leading to quality - south west yorkshire partnership nhs ... · maggie bell, assistant director...
TRANSCRIPT

Participants Bradford District Care TrustHumber NHS Foundation TrustLeeds and York Partnership NHS Foundation TrustNAViGORotherham Doncaster and South Humber NHS Foundation TrustSouth West Yorkshire Partnership NHS Foundation Trust
AuthorsProfessor Beverly Alimo-MetcalfeMargaret BradleyDr John Alban-MetcalfeAlice Locker
Leading to QualityAn investigation of the impact of leadership and team working on staff morale and wellbeing, and team performance, among mental health teams within the Yorkshire and the Humber Strategic Health Authority.
March 2013
Leading toquality
Leading toquality

© Leading to Quality 2013 – All rights reserved
Contents
Page Foreward 1
Acknowledgements 2
Executive Summary 3
Chapter 1 Background to the Study and Relevant Literature 11
Chapter 2 Methodology 28
Chapter 3 Service User and Carer Constructs of High Quality Care 33
Chapter 4 Relationship between Team Leadership and Team Working, and Team Process Outcomes and Impact on Team Members
49
Chapter 5 Case Study Data and Analysis 67
Chapter 6 Discussion and Practical Application 104
References 120
Appendix 1.1 The I-M-O-I model of team working 126
Appendix 2.1 Instructions on using Repgrid Technique to elicit constructs of effective care
130
Appendix 2.2 Demographic/biographical data of sample for the EngagingTeams360
133
Appendix 3.1 Themes from service user and carer interviews on effective care 135
Appendix 3.2 Comparison of NICE Quality Standard for Service User Experience in Adult Mental Health and Service Users’ & Carers’ constructs of ‘high quality care’
139
Appendix 4.1 The reliability of the EngagingTeams360 142
Appendix 4.2 Results of the EngagingTeams360in rank order 143
Appendix 4.3 Structural Equation Modelling 144
Appendix 4.4 Correlations 148
Appendix 4.5 Correlations (cont’d) 149
Appendix 4.6 Discriminant Function Analysis by item 150
Appendix 4.7 The effect of team size 152
Appendix 4.8 Effect of ratio of occupational therapists and social workers to nurses 156
Appendix 4.9 Effect of case load size 158
Service User and Carer Quality of Care Questionnaires 161

© Leading to Quality 2013 – All rights reserved Page 1
Foreword Leading to Quality (LTQ) is a major research project, sponsored by the Chief Executives of the 6 participating organisations, to help Trusts gain a greater understanding of the nature of the leadership challenge for community mental health services as part of the transformation agenda facing the NHS. The research was designed to explore the linkages between strong leadership, good team-working, staff engagement and positive wellbeing, which are believed to be at the heart of delivering high quality, safe and effective care and support to service users and their carers. This belief combined with a commitment from all the participating organisations to strengthening and embedding innovation and service improvement led to the commissioning of this 3 year research project. The study was aimed at informing system transformation of structures and leadership arrangements in the provision of community mental health services for adults of working age. It builds on previous research and provides a more detailed and in depth understanding of what service users and carers regard as important aspects of high quality care as well as healthcare professionals. The study reinforces and adds to those standards of care articulated in NICE guidelines and identifies enablers and barriers to good quality care provision. It examines both team leadership and team-working and offers a new evidence-based model of the relationship between these and team outcomes. Best practice case studies are summarised in the report and have been used to provide a richer understanding of the learning from the project and are a valuable reference resource. An important aspect of the project was to use learning and results from LTQ to develop a set of practical toolkits for the Trusts to use within their organisations as part of their transformation programme. I consider this study to not only have significant implications for leadership and team-working, but also organisational development and the management of change to enable us to transform services effectively and deliver the quality of service we aspire to. Finally, I would like to thank the Yorkshire and Humber Strategic Health Authority who supported the research, the members of the steering group for their commitment and input over the last 3 years and particularly Maggie Bell and Margaret Bradley who were both key to the success of the project.
Alan Davis Chair of the Leading to Quality Steering Group (Director of Human Resources and Workforce Development, South West Yorkshire Partnership NHS Foundation Trust)

© Leading to Quality 2013 – All rights reserved Page 2
Acknowledgements We would like to express our sincere gratitude to all those that have made this research possible. We warmly thank the service users and carers that gave us their time to participate in the interviews and questionnaires. Their involvement allowed us to obtain a unique perspective of the service user and carer experience. We would also like to express our heartfelt thanks to all the staff from the community teams who generously provided us with their precious time to participate in interviews and questionnaires. Their contribution allowed us to develop a greater understanding of the impact of leadership and team working in practice. The work of the Research Champions has been invaluable, and is sincerely acknowledged, including: Mark Wilbram, Priyanka Bichala, Nick Turner, Val Berry, Dave Rainforth, Joann Gibson, Lisa Connor, Julie Sheldon and Wayne Reece-Gorman. Their willingness to learn new research skills and apply these to conducting the service user and carer interviews allowed us to bridge the academic/practice divide and helped us to really understand what is important to service users and carers. The support and guidance of the Project Steering Group has been essential in providing direction for the Project and ensuring it remains relevant to the current context in the NHS. We would like to thank the members of the Steering Group who have given their time, including the service representatives from each of the participating trusts and the service user and carer representatives. We would like to thank our colleagues at South West Yorkshire Partnership NHS Foundation Trust for hosting the research on behalf of the Yorkshire and the Humber Strategic Health Authority. In particular we would like to express our sincere gratitude, and warmly thank, Maggie Bell, Assistant Director of Human Resources (Leadership, Wellbeing & Research), for her hard work and perseverance to ensure the successful running of the Project in the NHS. We would also like to thank Alan Davis, Director of Human Resources and Workforce Development, for chairing the Steering Group so effectively. We are very grateful for the input of Professor Steve Onyett and Dr Jeff Overall, researchers that contributed to the data analysis but who are not part of the core research team. Finally, we thank the Strategic Health Authority and the Chief Executives from the participating trusts for their vision in realising the importance of the research and offering their support.
Professor Beverly Alimo-Metcalfe (Principal Investigator) & the Bradford University School of Management Research Team

© Leading to Quality 2013 – All rights reserved Page 3
Executive Summary
I. Background and aims The Yorkshire and the Humber Strategic Health Authority recognises that team working and leadership are essential in the provision of high quality care, staff wellbeing and productivity. As such, they commissioned the Leading to Quality project to build on existing research to increase theoretical and practical understanding of how leadership and team working has a positive impact.
To this end, the overall aims of the Project were:
To understand how leadership behaviour enables multi-professional teams to function most effectively in working to promote and sustain improved quality of care for service users and carers;
To devise and develop a set of guidelines and developmental activities to enable mental health professionals, and others, to improve the quality of care for service users and their carers.
The study focused on community mental health teams serving working age adults across six participating trusts.
II. Methodology In brief, the methodology comprised:
1. Preliminary qualitative interviews
68 interviews with leaders of mental health teams about their experience of the nature of team working and leadership in mental health teams, and the range of contextual factors that affect provision within their team;
65 interviews with service users/carers about what good quality of care looks like from their perspective and their experiences of the quality of the service provided;
2. The design of two ‘Quality of Care Questionnaires’, one for service users and one for carers, based on the constructs of high quality care elicited from the preliminary qualitative interviews;
3. Quantitative data collection from 452 service users and 197 carers using the ‘Quality of Care Questionnaires’;
4. Quantitative data using the EngagingTeams360 from 590 mental health professionals across the Region about: team leadership, team working, and the impact of these on the team in terms of team process outcomes (Innovation; Focus on Quality, and Improvement) and Impact on Team Members (Team Engagement, and Wellbeing at Work);
5. Collecting contextual information about the teams, including: caseload size of key worker; size of team; multi-disciplinary nature of the team, age of team, and time team lead in post;

© Leading to Quality 2013 – All rights reserved Page 4
6. Six best practice case studies to obtain an in-depth understanding of leadership and team working in practice, and to look at the relationship between this and staff engagement and wellbeing, and quality of care. Forty-six interviews were conducted in total;
7. The production of a Developmental Toolkit based on the results of the research containing a series of workbooks aimed at developing team working and leadership.
III. Main Findings Service user and carer constructs of high quality of care
The preliminary qualitative interviews and analysis identified essential dimensions on which high quality care is judged and the specific behaviours of professionals that result in such care. These interviews provided a much richer, more detailed, and comprehensive understanding of what service users and carers regard as important aspects of high quality care than has previously been published. They reinforced the NICE Quality Standards (2011) and provided explicit examples of how these can be enacted in care. The interviews identified an aspect of care that is of crucial importance to service users, namely the importance of care that supports an individual’s sense of self-efficacy, which was not explicitly referred to in the NICE standards. The themes to emerge from the interviews were also consistent with the recovery model and with the Triangle of Care (Worthington & Rooney, 2012).
The Quality of Care Questionnaires
Service User Quality of Care Questionnaire
From the factor analysis of the Service User Quality of Care Questionnaire it was possible to conceptually group the questionnaire into 4 main dimensions (scales):
1. Strengthens self-efficacy and control over care: this scale assesses those aspects of MH provision that service users seek from professionals in relation to enabling them to achieve their personal goals;
2. Quality of personal relationships with the professionals: this scale describes the importance to individuals of having a relationship with professionals in which empathy, genuine concern for the individual, and openness are clearly exhibited;
3. Respect for me as a person: this scale builds on the previous two dimensions by emphasising the importance of care that is holistic in nature, and is particular to the individual and their perspectives, experiences, aspirations, and ‘whole life’ situation;
4. Aspects of delivery of care: this scale serves to emphasise that care should be provided by the most appropriate people, who tell the truth, and offer provision in a location that is convenient to the service user.
Carer Quality of Care Questionnaire
From the factor analysis of the Carer Quality of Care Questionnaire it was possible to conceptually group the questionnaire into 2 main dimensions (scales):

© Leading to Quality 2013 – All rights reserved Page 5
1. Support for carers: this scale reveals the nature of the support that carers seek from professionals and teams working with those for whom they care;
2. Respect for, and commitment to, the service user: this scale echoes the needs expressed by service users to be treated with genuine care, as an individual, about whom professionals should not make assumptions, and for whom the pursuit of their personal goals is of paramount importance. Also, in ways that strengthen their self-efficacy.
Satisfaction with quality of care
Service user satisfaction with quality of care
The analysis of the service user results showed that service users that responded to the survey felt very satisfied with the care they receive. The most positive items were in relation to personal relationships and respect for service users as people. It is interesting to note that the items that were the lowest scoring (although still positive) were the ones associated with increasing self-efficacy, which are items that are very consistent with the recovery model.
Carer satisfaction with quality of care
The results of the Carer Survey were also positive but less positive than the service user results. The most positive areas emerging from the carer questionnaire were similar to the service user questionnaire, in that carers find professionals to be approachable and communicate in a way that carers can understand. Carers also think that the person they care for is treated as an individual. Areas in which carers felt less positive were in relation to how involved in/ informed about they were in the person they care for’s care.
Quantitative data collected from teams
The results from the EngagingTeams360, which was distributed across community mental health teams in the Region, demonstrated positive levels of team leadership, team working and team engagement across the Region. However, of concern was that the mean ratings for Wellbeing at Work were the lowest out of all the areas assessed, which should be of considerable concern.
Consistent with the findings of others, team leadership and team working were significantly correlated. However, evidence indicates that, contrary to what was expected, team leadership acts through team working, rather than directly on team process outcomes (Innovation, Focus on Quality, and Improvement), and on team members (Team Engagement and Wellbeing at Work). This finding offers a new evidence-based model of the relationship between these and team outcomes and has important implications for the nature of team leadership development, and the context in which it is offered.
The findings also highlight the importance of contextual factors on team working and leadership, with team size and professional mix found to be important. This has implications for service design and organisation.

© Leading to Quality 2013 – All rights reserved Page 6
On the whole, the results:
Provide valuable information as to relative areas of strength, and those for development;
Provide important insights into specific and differential ways that team leadership and team working have an impact on team members and on team performance, and
Point to practical actions that can be taken to increase the effectiveness of MH teams.
Best practice case study findings
Effective team working
The themes to have emerged from the case studies regarding effective team working were:
An overwhelmingly strong vision and values amongst the teams to provide good quality, recovery-focused care for service users;
Effective multidisciplinary team working, allowing for a holistic, flexible and seamless service;
Positive relationships within the teams, being characterised by harmony, although with the right degree of challenge, support and respect;
Effective and engaging communication within the teams on an informal and formal level. A particularly strong theme was that there were regular team meetings, which were prioritised and valued by the teams;
All the teams, to a greater or lesser extent had a culture of innovation and improvement within the teams, where creative ideas, reflection, problem-solving, and individual and team development were encouraged. There was also a genuine commitment to development and supervision, at the individual and group level;
Relationships with other teams and agencies were generally felt to be positive. The teams try to ensure this is the case, as they recognise positive relationships are important for service user care;
The effective team working described above was considered to be key to helping the teams adapt to organisational changes.
Effective Leadership
The effective leadership displayed in the case studies orchestrated the effective team working described above. The themes to have emerged regarding effective leadership were:
Team leads were felt to be extremely passionate about providing a good quality service, consistent with their team’s values. This served to unite and motivate the teams;
© Leading to Quality 2013 – All rights reserved Page 7
In relation to the above, the team leads were considered to be inspirational by their passion and determination, strong work ethic and the way in which they acted as a role model;
The team leads displayed very similar engaging leadership styles which were characterised by: being democratic but decisive, situational leadership, open and honest, positive leadership, hands on leadership, and empowering leadership;
It was clear from all the case studies that the team leads were very focused on the team as a unit and the individuals within it. They recognised that staff were the key to working effectively and achieving the teams’ goals, and work hard to ensure that the right culture and support exists for the team to flourish;
Team leads, to a greater or lesser extent, were willing to manage performance within the team;
One of the challenges team leads faced was being able to balance the needs of the team/service with the needs of the organisation. This was something they were felt to do effectively;
The team leads’ employed a variety of approaches to managing change within the teams, which were felt to have led to the effective management of change.
Staff wellbeing and engagement
There were high levels of motivation, commitment and job satisfaction within the teams, with good intrinsic motivation, the nature of the work, team working and leadership playing a key role in this. Levels of stress were lower than the overall sample average, which was largely attributed to the team lead and the supportive relationships within the team. Factors that detracted from staff engagement and wellbeing were: difficult to engage service users, organisational changes and the perceived business culture that now exists within the health sector.
Quality of care
The teams generally felt they provided good quality care, which was due to effective team working and staff engagement, facilitated by good leadership. However, quality of care was considered to be compromised by time constraints, skills shortages (where present), and difficulties experienced with teams and services external to the teams.
On the whole, it was evident when the research team sought uniformity across trusts that there appeared to be little in the way of a systematic or uniform approach to assessing service user and carer perceptions of quality of care across the trusts.
IV. Recommendations for practice The following areas emerged from the research that would benefit from being taken forward locally, including:

© Leading to Quality 2013 – All rights reserved Page 8
1. Case studies as a source of reference: the case studies provide rich information and guidance on best practice in leadership and team working. They can be a source of reference for teams and leaders to learn from;
2. Team and leadership development: data from the analyses of the EngagingTeams360 instrument described in detail in Chapter 4 provide very clear indications of which aspects of team working significantly impact on which outcomes, and identify specific behaviours. To this end, team and leadership development that improves and promotes engaging teams and engaging leadership should be encouraged. As part of the Leading to Quality project, a team and leadership Development Toolkit is being produced that provides development materials for teams and leaders to do just this; it is recommended that teams/trusts utilise these resources. The Toolkit is based on the quantitative and qualitative findings from the research;
3. Prioritising effective and engaging communication, improvement, innovation and development: mental health teams should prioritise the time to allow the team to develop, improve and innovate;
4. The importance of Innovation, Focus on Quality, and Improvement: in relation to the above, the importance of innovation, quality and improvement have been made clear by the Department of Health (DH, 2012), which is entirely consistent with the aims of the Leading to Quality research. Given the relatively low scores for Focus on Quality, and Improvement, this should be considered carefully by teams;
5. Enhancing staff wellbeing: considering the worrying finding from the EngagingTeams360 data that team wellbeing scores were the lowest of all 21 scales, trusts should use the findings from the research to enhance wellbeing;
6. Reducing administrative demands: in relation to the above, trusts should consider if it is possible to reduce the administrative requirements placed on staff by finding the most efficient ways to collect the information required;
7. Quality of care: the findings from the Quality of Care Questionnaires has provided the participating trusts with valuable feedback from a significant number of service users and carers. The analysis has shown which aspects of care quality is highest, and which are the aspects of care that can be improved. Teams and trusts can refer to these results to identify areas where they might try and improve;
8. Collecting service user and carer feedback: on the whole, there appeared to be little in the way of a systematic or uniform approach to assessing service user perceptions of quality of care at a team level within, and between, trusts. The use of the Quality of Care Questionnaires developed from the Leading to Quality research across a range of mental health organisations within the region (or nationally) would enable the standardisation of assessments of the quality of care provided, and significantly increase the validity of the data collected;
9. Repertory Grid interviews: an unanticipated benefit from the process of Repgrid interviews was that several service users and carers remarked that the interview process was a valuable experience for themselves. It is worth considering whether repertory grid interview training should be offered to more professionals in the trusts.

© Leading to Quality 2013 – All rights reserved Page 9
V. Implications for service organisation and transformation Several of the findings have implications for service organisation and design, which include:
1. The significance of team size on effective team working, with smaller teams being more effective than larger teams;
2. The importance of multidisciplinary team working;
3. The importance of promoting a shared sense of purpose;
4. The implications of changes in the nature of work on staff wellbeing and engagement;
5. The implications of the importance of effective and engaging communication on working practices that involve remote and agile working;
6. The support offered to team leaders during times of change.
VI. Project achievements The Project has been a substantial piece of research, which is evident from what it has achieved. These achievements include:
1. An in-depth understanding what quality of care means;
2. The development of 2 new psychometrically robust Quality of Care Questionnaires which provide an extremely useful (and valid) basis for evaluating service user and carer satisfaction with quality of care.;
3. Developing internal research capacity through training mental health professionals in the participating trusts as research champions;
4. The benefits of participating in the interviews to service users and carers;
5. A new evidence-based model of the relationship between team leadership and team working, and team outcomes;
6. Specific understanding of behaviours that lead to positive outcomes;
7. An in-depth qualitative understanding of leadership and team working;
8. Team and trust level reports of the findings;
9. This overall report of the findings, which should be a useful reference to leaders and teams working in mental health services. It identifies areas for action and best practice that can be utilised to enhance leadership, team working, staff engagement and wellbeing, and, as a result, the quality of care experienced by service users and carers;
10. The production of a Developmental Toolkit based on the results of the research containing several practical activities that teams, leaders and trusts can utilise;

© Leading to Quality 2013 – All rights reserved Page 10
11. A Leading to Quality stakeholder event to disseminate the findings from the study and discuss their practical application;
12. Professional and academic articles to disseminate the research findings.
VII. Project limitations
The Project has two main limitations:
1. Difficulty obtaining service user and carer feedback: due to the major changes mental health services have experienced in recent times, it was not possible to obtain sufficient service user and carer feedback at the team level for a statistical link to be made between service user and carer feedback on the one hand, and leadership, team working and staff engagement on the other;
2. Limited generalisation: the study was restricted to community mental health teams for adults of working age in the Yorkshire and the Humber region; as such, it would benefit from being extended to other types of mental health services, and other areas of healthcare.
Conclusion
The principle aim of the Leading to Quality research project was to build on previous research through enhancing understanding of how leadership behaviour in multi-professional mental health teams enables teams to work most effectively, by ensuring their engagement and wellbeing, so that they deliver the highest quality of care. The multi-method approach employed in the research enabled the triangulation of the results to do just this. The combination of qualitative and quantitative research methods identified how team working and leadership impacts on staff well-being and engagement, team process outcomes (innovation, focus on quality, and improvement), and quality of care. The statistical data analysis produced a new evidence-based model of the relationship between leadership, team working and team outcomes, and an understanding of the specific behaviours that lead to positive outcomes. The focus on service user and carer experiences has provided a robust and in-depth understanding of what quality of care means from their perspective. The study reinforces and adds to the NICE Quality Standards (2011). Apart from increasing theoretical understanding, the study has highly practical applications that can be utilised to enhance leadership and team working and, ultimately, to improve the quality of care offered to service users and carers, locally and across the whole NHS.

© Leading to Quality 2013 – All rights reserved Page 11
Chapter 1 Background to the Study and Relevant Literature This chapter presents the background to the Leading to Quality study, including why it was commissioned. It goes on to consider: the nature of effective team working, including the distinction that can be drawn between ‘genuine’ and ‘pseudo’ teams; recent developments in notions of what is leadership, and the evidence of the impact that leadership and team working can have on different aspects of team performance, and on team engagement and wellbeing at work. It presents a new model of team leadership and team working that will be tested in the study, so as to gain a clearer idea of what affects effective team working in community mental health teams serving working age adults in the Yorkshire and the Humber Region. Full title of the research project: ‘An investigation of the impact of leadership and team working on staff morale and wellbeing, and team performance, among mental health teams within the Yorkshire and the Humber Strategic Health Authority’. Once the study commenced and following consultation with the Project Steering Group, the title of the project was more succinctly referred to as ‘Leading to Quality’. 1.1 Why the research was commissioned The Yorkshire and the Humber Strategic Health Authority (SHA) commissioned the research study to investigate the processes and key factors for effectiveness, leadership and team working in the delivery of community mental health services linked to service user outcomes. The SHA recognises that team working and leadership are essential in the provision of high quality care, staff wellbeing and productivity. The SHA also recognises that, despite the importance of team working, data from the Healthcare Commission has found that many of the teams in the NHS do not work in what can be described as functional teams. ‘High quality care for all’ (DH, 2008) and ‘Healthy Ambitions’1 have reiterated the importance of the role of high quality leadership in the future success of the NHS. ‘Workforce Ambitions’2, the SHA’s strategy for workforce development and education, demonstrates a commitment to creating a culture of excellence in leadership and sets out plans to develop this across the authority. The commissioning of this piece of research reflects the Yorkshire and the Humber SHA’s and the chief executives’ of the participating trusts’ vision and commitment to enhance the quality of mental health provision by involving service users and their carers in determining the criteria by which it should be judged. Furthermore, because of their recognition that strong leadership, effective team working, and staff engagement and wellbeing can have a significant impact on the care that service users receive, and on sustaining it by strengthening cultures of innovation and improvement, it seeks to understand how these factors can be assessed and strengthened so as to inform improved practice both within mental health services and more widely in health and social care.
1 www.healthyambitions.co.uk 2 http://www.yorksandhumber.nhs.uk/what_we_do/workforce_education_and_training/workforce_strategy

© Leading to Quality 2013 – All rights reserved Page 12
In commissioning the research, the SHA and the participating organisations were cognisant of the national study of the leadership of mental health (MH) crisis resolution teams, which found evidence of a significant cause-effect relationship between an engaging style of leadership and team productivity (Alimo-Metcalfe, Alban-Metcalfe, Bradley, Mariathasan & Samele, 2007, 2008; Alimo-Metcalfe, Bradley & Conway, 2013). 1.2 Aims & objectives The overall aims of the project were:
1. to understand how leadership behaviour enables multi-professional teams to function most effectively in working to promote and sustain improved health outcomes for service users and carers;
2. to devise and develop a set of guidelines and developmental activities to enable mental health professionals, and others, to improve the quality of provision for service users and their carers.
The objectives were:
to identify the particular processes within teams that ensure engagement and wellbeing of team members and enable them to work most effectively;
to identify ways in which the leadership style and behaviours of the team manager have an impact on team functioning and performance;
to develop in-house research capacity by involving staff in the participating trusts in data-gathering processes;
to adapt and develop diagnostic tools and interventions that can be used across a wide variety of health and social care contexts for:
- measuring service users’ and carers’ perceptions of quality of care;
- developing multi-professional team processes, leadership behaviour, staff engagement and wellbeing, and team effectiveness;
to use the research findings to inform improved practice both within mental health services and more widely in health and social care.
1.3 Building on the research on Crisis Resolution Teams Earlier research focused on crisis resolution teams (CRTs) across England, and identified aspects of an ‘engaging culture’ that significantly predicted both the productivity, and the morale and wellbeing, of these teams. This project will build upon and extend this earlier study in five principal ways:
include an increased range of types of mental health teams (MH teams);
the assessment of leadership with reference to dimensions that emerged as significant predictors of organisational performance in multi-professional teams;
the identification of service users’ and carers’ constructs of what constitutes effective care;
© Leading to Quality 2013 – All rights reserved Page 13
the identification of healthcare professionals’ constructs of what constitutes effective care;
the assessment of the nature of team working processes.
1.4 Methodology overview It was proposed that the methodology adopted would comprise the following elements:
collecting both quantitative and qualitative data from service users, carers and staff to identify:
- constructs of what constitutes quality of care
- perceptions of quality of care within the Yorkshire and the Humber region
- perceptions of leadership and team working within the Region
- key factors affecting the effectiveness of teams and the leadership within them;
developing a series of case studies and practical guidance for use in mental health and more widely in health and social care;
building internal capacity through the identification of local Research Champions to conduct repertory grid interviews with users/carers;
a steering group, made up of service users, carers, representatives from the SHA and participating trusts to advise on the project as it progressed.
It was acknowledged at the outset that the methodology would need to be an iterative process, requiring continual reflection and evaluation to take account of experiences and changing circumstances over the 3 years. The detailed methodology for the project is outlined in Chapter 2. Nature of the teams involved in the study
The current range of community provision for adult MH service users within the NHS in England and Wales varies across trusts. The main different types of team included in this study were: Access Teams: Single point of access/referral/contact or assessment services available
in some trusts; Assertive Outreach Teams (AOTs): for ‘difficult to engage’ people living in the
community;
Community Mental Health Teams (CMHTs): offering a generic mental health service;
Crisis Resolution Teams and Intensive Home Based Treatment Teams (CRT/IHBTTs): working with people in the community experiencing acute crisis in their mental health, offering an alternative to hospital admission;
Early Intervention Teams (EITs): working with people between 14 and 35 years of age experiencing a first episode of psychosis;
Rehabilitation and/or Recovery Teams: teams that undertake a number of tasks to support service users in their recovery from mental illness as they move from inpatient units to less dependent settings in the community.

© Leading to Quality 2013 – All rights reserved Page 14
As trusts are transforming their services, the nature of the teams is changing. For example, some trusts are splitting their generic mental health teams into common mental health problems on the one hand, and severe and enduring on the other. MH teams are multidisciplinary and usually comprise: dedicated psychiatrist input, either on a full time or part time basis; community mental health nurses; ‘non-qualified’ support workers; support time and recovery workers, social workers, occupational therapists (OTs) and administrators. Many have at least access to a clinical psychologist, a counsellor or psychotherapist. MH teams generally have a team manager who has the overall responsibility for the management of the team. They may have a separate clinical lead, which could be the psychiatrist or another clinician in the team. However, all professionals involved are accountable for their own practice. This is consistent with NIMHE’s ‘Mental Health: New Ways of Working for Everyone’ (2007) which promotes a model where ‘distributed responsibility’ is shared amongst team members, and no longer delegated by a single professional such as the consultant psychiatrist. This has significant implications both for intra- and inter-team relations, and for team leadership. 1.5 Review of the literature The last 20 years have witnessed an increasing recognition of the importance of placing mental health high on the healthcare agenda, coupled with a greater emphasis on providing for people with a MH problem within their own community. The Government’s strategy is set out in the publication ‘No health without mental health’ (Department of Health, 2011). In order to meet the challenges of ensuring MH provision offered within the community is effective, there has been (in common with other areas in the NHS) an increasing interest in, and recognition of the value of, team working. In relation to the above, a concerning finding has been that whilst 92% of NHS staff say they work in teams (Healthcare Commission, 2006), further analysis of the data suggest that only 42% work in well-structured (‘genuine’) teams, that is, those where the members say they have:
clear team objectives;
interdependent working;
regular meetings to discuss effectiveness (e.g., Dawson, 2007; West, et al., 2012).
It follows, therefore, that 50% of all NHS staff work in ‘pseudo’ teams, defined as poorly-structured, whose members report high levels of errors, accidents and poor staff wellbeing at work (Dawson, 2007). While there is evidence of a significant positive relationship between team working and organisational performance in a range of healthcare and non-healthcare settings (Richter et al., 2006), a variety of factors have been found to influence effective team working.

© Leading to Quality 2013 – All rights reserved Page 15
1.5.1 A New Model of Team Leadership and Team Working The model informing the current research is an adapted version of the Input-Mediation-Output-Input (I-M-O-I) Model of team working. In brief, Ilgen et al (2005) developed this model of team working to advance traditional Input-Processing-Output (I-P-O) models of team working, which imply a simple cause and effect relationship between team inputs (e.g. resources), team processing (e.g. innovation and creativity) and team outputs (e.g. job satisfaction). The reasons for the advancement from the I-P-O model to the I-M-I-O model are that:
1. teams are complex, adaptive, dynamic systems, which exist in a context and perform over time;
2. they comprise members who interact among themselves and with other individuals; 3. as a consequence of these interactions, teams, team members, and their contexts
change; 4. these changes take place in ways that are more complex than can be captured by
simple cause and effect perspectives; 5. because of this, a new ‘Input-Mediation-Output-Input (I-M-O-I)’ model should replace
the traditional ‘Input-Processing-Output (I-P-O)’ model (Ilgen et al., 2005).
Two features of the I-M-O-I model that are of crucial importance are:
1. Mediation: When addressing an issue or solving a problem, teams do not function simply by processing information in a ‘mechanical’ way. Rather, the way in which team members act and interact with one another (and with other teams) is influenced to a greater or lesser degree by 3 ‘mediational’ or ‘intra-team functioning’ factors. These factors are referred to as: ‘affective states’ (feelings and emotions); ‘behavioural processes’; and ‘cognitive states’ (thinking). In practice, this means that the way in which any input to the team (for example, a new issue to address, or a new problem to solve) is treated will be through dynamic interaction between affective, behavioural, and cognitive elements of team working.
2. Iteration: the cyclical way in which ‘products’ and ideas are continuously analysed, evaluated, and modified, as appropriate. The iterative nature of the I-M-O-I model is consistent with the concept of ‘double-loop learning’ (Agyris, 1993). Iterative or ‘double-loop’ learning is seen as an essential feature of the implementation of innovation in the NHS (DH, 2012).
It is these complex, adaptive and dynamic processes that affect intra-team working, inter-team working and team performance (Ilgen at al., 2005). The current research seeks to capture these complexities by measuring and analysing the mediative (affective, behavioural and cognitive) and iterative effects of team working (see Chapter 4 and Appendix 1.1 for the measures used to assess these). In addition to, and in relation to the I-M-I-O model, the study looks at the leadership processes and contextual variables that affect team effectiveness – hence the model is adapted for the purposes of this research.
© Leading to Quality 2013 – All rights reserved Page 16
For a full description of the adapted I-M-I-O model and how it relates to the current study see Appendix 1.1. The subsequent sections will summarise, briefly, the relevant key findings from recent reviews of the literature on the core elements of this study: leadership and effective team working, incorporating staff wellbeing and engagement, and team performance. 1.5.2 Leadership It is hardly surprising that leadership plays a critical role in the effectiveness of team working. In fact, some researchers have stated that “leadership may have its most important consequences for teams and thus a focus on the team level is also important” (Lim & Ployhart, 2004, p. 610). Yet, despite this obvious truism, relatively little is known about the influence of team leadership on team performance (e.g. Burke et al., 2006; Schaubroeck, Lam & Cha, 2007). The question then, is what is the most appropriate approach to leadership to ensure effective team working? Changing notions of leadership
Notions of what leadership is are constantly changing, largely influenced by changes in society, including social, economic, technological, and political (Alimo-Metcalfe, 2013). In understanding the context in which effective team leadership operates, it is useful to consider the comments of one of the foremost writers in the field of organisational studies, who has summarised the ‘new reality’ facing organisations, and the agenda for leadership in this way:
Organisational learning is critical for long-term survival;
Old models of leadership have focused on position and the influence of a few; they are now obsolete as new models have disrupted this order;
One of the greatest challenges for leadership is how to create the conditions that encourage, facilitate, and sustain a favourable level of innovation, exploitation of ideas and collective learning.
(Source: Yukl, 2009)
Although not stated explicitly in Yukl’s summary, it goes without saying, that the need to be able to create a culture of high ‘readiness for change’ (RfC) is also of critical importance to leadership in the NHS, never more so than now. Teams and organisations that have high RfC are those in which:
people are open to change, rather than being resistant;
a range of suggestions/solutions for dealing with challenges are generated;
change initiatives are successfully implemented.
Academics often refer to the fact that we are now in the era of ‘post-heroic leadership’ (Alimo-Metcalfe, 2013). Traditional models of leadership, including the ‘heroic’ models of

© Leading to Quality 2013 – All rights reserved Page 17
‘inspirational’ and charismatic’ leadership, which focus on individuals who are defined as leaders by virtue of the fact that they occupy a particular hierarchical role, are being replaced by the concept that leadership is essentially a relational and shared process, and that it is the interaction of people working in collaboration, that creates ‘leadership’, irrespective of the role they occupy. This does not absolve individuals who occupy formal leadership roles of their responsibility for the outcomes of their teams, nor, importantly, for the effect of their leadership behaviours on their team, and for the impact that working in the team has on their colleagues’ wellbeing. Indeed, it could be argued that such responsibilities are seen as even more important for judging their effectiveness. But it does emphasise that they cannot ‘do’ leadership alone; it is a social process, and it is dynamic. Leadership and team working
Not surprisingly, this concept of leadership being a distributed and shared process has been related to recent developments in the study of the nature of leadership in team working. Whereas, formally, leadership has been regarded as what a ‘team leader’ brings to a team, such as their knowledge, expertise, ‘charisma’, and so on – that is, as an input to team working - more modern perspectives consider that leadership is also what ‘merges or is drawn from teams as a function of working on and accomplishing shared work’ (Day et al., 2004, p.859). Taking this perspective, leadership is also viewed as an outcome, and, indeed, the very process of doing leadership as a collective endeavour. Bringing these ideas together, of leadership being a shared process, and leadership and team working being inextricably linked, Zaccaro & Klimoski (2002) refer to ‘team interface’, which is the interface of leadership and team processes – ‘the various ways that leadership and team processes become intertwined so as to influence collective performance’ (p.6). Directly related to this conceptualisation of leadership in the context of intra-team working, but also relevant to inter-team working, is the principle of ‘distributed responsibility’ (NIMHE, 2007). This denotes a situation in which team members share responsibility, rather than having responsibility delegated by a single professional, such as the Team Lead. Integrative leadership and partnership working
Another concept of interest, particularly in the context of partnership working, and a relatively new one being discussed in the leadership literature, is that of ‘integrative’ leadership, which refers to the situation in which the leadership role is undertaken by a group of individuals from different organisations, agencies, or groups, working in concert (Alban-Metcalfe & Alimo-Metcalfe, 2010; Morse, 2010). In their definition of integrative leadership, Crosby and Bryson (2010) suggested that it involves:
‘bringing diverse groups and organizations together in semi-permanent ways – and typically across sector boundaries – to remedy complex public problems and achieve the common good’ (p.211).

© Leading to Quality 2013 – All rights reserved Page 18
Although not only exclusively related to partnership working, it reflects new ways of seeing leadership as a ‘what makes things happen in a collaboration’ (Huxham & Vangen, 2005, p.202), an approach in which structures, processes and people are inextricably interconnected. The concepts of ‘collective leadership’, ‘distributed leadership’, and ‘integrative leadership’ in teams have important implications for the effective delivery of MH services, and for the relationship between responsibility and accountability. That is, that while those in formal leadership roles, such as team managers, are responsible for the achievements of the team as a whole, all team members, and other teams, individuals, and agencies with whom they work, have accountability for delivering the highest quality of care for their service users. These are principles of which the commissioners and researchers for the LTQ study are particularly mindful.
Leadership and employee engagement
Finally, the critical importance of employee engagement, which has been found from numerous research studies to have a significant impact on individual and organisational performance, and on staff morale and wellbeing (e.g. Alimo-Metcalfe & Alban-Metcalfe, 2008; Macleod & Clarke, 2009; Wollard & Shuck, 2011), is central to the activities and responsibilities of leadership. The concept of ‘engagement’ could be regarded as the underlying theme of ‘connectedness’ which relates to all the concepts mentioned below with respect to effective intra-team working, inter-team and inter-agency working. A 3-year investigation of the nature of day-to-day leadership that significantly impacts levels of employee engagement was undertaken initially in the NHS and local government, and later extended across public and private sector organisations (Alban-Metcalfe & Alimo-Metcalfe, 2007; Alimo-Metcalfe & Alban-Metcalfe, 2001; 2003). It identified a 14-scale model of ‘engaging leadership’, which relates to individual, team, organisational, and inter-organisational relationships, and partnership working (Alban-Metcalfe & Alimo-Metcalfe, 2010). It is shown in Figure 1.1 overleaf. Several studies have provided evidence of its validity in significantly predicting levels of employee engagement and wellbeing in the public and private sector (e.g., Alban-Metcalfe & Alimo-Metcalfe, 2000; Kelly et al., 2006; van der Kleij, 2011; Alban-Metcalfe & Jtte Alimo-Metcalfe, 2013). While it is undoubtedly important to know that there is evidence that the model of engaging leadership predicts engagement and wellbeing of staff, the ultimate test of any leadership model is whether it predicts performance or productivity. Furthermore, since the Leading to Quality study was concerned not only to investigate the impact of leadership in teams on team performance, but also, importantly, on team members’ morale and wellbeing, it is important to look at relevant studies, such as the one described below (leadership of crisis resolution teams).

© Leading to Quality 2013 – All rights reserved Page 19
Figure 1.1 The Model of Engaging Leadership
While it is undoubtedly important to know that there is evidence that the model of engaging leadership predicts engagement and wellbeing of staff, the ultimate test of any leadership model is whether it predicts performance or productivity. Furthermore, since the Leading to Quality study was concerned not only to investigate the impact of leadership in teams on team performance, but also, importantly, on team members’ morale and wellbeing, it is important to look at relevant studies, such as the one described below (leadership of crisis resolution teams).
The link between leadership in teams, team members’ engagement and wellbeing, and performance of the team
Studies showing a predictive, or causal, link between leadership and objective measures of performance are rare (e.g., Jing & Avery, 2008; Keller, 2006). Most studies which show a link between leadership and performance are based on correlations, rather than cause and effect relationships. Among the reasons for the rarity of predictive studies are that they are complex, expensive, and take at least 3-years on average. Leadership of Crisis Resolution Teams
The national study of CRTs, referred to earlier, was a 3-year SDO-funded longitudinal study to examine whether there was a causal relationship (rather than simply a correlational relationship) between the quality of leadership in the teams and:
the team members’ engagement and wellbeing;
the productivity of the teams.

