lactation and lactational complaints
TRANSCRIPT
OBS&GYN

Why Breastfeed?
Literature is replete with scientific evidence on the benefit of the most natural process of a mother-
breast feeding her baby
Exclusive breast feeding in the first six months of life can cut down under-five child mortality by
13-15%
Lactation Anatomy and Physiology
Breast enlargement
During pregnancy and lactation indicates the mammary glands
are becoming functional
Breast size before pregnancy does not determine the amount
of milk a woman will produce
Lactation Anatomy and Physiology
Hormones during pregnancy
Estrogen stimulates the ductile systems to grow, then
estrogen levels drop after birth
Progesterone increases the size of alveoli and lobes
Prolactin contributes to increasing the breast tissue during
pregnancy
Lactation Anatomy and Physiology
Alveoli secrete milk and contract when stimulated
Oxytocin stimulates milk secretion and is released
during the ‘let down’ or milk ejection reflex
After let down, milk travels into the ductules, then to
the larger – lactiferous or mammary ducts
Lactation Anatomy and Physiology
Hormones during breastfeeding
Prolactin levels rise with nipple stimulation
Alveolar cells make milk in response to prolactin when the
baby sucks
Oxytocin causes the alveoli to squeeze the newly produced
milk into the duct system

Lactation Anatomy and Physiology
Latch On and sucking
Oxytocin Release
Releases Milk
Infant Empties Breast
Production Increases
Milk Production Occurs
Interference with this cycle decreases the milk supply.
Advantages
Baby Mother Family

Breastfeeding Mother Health Benefits
Less postpartum bleeding
More rapid uterine involution
Weight loss
Decreased premenopausal breast cancer rates
Decreased ovarian cancer rates
Lactational amenorrhea Should still use progesterone only contraceptives
Combined contraceptives dry up milk
Advantages to the baby
Decreased incidence of infections- diarrhea, RTI, otitis media, NE, late onset sepsis in pre term
Reduction of both Type I and II diabetes, leukemias, lymphomas, asthma and obesity.
Enhances performance on cognitive development

Advantages to the family
Readily available
Hygienic
Economical
Keeps children healthy

The first few steps…..
Proper antenatal counseling
A well informed, supportive husband
Relative or nurse in the labour room
At The Earliest
In the healthy neonate suckling reflex is at its peak- 30 to 40 mins after birth
Early feeds stimulate production of prolactin and increases the mean duration of breast feeding

The first few steps…..
Placed prone on the mother’s abdomen
Feed in the 1st hr of delivery
on the labour table itself
Breast Feeding In Operative Delivery
Maintain skin to skin contact
Breast feeding within 1 hr when LSCS under spinal anesthesia; otherwise when the effect of GA weans off.
Women should not have pain, as it decreases production of milk
Position of baby is important
Frequency And Length Of Breast Feeding
Exclusive breast feeding for 6 months
On an average 650 to 850 ml milk is produced per day.
2 to 3 hourly or 8 feeds per day or feed on demand
Duration time is 25 to 30 min- both breasts should be fed each time

Indicators Of Adequate Feed
No of feeds each day (8 or on demand)
If baby sleeps well for 2 to 3 hours after feed
Urine output- 6 to 8 diapers per day
No of stools- 4 to 5 times per day
Weight gain- 30 gm per day

Care Of Mother
Calorie intake- 300 to 500 extra calories
( 2200 to 3000 kcal per day)
Balance diet and no weight reduction
Fluid intake : 22% from well balanced diet; increase fluid intake is essential)
Iron and Calcium Supplementation
GALACTOGOGUES
There is no ideal galactogogue
Chlorpromazine and metoclopromide- 10 mg 3 times daily for 7 days
Self confidence, freedom from anxiety, soothing environment with vigorously sucking by an active
baby are the most effective pre-requisites for successful establishment of lactation.
Chlorpromazine
Chlorpromazine is a dopamine antagonist
maternal side effects are more frequent
Adverse effects include extrapyramidal reactions, orthostatic hypotension, anticholinergic effects, and altered cardiac conduction.
This drug for selected refractory cases
Metoclopramide
Reproductive Considerations
Metoclopramide may increase prolactin concentrations;
hyperprolactinemia may suppress hypothalamic GnRH,
inhibit reproductive function by impairing gonadal steroidogenesis.
Amenorrhea and impotence have been reported.
Domperidone
is not currently approved in any country as a galactagogue (Sewell 2017).
Domperidone may increase prolactin concentrations and cause galactorrhea and gynecomastia
As such, it has been used off-label as a galactagogue in patients with insufficient milk production.
SUPPRESSION
Estrogen
Bromocriptin
Cabergolin
Thiazide
Pyridoxine
OCP
Testosterone

Breastfeeding Barriers
Early breastfeeding failures deprive infants of the
benefits, and leave many mothers disappointed
It is a natural process, but many mothers need a lot
of help

