lecture 22 cancer genetics ii: inherited susceptibility to cancer stephen b. gruber, md, phd...
TRANSCRIPT

Lecture 22Cancer Genetics II:
Inherited Susceptibility to Cancer
Stephen B. Gruber, MD, PhD
November 19, 2002

Cancer Genetics: IISummary
• Inherited susceptibility to cancer due to germline mutations• Causes of inherited susceptibility to colorectal cancer• Familial Adenomatous Polyposis• Hereditary Non-Polyposis Colorectal Cancer
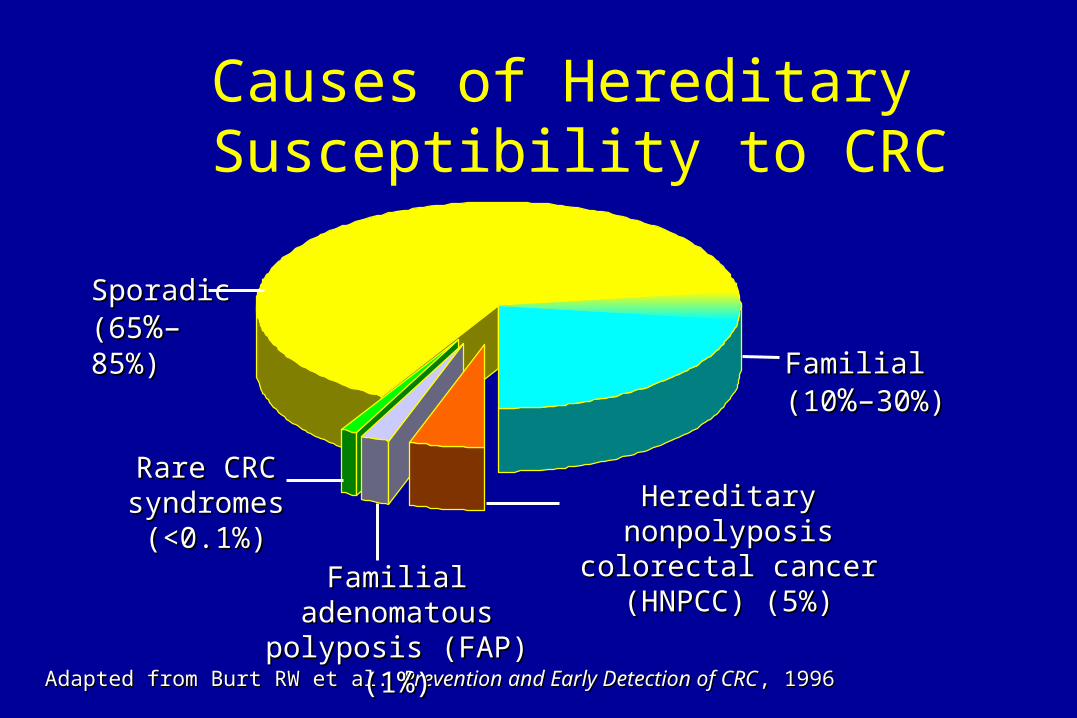
Causes of Hereditary Susceptibility to CRC
Adapted from Burt RW et al. Adapted from Burt RW et al. Prevention and Early Detection of CRCPrevention and Early Detection of CRC, 1996, 1996
Sporadic Sporadic (65(65%–%–85%)85%)
Familial Familial (10(10%–%–30%)30%)
Hereditary nonpolyposis Hereditary nonpolyposis colorectal cancer colorectal cancer (HNPCC) (5%)(HNPCC) (5%)Familial adenomatous Familial adenomatous
polyposis (FAP) (1%)polyposis (FAP) (1%)
Rare CRC Rare CRC syndromes syndromes
(<0.1%)(<0.1%)

Multi-Step Carcinogenesis
Normal Normal epitheliumepithelium
Hyper-Hyper-proliferativeproliferativeepitheliumepithelium
EarlyEarlyadenomaadenoma
LateLateadenomaadenoma CarcinomaCarcinoma MetastasisMetastasis
Loss ofLoss ofAPCAPC
ActivationActivationof K-rasof K-ras
Loss ofLoss of18q18q
Loss ofLoss ofTP53TP53
Other Other alterationsalterations
Adapted from Fearon ER. Adapted from Fearon ER. CellCell 61:759, 1990 61:759, 1990
Inter-Inter-mediatemediate
adenomaadenoma
ASCO

