laparoscopic treatment of stage iv … stage iv endometriosis ... • total abdominal hysterectomy...
TRANSCRIPT
LAPAROSCOPIC TREATMENT
OF STAGE IV ENDOMETRIOSIS
‘’Intestinal complications’’ Korhan Taviloglu, MD
Department of Surgery Florence Nightingale Hospital,
Istanbul, Turkey www.taviloglu.com
1

2 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.

3 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.
Endometriosis

4 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.
Endometriosis epithelium
5 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.
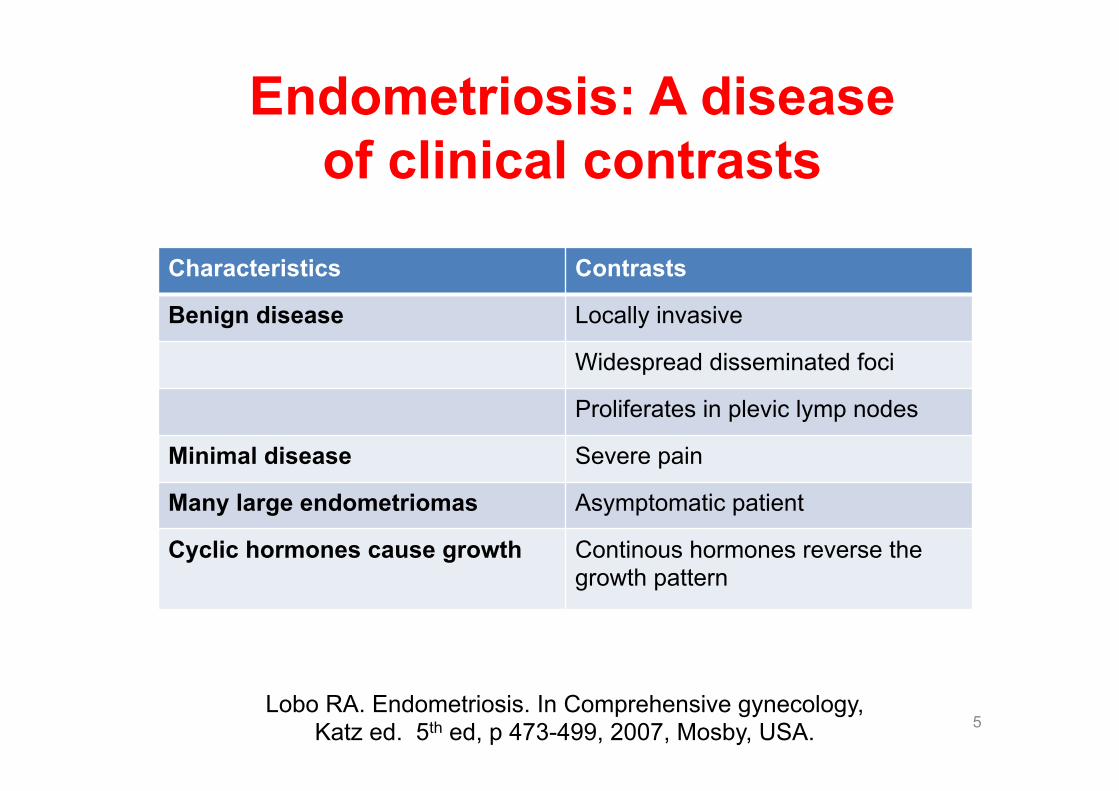
Characteristics Contrasts
Benign disease Locally invasive
Widespread disseminated foci
Proliferates in plevic lymp nodes
Minimal disease Severe pain
Many large endometriomas Asymptomatic patient
Cyclic hormones cause growth Continous hormones reverse the growth pattern
Endometriosis: A disease of clinical contrasts

Endometriosis etiology • Retrograde Menstruation
and Implantation Theory (Sampson’s Theory)
• Coelomic Metaplasia (Meyer’s Theory) and the Induction Theory
• Vascular and Lymphatic Metastasis (Halban’s Theory)
6
Kocakoc E, et al, Ultrasound Clin 2008. Tepleman C, Obstet Gynecol Clin N Am, 2009.
Lobo RA. Endometriosis, 2007,

