laboratory diagnosis of viral infections affect the lower...
TRANSCRIPT
Laboratory Diagnosis of Viral I f i ff h LInfections affect the Lower
Respiratory TractRespiratory Tract
M Parsania, Ph.D.M Parsania, Ph.D.Tehran Medical Branch, Islamic Azad University
Overview of viral infections affect the lower respiratory tract
• Influenza A BInfluenza A, B• Parainfluenza virus 1‐4
i S i l i• Respiratory Syncytial Virus• Human Metapneumovirus• More recently described respiratory virus:
–Human bocavirusHuman bocavirus
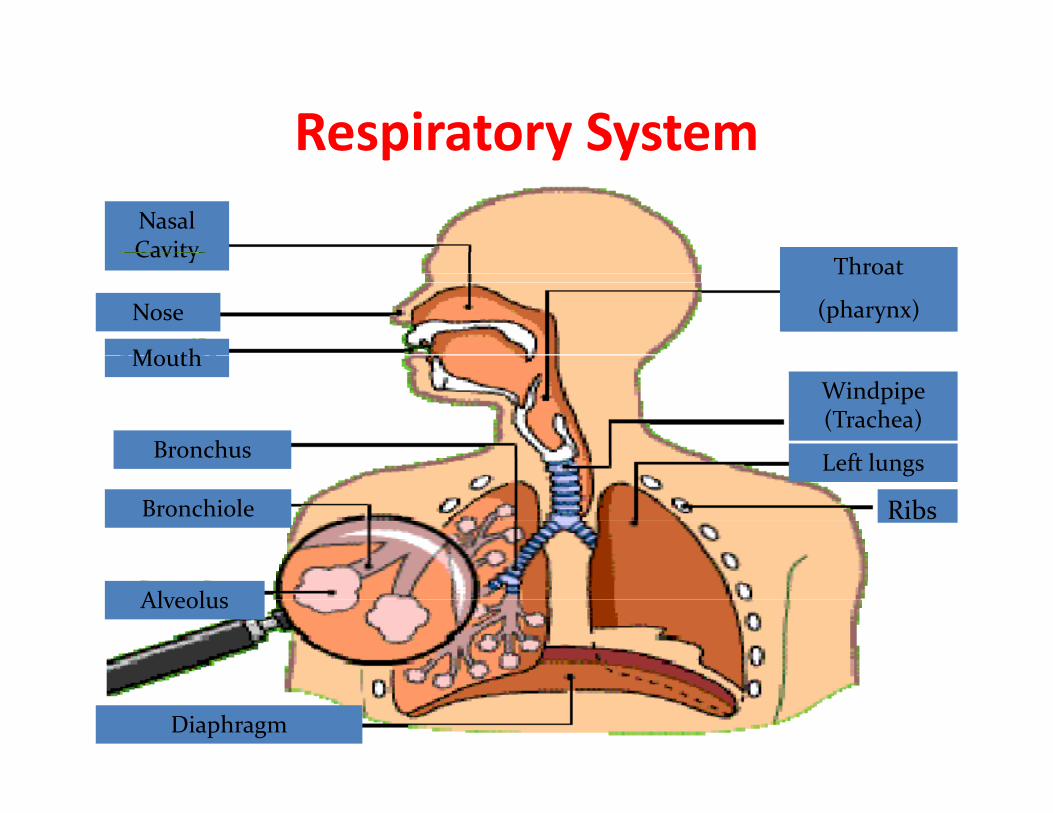
Respiratory System esp ato y SysteNasal CavityCavity
Nose
Mouth
Throat
(pharynx)
Mouth
Bronchus
Windpipe (Trachea)
L ft l
Bronchiole
Left lungs
Ribs
Alveolus
Diaphragm
Influenza virusInfluenza virus
CLASSIFICATIONFamily Orthomyxoviridae
on the basis of antigenicity of virus proteins g y p(NP and MP) Classified into three main groups:
Influenza A Influenza B Influenza C
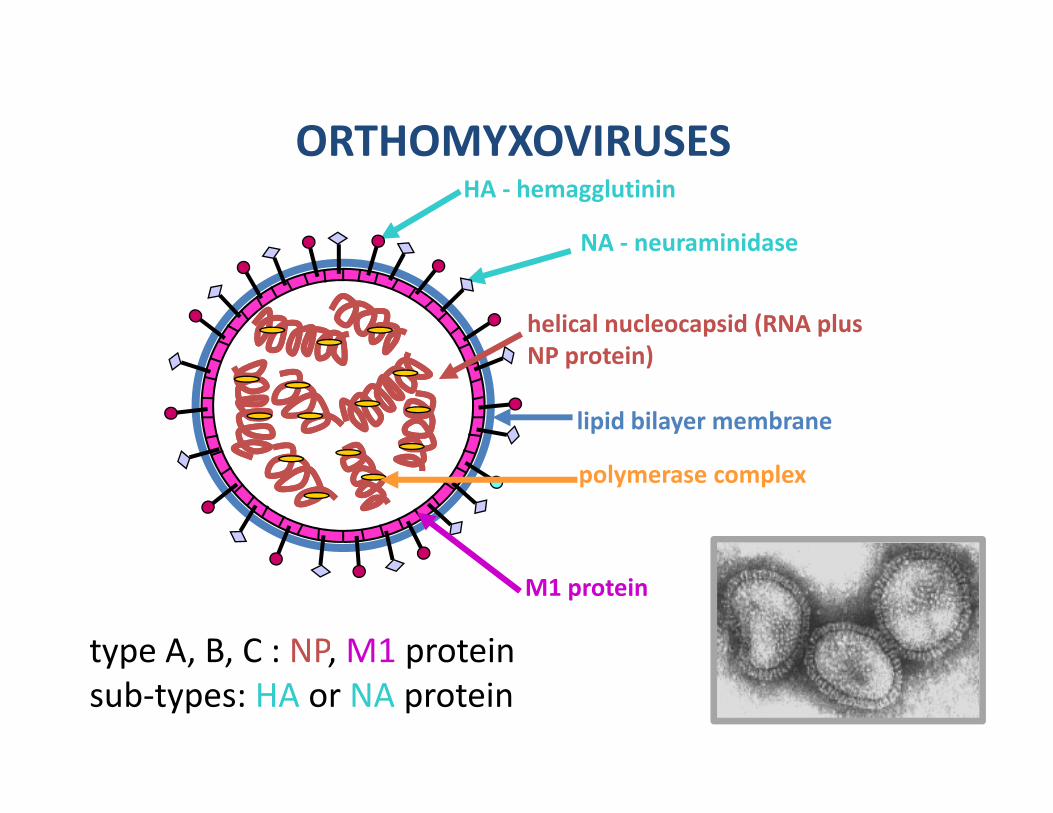
ORTHOMYXOVIRUSESORTHOMYXOVIRUSESHA ‐ hemagglutinin
NA ‐ neuraminidase
helical nucleocapsid (RNA plus NP protein)NP protein)
lipid bilayer membrane
polymerase complex
M1 protein
type A, B, C : NP, M1 protein
٧
yp , , , psub‐types: HA or NA protein

Three viral types are distinguished by th i t i d l t i
Clinical Pattern of
their matrix and nucleoproteins
Type HostClinical Importance
Pattern of Occurrence Subtypes
A Humans,birds, horses,
Moderate to severe
Sporadic,epidemics,
YesH1-H16†
other mammals disease pandemics N1-N9‡
B Humans Moderate to severe
Sporadic,epidemics
No2 lineages
disease co-circulate
C Humansand swine
Milddisease
Sporadic, localized
No
Influenza A is further classified according to its H and N subtypes, e.g.A/H3N2, A/H1N1
outbreaks
Bridges et al. 2008.
A/H3N , A/H N†H = hemagglu nin; ‡N = neuraminidase.