Risk of Colorectal Cancer (CRC)
0 20 40 60 80 100
General populationGeneral population
Personal history of Personal history of colorectal neoplasiacolorectal neoplasia
Inflammatory Inflammatory bowel diseasebowel disease
HNPCC mutationHNPCC mutation
FAPFAP
6%6%
15%–20%15%–20%
15%–40%15%–40%
70%–80%70%–80%
>95%>95%
Lifetime risk (%)Lifetime risk (%)
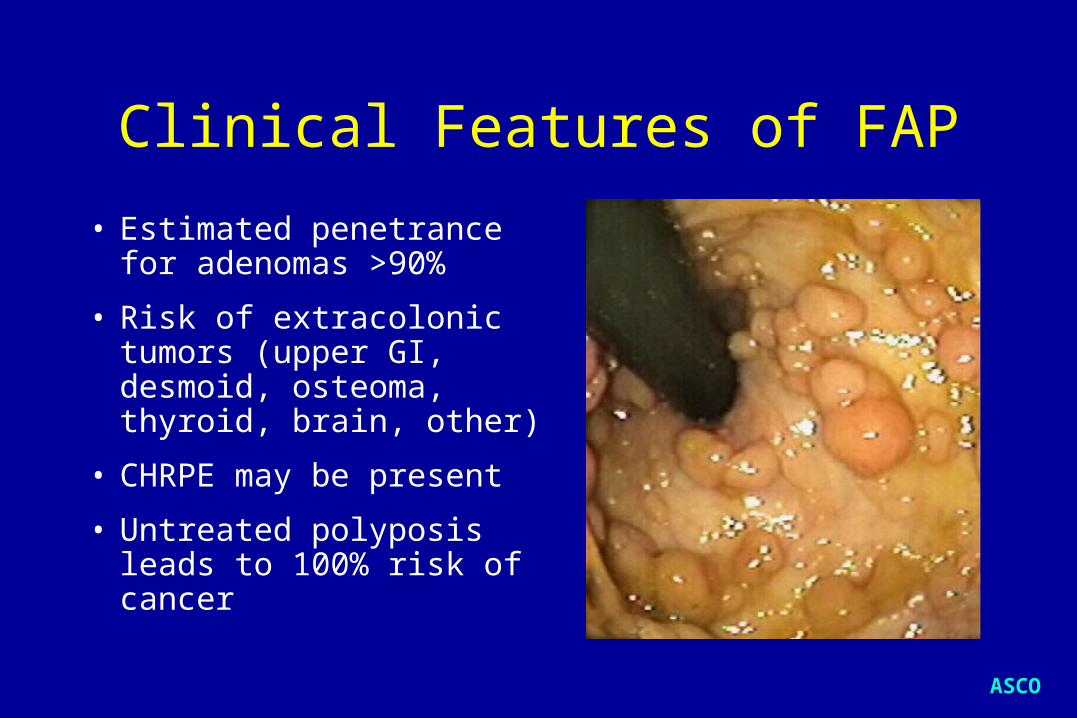
Clinical Features of FAP
• Estimated penetrance for adenomas >90%
• Risk of extracolonic tumors (upper GI, desmoid, osteoma, thyroid, brain, other)
• CHRPE may be present
• Untreated polyposis leads to 100% risk of cancer
ASCO

Some FAP Manifestations Correlate
With Specific APC Gene Regions
Attenuated FAPAttenuated FAPClassic FAPClassic FAPCHRPECHRPE
1 2 3 4 5 6 7 8 9 10111213 14 15
5'5' 3'3'

Attenuated FAP
ASCO
• Later onset (CRC ~age 50)Later onset (CRC ~age 50)
• Fewer colonic adenomasFewer colonic adenomas
• Not associated with CHRPENot associated with CHRPE
• UGI lesionsUGI lesions
• Associated with mutations at Associated with mutations at 5' and 3' ends of 5' and 3' ends of APCAPC gene gene

Clinical Features of HNPCC• Early but variable age at
CRC diagnosis (~45 years)
• Tumor site in proximal colon predominates
• Extracolonic cancers: endometrium, ovary, stomach, urinary tract, small bowel, bile ducts, sebaceous skin tumors
Amsterdam Criteria 33 or more relatives with verified CRC in family or more relatives with verified CRC in family
- - One case a first-degree relative of the other twoOne case a first-degree relative of the other two 22 or more generations or more generations 11 CRC by age 50 CRC by age 50 FAP excludedFAP excluded
Vasen HFA et al. Vasen HFA et al. Dis Colon RectDis Colon Rect 34:424, 1991 34:424, 1991
Failure to meet these criteria Failure to meet these criteria does does notnot exclude HNPCC exclude HNPCC
Genetic Features of HNPCC
• Autosomal dominant inheritance
• Penetrance ~80%
• Genes belong to DNA mismatch repair (MMR) family
• Genetic heterogeneity (MLH1, MSH2, MSH6, PMS1, PMS2)