Endometriosis incidence • Affects about 4-17% of women of reproductive
age, highest rate in Japan. • The mean age at diagnosis is 25 to 29 years. • It is an important cause of infertility (30-50 %)
and pelvic pain. • 20% of women undergoing laparoscopic
evaluation for infertility and 25% of women who have pelvic pain have endometriosis.
• 50-80% of patients are symptomatic; such as dysmenorrhea, dyspareunia, and infertility.
7
Kocakoc E, et al. Endometriosis. Ultrasound Clin 2008. Tepleman C. Adolescent endometriosis. Obstet Gynecol Clin N Am, 2009.
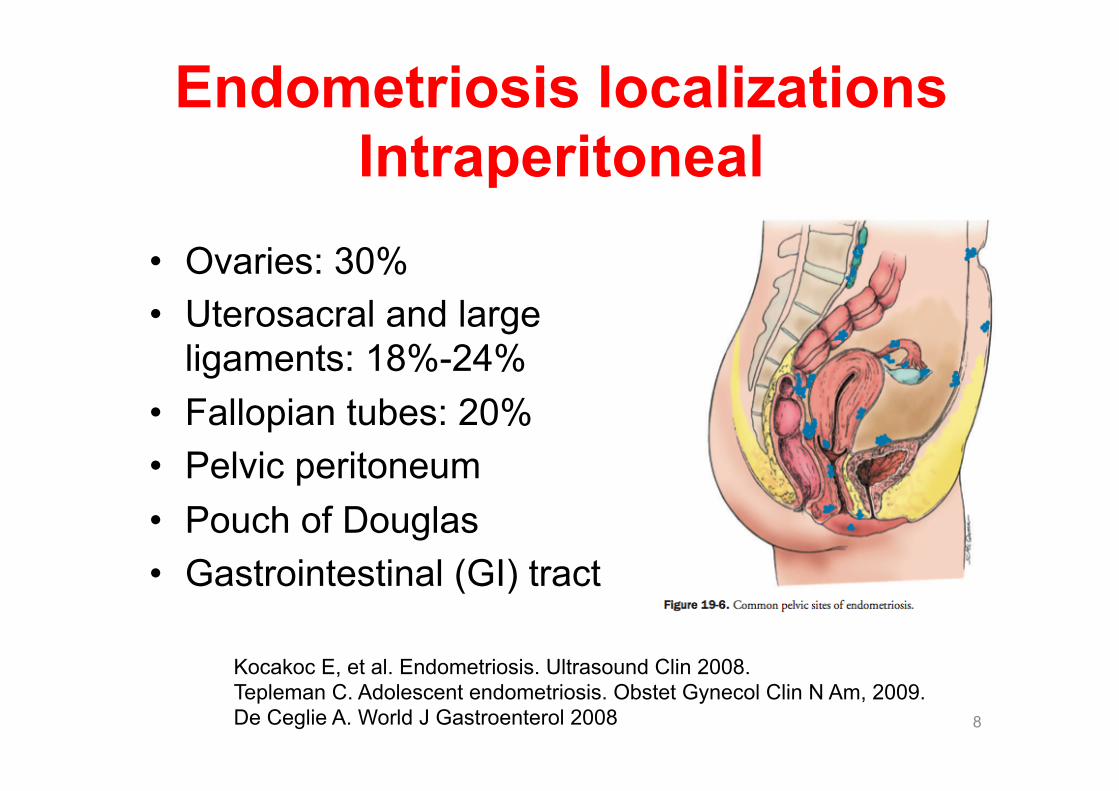
Endometriosis localizations Intraperitoneal
• Ovaries: 30% • Uterosacral and large
ligaments: 18%-24% • Fallopian tubes: 20% • Pelvic peritoneum • Pouch of Douglas • Gastrointestinal (GI) tract
8
Kocakoc E, et al. Endometriosis. Ultrasound Clin 2008. Tepleman C. Adolescent endometriosis. Obstet Gynecol Clin N Am, 2009. De Ceglie A. World J Gastroenterol 2008

Endometriosis localizations Extraperitoneal
9
Kocakoc E, et al. Endometriosis. Ultrasound Clin 2008. Tepleman C. Adolescent endometriosis. Obstet Gynecol Clin N Am, 2009. De Ceglie A. World J Gastroenterol 2008
• Cervical portio: 0.5% • Vagina • Rectovaginal septum • Round ligament • Inguinal hernia sac: 0.3%-0.6% • Umbilicus (1%) • Abdominal scars after
gynaecological surgery: 1.5% • Lungs • Nasal • Arms

Endometriosis intestinal involvement
Endometriosis involves the intestine in 4-35 % of patients.
10 Indraccolo U. Cecal endometriosis. JSLS 2010

11 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.
Locations of bowel endometriosis
68 % 31 %

Bowel endometriosis characteristics
12
• Multiple and vary in size. • Generally serosal, sometimes intramural, and only
rarely mucosal. • Often on the antimesenteric surface of the bowel,
or as a nodular constricting lesion extending into the wall or encircling it .
• Further inspection may reveal rusty brown or purplish specks.
• Thickening of the colonic wall. • May enlarge to present as a mass; endometrioma.
Gordon PH. Endometriosis. In: Principles and Practice of Surgery for the Colon, Rectum, and Anus. Eds: Gordon PH, Nivatvongs S, Informa, 2007.