© Leading to Quality 2013 – All rights reserved Page 20
Working in partnership with colleagues at The Sainsbury Centre for Mental Health, Alimo-Metcalfe et al., (2007, 2008, 2013) gathered data from 42 CRTs at two time points. They collected information on:
team leadership (3 scales ‘engaging with others’, ‘building shared vision’ and ‘leadership capabilities’) and staff engagement and wellbeing;
objective information on team productivity;
contextual/background information about the team (e.g. age of team, size of team, caseload size, local mental health needs using the Mental Illness Needs Index) to:
- make sure that the results were not being unduly influenced by contextual factors, rather than leadership, staff engagement and wellbeing;
- understand the impact of context on leadership, staff engagement, staff wellbeing and productivity.
The research found that:
all 3 leadership scales correlated significantly with levels of team members’ engagement and wellbeing ratings;
there was a cause and effect relationship between ‘engaging with others’ and team productivity, measured objectively (while controlling for the possible confounding effect of the contextual variables);
7 of the 9 contextual variables were found to significantly predict levels of productivity (for details see Alimo- Metcalfe et al., 2007).
This provides an extremely important source of validation of the model of engaging leadership, and also provides one of the few studies to show a cause-effect relationship between a model of leadership and how it actually predicts the performance of teams (which in this case were CRTs in the NHS) 1.5.3 Effective team working Apart from leadership, other factors influence the effectiveness of teams including:
1. intra-team working;
2. inter-team and inter-agency working;
3. contextual factors. 1.5.3.1 Intra-team working The research evidence points to several factors affecting team effectiveness; the most pertinent factors in relation to this study include:
expertise & professional diversity
collective identity
team potency (the belief that the team can achieve its goals)
social support
psychological safety

© Leading to Quality 2013 – All rights reserved Page 21
team reflexivity These factors are examined briefly below. Expertise and professional diversity
Research findings are mixed in relation to the potential benefits of expertise and professional diversity and how it can affect the affective, behavioural, and cognitive contributions to team performance. It can be beneficial to team performance because of the variety of knowledge, expertise, information, access to networks, etc., that it offers the team (i.e. cognitive and behavioural); in which case this is referred to as ‘diversity as variety’ (Harrison & Klein, 2007). However, the presence of expertise and professional diversity may also lead to the formation of subgroups and cliques within teams; in which case, it is referred to as ‘diversity as separation’ (Harrison & Klein, 2007), which may be deleterious to effective team performance (van Knippenberg & Schippers, 2007).
Research into what is known as ‘faultline theory’ (Lau & Murnighan, 1998) has made a significant contribution to understanding under what circumstances professional diversity is a help or a hindrance. ‘Faultlines’ in teams can appear because of differences between team members, for example, their gender, age, professional discipline, length of time being associated with the team, professional values, and so on. They have the potential to create intra-team conflict, which, in turn, affects the performance of the team.
One obvious way in which the dysfunctional potential of ‘faultlines’ in teams can be attenuated is by the team sharing the same vision, and objectives. Team leadership plays a key role in achieving these conditions, and, indeed, they are generally regarded as a major leadership responsibility, and/or criterion for judging the effectiveness of an individual in a leadership role (e.g. Bass, 1998; Alimo-Metcalfe & Alban-Metcalfe, 2008). In the longitudinal study of CRTs cited above, the leadership scale of ‘engaging others’ that predicted team productivity, included the following two items: “Involving all staff in developing the vision”, and “Involving all staff in determining how to achieve the vision” (Alimo-Metcalfe et al., 2007. 2008). Collective identity
Another related aspect of exploiting team diversity for its potential, rather than its problems, is to focus on the motivational or affective climate of the team, by creating shared sense of identification within the team: a ‘collective identity’ . As leading researchers in the field have stated: ‘One of the principal explanations for how expertise diversity might be beneficial is that a diversity of knowledge and expertise within a group can promote learning and search behaviors that in turn lead to adaptive, innovative solutions’ (van der Vegt & Bunderson, 2006, p.533). In their study of teams in the oil and gas industry, they examined the relationship between expertise diversity and team learning and team performance under varying levels of collective team identification and found that:
for teams with low collective identification, expertise diversity was negatively related to team learning & performance;
for teams with high team identification, the relationship between expertise diversity & team learning & performance were positive.

© Leading to Quality 2013 – All rights reserved Page 22
These findings are of direct relevance to the current context of MH teams working in the NHS, where learning and innovation are of such importance to the current NHS agenda, and to the benefit of service users. Clearly, they identify a key focus for team leads, and the nature of leadership and culture within MH teams. West (2004), for example, obtained evidence that when teams are led and managed effectively, diversity is positively associated with innovation. The findings are also supported by the research on the nature of engaging leadership, and are consistent with the predictors identified in the longitudinal study of CRTs.
Team potency
It has long been known in the field of organisational psychology that an individual’s sense of ‘self-efficacy’ (a confidence in one’s ability to achieve tasks and goals) (Bandura, 1977), plays a key role in influencing the degree to which people will take risks in learning new behaviours, being pro-active, and so on. In relation to teams, it is often referred to as ‘team potency’ (Guzzo et al, 1993), which refers to a team’s belief and confidence that it can be effective in what it undertakes and successful in what it aims to achieve. It has been found to have an important impact on team performance and team effectiveness (Tesluk & Mathieu, 1999; Hu and Liden, 2011), and is highly relevant in the context of an environment of constant change in the NHS, where a sense of confidence and control over one’s work and the ability to give of one’s best can be so badly damaged. Leadership behaviours, especially those consistent with an engaging leadership style (described above), have been found to be critical in promoting a sense of team potency and, consequently, improved team effectiveness (Schaubroeck et al., 2007; Hu and Liden, 2011).
Social support
The importance of social support in teams in strengthening their effectiveness and wellbeing of members has been well-established in the research literature (e.g. van Mierlo et al., 2006). The concept refers to members of the team supporting each other by listening, appreciating, affirming reality, making suggestions, encouraging, etc. It has been found to promote a sense of self-efficacy, or confidence that one can succeed in what one does, and handle difficult situations (Hobfoll, 2002). In addition, among the important benefits it can have are that of helping to ‘buffer’ against the harmful effects of heavy workload and work-related stress (Nahum-Shani & Bamberger, 2011), which is invaluable in the context of the challenges facing staff in the NHS. Furthermore, its physiologically beneficial effects have also been evidenced (Heaphy and Dutton, 2008 cited in Nahum-Shani & Bamberger, 2011, p. 50). Some researchers have distinguished between ‘affective’ (emotional) and ‘task-related’ social support, finding that ‘affective support predominantly increases individual members' motivation, while task-related support predominantly improves coordination within teams’ (Hüffmeier & Hertel, 2011).

© Leading to Quality 2013 – All rights reserved Page 23
Psychological safety
Teams which offer a ‘psychologically safe’ environment, are those in which members feel safe to make mistakes without being ridiculed or penalised, and in which they can ask for help, information or support and still be valued and respected. Working in such a team encourages judicious risk-taking and experimentation, and opportunities to learn from mistakes. It thereby supports innovation and improvement. For example, in a psychologically safe environment team members are more likely to come up with a novel way in which a particular problem can best be solved (e.g., Edmondson et al., 2001). Team leaders have a powerful effect on creating a culture of psychological safety by their attitudes and also by their behaviours of:
being accessible;
admitting when they have made mistakes;
reducing a sense of hierarchy and not being status-conscious. Team reflexivity
Another key aspect of a team’s effectiveness is the extent to which teams meet to review and modify objectives, strategies and processes in service of their overall goal (referred to as reflexivity). This has also been found to be a powerful predictor of effectiveness and innovation (West, 2000). A recent study by West et al (2012) based in community mental health teams found that ‘many teams are so consumed by the task or so resistant to change that they fail to review and revise their approaches, continuing to expend energies in directions that are sub-optimal for service user care’ (p20).
1.5.3.2 Inter-team and inter-agency working As mentioned above, a key element of effective team working is how teams relate to and work with other teams and agencies. Two aspects of inter-team and inter-agency working which are of considerable interest to the current project, and on which there are research data available are ‘partnership working’ and ‘integration’. Partnership working
Partnership working refers to the establishment of working relationships between two or more teams or agencies. Where partnership arrangements have been set up, with clear guidelines for their functioning, there is the possibility of offering the kind of provision proposed in the NIMHE (2007) programme. Conversely, an over-emphasis on maintaining a peaceful partnership arrangement in developing ‘synergy’ with other agencies can stifle radical innovation (Dickinson et al., 2007; Platt, 2007). This may be especially true in the case of ‘disruptive’, as distinct from ‘incremental’ innovation (Christensen, 1997). The former refers to the concept of a radically new way of doing something, or of delivering a service, etc., whereas the latter refers to the typical process by which improvement is realised, which is through incremental steps.

© Leading to Quality 2013 – All rights reserved Page 24
A compounding factor emerges when team members work for different employers, particularly when such differences coincide with demographic or professional differences between team members (van Knippenberg et al., 2007). It is common for community mental health teams to contain staff from both NHS and social service organisations.
Integration
Some researchers have found that integration in the context of inter-team and inter-agency working may be more important than intra-team functioning in terms of the delivery of services (e.g., Richter et al., 2006). Community mental health teams need to interact with other teams within their own organisation, and with teams from other agencies, such as housing and social services, to ensure an integrated service. Factors that have been found to impact on inter-team and inter-agency working have been:
capacity problems in other parts of the local service system, and particularly among generic CMHTs (Onyett et al., 2008);
‘structural’ variables, such as inter-group competition, hinder effective inter-team collaboration (e.g., Mohrman et al., 1995);
frequency and quality of contact between teams under conditions of collaboration assumes a central role in creating effective relationships between teams (Pettigrew & Tropp, 2006, 2011);
frequent task-related contact between teams (Richter et al., 2006), which can be facilitated by the existence of ‘boundary spanners’;
the extent to which the team leader identifies with the overall health care organisation;
‘attitudinal’ variables, such as hostile inter-group attitudes (Hogg & Terry, 2000);
the negotiation style adopted by the team leader, which can impact on inter-group competition/collaboration (Richter, West, Sacramento & Hirst, 2005).
The quality of inter-team working in mental health is particularly topical in light of the introduction of the UK Health and Social Care Bill in 2011 (Timmins, 2012). One of the principal criticisms of this Bill was that the proposals (as initially expressed) seemed to place significant emphasis on promoting competition (rather than co-operation and collaboration). Thus, for example, the role of Monitor was to change to that of being an economic regulator, with an explicit duty to promote competition. However, this role was subsequently modified. As Monitor states on its website, there were significant ‘concerns [in Parliament] that Monitor would pursue competition as an end in itself [and that]… under the Act Monitor's role will focus on making sure that competition is fair and that it operates in the interests of patients’ (Monitor website, 2013). The central issue here is that people with complex needs, mental health being a good example, need an integrated approach to their care, involving multiple health care disciplines and possibly health and social care agencies. The on-going dilemma of how to promote competition and collaboration at the same time, and how to strike an appropriate balance, has been addressed by the NHS Future Forum. On the basis of its consultations with service users and professionals, the Forum produced a

© Leading to Quality 2013 – All rights reserved Page 25
first report, which led to significant changes in the Bill. The Forum has been asked to continue for a second phase, with one of the work streams providing independent advice on how to ensure that ‘the modernisation programme leads to better integration of services around people’s needs’.
1.5.3.3 Contextual factors As discussed earlier in the chapter, contextual factors are variables that add information about the background to the team and the context in which they work. They can include a substantial range of factors including age of team, case load size of key worker, mental health needs index, time team lead in post. Contextual variables can add considerable value at a practical and theoretical level, through adding to the broader understanding of the factors that influence leadership and team working. However, they may also influence the key relationships being investigated and, therefore, skew the results. For example, the relationship between leadership and staff wellbeing may well be influenced by the contextual variable ‘caseload size of key worker’; if caseload size is not controlled for statistically then it might look like there is a very strong relationship between leadership and staff wellbeing, when really the relationship could, to a large extent, be due to caseload size. In this example, contextual factors are confounding variables. In order to have a complete understanding of the effectiveness of team working and team leadership, it is important to recognise the reciprocal relationships between team leadership and team working, and between both and their organisational context and the wider context (Glasby, Dickinson, & Peck, 2006; West & Markiewicz, 2004).
1.5.4 Impact of Team Leadership and Team Working: Outcome measures The ideal outcome measure for a study that is investigating, for example, the association between leadership and team performance, is to obtain ‘objective’ measures of performance outcomes, and to employ a longitudinal design, so that leadership can be assessed at Time 1, and outcomes of team effectiveness, at Time 2, 10-12 months later. However, since this can be highly problematic in terms of the practicality of collecting the relevant data, such studies are very rare.
Where objective data are unavailable, the recognised practice is to identify the most valid ‘proxies’. In the present Leading to Quality investigation, following a discussion with the Steering Group overseeing the project, it was decided to use team members’ ratings of the effectiveness in terms of three outputs that are high on the DH Quality of Care agenda (DH, 2012): ‘innovation’, ‘focus on quality’, and ‘improvement’. These have the potential to provide rich, highly valuable, and relevant data since:
they enable comparisons to be made between the current findings and other comparable research studies in the literature;

© Leading to Quality 2013 – All rights reserved Page 26
the data can also then be compared with other studies which have used ‘objective’ outcome measures;
similarities between the present and other studies can be compared to determine whether any themes emerge.
Service user performance ratings
If teams’ effectiveness relates to the quality of service offered, the most valid source would be the users of the service. However, as the current investigation found, gathering data from service users and carers can be problematic, especially if the sample size needs to be substantial to allow the application of rigorous statistical analyses. In which case, team members’ ratings might best be regarded as ‘proxies’ for these measures, and allowance must be made for potential subjective bias. Impact of Team Working on Team Members
Here, some studies have used satisfaction with different aspects of how the team functions, and attachment to the team and fellow team members, as outcome measures (e.g., West et al., 2005). The justification for this is threefold:
there are theoretical reasons for using measures of job satisfaction, and motivation, as ‘proxies’ for effective performance (e.g., Alban-Metcalfe & Lloyd, 2013; Bass, 1998);
there is empirical evidence of a significant link between job satisfaction and organisational performance, measured objectively (Patterson, Warr & West, 2004; Xenikou & Simosi (2006);
it might also be the case that the subject of the study is an investigation of the impact of leadership on motivational, wellbeing, and other aspects of team members’ experience, such as ‘engagement’, in which case these measures are the most valid for this purpose.
In each of these cases, the criteria used are subjective in nature. However, the use of subjective criteria can be justified since feelings of, for example, satisfaction and motivation to act are essentially personal, and are, therefore, by their very nature, subjective. The current study assesses the impact of team leadership and team working with reference to levels of team engagement and wellbeing at work. The decision to measure team engagement was taken in light of consistent evidence from private, public and third sector organisations of the effect on employee engagement both on staff wellbeing and on organisational performance. The relevance of wellbeing at work is that it contributes to an employer’s duty of care, and has been shown to be a significant predictor of organisational performance (Alban-Metcalfe & Lloyd, 2013; Macleod & Clarke, 2009). 1.6 In summary This chapter has reviewed, briefly, the literature relating to leadership, particularly team leadership, and its impact on staff engagement and wellbeing at work, to the nature of effective team working, and factors that have been identified as affecting team performance.

© Leading to Quality 2013 – All rights reserved Page 27
In order to achieve the aim of the study, which is to investigate the impact of leadership and team working on staff morale and wellbeing, and team performance, among mental health teams, a model of the relationship between the various variables in the study (the I-M-O-I model), has been adopted, which provides a reasoned framework for assessing and examining the relationships between the various interacting factors. To summarise, the research is examining the impact of leadership and team working on team outcomes including staff engagement and wellbeing, focus on quality, innovation and improvement, and, qualitatively, the impact on quality of care. The next chapter explains the methodology adopted in the study.
© Leading to Quality 2013 – All rights reserved Page 28
Chapter 2 Methodology This chapter describes the aims and objectives of the present investigation, the principal characteristics of the sample, and the methodology adopted. 2.1 Aims and Objectives As noted in Chapter 1, the primary aims of the research were to understand how the leadership of multi-disciplinary MH teams and the way that such teams function, promote and sustain positive outcomes for service users, and to provide guidance for future practice. Once the project commenced, it was agreed that the outcome for service users was to be good quality of care, as perceived by service users and carers3. The objectives were:
1. To identify the particular team leadership and team working behaviours that have an impact on team performance (as measured by service users’ and carers’ perceptions of quality of care);
2. To identify the particular team leadership and team working behaviours that have an impact on team engagement and wellbeing at work;
3. To develop a series of workbooks and related activities, based on the findings of the research.
To this end, a combination of quantitative and qualitative data was gathered. Mixed method approaches to data-gathering typically produce rich data, and also strengthen the validity of the research findings because the use of different sources allows for triangulation of the data. 2.2 Stages of the Investigation The research consisted of 6 main phases described below with their associated methodology. 2.2.1 Stage 1: Preliminary qualitative interviews This stage comprised two principal aspects:
1. To collect information from the leaders of MH teams about:
their experience of the nature of team working, and of the leadership of MH teams;
the range of contextual factors that affect the successful provision of MH within their team.
3 It was initially proposed to use these questionnaires as independent measures of the quality of the service offered by the MH teams. For a number of reasons, principally difficulty in gaining access to service users and carers, coupled with large scale changes in the structure of MH provision in many of the Trusts, it did not prove possible to match service users’ and carers’ responses to the questionnaires with their MH team.

© Leading to Quality 2013 – All rights reserved Page 29
Sixty-eight team leads were interviewed. 2. To collect information from MH service users and carers about:
their experience of the quality of the service provided by MH professionals;
what good quality of care looks like from their perspective.
Sixty-five service users/carers were interviewed.
The users of mental healthcare provision (referred to here as ‘service users’) and those who have the role of acting as their carers (‘carers’) can be considered as the ultimate judges of the quality of MH provision. A large number of MH teams commonly ask service users, in particular, to comment on the service that they have received, in the form of a Satisfaction Survey. However, such surveys:
appear mostly to be based on MH providers’, rather than service users’, perceptions of the criteria against which quality of provision should be judged, in other words, a ‘provider-centric’ view, rather than a ‘user-centric’ view;
are not standardised across regions or teams;
do not adequately reflect carers’ perspectives. Given that carers are one of the most important sources of support available to MH service users, this last factor is a serious omission. More recently, NICE (‘Quality Standards for Service Users Experience in Adult Mental Health’, 2011) have issued guidelines about the criteria against which MH and related provision should be judged.
The service user and carer interviews at this stage were used to develop the service user and carer questionnaires used as part of the research (see Stage 2 below). As such, these questionnaires were developed from the perceptions of service users and carers, hence overcoming the ‘provider-centric’ viewpoint of other questionnaires. Repertory Grid technique
In order to address the criterion issue (what quality of care is), the Leading To Quality research sought to determine the dimensions or ‘constructs’ that (a) service users, and (b) carers use to assess the quality of the service provided. It did so using an established technique, Role Construct Repertory Grid (Repgrid) (Kelly, 1955). This technique, which takes the form of a semi-structured interview, is described in Appendix 2.1. 2.2.1.2 Training of Research Champions Because of the potentially sensitive nature of (a) the process and (b) the kind of constructs that might emerge, a number of Research Champions (RCs) (each of which was a qualified MH professional with a number of years’ experience) were trained in Repgrid technique as part of the Leading To Quality project, and were the only researchers involved in this element of the data collection. For professional reasons, RCs only worked with service users and carers in a different locality to their own. Each RC undertook Repgrid interviews with not more than 10 service users and 10 carers. In order for service users and carers to

© Leading to Quality 2013 – All rights reserved Page 30
feel they could be open and honest about their experiences of care, the RCs did not conduct interviews with service users and carers from their team. 2.2.2 Stage 2: Designing the service user and carer questionnaires During this stage the data collected at stage 1 was used to develop two quality of care assessment tools (one for service users and one for carers). The emergent constructs from the interviews were content-analysed during a 1-way workshop in which the university researchers, the RCs, a service user, a carer, and an expert in the area of MH participated. The themes that emerged from the service users and, separately, from the carers, were summarised, and formed the basis of two questionnaires, one for service users, the other for carers. Stage 2 of the research is discussed in-depth in Chapter 3. 2.2.3 Stage 3: Quantitative data collection and analysis 2.2.3.1 Questionnaire data from mental health teams The EngagingTeams360 was used to collect quantitative data from MH teams about the key factors in this study including: Team Leadership, Team Working, and the impact of these on the team, measured in terms of: Team Process Outcomes (Innovation; Focus on Quality, and Improvement) and Impact on Team Members (Team Engagement, and Wellbeing at Work). The EngagingTeams360 had been developed prior to the current study (Real World Group, 2008). The interviews with team leaders at stage 1 were conducted in order to elicit their constructs of leadership and effective teams, so as to be able to compare them with the items in the EngagingTeams360, and, thus, its face and construct validity among MH professionals. The emergent constructs from the interviews were content-analysed, and the emergent themes compared to the items of the EngagingTeams360. Other than in specific wording, for example, ‘service user’ or ‘professional’, rather than ‘client’ or ‘manager’, each of the items relating to team leadership and team working were found to be relevant.
Data collection and responses
The EngagingTeams360 was administered to teams primarily via the team lead. Data collection was extended due to difficulties in obtaining sufficient responses. A total of 590 questionnaires were collected from team members. The breakdown of the sample is presented in Appendix 2.2. 4 The analysis and results from the EngagingTeams360 are presented and discussed in Chapter 4. 4 Since the EngagingTeams360 tool was made available on‐line was well as hard copies, it is not possible to calculate the actual response rate.

© Leading to Quality 2013 – All rights reserved Page 31
2.2.3.2 Contextual information Contextual information was collected about the teams, including: caseload size of key worker; size of team; multi-disciplinary nature of the team, age of team, and time team lead in post. These variables were incorporated into the data analysis (discussed in Chapter 4). 2.2.3.3 Questionnaire data from service users and carers The service user and carer questionnaires were circulated among service users and carers in each of the participating trusts. The responses (n = 452 for service users, n = 197 for carers) were analysed using principal components analysis. The psychometric properties of the components (‘factors’) that emerged were examined to test for internal consistency (reliability). This is an important activity to undertake in order to check that the factors (which are groups of items that correlate together highly) do represent an underlying dimension. The analysis and results from the service user and carer questionnaires are presented and discussed in Chapter 3. Overall comment on the quantitative data collection An aim of the research was to look at the quantitative relationship between leadership, team working, staff engagement and wellbeing on the one hand, and quality of care the team provides on the other. However, whilst the number of service user and carer questionnaires returned was substantial, at a team level there was not a sufficient enough response to provide a valid measure of the quality of care delivered by the team. As such, it was not possible to make the quantitative link between these elements of the research. 2.2.4 Phase 4: Case studies In order to obtain and in-depth understanding of leadership and team working in practice, and to look at the relationship between this and staff engagement and wellbeing, and quality of care, case studies were conducted.
It was decided that the case studies would be a series of best practice case studies, focusing on the positive aspects of leadership and team working in community mental health teams. As such, the case study teams were selected based on the results from the EngagingTeams360, with, where possible, the team with the most positive questionnaire results being selected for the case study.
Across six teams 46 interviews were conducted. Interviews were undertaken with the team lead and with other staff within the team, including a variety of different roles (nurses, occupational therapists, social workers, psychiatrists, support workers, administrators, and therapists).
The detailed methodology for the case studies is outlined in Chapter 5.
© Leading to Quality 2013 – All rights reserved Page 32
2.2.5 Phase 5: Developmental Toolkit
On the basis of the research findings a developmental toolkit is being written which contains a series of workbooks. Each of the workbooks draws together evidence on a particular theme and offer practical guidance of the kind of actions that can be taken to increase the quality of team leadership and team working among MH teams, other teams with which they work, and more widely in the NHS. 2.2.6 Reports In addition to this report, reports will be presented to each of the trusts, identifying themes and areas to support development. Each team that had a 30% or over response rate to the EngagingTeams360 questionnaire has been given a tailored report on their findings. Summary This chapter has explained the rationale for the methodology adopted in the study, the stages in the investigation, the nature of the data gathered, and the samples on which the data were based. The analyses of these data will enable the researchers to learn about the relationship between leadership, effective team working, and their impact in mental health teams and quality of care.
It is hoped that the reports and workbooks produced as part of the research will be used by trusts and teams to bring about improvements in team working and leadership across the region, so as to enhance staff engagement and wellbeing, and the quality of care provided by the teams. The next chapter focuses specifically on another crucial question investigated in this study, namely, what do service users and carers regard as high quality care, which is, ultimately, at the heart of the Leading to Quality study.

© Leading to Quality 2013 – All rights reserved Page 33
Chapter 3 Service User and Carer Constructs of High Quality Care A key aspect of the research project was an investigation of the criteria by which service users and carers judge the quality of care they receive. Thus, a crucial initial stage of the project was to gather information directly from service users and their carers, as to what they regard (or ‘construe’) as high quality care. From these data a questionnaire could be developed to assess quality of care from a wide sample of service users and carers, and provide invaluable information for mental health professionals to inform their approach to providing high quality care. 3.1 Development of the Service User and Carer Questionnaires 3.1.1 Use of Repgrid Technique The rationale for adopting the repgrid technique of interviewing with users and carers is explained in the previous chapter. In line with one of the aims of the research project (cf Chapter 1) the intention was to build in-house expertise in the participating trusts. One of the main ways of achieving this aim was to train RCs from among a group of volunteer MH professionals working in the teams involved in the study. RCs were trained in each of the participating trusts. The two day training course was delivered by the university researchers, all of whom are psychologists with considerable experience and knowledge of the technique. Once the RCs felt confident in using the repgrid interviewing technique they undertook interviews with a total of 65 service users and carers. Most of the interviews took around 45 to 60 minutes. Each interview elicited, on average, 10 to 12 ‘major’ constructs relating to quality of care. A total of over 450 constructs of what constitutes ‘high quality care’ were elicited. Since the constructs from users and carers were virtually identical, their constructs were combined. While this large range of constructs provided a rich source of information as to how service users and carers view quality of care, it was crucial to identify which were the most important aspects by which quality of care could be judged, and, in addition, to broaden the sample of service users and carers so as to be able to have greater confidence in drawing conclusions from the data. The means of achieving these aims was by developing a questionnaire, based on a ‘distillation’ of the 450+ constructs obtained. The questionnaire could then be used to assess the quality of care as perceived by a substantially larger sample of service users and carers. Such analyses could valuably inform mental health teams in relation to:
which aspects of their team working related directly to users’ and carers’ notions of quality of care;
the questions on which they should seek feedback from service users and carers;
how best to review their effectiveness as a team;
what areas, if any, required attention to improve leadership and team working;

© Leading to Quality 2013 – All rights reserved Page 34
areas for discussion in regular team meetings and reviews of progress;
possible topics for discussion in individual supervision/appraisals;
informing conversations with other teams/agencies as to how to improve their relationship;
working arrangements.
3.1.2 Analysis of the constructs from service users & carers of high quality care For the purpose of forming the basis of developing the ‘Quality of Care Questionnaires’, the university researchers content analysed the constructs to identify important themes. Appendix 3.1 shows the 23 groups of constructs, examples of the constructs, and the approximate number of constructs elicited, in each group (shown in brackets). However, there were too many themes from which to develop a questionnaire that would be of a length that would not deter responses. An additional concern was that the themes had been identified by the university researchers, rather than by a user and carer representative, and the RCs - the very people who had elicited them from users and carers, and who were professionals working in the mental health teams. Accordingly, a one day workshop was held, attended by 4 university researchers, 8 RCs, 1 service user, 1 carer, a representative of the Steering Group, and a mental health adviser to the project, at which the 23 groups of constructs were sorted into major themes, on the basis of conceptual analyses of the constructs. The participants were divided into 6 groups, each of which group included at least one RC. The university researchers supported the discussions. The themes to emerge fell into seven main groups:
working in genuine partnership with professionals;
supporting me to achieve my goals and strengthen my self-efficacy;
the nature of the therapeutic relationship;
being treated as an individual in planning my personalised care;
the quality of the professionals involved;
access to support services;
good intra-team, and inter-team and inter-agency communication. 3.1.3 Turning service users’ and carers’ constructs into questionnaire Items During the second part of the workshop, each of the six groups were tasked with turning the constructs into questionnaire items, so as to ensure their validity. 3.1.3.1 Issues of validity The validity or ‘truthfulness’ of a questionnaire can be determined in a number of ways, including:

© Leading to Quality 2013 – All rights reserved Page 35
Content validity – the extent to which it covers all the major aspects of the concept being investigated, for example, a questionnaire that focuses only on measuring the quality of ‘listening’ shown by a MH professional, but does not include topics about the quality of care, such as, ‘providing enough information’, or ‘discussing care plans’, would not be valid;
Face validity – concerned with whether the questions look sensible to, and are readily understood by, the individual completing the questionnaire, and will affect factors such as whether sufficient thought is given to completing it;
Construct validity – a somewhat more abstract concept, which refers to the extent to which the questionnaire really measures the underlying idea or construct, which in this case is quality of care. One practical way of assessing construct validity is to compare its contents with the wider literature. A further issue is the extent to which each of the items complies with Facet Theory (cf. Chapter 2).
3.1.3.2 Developing and piloting the questionnaires On the basis of the analyses, it was decided to produce two separate ‘Quality of Care Questionnaires’, one for service users, the other for carers. The final questionnaires are shown in full at the very end of this report5. It can be seen that the service users’ questionnaire contained 29 items, and the carers’ questionnaire 31 items. Twenty-seven of the items in the two questionnaires referred to the same underlying constructs, although some were phrased slightly differently, to match the person completing the questionnaire. For example, “Works on goals that are meaningful to me” (service user item), versus “Works on goals that are meaningful to the person I care for” (carer item). In addition, 2 items were unique to the service users’ questionnaire, namely: “Gives me continuous support when I move from one service to another”, and “Involves the right people in my care planning”. In relation to the Carers’ questionnaire, 1 item was unique: “Is sensitive to the stress of everyday living for carers”. 3.1.3.3 Testing validity The face validity of the questionnaires was assessed by sending them to the RCs for comment. The questionnaires were then distributed to service users and carers in the Yorkshire and the Humber region. In order to ensure anonymity, service users and carers were not asked for any biographical data, but they were asked to give the name of the team with whom they had worked, or were currently working. A total of n = 649 usable questionnaires were returned (452 from service users, and 197 from carers). The content and construct validity of the questionnaires were determined by comparing them with the themes underlying the ‘Recovery Model’ of MH provision. The content and construct validity of both questionnaires have subsequently been confirmed by comparing them with ‘NICE Guidelines’, which were not available at the time (see below).
5 The questionnaires are also available to download from: http://www.brad.ac.uk/management/cme/related‐links/

© Leading to Quality 2013 – All rights reserved Page 36
3.1.4 Analysis of responses to the service user and carer questionnaires The responses to each questionnaire were factor analysed, so as to determine whether any major themes could be detected. Factor analysis looks for patterns in the data in how people responded to the items. It ensures that the items reflect the respondents’ perceptions of what are meaningful dimensions of care, since items that strongly correlate together are assessing some similar aspect of quality of care. 3.1.4.1 Service User Quality of Care Questionnaire Factor analysis of the results identified four clear themes or dimensions (scales) by which service users judge quality of care. The largest number of items was included in one of the scales (Table 3.1). The emergent scales were labelled: ‘Strengthens self-efficacy and control over care’ (11 items); ‘Personal relationships’ (6 items); ‘Respects me as a person’ (4 items); ‘Aspects of the delivery of the service’ (3 items). In order to reflect fully the range of relevant dimensions that service users employ in judging the quality of care, the 5 items that did not load on any of the factors were grouped together under the heading ‘Other considerations’. Each of the scales was found to be highly reliable illustrated by the Cronbach’s alpha coefficients for the scales (see Table 3.3 ).
Table 3.1 – Service User Questionnaire
Scale 1: Strengthens self-efficacy and control over care
Helps me to overcome barriers to achieving what I want for myself Works on goals that are meaningful to me Gives me the self-belief that I can achieve what I want for myself Gives me continuous support when I move from one service to another* Lets me know how to access help and support Enables me to work in partnership with healthcare professionals Responds promptly to my needs Is provided by healthcare staff who give me full information about my condition &
treatment Gives me correct contact information Helps me to understand my condition and the treatment options available Gives me the opportunity to express my views and be listened to
Scale 2: Personal relationships
Is provided by staff who are approachable Is provided by staff who put me at ease and make me feel comfortable is provided by people that I have got to know Is based on an open and trusting relationship with staff Makes me feel that I am genuinely cared for Explains things to me in a way that I can understand

© Leading to Quality 2013 – All rights reserved Page 37
Scale 3: Respect for me as a person
Does not make assumptions about me Treats me as an individual Treats me as a whole person with a focus on improving all aspects of my life Is provided by healthcare staff who are reliable
Scale 4: Aspects of Delivery of the service
Is located in places that are easy for me to get to Involves the right people in my care planning* Is delivered by people who tell me the truth
Other items
Makes me feel understood Makes sure that accurate information is accessible at all times Allows me to take as much time as I need during visits Takes the time to get to know me Involves me in making choices about my care
*denotes item not reflected in NICE Standards (see below) 3.1.4.2 Carer Quality of Care Questionnaire Corresponding analyses of the results of the Carer Quality of Care Questionnaires suggested that there are 2 dimensions (factors) relating to quality of care assessed by the questionnaire. The largest number of items was included in one of the factors (Table 3.2). The emergent scales were labelled: - ‘Provides support for carer’ (18 items); and ‘Respects and is committed to help the service user’ (11 items). Two questions did not load on either of the factors, but were retained so as to reflect fully the range of relevant dimensions that carers employ in judging the quality of care received by them and the person whom they support. Again, the scales were found to be highly reliable. The means, standard deviations, and Cronbach’s alpha-coefficients are shown in Table 3.4.
Table 3.2 – Carer Questionnaire
Provides support for Carer
Gives me correct contact information Makes sure that accurate information is accessible at all times Helps me to understand the condition and the treatment options available to the
person I care for Is based on an open and trusting relationship with staff Is provided by people that I have got to know Is provided by healthcare staff who give me full information about the condition and

© Leading to Quality 2013 – All rights reserved Page 38
treatment of the person I care for Allows me to take as much time as I need during visits Is sensitive to the stress of everyday living for carers* Makes me feel understood Involves me in the choices about the care offered to the person I care for Lets me know how to access help and support Is provided by staff who put me at my ease and make me feel comfortable Gives me the opportunity to express my views and be listened to Responds promptly to my needs Explains things to me in a way that I can understand Is provided by staff who are approachable Enables me to work in partnership with healthcare professionals Is provided by healthcare staff who are reliable
Scale 2: Respect for the Service User
Treats the person I care for as an individual Does not make assumptions about the person I care for Works on goals that are meaningful to the person I care for Treats the person I care for as a whole person with a focus on improving all aspects
of their life Takes the time to get to know the person I care for Gives the person I care for the self-belief that they can achieve what they want for
themself Makes the person I care for feel that they are genuinely cared for Helps the person I care for to overcome barriers to achieving what they want for
themself Gives the person I care for continuous support when they move from one service to
another Involves the right people in the care planning of the person I care for Is aware of what actions can upset the person I care for
Other items
Is delivered by people who tell me the truth Is located in places that are easy for me to get to
*denotes item not reflected in NICE Standards (see below) 3.2 What service users want from professionals The results are valuable in informing the delivery of high quality care in adult MH services because they identify:
what care should focus on achieving (the dimensions identified above);
how these goals can be achieved (the specific behaviours that professionals should enact, which are represented in the items).
3.2.1 Strengthens self-efficacy and control over care (Scale 1)

© Leading to Quality 2013 – All rights reserved Page 39
This scale assesses those aspects of MH provision that service users seek from professionals in relation to enabling them to achieve their personal goals. These include:
behaviours that strengthen their belief in their ability to do this;
providing service users with full information so that they can understand their condition and its treatment;
offering support;
working together in partnership. The findings endorse the value of professionals and organisations adopting the philosophy that underlies the ‘Recovery-orientated’ approach, which emphasises the importance of individuals’ rights of self-determination and choice by supporting them in building and maintaining a meaningful and satisfying life and personal identity (Shepherd, Boardman & Slade, 2008). It also reflects the guidelines provided in the Recovery Star® ‘Ladder of Change’ model (MacKeith & Burns, 2008) produced by the Mental Health Providers Forum, particularly the ‘identity and self-esteem ladder’ of personal growth and wellbeing. Such findings emphasise the point discussed below, in relation to the value of explicitly augmenting the NICE standard #1, ‘feeling optimistic about care’ (see below), and specifically: the importance of professionals focusing on individuals’ personal goals; strengthening their ability to control their care; and reinforcing the strength of their self-efficacy in relation to this. The one item that was unique to service users falls in this dimension and relates to their concern for seamless care when moving between services, which is included under the NICE standard ‘Continuity of Care’. In the current study, several constructs elicited from service users and carers during the repgrid interviews provided examples of what ‘continuous/seamless’ care implies, including:
good communication and team working between different members of the MH team, such that those standing in for a colleague when a particular professional was not available/on holiday were well-informed about the service user’s situation;
information being passed on to out-of-hours services, and the service users’ GP;
the importance of MH team members having good relationships and effective communication with other teams and agencies, so that, for example, “all the angles are taken into account when deciding treatment”, and between the MH team and relevant third sector/community organisations that could support the service users and their family, including when the service users makes a transition between services.
3.2.2 Quality of personal relationships with the professionals (Scale 2) This scale, and the group of items of which it is comprised, describes the importance to individuals of having a relationship with professionals in which empathy, genuine concern for the individual, and openness are clearly exhibited. It reflects the NICE standard #2, ‘Empathy, dignity, and respect’, and the basic tenets of the recovery model. 3.2.3 Respect me as a person (Scale 3)

© Leading to Quality 2013 – All rights reserved Page 40
This small group of items builds on the previous two dimensions, and can be related to the NICE standards and the recovery model. They emphasise the importance of care that is holistic in nature, and is particular to the individual and their perspectives, experiences, aspirations, and ‘whole life’ situation. 3.2.4 Aspects of delivery of care (Scale 4) The items in this scale serve to emphasise that care should be provided by the people most appropriate, who tell the truth, and offer provision in a location that is convenient to the service user.
3.2.5 Items that did not load on any of the 4 factors Although not readily relatable to the other scales, these items are, nonetheless, of relevance to service users, and valuable in their own right. Given the tenor of the dimensions described above, they add specific, additional, valuable information about the nature of high quality care. 3.3 What carers want from professionals These results are also valuable in informing the delivery of high quality care in adult MH services because they identify:
what care should focus on achieving
how these goals can be achieved (the specific behaviours that professionals should enact, which are represented in the items).
3.3.1 Support for carers (Scale 1) This scale reveals the nature of the support that carers seek from professionals and teams working with those for whom they care, including:
having correct contact information;
being provided with accurate information that enables the carer to understand the condition of the person for whom they care;
being involved in the possible choice of treatment;
being understood by professionals whom they know and who (a) understand their stresses and concerns, and (b) work in partnership with the carer.
These aspects of quality of care reflect the concept of the ‘Triangle of Care’ (Worthington & Rooney, 2012) which has been defined as ‘the therapeutic alliance between service user, staff and carer that promotes safety, supports recovery and sustains wellbeing’ (Worthington

© Leading to Quality 2013 – All rights reserved Page 41
& Rooney, 2010, p.3). It was originally developed by carers and professionals wishing to strengthen the engagement of carers to improve the quality of care in acute inpatient services. The model has, however, been extended to also include home treatment services. One of the reasons for its creation was the frequency with which carers “report that their involvement in care is not adequately recognised and their expert knowledge of the ‘well person’ is not taken into account” (Worthington & Rooney, op. cit., p.5). The model emerged from the desire of many carers to become ‘active partners’ within the care team. The importance of MH professionals paying heed to the emergence of this dimension in the current study can be ascertained in the following quote from the ‘Triangle’ publication:
“Carers say their wish to be effective is commonly thwarted by failures in communication. At critical points and in specific ways they can be excluded by staff and requests for helpful information, support and advice ‘are not heard” (p.6).
The unique item for carers was located in this 1st factor, and was “Is sensitive to the stress of everyday living for carers”. This would seem to emphasise the benefits of the ‘therapeutic alliance’ described as the ‘Triangle of Care’, also being extended to carers. Finally, in relation to this dimension, it is interesting to note that when items from the service users’ dimensions were mapped against those identified by carers, this 1st dimension reflects many of the items included in service users’ first 2 factors. 3.3.2 Respect for, and commitment to, the service user (Scale 2) The items in this scale echo the needs expressed by service users to be treated with genuine care, as an individual, about whom professionals should not make assumptions, and for whom the pursuit of their personal goals is of paramount importance. Also, in ways that strengthen their self-efficacy. 3.3.3 Items that did not load in the factors There were 2 items which did not load on the factors but which are, nonetheless, important and meaningful to carers. Interestingly, they were 2 (out of 3) of the same items to load on service users’ factor 4 regarding aspects of ‘Delivery of care’. They related to: being told the truth; and care being located in places that are easily accessible to carers. 3.4 Comparison of NICE Quality Standard for Service User Experience in Adult
Mental Health with Service Users’ and Carers’ Constructs of High Quality Care in the Present Study
It should be noted that the present research was undertaken prior to publication of the NICE Quality Standards (2011). A mapping exercise was undertaken to compare the constructs which emerged from users and carers in the Leading to Quality project with the standards published by NICE (See Appendix 3.2).