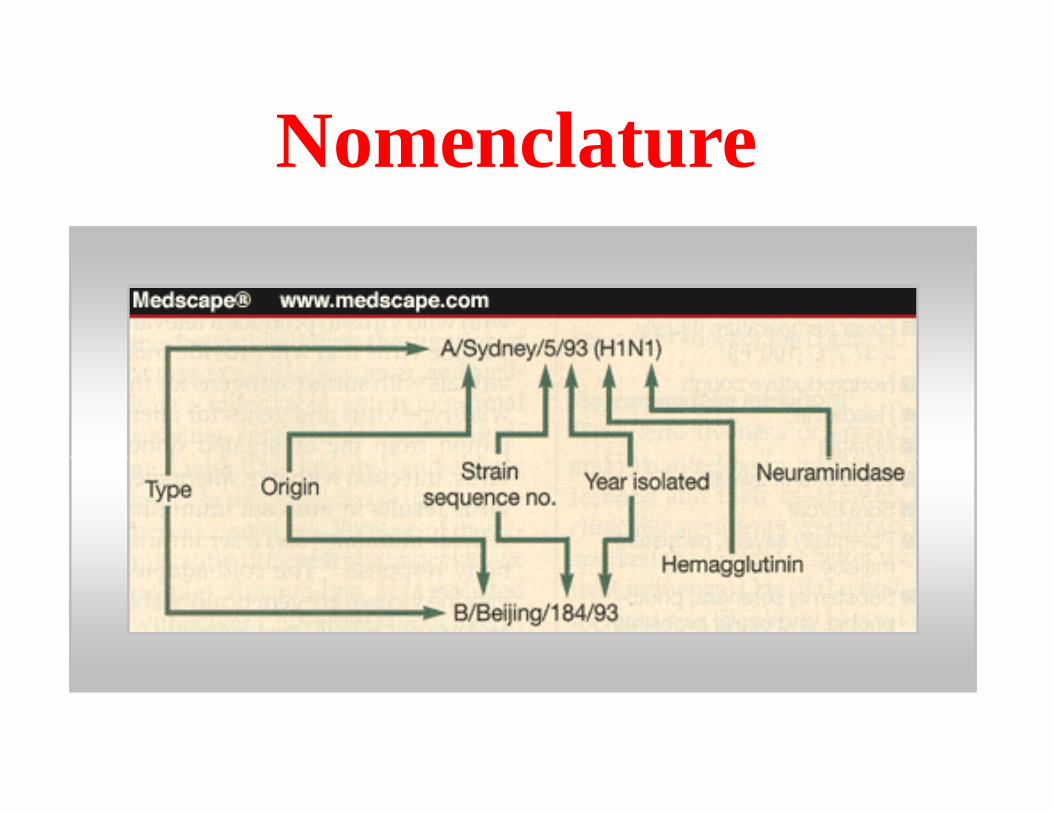
NomenclatureNomenclature
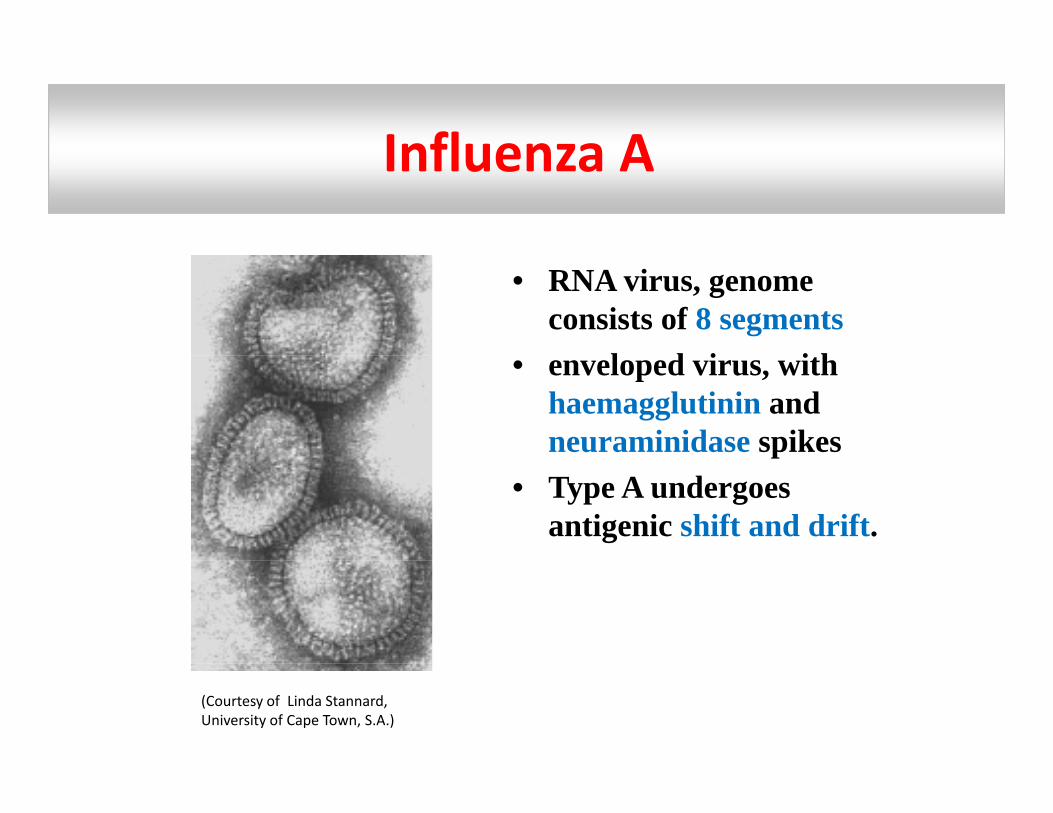
Influenza AInfluenza AInfluenza AInfluenza A
• RNA virus, genome consists of 8 segments
l d i ith• enveloped virus, with haemagglutinin and neuraminidase spikesp
• Type A undergoes antigenic shift and drift.
(Courtesy of Linda Stannard, University of Cape Town, S.A.)
Influenza BInfluenza B
P d l i di th d
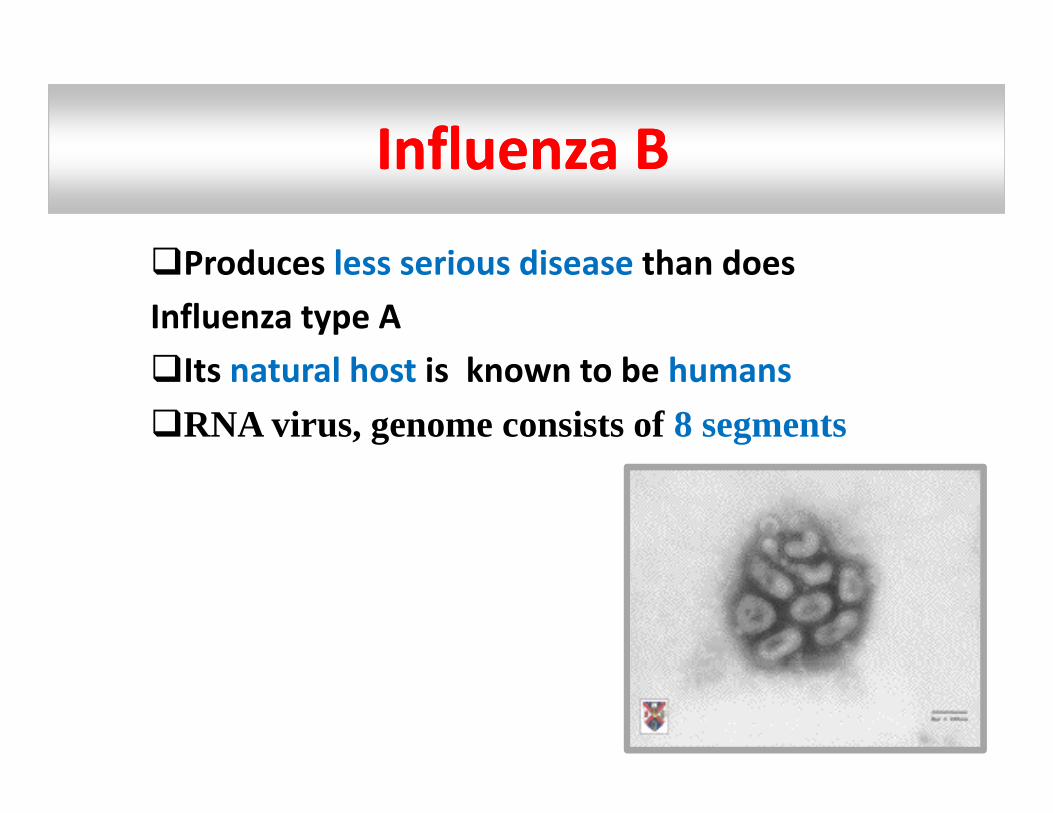
Influenza BInfluenza B
Produces less serious disease than does Influenza type AIts natural host is known to be humansRNA virus, genome consists of 8 segments
Influenza CFirst isolated in 1949
Influenza CFirst isolated in 1949
Not known to be responsible for epidemicsNot known to be responsible for epidemics
I l h i k b h dIts natural host is known to be humans and swineRNA i i t f 7 tRNA virus, genome consists of 7 segments
Viral Structure
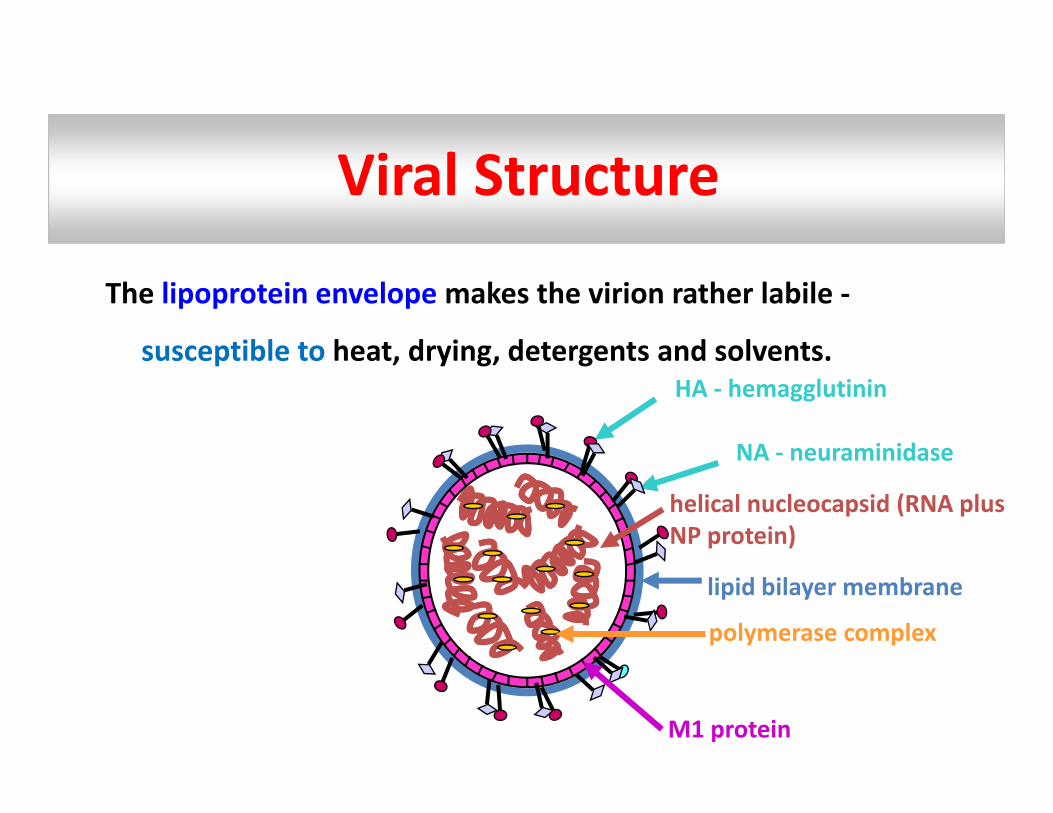
The lipoprotein envelope makes the virion rather labile ‐
susceptible to heat drying detergents and solventssusceptible to heat, drying, detergents and solvents. HA ‐ hemagglutinin
NA ‐ neuraminidase
helical nucleocapsid (RNA plus NP protein)
NA neuraminidase
polymerase complex
lipid bilayer membrane
M1 protein
Influenza A Virus Viral Structure
The virion is generally rounded but may be long and
filamentous.a e ous
A single‐stranded RNA genome is closely associated with a
helical nucleoprotein (NP) and is present in eight separatehelical nucleoprotein (NP), and is present in eight separate
segments of ribonucleoprotein (RNP), each of which has to
be present for successful replication.
