laparoscopy for contralateral patent processus vaginalis (cppv) and non-palpable testis george w....
TRANSCRIPT
Laparoscopy for Contralateral Patent Processus Vaginalis
(CPPV) and Non-Palpable Testis
George W. Holcomb, III, M.D., MBAChildren’s Mercy Hospitals and Clinics
Kansas City, Missouri
The Child with a Unilateral Hernia
What about the other side?
J.Ped. Surg. 29:970-974, 1994J.Ped. Surg. 29:970-974, 1994
J.Ped. Surg. 31:1170-1173, 1996J.Ped. Surg. 31:1170-1173, 1996
Urology 51:480-483, 1998Urology 51:480-483, 1998
Unilateral Hernia
• Unilateral hernia repair only
• Bilateral exploration and repair
• Goldstein Test
• Unilateral hernia repair and diagnostic laparoscopy
• Laparoscopic hernia repair
Options
Unilateral Hernia Repair Only
Advantages
• Repairs known disease
• No contralateral incision or complications
Disadvantages
• 10 - 30% return for contralateral repair
Unilateral Hernia Repair with Diagnostic Laparoscopy
Advantages• Selects contralateral
repair for those with CPPV
• Less than 1% false-positive contralateral explorations
Disadvantages• Uncertain which
child with CPPV will return with symptomatic hernia
Bilateral Exploration and Repair
Advantages
• 10 - 30% have CPPV
• Avoids need for possible second anesthesia and operation
Disadvantages
• 70 - 90% do not have CPPV
• ? Increase injury to spermatic cord
Contralateral InspectionContralateral Inspection

Ambiguous Findings
Geiger, JD - J Pediatr Surg 35:1151-1154, 2000
Study
May 1, 1992 - To evaluate the role
of diagnostic laparoscopy in the
child less than age 10 years with a
known unilateral inguinal hernia
IPEG 2005
JLAST 16:650-653, 2006
May 1, 1992 – January 1, 2003
Total Number of Patients 1870
Known Bilateral Hernia 194
No lap.; Tech. Reasons 73
Total Number Scoped 1603
1603 Patients
Unilateral hernia Bilateral disease
960 643
(60%) (40%)
1603 PatientsPhysical Exam
• #Patients suspected on #Patients suspected on exam to have CPPVexam to have CPPV
• #Patients with CPPV#Patients with CPPV
446
192
(43%)
1603 PatientsPhysical Exam
• #Patients suspected on exam not to have CPPV
• #Patients without CPPV
1157
706
(61%)
Laparoscopy for CPPV1603 Patients