© Leading to Quality 2013 – All rights reserved Page 42
The constructs elicited by service users in this study matched the statements of the NICE Quality Standard, with the exception of Standard # 9, ‘Crisis Planning’. This might reflect the fact that while support for crisis planning was not stated explicitly by service users or carers, it is implicit in constructs such as: “gives advice when needed/when hit barriers”; “discusses what is happening to me”; “I am involved in discussions/decisions about care planning”; “I am given the right amount of information at the right time”; “everything is explained about my care”; “staff help me to understand my condition and treatments”; “staff let me know about other services I can access”; “I know how to access appropriate services when needed”; “staff respond promptly to my needs”; “information about my treatment is passed onto out of hours services”. 3.4.1 Aspects of high quality care not explicitly described in the NICE standards There appear to be some aspects of what service users and carers regard as high quality care that, while they relate to a particular standard, are not explicitly described in the NICE statements. These are marked with an asterisk in Tables 3.1 and 3.2. The NICE Standards, and the dimensions that emerged in the present study are as follows: NICE Standard #1: ‘Feeling optimistic about care’, for which the constructs elicited from service users and carers, identified the particular importance of professionals ‘building the service user’s sense of self-efficacy’. The concept of ‘optimism’ and ‘self-efficacy’ are related, but, importantly, are also distinct from each other. While ‘optimism’ refers to a positive belief in the future, self-efficacy refers to an individual’s belief that they can determine their future. The importance of this concept for wellbeing is stressed by the general psychological studies literature, having been initially identified by Canadian-born psychologist Alfred Bandura (1977), and written about extensively in the 1970s. It refers to the belief in oneself that one can succeed in one’s efforts to achieve tasks, and relates to a sense of control over one’s fate, and one’s sense of self-confidence. Research has found that individuals with high self-efficacy are more likely to take risks, such as trying out new behaviours; being pro-active in their behaviour; and striving to master a challenge they face, rather than avoiding it (e.g., Parker, 2000). In the field of mental health, it forms a critical component of the recovery-orientation to practice. The aim of this “is to support people to build and maintain a (self-defined and self-determined) meaningful and satisfying life and personal identity, regardless of whether or not there are on-going symptoms of mental illness (Shepherd, Boardman & Slade, 2008)…[and represents]...a movement away from a primarily biomedical view of mental illness to a holistic approach to wellbeing that builds on individual strengths (Davidson, 2008)… [Importantly, this approach to mental health care] “encompasses principles of self-determination and personalised care. Recovery-oriented practice emphasises hope, social inclusion, community participation, personal goal setting and self-management. Typically, literature on recovery-oriented practice promotes a coaching or partnership relationship between people accessing mental health services and mental health professionals, whereby people with lived experience are considered experts on their lives and experiences while mental health professionals are considered experts on available treatment services”.

© Leading to Quality 2013 – All rights reserved Page 43
(Extract from Framework for Recovery-Oriented Practice, State Government of Victoria, 2011, p.2). In the highly practical Users’ Guidelines to adopting the ‘Recovery Star’® ‘Ladder of Change’ model (MaKeith & Burns, 2011) the concept of self-efficacy is central to the ‘Believing’ stage, which follows the ‘Stuck’ and ‘Accepting Help’ stages, and precedes the ‘Learning’ and ‘Self-reliant’ stages. The Believing stage is characterised by the conviction that “we can make a difference ourselves in our life. We look ahead towards what we want as well as away from the things we don’t want. We start to do things ourselves to achieve our goal as well as accepting help from others” (MaKeith & Burns, 2011 p.2). Given the unequivocal importance of self-efficacy for mental health and wellbeing, it would seem to be of critical importance to include explicit reference to it in standards of quality of care. This point is reinforced by the analyses of what emerged from an analysis of service users’ responses to the questionnaire developed from the constructs, described above. NICE Standard #4: ‘Continuity of care’, for which the constructs elicited, identified the particular importance of professionals:
(1) ‘working together as an effective team’ (2) having good communications and effective inter-team relationships with other MH teams, and/or relevant agencies, including ‘uninterrupted care when moving between care services’. (1) The importance of ‘effective team working’ for MH teams, and effective inter-team and
inter-agency working, have been discussed in Chapter 1 of this report.
In an earlier longitudinal investigation of the impact of leadership in teams predicting their effectiveness, it was found that the extent to which crisis resolution teams embedded a culture of engaging leadership, significantly correlated with the motivation and morale of team members, and, importantly, predicted their productivity, as assessed by standardised ‘objective’ measures of performance (Alimo-Metcalfe et al., 2007, 2008, 2013). A recent study investigating the main factors affecting the effectiveness of multi-professional teams working in a national study of adult mental health services also found that the quality of intra-team working was a strong predictor of their effectiveness in delivering high quality care, as rated by team members (West et al., 2012). Among the most important characteristics of effective team working were team members participating in decision-making, trust among team members, social support, the frequency of meetings, and team leadership.
(2) In relation to the importance of effective inter-team working, interestingly, the same
study found that, while mental health professionals involved in the investigation did refer to the quality of communications and inter-team and inter-agency working as critical to the effectiveness of the teams participating in their study, and in particular, ‘clear and unambiguous referral processes, shared electronic service user records, joint meetings and less formal communication/individual relationships, shared premises, and a
© Leading to Quality 2013 – All rights reserved Page 44
willingness to reciprocate and be flexible’ (West et al., 2012, p. 103), these factors were not identified by the service users and carers who participated in their investigation.
The reason why the current study did obtain comments from service users and carers as to the importance of good communication and relationships with other teams might be a function of the methodology adopted; namely the use of the repertory grid technique, which was not the technique used in the national study. It might be that the repertory grid process encouraged individuals to be more analytical in their thinking, as they were required to make detailed comparisons, and reflect deeply (laddering), on the differences between the way in which different professionals interacted with them, and/or on specific intervention experiences. Another reason for the difference in findings might relate to the fact that since the repgrid interview was a private one-to-one discussion with the interviewer, under conditions of complete confidentiality, rather than a ‘public’ discussion in a focus group (used for the West et al, 2012 study), people felt less inhibited, and were encouraged, and enabled, to reflect more deeply on their experiences. Alternatively, it might have been because the people eliciting constructs from the service users and carers in the current study were themselves all highly experienced MH professionals. Or it could have been a combination of these factors, or, indeed, some other reason, which future research might reveal. The critical importance of continuous care when service users move between services was stressed in several constructs elicited from both service users and carers. It was also a major topic discussed in the national study of adult mental health teams (West et al., 2012), which included not only effective working between various agencies, but also with individuals’ GPs.
NICE Standard #8: ‘Care planning’. This was the subject mentioned most frequently by users and carers in the current study, and reflects strongly the NICE standard. However, it is important to stress that the focus of the care – namely that it is holistic in nature – was a prominent theme in the constructs elicited. This is reflected in constructs such as “will ask me about things other than my mental health (e.g. the garden, family)”; “gives practical advice about daily living (e.g., educational opportunities, advice with financial matters)”; “supports me to live a healthier lifestyle in general”. This ‘whole person’ approach is consistent with the recovery-orientation to mental healthcare which enables ‘an on-going holistic process of personal growth, healing and self-determination’ (Slade, 2009)... [and reflects]... ‘an overarching philosophy that encompasses notions of self-determination, self-management, personal growth, empowerment, choice and meaningful social engagement’ (State Government of Victoria, 2011, p.2). NICE Standard #10: ‘Assessment in a crisis’. The statement provided by NICE for this standard is: “Service users accessing crisis support have a comprehensive assessment undertaken by a professional competent in crisis working”. The current study obtained a large range of constructs which, unsurprisingly, made explicit reference to the quality of professionals involved in individuals’ care, but not only in relation

© Leading to Quality 2013 – All rights reserved Page 45
to ‘assessment in a crisis’. In general, the constructs referred to the professionals’ knowledge, competence and experience, their reliability, and consistency in doing what they say they will.
3.5 Quantitative analysis of the Quality of Care questionnaire results The following section examines the results of the service user and carer responses to the quality of care surveys. Table 3.3 presents the results of the service user questionnaire and Table 3.4 presents the results of the carer questionnaire.
Table 3.3 Service User Quality of Care Questionnaire Results The service I receive…
Scale 1: Strengthens self-efficacy and control over care (α-coefficients = .97) N Mean St.d* Enables me to work in partnership with healthcare professionals 427 5.05 1.06
Helps me to overcome barriers to achieving what I want for myself 436 4.81 1.16 Gives me continuous support when I move from one service to another 351 4.91 1.19
Helps me to understand my condition and the treatment options available 442 4.86 1.29
Gives me the opportunity to express my views and be listened to 446 5.16 1.03
Lets me know how to access help & support 448 5.11 1.04
Gives me correct contact information 443 5.14 1.02
Responds promptly to my needs 445 4.96 1.21 Is provided by healthcare staff who give me full information about my condition & treatment 441 4.91 1.27
Works on goals that are meaningful to me 442 4.94 1.10
Gives me the self belief that I can achieve what I want for myself 438 4.83 1.18
Scale 2: Personal relationships (α-coefficients = .96)
Explains things to me in a way that I can understand 446 5.14 1.06
Is provided by staff who are approachable 447 5.28 1.02 Is provided by staff who put me at ease and make me feel comfortable 447 5.18 1.12
Is based on an open and trusting relationship with staff 443 5.07 1.15
Makes me feel that I am genuinely cared for 447 5.09 1.18
Is provided by people that I have got to know 447 5.23 0.99Scale 3: Respect for me as a person (α-coefficients = .91)
Is provided by healthcare staff who are reliable 443 5.18 1.08
Treats me as an individual 449 5.22 0.99
Does not make assumptions about me 436 4.94 1.26 Treats me as a whole person with a focus on improving all aspects of my life 446 5.09 1.13
Scale 4: Aspects of delivery of the Service (α-coefficients = .86)

© Leading to Quality 2013 – All rights reserved Page 46
Is located in places that are easy for me to get to 429 4.92 1.28
Involves the right people in my care planning 422 5.07 1.16
Is delivered by people who tell me the truth 437 5.07 1.23
Other items
Takes the time to get to know me 449 5.15 1.07
Involves me in making choices about my care 440 5.00 1.15
Allows me to take as much time as I need during visits 437 4.86 1.22
Makes me feel understood 443 4.98 1.16
Makes sure that accurate information is accessible at all times 432 4.92 1.12
*St.d = Standard deviation
Green shading = top 5 score, Red shading = lowest 5 score
All questions are scored on a scale of 1-6 (1 = strongly disagree and 6 = strongly agree); 1 is the least positive score and 6 is the most positive score.
Comments on the Service User Quality of Care results Of particular interest here is the mean scores for the different items. The service user questionnaire results were extremely positive, which is very reassuring. They show that, on average, service users who responded to the survey felt very satisfied with the care they receive. The most positive items were in relation to personal relationships and respect for service users as people. This suggests that service users were very happy with the quality of the relationships they have with their professionals and the extent to which they were treated as individuals. It is interesting to note that the items that were the lowest scoring (although still positive) were the ones associated with increasing self-efficacy, which, as discussed below, are items that are very much related to the recovery model.
Table 3.4 Carer Quality of Care Questionnaire Results The service provided…
Scale 1: Respect for Service User (α-coefficients = .98) N Mean St.d*Treats the person I care for as a whole person with a focus on improving all aspects of their life 193 4.91 1.34
Does not make assumptions about the person I care for 184 4.95 1.22
Treats the person I care for as an individual 193 5.04 1.21
Works on goals that are meaningful to the person I care for 185 4.76 1.34
Takes the time to get to know the person I care for 192 4.91 1.35 Gives the person I care for the self belief that they can achieve what they want for themself 186 4.78 1.25
Helps the person I care for to overcome barriers to achieving what they want for themself 185 4.70 1.31
Gives the person I care for continuous support when they move from one service to another 156 4.62 1.49
Makes the person I care for feel that they are genuinely cared for 189 4.80 1.42
Involves the right people in the care planning of the person I care for 183 4.90 1.37

© Leading to Quality 2013 – All rights reserved Page 47
Is aware of what actions can upset the person I care for 185 4.90 1.33
Scale 2: Support for Carer (α-coefficients = .99)
Enables me to work in partnership with healthcare professionals 183 4.78 1.40
Gives me the opportunity to express my views and be listened to 190 4.78 1.37
Lets me know how to access help & support 192 4.89 1.38
Gives me correct contact information 193 5.04 1.22
Responds promptly to my needs 188 4.66 1.44
Is provided by healthcare staff who are reliable 188 4.91 1.28 Is provided by healthcare staff who give me full information about the condition & treatment of the person I care for 185 4.65 1.51
Is provided by people that I have got to know 189 4.78 1.40
Involves me in the choices about the care offered to the person I care for 190 4.57 1.57
Is based on an open and trusting relationship with staff 186 4.80 1.41 Helps me to understand the condition and the treatment options available to the person I care for 188 4.64 1.53
Allows me to take as much time as I need during visits 170 4.77 1.41
Makes me feel understood 190 4.75 1.43
Makes sure that accurate information is accessible at all times 189 4.63 1.45
Is provided by staff who put me at my ease and make me feel comfortable 189 4.95 1.38
Is provided by staff who are approachable 191 5.05 1.27
Explains things to me in a way that I can understand 189 5.03 1.25
Is sensitive to the stress of everyday living for carers 190 4.77 1.48
Other items
Is delivered by people who tell me the truth 178 5.01 1.22
Is located in places that are easy for me to get to 181 4.86 1.30
*St.d = Standard deviation
Green shading = top 5 score, Red shading = lowest 5 score
All questions are scored on a scale of 1-6 (1 = strongly disagree and 6 = strongly agree); 1 is the least positive score and 6 is the most positive score.
Comment on Carer Quality of Care questionnaire results While the results of the Carer Survey were positive, they were less positive than the service user results. The most positive areas emerging from the carer questionnaire were similar to the service user questionnaire, in that carers find professionals to be approachable and communicate in a way that carers can understand. Carers also think that the person they care for is treated as an individual. Areas in which carers felt less positive were in relation to how involved in and informed they were in the person they care for’s care, suggesting that work could be done on improving the “triangle of care”.
© Leading to Quality 2013 – All rights reserved Page 48
3.6 Conclusions This section describes findings in relation to one of the key aims of the current investigation, which was to identify what service users and carers regard as critical characteristics of high quality care. By employing the repertory grid interviewing process, and distilling the essence of the themes from the 450+ constructs into items forming a questionnaire, and then gathering responses from a wide range of users and carers as to their experience of care, and then analysing them using rigorous statistical methods, it has identified essential dimensions on which high quality care is judged. It has also identified the specific behaviours of professionals that result in such care. The analysis of the service user results showed that service users that responded to the survey felt very satisfied with the care they receive. The most positive items were in relation to personal relationships and respect for service users as people. It is interesting to note that the items that were the lowest scoring (although still positive) were the ones associated with increasing self-efficacy, which are items that are very consistent with the recovery model. The results of the Carer Survey were also positive but less positive than the service user results. The most positive areas emerging from the carer questionnaire were similar to the service user questionnaire, in that carers find professionals to be approachable and communicate in a way that carers can understand. Carers also think that the person they care for is treated as an individual. Areas in which carers felt less positive were in relation to how involved in/ informed about they were in the person they care for’s care. The research findings from this component of the Leading to Quality project adds to previous research, and contributes to the increased effectiveness of MH teams and professionals and, consequently, to high quality care provision in MH in several ways, including:
providing a much richer, more detailed, and comprehensive understanding of what service users and carers regard as important aspects of high quality care than has previously been published;
this serves to not only reinforce NICE guidelines regarding standards of care, but also provides explicit examples of how these can be enacted in care;
the identification of an aspect of care that is of crucial importance to service users, namely the importance of care that supports an individual’s sense of self-efficacy, which was not explicitly referred to in the NICE standard;
the development of 2 new ‘Quality of Care Questionnaires’– one for service users, and a separate one for carers, which are psychometrically robust and could be used across a range of mental health organisations to enable the standardisation of assessments of the quality of care provision.
It is clear, that given the evidence described above regarding the findings from this aspect of the Leading to Quality research, that outcomes should form a strong basis on which

© Leading to Quality 2013 – All rights reserved Page 49
professionals, teams, and organisations working in the area of adult mental health should focus their activities, reviews, feedback, and developmental interventions.
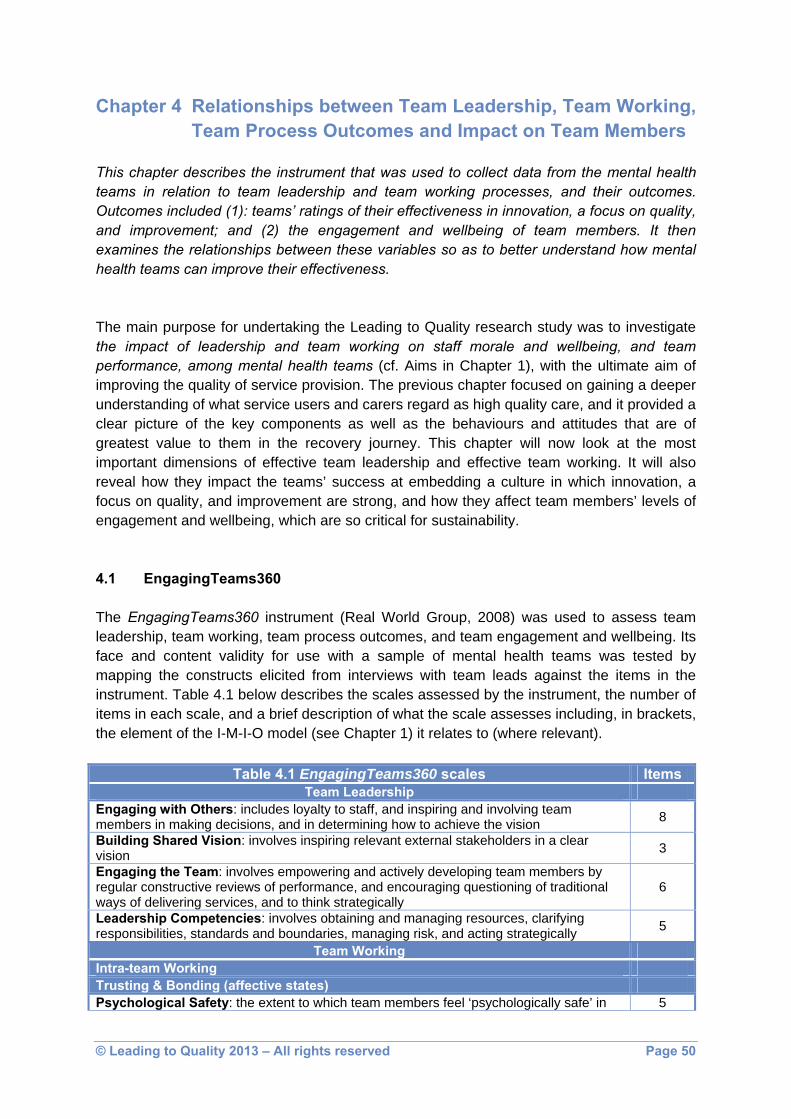
© Leading to Quality 2013 – All rights reserved Page 50
Chapter 4 Relationships between Team Leadership, Team Working, Team Process Outcomes and Impact on Team Members
This chapter describes the instrument that was used to collect data from the mental health teams in relation to team leadership and team working processes, and their outcomes. Outcomes included (1): teams’ ratings of their effectiveness in innovation, a focus on quality, and improvement; and (2) the engagement and wellbeing of team members. It then examines the relationships between these variables so as to better understand how mental health teams can improve their effectiveness. The main purpose for undertaking the Leading to Quality research study was to investigate the impact of leadership and team working on staff morale and wellbeing, and team performance, among mental health teams (cf. Aims in Chapter 1), with the ultimate aim of improving the quality of service provision. The previous chapter focused on gaining a deeper understanding of what service users and carers regard as high quality care, and it provided a clear picture of the key components as well as the behaviours and attitudes that are of greatest value to them in the recovery journey. This chapter will now look at the most important dimensions of effective team leadership and effective team working. It will also reveal how they impact the teams’ success at embedding a culture in which innovation, a focus on quality, and improvement are strong, and how they affect team members’ levels of engagement and wellbeing, which are so critical for sustainability. 4.1 EngagingTeams360 The EngagingTeams360 instrument (Real World Group, 2008) was used to assess team leadership, team working, team process outcomes, and team engagement and wellbeing. Its face and content validity for use with a sample of mental health teams was tested by mapping the constructs elicited from interviews with team leads against the items in the instrument. Table 4.1 below describes the scales assessed by the instrument, the number of items in each scale, and a brief description of what the scale assesses including, in brackets, the element of the I-M-I-O model (see Chapter 1) it relates to (where relevant).
Table 4.1 EngagingTeams360 scales Items Team Leadership
Engaging with Others: includes loyalty to staff, and inspiring and involving team members in making decisions, and in determining how to achieve the vision 8
Building Shared Vision: involves inspiring relevant external stakeholders in a clear vision 3
Engaging the Team: involves empowering and actively developing team members by regular constructive reviews of performance, and encouraging questioning of traditional ways of delivering services, and to think strategically
6
Leadership Competencies: involves obtaining and managing resources, clarifying responsibilities, standards and boundaries, managing risk, and acting strategically 5
Team Working Intra-team Working Trusting & Bonding (affective states) Psychological Safety: the extent to which team members feel ‘psychologically safe’ in 5

© Leading to Quality 2013 – All rights reserved Page 51
the contributions they make Social Support: the extent to which team members can call on others for emotional or other support, if required 5
Team Potency: the extent to which team members feel they have the capacity as a team to succeed in the tasks that are set 5
Valuing Different Perspectives: being open to minority views, rather than allowing ‘established’ perspectives to dominate 5
Supporting a Development Culture: ensuring there is a supportive, learning-orientated culture, rather than a culture of blame 6
Planning (behavioural processes) Information Gathering: gathering a wide range of relevant information 3 Roles and Responsibilities: having clear goals and objectives, coupled with knowing who is responsible for each task 4
Updating: ensuring that team members are kept up-to-date with current information, and have opportunities to discuss any problems that arise 5
Collective Experience: having opportunities for all team members to share specialist knowledge and experience, and to reflect on how to apply it 9
Adaptability: using the team’s resources in a strategic way, so as to deal with pressures and changes imposed from outside (iteration) 5
Inter-team Working Inter-team and Inter-agency Relationships: relationships based on mutual respect (affective); sharing information in a timely manner (behavioural); and understanding each others’ role
8
Inter-team and Inter-agency Collaboration: promoting inter-team collaboration (affective and behavioural); promoting inter-agency collaboration (affective and behavioural); and undertaking strategic planning
3
Outcome Variables Team Process Outcomes Innovation: thinking about new ideas and approaches; being open to change (iteration) 3 Focus on Quality: seeking feedback from service users and carers, so as to implement a shared vision of high quality provision (iteration) 4
Improvement: modifying current practice in the light of evidence; thinking through the implications of proposed change; working together to achieve improvements to the service provided (iteration)
8
Impact on Team Members Team Engagement: having a strong sense of team spirit, and commitment to the team 5 Wellbeing at Work: having a sense of job satisfaction and job fulfilment, and a low level of job-related stress 4
4.2 Results from EngagingTeams360 A total of 590 usable responses were available for analysis. The breakdown of the sample is presented in Appendix 2.2. Since the instrument was available in hard copy and was also available to download from the internet it is not possible to provide an accurate response rate. 4.2.1 Reliability The reliability of the EngagingTeams360 was tested and found to be high (Appendix 4.1).
4.2.2 Means and standard deviations

© Leading to Quality 2013 – All rights reserved Page 52
The means and standard deviations for the scales (Appendix 4.1) are represented in Figure 4.1 which illustrates the results graphically. Appendix 4.2 shows the scores in rank order. Figure 4.1
EngagingTeam360 overall sample results
5.3
4.25
4.91
4.61
4.55
4.72
4.74
5.01
4.99
4.87
4.58
4.99
4.76
5.04
4.99
4.71
4.71
4.76
4.71
4.78
4.71
1 2 3 4 5 6
Team engagement
Wellbeing at work
Innovation
Focus on quality
Improvement
Inter-team relations
Inter-team collaboration
Collective experience
Adaptability
Information gathering
Roles and responsibilities
Updating
Psychological safety
Social support
Team potency
Valuing different perspectives
Supporting a development culture
Engaging with others
Building a shared vision
Enabling the team
Leadership capabilities
Impa
ct o
nTe
amM
embe
rs Te
am P
roce
ssO
utco
mes
Inte
r-te
amW
orki
ng S
truct
urin
gan
dLe
arni
ng
Pla
nnin
g Tr
ustin
g an
d B
ondi
ng
Team
Lea
ders
hip
Mean
All items in the questionnaire were scored on a scale of 1-6, with 6 being the most positive score and 1 being the least. As can be seen from Figure 4.1, the results are extremely positive, being 4.5 or above, except in the case of Wellbeing at Work. Highest ratings:
The highest ratings were for:
Team Engagement, a Team process Impact measure, which includes a strong commitment to the job, the team, and each other, achieved a very high mean score,

© Leading to Quality 2013 – All rights reserved Page 53
and one that is much higher when compared to other comparable ratings in studies of mental health teams (e.g., Alimo-Metcalfe et al., 2007, 2008, 2013; West et al., 2012);
2 aspects of Trusting and Bonding: Social Support, which is concerned with supportive relationships within the team; and Team Potency, the extent to which the team believes in its capacity to succeed;
1 aspect of Planning: Updating, which relates regular face-to-face meetings to share information and experiences in relation to cases and other relevant information
2 aspects of Structuring and Learning: Collective Experience, concerned with sharing knowledge and experience so as to offer optimal provision to service users; and Adaptability, which is concerned with operating effectively under pressure;
1 Team Process Outcome: Innovation, which includes identifying new solutions to problems, or new ways of delivering services.
Lowest ratings:
The lowest ratings were for:
Wellbeing, which is critical for sustaining individuals’ motivation, job satisfaction, fulfilment, and general health
2 of the Team Process Outcomes (Improvement, and Focus on Quality, both of which are high on the DH agenda);
1 aspect of Planning (Roles and Responsibilities, which is concerned with issues that are fundamental to ‘genuine’ as opposed to ‘pseudo’ team working);
2 aspects of Trusting and Bonding (Valuing Different Perspectives, and Supporting a Development Culture, both of which reflect the culture that exists within the team;
1 Team Leadership scale: Building Shared Vision, which involves inspiring relevant external stakeholders in a clear vision.
Interpreting the ratings:
Four apparent themes emerge from an observation of the comparative ratings for the scales:
Focusing on the scales that fall within the ‘Team Working’ domain and comparing those rated highest (i.e., Social Support, Collective Experience, Updating, Team Potency, Adaptability), and those rated lowest (i.e., Roles & Responsibilities, Valuing Different Perspectives, Supporting a Developmental Culture) might suggest that the teams are particularly effective at supporting each other, in terms of:
- emotional support
- sharing their knowledge
- learning from each other
- sharing problems
- working together to deal with pressures and challenges,

© Leading to Quality 2013 – All rights reserved Page 54
and that this leads to them having a strong confidence in their resilience, ability to work together effectively, achieve goals, and to succeed as a team (i.e., Team potency) and as a result, to be open to change and trying new ways of delivering services (Innovation). Research shows that as team potency develops, so do team members’ willingness to work harder and more innovatively to enable the team to succeed (McDowell & Zhang, 2009). Such strengths also refer to the ability to adapt to change and suggest a ‘high readiness for change’ in the teams, and is consistent with the research literature in this area (e.g., Cunningham et al., 2002). Furthermore, these findings, combined with the high levels of social support that emerged - which includes loyalty, reliability, cohesiveness and collaboration - would also explain the high levels of Team Engagement, of which one key component is strong sense of team spirit. There is now substantial research providing evidence of the benefits of engagement to individuals, teams, and organisations (e.g., Alimo-Metcalfe & Alban-Metcalfe, 2008; Macleod & Clarke, 2009; Wollard & Shuck, 2011). 1. In comparison, the lowest rated scales in relation to ‘Team Working’ (Roles &
Responsibilities, Valuing Different Perspectives, Supporting a Developmental Culture), are more difficult to interpret.
Firstly, it should be noted that although all of these ratings were 4.55 or above - apart from Wellbeing (4.25) which is the lowest rated of all 21 scales (discussed below under point 4) - this study is about identifying ways in which team effectiveness can be improved. One way of identifying a theme in these scales is by reflecting on how the team strengths, described above, appeared to emphasise the relational behaviours, attitudes and beliefs in the teams, about themselves as individuals working together effectively. The lowest rated scales include the scale of Roles & Responsibilities which relates to:
- having a manageable number of well-defined goals
- being clear about the team’s goals and sense of direction
- having clearly defined processes and procedures
- having a clear understanding of each other’s roles and responsibilities. Valuing Different Perspectives is about being open to each other’s ideas, valuing their knowledge and expertise and ensuring that all views are listened to and considered, irrespective of whose views, and whether they agree or not. It is also about ensuring discussions are not unduly dominated by a particular person or profession. Supporting a developmental culture includes being tolerant of others’ failings and using mistakes as learning opportunities, rather than a cause for blame, sharing problems or mistakes openly, and giving and receiving developmental feedback. The theme here can be seen to be a more task, and/or information, knowledge and decision-focused set of behaviours. Perhaps the lower ratings on these scales explain the fact that Improvement was rated the 2nd lowest of all 21 scales, and that a Focus on Quality was 4th lowest. The Improvement scale includes items which refer to the team meeting regularly to discuss the team’s criteria for judging success, modifying the way the team works in the light
© Leading to Quality 2013 – All rights reserved Page 55
of feedback, making evidence-based decisions, and thinking through the implications of new systems and processes for improving services. The higher ratings related more to relations within the team, the lower rated items are more clearly focused on performance, quality, and improvement. 2. The rating for the Team Leadership scale of Building Shared Vision was one of the
lowest-rated scales. It relates to inspiring relevant external stakeholders to share in a clear, common vision.
It is informative to look at this result in the context of the ratings for 2 other scales which relate directly to working with external stakeholders. These are the Inter-team & Inter-agency Relations and the Inter-team & Inter-agency Collaboration scales, since their ratings were around the relatively low, to medium, rated group.
The ‘Relations’ scale is concerned with:
- mutual respect
- understanding each other’s roles and context
- sharing information
- being open to receiving feedback
- attempting to achieve a win-win solution to potential conflicts.
The ‘Collaboration’ scale is concerned with better meeting service users’ needs by:
- being proactive in promoting inter-team collaboration within the trust
- promoting collaboration with other agencies
- undertaking strategic planning in relation to the ways in which teams and agencies can collaborate more effectively.
This ‘triumvirate of scales’ (Building Shared Vision, Inter-team/agency working) suggests the need to pay greater attention to working closely with other teams and agencies, for the benefit of service users. The enormous importance of inter-team and inter-agency working for improving services for users, and ensuring that they experience continuous and seamless care, is indisputable, and is reinforced by the NICE Guidelines (2011) referred to in the previous chapter. Indeed, good support services, and good communication between various agencies, was one of the 7 key themes to emerge from an analysis of what users and carers believe high quality care to be (cf. Chapter 3). As such, it goes to the heart of the Leading to Quality project. Furthermore, in the context of current dramatic changes in the NHS, where inter-agency working will be critical for supporting high quality services, these findings need to be considered with urgency.

© Leading to Quality 2013 – All rights reserved Page 56
Moreover, as shall be seen in a section below, the evidence from this study is that the extent to which teams are effective in relation to the behaviours represented in these scales, has a significant impact on their innovation, focus on quality, and improvement. 3. The final theme, and an equally critical one for the teams, is that the lowest rating of all
21 scales, was that of team member Wellbeing at Work. This also revealed the largest difference between the ratings of scales as they progressed in rank order (cf., Appendix table 4. 2). It had a conspicuously lower score than the second lowest item. The results appear to send a strong message from the team members in relation to their feelings about their job/work situation. Apart from the damage to their own health, there is clear evidence from data collected in the NHS published in the report ‘NHS Health & Wellbeing’ (Boorman, 2009) of a relationship between the stress experienced by staff and its effect on patient care. This is in no way intended to imply that this will lead directly to reduced quality of care for service users. However attention must be paid to what may be the consequences for highly committed staff, if their levels of satisfaction, fulfilment and wellbeing are relatively low, and their job-related stress is high.
There is a plethora of research evidence in the field of organisational psychology, of a significant link between job satisfaction and work performance (e.g., Judge et al., 2001). Given the unprecedented level of change and challenge facing the NHS, the need for resilience is crucial. A final comment in relation to the highest and lowest mean scores for the scales is how unusual it is to see that in a range of 21 scales, the ‘Team Engagement’ score is the highest, and the ‘Wellbeing’ score the lowest. Typically, these concepts are strongly related (Maslach 2011; Maslach & Leiter, 2008). In view of the patterns that have been observed in the data and described above, it may be the case that the strength of team spirit and sense of social support, and strong collaboration among team members is buffering them from the personal impact of their work/jobs, and enabling them to continue to be highly engaged. However, the question must be posed: for how long can this be sustained if the negative experiences of their job are not ameliorated? This, and the other issues raised above, suggest that this is a matter on which all those
in a leadership role in teams should reflect, with urgency. This section has been based on a discussion of the simple comparison of higher versus lower-rated scales, and some interpretation offered. The next sections are based on what emerged from more complex statistical analyses of the relations between the scales, and the practical implications for teams and team development. 4.3 What do we know about team working?
As noted in Chapter 1, one of the issues about which the literature appears to be relatively silent is the relationship between team leadership and team working in the impact on team members’ level of engagement and wellbeing at work, and on team performance.
© Leading to Quality 2013 – All rights reserved Page 57
At issue, is whether:
team leadership has a direct impact on team engagement and wellbeing at work (as is evident from the findings of Alimo-Metcalfe and colleagues, 2007, 2008);
team working has a direct impact on team process outcomes (as is evident from the findings of West and colleagues (2012), and others);
team leadership has a mediating (moderating/influencing), rather than a direct effect, on the relationship between team working and impact on staff and team performance; or
team working has a mediating effect on the relationship between team leadership and impact on staff and team performance.
While this may sound rather technical, the answer to these questions is central to the investigation and its aims to improve team effectiveness, since:
it is essential to understand what has the greatest impact on team performance, and on team engagement and wellbeing – the latter of which significantly affect and sustain performance, and
such information can help guide the way in which the development of leadership and team working can be offered most effectively.
A statistical procedure known as structural equation modelling (SEM) calculates the relationship between variables to enable a researcher to establish whether certain variables (e.g., team leadership) have a direct impact on, for example, team performance, or whether other variables have a greater impact. Technical aspects of this are presented in Appendix 4.3. Figure 4.2 shows a diagrammatic representation of how various aspects of team leadership and team working contribute to the outcomes of team working (Innovation, Focus on Quality, Improvement) and impact on team members (Team Engagement and Wellbeing at Work).
Thus, as Figure 4.2 indicates, there is significant evidence for the following conclusions to be drawn:
team working is very much more than a behavioural process;
different aspects of building trust within the team and the extent to which the team bonds together as an effective, respecting and respectful functioning unit, have a profound impact not just on the team members’ level of engagement and sense of wellbeing, but also on the team process outcomes (affective states);
different aspects of sharing knowledge and expertise within the team, and using the shared mental models that emerge so as to provide optimal MH and related provision, also have a profound impact on team members and team performance (cognitive states);
inter-team and inter-agency working also has, consistent with a growing body of evidence, a very important role to play in that it impacts particularly on the team process outcomes (Innovation, Focus on Quality, Improvement);
team leadership does not operate ‘directly’, in a vacuum (as it were), but rather that its impact is through the actions of those in a leadership role on their team.

© Leading to Quality 2013 – All rights reserved Page 58
The last point about team leadership is especially important as the present study presents empirical evidence that:
team leadership and team working are not just correlated (as shown in many other studies), but that team leadership has an impact on team working;
that, in combination, team leadership and team working have an impact on both team process outcomes (Innovation, Focus on Quality, and Improvement) and on team members’ Team Engagement and Wellbeing at Work
supports theoretical arguments in favour of providing context-related, in-situ leadership development (e.g., Alban-Metcalfe & Alimo-Metcalfe, 2010; Bennington & Hartley, 2009).
4.4 Product-moment correlations 4.4.1 Relationship between team leadership and team working, and team process
outcomes and impact on team members
In order to examine further the relationships between the independent variables (Team Leadership and Team Working) and the dependent variables (Team Process Outcomes and Impact on Team Members), product-moment correlations were calculated between the two sets of variables (Appendix 4.4).
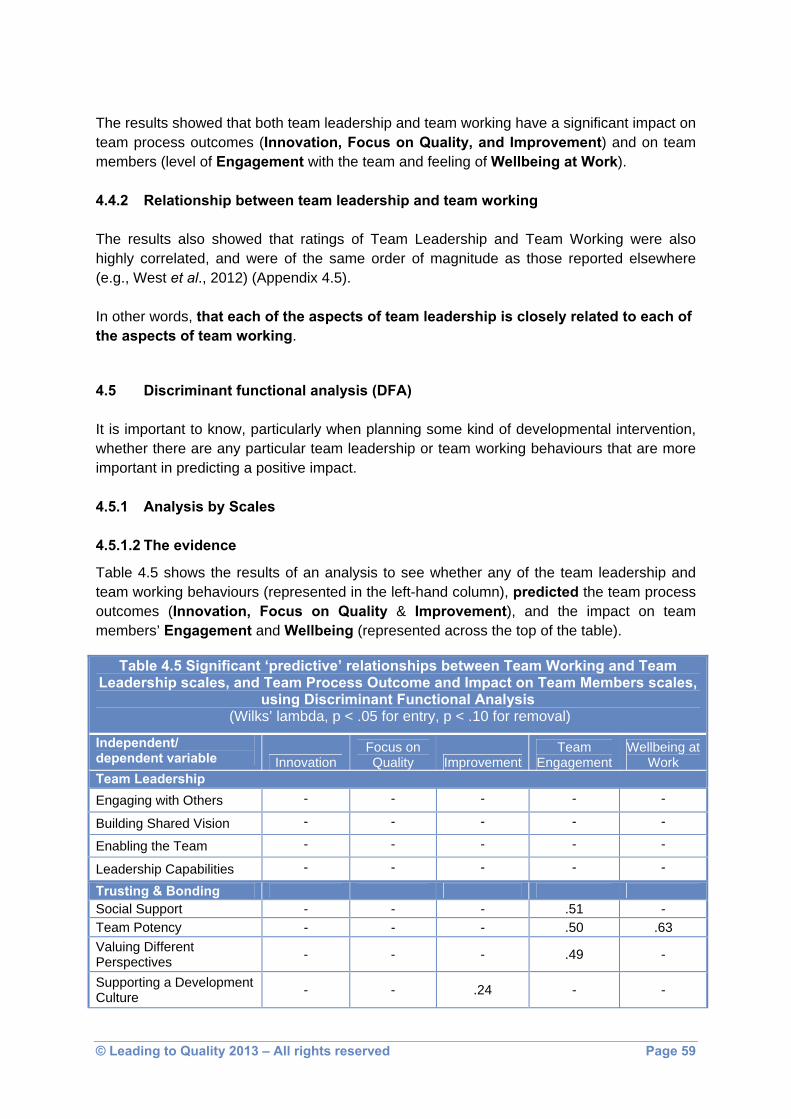
© Leading to Quality 2013 – All rights reserved Page 59
The results showed that both team leadership and team working have a significant impact on team process outcomes (Innovation, Focus on Quality, and Improvement) and on team members (level of Engagement with the team and feeling of Wellbeing at Work). 4.4.2 Relationship between team leadership and team working
The results also showed that ratings of Team Leadership and Team Working were also highly correlated, and were of the same order of magnitude as those reported elsewhere (e.g., West et al., 2012) (Appendix 4.5).
In other words, that each of the aspects of team leadership is closely related to each of the aspects of team working.
4.5 Discriminant functional analysis (DFA) It is important to know, particularly when planning some kind of developmental intervention, whether there are any particular team leadership or team working behaviours that are more important in predicting a positive impact. 4.5.1 Analysis by Scales 4.5.1.2 The evidence
Table 4.5 shows the results of an analysis to see whether any of the team leadership and team working behaviours (represented in the left-hand column), predicted the team process outcomes (Innovation, Focus on Quality & Improvement), and the impact on team members’ Engagement and Wellbeing (represented across the top of the table).
Table 4.5 Significant ‘predictive’ relationships between Team Working and Team Leadership scales, and Team Process Outcome and Impact on Team Members scales,
using Discriminant Functional Analysis (Wilks’ lambda, p < .05 for entry, p < .10 for removal)
Independent/ dependent variable Innovation
Focus on Quality Improvement
Team Engagement
Wellbeing at Work
Team Leadership Engaging with Others - - - - -
Building Shared Vision - - - - -
Enabling the Team - - - - -
Leadership Capabilities - - - - -
Trusting & Bonding Social Support - - - .51 - Team Potency - - - .50 .63 Valuing Different Perspectives - - - .49 -
Supporting a Development Culture - - .24 - -

© Leading to Quality 2013 – All rights reserved Page 60
Independent/ dependent variable Innovation Focus on
Quality Improvement Team Engagement
Wellbeing at Work
Planning Roles and Responsibilities - .35 .24 - .61 Structuring & Learning Collective Experience - - .23 - - Adaptability - - .24 - - Inter-team Working Inter-team Relations .36 .34 .24 - - Inter-team Collaboration - .33 - - - What these analyses show is that, in relation to team working:
Team Potency significantly predicts, both, Team Engagement and Wellbeing at Work;
Social Support and Valuing Different Perspectives significantly predict Team Engagement;
Supporting a Developmental Culture significantly predicts team process outcome measure of Improvement.
These are measures of ‘affective states’, or degree of emotional involvement and feeling of being supported.
Roles and Responsibilities was a significant predictor of two aspects of team process outcomes (Focus on Quality, and Improvement), and of one aspect of impact on team members (Wellbeing at Work)
These are measures of ‘behavioural processes’, or the extent to which the team functions effectively and efficiently.
Collective Experience and Adaptability were each significant predictors of one aspect of team process outcomes (Improvement)
These are measure of ‘cognitive states’, or the extent to which the team shares its collective knowledge and experience openly, so as to ensure that the highest quality of provision is offered to service users and carers.
Inter-team and Inter-agency Relations was a significant predictor of all three aspects of team process outcomes, namely, Innovation, Focus on Quality, and Improvement.
Inter-team and Inter-agency Collaboration, was a significant predictor of Focus on Quality.
These are measures of inter-team and inter-agency working, or the extent to which the team shares information and approaches with other teams and agencies, so as to ensure a more holistic MH and related provision.
4.5.1.2 Practical implications of the findings from the data analysis It is important to note that, of the intra-team working scales that have been found to significantly predict team process outcomes (Innovation, Focus on Quality, and

© Leading to Quality 2013 – All rights reserved Page 61
Improvement) and Team Engagement and Wellbeing, 3 of the 7 are scales that were rated lowest. At a practical level, this means that information from this kind of analysis can serve as a valuable starting point for an intervention, because:
it has identified the scales that have the strongest links between team leadership and team working behaviours, and their impact in terms of team members’ level of Engagement and Wellbeing in terms of team process outcomes (Innovation, Focus on Quality, and Improvement);
it points to the aspects of team working, which, if strengthened, will achieve the most significant impact on these outcomes;
it also identifies the 2 Inter-team/agency scales, as important areas for increasing team effectiveness.
The next section looks at whether an analysis at an item level (rather than a scale level) can provide more specific information as to how best strengthen team effectiveness.
4.5.2 Analysis by Items In order to provide information about which actual behaviours had an impact on team process outcomes and/or impact on team members, DFAs were also carried out using the items of those scales that had a significant predictive link with an outcome variable. The results are described below and presented in Appendix 4.6.
4.5.2.1 Intra-team Working
Two of the items in the Roles and Responsibilities scale were significant predictors of three measures of team output/impact on staff (Focus on Quality, Improvement, and Wellbeing at Work):
‘Are clear about the team's goals and sense of direction’, and
‘Have a manageable number of well-defined goals’,)
Two other items significantly predicted Wellbeing at Work:
‘Have clearly defined processes and procedures’, and
‘Have a clear understanding of each other's roles and responsibilities’ 23 different items were significant predictors of Improvement. These were from 4 intra-team working scales, namely Roles and Responsibilities (note above), Collective Experience, Supporting a Development Culture, and Adaptability, and from both inter-team and inter-agency working scales. The evidence of the significant effect of the items in the Roles and Responsibilities scale is wholly consistent with ‘genuine’ (rather than ‘pseudo’) teams (West et al., 2003) being associated with high quality performance and fewer errors in the NHS (Dawson, 2007).