Influenza A VirusInfluenza A Virus Viral Structure
The envelope carries two types of protruding spikes.
One is a box ‐ shaped protein, called the neuraminidase
(NA), of which there are 9 major antigenic types, and(NA), of which there are 9 major antigenic types, and
which has enzymic properties as the name implies
Influenza A VirusInfluenza A Virus Viral Structure
The other type of envelope spike is
a trimeric protein called the haemagglutinin (HA)
which there are 16 major antigenic types.j g yp
Surface glycoproteinsSurface glycoproteins
H l ti iHaemagglutininH or HA
responsible for pathogenicity of the virusresponsible for pathogenicity of the virusallows virus to adhere to endothelial cells in the
respiratory tractp ymain determinant of immunity
NeuraminidaseN or NA
allows release of newly formed viruses within hosthost
determinant of disease severity
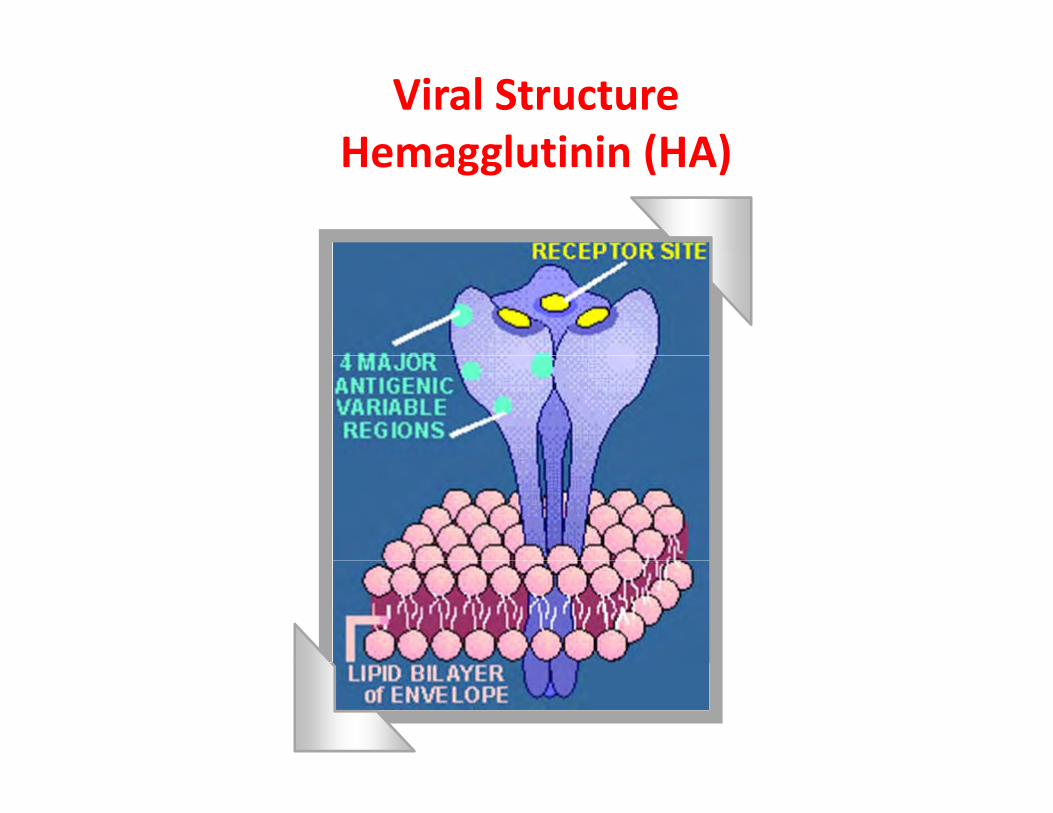
Viral StructureHemagglutinin (HA)Hemagglutinin (HA)
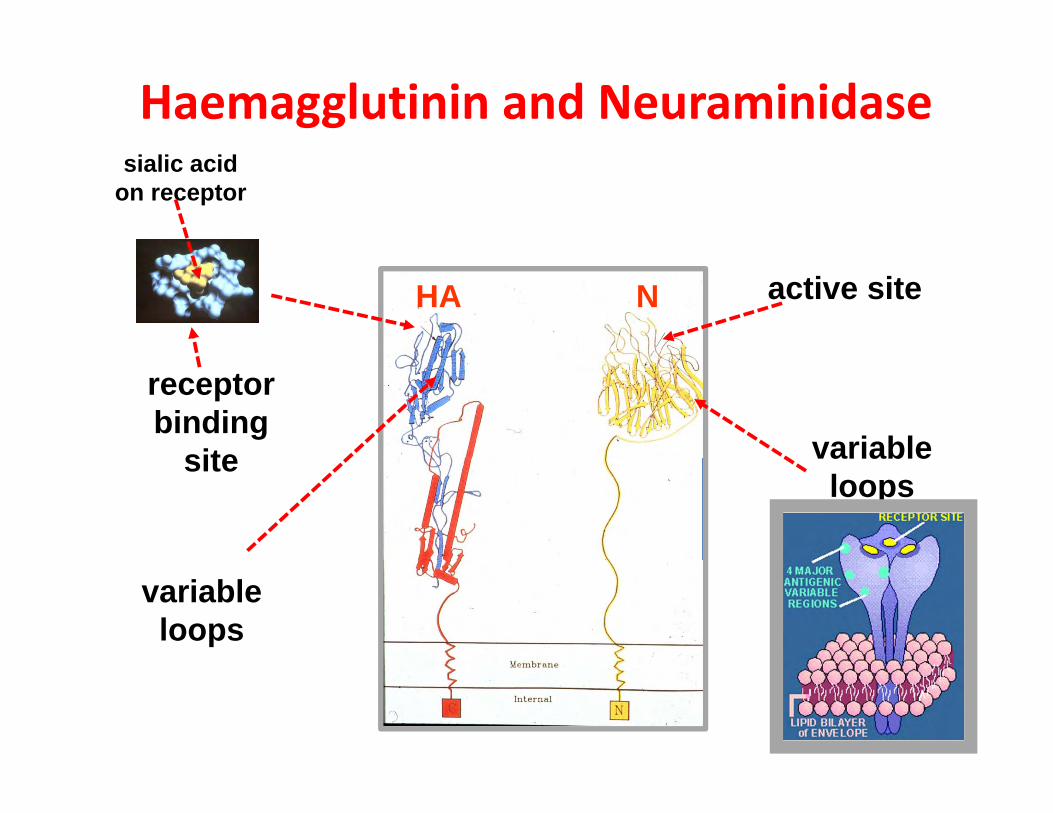
Haemagglutinin and Neuraminidasesialic acid
on receptor
active siteHA N
receptorbinding
site variablesite variableloops
variableloops
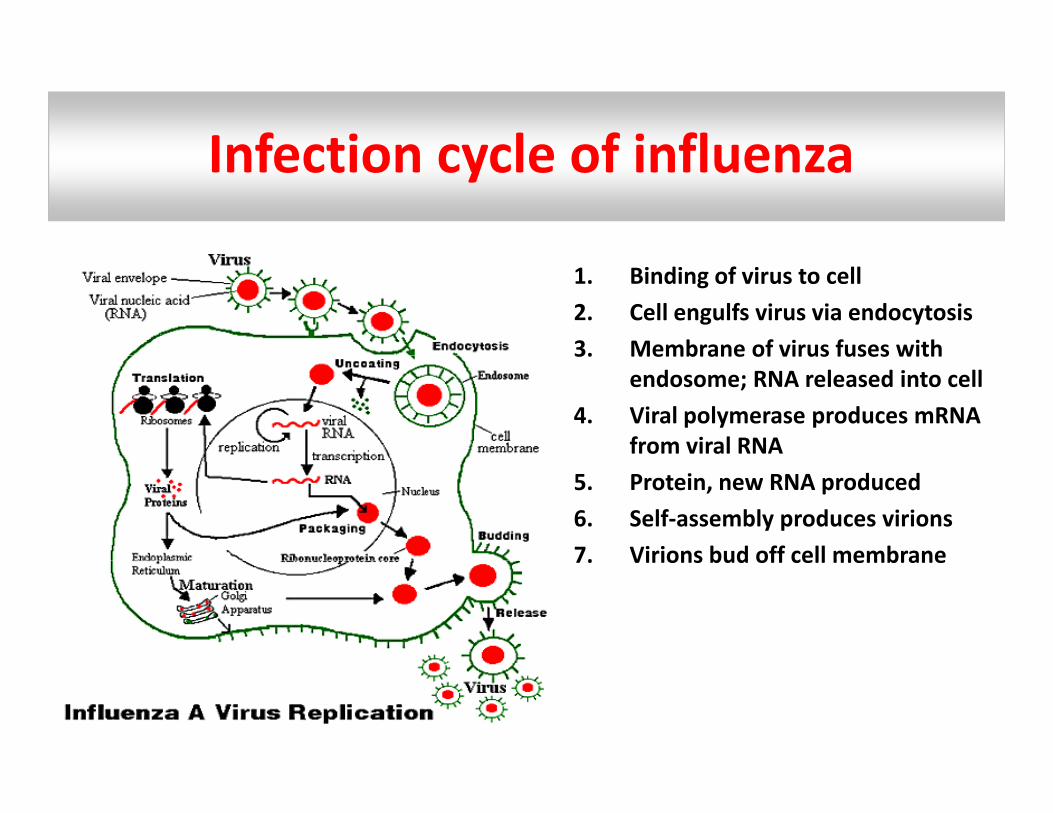