Genetic Heterogeneity in HNPCC
HNPCC is associated with germline mutations HNPCC is associated with germline mutations in any one of at least five genesin any one of at least five genes
Chr 2Chr 2Chr 3Chr 3
Chr 7Chr 7
MSH2MSH2
PMS1PMS1
MLH1MLH1PMS2PMS2
MSH6MSH6
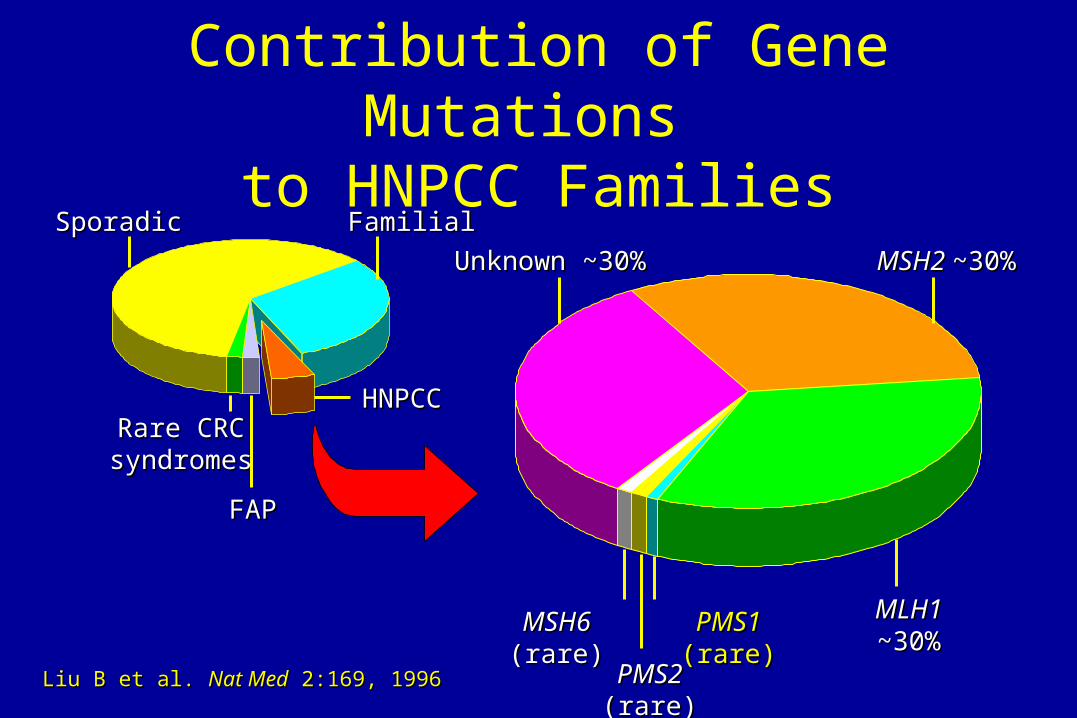
Contribution of Gene Mutations to HNPCC Families
MSH2 MSH2 ~30%~30%
MLH1MLH1~30%~30%
PMS1 PMS1 (rare)(rare)
PMS2PMS2 (rare) (rare)
MSH6 MSH6 (rare)(rare)
Unknown ~30%Unknown ~30%
SporadicSporadic FamilialFamilial
HNPCCHNPCC
FAPFAP
Rare CRC Rare CRC syndromessyndromes
Liu B et al. Liu B et al. Nat MedNat Med 2:169, 1996 2:169, 1996

Cancer Risks in HNPCC
Aarnio M et al. Aarnio M et al. Int J CancerInt J Cancer 64:430, 1995 64:430, 1995
% with % with cancercancer
100100
8080
6060
4040
2020
002020 4040 6060 808000
Age (years)Age (years)
Colorectal 78%Colorectal 78%
Endometrial 43% Endometrial 43%
Stomach 19%Stomach 19%Biliary tract 18%Biliary tract 18%Urinary tract 10%Urinary tract 10%Ovarian 9%Ovarian 9%
ASCO

HNPCC Results From Failure of Mismatch Repair (MMR) Genes
Base pair Base pair mismatchmismatch
Normal DNA Normal DNA repairrepair
Defective DNA Defective DNA repair (MMR+)repair (MMR+)
TT CC TT AA CC
A G C T GA G C T G
T C G A CT C G A C
A G C T GA G C T G
TT CC TT AA CC
A G C T GA G C T G A G A G AA T GT G
T C T C TT A C A C

Structure of Mismatch Repair
Obmolova G, Nature 407;703, 2000Lamers et al, Nature 407;711, 2000