© Leading to Quality 2013 – All rights reserved Page 62
That Improvement should be predicted by a large number of items (specific behaviours) is not surprising given the complex nature of improvement in organisations, such as the NHS, where a large number of, sometimes counter-veining, factors can have a significant impact on what is achieved – or even tackled! This complexity is, perhaps, most evident among MH teams, which are not only multi-disciplinary, but also work closely with other teams and agencies. Indeed, there is evidence of an increase in the ways that MH teams comprise team members who are employed by agencies other that the NHS, notably local government (van Knippenberg et al., 2007). A total of 7 items were significant predictors of Team Engagement. (Next to each scale is a note as to whether it was rated among the higher or lower scales, or in the mid-range):
Two were from the Social Support scale (high):
- ‘Show great loyalty to the team’
- ‘Work collaboratively & cohesively as a team’
Two were from the Team Potency scale (high):
- ‘Are confident as a team in our ability to work effectively together’
- ‘Are confident in our ability as a team to achieve our goals’.
Three were from the Valuing Different Perspectives scale (low):
- ‘Are open to ideas from all team members’
- ‘Value the particular knowledge and experience that each team member can offer’
- ‘Ensure that team decisions are not unduly influenced by more 'vocal' or more 'high status' team members’
Given that Team Engagement, as measured here, is a reflection of a belief that other team members will offer support, the items (intention to stay, commitment to job and to the team, and team spirit) are in line with expectations. That Social Support and Team Potency predicted Engagement, is consistent with previous research on CRTs (Alimo-Metcalfe et al., 2007, 2008; Schaubroeck et al., 2007). The items from both scales were concerned with how cohesive and collaborative the teams were, which would no doubt impact on their sense of collective identity, and confidence in each other (McDowell & Zhang, 2009). The items from the Valuing Different Perspectives scale that were significant predictors of Team Engagement were concerned with openness, valuing, and ensuring that all could participate/engage in team decisions.
4.5.2.2 Inter-team & Inter-agency working
In the light of the increasing importance of inter-team and inter-agency working, it is not surprising that no fewer than 8 inter-team working items were significant predictors of Improvement.
Six items were from Inter-team and Inter-agency Relations scale (mid-range):

© Leading to Quality 2013 – All rights reserved Page 63
‘Resolve conflicts with other teams and/or agencies by attempting to see both sides of an argument’
‘Seek to understand the different policies and procedures with which other teams and/or agencies have to comply’
‘Strive to achieve a non-bureaucratic approach to inter-team and/or inter-agency communication’
‘Give and are open to receiving feedback from other teams and/or agencies’
‘Seek to develop a shared understanding of the role of our own and other teams and/or agencies in providing for service users and carers’
‘Seek to establish face-to-face communication with staff in other teams and/or agencies’
Two items were from the Inter-team and Inter-agency Collaboration scale (mid-range):
‘Undertake strategic planning in relation to the ways in which teams and agencies can collaborate more effectively in meeting service users' needs’
‘Are proactive in promoting inter-team collaboration, within the Trust, to meet service users' needs’
There were also 5 items from the Inter-teams and Inter-agency Relations scale that predicted Innovation, and 5 that predicted Focus on Quality. These findings are wholly consistent with research cited in Chapter 1 about the impact of the quality of inter-team and inter-team working relations, evidenced in: inter-group collaboration and frequent task-related contact between teams (Richter et al., 2006); the team leader’s negotiation style (Richter et al., 2005); frequency and quality of contact (Allport, 1954; Pettigrew & Tropp, 2006, 2011), and in contrast to the hindering effect of ‘structural’ variables, such as inter-group competition (e.g., Mohrman et al., 1995), and inter-group hostility (Hogg & Terry, 2000). The wider implications, at a highly practical level, of this kind of analysis, particularly where the data come from a single organisation, are that:
the information and insights gained can provide detailed information about which specific team working actions can impact on team members’ level of engagement and wellbeing, and team performance; and
this information can contribute to identifying a starting point for an intervention, because it points to specific actions that have an impact on team members’ level of engagement and wellbeing, and team performance.
4.6 The effect of contextual factors Of 12 contextual factors examined, seven were found to have a significant impact on different scales. 4.6.1 Size of team
© Leading to Quality 2013 – All rights reserved Page 64
A consistent pattern emerged, such that the smaller the team (up to a maximum of 10 team members), the higher the mean scores on each of the scales. The relationship between team size and ratings on the scales was linear, with teams with 30 or members being rated lowest on each of the scales (Appendix 4.7). The reason for this may be that the larger teams do not actually function as ‘genuine’ teams (clear team objectives; interdependent working; and regular meetings to discuss effectiveness). The implications of these findings are:
the extent to which larger teams meet the criteria for being ‘genuine’ teams should be explored;
such a clear, linear relationship between team size and (a) ratings of team leadership and team working, and (b) ratings of team process outcomes and impact on staff, is a matter that may be something to consider in future organisational and service redesign decisions.
4.6.2 Ratio of occupational therapists and social workers to nursing staff Once again a consistent pattern emerged, such that in this case the highest ratings on each of the scales were among teams in which the ratio of occupational therapists and social workers to nurses was between 35% and 50% (Appendix 4.8). This finding can be related to what is at the heart of multi-disciplinary team working. That is:
- that multi-disciplinary teams can draw on the wide (and often unique) knowledge and expertise that team members from different professional backgrounds can offer;
- consequently, more informed and better decisions can be taken.
This said, this potential value is not always realised, and should not, therefore, be taken for granted (e.g., Hambrick et al., 1996; Murray, 1989; Salas et al., 2009; Simons et al., 1999). As discussed in Chapter 1, diversity in teams, including professional diversity, can lead to ‘faultines’ (Lau & Murnighan, 1998), which can divide rather than strengthen teams; however, a team sharing the same vision and goals can attenuate the destructive potential. Team leadership plays a crucial role in this process through creating a culture of mutual respect and shared learning. Overall, the implications of the findings include that:
at a systemic level, there is the need to recruit teams that comprise an appropriate range and ratio of relevant disciplines;
the most appropriate range and ratio will vary with the type of team;
at an intra-team level, those in a leadership role need to be active in promoting their team’s capabilities in areas such as quality of communication, and decision-making;
again, at an intra-team level, those in a leadership role need to be active in promoting a team culture that is supportive, learning-orientated, and is based on trust, respect,

© Leading to Quality 2013 – All rights reserved Page 65
mutual understanding, the valuing of others, and belief in the team’s potential to succeed;
at an inter-team and inter-agency level, for those in a leadership role to be active in promoting genuine partnership, recognising that each team may not possess all the discipline-related knowledge and experience required to provide service users with the best quality of MH and related provision;
effective inter-team and inter-agency working is based on both shared capabilities and culture;
those in a leadership role need to be sensitive to, and respond appropriately to, any kind of inter-disciplinary conflict.
It follows from this that there is a need to determine those discipline-related factors that promote and support effective team working, and those that impede or prevent it. 4.6.3 Case load The pattern that emerged here was the ratings by teams in which the case load was between 10 and 19 were either the highest or joint highest on 10 of the 11 scales (Appendix 4.9). In addition:
On 8 of the scales, ratings by teams with a case load fewer than 10 were either highest (for Wellbeing at Work), jointly highest, or second highest.
On 2 of the scales (Team Leadership and Planning), the second highest ratings were by teams with a case load of more than 30.
The lack of linear relationship between caseload and effective team working may reflect that the impact of caseload is not just about numbers, it is also about the nature and intensity of the caseload. Thus, for some service users, the amount of contact is low, for others it is high. In other words, any meaningful statistic should reflect both the size and the nature of the case load. The implications in terms of case load are that:
it will be instructive, when considering the ratio of MH staff to cases, to recognise, and to try to quantify, the quality of the provision that each service user needs;
the practice found among several teams was that they have ‘weighted’ case loads, such that the intensity of the care provision required is taken into account as well as numbers.
4.6.4 Age of team, length of time team leader in post, & quality of accommodation Although data were collected in relation to each of these variables, detailed examination of the evidence pointed to a lack of comparability between the data provided by the teams.
4.7 Conclusions The evidence presented in this chapter provides clear support for the following conclusions: Team leadership

© Leading to Quality 2013 – All rights reserved Page 66
the mean ratings on each of the four team leadership scales (Engaging with Others, Building Shared Vision, Enabling the Team, and Leadership Capabilities) were of the same order of magnitude as found in comparable studies;
quality of the leadership of multi-disciplinary teams is significantly correlated with
- 10 aspects of intra-team working, which assess (1) relationships within the team, such as trust and a supportive team culture, (2) the processes involved in team work, such as being clear about tasks and roles and responsibilities, and (3) the extent to which team members share their knowledge and experience openly, so as to offer an optimal quality of care;
- 2 aspects of inter-team and inter-agency Working: quality of Relationships and Collaboration;
- 3 aspects of team output: Innovation, Focus on Quality, and Improvement;
- 2 aspects of the impact on team members: Team Engagement and Wellbeing at Work.
Team working
the mean ratings on the team working scales were also of the same order of magnitude as found in other comparable studies;
that quality of the leadership of team working is also significantly correlated with:
- 3 aspects of team process outcomes: Innovation, Focus on Quality, and Improvement;
- 2 aspects of the impact on team members: Team Engagement and Wellbeing at Work.
ratings on certain of the intra-team and inter-team and inter-agency scales were significant predictors of certain elements (scales) of team process outcomes and impact on team members;
ratings on certain of the intra-team and inter-team and inter-agency items were significant predictors of certain elements (scales) of team process outcomes and impact on team members;
such whole scale, and individual item, predictive information can provide a valuable starting point for a practical intervention;
Team process outcomes
the mean ratings on the team process outcome scales (Innovation, Focus on Quality, and Improvement) were also of the same order of magnitude as found in comparable studies; but
while the ratings for Innovation were relatively high, those for Focus on Quality, and Improvement were either the lowest and third lowest (of 21 scales) measured here;
that this last finding is a matter of concern, particularly as these outcomes are high on the DH agenda.
Impact on team members mean ratings on the impact on team member scales (Team Engagement and
Wellbeing at Work) were also of the same order of magnitude as found in comparable studies;

© Leading to Quality 2013 – All rights reserved Page 67
mean ratings for Team Engagement were the highest (of 21 scales); but mean ratings for Wellbeing at Work were the lowest – a matter that should be of
considerable concern (1) in itself, and (2) because these are only average ratings for the sample as a whole, and merits action.
Relationship between team leadership and team working
consistent with the findings of others, team leadership and team working were significantly correlated;
the evidence indicates that, contrary to what was expected, team leadership acts through team working, rather than directly on team process outcomes (Innovation, Focus on Quality, and Improvement), and on team members (Team Engagement and Wellbeing at Work);
that this finding has important implications for the nature of team leadership development, and the context in which it is offered.
4.7.1 Bringing the evidence together This chapter describes findings which relate directly to the key aim of the Leading to Quality study, which is: “to investigate the processes and key factors for effectiveness, leadership and team working in the delivery of community mental health services”. Based on a sample of 590 team members from MH trusts across Yorkshire and the Humber, the overall findings reported in this chapter:
Demonstrate positive levels of team leadership, team working and team engagement across the region;
provide valuable information as to relative areas of strength, and those for development;
provide important insights into specific and differential ways that team leadership and team working have an impact on team members and on team performance, and
point to practical actions that can be taken to increase the effectiveness of MH teams.

© Leading to Quality 2013 – All rights reserved Page 68
Chapter 5 Case study Data and Analysis
This chapter reports on the findings from the six case studies conducted as part of the research. It has seven main parts:
5.1 Introduction and methodology
5.2 Effective team working
5.3 Effective leadership
5.4 Staff wellbeing and engagement
5.5 Quality of Care
5.6 Synthesis of the quantitative and qualitative data
5.7 Summary of findings and conclusions
The chapter incorporates and builds on the findings from Chapters 3 & 4, illustrating their practical relevance to leadership, team working, staff engagement and wellbeing and quality of care.
The findings are discussed in relation to the model below.
Essentially, what the model shows is that:

© Leading to Quality 2013 – All rights reserved Page 69
Effective team working was perceived to be critical to staff wellbeing and engagement, to quality of care for service users, and to team process outcomes;
Leadership mediated the effective team working to have this impact but also was felt to independently impact on staff wellbeing and engagement, on quality of care and on team process outcomes;
Staff wellbeing and engagement, and team process outcomes had an independent impact on quality of care but this relationship was also mediated through effective team working and effective leadership.
The model is, on the whole, consistent with the model to emerge from the quantitative results in Chapter 4; however, as discussed, this model did not provide a direct causal link between leadership and staff engagement and wellbeing.
5.1 Introduction and methodology 5.1.1 Introduction to case study approach The case study approach is particularly suited to research that requires a detailed understanding of social or organisational processes because of the rich data collected in context (Hartley, 2004). Case studies use multiple methods, of which the different data sources are used to triangulate the findings, therefore increasing the validity of the results. As such, the case studies enabled us to examine team working and leadership processes in-depth and in context and, therefore, added substance to the data that the quantitative research provided.
5.1.2 Methodology It was decided that the case studies would be a series of best practice case studies, focusing on the positive aspects of leadership and team working in community mental health teams. As such, the case study teams were selected based on the results from the EngaginTeams360, with, where possible, the team with the most positive questionnaire results being selected for the case study. Six case studies were conducted in total – one from each of the participating trusts that had a sufficient response rate to select a best practice team. The researchers spent one or two days with each of the case study teams collecting data. The case studies primarily consisted of semi-structured interviews with team members and the team lead (TL); where possible observations of the teams in their natural environment and observations of team meetings were undertaken. Across the six teams 46 interviews were conducted. Interviews were undertaken with the team lead and with other staff within the team, including a variety of different roles (nurses, occupational therapists, social workers, psychiatrists, support workers, administrators, and therapists).

© Leading to Quality 2013 – All rights reserved Page 70
5.1.3 Grounded Theory A grounded theory approach was adopted to conduct the case studies. Grounded theory is a systematic methodology in the social sciences involving the discovery of theory through what emerges from the analysis of data, rather than starting with a pre-conception of what would emerge. It involves coding and categorising the data collected so that broad groups of similar concepts are used to generate a theory (Parry, 1998). Adopting the grounded theory approach enabled the study to truly triangulate the data as it allowed a comparison of the theory-led quantitative data with the more open-minded, theory-generating, case study data.
5.2 Effective team working This section outlines the themes that emerged from the case studies about what makes teams function effectively.
5.2.1 Strong and passionate vision for providing good quality care It was clear from the interviews with the teams that there was an overwhelmingly strong vision and values amongst the teams to provide good quality, recovery-focused care for service users. This strong vision is very consistent with the themes identified at stage one of the research (see Chapter 3). In essence, teams strive to provide care that is service user centred, holistic and recovery focused. This strong vision and values provides a guiding framework for how the team operates. It translates into staff who are passionate, enthusiastic and committed to providing an excellent service.
Why such a strong vision? Recruitment
It was clear from the interviews with team members that staff were recruited to the team based largely on the values they hold. As one of the team leads explained:
“I want people with the right values. People that can see the potential in service users and have a humanistic approach. It’s not just about experience – that doesn’t account for quality; it’s the values I’m after”.
This is not to say that teams used specific tools for assessing applicants’ values, more that they would be assessed in relation to open-ended questions.
Clearly defined service
This was a theme that emerged strongly in relation to the early intervention teams, where their aims and goals are clearly articulated in the Policy Implementation Guide. This guide outlines the philosophy of EI teams and provides a framework for how the teams should operate.

© Leading to Quality 2013 – All rights reserved Page 71
When teams are going through periods of great change (e.g. with service transformation), this clarity of definition is reduced as the teams seek to re-establish themselves. This point is illustrated by the following quote from a member of a team that has been through service transformation:
“We don’t know where we are or what we’re trying to achieve”.
The importance of a clearly defined service was a clear finding from the West et al (2012) study and has implications for service design and service transformation.
Team Communication (formal and informal)
The vision and values were reinforced through the teams’ communication, both formal (e.g. meetings/supervision) and informal (e.g. discussions around the office), where service users’ care is discussed and evaluated in relation to the vision and values of the team; as one of the interviewees said, “the ethos becomes self-sustaining”.
Effective team working generally
The vision and values were reinforced through effective team working, as described throughout the rest of this section; the following quote from one of the interviewees when asked why the team has such a strong visions and values illustrates this point:
“We communicate well and have lots of meetings. We all have similar training, share ideas, pool resources and are all heading towards the same goal”.
Leadership
There was a strong sense from the interviews that the team leaders are instrumental in ensuring that the team’s vision and values stay at the fore. The following comment from one of the interviewees illustrates this:
“Everyone holds the view of recovery at their heart. It’s a shared vision and a way of being. This was in me before I came to the team but it’s stronger now. TL’s enthusiasm and way of working rubs off”.
The effect of leadership on sustaining shared vision is discussed in greater depth in Section 5.3. The research literature on leadership and effective team working emphasises the critical importance of shared vision and values, in uniting teams through a clear and meaningful vision to which all are committed (e.g. Bass, 1998; Kouzes & Posner, 2009) and is fundamental to increasing a culture of strong engagement (e.g. Alimo-Metcalfe & Alban-Metcalfe, 2008). In a research study investigating the relationship between leadership in CRTs and their productivity, it formed part of the major predictor of their success, and of their engagement and wellbeing (Alimo-Metcalfe et al., 2007, 2008).
5.2.2 Team composition Multidisciplinary teams

© Leading to Quality 2013 – All rights reserved Page 72
The teams were all to a greater or lesser extent multidisciplinary, which was considered to be a considerable strength for each of the teams. The teams truly value the unique skills that each discipline brings. There were considered to be multiple advantages of having a multidisciplinary team, which are discussed below.
Holistic service
A multidisciplinary team enables the team to provide a holistic service “because there are no boundaries or limitations”. A good example of this is the work of a health and wellbeing practitioner in one of the teams. This person undertakes a nutritional and physical assessment when the service user joins the team and then works with them to optimise their physical health. Physical activity is a large element of this work, which is felt to have many benefits such as service user engagement and social inclusion. As discussed in Chapter 3, this was a clear theme emerging from the constructs of service users and their carers at stage one of the research. They emphasised that the most effective care was that which took account of their ‘whole life situation’, including domestic circumstances, social, educational, and physical health. The importance of a holistic service is a feature of the NICE Quality Standards (2011).
Flexible service
A multidisciplinary team was also felt to allow the team to deliver a flexible service. Having all disciplines within one team means that the team can respond promptly and appropriately to the changing needs of service users, which was felt to be critical in ensuring care remains in the community rather than in hospital. A good example of how a lack of disciplines can detract from team flexibility is from one of the teams where support workers had been removed from the team to sit in a central location. This team felt that the referral process required to utilise the skills of support workers has resulted in a lack of flexibility for the team to respond to needs as they arise. Service users identified team flexibility and adaptability as important to their care at stage 1 or the research. A further example of the constraining effect of a shortage of disciplines is surrounding psychiatric input into the team. All but one of the case study teams felt that they had sufficient medical input into the team. Four of the teams had a dedicated psychiatrist attached to the team on a part-time basis, which was considered to be sufficient. For one of the teams there was a full time psychiatrist dedicated to the team, which meant there was a continual formal and informal dialogue with the medics about service users, which was “key” to what the team does. In contrast, one of the teams had no dedicated psychiatric input into the team, with service users having to wait weeks for a medical opinion. This team felt that the service they provided was significantly constrained by the lack of psychiatric input into service user care.
Seamless service
In relation to the above, a multidisciplinary team helps teams provide a seamless service, especially where the team is exceptionally multidisciplinary. For example, one of the teams

© Leading to Quality 2013 – All rights reserved Page 73
had many disciplines, including an art therapist and a clinical psychologist. This minimised the need for service users to be referred to other services or teams and, therefore, avoids the communication problems and waiting lists that working with other services/team can result in. For example, other teams spoke of difficulties in accessing psychological therapy services and how, with these services being external to the team, this can result in fragmented care. The exceptionally multidisciplinary teams did not experience this problem. Continuous and seamless care was a strong element emerging from the constructs of services users and carers, and appeared to reduce anxiety and unpredictability, and is reflected in an item in the ‘Quality of Care Questionnaire’. ‘Continuous care’ also forms one of the 15 Quality standards identified by NICE in relation to service user experience in adult mental health (NICE, 2011).
Learning opportunities for team members
One of the additional benefits the teams considered to be of having a multidisciplinary team is the learning opportunities it provides to team members. Several of the interviewees spoke of how much they valued the opportunity to learn from other team members’ skills and experience, with the following quote from one of the interviewees illustrating this point:
“We all learn from each other – everyone is excited about the different skills within the team. Everyone has a thirst for knowledge”.
Experience
Apart from a good mix of disciplines, there was also considered to be a good mix of experience within the teams, with very experienced staff being complemented by less experienced staff who can offer a fresh perspective. Stable teams
Whilst some of the teams had undergone major changes, all the teams were relatively stable in their composition, with team members knowing each other well. This was felt to significantly contribute to the positive relationships within the teams (discussed below).
Discussion
Effective team working needs to be in place to ensure that the disciplines, skills and experience of each team member are exploited fully. Case load allocation is important and, on the whole, service users were allocated to team members according to people’s specialities; if necessary, staff will co-work with other team members to add their unique expertise. Also, the right kind of environment needs to exist. According to one of the interviewees, “the mixture of disciplines works really, really well because the team is so integrated. There are no silos and you can draw on other people’s skills”. The good communication and support within the team, discussed below, ensure that there are formal and informal forums for the different disciplines to input into service user care.
© Leading to Quality 2013 – All rights reserved Page 74
The skills and experience of team members adds to the sense of team potency within the teams; i.e., the teams believe that they are effective because of the skills and experience of team members. Research shows that professional diversity in a team brings the potential of considerable benefits from the knowledge, expertise, information, access to networks, etc., that it offers the team. But the same diversity has the potential to create ‘faultlines’ or divisions in teams (van Knippenberg & Schippers, 2007). The fact that the teams had a shared vision and values about which team members felt so passionate, serves to enable the benefits of diversity to be realised (Lau & Murnighan, 1998). Together with a strong sense of team potency, that is the belief in the team that it can achieve its aims and vision, it significantly increases the chances of high quality performance (Guzzo et al., 1993; Tesluk & Mathieu, 1999). As discussed in Chapter 4, the quantitative findings from the research indicated that multidisciplinary teams are important for effective team working. The case study findings support and supplement these by adding detail to how and why multi-professional team working is effective. The perceived importance of the stability of the team on the positive relationships within the team (which, as seen below, were considered to be critical for effective team working) is an important practical implication for service redesign and team restructure. The case studies found that these relationships, rather than the nature of the work, were of importance to staff when faced with a choice about which team to work in following service redesign.
5.2.3 Positive relationships within the team It was clear from all the case studies and from general observations of the teams that there were very positive relationships between the members of the team, which was considered by all the teams to be one of the main strengths of the team. An analysis of the data found there to be three main themes regarding relationships within the team: harmony, support and respect.
Harmonious relationships
For the majority of the teams, relationships within the team were felt to be very harmonious. There was considered to be “no backbiting” or “cliques”, with any personal issues being sorted out in an open and “grown-up way”. An associated element of harmonious relationships is acceptance. The stability of the relationships within the teams (mentioned above) led one of the interviewees to describe relationships within his/her team “as very familyish – we accommodate people’s foibles”. Accommodating people’s foibles indicates there is an acceptance of individual differences within the team and that people can feel comfortable in being themselves. The existence of harmony within teams does not mean differences of opinion or disagreements are not allowed. For example, one of the team leads distinguished between

© Leading to Quality 2013 – All rights reserved Page 75
conflict and disagreement saying that “we don’t have conflict, we have disagreements. When we have disagreements I will say “let’s sit down and talk about this””.
Having disagreements in a team is a very healthy aspect of team functioning as it is these disagreements that are likely to lead to improvement and innovation. If disagreements did not occur it would be of concern as it could be an indication that people were not able to be open and honest and, therefore, not feel able to challenge the status quo. In relation to harmonious relationships, a theme to have emerged from all the teams was that there was a good sense of humour within the team. Teams spoke of the fun they have together and how they “laugh a lot”. It was felt that this humour was a good way to off load, especially knowing that no one would be judgemental about what was being said.
Supportive relationships
It was clear from the interviews that relationships are very supportive, both on a personal and professional level. There is the belief that the teams genuinely care about their members. It is okay for team members to say when they are having a bad day or to ask for help if needed. As one of the team members said:
“as a team we will not let anyone struggle – everyone wants to help”. The supportive nature of the teams is very helpful in a job that can be stressful. One of the team members explained how s/he felt frustration at “hitting a brick wall with clients” but that “as a team we’re always here to off load; to get through things”. The sense of support within the team gives people the confidence to “put their hands up when they’ve done something wrong”, as they do not have to fear recrimination. Having a supportive approach to mistakes is the sign of a learning culture, which can lead to service improvement and innovation and can also contribute to the avoidance of more serious mistakes. Respectful relationships
Generally relationships within the teams were felt to be very respectful. As one of the team leads commented about his/her team: “it is a truly lovely team where there is mutual respect”. A clear theme in relation to respectful relationships was that all members of the team, irrespective of grade or professional background, were considered to be equal – as such the teams were felt to be non-hierarchical. All team members are considered to be valued the same, with all opinions being listened to. The following comment from one of the interviewees summarises this view:
“There is mutual respect, regardless of role, regardless of being qualified or unqualified. Everyone has a voice and there is no hierarchy – this is something I really value”.

© Leading to Quality 2013 – All rights reserved Page 76
This inclusivity is important because it means that all people are willing to share their valuable insights and perspectives on service user care, which, in a more hierarchical team, may be quite difficult for people at the lower bands/grades to do.
Discussion
The different types of relationships described above (harmonious, supportive and respectful), although combined with healthy and constructive challenge, indicate that there is a great deal of social support, trust and psychological safety within the teams, which sets the right culture for individuals to perform at their best and to deliver an effective service. They are very important for the themes of ‘effective communication’ and ‘culture of innovation, improvement and development’, discussed below. The positive relationships within the teams were also a reason for positive levels of staff engagement and wellbeing, discussed later in this chapter. The crucial importance of social support in teams in strengthening their effectiveness and wellbeing of members is consistent with the well-established research literature (e.g. van Mierlo et al., 2006) and from the quantitative findings discussed in Chapter 4.
5.2.4 Effective and engaging communication Effective and engaging communication was considered to be one of the key strengths for all the case study teams, which, as said, is very much related to the positive relationships discussed above. There was felt to be good communication on an informal and formal level. With regards to informal communication, the teams generally work closely together in their physical environment and talk through issues as they arise. As mentioned above in relation to support, teams value the opportunity to discuss things with their colleagues on an ad hoc basis, taking opportunities where they can to catch-up and debrief. In relation to formal communication, all the teams had regular team meetings, which were prioritised and valued by the teams. For some teams these were weekly meetings, whereas for others they were twice weekly, or even daily. During the team meetings individual service users were discussed, with everyone becoming aware of what is happening for each service user. These meetings were an opportunity for the team to actively engage with each other and the team’s work by evaluating progress, sharing ideas, problem solving and planning for the future. They provided a forum for all disciplines to work together and to provide their specialist knowledge and experience. They were considered to be very useful from a positive risk taking perspective as is gives team members a sense of shared decision making and shared responsibility, rather than one person being solely responsible, which strengthened a sense of ‘collective and shared leadership’. This in-depth communication also ensures that there is good continuity of care for service users in the absence of their care coordination, which as seen in Chapter 3, is important to service users and carers.

© Leading to Quality 2013 – All rights reserved Page 77
Apart from service user care, business matters were also discussed during the team meetings, providing the team lead with the opportunity to update and discuss with the team business matters such as impending changes. As is evident from the above, effective and engaging communication is critical for an effective service user experience as it leads to truly integrated working within the team. As well as having a positive impact on the service user experience, the regular team meetings also help from a team bonding perspective as they provide a forum for all team members to be together. This was especially important for one of teams who work over split sites. In relation to this, the opportunity to “off load” to colleagues and discuss concerns, helps with staff wellbeing through reducing stress. The importance of the effective communication described above is well documented within the literature (e.g. West et al., 2012). The effective and engaging communication, described above, results in a cognitive state mediator (I-M-O-I model), as it leads to ‘shared mental models’ and ‘collective experience’. It also helps shape the positive affective states of psychological safety, social support and team potency.
5.2.5 Culture of innovation, improvement and development All the teams, to a greater or lesser extent, had a culture of innovation, improvement and development within the team, where creative ideas, reflection, problem-solving, and individual and team development were encouraged. This culture was driven by “everyone being so committed to doing a good job” and “always striving to be better and give better delivery of care”. Interviewees from the different teams spoke of how there was “no such thing as a bad idea”, with people feeling able to speak with confidence about their ideas. One of the interviewees spoke of how empowering this was as s/he felt “there are no barriers to doing what I want to do”. A “no blame culture” was also felt to exist, where there was a supportive approach to mistakes. Adopting such an approach can lead to service improvements and can also contribute to the avoidance of more serious mistakes. Teams adopt a reflective and problems solving approach to the care they deliver and how they operate, as the following quote from one of the interviewees illustrates:
“We don’t get stuck in the mud. The team lead encourages people not to get stuck in the mud. Sometimes with clients you might get a bit stale but it’s about recognising when you are – when you need out. Clients might be allocated to someone else if this is the case”. There were excellent examples of innovative practice within the teams. However, innovation was felt to be constrained by the demands the teams are facing in delivering the service, with teams feeling that lack of time can restrict innovative practice.
Team and individual development

© Leading to Quality 2013 – All rights reserved Page 78
Part of a culture of innovation and improvement is for development at the individual and team level to be encouraged and valued. It is clear from what has been discussed already that development within the teams was prioritised, with regular meetings, open communication, reflection, problem-solving and creativity being routine aspects of team functioning. In addition to the above, there were more formal methods of team development including annual/biannual team away days and group supervision. In some teams group supervision was incorporated into the team meetings. For example, for one of the teams there was monthly group clinical supervision where staff are given training and support in psychological therapies, such as cognitive behavioural therapy and psychosocial interventions. This was a way of “up-skilling staff when there is little funding for psychological therapies from other services”. With regards to individual development, interviewees feel there were good opportunities for individuals to develop within the teams. On the whole, teams were considered to be very empowering, with individuals being given the space and support to develop in their roles. In relation to more formal development, teams were considered to be supportive of formal training and development if the outcome would be improvement for service users. There were positive examples of how individuals were given training and development opportunities. One of the teams in particular required all members of the team to undertake the same psychosocial interventions course; this unified approach was felt to unite the team in their understanding and approach, and also allowed the team to provide evidence based care.
Genuine commitment to supervision
In relation to more formal development, the teams were characterised by a genuine commitment to clinical supervision (and case load management for some teams). All the teams had clinical supervision every 4-6 weeks. Clinical supervision is a one-to-one activity where staff discuss individual service users with their supervisor and is a time for staff to reflect on, discuss, problem solve and plan the care of service users on their caseload. Whilst supervision is a requirement for most teams, there can be a tendency for some to regard it as going through the hoops, which was certainly not the case for the case study teams.
Discussion All the teams, to a greater or lesser extent had a culture of innovation and improvement within the teams, where creative ideas, reflection, problem-solving, and individual and team development were encouraged. There was also a genuine commitment to development and supervision, at the individual and group level. There was a sense that teams were striving to be the best they could be. The culture of innovation, improvement and development very much relates to the afore mentioned themes of ‘Positive Relationships within the Team’ and ‘Effective Communication’. Feeling ‘safe’ to make suggestions, admit mistakes and having

© Leading to Quality 2013 – All rights reserved Page 79
opportunities to communicate and engage meaningfully, meant that a culture of innovation, improvement and development could flourish. Understanding the conditions that encourage and sustain an innovative culture is a challenge for leaders (Yukl, 2009), which is especially important at a time when the importance of innovation is increasingly being recognised (DH, 2012); the innovative culture within the case study teams provides a useful illustration of innovation in practice.
5.2.6 Relationships with other teams and agencies
Relationships with other teams and agencies differed quite a lot between each of the case study teams. Generally relationships were felt to be positive, which was fostered by:
A service user centred approach: interviewees recognised the vital importance of having good relationships with all agencies involved in their service users’ care because, as one interviewee said, “it is important to get the whole picture”.
The team lead: some team leads were active in networking and building relationships with other teams and agencies.
Individual practitioners’ behaviour: There was a recognition that positive relationships with other teams and agencies were largely down to the individual relationships that team members build with other teams. There was an understanding that it is important to work well with teams at an individual level, as the following quote illustrates:
“Relationships with other teams come down to what you demonstrate as an individual and how you work with others”
Link people: There were link people within most of the teams that coordinated with specific teams and agencies to facilitate good relationships. These link people acted as boundary spanners between the teams.
Why do difficulties arise with relationships with other teams and agencies?
Pressures on other teams and agencies: this emerged in relation to:
- Difficulties in accessing crisis care: a clear theme to have emerged from a few of the teams was that the crisis services in their area were under considerable pressure, making it difficult to get referrals accepted
- Difficulties in discharging service users to other community teams: this was particularly relevant for a couple of the early intervention teams who found it difficult to place their service users when they were ready for discharge from their team. The following quote illustrates this problem:
“EI cases are not regarded as a priority because they are already getting a service – there are waiting lists for other services”.
Different perceptions of risk: again, in relation to accessing crisis care, it was apparent from a couple of the case study teams that the crisis teams were reluctant to accept
© Leading to Quality 2013 – All rights reserved Page 80
some service users because they did not perceive the service user to be at a level of risk that required crisis intervention. This was a cause of frustration for the case study teams concerned, as they felt the crisis teams were undermining their professional judgement.
Service transformation: it was evident from the teams where their trusts had undergone significant service transformation that referral processes had resulted in “too many interfaces” and “team boundaries becoming blurred”. There was confusion as to “who’s who”, resulting in referrals getting “batted about”. Once the service changes had settled, processes appeared to become smoother.
Establishing appropriateness of service user for the team: this was an issue for the EI teams in particular where: “deciding on whether someone is appropriate for the team is very difficult – they need to be assessed on multiple occasions”.
Teams’ approach to overcoming difficulties with other teams/external agencies
All of the teams recognised the vital importance of effective relationships with other teams/external agencies for a positive service user experience. As such, they try and overcome the difficulties experienced. Below are a number of strategies the teams employ to do this:
Face-to-face meetings: in order to try and address difficulties with other teams and agencies. For example, one of the early intervention team leads worked hard at building relationships with child and adolescent mental health services when she came to post:
“It was a conscious decision when I started to build up these relationships as they have been problematic in the past. I invited them to come to the team for dinner. Now we have a fantastic relationship. We do joint appointments. There are no formal procedures, we just pick up the phone. None of this is rocket science”.
Flexibility: one of the teams spoke of how they aim to be flexible with the other teams they work with so that relationships remain harmonious, as one of the interviewees explained:
“We all sometimes have the same disgruntlement with other services but we foster an ethos of flexibility. We don’t want to get defensive with other teams”.
Depoliticising the situation: one of the teams spoke of how they try to depoliticise difficult relationships:
“We ignore politics. We are here for the benefit of service users – they are at the heart of everything. We depoliticise things by saying “there’s someone in need””.
Discussion
Relationships with other teams and agencies were generally felt to be positive. The teams try to ensure that this is the case, as they recognise positive relationships are important for service user care. They do this through trying to work effectively and engaging with teams on an individual level and also through having members of the team that formally link with other teams. Difficulties arise due to pressures on other teams and agencies, different perceptions of risk, service transformation, and establishing the appropriateness of service users for the

© Leading to Quality 2013 – All rights reserved Page 81
team. Teams try and overcome these difficulties through organising face-to-face meetings, being flexible, and depoliticising the situation. These findings from the study regarding inter-team working provide practical advice to help teams work effectively with other teams and agencies.
5.2.7 Adapting to change Three of the case study teams had been through major changes/were in the processes of major changes at the time of the case studies. The effective team working described above was considered to be key to helping the teams adapt to these changes, illustrated by the following quote:
“We get through it. We think about how we can make the most of the skills we’ve got. We get on as a group, have a laugh and don’t worry too much about the bigger change. People support each other – it feels like we’re more supportive than other teams”.
As well as effective team working, the team leaders, as seen in the next section, were considered to be key to facilitating teams to adapt to the change.
Overall comment on effective team working
The case study findings are consistent with the I-M-I-O model. The effective team working described above illustrate the mediative and iterative processes involved in the I-M-I-O model of team working. Mediation is evident from the positive affective states (e.g. social support and psychological safety), behavioural processes (e.g. regular team meetings) and cognitive states (e.g. shared mental models). The reflection and culture of innovation and improvement are examples of the iterative nature of team working also featured, also central to the I.M.I.O model.
The case study results also illustrate that the case study teams are ‘genuine’ rather than ‘pseudo’ teams as they have clear team objectives, interdependent working and regular meetings to discuss effectiveness, which, according to West et al (2003) are the characteristics of effective team working.
5.3 Effective Leadership
All of the team leads were respected and valued greatly, for some teams this strength of feeling was exceptionally strong. There were many similarities in their leadership approaches, which were very consistent with the Model of Engaging Leadership (Alban-Metcalfe & Alimo-Metcalfe, 2007; Alimo-Metcalfe & Alban-Metcalfe, 2001; 2003; 2010) outlined in Chapter 1. The effective leadership displayed in the case studies orchestrated the effective team working described above.