Breastfeeding Barriers
Breast Pathology Flat/inverted nipples, breast reduction surgery that severed
milk ducts, previous breast abscess, extremely sore nipples (cracked, bleeding, blisters, abrasions)
Hormonal pathology Failure of lactogenesis, hypothyroidism
Overall health Smoking, anemia, poor nutrition, depression
Psychosocial Restrictive feeding schedules, mother without support
system, not rooming in with baby, bottle supplementing when not medically required
Other Previous breastfed infant who failed to gain weight well,
perinatal complication (hemorrhage, htn, infection

Breastfeeding Hospital Discharge Support
Mother breastfeed longer if they: Are confident at hospital discharge
Have a good support system after discharge
Receive follow up after discharge
Upon discharge Give written information
Recommend mom to keep breastfeeding record
Give mom phone number for a telephone helpline
Lactation consultant follow-up

AN AC U T E I N F L AM M AT I O N O F T H E
I N T E R L O B U L AR C O N N E C T I V E T I S S U E W I T H I N
T H E M AM M A RY G L AN D
Mastitis
Mastitis
Normal breast
architecture

Outline
Epidemiology
Presentation
Predisposing factors
Microbiology
Treatment
Complications
Effect on breast milk
Epidemiology
Incidence 2-10%
Hospitalization is low (9 / 10000 delivery)
Most common worldwide <10%
Most common 2nd-3rd week postpartum 74-95% in first 12 weeks
Can occur anytime in lactation
Recurrence is more in prior history

Presentation
Systemic illness: Chills, myalgias
Fever of ≥ 38.5
Tender, hot, swollen wedge-shaped erythematous
area of breast
Usually one breast
Differential Diagnosis
Fullness: bilateral, hot, heavy, hard, no redness
Engorgement: bilateral, tender, +/- fever, minimal diffuse erythema
Blocked Duct: painful lump with overlying erythema, no fever, feel well, particulate matter in milk
Differential Diagnosis
Galactocele: smooth rounded swelling (cyst)
Abscess: tender hard breast mass, +/- fluctuance,
skin erythema, induration, +/- fever
Inflammatory Breast Carcinoma: unilateral, diffuse
and recurrent, erythema, induration
Causes
Milk Stasis
Stagnant milk increases pressure in breast leading to leakage
in surrounding breast tissue
Milk, itself, causes an inflammatory response
+/- Infection
Milk provides medium for bacterial growth

Causes
3 groups Milk stasis (bacteria<10^3, leuk<10^6)
Noninfectious inflammation (bacteria <10^3, leuk >10^6)
Infectious (bacteria >10^3, leuk>10^6)
Randomized treatment No intervention
Systematic emptying of breast
Infectious group with 3rd intervention: antibiotics and systematic emptying

Causes
“Poor results” Milk stasis 3 recurrences, 7 impaired lactation
Noninfectious 13 recurrences
Infectious 6 abscesses, 21 recurrences
Conclusion: Treat with antibiotics
Predisposing factors Improper nursing technique Timing of feeds Poor attachment
Oversupply of milk Overabundant milk supply Lactating for multiples Rapid weaning Blocked nipple pore or duct
Pressure on Breast Tight Bra Car seatbelt (yes, this is actually listed) Prone sleeping position
Predisposing factors
Damaged nipple (nipple fissure) Primiparity
Previous history of mastitis
Maternal or neonatal illness
Maternal stress
Work outside the home
Trauma
Genetic

Microbiology
Detection of pathogens difficult
Usually nasal/skin flora
Difficult to avoid contamination
Milk culture
Encouraged in hospital acquired, recurrent mastitis, or no
response in 2 days
Microbiology
Staph Aureus
MRSA (IMPORTANT PATHOGEN)
Coag neg staph
Also, Group A and B βhemolytic Strep, E Coli, H. flu
Fungal infections
TB where endemic – 1% of cases
Fungal infections
Based on case reports that anti-fungal cream improves
Case reports of cyptococcal infection Most common: Candida Albicans Genital tract Newborn oral colonization
May lead to nipple fissure Thought to be associated with deep, shooting
pains and nipple discomfort Most commonly treated with fluconozole to ,
oral nystatin to infant

Candida Infection
Treatment
Supportive Therapy Rest, fluids, pain medication, anti-inflammatory agents,
encouragement
Continue breast feeding
Antibiotics that cover Staph and Strep Culture results
Severe symptoms
Nipple fissure
No improved after 12-24 hours of milk removal
Treatment
Dicloxicillin 500 mg qid
Cephalexin 500 mg qid
Erythromycin 500 mg bid if PCN allergic
If resistant to treatment penicillinase-producing
staph, then vancomycin or cefotetan until 2 days
after infection subsides
Minimum treatment 10-14 days but 5-7 days enough
for good and fast response