Infection cycle of influenzaInfection cycle of influenza
1. Binding of virus to cell2. Cell engulfs virus via endocytosis3. Membrane of virus fuses with3. Membrane of virus fuses with
endosome; RNA released into cell4. Viral polymerase produces mRNA
from viral RNA5. Protein, new RNA produced6. Self‐assembly produces virions7. Virions bud off cell membrane7. Virions bud off cell membrane
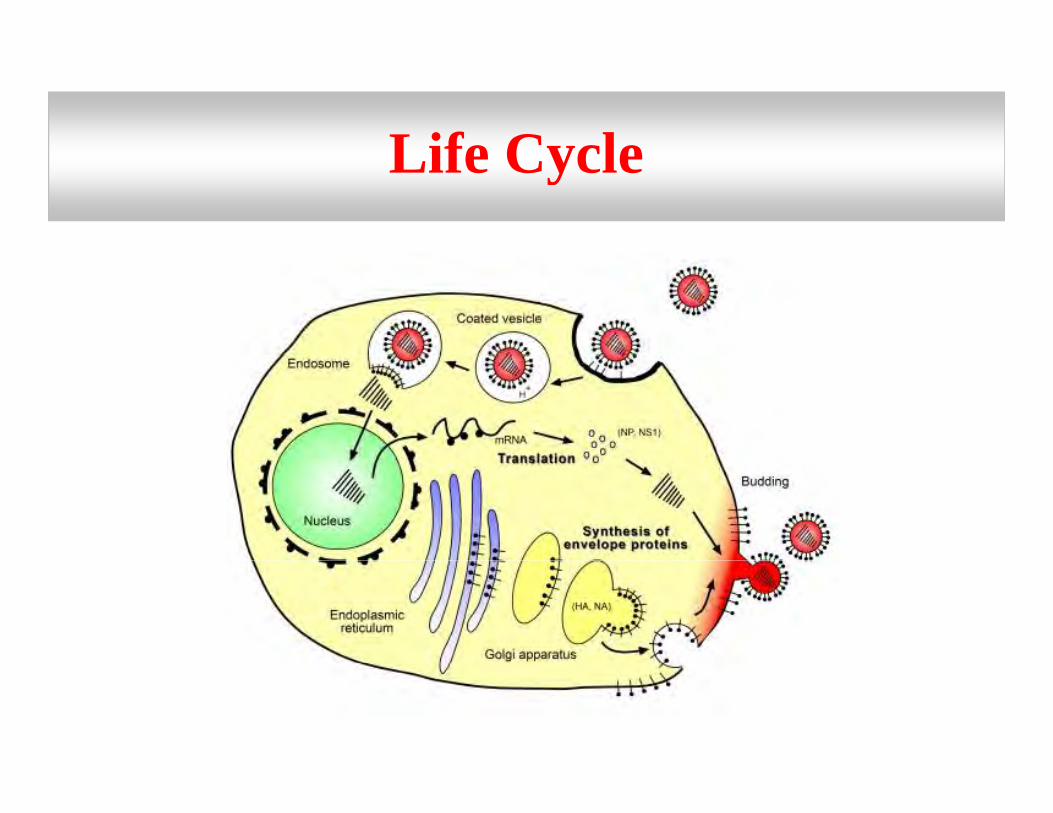
Life CycleLife Cycle
Viral ReplicationViral Replication
Progeny virions are released by budding
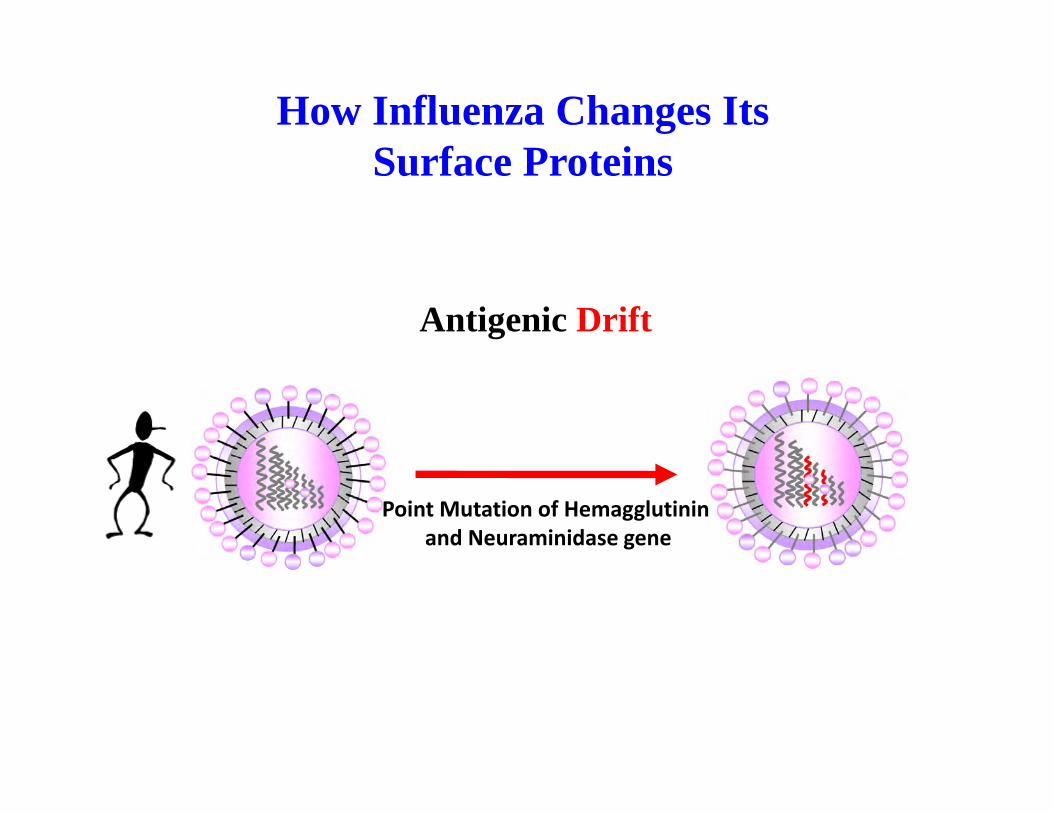
How Influenza Changes Its S f P t iSurface Proteins
Antigenic Drift
Point Mutation of Hemagglutinin and Neuraminidase gene
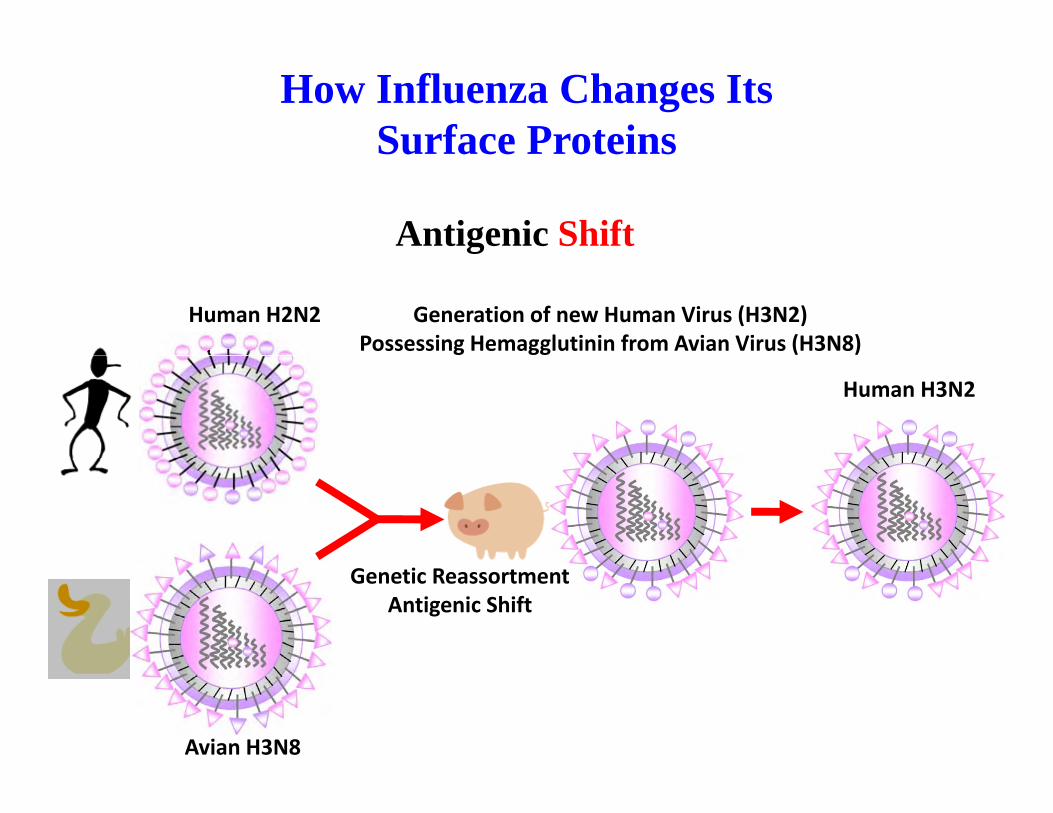
How Influenza Changes Its Surface ProteinsSurface Proteins
Antigenic Shiftg
Human H2N2 Generation of new Human Virus (H3N2)Possessing Hemagglutinin from Avian Virus (H3N8)
Human H3N2
Genetic ReassortmentAntigenic Shift
Avian H3N8
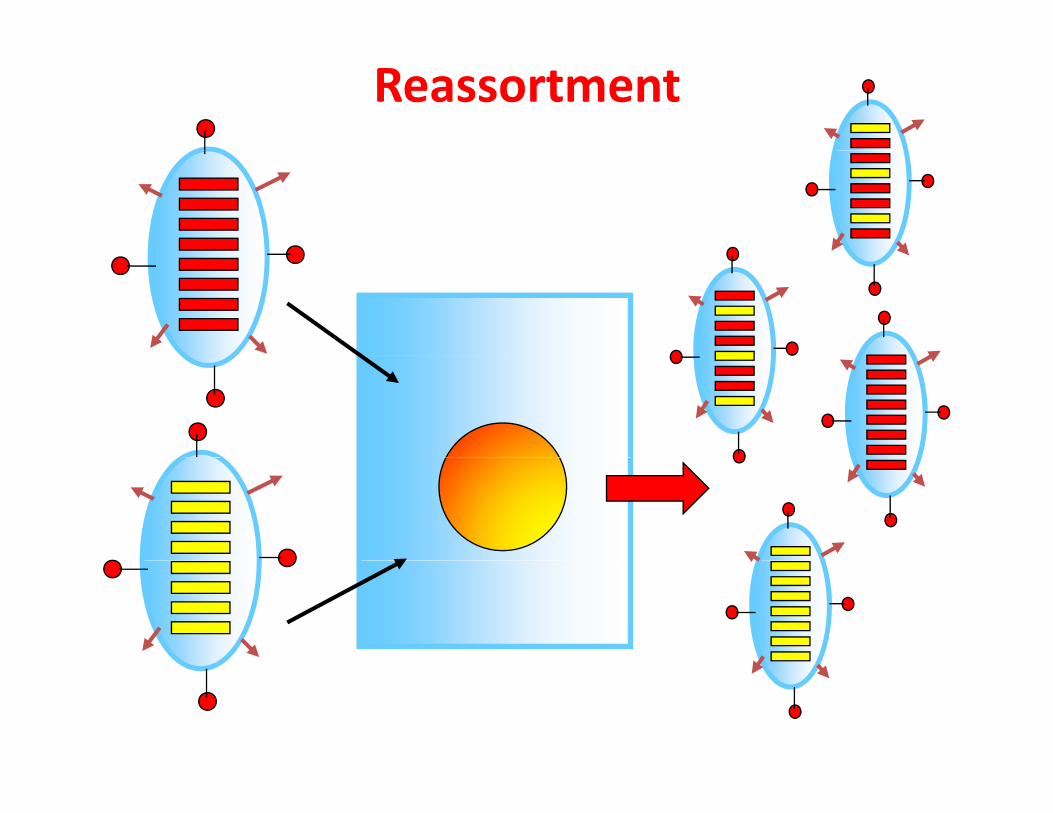
Reassortment
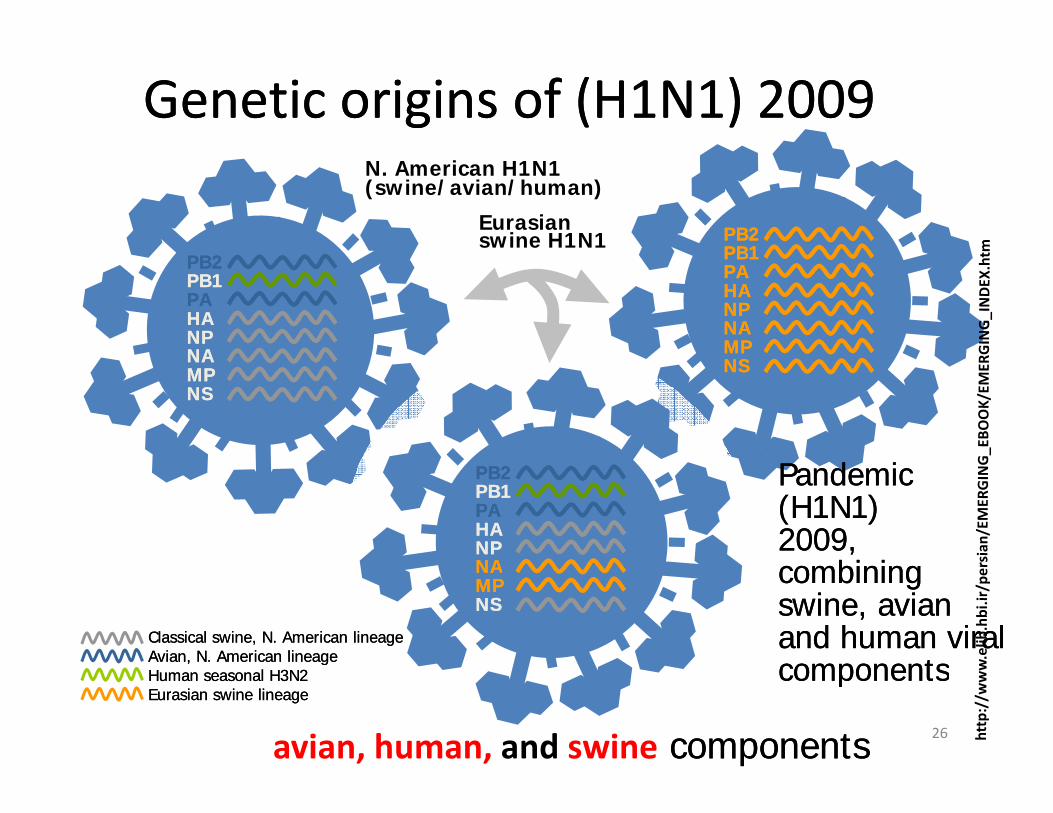
Genetic origins of (HGenetic origins of (H11NN11) ) 20092009
PBPB22PBPB11
Eurasian swine H1N1
N. American H1N1(swine/avian/human)