© Leading to Quality 2013 – All rights reserved Page 82
The main themes to have emerged regarding effective leadership are discussed below.
5.3.1 Sustaining shared vision It is clear from the previous section that the case study teams have a strong vision and values for providing good quality care, which they are enthusiastic about and committed to. A theme to have emerged from the majority of the teams was that the TL was key to keeping these passionate vision and values alive. The following is an abstract from one of the case study teams that illustrates this point:
“I admire the TL’s leadership style. S/he makes sure we’re all singing from the same song sheet and that we all share the same values”.
This TL was felt to do this through continually verbalising the vision, formally and informally (e.g. reminding the team of their ethos was by saying “this is what we should be doing”. The TLs were felt to be extremely passionate about providing a good quality service, consistent with their team’s values. This served to unite and motivate the teams. As discussed previously, building shared vision is a key element of an engaging leadership style (Alban-Metcalfe & Alimo-Metcalfe, 2007; Alimo-Metcalfe & Alban-Metcalfe, 2001; 2003; 2010).
5.3.2 Inspiring others In relation to the above, a theme to have emerged from the majority of the teams was that their TL inspired others due to their:
Vision and values
Passion and determination
Strong work ethic
Acting as a role model, both in relation to clinical leadership (discussed below in relation to ‘hands on leadership’, and the supportive/team culture they foster (discussed below).
For a couple of the team leads their inspirational characteristics seemed to result in them being able to secure resources for their teams, illustrated by the following quote from one of the team members about their team lead: “People are drawn to him/her, they will give him/her money”. This team lead had been successful in growing the team at a time when resources are difficult to obtain. Inspiring others is also a key element of an engaging leadership style (Alban-Metcalfe & Alimo-Metcalfe, 2007; Alimo-Metcalfe & Alban-Metcalfe, 2001; 2003; 2010).
5.3.3 General leadership style

© Leading to Quality 2013 – All rights reserved Page 83
All the TLs displayed very similar leadership styles, which were characterised by being strongly engaging - with individuals, the team, and other teams and agencies. The main themes that emerged regarding their leadership styles are outlined below. Democratic but decisive
Generally the team leads were considered to have a democratic leadership style. They were open-minded about people’s views and opinions and considered these when making decisions. Ultimately, however, the TL will make the decision and, if the decision is not consensual s/he will say “Thank you. I’ve listened to what you’re saying but this is what we’re doing”. Situational leadership
In relation to the above, team leads were felt to vary their leadership style according to the situation. For example, one of the TLs would be democratic generally but autocratic when required, such as managing performance or ensuring compliance with trust requirements. Similarly, it was mentioned a few times that TLs would generally empower staff through giving them autonomy in their role but would, however, apply more control to people with less experience. Open and honest
A theme to have emerged from the majority of teams was that TLs were felt to have an open and honest approach. A quote about one of the TLs illustrates this point:
“S/he is open and honest and doesn’t have a hidden agenda. We can also be honest with him/her”.
The main ways in which the TLs were felt to be open and honest were in relation to:
Keeping staff informed about managerial issues: TLs would keep staff up to date on managerial issues within the organisation, including impending changes and the consequences of these on the team. One TL did say, however, that s/he would pace the flow of information s/he gave to the team in order to protect staff morale.
Encouraging open and honest debates: the TLs saw conflict as healthy and promoted a culture where challenge was acceptable. They were willing to be challenged and would manage this challenge in an open and honest way.
Positive leadership
TLs were considered to have a positive approach to leading the team, displaying positivity in their attitude and behaviour. For example, one team member said of his/her team lead: “You never hear one bad word from him/her”. This positivity was evident at even the most difficult of times, which a few of the teams were currently or had recently been faced with. For example, one of the teams had recently undergone significant change due to service transformation. When speaking of how their TL had managed this situation, a team member indicated that the TL was positive and pragmatic:

© Leading to Quality 2013 – All rights reserved Page 84
“The TL tries to frame things in a positive way. S/he says “we’re a team, we’ve got to do it, so let’s work in a positive way to make it happen”. If it was all doom and gloom it would be awful”.
It is clear from this quote that a positive approach has a positive impact on the team. Another theme to have emerged in relation to positive leadership was the TLs’ desire to shield staff from their own moods or stress, which is evident from the following quote from one of the TLs:
“I don’t let my off days impact on my colleagues. I want people to enjoy their work so I always put a smile on my face”.
The following quote from another TL illustrates this point in relation to change management:
“It would have been stressful for TL but s/he managed to keep herself together and support others. All the team follows his/her lead”.
Again, it is evident from this how such a positive approach has a positive impact on the team. Finally in relation to positive leadership, a clear theme to have emerged from the case studies was that the team leads had a good sense of humour, which was valued considerably. There was felt to be lots of fun in the teams, with TLs “having a laugh” and using humour to diffuse stressful situations. Hands-on leadership
All the TLs in the case studies were considered to have a hands-on approach to leading the team, whether or not they still maintained a caseload. Three of the TLs did still have a small caseload. One of the TLs explained that this clinical activity was important for the credibility and respect from the team. It was clear from the teams where the TLs still had a case load that this was the case:
“S/he is excellent. Very knowledgeable. S/he has a good grounding in EI and you know what s/he says has substance to it”.
“If no one’s willing to do anything s/he’ll do it. S/he’s very persistent, very proactive
and acts as a role model”. “His/her engagement skills are brilliant with clients”.
Those that did not have a case load also had a hands-on approach, through being integrated as part of the team, supporting the team practically and leading by example. For example, one team member said of his/her TL: “S/he will do anything s/he asks the team to do”. Also, s/he will support staff at times of pressure, for example, doing assessments when other staff are busy. As mentioned above, this hands on approach to leading the promotes respect and credibility in team members through teams leads:
“Working hard, acting as a role model, and practicing what s/he preaches”.

© Leading to Quality 2013 – All rights reserved Page 85
In association with this, the clinical expertise that all the TLs were felt to have meant they were a reliable and credible source of support to team members when they need help and advice with regards to service user care.
Empowering leadership
Consistent with the belief that leadership emerges from within the team, and is not just present in formal leadership roles (Day et al., 2004), it was clear from the case studies that team members were empowered to be leaders within their own role through the team leads’ engaging leadership style. There were three main elements to empowering leadership:
1. Distributed leadership: leadership roles were generally distributed throughout the teams. For example, in one team there was a clinical lead within the team, and, apart from this, other members of the team have leadership roles. As one of the interviewees said, “leadership is spread throughout the team; people have specialist skills that they take the lead on, for example eating disorders. Others will step in when the leaders aren’t there”.
2. Facilitative leadership: Team leads seemed to adopt a facilitative approach to leading the team and, instead of telling people what to do they would adopt a “problem solving approach”, where they get people to think of solutions for themselves. As one or the TLs explained, “I want people to grow within their role and to get people thinking about their own responses”. One of the team members spoke of the impact of his/her team leads facilitative leadership style by saying “s/he makes be believe in myself – s/he gives me confidence”.
3. Autonomy: On the whole, team members were given autonomy to decide how to do their work, with the TLs supporting them to do this. For example, when talking about his/her TL one of the interviewees said “s/he trusts staff, recognises their strengths and lets them get on with things”. This person went on to explain that the TL will give people the freedom to manage their own time and identify their own priorities. S/he makes it clear that s/he relies on everyone to do their job to the best of their ability but will let them decide the best means to do this. However, s/he will recognise when people need a higher degree of support and will take a more directive approach at these times. This approach makes team members feel valued and trusted by the TL.
Conclusion and discussion
The TLs displayed very similar engaging leadership styles: democratic but decisive, situational leadership, open and honest, positive leadership, hands on leadership, and empowering leadership. These leadership styles promoted a sense of trust and respect for the leadership, with team members feeling they were in ‘safe hands’. They were also important to promoting a sense of staff engagement, especially through the leaders’ positivity, democracy and the extent to which they empowered the members of the team.
5.3.4 Team focused

© Leading to Quality 2013 – All rights reserved Page 86
It was clear from all the case studies that the TLs were very focused on the team as a unit and the individuals within it. They recognise that staff are the key to working effectively and to achieving the teams’ goals, as illustrated by the following comments by two of the TLs:
“My leadership style is to look after staff – their welfare has always been a priority. Some say that service users should be put first but I believe you need to look after staff first, because they are the ones that look after service users. Staff need to be equipped with the skills, confidence and support to do their best”.
“My job is to get the best out of people. I will invest time in people and go the extra
mile for people - because of that, people are willing to work for me”.
Five main themes emerged regarding TLs being team focused: developing a team culture, understanding the team, valuing the team, support, developing the team.
Developing a team culture
It was clear from the interviews that the TLs “develop a team culture” so that all team members felt they were working as part of a united team. As one of the interviewees explained about his/her TL:
“S/he encourages us to think about other members of staff. We need to be aware that we are part of a team and that how we behave affects others. People have responsibilities to the team and they have to you”.
The TLs create the team culture in their everyday activities. They are inclusive, fair and consistent with all members of staff, helping to ensure there are no cliques. As discussed above, the TLs are an integrated part of the team and do “not sit on a pedestal”, which enriches the sense of team, and also gives them the opportunity to model appropriate team behaviour. Their interpersonal skills mean that they can relate to staff and brings a “human element to the team”. As discussed above, humour is a key element of their leadership style that binds the team together. The effective team communication and team development, discussed in the previous section, is critical to developing a team culture; the TL is instrumental in ensuring the success of these activities. Also, the development of a team culture is critical to the positive relationships discussed in the previous section. Understanding team members
Part of the TL’s team focus is to ensure s/he understands the members of the team, including their skills, abilities and personalities. It was clear from the interviews that this understanding helps the team work effectively as it allows the TL to work towards people’s strengths and, where necessary, provide extra support. It also helps maintain the harmonious relationships discussed in the previous section. Valuing team members
It was evident from the TL and team member interviews that the TLs value the team and the individuals within it. The following quote from one of the TLs illustrates this point:
© Leading to Quality 2013 – All rights reserved Page 87
“I am really, really lucky to have such a good team where “all staff are qualified to do the job and do it fantastically well”. It was clear from the interviews with the team members that, on the whole, staff felt valued by the TL. For example, many interviewees mentioned how their TL praised them and thanked them genuinely for their efforts. Supportive
All the TLs were felt to be very supportive, both on a professional and personal level, and were felt to genuinely care about the members of their team. They were approachable and accessible to staff, helping them problem solve and offering advice. The following comments illustrate this supportive approach:
“His/her door is always open. If s/he’s not got the time s/he will make time. S/he will always listen”.
“Managers are under more and more pressure but s/he is always there for you. S/he will drop anything. S/he will problem solve with you”. It was seen in the previous section that relationships within the teams were very supportive. The TLs were instrumental to this and would not tolerate any behaviour that contradicts the supportive culture of the team. As one of the TLs explained, “the team attitude is to support each other and staff would be challenged if there was a bad apple”. On a more formal level, TLs offer support during caseload management and/or clinical supervision (as discussed previously). The support TLs offer team members is critical to staff wellbeing as is helps avoid/relieve stress and anxiety (discussed in relation to staff wellbeing and engagement), and also helps with positive risk taking. For example, one TL spoke of how conscious s/he was about the high level of risk and responsibility staff members work with. S/he will ensure that the level of individual responsibility is diluted through working with staff and supporting them to make difficult decisions. As such, these decisions become consensual, rather than individual. This also helps with positive risk taking, which is beneficial for the service user experience. Developing the team
The TLs were instrumental in promoting the team and individual development, and the genuine commitment to supervision discussed in the previous section.
Conclusion
It was clear from all the case studies that the TLs were very focused on the team as a unit as well as the individuals within it. They recognise that staff are the key to working effectively and achieving the teams’ goals, and work hard to ensure that there is the right culture and support for the team to flourish. They promoted a sense of “team”, so that all team members felt they were working as part of a united team, facilitated by the effective communication and team development discussed previously. This promotion of the sense of team was critical to the positive relationships found within the teams. The TLs understood their team

© Leading to Quality 2013 – All rights reserved Page 88
members, making sure they worked to their strengths and providing extra support in relation to their limitations. They also valued team members, which had a positive impact on team members’ motivation and commitment. The TLs were considered to be exceptionally supportive, which was critical to staff wellbeing as it helped to avoid/relieve stress and anxiety, and also was felt to help with positive risk taking. Finally, the TLs were instrumental in promoting the team and individual development, and the genuine commitment to supervision discussed in the previous section. The themes discussed in team focused are very similar to the work of Schaubroeck et al (2007) when they identified the team leader behaviours that create a culture in which team cohesiveness and team potency can develop and flourish. Again illustrating the mediative effect of leadership.
5.3.5 Performance Management A theme to have emerged from the case studies, to a greater or lesser extent, was that TLs were willing to manage performance within the team. On the whole, TLs were proactive at managing performance and were not afraid to have the difficult conversations this requires.
Key areas for performance management
There were not considered to be any major performance issues within any of the teams. However, the main areas that emerged in relation to performance management were:
Behaviours that undermine the supportive culture of the team (as discussed above in relation to support);
Adherence to trust administrative requirements (discussed below in relation to balancing the needs of the organisation with the needs of the team);
Workload allocation – ensuring that this is done fairly.
Team leads’ approach to managing performance
Setting direction: An overarching way in which TLs manage performance is through setting direction. As one of the team members explained about their TL:
“S/he is very clear about what s/he wants and about the expectations of the team. S/he communicates well so that you know exactly what you need to do”.
Role modelling appropriate behaviours: As discussed before in relation to hands-on leadership, the way in which TLs are integrated within the team means gives them the opportunity to act as a role model for team members. Performance management is in itself a form or role modelling. As one of the TLs explained in relation to dealing with interpersonal conflicts within the team:
“It’s important to be a role model. I need to send a message that it is not acceptable and there will be consequences if it carries on”.

© Leading to Quality 2013 – All rights reserved Page 89
Supportive approach: Generally the TLs adopted a supportive approach to managing performance within their teams, which is consistent with their supportive approach generally. This point is illustrated by the following comment from one of the TLs:
“People generally work above and beyond so I won’t bawl anyone out. If someone is regularly not sticking to things then that breeds resentment. I will speak to these individuals confidentially and ask “is there anything I can do to support you?” Or “Is there a problem, I’ve noticed…””.
Light hearted approach: as discussed above in relation to humour, TLs will sometimes use humour to diffuse potentially difficult situations. For example, one of the interviewees said of their TL: “s/he isn’t formal when s/he’s telling us off – s/he’ll use humour”.
This supportive and light hearted approach to managing performance meant that issues were resolved in a way that was agreeable to the team members involved. For example, one of the team members said of their TL: “you can have a telling off but it doesn’t feel like it”.
Pulling rank: a theme to have emerged from the case studies was that TLs would be prepared to pull rank when necessary, as illustrated by the following comment from one team member about their TL: “S/he will say “I hear what you’re saying, it’s not great, I understand, but you’re doing it””.
Adhering to policies: Adhering to policies was a theme to have emerged from a couple of the case studies. For example, one of the TLs spoke of how s/he follows formal policies and procedures with regards to issues of sickness. S/he explained that adopting such an approach means that:
“Everyone is treated the same and that things are being done fairly. It allows the situation to me monitored and evaluated”.
Conclusion and discussion
TLs, to a greater or lesser extent, were willing to manage performance within the team. On the whole, TLs were proactive at managing performance and were not afraid to have the difficult conversations this requires.
It was clear from the interviews that the TLs’ ability and willingness to manage performance in a timely and effective manner had a positive impact on the teams because it:
Promoted respect, confidence and reassurance in the TL because, as one of the team members explained, “you need to have confidence that managers will deal with things”;
Promoted a sense of trust because TLs are considered to be open and honest, meaning team members “know where they stand”;
Meant there were clear standards of acceptable behaviour within the team, which promotes positive team functioning and positive service user experiences.
Managing performance is a leadership competency and is a critical element of managing NHS services (see, for example, the NHS Leadership Framework). The leadership style the case study team leaders adopted to manage performance was primarily engaging, resulting
© Leading to Quality 2013 – All rights reserved Page 90
in improved performance without causing upset or conflict within the team. If this engaging style was not effective, then a more autocratic approach would be used. 5.3.6 Balancing the needs of the team/service with the needs of the organisation Two main themes emerged regarding balancing the needs of the team/service with the needs of the organisation: compliant with trust/organisation requirements and acting as an advocate for the team. Compliant with Trust/organisation requirements
This was a strong theme to have emerged from the three case study teams that experienced significant organisational change. Generally the requirements related to the increase in “paperwork” that teams felt they were experiencing. It was considered that work had become more bureaucratic, with more policies and protocols to follow and “paperwork” to complete; documentation needs to be “defensible”, and performance information required for the organisations is increasing. Generally there was a feeling from team members that the level of paperwork was very time consuming and detracted from time spent providing service user care; as such, it was a cause of resentment. TLs could, on the whole, understand the rationale for the trust requirements. For example, one TL when talking about policies and protocols explained that “they are there to support and protect staff and are sometimes helpful”. The TLs’ approach to getting the team to comply with what is expected of them was to communicate the rationale to the team, “helping them see the bigger picture – from the Trust perspective”. TLs were, on the whole, respected for this, as the following quote from one of the team members illustrates:
“S/he expects us to appreciate the current business model – to see the bigger picture. This is reassuring professionally”. The TLs concerned were very clear that the team need to comply with the expectations of the Trust and, consistent with their approach to performance management (discussed above), would ensure that the teams undertake what is expected of them. They will support staff to do this if they are having difficulties, for example, through reducing a person’s caseload so that they can input their contact information. This need to comply can be a cause of friction between the TLs and the team, with some team members being very frustrated at the increasing administrative burden. As explained above, to help manage the situation the TLs will explain the rationale for certain activities and will sometimes say “I know it’s rubbish but you’ve got to get it done”. Team members could generally appreciate why they needed to undertake the admin. The TLs do not blindly comply with trust initiatives and, as described below, will act as an advocate for the team to try and shape/influence what is required.

© Leading to Quality 2013 – All rights reserved Page 91
Acting as an advocate for the team and the service
A clear theme to have emerged from all of the case studies was that the team leaders were prepared to act as an advocate for the team and the individuals within it, as the following quotes illustrate:
“TL is the backbone – s/he is willing to fight our corner and to stand up for individuals and the service”.
“The TL can be a bit corporate but s/he is not a “yes person”. S/he will stand up for
the team and will challenge managers”. The areas in which TLs were felt to advocate for the team included:
Advocate with trust managers: it was felt the TLs would advocate for the team when working with more senior managers in their trust. This was particularly strong in relation to organisational changes, summarised by the following quote:
“The TL will defend and support the team against changes that haven’t been agreed, s/he will act as an advocate for us”.
Advocate to obtain resources: it was felt in some of the teams that the TLs were able to secure resources in order to develop the service, illustrated by the following quote:
“You get the feeling s/he’s fighting for the team – it feels like s/he’s created more jobs and opportunities for the team”.
Advocate with other teams: TLs were prepared to advocate on behalf of the team with other teams and services so that the team’s perspective is heard.
Advocate for individuals: there was a sense that TLs would advocate for individual team members with other teams, the trust and service users and carers when required. For example, one of the interviewees spoke of how the TL had supported him/her to undertake some training that was difficult to secure funding for:
“The TL gave me the belief as a person – s/he stuck his/her neck out to say I could have time, despite some opposition”.
Advocate for service users: TLs want the best possible experience for service users and will advocate for their best interests at a clinical and managerial level.
Ambassador for the team: A theme to have emerged from some of the case studies was that the TL would act as an ambassador for the team, networking with other teams and agencies and promoting the service.
Consequences of acting as an advocate for the team and the service
The TL acting as an advocate for the team inspires trust and confidence in team members, making them “feel safe” and supported. It is very consistent with the team focused and supportive approach of the TLs.

© Leading to Quality 2013 – All rights reserved Page 92
Conclusion and discussion
One of the difficulties TLs faced was having to balance the needs of the team/service with the needs of the organisation – they are the interface between the team and the more senior management of the organisation. It was evident from the interviews that this balance was difficult for TLs. There was a general perception that initiatives from the wider organisation had become more bureaucratic, which was a cause of resentment. The TLs could, on the whole, understand the rationale for the trust requirements. They would communicate this to the team, expect that there was compliance and, where necessary, support team members to comply. However, the TLs were individuals that were able to question and challenge trust initiatives and were prepared to act as an advocate for the team to try and shape/influence what is required. The TLs’ willingness to act as an advocate for the team inspired confidence and trust in team members, making them feel safe and supported.
5.3.7 Effective change management As mentioned previously, 3 of the teams had gone through/were in the process of going through major change; the TLs for these teams were felt to be effective at managing this change. The way in which the TLs have managed the teams through the change process is a good example to illustrate a lot of what has been discussed regarding effective leadership. The main themes to have emerged regarding effective change management were:
Open communication: On the whole, the TLs kept their teams informed of the changes as and when they knew any information. This, according to one team member, has helped “manage the team’s anxieties”. One of the TLs would pace the flow of information at times so as not to overwhelm team members
Supportive: The TLs were very supportive to their teams throughout the change process, which was a source of strength for team members. They were approachable and accessible throughout the process, giving people the time to express their concerns and anxieties. They actively listened, shared staffs’ frustrations and gave people the time to adjust to the transition.
Positive and pragmatic approach: TLs would manage change in a positive and pragmatic manner, as illustrated from the comment below:
“The TL tries to frame things in a positive way. S/he says “we’re a team, we’ve got to do it, so let’s work in a positive way to make it happen”. If it was all doom and gloom it would be awful”.
The TLs would also maintain positivity through shielding staff from the stress and anxieties they were experiencing, illustrated by one team member’s comments:
“The TL has taken things on the chin and just got on with it”.
As mentioned previously, TLs will also lighten the mood with humour. For example, one of the TLs was said to break bad news in a light-hearted manner, such as breaking into song.
One of the team members described the impact of this approach:

© Leading to Quality 2013 – All rights reserved Page 93
“Even when s/he has to gives us more work s/he makes it okay. Sometimes s/he sings, which softens the blow. Because s/he does that the team are willing to do anything – we get on and do it”.
Taking local ownership: A clear theme to have emerged from the case studies was the team leader promoting local ownership of the change. For example, presenting the team with the situation they were confronted with and taking a problem-solving approach to how it should be implemented locally.
Prioritising team development: In relation to the above, the TLs prioritised team development following the implementation of major changes in the form of away days. This gave the teams chance to formulate a plan for implementing the changes and also helped from a team bonding perspective where there were new members to the team.
Acting as an advocate for the team: As mentioned above, TLs will advocate on behalf of the team to try and influence the nature and extend of the changes.
Practical support: A theme to have emerged from one of the case studies was the TL’s practical support during the change process, which was described by one of the team members:
“S/he familiarised herself with new systems and processes so that s/he could cascade them down”.
This level of practical support is likely to help the team in the transition, and is an illustration of the TL’s hands-on leadership style.
Positive feedback regarding change management
It was felt that the TLs’ approach to managing the changes within the team have facilitated the team to adapt well to the situation they were faced with, as illustrated by the following comments:
“We’re a different team but it’s been quite seamless, which is due to how it has been managed. I sometimes think “What if we had been managed by someone else?”.
“the TL took responsibility and you can’t beat a good manager in situations of chaos”.
“The current changes have really brought this to light – they’ve made it clearer what good leadership means”. It was also clear that the respect team members had for their TL was critical in ensuring positive adaption to change, as the following quotes illustrate:
“I respect him/her as a manager so I take things as a positive. I try to take things on board and comply with things in a way that suits”.
Conclusion and discussion
To conclude, the TLs’ approaches to managing change inspired confidence and trust in team members, promoting positivity and relieving the anxieties caused by uncertainty. They also helped staff feel supported at an individual and team level. The approach the TLs have

© Leading to Quality 2013 – All rights reserved Page 94
adopted seems to have led to the effective management of change. These are very rich and practical findings to emerge from the research that can help inform practice.
5.4 Staff Engagement and Wellbeing It is clear from what was discussed during the interviews and from the questionnaire data that the effective team working within the teams had a positive impact on staff. Staff were motivated and committed to their work, experienced high levels of job satisfaction, had a strong commitment to the team and a strong sense of team spirit. The effective team working also contributed to lower levels of stress than the overall sample. Figure 5.2 illustrates the positive levels of staff engagement and wellbeing of the case study teams compared with the overall sample results.
Figure 5.2
Staff Engagement and Well-being
4.20
5.27
4.90
5.72
1 2 3 4 5 6
Well-being atWork
Team EngagementCase studyteams
Otherteams
(1 = least positive, 6 = most positive)
5.4.1 Reasons for positive staff morale and wellbeing
Intrinsic motivation
It is very clear from the interviews that the team members were extremely motivated by the nature of the job they do. This, in part, was down to the TLs’ ability to recruit the right staff to the team and, as discussed, have the right values to work in the team. Because of this, team members get immense satisfaction from seeing service users improve and recover, illustrated by the following quotes:
“The job is massively rewarding. I’ve seen lots of positive results and outcomes over the years”.
“The main goal is to discharge back to the GP. It’s really rewarding, really lovely to see – it’s so positive”.
Nature of the work
© Leading to Quality 2013 – All rights reserved Page 95
As is evident from the above, team members experience a great degree of satisfaction seeing service users having positive outcomes from their care. A couple of team members from separate teams explained that the degree of satisfaction staff experience in respect to this depends on the nature of the team’s work:
“It’s pretty clear we’re making a difference, unlike assertive outreach work which is for serious and enduring illnesses and difficult to engage clients. Early intervention is refreshing”. Early intervention is for a specific service user group and for a time limited period, which means the team can work with more focus than other teams. As such “you don’t get ground down with the issues other services have”.
This is an interesting observation and relevant to current service transformations. For example, some trusts have recently split generic CMHTs into common mental health problems on the one hand, and severe and enduring mental health problems on the other. Some concerns were expressed that people working purely with severe and enduring mental illnesses would experience higher levels of burnout and less satisfaction. Leadership
The TLs’ engaging leadership approach, as discussed in depth, is key to maintaining staff morale, engagement and wellbeing. The main themes relating to this are:
Motivating staff through their inspirational behaviours and attitude, their ability to sustain shared vision and their positive approach to leading the team. For example:
“TL is at the helm motivating and steering you. I love coming to work and doing my job”;
Increasing job satisfaction and self-confidence through their empowering style, their commitment to developing individuals and the team, and their genuine appreciation of staff’s contribution;
Promoting staff wellbeing through genuinely caring for staff, supporting them at times of difficulty, adopting a collective approach to managing risk, and being mindful of staff’s workload.
The following quote from one of the team members is a very powerful example of the impact his/her TL’s supportive approach to managing change had: “the TL is the only reason I didn’t go off sick”. In this circumstance, the TL did not only listen to people’s concerns, s/he acted on these and took practical steps to reduce stress (e.g. reducing caseload);
Consistently engaging the team in discussions regarding progress, problems, seeking suggestions, and being accessible to staff;
Creating a sense that the teams are in “safe-hands” due to the way in which they advocate on behalf of the team, manage performance in the team and balance the needs of the team with the needs of the organisation. This promotes a feeling of trust, confidence and reassurance
Team working

© Leading to Quality 2013 – All rights reserved Page 96
The effective team working, mediated through leadership, discussed in depth was felt to be crucial in maintaining staff wellbeing and engagement, as illustrated by the following quote:
“I feel that some of the other teams would benefit from our approach. Everyone starts work motivated but it’s how the team works that keeps this going”.
There were very positive relationships within the case study teams, with team members feeling valued and supported and enjoy coming to work. These relationships were considered to be a key reason as to why interviewees were motivated and committed to their work. In relation to this, team members “do not want to let colleagues down, so give 110% all of the time”. The supportive relationships within the team were considered to help because there is always support, help and advice available when problems are experienced. Also, as discussed, the humour present within the teams allows team members to off-load to their colleagues, knowing that they will not be judged.
5.4.2 Factors that detract from positive staff morale and wellbeing
Nature of the work
Whilst the nature of the work was a motivating factor for staff, as discussed above, this can also be quite demoralising as “some clients aren’t prepared to put the work in”. Also, one of the interviewees felt that the recent focus on severe and enduring mental illness, excluding psychosis, had left him/her feeling less motivated.
Business culture
A clear theme to have emerged from two of the case study interviews was that the business values people felt were emerging in the service and the bureaucracy associated with this were considered to be detracting from the morale and wellbeing, as the following quote illustrates:
“I feel committed at times and demoralised at times. I don’t agree with the values of the business culture – it makes me feel suspicious. I feel we should be prioritising high quality care”.
Organisational changes
The recent reconfiguration of the services for some teams has been a cause of anxiety for the team which, to a large extent, has been alleviated by the TL and the supportive team (as discussed above). However, people are still “worried about what is around the corner”. Organisational changes have also had a depletory effect on organisational commitment, as illustrated by the following quotes:
“My commitment hasn’t wavered but my satisfaction has gone down and my frustration has gone up”.
“I am a bit cynical about the organisation but still committed to my work”.
© Leading to Quality 2013 – All rights reserved Page 97
To conclude, there were high levels of motivation, commitment and job satisfaction within the case study teams, with good intrinsic motivation, team working and leadership playing a key role in this. Levels of stress were lower than the overall sample average, which was largely attributed to the TL and the supportive relationships within the team. Factors that detract from staff engagement and wellbeing were difficult to engage service users, organisational changes and the perceived business culture that now exists within .the health sector.
5.5 Quality of care It was generally felt by the case study teams that they do provide good quality of care and, as can be seen from the comments above, the teams’ ways of operating reflected most of the key themes in the constructs that emerged from service users and their carers as to what is high quality care. The teams’ belief with respect to this is an indication of their sense of team potency. Methods of collecting feedback on quality of care
The teams’ belief that they provided good quality care was informed through a variety of sources:
Feedback from service users
Good quality informal feedback from services users on a regular basis. Through conversations or actions such as “getting a hug on discharge”.
Formal feedback from service users in the form of questionnaires. The different teams collected this feedback to a greater or lesser extent and, on the whole, it was not a strong form of feedback for the teams. It was evident when the research team sought uniformity across trusts that there appeared to be little in the way of a systematic or uniform approach to assessing service user perceptions of quality of care across the trusts.
Feedback from service user events: One of the teams had an event called ‘Picnic in the Park’ where service users and staff spent time together identifying how the service could be improved. This event led to an action plan, which the team then followed-up. As an example, one of the outcomes last year was for the team to provide help numbers on the back of their appointment cards.
Observing service users’ recovery and discharge from their service
The most frequently mentioned way of assessing quality of care was the feedback teams got through seeing service users recover and being discharged from their service. Service audits
Service user audits were used by a couple of the teams to build an evidence base for the effectiveness of the service. For example:
One team had recently undertaken an audit to see how effective their psychosocial interventions were;

© Leading to Quality 2013 – All rights reserved Page 98
One team had undertaken an audit of their service users’ transition to work;
One team had been evaluating the work of their health and wellbeing practitioner through monitoring the impact of physical activity on weight gain/loss once service users have started on antipsychotic medication.
Outcome tools
One of the teams in particular spoke of how they used outcome tools to measure the effectiveness of the care they provide, such as the HONOS section of the Mental Health Clustering tool and using ‘The Recovery Star’ to demonstrate and map outcomes in specific domains.
Enablers to providing good quality care
In essence, all the previously mentioned elements of team working and staff engagement, facilitated by good leadership, come together to provide a good quality service for service users, including:
A strong and passionate vision for providing good quality care and the motivation and commitment of the teams to deliver this vision;
The multidisciplinary nature of the teams resulting in a broad range of expertise and experience, enabling the teams to provide a holistic, flexible and seamless service. As discussed, providing a holistic, flexible and seamless service were clear themes emerging from the interviews with service users and carers about what a good quality service consists of;
Positive relationships within the team, providing the support and trust required for the team to work collectively/cohesively to achieve their goals, combined with a strong sense of team potency;
Effective communication at a formal and informal level, allowing for good care planning, reflection, problem solving, timely response to issues and problems, and good positive risk taking;
A culture of innovation, improvement, learning and development in which the teams strive to ensure the care they deliver is the best it can be;
Effective individual and group clinical supervision, and, in some teams, case load management and managerial supervision. Again, these allow for good care planning, reflection, problem solving, timely response to issues and problems, and good positive risk taking;
Commitment to building positive relationships with other teams and agencies so that service users experience an integrated and seamless service;
Effectively adapting to change;
Effective performance management within the team;
The ability and willingness of the TL to advocate on behalf of the team and the service.

© Leading to Quality 2013 – All rights reserved Page 99
To illustrate the points made above, a good example of how effective team working and leadership can result in better quality of care for service users is in relation to positive risk taking. Positive risk taking ‘is about making good quality clinical decisions to support and sustain a course of actions that will lead to positive benefits and gains for the individual service user’ (Morgan 2000). A clear theme to emerge from the case studies was that the teams’ multidisciplinary nature and the trusting and supportive relationships, effective communication, and genuine commitment to individual and group supervision within the teams had a positive impact on the teams’ ability to take positive risks, as did the supportive and engaging approach of the TLs. The integrated working, lack of blame culture, and shared decision making associated with these promote a culture of positive risk taking (Morgan, 2000).
Barriers to providing good quality care
The main themes to emerge with regards to barriers to providing good quality care are discussed below.
Time
Lack of time was considered to be the main barrier to providing good quality care. The main reasons for this were:
Administrative demands, such as the performance management requirements of payment by results, that reduce the time spent on service user care;
The size of the geographical area the team have to cover, which for two of the teams had increased substantially since the reconfiguration of their service;
Size of caseload, although at the time of the interviews all the case study teams felt their caseload size was manageable.
As mentioned above, lack of time limits the time staff can spend on service user care. It also limits the extent to which teams can undertake innovation, improvement and development activities. Lack of skills On the whole the case study teams were multidisciplinary, which, as discussed, has many advantages. Where there was a perceived lack of skills this was felt to result in a less flexible and less integrated service for service users. Relationships with other teams
As previously mentioned, positive relationships with other teams in the same trust are critical for an integrated service. When there are difficulties with these relationships the quality of the service user experience can be reduced.
External agencies/interfaces with other services
A clear theme to have emerged from the case studies was an increasing lack of interface with external agencies, which was felt to have a constraining effect on quality of care. This was largely to do with limited funding available for other services. For example, a team

© Leading to Quality 2013 – All rights reserved Page 100
member from an early intervention team mentioned how funding for education is difficult to obtain once a person is over 18, meaning that service users may not be able to engage in this meaningful activity. Other teams spoke of how relevant services were being cut or closed, such as REMPLOY and day centres, meaning the package of care offered to service users is restricted.
To conclude, the teams generally felt they provide good quality care, which was due to effective team working and staff engagement, facilitated by good leadership. However, quality of care was considered to be compromised by time constraints, skills shortages (when present), and difficulties experienced with teams and services external to the teams.
5.6 Synthesis of the qualitative and quantitative data
The model of the relationships between team leadership, team working, and the impact of both on team goals (team process outcomes, or quality of care) and impact on team members (team engagement and wellbeing at work), that emerged from the case study data is very similar to the model that was validated on the basis of the quantitative data. It was evident that:
different aspects of team working had an impact on team engagement and wellbeing,
team leadership impacted on team working, and acted on both aspects of impact on team members through team working. These are important points of similarity.
intra-team working and inter-team and inter-agency working can be regarded as both contributing to team working overall.
At the same time, some differences between the two models were noted:
the leadership of the team, which was assessed with slightly different, but directly comparable, indicators of leadership, appeared to have an additional direct impact both on team engagement and wellbeing at work, and quality of care. However, as the case study data were collected among higher performing teams, it is not known whether these qualitative findings would generalise to all teams.
there was evidence from the case studies that level of team engagement and wellbeing at work could itself be seen to have a direct impact on quality of care.
In relation to the comparability of the data from these two qualitative and quantitative sources, it is relevant to note that:
the case studies provide a very rich source of information about MH teams and how they function that could not be obtained in any other way;
such information adds ‘flesh to the bones’ of the quantitative findings and, as such, provides enormously valuable information about team dynamics;
this ‘triangulated’ information is a source of confidence in the model of team leadership and team working that was tested;
in combination, the data point clearly to ways in which both team leadership and team working can be developed and enhanced.
© Leading to Quality 2013 – All rights reserved Page 101
The case study findings were consistent with the I-M-I-O model. The effective team working described by the teams illustrates the mediating and iterative processes involved in the I-M-I-O model of team working. Mediation is evident from the positive affective states (e.g. social support, trust and psychological safety), behavioural processes (e.g. regular team meetings) and cognitive states (e.g. shared mental models). Iterative processes were evident from reflective nature of the teams and culture of innovation and improvement evident – i.e. the teams reflect on and respond to their own performance and the environment around them.
5.7 Summary of main findings and conclusions 5.7.1 Effective team working
Effective team working was characterised by:
An overwhelmingly strong vision and values amongst the teams to provide good quality, recovery-focused care for service users. This strong vision and values was reflected by the staff, who were passionate, enthusiastic and committed to providing an excellent service, and it provided a guiding framework for the direction of the teams and how they operated.
The multidisciplinary nature of the teams, allowing for a holistic, flexible and seamless service. The good communication and support within the team ensured there were formal and informal forums for the different disciplines to input into service user care. The skills and experience of team members adds to the sense of team potency within the teams.
There positive relationships within the teams, being characterised by harmony, although with the right degree of challenge, support and respect. These relationships indicate that there was a high level of social support and a great deal of trust and psychological safety within the teams, which sets the right culture for individuals to perform at their best and to deliver an effective service. The positive relationships within the teams were also a reason for positive levels of staff engagement and wellbeing.
Effective and engaging communication within the teams on an informal and formal level. A particularly strong theme was that there were regular team meetings, which were prioritised and valued by the teams. These meetings were an opportunity for the teams to evaluate progress, share ideas, problem solve and plan for the future. They provided a forum for all disciplines to work together and to provide their specialist knowledge and experience. They were considered to be very useful from a positive risk taking perspective as they gave team members a sense of shared decision making and shared responsibility, rather than one person being solely responsible. This in-depth communication also ensures that there is good continuity of care for service users in the absence of their care coordinator. As well as having a positive impact on the service user experience, the regular team meetings also help from a team bonding perspective as they provide a forum for all team members to be together. This was especially important for one of teams who worked over split sites. In relation to this, the opportunity to “off load” to colleagues and discuss concerns, helps with staff wellbeing through reducing stress.