• 643 with CPPV
• 55 (8.5%) positive Goldstein test
Diagnostic Laparoscopy
• Allows surgeon to know which child needs contralateral repair
• Takes 3-5 minutes to accomplish
• Performed through known inguinal hernia sac
• No complications to date
The Parental Perspective Regarding The Contralateral Inguinal Region in
a Child With a Known Unilateral Inguinal Hernia
George W. Holcomb, III, MD, MBA,Kelly A. Miller, MD, Beverly E. Chaignaud, MD,
Stephen B. Shew, MD, Daniel J. Ostlie, MD
Children’s Mercy HospitalKansas City, Missouri
APSA 2003J Pediatr Surg 39:480-482, 2004
Parental Perspective
• Management of the contralateral inguinal region in a child with a unilateral inguinal hernia has been debated for 50 years
• Parental views regarding this issue have not been sought
Methods
• Prospective study with IRB approval
• November 2001 – February 2003
• All patients less than 10 years of age with a unilateral inguinal hernia seen by the senior surgeon (GWH) were eligible for study

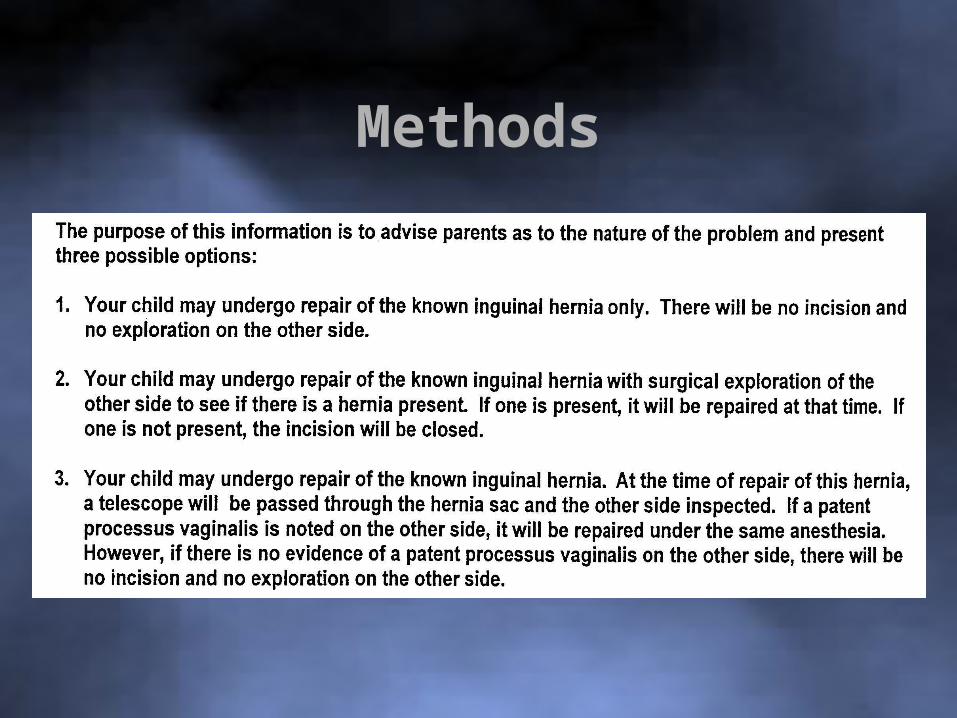
Methods
Methods
Methods
• Motives for parents’ decision
• Last 113 patients requesting contralateral inspection (either exploration or laparoscopy)
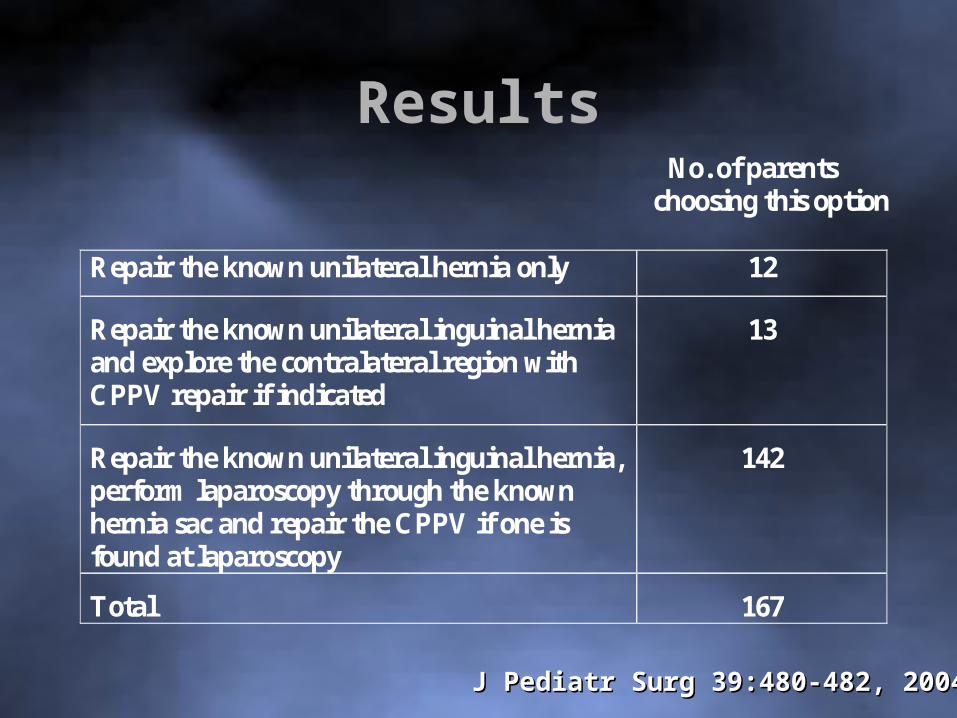
Results No. of parents choosing this option Repair the known unilateral hernia only 12
Repair the known unilateral inguinal hernia and explore the contralateral region with CPPV repair if indicated
13
Repair the known unilateral inguinal hernia, perform laparoscopy through the known hernia sac and repair the CPPV if one is found at laparoscopy
142
Total 167
J Pediatr Surg 39:480-482, 2004J Pediatr Surg 39:480-482, 2004
ResultsParents’ reasons for wanting to evaluate
the contralateral side
• 90 parents: convenience
• 21 parents: concerns about a second anesthesia
• 1 parent: thought there was a hernia on the other side
• 1 parent: 2 previous children with BIH – wanted contralateral
explorationJ Pediatr Surg 39:480-482, 2004J Pediatr Surg 39:480-482, 2004
Conclusions
• When given information about the possibility of a CPPV on the opposite side, over 90 percent of the parents in this study requested evaluation and repair, if needed.