PBPB22PBPB11PAPAHAHANPNPNANA
PBPB11PAPAHAHANPNPNANAMPMPNANA
MPMPNSNS
NSNS
PBPB22PBPB11PAPAHAHANPNPNANA
Pandemic Pandemic (H(H11NN11) ) 20092009, ,
bi ibi iNANAMPMPNSNS
Classical swine, N. American lineageClassical swine, N. American lineageAvian, N. American lineageAvian, N. American lineage
combining combining swine, avian swine, avian and human viral and human viral componentscomponents
26
, g, gHuman seasonal HHuman seasonal H33NN22Eurasian swine lineageEurasian swine lineage
componentscomponents
avian, human, and swine componentscomponents
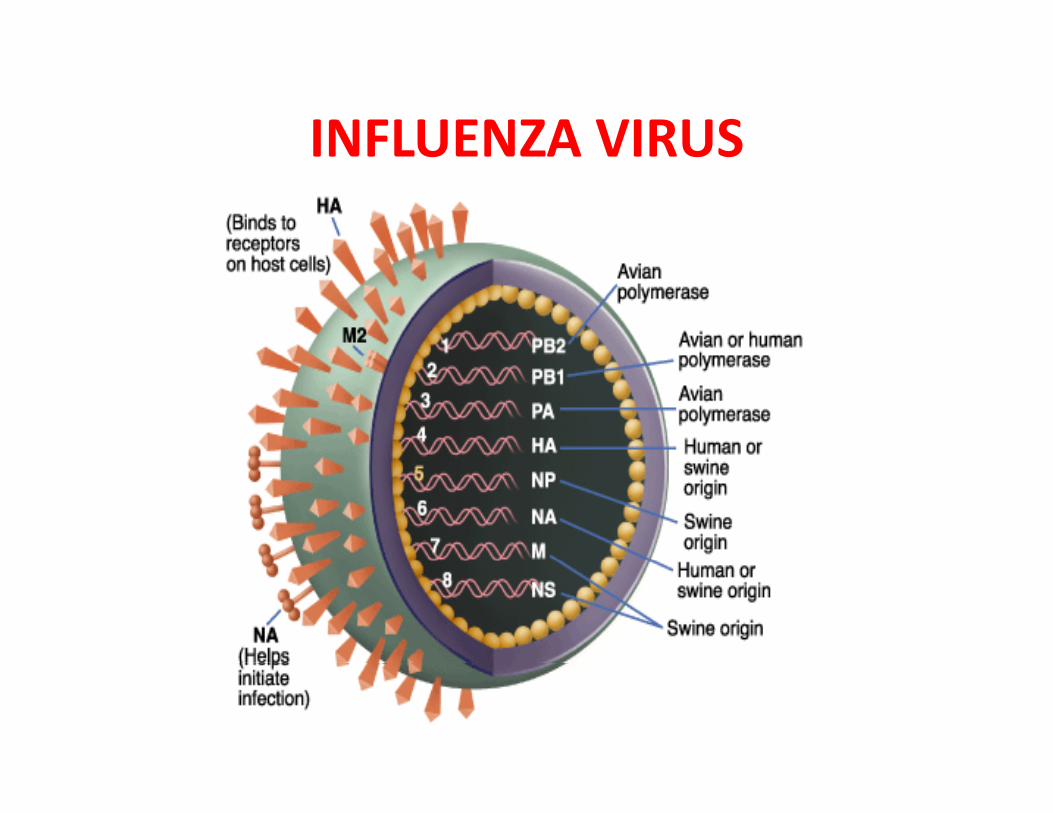
INFLUENZA VIRUSINFLUENZA VIRUS
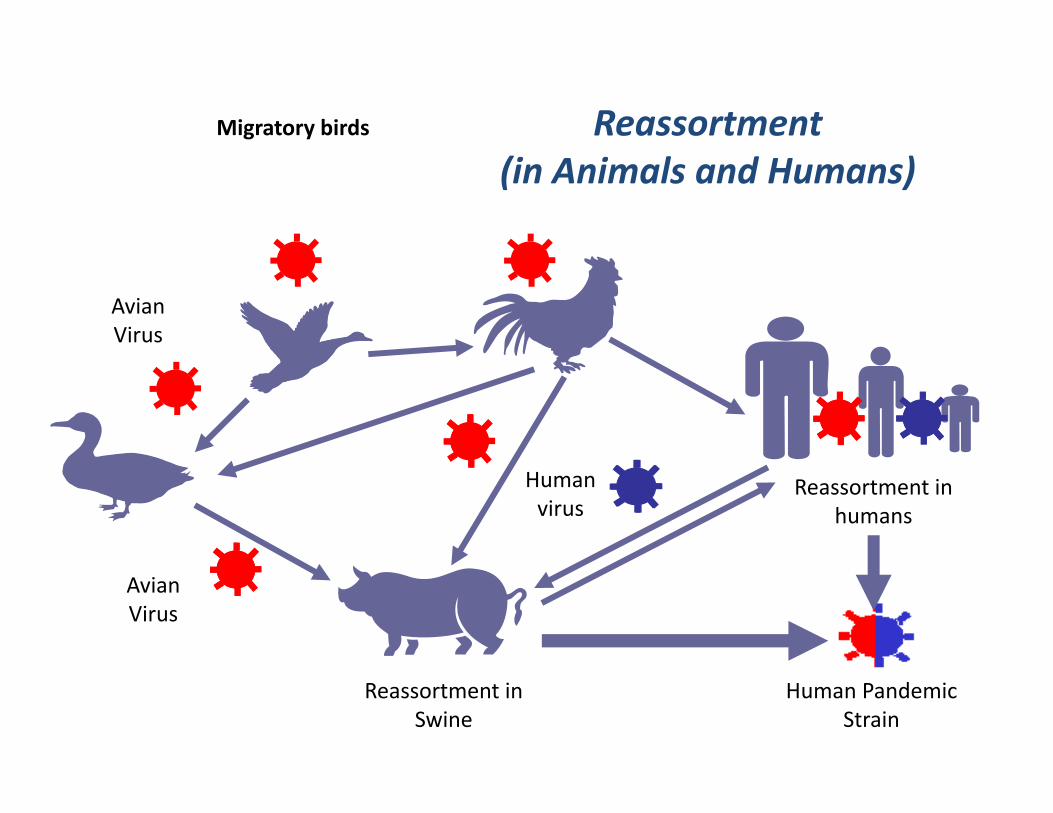
Reassortment Migratory birds
(in Animals and Humans)
Avian Virus
Human virus
Reassortment in humans
Avian Virus
Reassortment in Swine
Human Pandemic Strain
1918‐1919 influenza pandemic
EpidemiologyEpidemiology
• Pandemics - influenza A pandemics arise when a viruswith a new haemagglutinin subtype emerges as a resultgg yp gof antigenic shift. As a result, the population has noimmunity against the new strain. Antigenic shifts hadoccurred 3 times in the 20th centuryoccurred 3 times in the 20th century.