© Leading to Quality 2013 – All rights reserved Page 102
A culture of innovation and improvement within the teams, where creative ideas, reflection, problem-solving, and individual and team development were encouraged. There was also a genuine commitment to development and supervision, at the individual and group level. There was a sense that teams were striving to be the best they could be. The culture of innovation, improvement and development very much relates to the positive relationships within the team’ and effective communication. Feeling ‘safe’ to make suggestions, admit mistakes and having opportunities to communicate meaningfully, meant that a culture of innovation, improvement and development could flourish.
Positive relationships with other teams and agencies. The teams try to ensure that this is the case as they recognise positive relationships are important for service user care. They do this through trying to work effectively with teams on an individual level and also through having members of the team that formally link with other teams. Difficulties arise due to pressures on other teams and agencies, different perceptions of risk, service transformation, and establishing the appropriateness of service users for the team. Teams try and overcome these difficulties through organising face-to-face meetings, being flexible, and depoliticising the situation.
The effective team working described above was considered to be key to helping the teams adapt to organisational changes.
5.7.2 Effective Leadership
All of the TLs were respected and valued greatly, for some teams this strength of feeling was exceptionally strong. There were many similarities in their leadership approaches, which were very consistent with the Model of Engaging Leadership (Alban-Metcalfe & Alimo-Metcalfe, 2007; Alimo-Metcalfe & Alban-Metcalfe, 2001; 2003; 2010) outlined in the introduction to this report. The effective leadership displayed in the case studies orchestrated the effective team working described above. The TLs were felt to be extremely passionate about providing a good quality service,
consistent with their team’s values. This served to unite and motivate the teams.
As indicate above, the TLs were considered to be inspirational by their passion and determination, strong work ethic and the way in which they acted as a role model.
The TLs displayed very similar engaging leadership styles which were characterised by: being democratic but decisive, situational leadership, open and honest, positive leadership, hands on leadership, and empowering leadership. These leadership styles promoted a sense of trust and respect for the leader, with team members feeling they were in ‘safe hands’. They were also important to promoting a sense of staff engagement, especially through the leaders’ positivity, democracy and the extent to which they empowered and involved the members of the team.
It was clear from all the case studies that the TLs were very focused on the team as a unit and the individuals within it. They recognised that staff were the key to working effectively and achieving the teams’ goals, and work hard to ensure that there is the right

© Leading to Quality 2013 – All rights reserved Page 103
culture and support for the team to flourish. They promoted a sense of “team”, so that all team members felt they were working as part of a united team, facilitated by the effective communication and team development discussed previously. This promotion of the sense of team was critical to the positive relationships found within the teams. The TLs understood their team members, making sure they worked to their strengths and providing extra support in relation to their limitations. They also valued team members, which had a positive impact on team members’ motivation and commitment.
The TLs were considered to be exceptionally supportive, which was critical to staff wellbeing as it helped to avoid/relieve stress and anxiety, and also was felt to help with positive risk taking.
TLs, to a greater or lesser extent, were willing to manage performance within the team. It was clear from the interviews that the TLs’ ability and willingness to manage performance in a timely and effective manner had a positive impact on the team as it promoted respect, confidence, reassurance and trust, and meant there were clear standards of acceptable behaviour within the team, which promoted positive team functioning and positive service user experiences.
One of the difficulties TLs faced was having to balance the needs of the team/service with the needs of the organisation. There was a general perception that initiatives from the wider organisation had become more bureaucratic, which was a cause of resentment. The TLs could, on the whole, understand the rationale for the trust requirements. They would communicate this to the team, expect that there was compliance and, where necessary, support team members to comply. However, the TLs were individuals that were able to question and challenge trust initiatives and were prepared to act as an advocate for the team to try and shape/influence what was required. The TLs’ willingness to act as an advocate for the team inspired confidence and trust in team members, making them feel safe and supported.
The TLs’ employed a variety of approaches to managing change within the teams, which were felt to have led to the effective management of change. The approaches they adopted inspired confidence and trust in team members, promoting positivity and relieving the anxieties caused by uncertainty. They also helped staff feel supported at an individual and team level. This, combined with creating a learning and developmental culture in the team, and with high social support, will strengthen a team culture of ‘high readiness for change’, which is so critical in the NHS.
5.7.3 Staff wellbeing and engagement
There were high levels of motivation, commitment and job satisfaction within the teams, with good intrinsic motivation, the nature of the work, team working and leadership playing a key role in this. Levels of stress were lower than the overall sample average, which was largely attributed to the TL and the supportive relationships within the team. Factors that detract from staff engagement and wellbeing were difficult to engage service users, organisational changes and the perceived business culture that now exists within .the health sector.
5.7.4 Quality of care
© Leading to Quality 2013 – All rights reserved Page 104
The teams generally felt they provided good quality care, which was due to effective team working and staff engagement, facilitated by good leadership. However, quality of care was considered to be compromised by time constraints, skills shortages (where present), and difficulties experienced with teams and services external to the teams.
On the whole, it was evident when the research team sought uniformity across trusts that there appeared to be little in the way of a systematic or uniform approach to assessing service user and carer perceptions of quality of care across the trusts.
Conclusion
The results found that effective team working was perceived to be critical to staff wellbeing and engagement and to quality of care for service users. Leadership facilitated the effective team working to have this impact but also was felt to independently impact on staff wellbeing and engagement and on quality of care. Staff wellbeing and engagement had an independent impact on quality of care but this relationship was also facilitated through effective team working and effective leadership. The results are consistent with the model for the Leading to Quality research proposed at the outset of the project, confirming that effective team working and staff engagement lead to positive quality of care for service users and that leadership is instrumental in promoting effective team working and staff engagement.
© Leading to Quality 2013 – All rights reserved Page 105
Chapter 6 Discussion and Practical Implications
This final chapter brings together the findings from the data collected during the Leading to Quality research study. It focuses on addressing the aims and objectives of the study, which are described below. The chapter then goes on to explore the practical implications of the study, followed by an assessment of the project achievements and limitations.
6.1 Aims and Objectives of Leading to Quality
Title of the study:
‘An investigation of the impact of leadership and team working on staff morale and wellbeing, and team performance, among mental health teams within the Yorkshire & the Humber Strategic Health Authority’ The overall aims of the Project were to:
1. understand how leadership behaviour enables multi-professional teams to function most effectively in working to promote and sustain improved health outcomes for service users and carers;
2. devise and develop a set of guidelines, and a series of developmental activities, that will enable mental health professionals and others, to improve the quality of provision for people presenting with symptoms of mental ill-health and their carers.
In order to achieve this, the specific objectives were to:
identify the particular processes within teams that ensure engagement and wellbeing of team members and enable them to work most effectively;
identify ways in which the leadership of the TL has an impact on team functioning and performance;
develop in-house research capacity by involving local researchers in the trusts in data-gathering processes using the repertory grid interview technique and subsequent stages of the project;
adapt and develop diagnostic tools and interventions for measuring service users’ and carers’ perceptions of quality of care, and developing multi-professional team processes, leadership behaviour, staff engagement and wellbeing, and team effectiveness that can be used across a wide variety of health and social care contexts;
use the research findings to inform improved practice both within mental health services and more widely in health and social care.
6.2 Team leadership and team working: the research context The study of team leadership and team working has been the subject of discussion and research, not least in the UK National Health Service, with recent national studies of each providing important insights into both. So too, has the study of the impact of team leadership

© Leading to Quality 2013 – All rights reserved Page 106
on team performance, and of employee engagement and wellbeing at work. Each of these continues to be high on the DH agenda.
The Leading to Quality study builds on an earlier national study which provided evidence of:
a cause-effect relationship between an engaging style leadership on the performance of crisis resolution teams;
a predictive link between team leadership on the level of engagement and wellbeing of team members.
However, it extends it in two important ways:
by examining both team leadership and team working in terms of (a) the nature of the relationship between them, (b) the impact they have on quality of care and the team process outcomes of innovation and improvement, and (c) the impact they have on team engagement and wellbeing at work;
researching a much wider range of MH teams.
6.2 Results of the EngagingTeams360 questionnaire The results of the EngagingTeams360 were, overall, very positive, indicating positive levels of team working and leadership across the Region. The principal findings are outlined below.
6.2.1 Team working: Areas of relative strength & areas for potential development Areas of relative strength Of the 18 scales measuring either team leadership or team working, the highest average ratings were (in order of magnitude with highest first): Social Support; Collective Experience; Updating, and Team Potency. The scores ranged from 5.04-4.99 on a 6-point scale, with 6 being the most positive. Comment: Such ratings compare favourably with data from other MH team studies, and reflect areas of strength in these four key aspects of effective team working. The team strengths described above appear to emphasise the relational behaviours within the team (their attitudes and beliefs about their team, and about themselves as individuals working together effectively) and also team members’ belief that the team can be successful in meeting its objectives. Such behaviours have been found to be very important for creating a culture of ‘high readiness for change’, and of building a sense of ‘team resilience’.
Areas for potential development
Of the same 18 scales, the lowest scoring areas were (from lowest to highest ranging from 4.55 – 4.76): Roles and Responsibilities; Valuing Different Perspectives; Supporting a Development Culture; Inter-team and Inter-agency Relations, and Inter-team and Inter-agency Collaboration.

© Leading to Quality 2013 – All rights reserved Page 107
Comment: Although the average ratings are of the same order of magnitude as comparable data from other MH teams, they reflect areas of relative weakness in one of the aspects of team working (Roles and Responsibilities) that is crucial to defining ‘genuine’ teams as distinct from ‘pseudo’ teams. For teams where the ratings are low, this is an issue for concern. Of concern also are two aspects of the culture of the teams (Valuing Different Perspectives, and Supporting a Development Culture). Those in a leadership role should consider what action can be taken to ensure:
1. that the views of all team members are listened to and respected, and
2. that there a positive, learning-orientated, rather than a ‘blame’ culture, so commonly found in other areas of the NHS.
One way of interpreting these findings is to reflect on whether the underlying theme here concerns behaviours that are not sufficiently task-focused, information-focused, knowledge-focused and/or decision-focused. The lower ratings on these scales may explain why the team process outcomes (see below) of Improvement and Focus on Quality were relatively low.
Finally, a third area of concern is the relatively low scores of inter-team and inter-agency working, particularly as:
- there is consistent evidence of its importance to effective team working,
- the likelihood that such behaviours will increase in importance in the NHS,
- such behaviours are at the heart of multi-disciplinary team working in MH, and
- the evidence reported here indicates that service users and carers judge the effectiveness of the MH team to work closely with other teams and agencies as an important criterion for the quality of continuous care they received.
6.2.2 Team Leadership The team leadership was regarded positively (the results of the 4 scales ranged from 4.85-4.80). Such ratings are also of the same order of magnitude as comparable data from other MH teams. Given the evidence reported here and in other studies of the relationship between team leadership and team working, and – for reasons discussed below – the way that team leadership impacts on team process outcomes and on team members’ engagement and wellbeing at work, this constitutes reassuring evidence.
6.2.3 Team Process Outcomes
The ratings on the scales that measured two of the aspects of team process outcome were: Improvement (4.55), and Focus in Quality (4.61). Of the 21 scales measured, these scales were either lowest or third lowest.
© Leading to Quality 2013 – All rights reserved Page 108
Comment: Although the average ratings were of the same order of magnitude as comparable data from MH teams, for those teams with low ratings in relation to two goals that are not only important in themselves, but are also high on the DH agenda, are matters of concern. Clearly, they are key areas on which to focus development. Details are provided in Chapter 4 on which specific behaviours would appear to have the potential for the most positive effect. Interestingly, the rating for the team process outcome Innovation was 4.91 (seventh highest of 21 scales). Such ratings are also of the same order of magnitude as comparable data from other MH teams, but differences between ratings of innovation versus improvement does serve to underline the distinction between them.
Again, details are provided in Chapter 4 as to (1) which behaviours contribute most powerfully to innovation as distinct from improvement, and (2) would appear to have the potential for achieving the most positive developmental outcomes.
6.2.4 Impact on Team Members The average ratings on the two scales were: Team Engagement (5.30) – highest rating out of 21 scales, and Wellbeing at Work (4.26) – the lowest of 21 ratings.
Comment: This finding is almost the antithesis of what would be expected. This is because, although both scores are of the same as found in comparable MH teams, evidence from very many other studies suggests that level of employee engagement and wellbeing at work are highly correlated. Why there should be such a difference in the ratings here can only be the subject of speculation, though the hypotheses could be proposed (1) that levels of team engagement are high because of the personal dedication of members of MH teams to the work they do, and (2) that levels of wellbeing at work are lower because of the conditions under which they work. This issue would appear to merit urgent consideration. Valuable information is provided in Chapter 4 on the specific team working behaviours that predict Team Engagement and Wellbeing at Work.
6.2.5 The relationship between Team Leadership and Team Working Although a number of studies have found evidence (1) that team leadership and team working are significantly inter-correlated, and (2) that they are both correlated with impact on outcomes of team effectiveness, this study presents empirical evidence of the nature of the relationship between them.
What the empirical evidence presented here indicates is that team leadership acts through team working in the way that it impacts on (1) team performance (innovation, focus on quality, and improvement) and (2) team members (team engagement and wellbeing at work), and not directly.

© Leading to Quality 2013 – All rights reserved Page 109
Comment: This is an important finding, not just in itself, but because its significance is that it provides research support for the arguments, advanced by others, in favour of providing context-related, in-situ leadership and team working development (i.e., development that happens in the workplace and not in the classroom)
6.3 Case study results
The case studies provide a rich account of leadership and team working in community mental health services. They illustrate effective team working and leadership in practice, and also how teams and leaders cope with and adapt to the many changes they are faced. The relationships are presented in the model below.
Essentially, what the findings from the case study showed was that:
- Effective team working was perceived to be critical to staff wellbeing and engagement and to quality of care for service users;
- Leadership mediated the effectiveness of team working to have this impact, but also was felt to independently impact on staff wellbeing and engagement, and on quality of care;
- Staff wellbeing and engagement had an independent impact on quality of care (e.g., by affecting intrinsic motivation) but this relationship was also mediated through effective team working and effective leadership;

© Leading to Quality 2013 – All rights reserved Page 110
- Leadership and team working were critical to the team process outcomes of innovation and improvement, which had positive benefits for service users.
The case study results show evidence of qualitative support for the model for the Leading to Quality research proposed at the outset of the project; i.e., that effective team working and staff engagement lead to positive quality of care for service users and that leadership is instrumental in promoting effective team working and staff engagement. The case study results are, on the whole, consistent with the model to emerge from the quantitative results (Appendix 4.3); however the quantitative model did not provide evidence of a direct causal link between leadership and staff engagement and wellbeing. What it did provide evidence of, was that team leadership affects quality of care through its impact on the effectiveness of teams.
6.4 Quality of Care 6.4.1 Enhancing understanding of quality of care: contributions of Leading to
Quality
The project sought to understand ‘what is high quality care’ from the perspective of individuals for whom it is intended. Stage 1 of the research elicited over 450 constructs of ‘high quality care’ from 65 interviews with services users and carers, undertaken by the Research Champions, who were MH professionals in the participating trusts. The essential dimensions on which high quality care should be judged, and the specific behaviours of professionals that result in such care were identified. A comparison of the themes emerging from the constructs with the recently-published NICE Quality Standards for Service Users Experience in Adult Mental Health reveals that this aspect of the research augmented these guidelines significantly by:
- Providing a much wider-ranging understanding of the aspects of care mentioned by NICE
- Considerable detail in describing the ‘what’ and the ‘how’ of providing high quality care
As well as augmenting the NICE standards, the comparison identified at least 3 significant, and new, components of what is high quality care including: the critical importance of strengthening users’ sense of self-efficacy – not explicitly mentioned by NICE; (2) emphasising that care should be holistic – not explicitly mentioned by NICE; (3) stressing the importance of good communication in MH teams, and with other agencies and sources of support. 6.4.2 Developing Quality of Care Questionnaires
The constructs from the interviews with service users and carers formed the basis of the development of 2 new, psychometrically robust, ‘Quality of Care Questionnaires (QCQs)’ – one for service users, and a separate one for carers. These were then distributed amongst service users and carers, producing feedback from a total of n = 649 users and carers (452 from service users, 197 from carers).
6.4.3 Satisfaction with quality of care

© Leading to Quality 2013 – All rights reserved Page 111
Service user satisfaction with quality of care
The analysis of the service user results showed that service users responding to the survey felt very satisfied with the care they receive. The most positive items were in relation to personal relationships and respect for service users as individuals with specific needs. It is interesting to note that the items that were the lowest scoring (although still positive) were the ones associated with increasing self-efficacy, which is a major criterion by which quality of care is perceived by service users. It is also a fundamental component of the ‘recovery’ approach to care. Carer satisfaction with quality of care
The results of the carer ‘Quality of Care Questionnaire’ were also positive but less positive than the service user results. The most positive areas emerging from the carer questionnaire were similar to the service user questionnaire, in that carers find professionals to be approachable and communicate in a way that carers can understand. Carers also think that the person they care for is treated as an individual. Areas in which carers felt less positive were in relation to how involved in/informed they were in relation to the person for whom they care, suggesting that work could be done on improving the “triangle of care”. 6.4.4 The impact of team working and leadership on quality of care The impact of team working, leadership and staff engagement on quality of care could not be assessed by an independent outcome assessment from services users and carers, and/or by an ‘objective’ measure from the teams, since none was available that was standardised to all teams in the study. However, quantitative data collected from teams’ ratings of the outcome of their working, on their effectiveness, in relation to Innovation, Focus on Quality, and Improvement, served as a ‘proxy’ for these measures. Although the researchers are aware of the potential bias of such data, such measures have been used regularly in previous related studies (e.g. West et al., 2012), and comparisons of any emerging relationships between variables could be made with studies that have gathered objective measures (Alimo-Metcalfe et al., 2007, 2008).
Analyses of the data from the EngagingTeams360 questionnaire has identified which particular scales of team working, and specific behaviours, impact significantly on Innovation, Focus on Quality, and Improvement. Such analyses have also identified which particular scales and specific behaviours impact significantly on Team Engagement, and team members’ Wellbeing at Work. In addition, findings from the analysis of the teams’ quantitative data (described above) could be compared with (1) the qualitative data from the service user and carer interviews, and (2) from the case studies conducted in the Leading to Quality study, which provide rich data on this relationship, which serve to triangulate the findings, and thereby, create greater confidence is their validity. It was clear that the service provided by the best practice case studies (e.g. holistic, flexible and seamless) was consistent with the service user perceptions of what constitutes good

© Leading to Quality 2013 – All rights reserved Page 112
quality of care, as elicited from stage 1 of the research, and also with some of the NICE Quality Standards (2011).
6.5 Recommendations for practice 6.5.1 Case studies as a source of reference
The case studies provide rich information and guidance on best practice in leadership and team working. They can be a source of reference for teams and leaders to learn from. They provide very practical examples of how leaders manage change effectively, manage performance and how teams work effectively with other teams and agencies. They also illustrate the behaviours in team leaders and team members that promote the supportive, trusting and psychologically safe culture required for innovation and improvement, staff well-being and good quality of care.
6.5.2 Team and leadership development
Data from the analyses of the EngagingTeams360 instrument described in detail in Chapter 4 provide very clear indications of which aspects of team working significantly impact on which outcomes, and identify specific behaviours. However, it should be borne in mind that the analyses are based on the complete data set, and the relative priority areas of strength and development will vary between teams. To this end, team and leadership development that improves and promotes engaging teams and engaging leadership should be encouraged. As part of the Leading to Quality project, a team and leadership Development Toolkit is being produced that provide development materials for teams and leaders to do just this; it is recommended that teams/trusts utilise these resources. The toolkit will be based on the quantitative and qualitative findings from the research. Given the findings that leadership had a positive impact on outcomes, such as staff wellbeing and engagement, via influencing team working, this suggests that the most appropriate form of leadership development, and team development, is through in-situ development (i.e. in the classroom rather than in the workplace). This has been suggested in many commentaries in the development literature.
6.5.3 Prioritising effective and engaging communication, improvement, innovation and development
Some of the best practice findings to emerge from the case studies could be considered time consuming, for example regular in-depth team meetings, clinical supervision, and team away days. At a time when work demands are considered to be getting higher, especially with extra administrative requirements, it may be difficult for teams to feel they can prioritise such activity. However, considering the immense benefits to MH teams, and which, as a result, are most likely to benefit service users and carers, as was a evidenced in the study cited above of high-performing CRTs (Alimo-Metcalfe et al., 2007, 2008), it is urged that teams make the time for regular meetings that allow space for reflection, problem solving and shared decision making.

© Leading to Quality 2013 – All rights reserved Page 113
It is important also to note, that when activities such as team meetings and away days take place they are well structured and well managed, with their usefulness and effectiveness regularly reviewed (West et al, 2012).
6.5.4 The importance of Innovation, Focus on Quality, and Improvement
In relation to the above (6.5.3), the importance of innovation, quality and improvement have been made clear by the Department of Health (DH, 2012), which is entirely consistent with the aims of the Leading to Quality research. Given the relatively low scores for Focus on Quality, and Improvement, this should be considered carefully by teams.
6.5.5 Enhancing staff wellbeing
Considering the worrying finding from the team questionnaire data that team wellbeing scores were the lowest of all 21 scales scores, and combining this knowledge with the findings that emerged in the analysis of the team questionnaire, which identified the specific aspects of team working that significantly predict wellbeing, such as team members’ sense of social support, understanding of each other’s roles and responsibilities, etc., it is clear that this should be regarded as an investment, rather than a cost. This would appear to be a particularly strong message for trusts to convey to teams, as well as exploring with team leads how trusts can best support their efforts in this activity.
6.5.6 Reducing administrative demands
In relation to the above, trusts should consider if it is possible to reduce the administrative requirements placed on staff, such as collecting and inputting performance/contact information, and defensible documentation. It may be that there are more efficient ways of collecting this information that would release more time for staff to focus on improvement, innovation and service user care.
6.5.7 Quality of care
The findings from the analysis of data from the questionnaires has provided the participating trusts with valuable feedback from a significant number of service users and carers. The analysis has also shown in which aspects of care, quality is highest, and which are the aspects of care that can be improved. Teams and trusts care refer to these results to identify areas where they might try and improve.
6.5.8 Collecting service user and carer feedback
On the whole, there appeared to be little in the way of a systematic or uniform approach to assessing service user perceptions of quality of care at a team level within, and between, trusts. While some trusts had systems in place to collect this feedback routinely, there is not a uniform standardised quality measure used across teams, making it difficult to draw robust conclusions. In addition to this, as mentioned in Chapter 3, the questionnaires currently used to obtain service user feedback do not sufficiently measure service users’ and carers’ views of what is quality of care.

© Leading to Quality 2013 – All rights reserved Page 114
The use of the Quality of Care Questionnaires developed from the Leading to Quality research across a range of mental health organisations within the region (or nationally) would enable the standardisation of assessments of the quality of care provided, and significantly increase the validity of the data collected. This would have a variety of benefits:
- feedback to improve the service
- data on which to review individual, team, and inter-team and organisational performance
- support MH team development – identifying strengths and areas for development
- support leadership and professional development
- support individual supervision and appraisal
- identify the impact of an intervention
- use in research
While encouraging teams to collect more quantitative service user feedback might appear contradictory to the suggestion above of reducing the administrative demands on teams, it is such a fundamentally important means by which teams and trusts can ascertain the impact of their service provision, that trusts might consider how to collect the feedback in the least labour-intensive manner for staff who deliver the service.
6.5.9 Repertory Grid Interviews
An unanticipated benefit from the process of Repgrid interviews was that several service users and carers remarked that the interview process was a valuable experience for themselves. For example, some reported that it enabled them to express themselves with greater ease. It is worth considering whether repertory grid interview training should be offered to more professionals in the trusts. The process is extraordinarily versatile in how it can be applied to obtaining individuals’ views of the world, and for various diagnostic processes, including those relating to learning and development. One particularly valuable application of the process is with regards to evaluating the impact of an intervention, or change.
6.6 Implications for service organisation and transformation
6.6.1 Size of the team
It was clear from the quantitative and the qualitative results that team size was important for effective team working, with smaller teams being more effective than larger teams. There was a clear difference from the EngagingTeams360 results between teams that had fewer than 20 members, and teams that had 20 or more members. All the best practice case study teams had fewer than 20 members. From the case studies, it was clear that a lot of effective team working was due to a shared vision and sense of direction, effective and engaging communication within the team, as well as the supportive and trusting relationships. These elements of team working may be difficult to establish and sustain in larger teams. If teams comprise 20 or more members,
© Leading to Quality 2013 – All rights reserved Page 115
considerable thought needs to be given as to how effective team working and leadership can be sustained within this. For example, how are teams going to establish and maintain a supportive and cohesive culture, and ensure every member can regularly participate during meetings?
6.6.2 Importance of multidisciplinary team working
The quantitative findings from the research indicate that multidisciplinary teams are important for effective team working, which is consistent with the research literature. However, multidisciplinary working can also cause difficulties within teams due to the presence of ‘faultlines’ or divisions in teams. The case study findings support, and supplement, the quantitative findings from the research by adding detail as to how and why multi-professional team working is effective, and how it can be strengthened.
6.6.3 Stability of team membership
The perceived importance of the stability of the team on the positive relationships within the team is an important practical implication for service redesign and team restructure. For example, the case studies found that these relationships, rather than the nature of the work, were of more importance to some staff when faced with a choice as to which team to work following service redesign. While stability was important, the teams also recognised that some change was good, as new members of a team can bring a fresh perspective, bring new knowledge, expertise and skills, and contribute new ideas and a new approach to working. It is important for managers to consider how, during service redesign, positive relationships within a newly formed team can be nurtured and promoted. The case studies can be used as a source of reference for this as they illustrate how key leadership is to ensuring teams work well as a cohesive and integrated group, with shared aims and goals.
6.6.4 Shared sense of purpose
Having a clearly defined service with clarity of goals and purpose, is an important finding from the case studies, together with a collective commitment towards this within the team. When teams are undergoing periods of great change (e.g. with service transformation), this clarity of definition can be significantly reduced as the teams seek to re-establish themselves. Trusts, in partnership with the teams, need to provide teams with a clear purpose and goals, and ensure that the quality and regularity of two-way communication with the teams is high. Teams need to take ownership of this and establish how they can implement these goals in practice.
6.6.5 Nature of the work
A couple of the trusts had recently split their generic CMHTs into common mental health problems on the one hand, and severe and enduring mental health on the other. Some concerns were expressed that people working purely with severe and enduring mental illnesses would experience higher levels of burnout and less job satisfaction. During service
© Leading to Quality 2013 – All rights reserved Page 116
changes, trusts and team leaders should acknowledge that the change in the nature of the work may have implications for staff wellbeing and support staff to cope and adapt to this. This is particularly important in view of the fact that wellbeing was rated lowest by the teams.
6.6.6 The importance of effective and engaging communication
As discussed above, effective and engaging communication within teams is a key element of effective team working and leadership. This has implications for services that are considering designing working practices that involve remote and agile working. Services need to consider how effective and engaging communication can be maintained in any service redesign.
6.6.7 Supporting team leaders
It was evident from the case studies that managing a team, especially at times of major organisational change, is challenging for team leads. They are the interface between the team and the wider organisation, and balancing the sometimes conflicting needs of the two is difficult. As part of their positive and supportive leadership style, the team leaders in the case study organisations would shield their team from the stress/difficulties they were experiencing within their own role, whilst supporting their team through the changes. The team leads felt they were supported by their immediate manager, which was felt to be important. Support for team leads is a matter of serious consideration, especially at times of organisational change, since, as the Leading to Quality study found, they are critical to effective team working. A relationship with a line manager can have political elements to it and, therefore, may not provide the opportunity for team leads to ‘off load’ to the extent that they may need to, especially if part of this is due to their being loyal to their team. Apart from the potential personal damage to the individuals, it is well established in research, that stress is infectious. This needs to be a matter of reflection by trusts. Understanding how team leads cope with implementing change within their teams may be an avenue for future research.
6.7 Project achievements 6.7.1 In-depth understanding what quality of care means
As mentioned, the research obtained an in-depth understanding of what quality of care means from the perspective of service users and carers, and is probably the first to elicit such an extensive range of constructs of how services users and carers perceive high quality care. Many instruments developed to assess quality of care do not include such close involvement of service users and carers.
6.7.2 Development of 2 new psychometrically robust Quality of Care Questionnaires In relation to the above, the research has produced two valid and reliable questionnaires, developed from robust research, to measure service user and carer satisfaction with quality

© Leading to Quality 2013 – All rights reserved Page 117
of care. These questionnaires provide an extremely useful (and valid) basis for evaluating service user and carer satisfaction with quality of care.
6.7.3 Developing internal research capacity
The Research Champions, who conducted the service user and carer interviews at stage one of the Leading to Quality research study, were mental health professionals in the participating trusts. This investment in their development, plus the knowledge gained from their interviews with service users and carers, should significantly benefit the service. Their competence at undertaking repgrid interviews is evident from the extensive range and detail of constructs they elicited. They should not only be acknowledged by their trusts for their invaluable contribution to the study, but also their skills and expertise using this technique, positively exploited across the trust, for their benefit, and for that of the service. Clearly, given the extraordinary pressures they are under, resources would probably need to be provided to enable this to be of benefit to all involved. The Research Champions are being encouraged to write professional/academic articles about the research, with the support of the university research team.
6.7.4 Benefit of service user and carer interviews to service users and carers
A not insignificant outcome, and one directly related to the ultimate purpose of this project, was the unintended positive benefits to service users and carers of participating in the interviews. This was mentioned by almost all Research Champions, and, again, reflects their skill, commitment, and professionalism
6.7.5 Evidence- based model
A new evidence-based model of the relationship between team leadership and team working, and team outcomes – which was one of the key aims of the Leading to Quality research study.
6.7.6 Specific understanding of behaviours that lead to positive outcomes
The detailed quantitative analyses have allowed the identification of the specific team working and leadership behaviours that predict positive outcomes, including team engagement, staff wellbeing, innovation, focus on quality and improvement.
6.7.8 In-depth qualitative understanding of leadership and team working
The six best practice case studies have provided an in-depth understanding of the nature of team leadership and team working in community mental health services. They illustrate effective team working and leadership in practice, and also how teams and leaders cope with, and adapt to, the many changes they are facing.
6.7.9 Team level reports

© Leading to Quality 2013 – All rights reserved Page 118
Each team participating in the research that obtained a 30% response rate or more, for the EngagingTeams360 questionnaire, received a report of their findings, and a comparison of their results with the overall sample results. These reports provided useful feedback for the teams, including areas of strength and development.
6.7.10 Trust reports
Each trust involved in the research will receive a report of the findings for their trust, and a comparison of their trust results with the overall sample results. It will also incorporate their best practice case study.
6.7.11 Overall report of the findings
This overall report of the findings should be a useful reference to leaders and teams working in mental health services. It identifies areas for action and best practice that can be utilised to enhance leadership, team working, staff engagement and wellbeing, and, as a result, the quality of care experienced by service users and carers.
6.7.12 Developmental Toolkit
A practical developmental toolkit is in the process of being produced as an outcome of the research. This toolkit is based on the research results and contains several practical activities that teams, leaders and trusts can utilise to enhance:
- leadership and team working
- strengthen a culture of Innovation, Focus on Quality, and Improvement
- increase levels of Staff Engagement & Wellbeing
- strengthen inter-team working across the trusts and with other agencies
- quality of service provision
6.7.13 Leading to Quality stakeholder event:
A final event is to be held during May 2013 to disseminate the findings from the study and discuss their practical application. This event is open to the Chief Executives of the participating trusts and their teams.
6.7.14 Professional and academic articles
A series of articles will be produced to disseminate the research findings in professional and academic journals. As mentioned above, the Research Champions are being encouraged to participate in this activity. There has already been one article featured in the Health Service Journal about the findings from Stage 1 of the research6
6 Alimo‐Metcalfe, B. & Locker, A. (28.7.2011), High Five for Quality of Care, Health Service Journal.

© Leading to Quality 2013 – All rights reserved Page 119
6.8 Project limitations
6.8.1 Difficulty obtaining sufficient service user and carer feedback
The study commenced at the beginning of 2009, which was just prior to the major changes that mental health services have experienced in recent times. Whilst changes were anticipated, the extent of the changes in the NHS were difficult to foresee. As such it was: a) difficult to engage staff to participate in the research, and b) not possible to collect longitudinal data due to the lack of stability within the teams, which would affect the reliability of the data collected.
An alternative approach was considered, which was to attempt to collect standardised ‘objective’ measures of team effectiveness for all the teams and trusts, however, while trusts do collect such data, it is not standardised or uniform across, or sometimes within, trusts. There were also differences in the type of data collected, which meant that they could not be compared. Consequently, this suggestion had to be abandoned.
These difficulties meant that it was not possible to obtain sufficient service user and carer feedback at the team level for a statistical link to be made between service user and carer feedback on the one hand, and leadership, team working and staff engagement on the other. They also meant that, due to the lack of longitudinal data, it was not possible to establish a cause and effect relationship with any of the areas of investigation over time.
6.8.2 Limited generalisation
The study was restricted to community mental health teams for adults of working age in the Yorkshire and Humber region. It would benefit from being extended to other types of mental health services, and other areas of healthcare. This could be an area for further research.
Conclusion
The principle aim of the Leading to Quality research project was to build on previous research through enhancing understanding of how leadership behaviour in multi-professional MH teams enables teams to work most effectively, by ensuring their engagement and wellbeing, so that they deliver the highest quality of care. The multi-method approach employed in the research enabled the triangulation of the results to do just this. The combination of qualitative and quantitative research methods identified how team working and leadership impacts on staff well-being and engagement, team process outcomes (innovation, focus on quality, and improvement), and quality of care. The statistical data analysis produced a new evidence-based model of the relationship between leadership, team working and team outcomes, and an understanding of the specific behaviours that lead to positive outcomes. The focus on service user and carer experiences has provided a robust and in-depth understanding of what quality of care means from their perspective. The study reinforces and adds to the NICE Quality Standards (2011).

© Leading to Quality 2013 – All rights reserved Page 120
Apart from increasing theoretical understanding, the study has highly practical applications that can be utilised to enhance leadership and team working and, ultimately, to improve the quality of care offered to service users and carers, locally and across the whole NHS.

© Leading to Quality 2013 – All rights reserved Page 121
References Alban-Metcalfe, R. J. & Alimo-Metcalfe, B. (2000a).’An analysis of the convergent and discriminant validity of the Transformational Leadership Questionnaire’. International Journal of Selection & Assessment, 8, 3, 158-175. Alban-Metcalfe, J., & Alimo-Metcalfe, B. (2007).’Development of a private sector version of the (Engaging) Transformational Leadership Questionnaire’. Leadership & Organisation Development Journal, 28, 1 & 2, 104-121. Alban-Metcalfe, Jtte.& Alimo-Metcalfe, B. (2010). ‘Integrative leadership, partnership working, and wicked problems: A conceptual analysis’. International Journal of Leadership in Public Services, 6, 3, 3-13 Alban-Metcalfe, Jtte.& Alimo-Metcalfe, B. (2013) ‘Reliability and validity of the ‘Leadership Competencies and Engaging Leadership Scale’. International Journal of Public Sector Management (in press). Alban-Metcalfe, Jtte.&Llloyd, D. (2013). Employee Engagement with Systems Thinking and Lean: A Formula for Success. Leeds: Lædan Press. Alban-Metcalfe, Jtte.& Alimo-Metcalfe, B. (2010). ‘Integrative leadership, partnership working and wicked problems: a conceptual analysis’. International Journal of Leadership in Public Services, 6, 3, 3-13. Alimo-Metcalfe, B. (2013). ‘A critical review of leadership theory’.In Lewis, R., Leonard S. & Freedman, A. (Eds).The Psychology of Organizational Development, Leadership and Change. London: Wiley Blackwell. Alimo-Metcalfe, B. & Alban-Metcalfe, J. (2003). ‘Stamp of greatness’. Health Service Journal, June 26th. Alimo-Metcalfe, B., Bradley, M.& Conway, N. (2013). ‘Leadership for tough times: Evidence of a cause-effect relationship between engaging leadership and team productivity; a longitudinal study’. (In preparation). Alimo-Metcalfe, B. & Alban-Metcalfe, R.J. (2001).‘The development of a new transformational leadership questionnaire’. The Journal of Occupational & Organizational Psychology, 74, 1-27. Alimo-Metcalfe, B. & Alban-Metcalfe, J. (2008).Engaging Leadership: Creating organisations that maximise the potential of their people. London: Chartered Institute for Personnel Development. Alimo-Metcalfe, B., Alban-Metcalfe, J., Bradley, M., Mariathasan, J., &Samele, C. (2007). The impact of leadership factors in implementing change in complex health and social care environments: NHS Plan clinical priority for mental health crisis resolution teams. Research paper project reference SDO/22/2002. Alimo-Metcalfe, B., Alban-Metcalfe, J., Bradley, M., Mariathasan, J., &Samele, C. (2008). ‘The impact of engaging leadership on performance, attitudes to work and well-being at work: A longitudinal study’. Journal of Health Organization & Management, 22, 586–598. Allport, G. W. 1954. The nature of prejudice. Reading, MA: Addison-Wesley. Bandura, A. (1977) Self-efficacy: Toward a Unifying Theory of Behavioral Change, Psychological Review,, Vol. 84, No. 2, 191-215 Bennington, J. & Hartley, J. (2009). All systems go!: Improving leadership across the whole public system. Sunningdale, Berks: National School for Government. Bass, B. M. (1998). Transformational leadership: Industry, military, and educational impact. Mahwah, NJ: Erlbaum.
© Leading to Quality 2013 – All rights reserved Page 122
Boorman, S. (2009). NHS Health & Wellbeing. London: Department of Health. Christensen, C. (1997). The Innovator's Dilemma: When New Technologies Cause Great Firms to Fail. Boston: Harvard Business School Press. Cunningham, C.E., Woodward, C.A., Shannon, H.S., MacIntosh, J., Lendrum, B., Rosenbloom, D., & Brown, J. (2002). ‘Readiness for organisational change: A longitudinal study of workplace, psychological and behavioural correlates’. Journal of Occupational & Organisational Psychology, 75, 4, 377-392. Davidson L 2008, Recovery: concepts and application, Recovery Devon Group, UK. Cited in State of Victoria (2011) Framework for recovery-orientated practice. Mental Health, Drugs and Regions Division, Victorian Government Department of Health, Melbourne, Victoria Dawson, J. F. (2007). ‘Diverse meanings and measurements of diversity: An extension of Harrison and Klein’s (2007) typology’. Paper presented at the Academy of Management, Philadelphia, USA. Day, D. Gronn, P., & Salas, E. (2004). ‘Leadership capacity in teams’. Leadership Quarterly, 15, 857-880. Department of Health (2001).Mental Health Policy Implementation Guide. London: Department of Health. Department of Health (2008). High Quality Care for All NHS Next Stage Review Final Report. London: Department of Health. Edmondson, A. C., Bohmer, R. M. & Pisano, G. P. (2001). ‘Disrupted routines: team learning and new technology implementation in hospitals’. Administrative Science Quarterly, 46, 685–716. Glasby, J., Dickinson, H., & Peck, E. (eds.) (2006).’Partnership working in health and social care’. Special edition of Health and Social Care in the Community, 14, 373-4. Guzzo, R.A., Yost, P.R., Campbell, R.J., & Shea, G.P. (1993).‘Potency in groups: Articulating a construct’. British Journal of Social Psychology, 32, 87‐106. Hambrick, D., Cho, T., & Chen, M. J. (1996).The influence of top management team heterogeneity on firms' competitive moves. Administrative Science Quarterly, 41, 659-684. Harrison, D. A. & Klein, K. J. (2007).‘What’s the difference? Diversity constructs as separation, variety, or disparity in organizations’. Academy of Management Review, 32, 4, 1199–1228. Hartley, J. (2004) ‘Case study Research’, p323-333, in Cassell, C & Symon, G (eds) Essential Guide to Qualitative Methods in Organizational Research, London: Sage Healthcare Commission (2006). National findings from the 2005 NHS Staff Survey: Key findings summary. London: Healthcare Commission. Heaphy, E.D. & Dutton, J.E. (2008) ‘Integrating Organizations and Physiology: Getting Started’. Academy of Management Review, 33, 1009-1011 HM Government (2011).No health without mental health: a cross-government mental health outcomes strategy for people of all ages. Accessed at www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_123766 15th September 2011. Hobfoll, S.E. (2002). ‘Social and psychological resources and adaptation’. Review of General Psychology, 6, 307-324

© Leading to Quality 2013 – All rights reserved Page 123
Hogg, M. A., & Terry, D. J. (2000). ‘Social identity and self-categorization processes in organizational contexts’. Academy of Management Review, 25, 121-140. Hu, J & Liden, R.C. (2011) ‘Antecedents of team potency and team effectiveness: An examination of goal and process clarity and servant leadership’. Journal of Applied Psychology, 96, 851-862. Hüffmeier, J. &Hertel, G. (2011) ‘Many cheers make light the work: how social support triggers process gains in teams’. Journal of Managerial Psychology, 26, 3, 185 – 204. Huxham, C. &Vangen, S. (2005). Managing to Collaborate: The Theory and Practice of Collaborative Advantage. New York: Routledge Ilgen, D. R., Hollenbeck, J. R., Johnson, M. & Jundt, D. (2005). ‘Teams in Organizations: From Input-Process-Output models to IMOI models’. Annual Review of Psychology, 57, 517-543. Jing, F. F. & Avery, G.C. (2008). ‘Missing links in understanding the relationship between leadership and organizational performance’. International Business & Economics Research Journal, 7, 5, 67-78. Judge, T. A., Thoresen, C. J., Bono, J. E., & Patton, G. K. (2001). ‘The Job satisfaction-job performance relationship: a qualitative & quantitative review’. Psychological Bulletin, 127, 3, 376-407. Keller, R.T. (2006). ‘Transformational leadership, initiating structure & substitutes for leadership: A longitudinal study of research & development project team performance’. Journal of Applied Psychology, 91(1), 202-210. Kelly, G. A. (1955). The Psychology of Personal Constructs. Vols. 1 & 2. New York: Norton Kelly, A., Johnson, P. & Gill, R. (2006). ‘Time for a Change: A UK Model of Transformational Leadership’. Paper presented to the Annual British Academy of Management Conference, Belfast (September, 2006). Kouzes, J. M. & Posner, B. Z. (2009). ‘To lead, create a shared vision’. Harvard Business Review, January. Lau, D.C. & Murnighan, J.K. (1998). ‘Demographic diversity and faultlines: the compositional dynamics of organizational groups’. Academy of Management Review, 23, 324-340 Lim, B.C. & Ployhart, R.E. (2004). ‘Transformational leadership: relations to the five factor model and team performance in typical and maximum contexts’. Journal of Applied Psychology, 89, 610-621 Little, B. L. & Madigan, R. M. (1997).‘The relationship between collective efficacy and performance in manufacturing work teams’. Small Group Research, 28, 517–3. MacKeith, J. & Burns, S. (2008).Mental Health Recovery Star. London: Mental Health Providers Forum. MacLeod, D. & Clarke, N. (2009).Engaging for Success: Enhancing Performance Through Employee Engagement. London: Crown Copyright. McDowell, W.C. & Zhang, L. (2009). ‘Mediating Effects of Potency on Team Cohesiveness and Team Innovation’. Journal of Organizational Leadership & Business, Summer,1. Morgan, S. Clinical risk management: a clinical tool and practitioner manual. London: Sainsbury Centre for Mental Health (2000). Markiewicz, L. & West, M. (2011).‘Leading groups and teams. In Swannick, T & McKimm, J. (Eds.). ABC of Clinical Leadership. London: Wiley-Blackwell.