( O T H E R B AD T H I N G S R E L AT E D T O M AS T I T I S )
Complications

Breast Abscess

Breast Abscess
Breast abscess
with early skin
necrosis
Abscess
Most common in first 6 weeks
0/1 % of mastitis cases
No differences b/t groups by age, parity,
localization of infection, cracked nipples, + milk
cultures, mean lactation time
Duration of symptoms: only independent variable
favoring abscess development

Breast Abscess
Inflammatory
breast cancer
Other Complications
Distortion of breast
Chronic inflammation

Granulomatous Mastitis
Noncaseating granulomas in a lobular distribution
Differential Diagnosis TB mastitis
Foreign body
Fat necrosis
Autoimmune: sarcoid, erythema nodusum, polyarthritis
Presentation Unilateral Breast lump
No infection identified at presentation
Granulomatous Mastitis
Can mimic Breast Ca on clinical, radiological, and cytological exams
Diagnosis: Histology
Treatment: Antibiotics not helpful
Corticosteroids
Excision biopsy
Limited literature, but no clear association with breast feeding, OCPs

Neonatal Mastitis
Occurs up to 5 weeks of age
Girls outnumber boys 2 : 1
Etiology: 85% S. aureus, also E. coli, group D
Streptococcus
Treatment:
Prompt antibiotics (IV?)
Careful needle aspiration if abscess

Effect on Milk
Increased HIV transmission risk
Alternating breast/bottle increased risk
Role of free virus vs cell bound virus unclear
If ♀ must breast feed, then pump on affected breast
(pasteurize) and feed on unaffected

RETRACTED NIPPLE
Antenatal examination and counseling for cleaning of nipples and their aversion is important
20 cc syringe may also be used for correcting retraction
Nipple shield
Use of breast pump

SORE NIPPLE
Commonest
Cause improper latching
Symptoms: pain
Signs: nipple is red, cracked, bruised, blistered and tender
Treatment: linolin/ emolient cream; air drying and applying own milk, nipple shield for time being, EBM
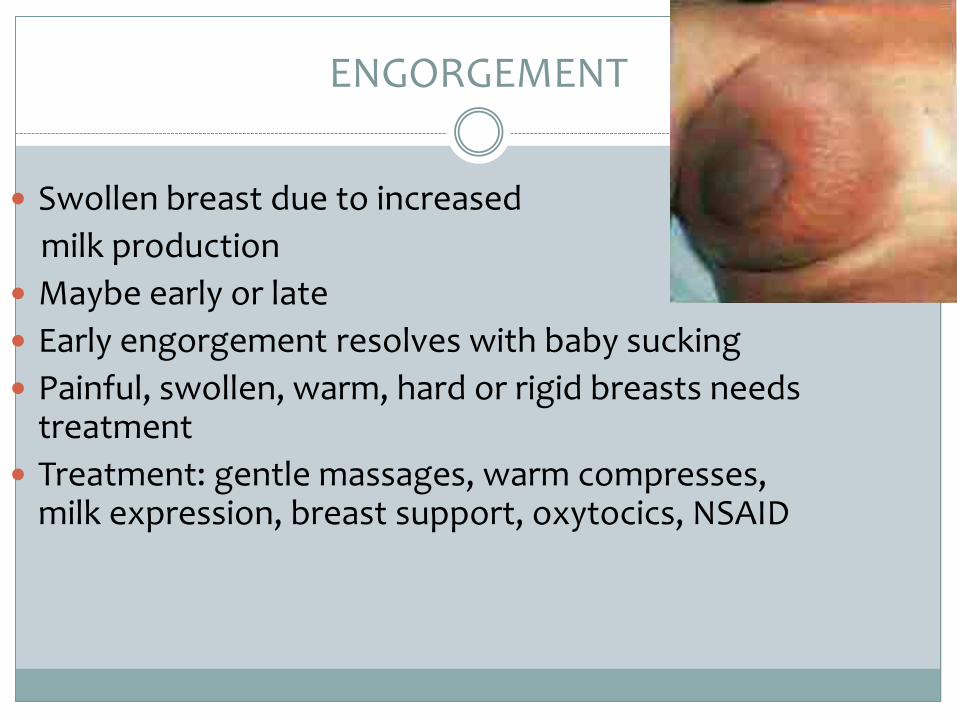
ENGORGEMENT
Swollen breast due to increased
milk production
Maybe early or late
Early engorgement resolves with baby sucking
Painful, swollen, warm, hard or rigid breasts needs treatment
Treatment: gentle massages, warm compresses, milk expression, breast support, oxytocics, NSAID


WEANING
Aim is to introduce- iron, calcium, vitamins and calories to baby in adequate quantity through liquid
and semisolid diet from 4 to 6 months of age
It should be done gradually
PREVENTION of lactational mastitis
administration of a Lactobacillus probiotic during late pregnancy may reduce the likelihood of lactational mastitis.
women who received oral Lactobacillus salivarius PS2 had a lower incidence of mastitis than those who received placebo
It is unknown whether administration of probiotic therapy would be beneficial for pregnant women with no history of lactational mastitis.