• Epidemics - epidemics of influenza A and B arisethrough more minor antigenic drifts as a result ofmutation.
Avian InfluenzaAvian InfluenzaH5N1• An outbreak of Avian Influenza H5N1 occurred in Hong Kong in
1997 h 18 i f d f hi h 6 di d1997 where 18 persons were infected of which 6 died.• The source of the virus was probably from infected chickens and the
outbreak was eventually controlled by a mass slaughter of chickensin the territoryin the territory.
• All strains of the infecting virus were totally avian in origin andthere was no evidence of reassortment.H th t i i l d hi hl i l t f th i t l• However, the strains involved were highly virulent for their naturalavian hosts.
H9N2H9N2 • Several cases of human infection with avian H9N2 virus occurred in
Hong Kong and Southern China in 1999.• The disease was mild and all patients made a complete recovery• The disease was mild and all patients made a complete recovery• Again, there was no evidence of reassortment
PreventionPrevention
• Inactivated and subunit vaccines are available againstInactivated and subunit vaccines are available againstinfluenza A and B.
• The vaccine is normally trivalent, consisting of one AH3N2 strain, one A H1N1 strain, and one B strain.
• The strains used are reviewed by the WHO each year.Th i h ld b i t d bilit t d d ld l• The vaccine should be given to debilitated and elderlyindividuals who are at risk of severe influenza infection.
• Amantidine can be used as an prophylaxis for thosep p ywho are allergic to the vaccine or during the periodbefore the vaccine takes effect.
Laboratory DiagnosisLaboratory Diagnosis• Rapid Diagnosis – nasopharyngeal aspirates, throat
d l b ll dand nasal swabs are normally used.– Antigen Detection – can be done by IFT or EIA– RNA Detection – RT-PCR assays give the best sensitivity and
specificity It is the only method that can differentiate the 2009specificity. It is the only method that can differentiate the 2009pandemic H1N1 strain from the seasonal H1N1 strain.However, it is expensive and technically demanding.
• Virus Isolation - virus may be readily isolated from• Virus Isolation - virus may be readily isolated fromnasopharyngeal aspirates and throat swabs.
• Serology - a retrospective diagnosis may be made byl CFT t id l d HAI d EIA bserology. CFT most widely used. HAI and EIA may be
used to give a type-specific diagnosis
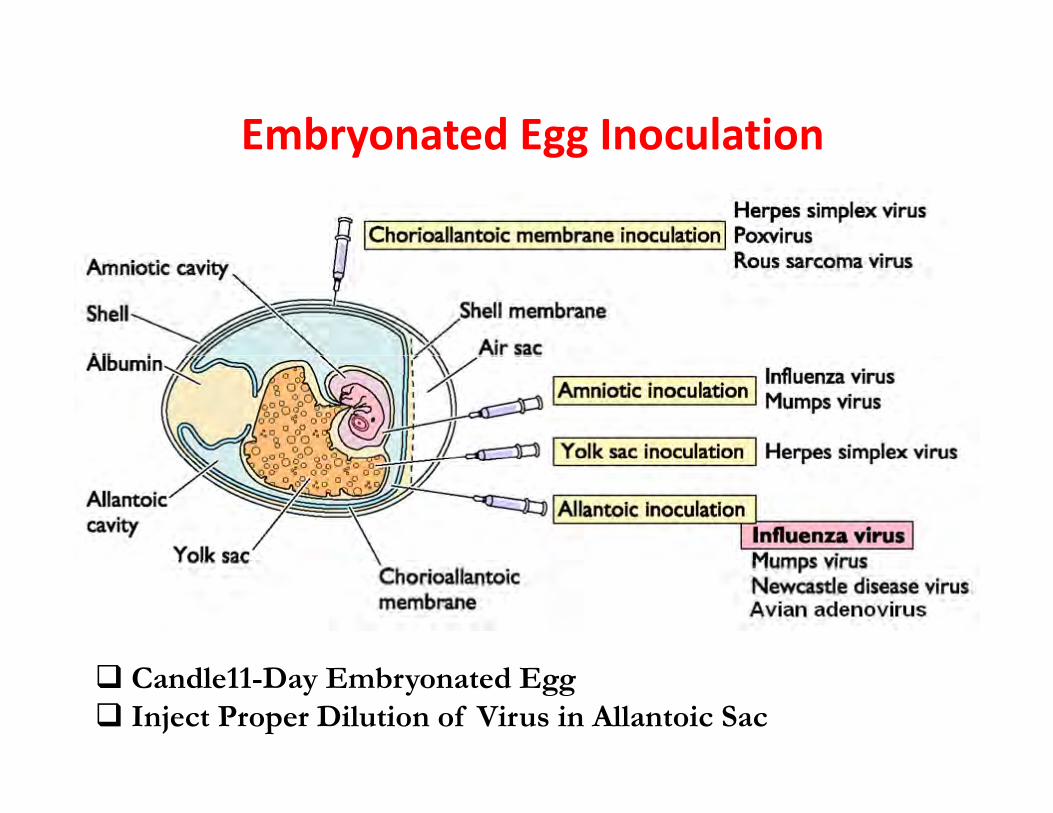
Embryonated Egg Inoculationy gg
Candle11-Day Embryonated EggInject Proper Dilution of Virus in Allantoic Sac
Alantoic Fluid Harvesting
•Harvest the Fluid•Harvest the Fluid•Centrifuge to Remove the Egg Stuff•HA Assay to titer the virus
Haemagglutination (HA)gg ( )
Virus Propagation in Cell Culture
MDCK C ll li Ad i
Virus Propagation in Cell Culture
MDCK Cell line AdaptationConfluent Monolayer Cell
l f l lInoculation of Serial Dilution of Virus to the Monolayer CPE Ob tiCPE ObservationHA Titration of Culture MediaH d tiHemadsorptionPlaque AssayC 0TCID50

MDCK Cell CultureMDCK Cell Culture
A non Infected MDCKB. A.