• The vast majority of those desiring contralateral evaluation preferred using laparoscopy as opposed to a contralateral incision
Conclusions
• Most of those desiring contralateral inspection did so for reasons of convenience as opposed to concerns about returning for a second operation and anesthetic
J Pediatr Surg 39:480-482, 2004J Pediatr Surg 39:480-482, 2004
? ? Questions ? ?
Laparoscopy For The Non-palpable Testis

Non-palpable Testis
• 10 percent of undescended testes
• Difficulty with orchiopexy is the length of testicular vessels
• Ultrasound unreliable for location
• Laparoscopy used to determine location/presence/absence of testis
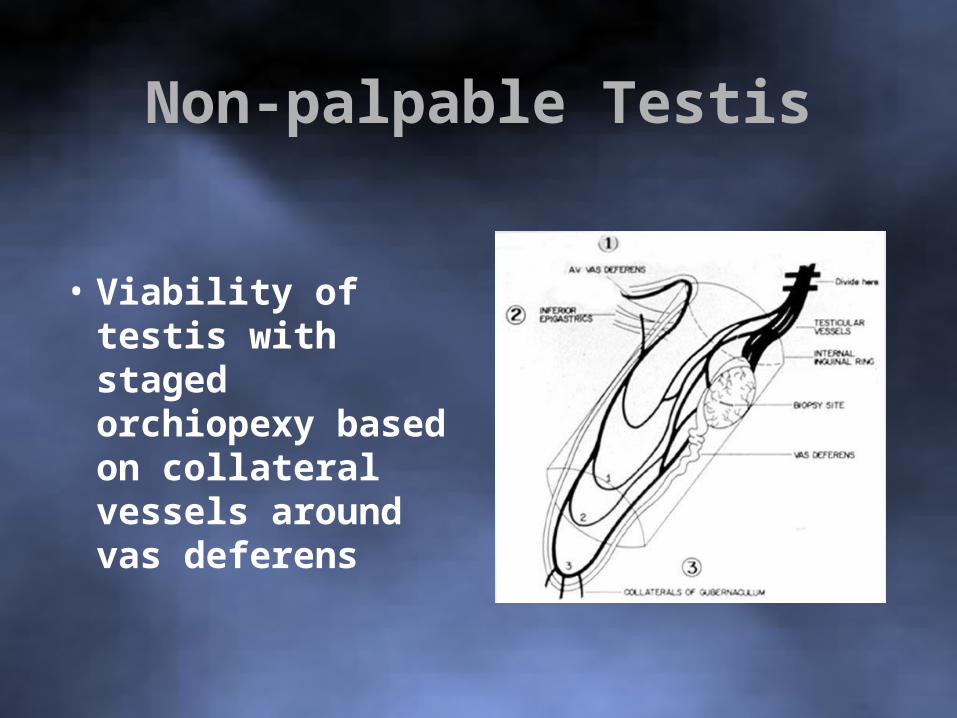
• Viability of testis with staged orchiopexy based on collateral vessels around vas deferens
Non-palpable Testis
Non-palpable Testis
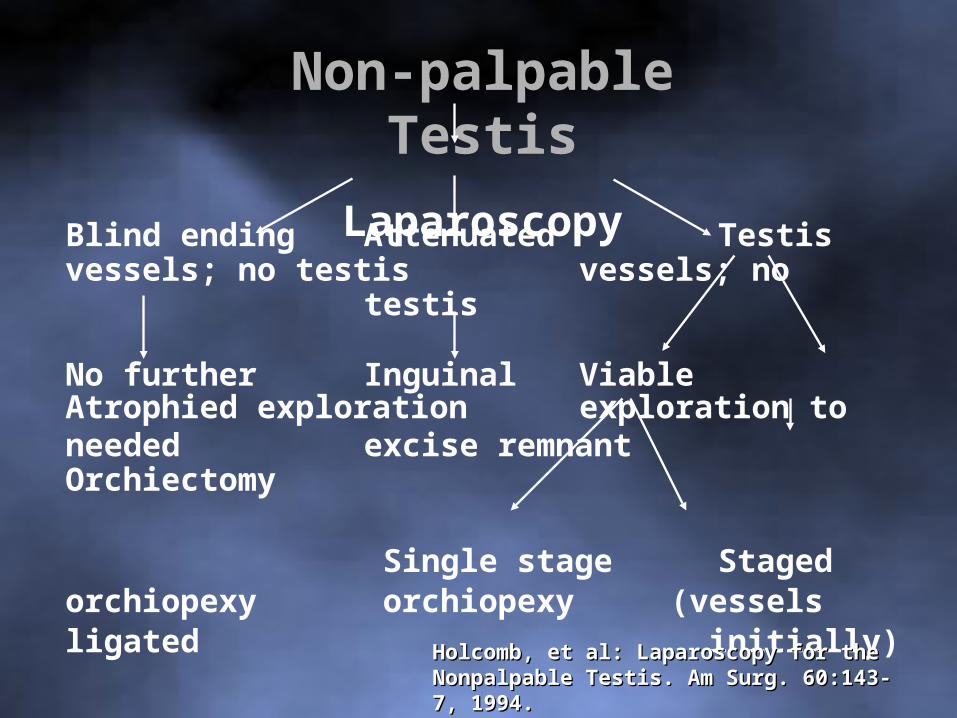
Laparoscopy
Blind ending Attenuated Testisvessels; no testis vessels; no
testis
No further Inguinal Viable Atrophied exploration exploration toneeded excise remnant Orchiectomy
Single stage Staged orchiopexy orchiopexy (vessels ligated
initially)Holcomb, et al: Laparoscopy for the Nonpalpable Holcomb, et al: Laparoscopy for the Nonpalpable Testis. Am Surg. 60:143-7, 1994.Testis. Am Surg. 60:143-7, 1994.