Mismatch Repair Failure Leads to Microsatellite Instability (MSI)
NormalNormal
Microsatellite Microsatellite instabilityinstability Addition of Addition of
nucleotide repeatsnucleotide repeats
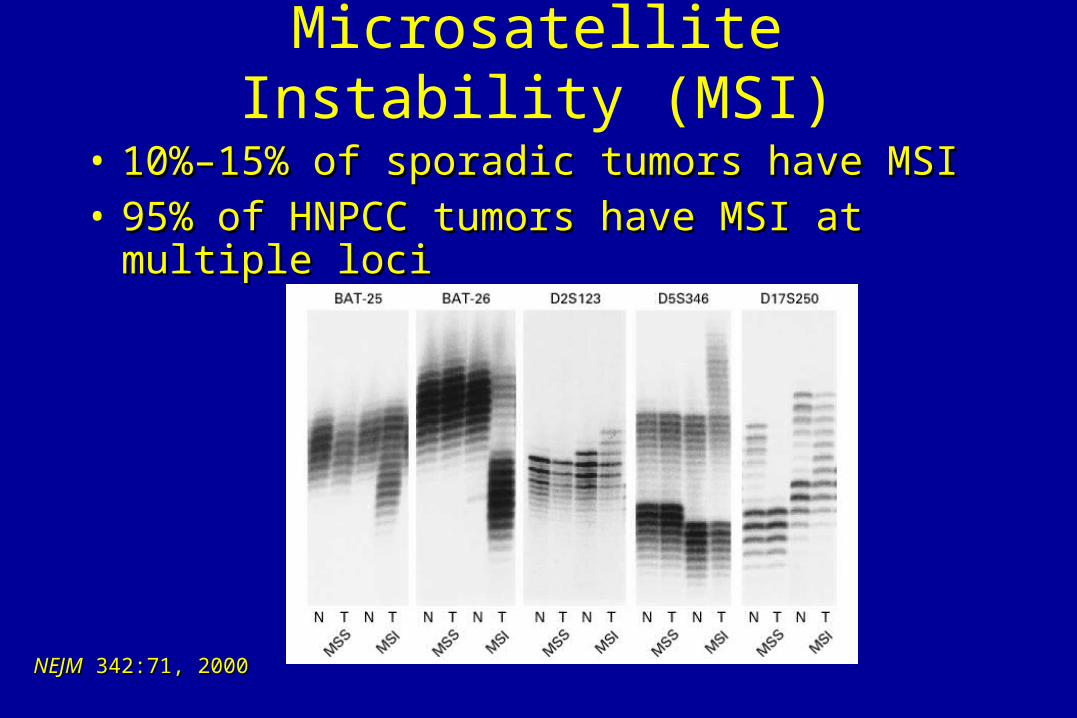
NEJMNEJM 342:71, 2000 342:71, 2000
Microsatellite Instability (MSI)
• 10%–15% of sporadic tumors have MSI10%–15% of sporadic tumors have MSI• 95% of HNPCC tumors have MSI at multiple loci95% of HNPCC tumors have MSI at multiple loci

Surveillance Options for Carriers of HNPCC-Associated Mutations
Cancer Genetics Studies Consortium Task Force RecommendationsCancer Genetics Studies Consortium Task Force RecommendationsModified from Burke W et al. Modified from Burke W et al. JAMAJAMA 277:915, 1997 277:915, 1997
InterventionIntervention
ColonoscopyColonoscopy
• Transvaginal Transvaginal ultrasound ultrasound
• Endometrial aspirateEndometrial aspirate
RecommendationRecommendation
Begin at age 20–25, Begin at age 20–25, repeat every 1–2 yearsrepeat every 1–2 years
Annually, starting at Annually, starting at age 25–35age 25–35
MalignancyMalignancy
Colorectal cancerColorectal cancer
Endometrial cancerEndometrial cancer

Surveillance Reduces Risk of Colorectal Cancer in HNPCC Families
Jarvinen HJ et al. Jarvinen HJ et al. GastroGastro 108:1405, 1995 108:1405, 1995
% of % of subjects subjects
with CRCwith CRC
3030
2020
1010
4.5%4.5%
11.9%11.9%
00 33 66 99Years of follow-upYears of follow-up
SurveillanceSurveillanceNoNo surveillancesurveillance
00
ASCO

Surveillance Improves HNPCC Survival
9
0.6
0.7
0.8
0.9
1.0
0.5
3 6 12 150
Jarvinen H et al Gastroenterology 118;829, 2000Jarvinen H et al Gastroenterology 118;829, 2000
Years of follow-upYears of follow-up
SurvivalSurvival
65% reduction in mortality
p = 0.05
SurveillanceSurveillanceNoNo surveillancesurveillance

Cancer Genetics: IISummary
• Inherited susceptibility to cancer due to germline mutations• Familial Adenomatous Polyposis• Hereditary Non-Polyposis Colorectal Cancer
– Amsterdam criteria
• Surveillance reduces the risk of cancer• Genetic counseling / testing plays an important role in the
management of families with inherited susceptibility to cancer

Special thanks to David Barrett
Please check out his latest CD, “It’s a long, long story”www.DavidBarrett.com
or in concert at the Greenwood Café Acoustic Series
December 6, 7:30pm