© Leading to Quality 2013 – All rights reserved Page 124
Maslach, C. (2011). ‘Engagement research: Some thoughts from a burnout perspective’. European Journal of Work and Organizational Psychology, 20, 47–52. Maslach C, Leiter M. P (2008). ‘Early predictors of job burnout and engagement’. Journal of Applied Psychology,93, 498–512. Mohammed, S. & Dumville, B.C. (2001). ‘Team mental models in a team knowledge framework: expanding theory and measurement across disciplinary boundaries’. Journal of Organizational Behavior, 22, 89-106. Mohrmann, S. A., Cohen, S. G., &Mohrmann, A. M. (1995).Designing Team-Based Organizations: New Forms for Knowledge Work. San Francisco: Jossey-Bass. Monitor website (2013) Re ‘Preventing anti-competitive behaviour’: http://www.monitor-nhsft.gov.uk/monitors-new-role/preventing-anti-competitive-behaviour; accessed January 8 2013. Morse, R.S. (2010). ‘Integrative public leadership: catalyzing collaboration to create public value’. Leadership Quarterly, 21, 231-245 Murray, A. I. 1989. ‘Top management team heterogeneity and firm performance’. Strategic Management Journal, 10, 125-141. Nahum-Shani, I. & Bamberger, P. A. (2011).‘Explaining the variable effects of social support on work-based stressor–strain relations: The role of perceived pattern of support exchange’. Organizational Behavior and Human Decision Processes, 114, 49–63. National Institute for Mental Health in England (2007).Mental Health: New ways of working for everyone. Accessed at: web.archive.org/web/20071130110626/http://www.nimhe.csip.org.uk/our-work/workforce/new-ways-of-working-in-mental-health.html (18th July 2011). National Institute of Health & Clinical Excellence (NICE) 2011). Quality Standards for Service Users Experience in Adult Mental Health: (NICE Quality Standard 14). Manchester: NICE. Onyett, S., Linde, K., Glover, G., Floyd, S., Bradley, S., & Middleton, H. C. (2008). ‘The Implementation of Crisis Resolution Teams in England: Findings of a National Survey 2005 – 06’. Psychiatric Bulletin, 32, 374-377. Parker, S. K. (2000). ‘From passive to proactive motivation: the importance of flexible role orientations and role breadth self-efficacy’. Applied Psychology: An International Review, 49, 447–469. Parry, K. W. (1998). ‘Grounded theory and social process: A new direction in leadership research’. Leadership Quarterly, 9, 1, 85-105. Patterson, M., Warr, P. & West, M. (2004). ‘Organizational climate and company productivity: The role of employee affect and employee level’. Journal of Occupational & Organizational Psychology, 77, 193-216; Pettigrew, T. F., & Tropp, L. R. (2006). ‘A meta-analytic test of intergroup contact theory’. Journal of Personality and Social Psychology, 90, 751-783. Pettigrew, T. F., & Tropp, L. R. (2011). When groups meet: The dynamics of intergroup contact. Philadelphia, PA: Psychology Press. Platt, D. (2007). The status of social care: A review 2007. London: Department of Health. Real World Group (2008). ‘The EngagingTeams360’.Leeds: Real World Group Richter, A. W., West, M. A., Sacramento, C. A., & Hirst, G. (2005). ‘The relationship between intergroup competition and longitudinal change in group effectiveness’. Poster presented at the Annual Meeting of the Academy of Management, Honolulu, HA.

© Leading to Quality 2013 – All rights reserved Page 125
Richter, A. W., West, M. A., van Dick, R. & Dawson, J. F. (2006). ‘Boundary spanners' identification, intergroup contact and effective intergroup relations’. Academy of Management Journal, 49, 1252-1269. Slade, M. (2009). ‘100 ways to support recovery: a guide for mental health professionals’, Rethink Recovery Series, vol. 1. Cited in State of Victoria (2011) Framework for recovery-orientated practice. Melbourne, Victoria: Mental Health, Drugs and Regions Division, Victorian Government Department of Health Salas, E., Rosen, M. A. & King, H. B. (2009).‘Integrating teamwork into the DNA of graduate medical education: Principles for simulation-based training’. Journal of Graduate Medical Education, 1, 243-244. Schaubroeck, J., Lam, S. S. K., & Cha, S. A. (2007). ‘Embracing transformational leadership: Team values and the impact of leader behavior on team performance’. Journal of Applied Psychology, 92, 1020-1030. Schippers, M., West, M. A., & Dawson, J. F. (2011). ‘Team reflexivity and innovation: The moderating role of team context.’ Paper submitted to the Journal of Management. Shepherd, G., Boardman, J., & Slade, M. (2008). Making Recovery a Reality. London: Sainsbury Centre for Mental Health. Simons, T., Pelled, L. H., & Smith, K. A. (1999). ‘Making use of difference: Diversity, debate, and decision comprehensiveness in top management teams’. Academy of Management Journal, 42, 662-673. State of Victoria (2011) Framework for recovery-orientated practice. Melbourne, Victoria: Mental Health, Drugs and Regions Division, Victorian Government Department of Health. Tesluk, P. E., & Mathieu, J. E. (1999). ‘Overcoming roadblocks to effectiveness: incorporating management of performance barriers into models of work team effectiveness’. Journal of Applied Psychology, 84, 200‐217. Timmins, N. (2012). Never Again? The Story of the Health and Social Care Act 2012. London: Institute of Government & The King’s Fund. Van der Kleij, J. F. M. (2011). ‘Engaging leadership in healthcare organisations: The mediating role of work engagement’. Unpublished Mastersthesis, MSc Human Recourse Management University of Groningen, Faculty of Economics and Business. September. Van der Vegt, G. S., & Bunderson, J. S. (2005). ‘Learning and performance in multidisciplinary teams: the importance of collective team identification’. Academy of Management Journal, 48, 532-547. Van Mierlo, H. H., Rutte, C.G., Vermunt, J., Kompier, M.A.J. & Doorewaard, J.A.C.M. (2006). ‘Individual autonomy in work teams: The role of team autonomy, self-efficacy, and social support ‘. European Journal of Work and Organizational Psychology, 15, 3, 281- 299. Van Knippenberg, D., Haslam, S. A., & Platow, M. J. (2007). ‘Unity Through Diversity: Value-in-Diversity Beliefs, Work Group Diversity, and Group Identification’. Group Dynamics: Theory, Research, and Practice, 11, 207-222. Van Knippenberg, D., &Schippers, M. C. (2007). Work group diversity. Annual Review of Psychology, West, M. A. (2000). Reflexivity, revolution, and innovation in work teams. In M. M. Beyerlein, D. A.Johnson, & S. T. Beyerlein (Eds.), Product development teams (pp. 1-29). Stamford, Connecticut: JAI Press.

© Leading to Quality 2013 – All rights reserved Page 126
West, M. A. (2004). Effective teamwork: Practical lessons from organizational research. (2nd edition). Oxford: Blackwell Publishing. West, M., Alimo-Metcalfe, B., Dawson, J., El Ansari, W., Glasby, J., Hardy G, et al. (2012) Effectiveness of Multi-Professional Team Working (MPTW) in Mental Health Care. Final report. NIHR Service Delivery and Organisation programme. West, M. A., Borrill, C. S., Dawson, J. F., Brodbeck, F., Shapiro, D. A. & Haward, R. (2003). ‘Leadership clarity and team innovation in health care’. The Leadership Quarterly, 14, 393-410. West, M. A. & Markiewicz, L. (2004). Building team-based working: A practical guide to organizational transformation. Oxford : Blackwell Publishing Inc. West, M.A., Markiewicz, L. & Dawson, J.F. (2005). Aston team performance inventory: Management Set. London: ASE. Wollard, K.K. & Shuck, B. (2011). ‘Antecedents to employee engagement: A structured review of the literature’. Advances in Developing Human Resources, 13, 4, 1429-446. Worthington, A. & Rooney, R. (2012). The Triangle of Care. Carers Included: A guide to best practice in acute mental health care. The Princess Royal Trust for Carers and The National Mental Health Development Unit. Xenikou, A. &Simosi, M. (2006). ‘Organisational culture & transformational leadership as predictors of business unit performance’. Journal of Management Psychology, 21, 566-579. Yukl, G. (2009). ‘Leading organizational learning: Reflections on theory and research’. Leadership Quarterly, 20, 49-53 Zaccaro, S. J. &Klimoski, R. J. (2002). ‘The nature of organizational leadership: An introduction’. In S. J. Zaccaro & R. J. Klimoski (eds.), The Nature of Organizational Leadership (pp. 3-41). San Francisco, CA: Jossey-Bass.
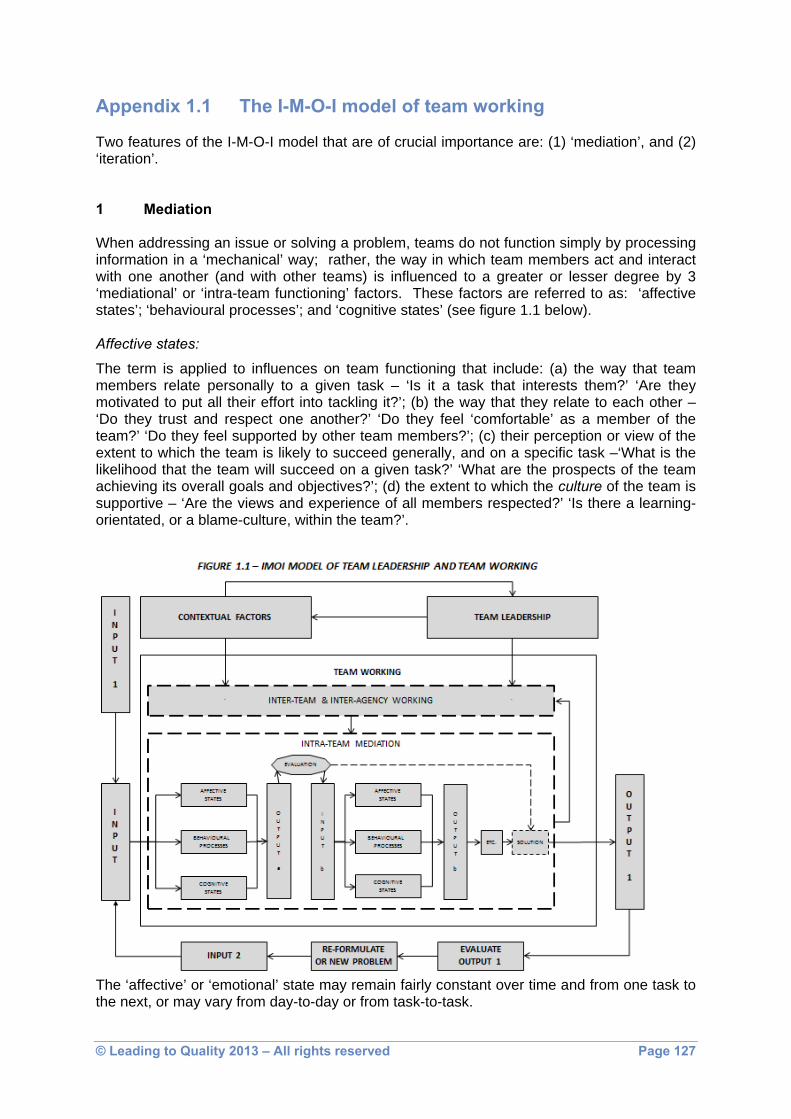
© Leading to Quality 2013 – All rights reserved Page 127
Appendix 1.1 The I-M-O-I model of team working Two features of the I-M-O-I model that are of crucial importance are: (1) ‘mediation’, and (2) ‘iteration’. 1 Mediation When addressing an issue or solving a problem, teams do not function simply by processing information in a ‘mechanical’ way; rather, the way in which team members act and interact with one another (and with other teams) is influenced to a greater or lesser degree by 3 ‘mediational’ or ‘intra-team functioning’ factors. These factors are referred to as: ‘affective states’; ‘behavioural processes’; and ‘cognitive states’ (see figure 1.1 below).
Affective states:
The term is applied to influences on team functioning that include: (a) the way that team members relate personally to a given task – ‘Is it a task that interests them?’ ‘Are they motivated to put all their effort into tackling it?’; (b) the way that they relate to each other – ‘Do they trust and respect one another?’ ‘Do they feel ‘comfortable’ as a member of the team?’ ‘Do they feel supported by other team members?’; (c) their perception or view of the extent to which the team is likely to succeed generally, and on a specific task –‘What is the likelihood that the team will succeed on a given task?’ ‘What are the prospects of the team achieving its overall goals and objectives?’; (d) the extent to which the culture of the team is supportive – ‘Are the views and experience of all members respected?’ ‘Is there a learning-orientated, or a blame-culture, within the team?’.
The ‘affective’ or ‘emotional’ state may remain fairly constant over time and from one task to the next, or may vary from day-to-day or from task-to-task.

© Leading to Quality 2013 – All rights reserved Page 128
The measures of affective states used in the study are:
the extent to which team members feel ‘psychologically safe’ in the contributions they make (psychological safety); in a psychologically safe environment, team members are more likely to come up with the novel way in which a particular problem can best be solved (e.g., Edmondson et al., 2001);
the extent to which team members can call on others for emotional or other support (social support); team members are likely to be willing to put more effort into tasks if they feel that they can call on others’ support, if required (e.g., Alimo-Metcalfe et al., 2007; 2008);
the extent to which they, as a team, feel that they have the capacity to succeed in the tasks that are set (team potency); a strong sense of team efficacy can have the effect of motivating team members to put in extra effort (e.g., Campion, 1996; Little & Madigan, 1997);
being open to minority views, rather than allowing ‘established’ perspectives to dominate (valuing different perspectives): the value of the perceptions of all staff, irrespective of role, grade or status can be of enormous value;
ensuring there is a supportive, learning-orientated culture, rather than a culture of blame (supporting a developmental culture): this can be thought of as the ‘oil in the wheels’ of team working; although the emphasis here is on learning, this affective state can be related readily to the affective state of psychological safety.
Behavioural processes:
These are aspects of team functioning that are normally associated with team working. They include: (a) the gathering of a wide range of relevant information; (b) the allocation of roles and responsibilities, such that each team member has a clear idea of what s/he is expected to do and achieve, and the way in which they should set about tasks, which includes working collaboratively with other team members, and members of other teams and agencies; and, (c) ensuring that all team members are kept up-to-date in all matters that are relevant to them.
The measures of behavioural processes used in the study are:
gathering a wide range of relevant information (information gathering); having clear goals and objectives, coupled with knowing who is responsible for each
task (roles and responsibilities); ensuring that team members are kept up-to-date with current information, and have
opportunities to discuss any problems that arise (updating). Cognitive states:
The behavioural processing referred to above does not take place in a ‘non-thinking’, ‘non-reflective’ way. Rather, each behavioural process is the subject to continuing reflective evaluation, so as to ensure (1) that the task is on-course, and (2) that the objective or goal will be achieved in the most efficient and effective way. To do this, each team member needs: (a) to ensure that they have the necessary knowledge and experience – ‘Am I able to carry out this task successfully?’; if not, (b) to know which member of the team (or non-team member) has the required knowledge and experience – ‘Who do I know that has the information or skills that I need?’ ‘How do I contact them?’; and (c) are capable of dealing with pressure or unforeseen circumstances – ‘Who can help me in an emergency situation?’ ‘Who can help me deal with pressures I am experiencing?’. The team as a whole also
© Leading to Quality 2013 – All rights reserved Page 129
needs to ensure (a) that knowledge and expertise are shared openly and freely; (b) that each member of staff knows exactly who to approach to specific help or guidance; and (c) that the exchange of knowledge and expertise is not prevented or impeded by issues such as differences in professional or other status – ‘Is this a team in which techniques and ideas are shared freely and openly?’ ‘Is this a team that ensure that everyone has access to all the knowledge and skills that they need?’. Two particular features of the cognitive component of the IMOI model are: ‘shared mental models’, which refers to “organizing [the] understanding of relevant knowledge that is shared by team members” (Mohammed & Dumville, 2001, p. 89), the focus being ‘collective knowledge’ regarding what individual team members hold in common; and ‘transactive memory’, that is, “a combination of the knowledge possessed by each individual and a collective awareness of who knows what” (Austin, 2003, p. 866). The measures of cognitive states used in the study are:
having opportunities for all team members to share specialist knowledge and experience, and to reflect on how to apply it (collective experience);
using the team’s resources in a strategic way, so as to deal with pressures and changes imposed from outside (adapting); in this way, the cognitive state elements can be seen to come together, and to inform the behavioural processes.
In practice, this means that the way in which any input to the team (for example, a new issue to address, or a new problem to solve) is treated will be through dynamic interaction between affective, behavioural, and cognitive elements of team working.
2 Iteration Iteration – the cyclical way in which ‘products’ and ideas are continuously analysed, evaluated, and modified, as appropriate – occurs at two levels in the I-M-O-I model.
Interaction with external environment:
Take as an example a decision to employ an additional administrative/clerical assistant so as to increase their capacity of the MH professionals within the team to work with service users and carers by assisting them with their paperwork for 3 full days a week. This proposal (‘INPUT 1’ in Figure 1) might be implemented (‘INPUT’) and its impact on the effectiveness of the team (‘OUTPUT 1’) evaluated after a period of 2 months (‘EVALUATE OUTPUT 1’). On the basis of the evaluation, it may be concluded (1) that the proposal was successful, in which case no further action would be needed, or (2) that, while the proposal had many advantages, it would be better for the support to be available for a full day on Mondays, and half a day from Tuesday to Friday (‘RE-FORMULATE’). ‘INPUT 2’, then, would be trying out, the modified proposal, and subsequently evaluating it. The I-M-O-I model serves to clarify the nature of this iterative process. Interaction within the team:
Take as an example the earlier stage in which a proposal was made to employ an additional administrative/clerical assistant. There is a multitude of ways in which the members of a team could respond to such a proposal. These include: (a) affective: one or more team members think that this would be a good idea, and are motivated to devote time and effort to thinking through the practical implications, and come up with a plan (‘OUTPUT a’). On the basis of discussion with others (‘EVALUATION’), they may spend more time and effort to revise the initial plan (‘INPUT b’), and come up with ‘OUTPUT b’; (b) behavioural:

© Leading to Quality 2013 – All rights reserved Page 130
one or more team members collect relevant information about how the proposal might work out in practice, perhaps allocating certain information gathering tasks to certain individuals. Again, they may evaluate their initial thoughts in the light of any new information that comes to light, and revise the proposal accordingly; (c) cognitive: one or more members of the team share their knowledge and experience of how the proposal might work out in practice, and come to a shared understanding of how to make best use of the additional resource. Following discussion with other team members, they may evaluate the initial proposal, and revise it accordingly. The iterative nature of the I-M-O-I model is consistent with the concept of ‘double-loop learning’ (Agyris, 1993). Iterative or ‘double-loop’ learning is seen as an essential feature of the implementation of innovation in the NHS (DH, 2012).

© Leading to Quality 2013 – All rights reserved Page 131
Appendix 2.1 Instructions on using Repgrid Technique to elicit constructs of effective care
1. On each of the 7 cards, ask the service user (or carer) to write the name or initials of:
2 people (elements) whom you consider to be an effective MH professional – 1 person per card
2 people whom you consider to be an ineffective MH professional – 1 person per card
2 people whom you consider to be in between – 1 person per card
Your ‘ideal’ MH professional
NB1. It is important (1) to explain that you do not want to know who the person is, and (b) to explain that the use of initials is to ensure anonymity. NB2: Rather than using professionals as the elements, you can alternatively use Examples/events of ‘good/outstanding’, ‘poor’, ‘average’ care experienced, and
‘my ideal’ care.
2. Shuffle the cards, choose 3 cards, and place them so that the initials can be read by the individual whose ‘constructs’ are being elicited.
3. Ask the individual to think of some important way in which 2 of them are similar to
one another, but different from the third.
4. Using the grid sheet (see below), or simply making notes, write the nature of the
difference (one ‘pole’ of the construct) in the left hand column, and leave some space below for adding additional constructs that emerge as the result of ‘laddering’, e.g., “is/was considerate of my feelings”. (See below for an explanation of the ‘laddering’ process of obtaining more explicit details of a construct).
It is usually not necessary to write down the opposite.
5. You may wish to write the opposite ‘pole’ in the right hand column, e.g., “is/was not
considerate of my feelings”.
Be careful to ensure that the ‘opposite’ is not actually a different construct, e.g., the construct of “arrogant” is not necessarily the opposite of a person’s construct of “sensitive”.
6. Continue eliciting constructs using this combination of elements until there are no
additional constructs. 7. You can then ask the individual to think about an important way in which 1 of the
elements is different to the other 2 elements, and/or all 3 are similar to each other. 8. Next, return the 3 cards to the stack, shuffle, and choose 3 more cards.

© Leading to Quality 2013 – All rights reserved Page 132
If this combination is either (a) the same as the previous combination, or (b) the individual thinks that it is difficult to think of similarities and differences, then you can take away one of the cards, and substitute it with another.
9. Once you have elicited the range of ‘higher order’ constructs, start the ‘laddering’
process.
Here, it is often useful to ask the individual to say something more about the construct, or to ask for an example. .
Continue the process until you have elicited all the constructs Laddering 1. Laddering is the process of probing into more detail, the behaviours, attitudes,
knowledge, etc in relation to a specific construct
2. For example, the construct elicited may have emerged such as ‘treats me with dignity’. The questions to probe into more detail might be, ‘how do they do/show this?’; ‘what do such people do that is different from someone who doesn’t show dignity to you?’; ‘what might I see if I was watching someone who treats service users with dignity?’
3. If events or ‘experiences’ are being used, then an example might be: “made me feel anxious”. In which case, similar probing questions must be asked to identify explicitly what the person means.
4. This is a crucial aspect of the process of eliciting constructs and understanding the person’s specific construct of ‘treating me with dignity’. It is very important to try to obtain as specific an idea as is possible, otherwise the researcher might impose their interpretation of the construct, or the construct would be too vague, ambiguous, misleading.
AN EXAMPLE OF A PARTIALLY COMPETED REP GRID
Emergent Construct
A B C D E F Its Opposite/Difference (not always necessary)
Treats me with dignity Isn’t interested in how I’m feeling
- doesn’t patronise me - Spends little time listening to me
- actively listens to what I say
– talks most of the time
© Leading to Quality 2013 – All rights reserved Page 133
- involves me in deciding what my treatment will be
- makes sure that I am happy with decisions made
- asks me if I want my partner to be involved
Helps strengthen my self-confidence
Always seems to focus on negatives, such as ……….
- encourages me to speak my mind openly about what I’m feeling
- respects my choices
- focuses on what I have achieved, and not what’s not gone well

© Leading to Quality 2013 – All rights reserved Page 134
Appendix 2.2 Demographic/biographical data of sample for the EngagingTeams360
The following tables outline the biographical and demographic for the Engaging Teams360. *NB: Percentages have been rounded to the nearest percent; as such, the combined total may not be exactly 100%.
Number of Responses by Trust
Number of Responses
Percentage of overall survey
sample Barnsley PCT 67 11 Bradford District Care Trust 27 5 Humber NHS Foundation Trust 114 19 Leeds Partnership NHS Foundation Trust 30 5 NAVIGO 45 8 Rotherham, Doncaster and South Humber NHS Foundation Trust 98 17
North Yorks & York Community Mental Health Services 53 9
South West Yorkshire Partnership NHS Foundation Trust 156 26
Total 590 100
Number of Responses by Team Type
Number of Responses
Percentage of overall survey
sample Access Team 66 11 CMHT 186 32 AOT 99 17 CRT/IHBTT 75 13 Early Intervention Team 48 8 Recovery Team 27 5 Unknown 89 16
Total 590 100

© Leading to Quality 2013 – All rights reserved Page 135
Number of Responses by Size of Team
Number of Responses
Percentage of overall survey
sample 10 or less 38 6 Between 11 and 15 155 26 Between 16 and 20 113 19 Between 21 and 30 111 19 Over 30 71 12 Unknown 102 17
Total 590 100
Number of Responses by Gender of Team Members
Number of Responses
Percentage of overall survey
sample Female 383 65 Male 150 25 Prefer not to say/Unknown 57 10 Total 590 100
Number of Responses by Age of Team Members
Number of Responses
Percentage of overall survey
sample <25 23 4 26-35 79 13 36-45 154 26 46-55 173 29 56-65 73 12 >66 4 1 Prefer not to say/Unknown 84 14 Total 590 100
Number of Responses by Ethnic Background of Team
Members
Number of Responses
Percentage of overall survey
sample White British 503 85 White Other 16 3 Other ethnicity (Black, Asian, Mixed) 12 2
Prefer not to say/Unknown 59 10 Total 590 100
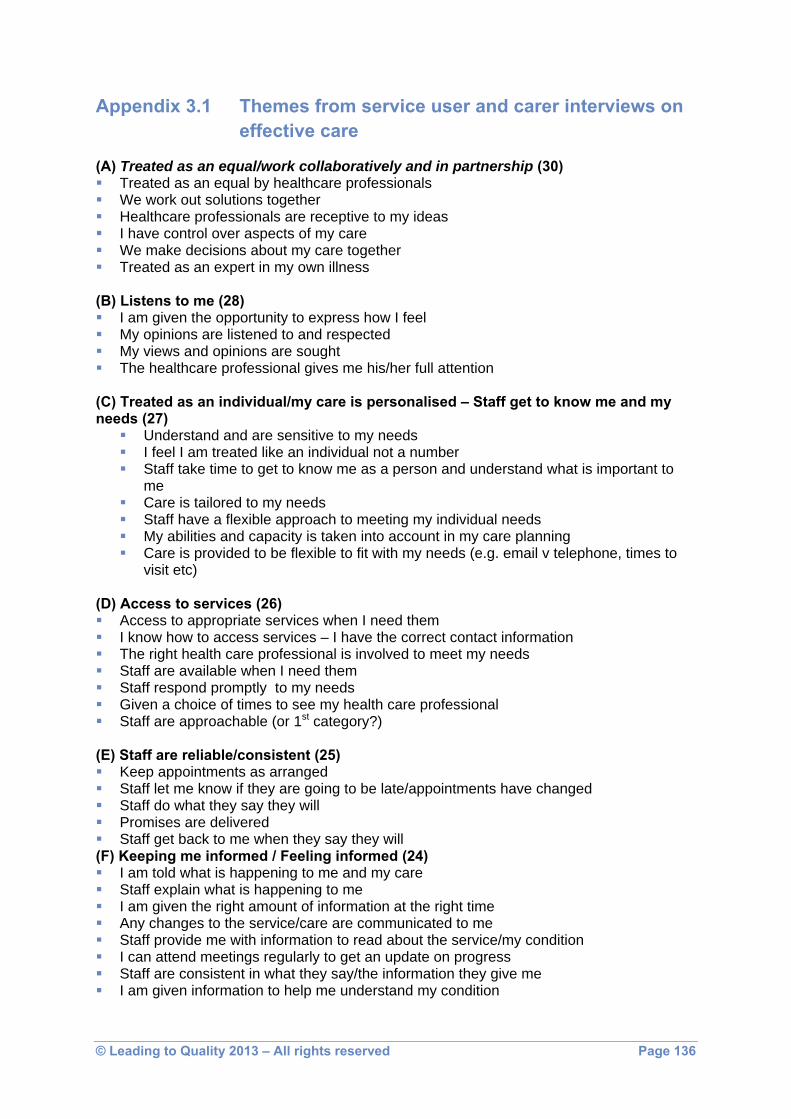
© Leading to Quality 2013 – All rights reserved Page 136
Appendix 3.1 Themes from service user and carer interviews on effective care
(A) Treated as an equal/work collaboratively and in partnership (30) Treated as an equal by healthcare professionals We work out solutions together Healthcare professionals are receptive to my ideas I have control over aspects of my care We make decisions about my care together Treated as an expert in my own illness
(B) Listens to me (28) I am given the opportunity to express how I feel My opinions are listened to and respected My views and opinions are sought The healthcare professional gives me his/her full attention
(C) Treated as an individual/my care is personalised – Staff get to know me and my needs (27)
Understand and are sensitive to my needs I feel I am treated like an individual not a number Staff take time to get to know me as a person and understand what is important to
me Care is tailored to my needs Staff have a flexible approach to meeting my individual needs My abilities and capacity is taken into account in my care planning Care is provided to be flexible to fit with my needs (e.g. email v telephone, times to
visit etc) (D) Access to services (26) Access to appropriate services when I need them I know how to access services – I have the correct contact information The right health care professional is involved to meet my needs Staff are available when I need them Staff respond promptly to my needs Given a choice of times to see my health care professional Staff are approachable (or 1st category?)
(E) Staff are reliable/consistent (25) Keep appointments as arranged Staff let me know if they are going to be late/appointments have changed Staff do what they say they will Promises are delivered Staff get back to me when they say they will
(F) Keeping me informed / Feeling informed (24) I am told what is happening to me and my care Staff explain what is happening to me I am given the right amount of information at the right time Any changes to the service/care are communicated to me Staff provide me with information to read about the service/my condition I can attend meetings regularly to get an update on progress Staff are consistent in what they say/the information they give me I am given information to help me understand my condition

© Leading to Quality 2013 – All rights reserved Page 137
(G) Supports me to achieve my goals/move forward (21) Focus is on working towards goals We set goals together Focus on positives and strengths, on what I can do Helps me to overcome barriers to achieving goals Encourages me to think about the future and what I can achieve Supports/empowers to achieve personal goals Inspires hope in me for the future Good range of support (phone, visits etc) Believes in me Makes me feel I can achieve things/move on Makes me feel I can achieve what I need to Encourages me to believe in myself
(H) Continuity of care/staff (19) Staff remain the same for some time Being seen by people who know me (don’t have to repeat my story) Smooth transition between services Care is uninterrupted, just mover between services
(I) Genuinely cares about me (17) Feel I am treated me in a caring way Spend time with me talking Ask me questions and are genuinely interested in my answers Will help in anyway they can – goes above and beyond Asked how I am feeling/coping and they really want to know Make me feel that I matter Takes time to offer support when I am upset
(J) Choices about my care (16) Offered choices about my care My opinions are sought about my care Have a say in what happens to me Involved in deciding what options would be best for me Options are described to me in a way I understand
(K) Trusting and being trusted (16) Able to open up to staff with confidence it will go no further I trust staff to do what they say they will – feel reassured Staff believe what I say – take my word Staff trust my judgement about what is going to help me I trust staff to tell me the truth/be honest with me I feel I can tell staff anything Promises made by staff are kept
(L) Knowledge and experience (15) Staff are knowledgeable about mental health issues (my condition) Staff help me to understand my condition and treatments Staff are able to answer my questions about my condition Staff share the knowledge they have with me Staff know about other services etc I can access
(M) 1:1 Time with staff (14) Staff give enough time to me Staff give me quality time

© Leading to Quality 2013 – All rights reserved Page 138
There is time to get to know each other Allows me to take as much time as I need
(N) Understands things from my point of view (14) Acknowledges what I have been through Understands my problems Can see things from my point of view Empathic
(O) Holistic care (12) Helps with things other than just symptoms and medication Gives practical support (e.g. with daily living activities) Finds out about other things which may help with care such as services and groups Looks at the wider picture of my health (e.g. diet, exercise etc) Treat me as a whole person (looks at my physical as well as mental wellbeing) Supports me to live healthier lifestyle in general Gives me information on other things that could help me (e.g. groups, courses etc) Focus is on improving all aspects of my life, not just symptoms
(P) Communication between teams/professionals/services (13) Good communication between staff/different professionals Different staff know my history so I don’t have to repeat myself Liaison between services/teams so that all angles have been taken into account when
deciding on treatment Staff work together as a team – good communication between them Staff talk to other professionals to tell them what is happening with me Information about treatment is passed on to out of hours services My GP is updated about my treatment regularly Team work in partnership with other services (e.g. GP) so information is shared Communicate with relevant voluntary/community organisations to support me
(Q) Makes to feel comfortable/at ease (12) I feel comfortable with my healthcare professionals I find it easy to talk to my care worker Makes me feel at ease I feel I can relate to staff Staff are warm and approachable
(R) Communicates with me in a way I understand (11) Communicates clearly - doesn’t use jargon, uses language I understand Explains things to me in a way I can understand Asks me questions to check I understand what is being said Will always have the answer to my questions or will find out Tells me the truth Is open and frank Is honest – I can ask a question and get an honest answer
(S) Being involved in my care planning (11) Involve everyone who is relevant in the care plan Options about the care plan are discussed with me I am fully involved in the care planning process Family involved in care planning I am involved in decisions made about care planning I have some control over my care plan

© Leading to Quality 2013 – All rights reserved Page 139
(T) Respected (10) Takes me and my beliefs seriously Speaks to me in a respectful manner (says ‘please’ and ‘thank you’); is courteous I feel valued as a person
(U) Non-judgemental staff (9) Staff are non-judgemental Staff accept me for who I am Staff are open minded Staff refrain from making assumptions about me based on my diagnosis/age/gender/race
etc (V) Support services (6) Staff help me to access other service in the community I am told about other services/activities that may help me
(W) Involved in decisions about my care (4) Given information so I can make informed decisions about my care Feel actively involved in decisions about my care
(X) Other themes/areas (small number) Facilities poorly managed, depressing environment etc Clear diagnosis Carer – involvement, listen to, opinions count etc (all included in main themes)

© Leading to Quality 2013 – All rights reserved Page 140
NICE Quality Statement Definition of statement LTQ constructs – additional constructs #1: Feeling optimistic about care People using mental health services,
and their families or carers, feel optimistic that care will be effective
There were numerous constructs endorsing this statement, and IN ADDITION, a strong theme reflecting the importance of building a SU’s sense of self-efficacy by: motivating SU to focus on the future; reinforcing belief and confidence in themselves, and their strengths; holds positive expectations of success; emphasising reflection of progress towards their goal achievement; inspiring and encouraging hope, even when things seem hopeless
#2: Empathy, dignity & respect People using mental health services, and their families or carers, feel they are treated with empathy, dignity and respect
Constructs clearly endorse this statement; in addition, genuine care & interest in how SU is feeling, and their personal situation; warm and approachable, welcoming and friendly; treated as an individual rather than ‘a case’; interest shown in all aspects of the person’s life, and not just their illness; listens, understands, and seeks and acknowledges SU’s opinions, ideas, problems and experiences; non-judgemental, open-minded and honest; accepts and values SU as who they are; doesn’t stereotype or make assumptions based on diagnosis, gender, race, age, etc.; trusts individual, and maintains confidentiality; promises are kept;
#3: Shared decision-making & self- management
People using mental health services feel actively involved in making decisions about their care and treatment and supported in managing their mental health problem(s)
Constructs clearly endorse this statement, including: a strong theme of SU working in partnership and collaboration with the professional in identifying choices and solutions, and making decisions, about their appropriate care, having provided them with full information about their condition and treatment; also of supporting SU in achieving their personal goals; being flexible to SU’s needs; and empowering & enabling individual to help themselves
#4: Continuity of care People using community mental health services are normally supported by staff from a single, multidisciplinary community team, familiar to them and with whom they have a continuous relationship
Constructs clearly endorse this statement, including: professionals remain the same, which enables them to get to know you and your circumstances, and you don’t have to repeat ‘your story’ to various unfamiliar people. IN ADDITION, constructs referred to the importance of: (1) good communication and team working between different members of the MH team, such that members of the team standing in when a particular professional was unavailable/on holiday, were well-informed; also “information was passed on to out of hours services”, and to the individual’s GP; (2) the importance of MH team members having good relationships and communication with other teams, agencies/services, so that, for example, “all the angles are taken into account when deciding on treatment”, and between the MH team and relevant 3rd sector/community organisations that could support the SU
Appendix 3.2: Comparison of NICE Quality Standard for Service User Experience in Adult Mental Health and Service Users’ & Carers’ constructs of ‘high quality care’

© Leading to Quality 2013 – All rights reserved Page 141
and their family, including when the SU makes a transition between services.
#5: Using views of service users to monitor and improve services
Mental health and social care professionals ensure service users are provided with opportunities to give feedback on their experience
Although there weren’t explicit constructs relating to seeking feedback so that services could be improved, it was implicit in the several examples of constructs in which the views and opinions of SUs were sought about the care provided, and being listened to and ‘taken on board’
#6: Access to services People can access mental health services quickly & easily when they need them
There were several constructs relating to this aspect of quality, including: knowing how to access services (having the correct contact information); having access to the right professional and being able to contact them easily; being responded to promptly, and being given a choice of times to see the professional. In addition, healthcare professionals knowing what other support services are available in the community, and how to access them
#7: Information and explanations People using mental health services understand the assessment process, their diagnosis and treatment options, and receive emotional support for any sensitive issues
Several constructs endorsed this statement, including: MH professionals providing a clear diagnosis and information to enable the SU to understand their symptoms/condition, and treatment options available, using jargon-free language, checking it’s understood; inviting questions and providing clear answers. Changes to the service/care are explained; appropriate information is provided to all those involved in the SU’s care; 1-to-1 time is provided when needed, and adequate time is given to make decisions; promises are kept
#8: Care planning People using mental health services jointly develop a care plan with mental health and social care professionals, receive a copy of the care plan and agree a date to review
The SU is treated as an expert in their own illness; care is personalised and tailored to the person’s needs and circumstances; individuals are given choices, and a clear care plan - which has been jointly created - is agreed; the SU is able to attend meetings regularly to update on progress; professionals keep appointments, or inform if they have to be changed, and inform SU when they will be away; there is sufficient flexibility to meet an individual’s needs (e.g. email vs telephone, times to visit, and locations, etc.). IN ADDITION, there were many constructs relating to the fact that high quality care is HOLISTIC in nature, that is, it encompasses not only mental health, but all aspects of one’s wellbeing, including physical, and social, and offers practical advice in relation to the individual’s personal circumstance, and their daily living activities, including diet, exercise, financial advice, family situation, educational opportunities, and support group/agency information; and that planning involves all those (e.g. carer and family) who are relevant to the care
#9: Crisis planning Service users who may be at risk of

© Leading to Quality 2013 – All rights reserved Page 142
crisis are offered a crisis plan. #10: Assessment in a crisis Service users accessing crisis
support have a comprehensive assessment undertaken by a professional competent in crisis working
Constructs were wider than this definition, in relation to professionals’ competence, irrespective of whether the situation is one of crisis.
ADDITIONAL DIMENSION OF QUALITY EMERGING FROM THE CONSTRUCTS – Quality of Professionals involved in care
Constructs included: the appropriate professionals are involved, who are knowledgeable in MH issues, and the individual’s condition, and share their knowledge with them; they are experienced, and know about other relevant services that the individual can access
NB: Statements #11 - #15 are not relevant for this study related to people who were in hospital for mental healthcare, whereas the service users participating in our research, were all being supported by MH teams in the community

© Leading to Quality 2013 – All rights reserved Page 143
Appendix 4.1 The reliability of the EngagingTeams360
Internal reliability, means and standard deviations for the EngagingTeams360 scales
α-
coefficients Ns Means Standard
deviations Psychological Safety .88 590 4.76 0.98 Social Support .88 590 5.04 0.86 Team Potency .87 590 4.99 0.81 Valuing Different Perspectives .89 590 4.71 1.00
Supporting a Developmental Culture .89 590 4.71 0.94
Information Gathering .75 590 4.87 0.79 Roles and Responsibilities .84 590 4.58 1.00 Updating .85 590 4.99 0.90 Collective Experience .91 590 5.01 0.75 Adaptability .88 590 4.99 0.81
Inter-team & Inter-agency Relations .89 590 4.72 0.76
Inter-team & Inter-agency Collaboration .73 590 4.74 0.84
Engaging with Others .96 589 4.76 1.09 Building a Shared Vision .90 585 4.71 1.02 Enabling the Team .94 588 4.77 1.05 Leadership Capabilities .93 587 4.71 1.04 Innovation .82 590 4.91 0.84 Focus on Quality .83 590 4.61 0.96 Improvement .86 590 4.55 0.82 Team Engagement .85 577 5.30 0.76 Wellbeing at Work .84 562 4.25 1.13

© Leading to Quality 2013 – All rights reserved Page 144
Appendix 4.2 Results of the EngagingTeams360 in rank order
Mean scores on the EngagingTeams360 scales, in order of size
Scale Dimension Mean score Team Engagement Impact on Team Members 5.30 Social Support Trusting and Bonding 5.04 Collective Experience Structuring and Learning 5.01 Updating Planning 4.99 Adaptability Structuring and Learning 4.99 Team Potency Trusting and Bonding 4.99 Innovation Team Process Outcome 4.91 Information Gathering Planning 4.87 Enabling the Team Team Leadership 4.78 Psychological Safety Trusting and Bonding 4.76 Engaging with Others Team Process Outcome 4.76 Inter-team& Inter-agency Collaboration Inter-team & Inter-agency Working 4.74 Inter-team & Inter-agency Relations Inter-team & Inter-agency Working 4.72 Leadership Capabilities Team Process Outcome 4.71 Valuing Different Perspectives Trusting and Bonding 4.71 Supporting a Development Culture Trusting and Bonding 4.71 Building Shared Vision Team Process Outcome 4.71 Focus on Quality Team Process Outcome 4.61 Roles and Responsibilities Planning 4.58 Improvement Team Process Outcome 4.55 Wellbeing at Work Impact on Team Members 4.25

© Leading to Quality 2013 – All rights reserved Page 145
Appendix 4.3 Structural Equation Modelling In order to examine the relationship between the independent variables (Team Leadership scales, and Team Working scales) and the dependent variables (Team Process Outcomes scales, and Impact on Team Members scales), and to test the validity of the EngagingTeams360, Structural Equation Modelling technique was used (Henseler, Ringle&Sinkovics, 2009).7 The hypothesised relationship between the independent and dependent variables, based on evidence from Alimo-Metcalfe et al. (2007) and West et al. (2012) and others, is presented below in Appendix Figure 4.1.
It was hypothesised that:
Ho 1 the team leadership scales would each contribute to a second-order factor, ‘Team Leadership’;
7Henseler, J. Ringle, C.M. &Sinkovics, R.R. (2009) The use of partial least squares path modeling in international marketing. Advances in International Marketing, 8: 20, pp.277‐319.