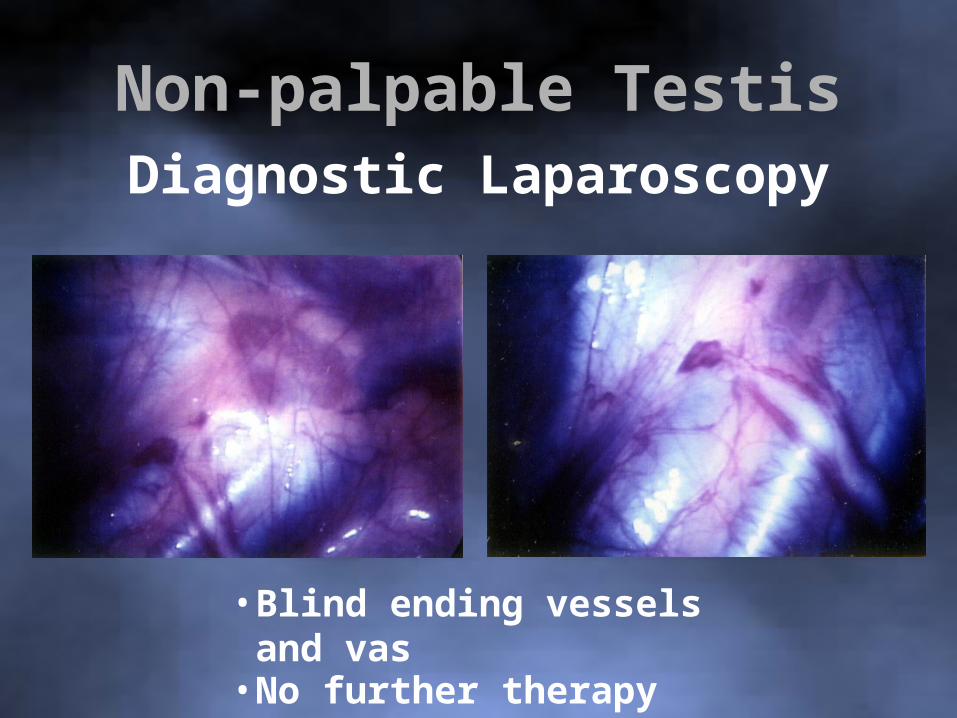
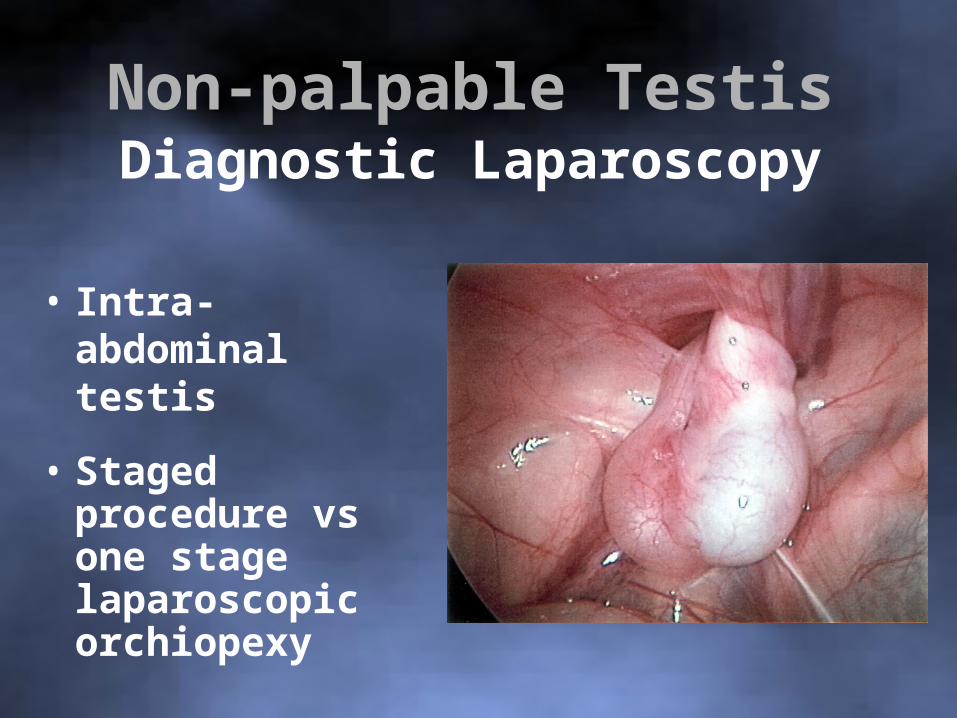
Non-palpable TestisDiagnostic Laparoscopy
• Blind ending vessels and vas• No further therapy

Non-palpable TestisDiagnostic Laparoscopy
• Attenuated vessels -No testis
• Inguinal exploration to excise remnant
Non-palpable TestisDiagnostic Laparoscopy
• Intra-abdominal testis
• Staged procedure vs one stage laparoscopic orchiopexy
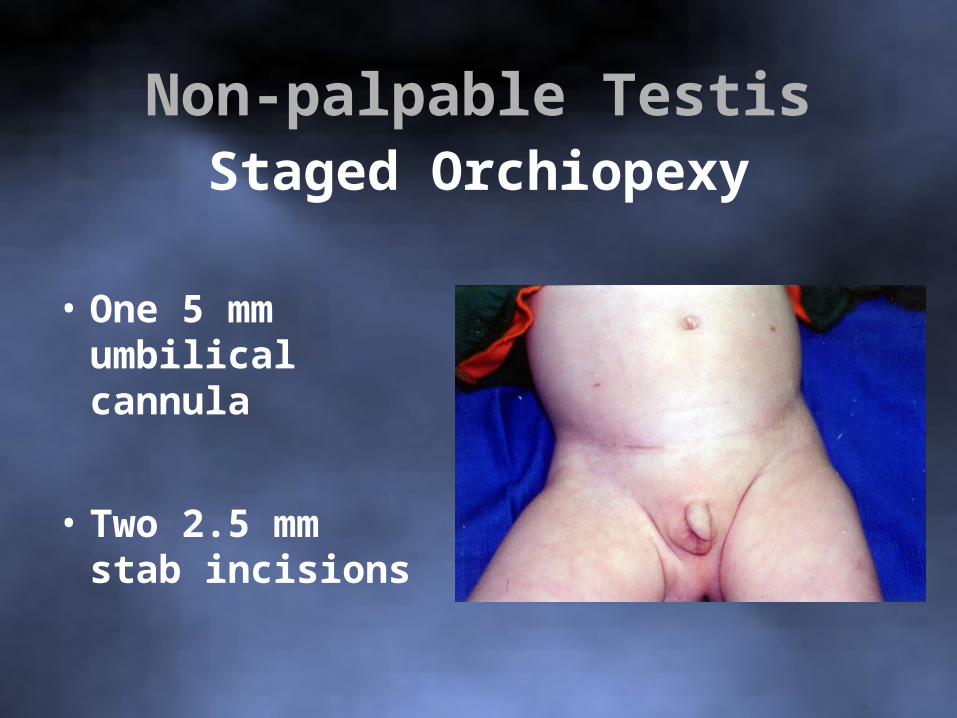
Non-palpable TestisStaged Orchiopexy
• One 5 mm umbilical cannula
• Two 2.5 mm stab incisions