A. non Infected MDCKB. Influenza Infected MDCK
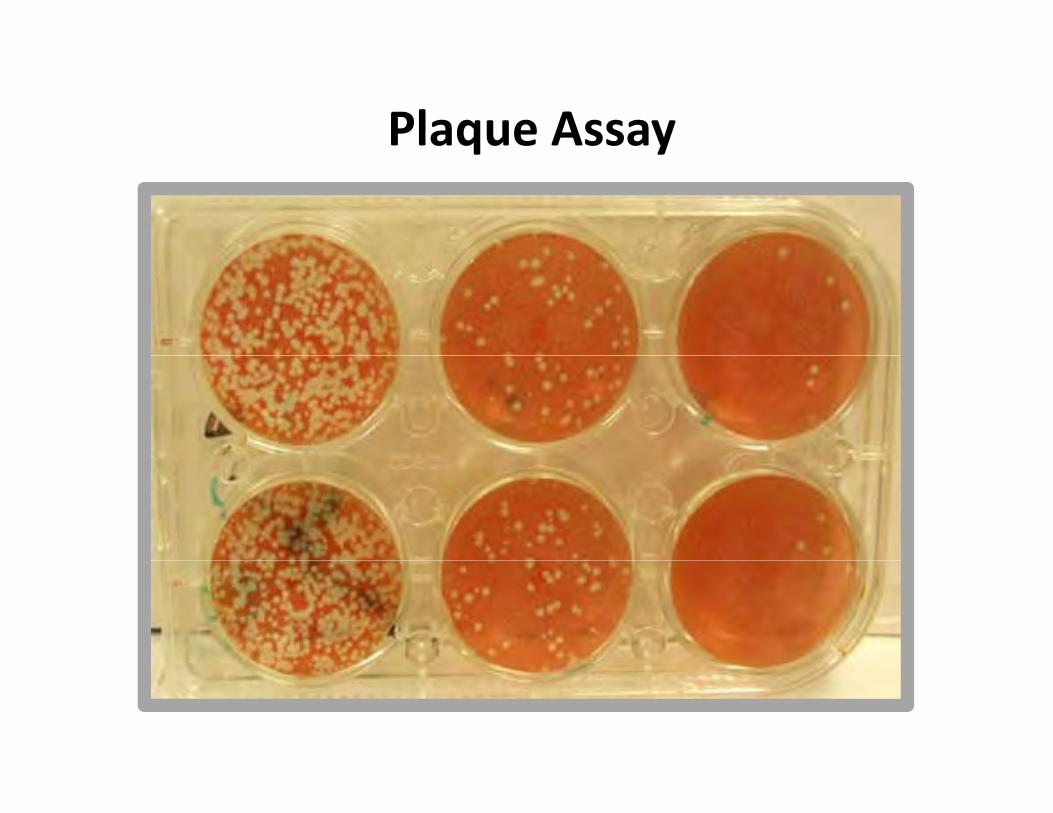
Plaque Assayq y
Molecular DiagnosisMolecular Diagnosis
Nasal & Pharynx Swab Sampling in
Transient MediaTransient Media
RNA Extraction
Multiplex RT-PCR Using Type- &
Subtype-Specific Primers
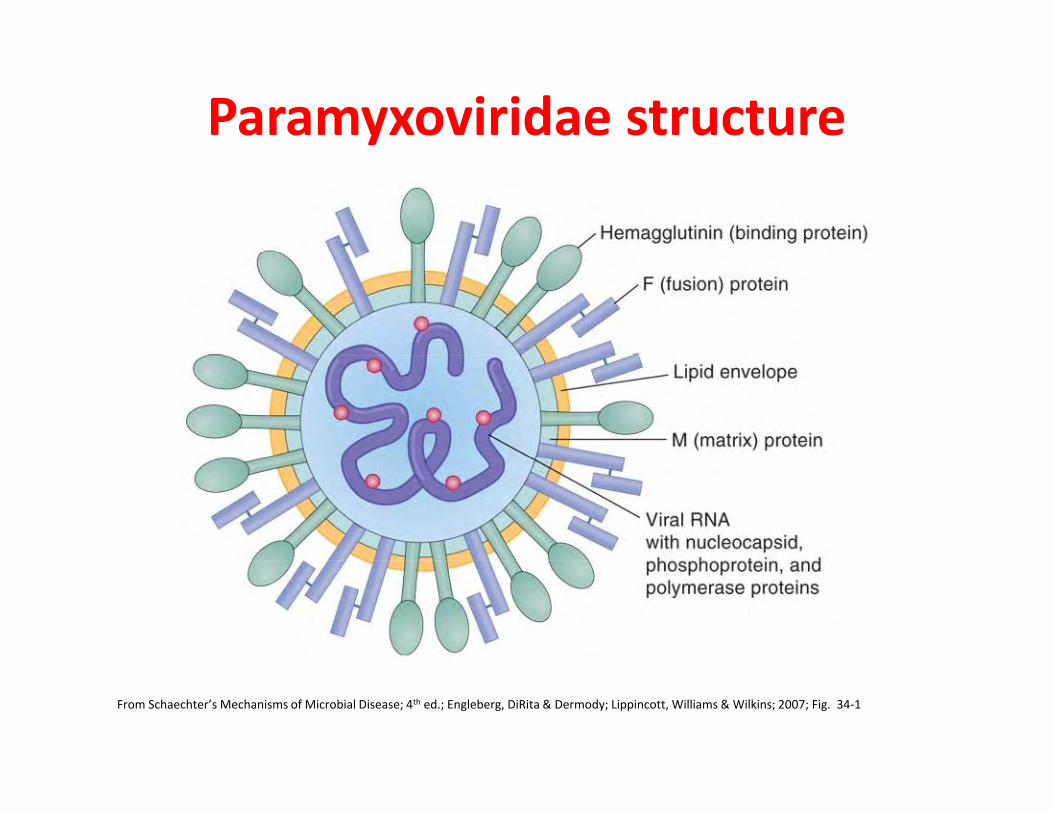
Paramyxoviridae structure
From Schaechter’s Mechanisms of Microbial Disease; 4th ed.; Engleberg, DiRita & Dermody; Lippincott, Williams & Wilkins; 2007; Fig. 34‐1
Paramyxovirus structureParamyxovirus structure
Paramyxovirus electron micrograph
http://web.uct.ac.za/depts/mmi/stannard/paramyx.html
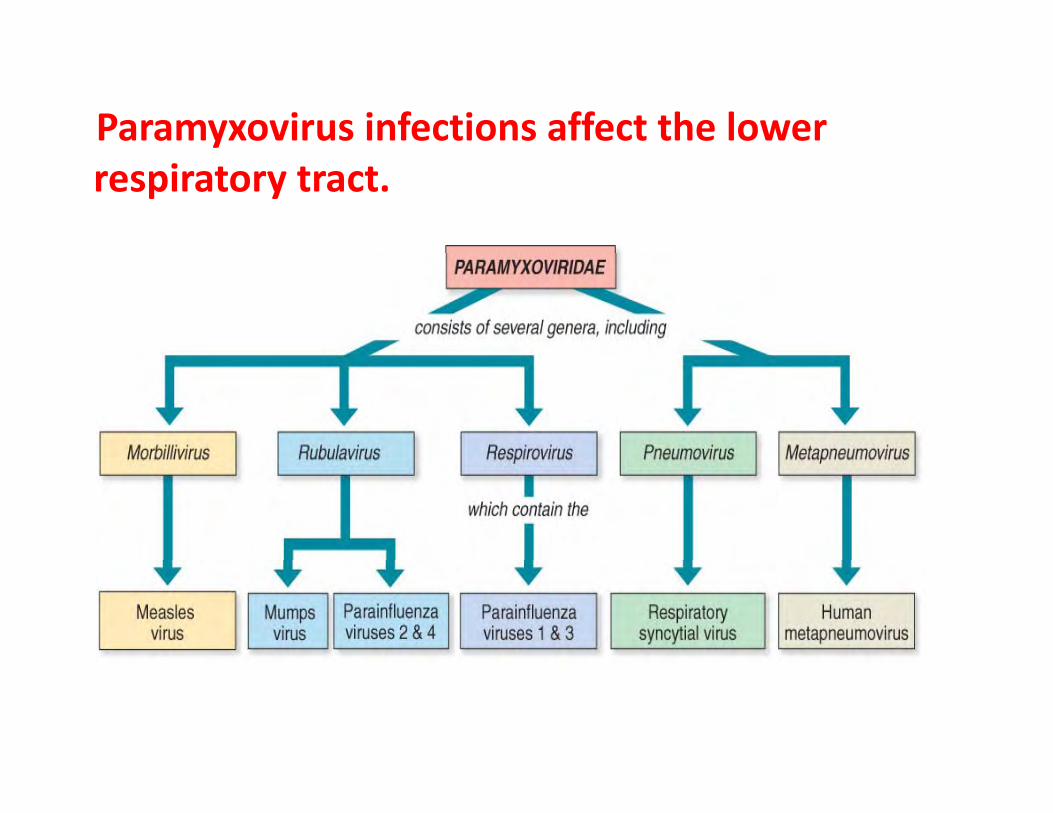
Paramyxovirus infections affect the lower respiratory tract.
Parainfluenza VirusParainfluenza Virus
• ssRNA virus• enveloped, pleomorphic
h lmorphology• 5 serotypes: 1, 2, 3, 4a and
4b
(Linda Stannard, University of Cape Town, S.A.)
PARAINFLUENZA VIRUSES
Croup (Acute Laryngotracheobronchitis) and
PARAINF U N A VIRUS S
Croup (Acute Laryngotracheobronchitis) and pneumonia in children
Common cold – like disease in adults.
5 bt 1 2 3 4 d 4b5 subtypes: 1, 2, 3, 4a and 4b
Surface spikes consist of H N and fusionSurface spikes consist of H, N and fusion proteins. H and N on the same spike while fusion protein is on a different spike.p p
EPIDEMIOLOGY
Transmission: respiratory droplets, winter thmonths.
Croup is the commonest clinical manifestation of parainfluenza virusmanifestation of parainfluenza virus infection, caused by subtypes 1 and 2. It occurs in children (below 3 years).It occurs in children (below 3 years).
Parainfluenza 3 is prone to produce bronchiolitis and pneumonia.
The majority of infections with parainfluenza viruses are subclinical.
Laboratory DiagnosisLaboratory DiagnosisCroup is a well‐defined, easily recognized clinical
entity• Detection of Antigen - a rapid diagnosis can be made by
the detection of parainfluenza antigen from
entity.
p gnasopharyngeal aspirates and throat washings.
• Virus Isolation - virus may be readily isolated fromy ynasopharyngeal aspirates and throat swabs.
• Serology - a retrospective diagnosis may be made byserology. CFT most widely used.
Respiratory Syncytial Virus (RSV)Respiratory Syncytial Virus (RSV)
RNA l d i• ssRNA eveloped virus.
• belong to the genus Pneumovirus of the P i f ilParamyxovirus family.
• Considerable strain variation exists, may be classified into subgroups A and B by monoclonal sera.
• Both subgroups circulate in the community at any one time.
• Causes a sizable epidemic each year.
EPIDEMIOLOGYRSV causes outbreaks of respiratory infections
every winter. y
RSV is a major nosocomial pathogen in pediatric wards.
The pathogen may be introduced by infectedThe pathogen may be introduced by infected infants who are admitted from the outside and adults, especially members of staff withand adults, especially members of staff with mild infections.
Infants at Risk of Severe InfectionInfants at Risk of Severe Infection
1. Infants with congenital heart disease - infants who were hospitalized within the first few days of life with congenital disease are particularly at risk. 2. Infants with underlying pulmonary disease - infants with underlying pulmonary disease, especially bronchopulmonary dysplasia, are at risk of developing prolonged infection with RSVprolonged infection with RSV.3. Immunocompromized infants - children who are immunosuppressed or have a congenital immunodeficiency di d l l i t t t di tdisease may develop lower respiratory tract disease at any age.
LABORATORY DIAGNOSISLABORATORY DIAGNOSIS
• Detection of Antigen - a rapid diagnosis can be made byg p g ythe detection of RSV antigen from nasopharyngealaspirates. A rapid diagnosis is important because of theavailability of therapyavailability of therapy
• Virus Isolation - virus may be readily isolated fromV us so at o v us ay be ead y so ated onasopharyngeal aspirates. However, this will takeseveral days.