© Leading to Quality 2013 – All rights reserved Page 146
Ho 2 the team leadership scales would each contribute to one of four second-order factors: ‘Trusting and Bonding’, ‘Planning’, ‘Structuring and Learning’, and ‘Inter-team and Inter-agency Working’;
Ho 3 the first-order team working factors would contribute to a third-order factor, ‘Team Working’;
Ho 4 the first-order Team Leadership factor would also contribute to a third-order ‘Team Working’ factor;
Ho 5 team members scales would each contribute to a second-order factor, ‘Impact on Team Members’;
Ho 6 the team process outcome scales would each contribute to a second-order factor, ‘Team Process Outcomes’;
Ho 7 Team Leadership would have a direct impact on Team Working; Ho 8 the second-order factors ‘Impact on Team Members’ and ‘Team Process Outcomes’
would be independent of each other; Ho 9 Team Working would have a direct impact on Team Members (Team Engagement,
and Wellbeing at Work); Ho10 Team Working would have a direct in impact both on Team Process Outcomes
(Innovation, Focus on Quality, and Improvement), and Team Members. Of four models that were tested, the model presented in Figure 4.2 (below) reached the required level of statistical significance (p ≤0.05).

© Leading to Quality 2013 – All rights reserved Page 147
As this figure indicates, there is significant evidence for the following conclusions to be drawn: There was support for Ho 1 – Ho 6, and for Ho 9 and Ho 10. In the cases of Ho 1 – Ho 6, the relationship was ‘reflective’. This means that (1) each of the scales contributes significantly to the relevant first-order factor, and (2) it is possible to discriminate between the contribution that each makes. There was no support for Ho 8, in other words, it was not possible to differentiate between the two sets of dependent variables, Impact on Team Members and Team Process Outcomes. This is not, perhaps, a surprising finding in that, while there are good reasons (specifically, that they are different constructs) for suggesting that they are both separable, there are also good reasons why they should be closely related (e.g., Patterson et al., 2004; Xenikou & Simosi, 2006). That there should be no support for Ho 7 is an important finding. As noted in Chapter 1, our previous understanding was (a) that certain forms of team leadership had a predictive relationship with the measures of impact on team members that were assessed here, and (b) that the relationship between team leadership was only correlational, as was the relationship between team working and its impact on team members and team process outcomes. What is important, then, is the evidence (1) that Team Leadership has a significant formative relationship with Team Working, and (2) that Team Working has a formative relationship with the impact measures (Team Process Outcomes, and Impact on Team Members).8 Put simply, this means (a) that team leadership acts through team working, rather than directly, and (b) that team leadership contributes to the impact of team working. As noted in Chapter 6, both of these findings have important implications for the development of leadership and of team working. In terms of interpreting the results in relation to the Leading to Quality project as a whole, the evidence suggests that:
the Psychological Safety, Social Support, Team Potency, Valuing Different Perspectives, Supporting a Developmental Culture scales all contribute significantly to the first-order affective states domain ‘Trusting and Bonding’ (reflective relationships), though each measures a different aspect of this domain (discriminant validity). This last point is important, since it means that the particular scales referred to (Psychological Safety, etc.) each impact uniquely on Trusting and Bonding.
the Information Gathering, Roles and Responsibilities, and Updating scales all contribute significantly to the first-order behavioural processes domain ‘Planning’ (reflective relationships), though each measures a different aspect of this domain (discriminant validity);
8 A ‘formative’ relationship is one in which one variable brings about some kind of change in another variable.

© Leading to Quality 2013 – All rights reserved Page 148
Collective Experience, and Adaptability, both contribute significantly to the first-order cognitive states dimension ‘Structuring and Learning’ (reflective relationships), though each measures a different aspect of this domain (discriminant validity);
the Inter-team and Inter-agency Relations and Inter-team and Inter-agency Collaboration scales both contribute significantly to the first-order domain ‘Inter-team and Inter-agency Working’ (reflective relationships), though each measures a different aspect of this domain (discriminant validity);
each of these first-order domains (Trusting and Bonding, Planning, Structuring and Learning, and Inter-team and Inter-agency Working) contribute significantly to a second-order dimension, ‘Team Working’ (reflective relationships);
the Engaging with Others, Building a Shared Vision, Enabling the Team, and Leadership Capabilities scales all contribute to the first order dimension ‘Team Leadership’ (reflective relationships), though each measures a different aspect of this domain (discriminant validity);
the Team Process Outcome scales (Innovation, Focus on Quality, and Improvement) and the Impact on Team Members scales (Engaging the Team, and Wellbeing at Work) all contribute significantly to a first-order impact measure ‘Team Output’ (reflective relationships), though each measures a different aspect of this outcome (discriminant validity);
in combination the first-dimension, ‘Team Leadership’, and the second-order dimension, ‘Team Working’, have a significant impact on ‘Team Output’ (formative relationship);
‘Team Leadership’ does not impact directly on ‘Team Output’, but rather Team Leadership has a mediating effect on the relationship between Team Working and Team Output;
the EngagingTeams360 model is a valid way of understanding the interrelations between Team Leadership, Team Working, and Team Outcomes.
Taken together, this evidence provides information about the ways in which the scales of the EngagingTeams360 tool interact with one another, and further empirical support for its validity.

© Leading to Quality 2013 – All rights reserved Page 149
Appendix 4.4 & 4.5 Correlations
Appendix 4.4: Product-moment correlations (r) between Team Leadership and Team Working scales And Innovation, Focus on Quality, Improvement, Engaging the Team, and
Wellbeing at Work (p < .001, in each case)
Team leadership/ team working scales
Innovation Focus on quality
Improvement Team engagement
Wellbeing at work
Engaging with Others .62 .61 .73 .52 .55
Building Shared Vision .63 .67 .75 .49 .51
Engaging the Team .66 .63 .75 .52 .54
Leadership Capabilities .66 .66 .76 .50 .53
Psychological Safety .75 .67 .80 .63 .61
Social Support .76 .64 .76 .70 .61
Team Potency .78 .71 .82 .70 .62 Valuing Different Perspectives .78 .71 .81 .60 .53
Supporting a Development Culture .78 .77 .86 .62 .63
Information Gathering .70 .77 .84 .57 .63
Roles and Responsibilities .78 .73 .81 .81 .60
Updating .70 .67 .78 .56 .53
Collective Experience .82 .77 .85 .68 .61
Adaptability .79 .68 .80 .66 .59
Inter-team Relations .81 .82 .86 .58 .55
Inter-team Collaboration .72 .79 .79 .49 .50
The Trusting and Bonding scales (Psychological Safety, Social Support, and Team Potency) were significantly correlated with each of the Team Process Outcome scales (Innovation, Focus on Quality, and Improvement) and each of the Impact on Team Member scales (Team Engagement, and Wellbeing at Work) (range r = 0.62 – 0.82). The corresponding correlations for the other team working dimensions were: Planning (Information Gathering, Roles and Responsibilities, and Updating) range r = 0.53 – 0.84; Structuring and Learning (Collective Experience, Valuing Different Perspectives, Supporting a Development Culture, and Adaptability) range r = 0.53 – 0.86; and Inter-team and Inter-agency Working (Relations and Collaboration) range r = 0.49 – 0.86 (p< 0.001 in each case). In order to test for the possibility of common methods bias (CMB), which is the possibility that the ‘variance … is attributable to the measurement method rather than to the constructs

© Leading to Quality 2013 – All rights reserved Page 150
the measures represent’ (Podsakoff, Mackenzie, Lee & Podsakoff, 2003, p. 8799), the correlation matrix was examined for any highly correlated variables (i.e., r> 0.90) (Bagozzi, Yi & Philips, 1991)10. There was no evidence that CMB had a significant impact on the results. These correlations, which are of the same order of magnitude as corresponding correlations reported by West et al. (2012), provide evidence of a significant impact of both team leadership and team working on both team process outcomes and impact on team members’ engagement with the team and their wellbeing at work.
Appendix 4.5: Product-moment correlations (r) between Team Working and Team Leadership scales
(p < .001, in each case)
Team working / Team leadership scales
Engaging with Others
Building Shared Vision
Enabling the Team
Leadership Competencies
Psychological safety .73 .69 .73 .72 Social support .64 .60 .62 .62 Team potency .65 .66 .66 .67
Valuing different perspectives .73 .67 .72 .70
Supporting a development culture .79 .76 .80 .77
Information gathering .61 .65 .64 .67 Roles and responsibilities .68 .72 .61 .74
Updating .72 .70 .74 .69
Collective experience .66 .67 .67 .68 Adaptability .64 .62 .63 .65 Inter-team relations .65 .67 .66 .68 Inter-team collaboration .61 .66 .63 .65
The coefficients ranged from r = 0.61 (Engaging with Others and Inter-team Collaboration) to r = 0.79 (Engaging with Others and Supporting a Development Culture) (p< .001 in each case). These correlations, which are again of the same order of magnitude as corresponding correlations reported by West et al. (2012), suggest that each of the aspects of team leadership and of team working is closely related to each other.
9 Podsakoff, P. M., MacKenzie, S.B., Lee, J-Y. & Podsakoff, N.P. (2003). ‘Common method biases in behavioral research: A critical review of the literature and recommended remedies’. Journal of Applied Psychology, 88, 879-903. 10 Bagozzi, R.P., Yi, Y. & Phillips, L.W. (1991) ‘Assessing Construct Validity in Organizational Research’. Administrative Science Quarterly, 36, 421-458.

© Leading to Quality 2013 – All rights reserved Page 151
Appendix 4.6 Discriminant Function Analysis by item
Appendix Table 4.6– Significant ‘predictive’ relationships between Team Working and Team Leadership items, and Team Process Outcome and Impact on Team Members scales, using
Discriminant Functional Analysis (Wilks’ lambda, p < .05 for entry, p < .10 for removal)
Independent variables (individual items) /dependent variables Innovation Focus on
Quality Improvement Team Engagement
Wellbeing at Work
Trusting and Bonding – Social Support Show great loyalty to the team - - - .66 - Work collaboratively & cohesively as a team - - - .59 -
Trusting and Bonding – Team Potency Are confident as a team in our ability to work effectively together - - - .66 -
Are confident in our ability as a team to achieve our goals - - - .60 -
Trusting and Bonding – Valuing Different Perspectives
Are open to ideas from all team members - - - .62 -
Value the particular knowledge and experience that each team member can offer
- - - .63 -
Ensure that team decisions are not unduly influenced by more 'vocal' or more 'high status' team members
- - - .62 -
Trusting and Bonding – Supporting a Development Culture
Share problems and mistakes openly, in the knowledge that we will be supported - - .37 - -
Give and receive developmental feedback face-to-face, at the appropriate time
- - .38 - -
Have a supportive developmental culture within the team - - .37 - -
Are tolerant of the failings of other team members, when they have tried to do their best
- - .37 - -
Planning – Roles and Responsibilities Are clear about the team's goals and sense of direction - .50 .40 - .69
Have a manageable number of well-defined goals - .44 .41 - .77
Have clearly defined processes and procedures - .43 .39 - -
Have a clear understanding of each other's roles and responsibilities - .43 .41 - -
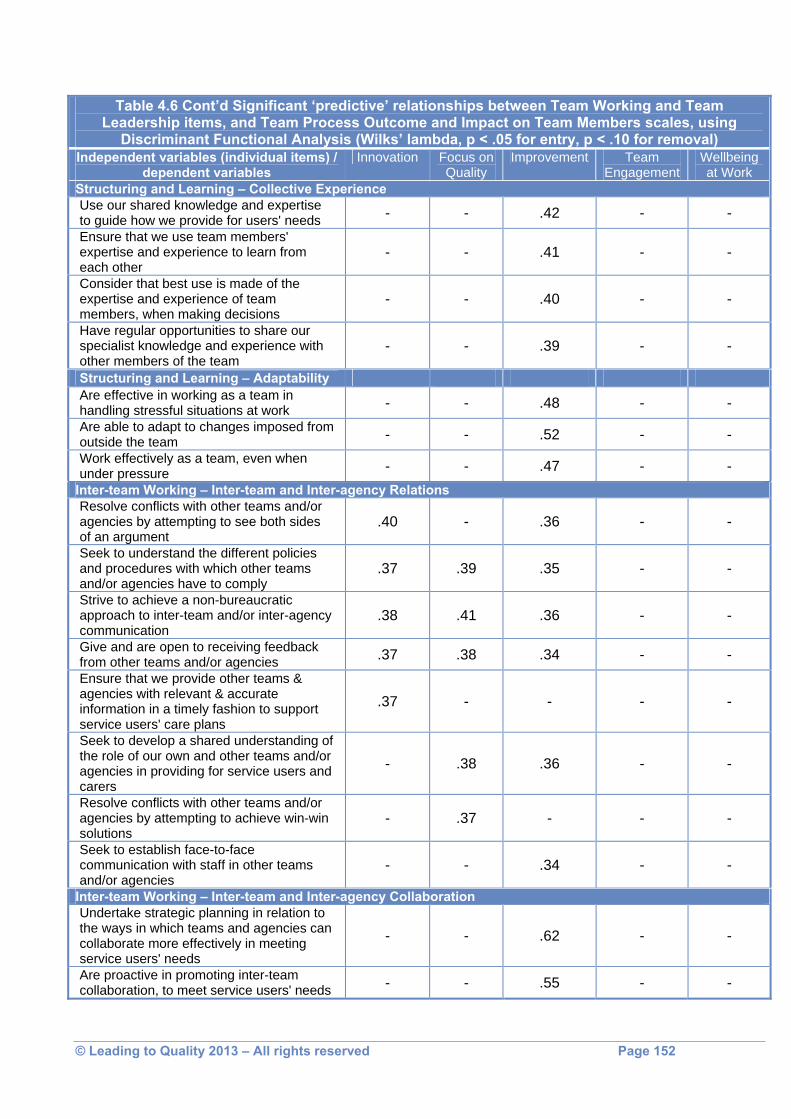
© Leading to Quality 2013 – All rights reserved Page 152
Table 4.6 Cont’d Significant ‘predictive’ relationships between Team Working and Team Leadership items, and Team Process Outcome and Impact on Team Members scales, using
Discriminant Functional Analysis (Wilks’ lambda, p < .05 for entry, p < .10 for removal) Independent variables (individual items) /
dependent variables Innovation Focus on
Quality Improvement Team
Engagement Wellbeing at Work
Structuring and Learning – Collective Experience Use our shared knowledge and expertise to guide how we provide for users' needs - - .42 - - Ensure that we use team members' expertise and experience to learn from each other
- - .41 - -
Consider that best use is made of the expertise and experience of team members, when making decisions
- - .40 - -
Have regular opportunities to share our specialist knowledge and experience with other members of the team
- - .39 - -
Structuring and Learning – Adaptability Are effective in working as a team in handling stressful situations at work - - .48 - - Are able to adapt to changes imposed from outside the team - - .52 - - Work effectively as a team, even when under pressure - - .47 - -
Inter-team Working – Inter-team and Inter-agency Relations Resolve conflicts with other teams and/or agencies by attempting to see both sides of an argument
.40 - .36 - -
Seek to understand the different policies and procedures with which other teams and/or agencies have to comply
.37 .39 .35 - -
Strive to achieve a non-bureaucratic approach to inter-team and/or inter-agency communication
.38 .41 .36 - -
Give and are open to receiving feedback from other teams and/or agencies .37 .38 .34 - - Ensure that we provide other teams & agencies with relevant & accurate information in a timely fashion to support service users' care plans
.37 - - - -
Seek to develop a shared understanding of the role of our own and other teams and/or agencies in providing for service users and carers
- .38 .36 - -
Resolve conflicts with other teams and/or agencies by attempting to achieve win-win solutions
- .37 - - -
Seek to establish face-to-face communication with staff in other teams and/or agencies
- - .34 - -
Inter-team Working – Inter-team and Inter-agency Collaboration Undertake strategic planning in relation to the ways in which teams and agencies can collaborate more effectively in meeting service users' needs
- - .62 - -
Are proactive in promoting inter-team collaboration, to meet service users' needs - - .55 - -

© Leading to Quality 2013 – All rights reserved Page 153
Appendix 4.7 Effect of team size
Means and standard deviations for the domains of EngagingTeams360 for teams by size of team
Domain and size of team Ns Means Standard deviations
Team Leadership 10 or fewer members 38 5.33 .64 11-15 members 153 5.09 .65 16-20 members 113 5.04 1.02 21-30 members 118 4.68 .98 More than 30 members 71 3.82 1.02
Trusting & Bonding
10 or fewer members 38 5.26 .62 11-15 members 155 5.10 .56 16-20 members 113 5.07 .84 21-30 members 111 4.63 .99 More than 30 members 71 4.22 .80
Planning 10 or fewer members 38 5.27 .57 11-15 members 155 5.10 .56 16-20 members 113 5.03 .77 21-30 members 111 4.66 .92 More than 30 members 71 4.29 .80
Structuring & Learning 10 or fewer members 38 5.35 .53 11-15 members 155 5.18 .52 16-20 members 113 5.12 .66 21-30 members 111 4.84 .93 More than 30 members 71 4.61 .71
Inter-team Working 10 or fewer members 38 5.13 .56 11-15 members 155 4.93 .55 16-20 members 113 4.92 .71 21-30 members 111 4.52 .88 More than 30 members 71 4.30 .76

© Leading to Quality 2013 – All rights reserved Page 154
Means and standard deviations for the domains of EngagingTeams360 for teams by size of team (continued)
Domain and size of team Ns Means Standard deviations
Innovation 10 or fewer members 38 5.20 .66 11-15 members 155 5.08 .64 16-20 members 113 5.15 .78 21-30 members 111 4.73 1.00 More than 30 members 71 4.40 .93 Focus on Quality 10 or fewer members 38 4.94 .78 11-15 members 155 4.83 .77 16-20 members 113 4.80 .94 21-30 members 111 4.40 1.07 More than 30 members 71 4.25 1.03 Improvement
10 or fewer members 38 4.89 .65 11-15 members 155 4.80 .59 16-20 members 113 4.77 .78 21-30 members 111 4.35 .94 More than 30 members 71 4.05 .84
Team Engagement 10 or fewer members 36 4.82 1.04 11-15 members 154 4.48 .98 16-20 members 112 4.34 1.18 21-30 members 105 4.07 1.17 More than 30 members 68 3.80 1.14
Wellbeing at Work 10 or fewer members 38 5.61 .58 11-15 members 147 5.42 .62 16-20 members 109 5.38 .88 21-30 members 107 5.19 .81 More than 30 members 66 5.07 .74

© Leading to Quality 2013 – All rights reserved Page 155
Summary of significant differences between ratings on EngagingTeams360 domains
(< denotes that ratings by size of team in first column are significantly lower than on other sizes of team; = denotes that ratings are not significantly
different, using Tukey’s test) Team Leadership 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = < < 16-20 < < 21-30 < Trusting & Binding 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = < < 16-20 = < < 21-30 = < Planning 11-15 16-20 21-30 More than 30 10 or fewer = = < < 11-15 = < < 16-20 = < < 21-30 = < Structuring & Learning 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = < < 16-20 = < < Inter-team Working 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = < < 16-20 = < <
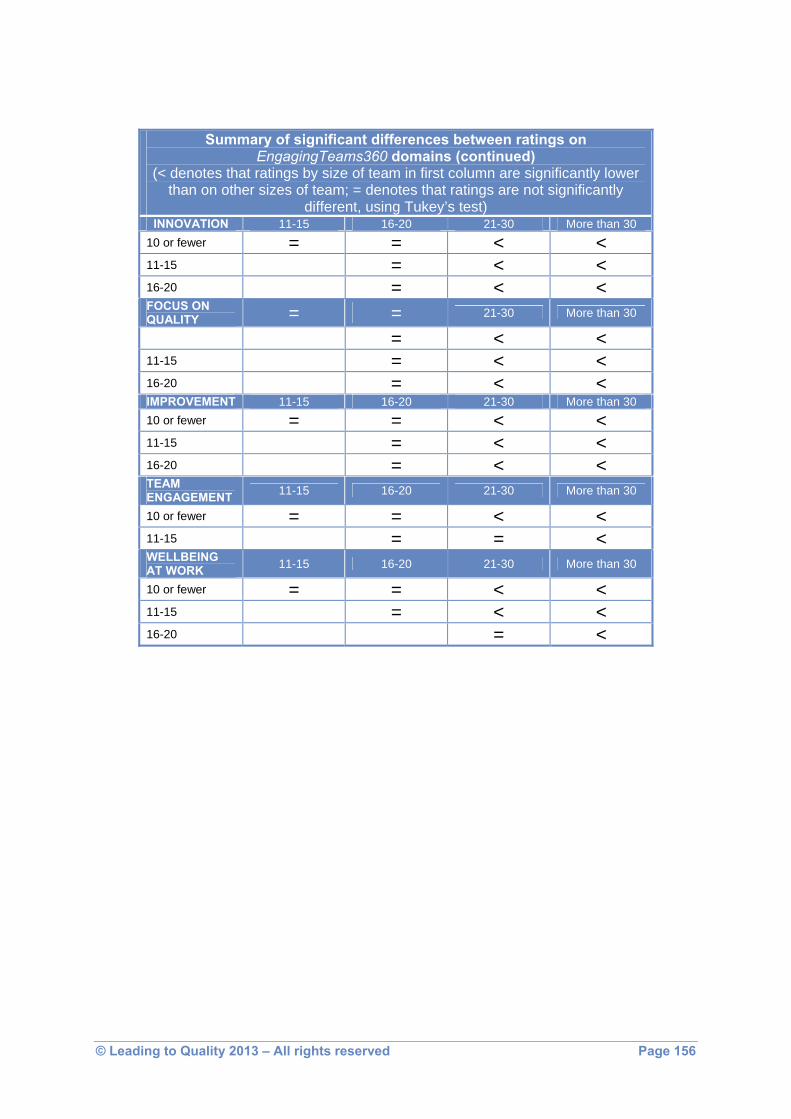
© Leading to Quality 2013 – All rights reserved Page 156
Summary of significant differences between ratings on EngagingTeams360 domains (continued)
(< denotes that ratings by size of team in first column are significantly lower than on other sizes of team; = denotes that ratings are not significantly
different, using Tukey’s test) INNOVATION 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = < < 16-20 = < < FOCUS ON QUALITY = = 21-30 More than 30
11-15 16-20 = < < 11-15 = < < 16-20 = < < IMPROVEMENT 11-15 16-20 21-30 More than 30 10 or fewer = = < < 11-15 = < < 16-20 = < < TEAM ENGAGEMENT 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = = < WELLBEING AT WORK 11-15 16-20 21-30 More than 30
10 or fewer = = < < 11-15 = < < 16-20 = <

© Leading to Quality 2013 – All rights reserved Page 157
Appendix 4.8 Effect of ratio of occupational therapists and social workers to nurses
Means and standard deviations for the domains of EngagingTeams360 for Teams divided by Ratio of Occupational Therapists and Social Workers to Nurses
Domain and ratio Ns Means Standard deviations
Team Leadership Fewer than 25% 85 4.70 1.14 25-35% 181 4.75 .98 36-50% 89 5.28 .68 More than 50% 94 4.97 1.00 Trusting & Bonding
Fewer than 25% 85 4.75 .90 25-35% 181 4.81 .88 36-50% 89 5.23 .58 More than 50% 94 5.05 .72 Planning
Fewer than 25% 85 4.82 .79 25-35% 181 4.85 .81 36-50% 89 5.20 .57 More than 50% 94 5.15 .76 Structuring & Learning
Fewer than 25% 85 5.02 .72 25-35% 181 4.96 .81 36-50% 89 5.31 .53 More than 50% 94 5.15 .59 Inter-team Working
Fewer than 25% 85 4.77 .73 25-35% 181 4.67 .77 36-50% 89 5.01 .65 More than 50% 94 4.86 .71
Innovation Fewer than 25% 85 4.87 .89 25-35% 181 4.85 .70 36-50% 89 5.22 .69 More than 50% 94 4.98 .82
Focus on Quality Fewer than 25% 85 4.58 1.03 25-35% 181 4.60 .94 36-50% 89 4.87 .88 More than 50% 94 4.74 .94
Improvement Fewer than 25% 85 4.52 .87 25-35% 181 4.51 .85 36-50% 89 4.86 .69 More than 50% 94 4.71 .68
Team Engagement Fewer than 25% 85 4..28 1.08 25-35% 181 4.25 1.13 36-50% 89 4.66 .99 More than 50% 94 4.23 1.21

© Leading to Quality 2013 – All rights reserved Page 158
Domain and ratio Ns Means Standard deviations
Wellbeing at Work Fewer than 25% 85 5.34 .84 25-35% 181 5.31 .72 36-50% 89 5.60 .55 More than 50% 94 5.32 .84
Summary of significant differences between ratings on EngagingTeams360 domains
(< denotes that ratings by ratio of OTs and social workers to nurses in first column are significantly lower than other ratios, using Tukey’s
test) Team Leadership 25-35% 36-50% More than 50%
Fewer than 25% < 25-35% < Trusting & Bonding 25-35% 36-50% More than 50%
Fewer than 25% < 25-35% < Planning 25-35% 36-50% More than 50% Fewer than 25% < 25-35% < Structuring & Learning 25-35% 36-50% More than 50%
Fewer than 25% < 25-35% < Inter-team Working 25-35% 36-50% More than 50%
25-35% < Innovation 25-35% 36-50% More than 50% Fewer than 25% < 25-35% < Improvement 25-35% 36-50% More than 50% Fewer than 25% < 25-35% < Team Engagement 25-35% 36-50% More than 50%
25-35% < Wellbeing at Work 25-35% 36-50% More than 50%
Fewer than 25% < 25-35% <

© Leading to Quality 2013 – All rights reserved Page 159
Appendix 4.9 Effect of case load size
Means and standard deviations for the domains of EngagingTeams360 for teams by case load size
Domain and type of team Ns Means Standard deviations
Team Leadership Fewer than 10 27 5.10 .72 10-19 119 5.15 .83 20-29 165 4.74 .92 30 or more 33 4.98 .65 Trusting & Bonding
Fewer than 10 27 4.98 .80 10-19 120 5.20 .73 20-29 167 4.69 .90 30 or more 34 5.02 .46 Planning
Fewer than 10 27 4.98 .80 10-19 120 5.20 .73 20-29 167 4.69 .90 30 or more 34 5.02 .46 Structuring & Learning
Fewer than 10 27 5.32 .51 10-19 120 5.24 .70 20-29 167 4.88 .82 30 or more 34 5.12 .55 Inter-team Working
Fewer than 10 27 4.99 .59 10-19 120 4.99 .71 20-29 166 4.61 .81 30 or more 34 4.77 .48 Innovation
Fewer than 10 27 5.19 .60 10-19 120 5.19 .83 20-29 167 4.72 .96 30 or more 34 4.94 .59 Focus on Quality Fewer than 10 27 5.02 .73 10-19 120 4.93 .84 20-29 167 4.47 1.01 30 or more 34 4.48 .77 Improvement Fewer than 10 27 4.86 .65 10-19 120 4.85 .78 20-29 167 4.45 .85 30 or more 34 4.55 .72 Team Engagement
Fewer than 10 27 5.67 .40 10-19 119 5.53 .71 20-29 159 5.16 .83 30 or more 31 5.53 .44 Wellbeing at Work
Fewer than 10 27 4.61 .92 10-19 112 4.65 1.05 20-29 159 4.10 1.16 30 or more 32 4.45 1.05

© Leading to Quality 2013 – All rights reserved Page 160
Summary of significant differences between ratings on EngagingTeams360 domains
(> denotes that ratings by case load in first column are significantly higher than on other case load size using Tukey’s test)
Team Leadership 10-19 20-29 30 and above
10-19 > Trusting & Bonding 10-19 20-29 30 and above
10-19 > Planning 10-19 20-29 30 and above
10-19 > Structuring & Learning 10-19 20-29 30 and above
10-19 > Inter-Team Working 10-19 20-29 30 and above
10-19 > Innovation 10-19 20-29 30 and above
10-19 > Focus on Quality 10-19 20-29 30 and above
Fewer than 10 > 10-19 > 20-29 > Improvement 10-19 20-29 30 and above
10-19 > Team Engagement 10-19 20-29 30 and above
Fewer than 10 > 10-19 > 20-29 > Wellbeing at Work 10-19 20-29 30 and above
10-19 >

Service User Questionnaire
Please complete this questionnaire to the best of your ability. Do not worry if you cannot complete it all. Section 1: Who provides your care?
Name of Team: Please provide the full name of the team (e.g. Community Mental Health Team East Leeds, Assertive Outreach York). If you are unsure of the name of the team, please ask a member of staff.
Section 2: The service I receive...
Stro
ngly
Dis
agre
e
Dis
agre
e
Slig
htly
Dis
agre
e
Slig
htly
Agr
ee
Agr
ee
Stro
ngly
Agr
ee
Don
’t K
now
/Not
R
elev
ant
1 Enables me to work in partnership with healthcare professionals
1
2
3
4
5
6
7
2 Gives me the opportunity to express my views and be listened to
1
2
3
4
5
6
7
3 Treats me as a whole person with a focus on improving all aspects of my life
1
2
3
4
5
6
7
4 Does not make assumptions about me
1
2
3
4
5
6
7
5 Treats me as an individual
1
2
3
4
5
6
7
6 Takes the time to get to know me
1
2
3
4
5
6
7
7 Lets me know how to access help and support
1
2
3
4
5
6
7
8 Gives me correct contact information
1
2
3
4
5
6
7
9 Responds promptly to my needs
1
2
3
4
5
6
7
10 Is provided by healthcare staff who are reliable
1
2
3
4
5
6
7
11 Is provided by healthcare staff who give me full information about my condition and treatment
1
2
3
4
5
6
7
12 Works on goals that are meaningful to me
1
2
3
4
5
6
7
13 Gives me the self belief that I can achieve what I want for myself
1
2
3
4
5
6
7
14 Helps me to overcome barriers to achieving what I want for myself
1
2
3
4
5
6
7
15 Gives me continuous support when I move from one service to another
1
2
3
4
5
6
7 Please turn over Page 1 of 2

Service User Questionnaire
Section 2 cont’d: The service I receive...
Stro
ngly
Dis
agre
e
Dis
agre
e
Slig
htly
Dis
agre
e
Slig
htly
Agr
ee
Agr
ee
Stro
ngly
Agr
ee
Don
’t K
now
/Not
R
elev
ant
16 Is provided by people that I have got to know
1
2
3
4
5
6
7
17 Makes me feel that I am genuinely cared for
1
2
3
4
5
6
7
18 Involves me in making choices about my care
1
2
3
4
5
6
7
19 Is based on an open and trusting relationship with staff
1
2
3
4
5
6
7
20 Helps me to understand my condition and the treatment options available
1
2
3
4
5
6
7
21 Allows me to take as much time as I need during visits
1
2
3
4
5
6
7
22 Makes me feel understood
1
2
3
4
5
6
7
23 Makes sure that accurate information is accessible at all times
1
2
3
4
5
6
7
24 Is provided by staff who put me at ease and make me feel comfortable
1
2
3
4
5
6
7
25 Is provided by staff who are approachable
1
2
3
4
5
6
7
26 Explains things to me in a way that I can understand
1
2
3
4
5
6
7
27 Is delivered by people who tell me the truth
1
2
3
4
5
6
7
28 Involves the right people in my care planning
1
2
3
4
5
6
7
29 Is located in places that are easy for me to get to
1
2
3
4
5
6
7 Section 3: Additional Comments If you have any comments about the care you receive, please write them in the box below.
Thank you for taking the time to complete this questionnaire Page 2 of 2

Carer Questionnaire
Please complete this questionnaire to the best of your ability. Do not worry if you cannot complete it all.
Section 1: Who provides services for the person you care for?
Name of Team: Please provide the full name of the team (e.g. Community Mental Health Team East Leeds, Assertive Outreach York). If you are unsure of the name of the team, please ask a member of staff.
Section 2: The service offered...
Stro
ngly
Dis
agre
e
Dis
agre
e
Slig
htly
Dis
agre
e
Slig
htly
Agr
ee
Agr
ee
Stro
ngly
Agr
ee
Don
’t K
now
/Not
R
elev
ant
1 Enables me to work in partnership with healthcare professionals
1
2
3
4
5
6
7
2 Gives me the opportunity to express my views and be listened to
1
2
3
4
5
6
7
3 Treats the person I care for as a whole person with a focus on improving all aspects of their life
1
2
3
4
5
6
7
4 Does not make assumptions about the person I care for
1
2
3
4
5
6
7
5 Treats the person I care for as an individual
1
2
3
4
5
6
7
6 Takes the time to get to know the person I care for
1
2
3
4
5
6
7
7 Lets me know how to access help and support
1
2
3
4
5
6
7
8 Gives me correct contact information
1
2
3
4
5
6
7
9 Responds promptly to my needs
1
2
3
4
5
6
7
10 Is provided by healthcare staff who are reliable
1
2
3
4
5
6
7
11 Is provided by healthcare staff who give me full information about the condition and treatment of the person I care for
1
2
3
4
5
6
7
12 Works on goals that are meaningful to the person I care for
1
2
3
4
5
6
7
13 Gives the person I care for the self belief that they can achieve what they want for themself
1
2
3
4
5
6
7
14 Helps the person I care for to overcome barriers to achieving what they want for themself
1
2
3
4
5
6
7
15 Gives the person I care for continuous support when they move from one service to another
1
2
3
4
5
6
7 Please turn over Page 1 of 2

Carer Questionnaire
Section 2 cont’d: The service offered...
Stro
ngly
Dis
agre
e
Dis
agre
e
Slig
htly
Dis
agre
e
Slig
htly
Agr
ee
Agr
ee
Stro
ngly
Agr
ee
Don
’t K
now
/Not
R
elev
ant
16 Is provided by people that I have got to know
1
2
3
4
5
6
7
17 Makes the person I care for feel that they are genuinely cared for
1
2
3
4
5
6
7
18 Involves me in the choices about the care offered to the person I care for
1
2
3
4
5
6
7
19 Is based on an open and trusting relationship with staff
1
2
3
4
5
6
7
20 Helps me to understand the condition and the treatment options available to the person I care for
1
2
3
4
5
6
7
21 Allows me to take as much time as I need during visits
1
2
3
4
5
6
7
22 Makes me feel understood
1
2
3
4
5
6
7
23 Makes sure that accurate information is accessible at all times
1
2
3
4
5
6
7
24 Is provided by staff who put me at my ease and make me feel comfortable
1
2
3
4
5
6
7
25 Is provided by staff who are approachable
1
2
3
4
5
6
7
26 Explains things to me in a way that I can understand
1
2
3
4
5
6
7
27 Is delivered by people who tell me the truth
1
2
3
4
5
6
7
28 Involves the right people in the care planning of the person I care for
1
2
3
4
5
6
7
29 Is located in places that are easy for me to get to
1
2
3
4
5
6
7
30 Is aware of what actions can upset the person I care for
1
2
3
4
5
6
7
31 Is sensitive to the stress of everyday living for carers
1
2
3
4
5
6
7 Section 3: Additional Comments If you have any additional comments, please write them in the box below.
Thank you for taking the time to complete this questionnaire Page 2 of 2