles. In absence of ADH, these are withdrawn by endocytosis.
Question #1: What happens to the tubular fluid if no ADH is present?
Collecting duct H20 permeability is low. A large volume dilute urine will be excreted.
Collecting Duct : Na+ & H20 Reabsorption
Important Points to Remember:

FirstFirst…… Collecting duct is only site in the nephronwhere H20 permeability is hormonally regulated.ADH increases H20 permability. (normally its very low)
SecondSecond……Collecting duct of inner medulla is a little bitdifferent. Even in absence of ADH, it has somesmall amount of H20 permeability. So, some H20will always be reabsorbed there.
ThirdThird…… ADH action is not all-or-none. A little ADH increasesH20 permeability a little. More ADH increases it more.
FourthFourth…… ADH increases apical H20 permeability by stimulating fusion of aquaporin-containingmembrane vesicles. In absence of ADH, these are withdrawn by endocytosis.
Important Points to Remember:
Question #2: What happens to the tubular fluid when ADH is present?
Collecting duct H20 permeability is high. A small volume concentrated urine will be excreted.
Collecting Duct : Na+ & H20 Reabsorption

Origin of the Hyperosmotic Renal MedullaOrigin of the Hyperosmotic Renal Medulla

Origin of the Hyperosmotic Renal Medulla
Medulla is hyperosmotic but there is also an
osmolarity gradient.
CortexMedulla
mOsM
300400500600700800900
10001100120013001400

The 3 Essential ElementsThe 3 Essential Elements::1) Active Na+ transport in thick ascending limb of loop. ( Overall, the loop always reabsorbs more Na+ than H20 )
CortexMedulla
mOsM
300400500600700800900
10001100120013001400
Na
NaNaNaNa
NaNa
H20H20H20H20H20
CountercurrentMultiplication
H20 reabsorbed
Na+
reabsorbed
Origin of the Hyperosmotic Renal Medulla

The 3 Essential ElementsThe 3 Essential Elements::1) Active Na+ transport in thick ascending limb of loop. ( Overall, the loop always reabsorbs more Na+ than H20 )
2) Unique arrangement of medullary peritubular capillaries.
( The vasa recta loop down into the renal medulla)
CortexMedulla
mOsM
300400500600700800900
10001100120013001400
Vasa RectaBlood Osmolarity
IN = OUTHair-pin looparrangementpreserves medullaryosmolarity
Origin of the Hyperosmotic Renal Medulla

The 3 Essential ElementsThe 3 Essential Elements::1) Active Na+ transport in thick ascending limb of loop. ( Overall, the loop always reabsorbs more Na+ than H20 )
2) Unique arrangement of medullary peritubular capillaries.
( The vasa recta loop down into the renal medulla )
3) Recycling of urea between loop and collecting duct. ( Urea provides about half of the high medullary osmolarity )
CortexMedulla
mOsM
300400500600700800900
10001100120013001400
Origin of the Hyperosmotic Renal Medulla
UreaRecycling
Urea Recycling: Keeps “dumping” urea (solute) back into medulla.
Rate of “dumping” depends on urea level in the tubular fluid (faster when higher).

Tubular Fluid Osmolarity Changes along Nephron
Percent filteredH20 Remaining
Hypo-osmoticto plasma
Approaches osmolatity of interstitium in cortex
Approaches osmolatity of interstitium in medulla
Iso-osmoticto plasma Dilute
urine
Conc.urine

Panel from Sistine Ceiling showing God Separating Earth from Waters (1511) by Michelangelo (a). Computer-assisted removal of the figures showing kidney shaped mantle of the Creator (b). Color highlighted version of (b) to demonstrate the vessels and ureter of the kidney (c). Reproduction of a medical illustration of the normal kidney (d) in which the ureter is shown in its normal course downward from the kidney. In the figure by Michelangelo, it is likely that the ureter is shown extended below the kidney and protruding at the left upper corner beyond the outline of the mantle (a). That would be the position of the empty ureter if the kidney were hurled at the viewer or traversing at high speed through space. Reproduced with permission from the Vatican Museum.

Renal Physiology Quiz for Lecture 4:
Note that this and other Renal Physiology quizzes are simply provided to you to help you self-test your understanding of each lecture. They are not a substitute for studying the other learning
materials presented to you. These questions are not intended to reflect the style or level of difficulty of questions on the Final Exam.

True/False Questions:1. About 99% of filtered Na+ is reabsorbed from the tubular fluid and most of this
reabsorption occurs from the proximal tubule. T 2. Reabsorption of Na+ from all tubular segments is ultimately dependent on
basolateral Na-K-ATPase activity. T3. Reabsorption of Cl- from all tubular segments occurs only along the transcellular
route. F4. The tubular fluid is hypo-osmotic (relative to plasma) when it leaves the loop of
Henle. T 5. Na+ is transported across the apical membrane of cells in the distal tubule by the
Na-K-2Cl symporter. F 6. Na+ is reabsorbed from the collecting duct by principal cells. T 7. Antidiuertic hormone (ADH) causes the water permeability of the collecting duct
to decrease. F 8. The cortex of the kidney is very hyperosmotic compared to the plasma. F

Multiple Choice Questions
9. When the body is conserving water, roughly half of the osmolality of the interstitial fluid in the inner medulla (in the presence of ADH) is usually accounted for by:
a. Urea b. Na+ c. K+ d. NH4+ e. none of the above10. Which of the following correctly describes the descending loop of Henle (DLH) and the ascending
loop of Henle (ALH): a. Na+ is reabsorbed from the DLH but not in the ALH b. Water is can easily cross the epithelial layer of the ALH but not of the DLH c. Cl- is reabsorbed from the DLH but not in the ALH d. The tubular fluid entering the DLH is hyper-osmotic (with respect to plasma) and the tublular fluid leaving the ALH is isotonic e. None of the above statements are correct11. Which of the following correctly describes renal urea recycling. a. Urea recycling occurs in the renal cortex. b. During urea recycling, urea is secreted into the proximal tubule and reabsorbed from distal tubule. c. During urea recycling, urea is secreted into the ascending limb of the loop of Henle and reabsorbed from the collecting duct. d. Urea recycling involves active and passive transport of urea. e. a and b are both correct12. Iso-osmotic H20 and Na+ reabsorption occurs in which of the following tubular segments: a. proximal tubule b. descending limb of the loop of Henle c. collecting duct d. b and c are both correct e. none of the above are correct

Microscopy of kidney tissue showing tubules. One tubule is highlighted to show epithelial cells (blue), cell nuclei (green) and the tubule lumen (dark center).