Bowel endometriosis characteristics
13 Bailey HR.. Perspect Colon Rectal Surg 1992.
• In 1,616 operations for endometriosis, only 1 % involved bowel resections.
• Endometriosis may mimic malignancy. • Gastrointestinal involvement commonly affects those
segments of bowel close to genital organs. • In most instances there is only serosal involvement. • If intestinal symptoms are present, endometriosis is
extensive, and resection is almost always required. • The diagnosis of small intestinal endometriosis is
rarely made prior to operation. A history of colicky abdominal pain might be suggestive.

Endometriosis bowel symptoms
14
• Intermittent abdominal crampy pain • Rectal or pelvic pain • Cyclical rectal bleeding • Tenesmus • Constipation (especially with menses) • Decreased stool caliber • Bloating • Nausea • Vomiting • Diarrhea
Gordon PH. Endometriosis. In: Principles and Practice of Surgery for the Colon, Rectum, and Anus. Eds: Gordon PH, Nivatvongs S, Informa, 2007.
Endometriosis gynecologic symptoms
15
• Dysmenorrhea • Cyclic lower abdominal &
pelvic pain • Dyspareunia • Menometrorrhagia • Infertility
Gordon PH. Endometriosis. In: Principles and Practice of Surgery for the Colon, Rectum, and Anus. Eds: Gordon PH, Nivatvongs S, Informa, 2007.

Intestinal perforation from endometriosis
16 Pisanu A, et al. World J Gastroenterol 2010.

Endometriosis diagnosis No radiologic tests are diagnostic of endometriosis. • Barium enema: narrowed luminal caliber, intramural,
intraluminal polypoid filling defect. • Endoscopy: stenotic lumen with normal mucosa, a
mass or polypoid lesion may be visualized. • IVP: 15 % ureteral involvement • Ultrasound (US) • ERUS • Computed tomography (CT) • Magnetic resonance imaging (MRI) • Laparoscopy: direct visualization & biopsy
17 Gordon PH. Endometriosis. In: Principles and Practice of Surgery for the Colon, Rectum, and Anus. Eds: Gordon PH, Nivatvongs S, Informa, 2007.

Endometriosis diagnosis
18
Kocakoc E, et al. Endometriosis. Ultrasound Clin 2008.
Utrasound MRI

Barium enema
19 Anaf V, et al. Anatomic Significance of a Positive Barium Enema in Deep Infiltrating Endometriosis of the Large Bowel. World J Surg, 2009

Barium enema
20 Anaf V, et al. Anatomic Significance of a Positive Barium Enema in Deep Infiltrating Endometriosis of the Large BowelWorld J Surg, 2009

Laparoscopy
21 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.

Endometriosis treatment 1. Danazol: antiestrogen & androgenic agent 2. Gonadotropin-releasing hormone
antagonists: Leuprolide (Lupron) and Nafarelin (Synarel)
3. Resection: for patients with obstructive symptoms
• Rules out malignancy • Prevents later development of endometrial
carcinoma. • Total abdominal hysterectomy and bilateral
salpingo-oophorectomy is the only option to prevent recurrence.
22 Lobo RA. Endometriosis. In Comprehensive gynecology,
Katz ed. 5th ed, p 473-499, 2007, Mosby, USA.

Colonic endometriosis treatment • Local excision of a colonic endometrioma
may be an effective treatment. • Coronado et al. presented 77 consecutive
patients with deep colorectal endometriosis treated with a full thickness resection.
• A low anterior resection was performed in 68 patients (88.3%); a disc excision of the anterior rectal wall in five (6.5%); sigmoid resection in three (3.9%), and partial cecal resection in one (1.3%).
23 Coronado C, et al. Fertil Steril 1990.

Colonic endometriosis treatment result of pelvic symptoms
• Complete relief: 49% • Improvement: 39% • No improvement: 11% • Worsening: 1%.
24 Coronado C, et al. Fertil Steril 1990.
THANK YOU!! Korhan Taviloglu, MD
Department of Surgery Florence Nightingale Hospital,
Istanbul, Turkey www.taviloglu.com
25