• Serology - a retrospective diagnosis may be made byserology. CFT most widely used.serology. CFT most widely used.
LABORATORY DIAGNOSIS
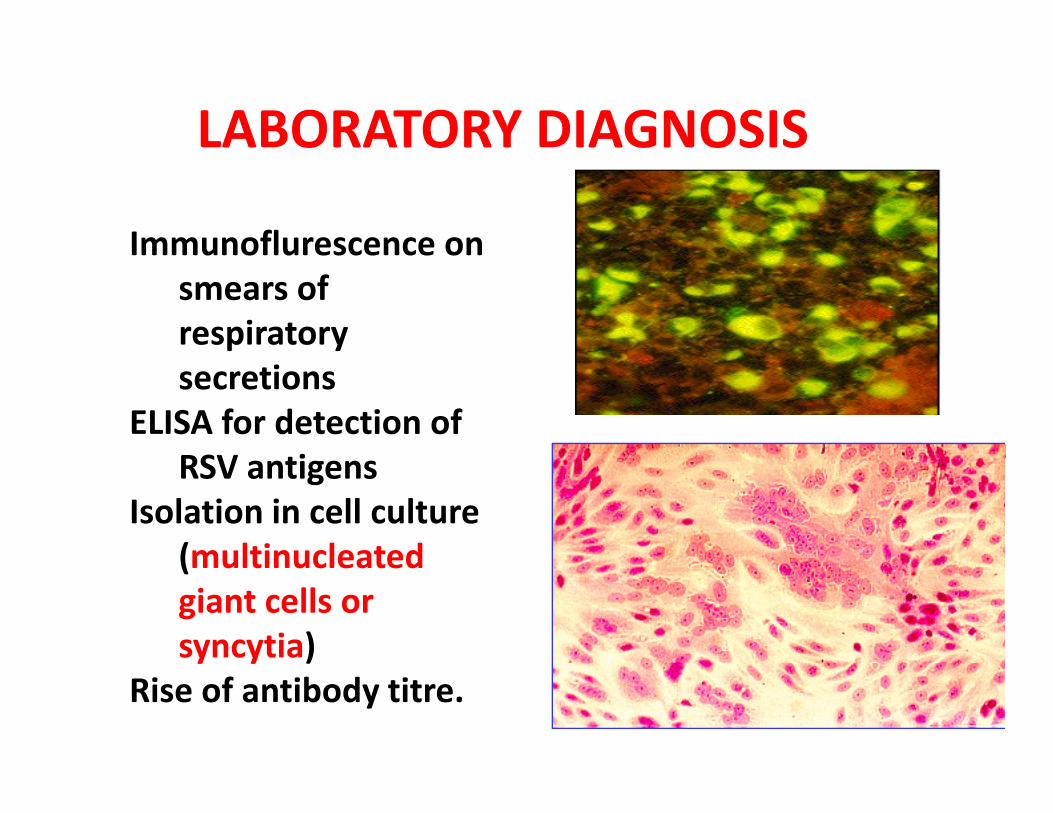
Immunoflurescence onImmunoflurescence on smears of respiratory secretions
ELISA for detection of RSV tiRSV antigens
Isolation in cell culture (multinucleated(multinucleated giant cells or syncytia) y y )
Rise of antibody titre.
Human MetapneumovirusHuman MetapneumovirusParamyxovirus first recognized in 2001hMPV and RSV in Pneumovirinae subfamily of the Paramyxoviridae family.2 major antigenic subgroups (A and B).Four major genotypes (A1,A2, B1,B2)It is about over 10% of all children with respiratory infection in winter.M h i h h iMay occur together with other virusesIt is mainly cause bronchopneumonia and bronchiolitis.
Human MetapneumovirusHuman Metapneumovirus
• Transmission likely by droplet spread.Transmission likely by droplet spread. – Healthcare associated infections documented
• Annual epidemics late winter early springAnnual epidemics late winter, early spring. – Coincides/overlaps with RSV season.Sporadic infection year round– Sporadic infection year round.
• Incubation period 3‐5 days.• Viral shedding 1 to 2 weeks• Viral shedding 1 to 2 weeks.
– Immunocompromised may shed for months.
Human metapneumovirus (hPMV)DIAGNOSIS
• antigen detectionantigen detection– commercially available
• PCR, culture– not yet commercially available
Human BocavirusHuman Bocavirus
• DNA virus family parvoviridae; firstDNA virus, family parvoviridae; first identified in 2005 in children with acute RTI.
• Name derives from similarity to bovine• Name derives from similarity to bovine parvovirus 1 and canine parvovirus. 2 di i d di• 2 distinct genotypes; no data regarding antigenic variation or distinct serotypes.
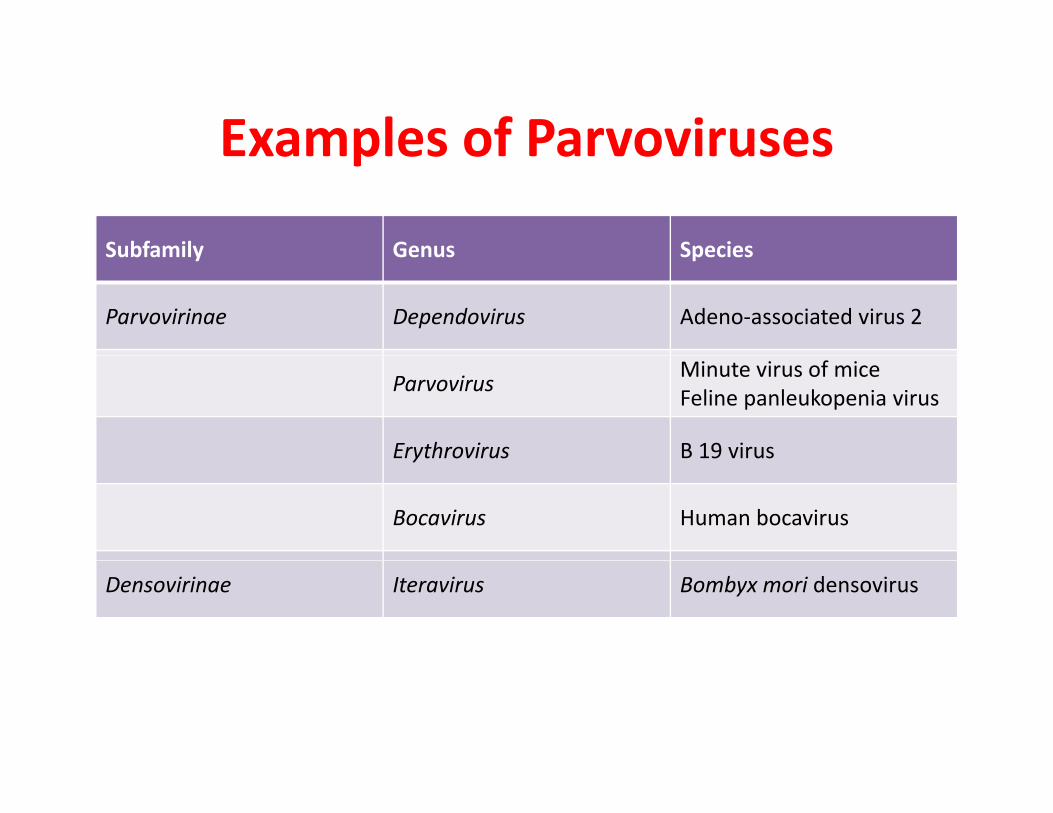
Examples of ParvovirusesExamples of Parvoviruses
Subfamily Genus SpeciesSubfamily Genus Species
Parvovirinae Dependovirus Adeno‐associated virus 2
Parvovirus Minute virus of miceFeline panleukopenia virus
Erythrovirus B 19 virusErythrovirus B 19 virus
Bocavirus Human bocavirus
Densovirinae Iteravirus Bombyx mori densovirus
Human BocavirusHuman Bocavirus
• Detection only described in humans.Detection only described in humans. • Transmission presumed respiratory secretions. • Duration of shedding not known• Duration of shedding not known. • Circulates worldwide and throughout the year. • Usually an issue in fall and winter• May cause bronchiolitis and pertussis‐like illness
Human BocavirusHuman Bocavirus
• Laboratory DiagnosisLaboratory Diagnosis• HBoV PCR and serology mostly used by research labsresearch labs.– Now included in commercial multiplex assays.
VIRAL IDENTIFICATIONVIRAL IDENTIFICATION
• Nasal wash or aspirateNasal wash or aspirate• Rapid antigen detection for RSV, parainfluenza influenza adenovirusparainfluenza, influenza, adenovirus (sensitivity 80‐90%)Di i fl• Direct immunofluorescence tests
• Culture• Serology• PCRPCR

Impact of Molecular Methods on lRespiratory Viral Diagnostics
• Much greater sensitivity vs culture and DFA. – Better understanding of epidemiology of respiratory viruses.
– Potential impacts on clinical care: less antibacterial ptherapy, shorter hospital stay, reduced mortality if earlier use of antivirals for influenza.
• Faster turnaround time – greater opportunity to guide therapy.
• Discovery of new viruses in respiratory tract in last decade– Metapneumovirusp– Multiple coronaviruses: SARS, 229E, NL63, OC43, HKU1. – Human bocavirus
• Viral coinfections recognised as a relatively common entity• Viral coinfections recognised as a relatively common entity.
Multiplex PCRMultiplex PCR
• Multiple viruses can cause same clinicalMultiple viruses can cause same clinical syndrome – Respiratory infections– Respiratory infections
• Can perform multiplex PCR assays to detect multiple viruses in one reactionmultiple viruses in one reaction.
• Commercial assays to detect up to 18 respiratory viruses in 1 test.
Multiplex PCRMultiplex PCR
• Multiplex–PCR System for the detection of 13Multiplex PCR System for the detection of 13 Respiratory Viruses (Influenza A/B virus, RSV A/B, Rhinovirus, Coronavirus OC43/HKU1, coronavirus229E/NL63, adenovirus, parainfluenza virus 1‐3m bocavirus, enterovirus