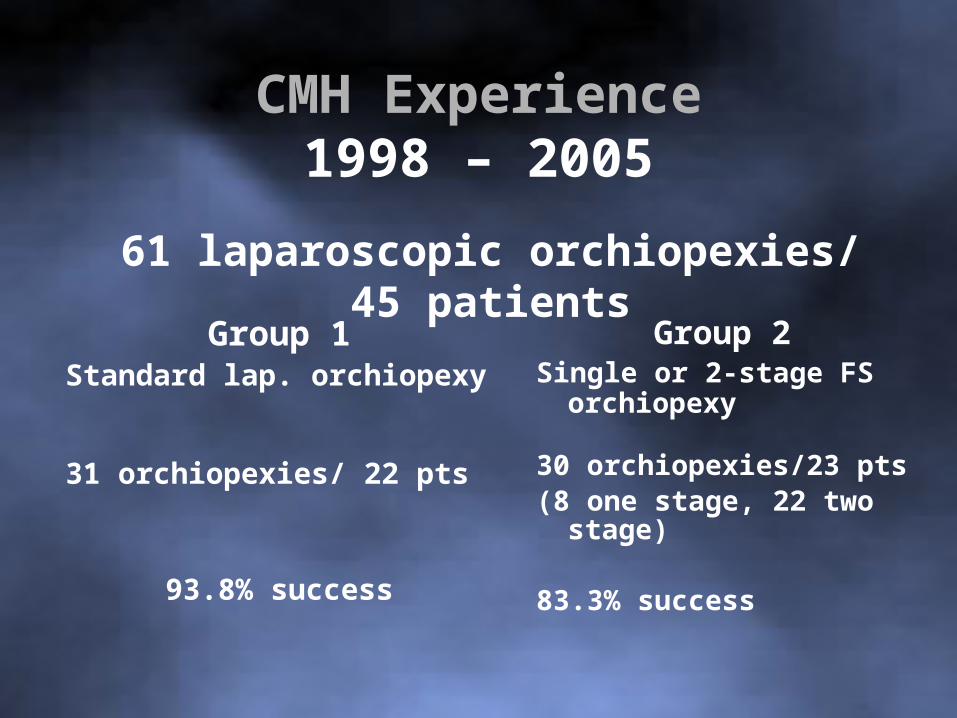
CMH Experience1998 – 2005
Group 1Standard lap. orchiopexy
31 orchiopexies/ 22 pts
93.8% success
Group 2Single or 2-stage FS
orchiopexy
30 orchiopexies/23 pts(8 one stage, 22 two stage)
83.3% success
61 laparoscopic orchiopexies/ 45 patients
CMH Experience1998 - 2005
Group 1
(2/32) – 6.3%
Group 2
(4/24) – 16.7%
Atrophy
Prospective Randomized Trial1 Stage vs 2 Stage F.S. Laparoscopic Orchiopexy
• Non-palpable testis
• Can not reach contralateral internal ring
• Pilot study - 30 patients
www.centerforprospectiveclinicaltrials.com
www.cmhcenterforminimallyinvasivesurgery.com